Rhode Island Exchange Planning March, 2012 Deb Faulkner Faulkner Consulting Group 1.
24
Rhode Island Exchange Planning March, 2012 Deb Faulkner Faulkner Consulting Group 1
-
Upload
clarissa-claudia-malloy -
Category
Documents
-
view
227 -
download
0
Transcript of Rhode Island Exchange Planning March, 2012 Deb Faulkner Faulkner Consulting Group 1.

Rhode Island Exchange Planning
March, 2012
Deb FaulknerFaulkner Consulting Group
1

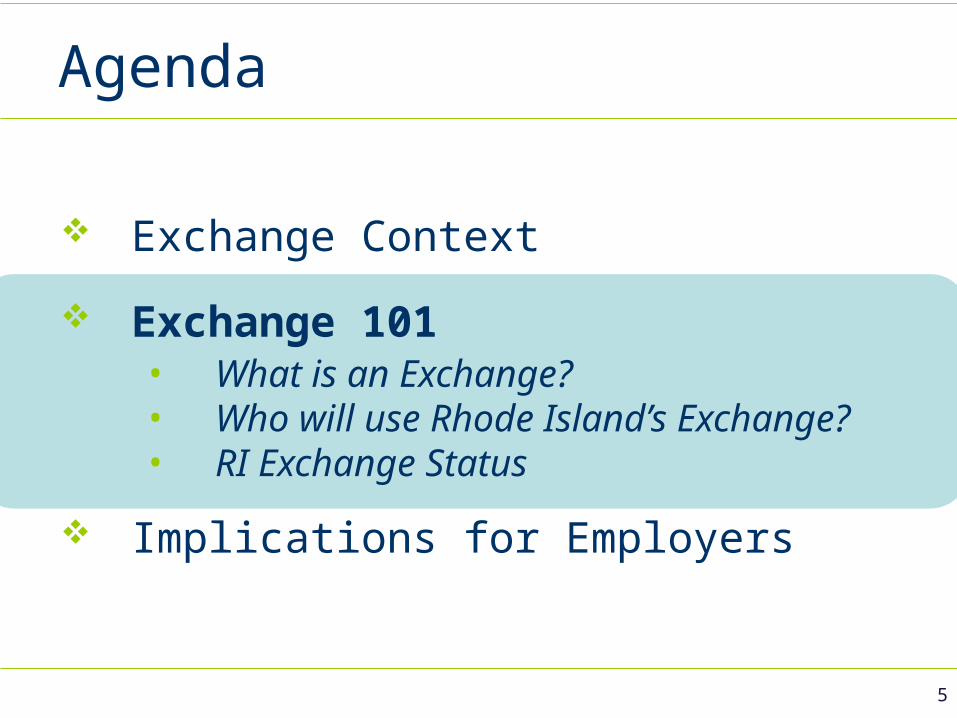
Agenda
Exchange Context
Exchange 101• What is an Exchange? • Who will use Rhode Island’s Exchange?• RI Exchange Status
Implications for Employers
2

Exchange Context
3
Federal reform, post 2014, envisions affordable coverage for virtually all RIers, through the following elements:
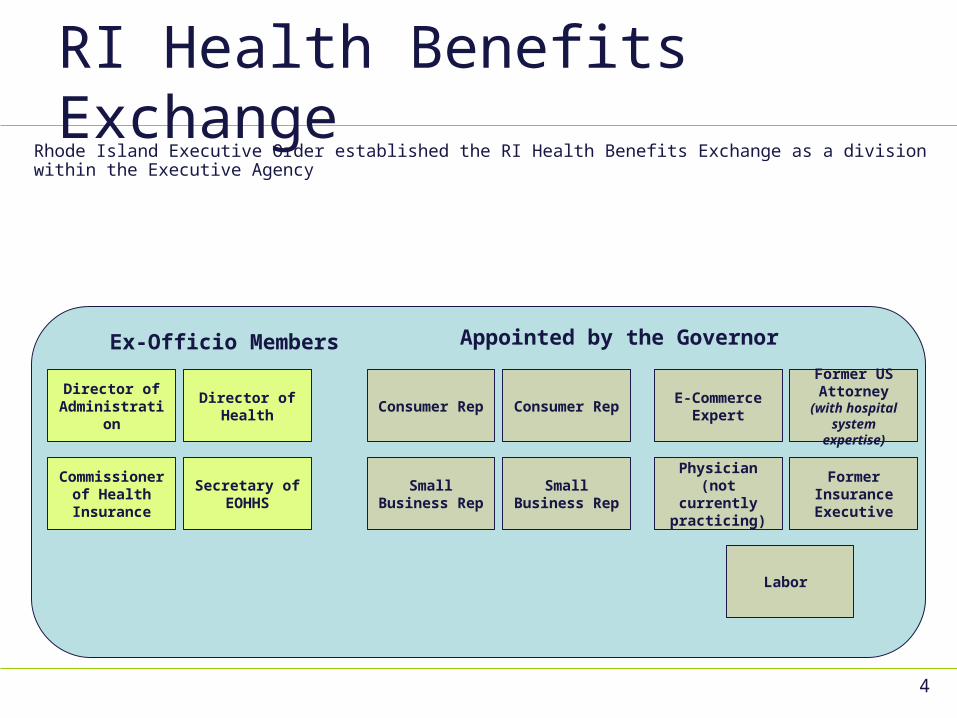
RI Health Benefits Exchange
4
Rhode Island Executive Order established the RI Health Benefits Exchange as a division within the Executive Agency
Director of
DOA
Commissioner
of Health
Insurance
Director of
Health
Small
Business
Rep
Small
Business
Rep
Consumer
Rep
Former Health
Insurance Executive
Labor
Former Delivery Sys Governance
Ex-Officio Members
E-Commerce Expert
Former Insurance Executive
Former US Attorney (with hospital system
expertise)
Physician (not currently
practicing)
Director of Administration
Secretary of EOHHS
Director of Health
Commissioner of Health Insurance
Appointed by the Governor
Consumer Rep Consumer Rep
Small Business Rep
Small Business Rep
Labor
Agenda
Exchange Context
Exchange 101• What is an Exchange? • Who will use Rhode Island’s Exchange?• RI Exchange Status
Implications for Employers
5

Why establish an Exchange?
6
Mission
The Rhode Island Health Benefits Exchange will
serve as a robust resource for Rhode Islanders and
Rhode Island businesses to learn about and easily
compare the quality and affordability of their health
insurance options, enroll in coverage and, if eligible,
access subsidies for coverage.

RI Exchange Goals
1. Improve the health of Rhode Islanders
2. Achieve near universal coverage
3. Favorably impact health insurance cost trends
4. Favorably impact health care delivery system
effectiveness and efficiency
5. Add value to employer health insurance
purchasing
7
Exchange Web Portal: Massachusetts
8

The RI Health Benefit Exchange
9
A robust marketplace for all Rhode Islanders
(1) Web Portal: a robust marketplace for all Rhode Islanders to identify health insurance options and purchase coverage
Medicaid eligible individuals
Subsidy eligible individuals
Individuals (self pay –
no subsidy)
Employees of Small Employers
Employees of Large Employers
Rhode Islanders seeking Health Insurance
(2) Help Rhode Islanders Choose Health InsuranceDisplay insurance options in an easy
to understand, highly interactive web page
(3) EnrollDetermine eligibility,enroll in coverage, &
facilitate subsidy
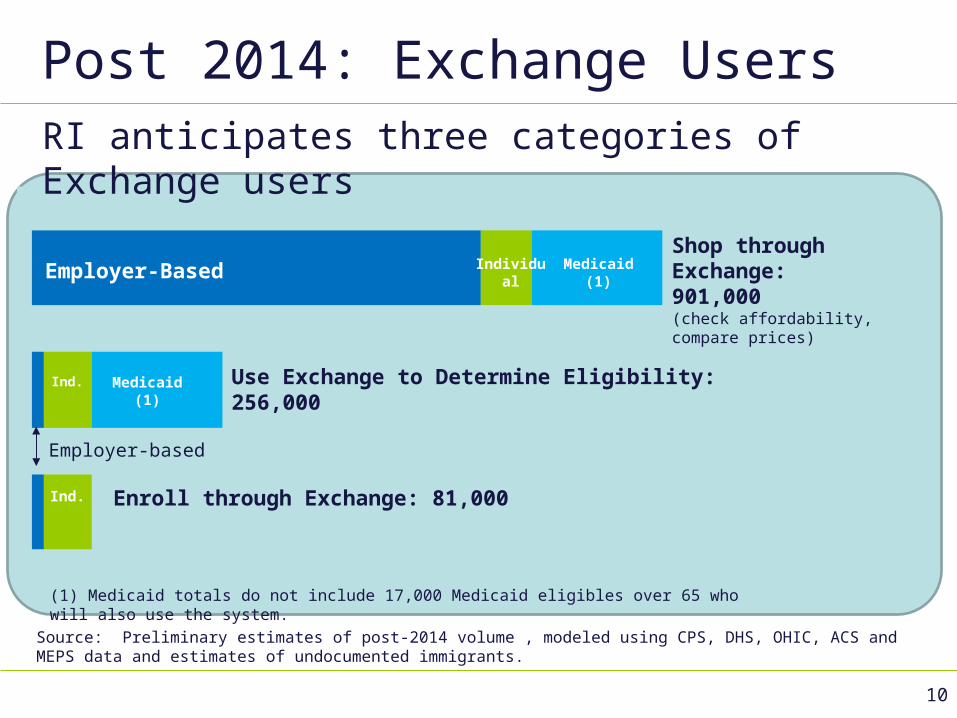
Post 2014: Exchange Users
Employer-Based Medicaid (1)
IndividualShop through Exchange: 901,000(check affordability, compare prices)
Use Exchange to Determine Eligibility: 256,000
Enroll through Exchange: 81,000
Medicaid (1)
Ind.
Ind.
Employer-based
Source: Preliminary estimates of post-2014 volume , modeled using CPS, DHS, OHIC, ACS and MEPS data and estimates of undocumented immigrants.
RI anticipates three categories of Exchange users
(1) Medicaid totals do not include 17,000 Medicaid eligibles over 65 who will also use the system.
10
Exchange Project StatusAchieving our mission requires an aggressive change initiative impacting:
Policy: business policy, practices and processes
Operations: people, roles & organizational structures
Technology: the systems that support the new policies & practices
11
Agenda
Exchange Context
Exchange 101• What is an Exchange? • Who will use Rhode Island’s Exchange?• RI Exchange Status
Implications for Employers
12
Implications for Employers
Individual Mandate
Employer Penalties (over 50), Tax Credits (Under 25)
Commercial Market Reforms
Essential Health Benefits
Exchange: SHOP (Small Business Health Options Program)Individual Exchange
Key Elements of ACA: Implications for Employers
13

Next Steps
14
Less than 18 months from today - need fully operational exchange
Fall 2012 “Operational Readiness”
January 2013 Achieve certification
Summer 2013 Soft Launch
October 2013 Open enrollment begins
December 2014 Exchange Establishment funding ends
December 2015 Medicaid funding (90% federal match) ends
Backup
15

Exchange Principles
Exceptional Customer Experience
Simplicity
Affordability
Flexibility
Transparency
Fiscal Prudence
Alignment with other governmental health reform initiatives
Catalyst16
Small Employer Tax Credits
17
Small employers will need to purchase insurance through the SHOP Exchange to access tax credits.
Who is EligibleEmployers with <25 employees with average wages of up to $50,000
Amount of CreditSliding scale up to 50% of the amount they contribute toward insurance premiums
SHOP Requirement (after 2014)In order to receive the credit after 2014, small employers must purchase through the state’s SHOP Exchange.
TimingCredits are available starting in 2010. Employers may only receive the credit for 2 years after 2013.
Source: Health Policy Brief: Small Business Tax Credits, Health Affairs, Jan 14, 2011, Robert Wood Johnson Foundation
Employer Penalties
WhoBusinesses with 51 or more FTEs
Penalty$2,000 per employee (excluding the first 30 employees) if they do not offer coverage for employees who average 30+ hours per week.1
CoverageMust cover at least 60% of the actuarial value of the cost of benefits.
Affordability RequirementEmployee’s premium cannot exceed 9.5% of their household income. If not, employees may purchase insurance on their own through the exchange using
tax credits. Employers will either pay $3,000 per employee receiving the tax credit, or $2,000 per
employee excluding the first 30 workers (whichever is less).
18
Beginning in 2014, some small businesses may have to pay a penalty if they do not offer affordable coverage.
1 Note that there is no penalty for part-time employees not offered coverage.Source: Kaiser Family Foundation employer penalty flowchart

Individual Mandate
Who is exempted from the requirement to purchase insurance? Religiously opposed to acceptance of benefits from a health insurance policy Undocumented immigrants Persons who are incarcerated Members of an Indian tribe Income below the threshold requiring filing a tax return ($9,350 - individual, $18,700 - family) Anyone who has to pay more than 8% of income for health insurance, after taking into account any employer contributions or tax credits.
What insurance coverage is acceptable? Medicare/Medicaid/CHIP TRICARE or veteran’s health program A plan offered by an employer Insurance bought directly that is at least at the Bronze level A grandfathered health plan in existence before the health reform law was enacted
What is the penalty for not having insurance? 1
2014: $95/adult, $47.50/child ($285 family max) or 1% of family income, whichever is greater 2015: $325/adult, $162.50/child ($975 family max) or 2% of family income, whichever is greater. 2016 and Beyond: $695/adult, $347.50/child ($2,085 family max) or 2.5% of family income, whichever is greater. After 2016, penalty
amounts are increased annually by the cost of living.
191 The penalty is pro-rated by the number of months without coverage, though there is no penalty for a single gap in coverage of less than 3 months in a year. The penalty cannot be greater than the national average premium for Bronze level coverage in an Exchange .
Source: Kaiser Family Foundation individual mandate flowchart

Context: Commercial Reforms
Young adults on parents’ coverage
Pre-existing condition protections
New restrictions on rate factors
“Essential benefits”
Making health insurance accessible to all, leveling the playing field
20

Starting Point
21Source: Census Bureau American Community Survey 2009, RI Medicaid, Commercial insurance data as reported to OHIC, Large Group/SI includes both carrier reported data and additional subscribers based on ACS data for total privately insured population.
Under 65 RI Population: Current Health Insurance StatusTotal = 901,000
(1) Medicaid total does not include 17,000 eligibles over 65. (2) Chart uninsured total based on ACS 2009 data. ACS data for 2010 shows 126,000 uninsured, mostly at lower incomes.

Work to Date: Policy
22
Populations Served
How Best to Serve Individuals
How Best to Serve Small Businesses

Work to Date: Operations
Detailed workplan for operationalizing RI’s Exchange by 2014
Business requirements
Business process designfocused on efficiencies across agencies, improved consumer experience
23
Work to Date: Technology
Translating business requirements into technical requirements
Technology “Gap Analysis”
New England Collaborative – Innovator grant
24