
Revo MRI Pacing System - Medtronic · Specifically engineered for MRI safety, with reliable lead...
12
www.medtronic.com Medtronic, Inc. 710 Medtronic Parkway Minneapolis, MN 55432-5604 USA Tel: (763) 514-4000 Fax: (763) 514-4879 Medtronic USA, Inc. Toll-free: 1 (800) 328-2518 (24-hour technical support for physicians and medical professionals) ENGINEERED WITH SURESCAN® TECHNOLOGY FDA-approved for MRI use The first pacing system to break the image barrier Revo MRI ™ Pacing System The Revo MRI SureScan pacing system is MR Conditional designed to allow patients to undergo MRI under the specified conditions for use. A complete system, consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan leads is required for use in the MRI environment. UC201004103b EN © Medtronic, Inc. 2012. Minneapolis, MN. All Rights Reserved. Printed in USA. 07/2012 Brief Statement The Revo MRI® SureScan® pacing system is MR Conditional and as such is designed to allow patients to undergo MRI under the specified conditions for use. Indications: The Revo MRI SureScan Model RVDR01 IPG is indicated for use as a system consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan 5086MRI leads. A complete system is required for use in the MRI environment. The Revo MRI SureScan Model RVDR01 IPG is indicated for the following: • Rate adaptive pacing in patients who may benefit from increased pacing rates concurrent with increases in activity • Accepted patient conditions warranting chronic cardiac pacing include: – Symptomatic paroxysmal or permanent second- or third- degree AV block – Symptomatic bilateral bundle branch block – Symptomatic paroxysmal or transient sinus node dysfunctions with or without associated AV conduction disorders – Bradycardia-tachycardia syndrome to prevent symptomatic bradycardia or some forms of symptomatic tachyarrhythmias The device is also indicated for dual chamber and atrial tracking modes in patients who may benefit from maintenance of AV synchrony. Dual chamber modes are specifically indicated for treatment of conduction disorders that require restoration of both rate and AV synchrony, which include: • Various degrees of AV block to maintain the atrial contribution to cardiac output • VVI intolerance (for example, pacemaker syndrome) in the presence of persistent sinus rhythm Antitachycardia pacing (ATP) is indicated for termination of atrial tachyarrhythmias in bradycardia patients with one or more of the above pacing indications. Atrial rhythm management features such as Atrial Rate Stabilization (ARS), Atrial Preference Pacing (APP), and Post Mode Switch Overdrive Pacing (PMOP) are indicated for the suppression of atrial tachyarrhythmias in bradycardia patients with atrial septal lead placement and one or more of the above pacing indications. Contraindications: The device is contraindicated for: • Implantation with unipolar pacing leads • Concomitant implantation with another bradycardia device • Concomitant implantation with an implantable cardioverter defibrillator There are no known contraindications for the use of pacing as a therapeutic modality to control heart rate. The patient’s age and medical condition, however, may dictate the particular pacing system, mode of operation, and implantation procedure used by the physician. • Rate responsive modes may be contraindicated in those patients who cannot tolerate pacing rates above the programmed Lower Rate • Dual chamber sequential pacing is contraindicated in patients with chronic or persistent supraventricular tachycardias, including atrial fibrillation or flutter • Single chamber atrial pacing is contraindicated in patients with an AV conduction disturbance • ATP therapy is contraindicated in patients with an accessory antegrade pathway Warnings and Precautions: Changes in patient’s disease and/or medications may alter the efficacy of the device’s programmed parameters. Patients should avoid sources of magnetic and electromagnetic radiation to avoid possible underdetection, inappropriate sensing and/or therapy delivery, tissue damage, induction of an arrhythmia, device electrical reset, or device damage. Do not place transthoracic defibrillation paddles directly over the device. Use of the device should not change the application of established anticoagulation protocols. Patients and their implanted systems must be screened to meet the MRI Conditions of Use. Do not scan patients who do not have a complete Revo MRI SureScan pacing system consisting of a SureScan device and two SureScan leads; patients who have previously implanted devices, or broken or intermittent leads; or patients who have a lead impedance value of < 200 Ω or > 1,500 Ω. Do not scan patients with a SureScan pacing system implanted in sites other than the left and right pectoral region; or patients positioned such that the isocenter (center of MRI bore) is inferior to C1 vertebra and superior to the T12 vertebra. Potential Complications: Potential complications include, but are not limited to, rejection phenomena, erosion through the skin, muscle or nerve stimulation, oversensing, failure to detect and/or terminate arrhythmia episodes, acceleration of tachycardia, and surgical complications such as hematoma, infection, inflammation, and thrombosis. Potential lead complications include, but are not limited to, valve damage, fibrillation, thrombosis, thrombotic and air embolism, cardiac perforation, heart wall rupture, cardiac tamponade, pericardial rub, infection, myocardial irritability, and pneumothorax. Other potential complications related to the lead may include lead dislodgement, lead conductor fracture, insulation failure, threshold elevation, or exit block. The SureScan system has been designed to minimize potential complications in the MRI environment. Potential MRI complications include, but are not limited to, lead electrode and/or device heating which may cause tissue damage, impact the pacing system functionality such as failure to detect/treat irregular heartbeats, or potential for VT/VF induction. See the device manuals before performing an MRI Scan for detailed information regarding the implant procedure, indications, MRI conditions of use, contraindications, warnings, precautions, and potential complications/adverse events. For further information, call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at www.medtronic.com. Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
Transcript of Revo MRI Pacing System - Medtronic · Specifically engineered for MRI safety, with reliable lead...

www.medtronic.com
Medtronic, Inc.710 Medtronic ParkwayMinneapolis, MN 55432-5604 USATel: (763) 514-4000 Fax: (763) 514-4879
Medtronic USA, Inc. Toll-free: 1 (800) 328-2518(24-hour technical support for physicians and medical professionals)
ENGINEERED WITH SURESCAN® TECHNOLOGY FDA-approved for MRI use The first pacing system to break the image barrier
Revo MRI™ Pacing System
The Revo MRI SureScan pacing system is MR Conditional designed to allow patients to undergo MRI under the specified conditions for use. A complete system, consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan leads is required for use in the MRI environment.
UC
2010
0410
3b E
N ©
Med
tron
ic, I
nc. 2
012.
Min
neap
olis
, MN
. All
Righ
ts R
eser
ved.
Prin
ted
in U
SA. 0
7/20
12
Brief Statement The Revo MRI® SureScan® pacing system is MR Conditional and as such is designed to allow patients to undergo MRI under the specified conditions for use.Indications: The Revo MRI SureScan Model RVDR01 IPG is indicated for use as a system consisting of a Medtronic Revo MRI SureScan IPG implanted with two CapSureFix MRI® SureScan 5086MRI leads. A complete system is required for use in the MRI environment.The Revo MRI SureScan Model RVDR01 IPG is indicated for the following:• Rate adaptive pacing in patients who may benefit from
increased pacing rates concurrent with increases in activity• Accepted patient conditions warranting chronic cardiac
pacing include: – Symptomatic paroxysmal or permanent second- or third-
degree AV block – Symptomatic bilateral bundle branch block – Symptomatic paroxysmal or transient sinus node
dysfunctions with or without associated AV conduction disorders
– Bradycardia-tachycardia syndrome to prevent symptomatic bradycardia or some forms of symptomatic tachyarrhythmias
The device is also indicated for dual chamber and atrial tracking modes in patients who may benefit from maintenance of AV synchrony. Dual chamber modes are specifically indicated for treatment of conduction disorders that require restoration of both rate and AV synchrony, which include:• Various degrees of AV block to maintain the atrial contribution to cardiac output
• VVI intolerance (for example, pacemaker syndrome) in the presence of persistent sinus rhythm
Antitachycardia pacing (ATP) is indicated for termination of atrial tachyarrhythmias in bradycardia patients with one or more of the above pacing indications.Atrial rhythm management features such as Atrial Rate Stabilization (ARS), Atrial Preference Pacing (APP), and Post Mode Switch Overdrive Pacing (PMOP) are indicated for the suppression of atrial tachyarrhythmias in bradycardia patients with atrial septal lead placement and one or more of the above pacing indications.
Contraindications: The device is contraindicated for:• Implantation with unipolar pacing leads• Concomitant implantation with another bradycardia
device• Concomitant implantation with an implantable
cardioverter defibrillator
There are no known contraindications for the use of pacing as a therapeutic modality to control heart rate. The patient’s age and medical condition, however, may dictate the particular pacing system, mode of operation, and implantation procedure used by the physician.• Rate responsive modes may be contraindicated in those
patients who cannot tolerate pacing rates above the programmed Lower Rate
• Dual chamber sequential pacing is contraindicated in patients with chronic or persistent supraventricular tachycardias, including atrial fibrillation or flutter
• Single chamber atrial pacing is contraindicated in patients with an AV conduction disturbance
• ATP therapy is contraindicated in patients with an accessory antegrade pathway
Warnings and Precautions: Changes in patient’s disease and/or medications may alter the efficacy of the device’s programmed parameters. Patients should avoid sources of magnetic and electromagnetic radiation to avoid possible underdetection, inappropriate sensing and/or therapy delivery, tissue damage, induction of an arrhythmia, device electrical reset, or device damage. Do not place transthoracic defibrillation paddles directly over the device. Use of the device should not change the application of established anticoagulation protocols.Patients and their implanted systems must be screened to meet the MRI Conditions of Use. Do not scan patients who do not have a complete Revo MRI SureScan pacing system consisting of a SureScan device and two SureScan leads; patients who have previously implanted devices, or broken or intermittent leads; or patients who have a lead impedance value of < 200 Ω or > 1,500 Ω. Do not scan patients with a SureScan pacing system implanted in sites other than the left and right pectoral region; or patients positioned such that the isocenter (center of MRI bore) is inferior to C1 vertebra and superior to the T12 vertebra.
Potential Complications: Potential complications include, but are not limited to, rejection phenomena, erosion through the skin, muscle or nerve stimulation, oversensing, failure to detect and/or terminate arrhythmia episodes, acceleration of tachycardia, and surgical complications such as hematoma, infection, inflammation, and thrombosis. Potential lead complications include, but are not limited to, valve damage, fibrillation, thrombosis, thrombotic and air embolism, cardiac perforation, heart wall rupture, cardiac tamponade, pericardial rub, infection, myocardial irritability, and pneumothorax. Other potential complications related to the lead may include lead dislodgement, lead conductor fracture, insulation failure, threshold elevation, or exit block. The SureScan system has been designed to minimize potential complications in the MRI environment. Potential MRI complications include, but are not limited to, lead electrode and/or device heating which may cause tissue damage, impact the pacing system functionality such as failure to detect/treat irregular heartbeats, or potential for VT/VF induction.See the device manuals before performing an MRI Scan for detailed information regarding the implant procedure, indications, MRI conditions of use, contraindications, warnings, precautions, and potential complications/adverse events. For further information, call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at www.medtronic.com.Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.

Specifically engineered for MRI safety, with reliable lead technology and a proven pacemaker platform – this is state-of-the-art pacing.
Now your patients get proven cardiac care with MRI access.
The First and Only Pacing System FDA-Approved for MRI Use
MRI D
evelopment Program
1997 2001 2004 2005 2006 2007 2009
Initiated research
Began technology work with international
experts
Commenced formaldiscussions with regulatory bodies
(TUV, FDA…)
Completed first system modifications; started extensive test
program
Finalized device modifications;
defined human clinical trial 2011
Revo MRI pacing system receives
FDA approval Commenced worldwide 1st-generation Revo MRI SureScan pacing system
clinical trial
Clinical trial completed

Pacemaker Implants in an Aging Population• The number of pacemakers currently implanted in the United States is approximately 1.5 million1,2
Meeting the Need for MRI
The Pacemaker Population
Average Age of Pacemaker Patient
13%Age 25–64 86%
Age 65+
Elderly patients are the primary users of MRI: individuals over age 65 are twice as likely to need an MRI compared to younger recipients.3

DEVICE CHOICE
Cardiologist Electrophysiologist
Comprehensive Care
• Given that 85% of all pacemaker patients have one or more comorbidities, facilitating comprehensive multi-specialty care is important in today’s environment
Number of Comorbidities in Pacemaker Patients
Part of Comprehensive Patient Care• Now, for the first time, you can implant a state-of-the-art pacing
system to provide proven cardiac care AND MRI access when your patients need it
Medical and Surgical Specialties Rely on MRI for Diagnosis.
• Your choice can affect their decisions and diagnostic capabilities
15%0 comorbidities
27%3 or more
comorbidities
30%1 comorbidity
28%2 comorbidities
85%1 1 or more comorbidities
Neurosurgery
Oncology
Gastrointestinal Surgery
Otolaryngology
Cardiothoracic Surgery
Surgical Oncology
Ophthalmology
Nephrology
Gynecologic Oncology
Urology
Rheumatology
Neurology
Vascular Surgery
Radiation Oncology
Interventional Radiology
Orthopedic Surgery
18%
16%
14%
12%
10%
8%
6%
4%
2%
0%30s 40s 50s 60s 70s
Prev
alen
ce in
US
Pop
ulat
ion
Age by Decade
StrokeProstate CancerOsteoarthritisColorectal Cancer
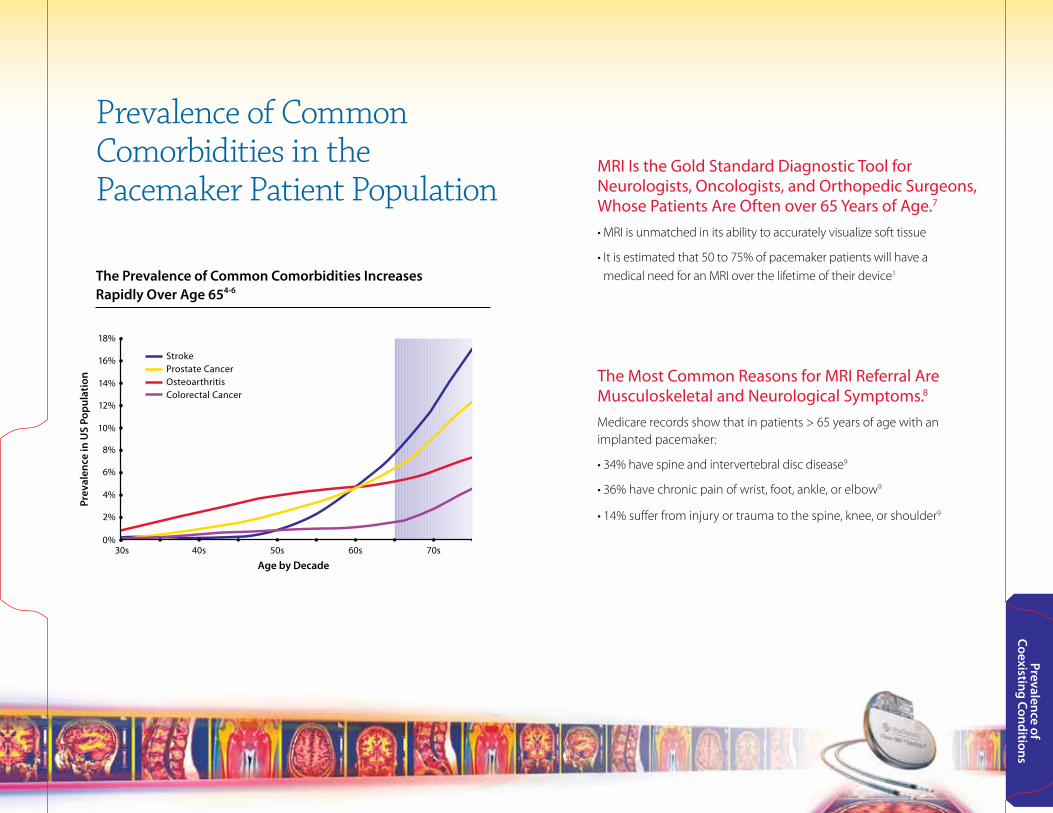
Prevalence of Common Comorbidities in the Pacemaker Patient Population
MRI Is the Gold Standard Diagnostic Tool for Neurologists, Oncologists, and Orthopedic Surgeons, Whose Patients Are Often over 65 Years of Age.7
• MRI is unmatched in its ability to accurately visualize soft tissue
• It is estimated that 50 to 75% of pacemaker patients will have a medical need for an MRI over the lifetime of their device1
The Most Common Reasons for MRI Referral Are Musculoskeletal and Neurological Symptoms.8 Medicare records show that in patients > 65 years of age with an implanted pacemaker:
• 34% have spine and intervertebral disc disease9
• 36% have chronic pain of wrist, foot, ankle, or elbow9
• 14% suffer from injury or trauma to the spine, knee, or shoulder9
Prevalence of Coexisting Conditions
The Prevalence of Common Comorbidities Increases Rapidly Over Age 654-6

Hazards and Risks of M
RI
Hazards and Risks of MRI with Current Pacing SystemsSince 2008, the safety and risk concerns of MRIs in cardiac device patients have been documented in 17 studies10-26
MRI can put pacemaker patients at risk for any of the following25:
Device FieldImpact Static Gradient RF
Pote
ntia
l Haz
ard
Lead Heating The conductive pacing lead acts as an antenna, picking up radiofrequency energy. A portion of this energy is dissipated as heat in the cardiac tissue nears the tip electrode.
Tissue damage may affect pacing therapy.
Unintended Cardiac Stimulation The gradient and radiofrequency fields will induce voltages in pacemaker leads that will be applied to the pacing lead electrodes. If these voltage pulses are large enough, they may directly stimulate the heart.
May lead to a single or intermittent stimulation, or sustained tachycardia.
Device Interactions The gradient, radiofrequency, and static fields may adversely affect the electrical operation of the pacemaker system if its operation is not protected from the effects of those fields.
Pacemaker malfunction or failure may affect pacing therapy.
MR Conditional Risk Information
• A complete Revo MRI SureScan pacing system including a Revo MRI SureScan IPG and two CapSureFix MRI SureScan leads is required for use in the MRI environment
• Any other pacing system combination may result in a hazard to the patient during an MRI scan
• When programmed to On, the MRI SureScan feature allows the patient to be safely scanned while the device continues to provide appropriate pacing
• Refer to the Revo MRI Pacing System Conditions for Use located in the device manuals prior to scanning a patient. Consult Medtronic’s website at www.medtronic.com or call Medtronic at 1 (800) 328-2518.

Revo MRI Pacing SystemSize 12.7 cc
Weight 21.5 g
Specifically Engineered for MRI Safety
Key Product Features
Device Design Solutions• Input circuits optimized
• Circuit design immune to interference
• SureScan pacing mode– Asynchronous pacing– High pacing outputs
• The Revo MRI SureScan pacing system has completed clinical evaluation, regulatory review, and FDA approval and is safe for use when used according to the MRI conditions for use as defined in the SureScan manual
• The implanted system must consist solely of a Medtronic Revo MRI SureScan Model RVDR01 device and two CapSureFix MRI SureScan Model 5086MRI leads
Revo MRI SureScan Pacemaker – A Pacemaker Engineered with Multiple Safety Features
• Device verification appears on pacemaker programmer screen
• Automatic testing ensures only appropriate battery and impedance data are collected during MRI
• Dedicated programming mode provides additional security/backup for Power On Reset (POR)
• Hall sensor immune to strong magnetic fields
Easily Identifiable, Radiopaque Icon Confirms SureScan Device Implant

90
100
80
70
60
50
40
30
20
10
00 5 10 15 20 25 30 35 40 45 50
Perc
ent o
f Max
imum
Tem
per
atur
eLead Path
Model 5076-52
Model 5086-52
– the x-axis represents 50 anatomically relevant leads paths– the results demonstrate significant variability in lead tip heating as a function of the lead path– overall the 5086MRI lead heats approximately 3 times less than the 5076 for most lead paths
CapSureFix MRI SureScan Lead Model 5086 – A Lead Designed for MRI Use• The state-of-the-art 5086 leads are specifically designed and engineered for safety within an MRI environment
• The 5086 lead is based on the CapSureFix® family of leads, which have been implanted in more than 1 million patients worldwide – that’s 2.5 million leads, with 99.5% reliability
• Materials identical to 5076*
• Model 5086MRI lead flex testing– Connector/body– Lead body
• Model 5086MRI clinical implant experience starting February 2007 (928 leads implanted)
Lead Heating Design Solution• Lead inner conductor coil design mitigates lead heating
• 4 filar to 2 filar increases inductance and reduces heating
* Exception of MRI Marker band and electrode coating
CapSureFix MRI Model 5086Polarity Bipolar
Shape
Fixation
Inner/Outer Insulator
Body
Recommended Introducer Size
Tip-to-Ring Spacing
Standard Lengths
Straight
Screw-in
Silicone
7 Fr
10 mm
45 cm, 52 cm, 58 cm
8 Fr (without guide wire)
Easily Identifiable, Radiopaque Icon Confirms SureScan Device Implant
Lead Heating Model 5076 versus Model 5086MRI

0
5
10
15
20
0 0.010
1/1,000 Pulse Amplitude
1/1,000 Pulse Width
0.020 0.030 0.040 0.050Vo
ltag
e (V
)Effective Pulse Width (ms)
Capture
Gradient Stimulation
Range
Preclinical Research
Preclinical Research Demonstrates the Safety of Revo MRI Pacing System7
Testing Summary Extensive preclinical evaluation was based on clinically relevant as well as worst-case scan conditions, using in vitro (bench) testing, in vivo (animal) testing, and computer simulations (modeling).
MRI-Induced Lead Heating Simulations in Human Body Models Using Different Lead Combinations
Lead PathsHuman Body Library
• Human body models encompassed 2nd to 97th percentile of all human bodies, with ten different lead paths
• Over 400,000 different lead/body combinations were analyzed to derive a minimal probability of a 0.5 V threshold
MRI-Induced Unintended Cardiac Stimulation (UCS)• Analysis combined a prediction for the induced voltage pulse
widths and amplitudes and an in vivo canine study to evaluate the stimulation threshold to these pulses
• The risk of reaching the gradient stimulation range is 1/1,000,000 – which remains outside the capture range
• Results confirmed that patient risk from UCS is at an acceptable level
Gradient Stimulation Strength Duration Curve

Pre-MRI
9-12-Week Visit
Post-MRI
1-Week Post-MRIVisit
1-Month Post-MRIVisit
6-MonthPost-Implant Visit
and Every 6Months Thereafter
MRI GroupMRI Scans
Control GroupNo MRI
Enrollment
Implantand Randomization
2-Month Visit
90
100
80
70
60
50
40
30
20
10
0-0.5 0 0.5
Perc
ent o
f Sub
ject
s
Change in Atrial Threshold (V)
MRI Group
Control Group
90
100
80
70
60
50
40
30
20
10
0-1 -0.5 0 0.5 1
Perc
ent o
f Sub
ject
s
Change in Ventricular Threshold (V)
Clinical Trial Demonstrates the Safety of Revo MRI SureScan26
Clinical Support
Study Design• Multicenter, randomized, controlled clinical trial designed to evaluate
the safety of the Revo MRI SureScan pacing system, including any MRI-related complications, as well as to analyze pacing capture thresholds and sensing amplitude
• 464 patients received a Revo MRI SureScan pacing system and were then randomized to elective MRI or no MRI, approximately 9-12 weeks post-implant
• MRI imaging intended to represent commonly used, clinically relevant scans
Methods – Visit Schedule
Key Results• 100% were free of MRI-related complications (n = 211, p < 0.001)
• No sustained atrial or ventricular arrhythmias, no asystole, no pacemaker output inhibition, and no electrical resets in the group receiving MRI
• Minimal changes in pacing capture thresholds, as shown on the following chart
Primary Effectiveness End Point: Atrial and Ventricular Capture Threshold
Threshold changes pre-MRI/control visit to 1-month post-MRI/control visit
No discernible difference between the MRI and control groups

1949 1958 1986 1995 1998 2002
Medtronic founded
First externalpacemaker
Activitrax® pacemakerrate response
Thera® pacemaker first microprocessor-based,
mode switching
Kappa® pacemakerrate-response via activity and
minute ventilation2011
Revo MRI Pacing System
Medtronic CareLink®Network
MVP® promotes intrinsic conduction
A H
istory of Innovation
Builds upon Medtronic Innovations
MVP – Managed Ventricular Pacing• Exclusive technology that used Atrial Pacing (AAIR) primarily with
DDD pacing only when necessary
• MVP reduces unnecessary RV pacing by 99%27
ACC/AHA/HRS guidelines28 state the need to reduce unnecessary pacing as much as possible. The following studies support the guidelines:
MOST29: Every incremental 1% of unnecessary VP increases the risk for heart failure hospitalizations by 5.4% and for AF by 1%.
Danish II30: Even with long AV delays, the risk of AF doubles with DDD(R) pacing compared to AAI(R) with DDD(R) backup.
Gardiwal31: Patients with 72% RV pacing are at increased risk for VT/VF.
CareLink® Network* • The leading Internet-based remote monitoring service for implanted devices32
• Serving nearly 500,000 patients in 3,000 clinics in the United States
* Not all devices are available on the CareLink Network.

Revo MRI Pacing System – Conditions for Use
A complete Revo MRI SureScan pacing system, including a Revo MRI SureScan IPG and two SureScan leads is required for use in the MRI environment. Any other combination may result in a hazard to the patient during an MRI scan. The SureScan feature must be programmed to On prior to scanning a patient according to the specified conditions for use.
Cardiology requirements: • Patients and their implanted systems must be screened to
meet the following requirements:– no previously implanted (active or abandoned) medical
devices, leads, lead extenders, or lead adaptors– no broken leads or leads with intermittent electrical
contact as confirmed by lead impedance history– a Revo MRI SureScan pacing system that has been
implanted for a minimum of 6 weeks– a Revo MRI SureScan pacing system implanted in the left
or right pectoral region– pacing capture thresholds of ≤ 2.0 volts (V) at a pulse
width of 0.4 milliseconds (ms)– a lead impedance value of ≥ 200 ohms (Ω) and ≤ 1,500 Ω– no diaphragmatic stimulation at a pacing output of 5.0 V
and at a pulse width of 1.0 ms in patients whose device will be programmed to an asynchronous pacing mode when MRI SureScan is on
Radiology requirements:• Horizontal cylindrical bore magnet, clinical MRI systems
with a static magnetic field of 1.5 Tesla (T) must be used• Gradient systems with maximum gradient slew rate
performance per axis of ≤ 200 Teslas per meter per second (T/m/s) must be used
• The scanner must be operated in Normal Operating Mode:– The whole body averaged specific absorption rate
(SAR) must be ≤ 2.0 watts per kilogram (W/kg)– The head SAR must be < 3.2 W/kg
• The patient must be positioned within the bore such that the isocenter (center of the MRI bore) is superior to the C1 vertebra or inferior to the T12 vertebra
• Proper patient monitoring must be provided during the MRI scan. The methods include visual and verbal contact with the patient, electrocardiography, and pulse oximetry (plethysmography)
Training requirements:• A health professional who has completed cardiology
SureScan training must be present during the programming of the SureScan feature
• A health professional who has completed radiology SureScan training must be present during the MRI scan
Brief Statement Medtronic CareLink® Monitor/CareLink® Network
Intended UseThe CareLink Monitor and the CareLink Network are indicated for use in the transfer of patient data from some Medtronic implantable cardiac devices based on physician instructions and as described in the product manual. These products are not a substitute for appropriate medical attention in the event of an emergency and should only be used as directed by a physician.
ContraindicationsThere are no contraindications for the CareLink Monitor.
Potential complications include, but are not limited to, rejection phenomena, erosion through the skin, muscle or nerve stimulation, oversensing, failure to detect and/or terminate arrhythmia episodes, acceleration of tachycardia, and surgical complications such as hematoma, infection, inflammation, and thrombosis.
Warnings and PrecautionsThe CareLink Monitor must only be used for interrogating compatible Medtronic implantable devices. The CareLink Monitor is intended for use within the prescribing country.
See the device manual for detailed information regarding the instructions for use, indications, contraindications, warnings, precautions, and potential complications/adverse events. For further information, please call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
References1 Kalin R, Stanton MS. Current clinical issues for MRI
scanning of pacemaker and defibrillator patients. PACE. April 2005;28(4):326-328.
2 Zhan C, Baine WB, Sedrakyan A, Steiner C. Cardiac device implantation in the United States from 1997 through 2004: a population-based analysis. Gen Intern Med. January 2008;23(suppl 1):13-19.
3 Global Industry Analysts, Inc. Magnetic Resonance Imaging (MRI) Equipment – A Global Strategic Business Report. San Jose, CA. 2002.
4 National Cancer Institute April 2009. US estimated complete prevalence (including counts) by age on 1/1/2006. Based on November 2008 SEER data submission; DCCPS, Surveillance Research Program, Statistical Research and Applications Branch.
5 Lawrence RC, Helmick CG, Arnett FC, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum. May 1998;41(5):778-799.
6 American Heart Association. Heart Disease and Stroke Statistics – 2010 Update: Learn and Live. Prevalence of stroke by age and sex (NHANES: 2003-2006).
7 Medtronic Revo MRI FDA Panel Pack: http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/CirculatorySystemDevicesPanel/ucm204585.htm.
8 Medical Imaging Survey, 2009.9 Medicare Fee-for-Service Review, 2007.10 Naehle CP, Zeijlemaker V, Thomas D, et al. Evaluation
of cumulative effects of MR imaging on pacemaker systems at 1.5 Tesla. Pacing Clin Electrophysiol. December 2009;32(12):1526-1535.
11 Goldsher D, Jahshan S, Roguin A. Successful cervical MR scan in a patient several hours after pacemaker implantation. Pacing Clin Electrophysiol. October 2009;32(10):1355-1356.
12 Gimbel JR. Unexpected asystole during 3T magnetic resonance imaging of a pacemaker-dependent patient with a “modern” pacemaker. Europace. September 2009;11(9):1241-1242.
13 Naehle CP, Strach K, Thomas D, et al. Magnetic resonance imaging at 1.5-T in patients with implantable cardioverter-defibrillators. J Am Coll Cardiol. August 4, 2009;54(6):549-555.
14 Roguin A. Magnetic resonance imaging in patients with implantable cardioverter-defibrillators and pacemakers. J Am Coll Cardiol. August 4, 2009;54(6):556-557.
15 Mollerus M, Albin G, Lipinski M, Lucca J. Cardiac biomarkers in patients with permanent pacemakers and implantable cardioverter-defibrillators undergoing an MRI scan. Pacing Clin Electrophysiol. October 2008;31(10):1241-1245.
16 Pulver AF, Puchalski MD, Bradley DJ, et al. Safety and imaging quality of MRI in pediatric and adult congenital heart disease patients with pacemakers. Pacing Clin Electrophysiol. April 2009;32(4):450-456.
17 Nordbeck P, Weiss I, Ehses P, et al. Measuring RF-induced currents inside implants: impact of device configuration on MRI safety of cardiac pacemaker leads. Magn Reson Med. March 2009;61(3):570-578.
18 Sutton R, Kanal E, Wilkoff BL, et al. Safety of magnetic resonance imaging of patients with a new Medtronic EnRhythm MRI SureScan pacing system: clinical study design. Trials. December 2, 2008;9(1):68.
19 Naehle CP, Meyer C, Thomas D, et al. Safety of brain 3-T MR imaging with transmit-receive head coil in patients with cardiac pacemakers: pilot prospective study with 51 examinations. Radiology. December 2008;249(3):991-1001.
20 Calcagnini G, Triventi M, Censi F, et al. In vitro investigation of pacemaker lead heating induced by magnetic resonance imaging: role of implant geometry. J Magn Reson Imaging. October 2008;28(4):879-886.
21 Dyrda K, Khairy P. Implantable rhythm devices and electromagnetic interference: myth or reality? Expert Rev Cardiovasc Ther. July 2008;6(6):823-832.
22 Gimbel JR. Magnetic resonance imaging of implantable cardiac rhythm devices at 3.0 tesla. Pacing Clin Electrophysiol. July 2008;31(7):795-801.
23 Nordbeck P, Bauer WR. [Safety of cardiac pacemakers and implantable cardioverter-defibrillators in magnetic resonance imaging. Assessment of the aggregate function at 1.5 tesla.] Dtsch Med Wochenschr. March 2008;133(13):624-628. [Article in German.]
24 Tandri H, Zviman MM, Wedan SR, Lloyd T, Berger RD, Halperin H. Determinants of gradient field-induced current in a pacemaker lead system in a magnetic resonance imaging environment. Heart Rhythm. March 2008;5(3):462-468.
25 Roguin A, Zviman MM, Meininger GR, et al. Modern pacemaker and implantable cardioverter/defibrillator systems can be magnet resonance imaging safe: in vitro and in vivo assessment of safety and function at 1.5 T. Circulation. August 3, 2004;110(5):475-482.
26 Medtronic, Inc. Revo MRI SureScan pacing system clinical summary. http://manuals/medtronic.com.
27 Gillis AM, Pürerfellner H, Israel CW, et al. Reduction of unnecessary right ventricular pacing due to the Managed Ventricular Pacing (MVP) mode in patients with symptomatic bradycardia: benefit for both sinus node disease and AV block indications. Heart Rhythm. 2005;Abstract AB21-1.
28 Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. May 27, 2008;51(21):e1-62.
29 Sweeney MO, Hellkamp AS, Ellenbogen KA, et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. June 17, 2003;107(23):2932-2937.
30 Nielsen JC, Kristensen L, Andersen HR, Mortensen PT, Pedersen OL, Pedersen AK. A randomized comparison of atrial and dual-chamber pacing in 177 consecutive patients with sick sinus syndrome: echocardiographic and clinical outcome. J Am Coll Cardiol. August 20, 2003;42(4):614-623.
31 Gardiwal A, Yu H, Oswald H, et al. Right ventricular pacing is an independent predictor for ventricular tachycardia/ventricular fibrillation occurrence and heart failure events in patients with an implantable cardioverter-defibrillator. Europace. March 2008;10(3):358-363.
32 Medtronic CareLink Metrics Database.

















