Revisiting the Economic Efficiencies of Observation Units · 46 MANAGED CARE / MARCH 2015...
9
46 MANAGED CARE / MARCH 2015 Revisiting the Economic Efficiencies Of Observation Units Ibrahim M Abbass, RPh, PhD, 1 Trudy M. Krause, DrPH, CPHQ, 1 Salim S. Virani MD, PhD, 3,4 J. Michael Swint, PhD, 1,2 Wenyaw Chan, PhD, 1 and Luisa Franzini, PhD 1 1 University of Texas School of Public Health, Division of Management, Policy and Community Health, Houston, Texas 2 University of Texas School of Medicine, Center for Clinical Research and Evidence-Based Medicine, Houston, Texas 3 Health Policy, Quality & Informatics Program, Michael E. DeBakey Veterans Affairs Medical Center HSR&D, Houston, Texas 4 Center for Innovations; Section of Cardiovascular Research, Dept. of Internal Medicine, Baylor College of Medicine, Houston, Texas INTRODUCTION Since their inception in the 1980s, chest pain observation units (OUs) have been widely accepted as provid- ing care of equivalent quality to inpa- tient settings but at a lower cost (Ga- spoz 1998, Sayre 1994, Roberts 1997, Graff 1997, Wright 2013). A recent study reported that one third of U.S. hospitals have dedicated OUs within their facilities (Venkatesh 2011). e estimated annual cost savings to the U.S. health care system, if all U.S. hos- pitals adopted OUs for conditions that require short stay, has been estimated to be $3.1 billion (Baugh 2012). e proliferation of chest pain OUs was mainly driven by studies con- ducted in the 1990s and early 2000s that found them to be cost-effective (Gaspoz 1998, Sayre 1994, Roberts 1997, Graff 1997, Goodacre 2004). In the case of chest pain, no significant differences in cardiac outcomes were noticed between patients admitted to OUs or inpatient care (Abbass 2014, Cullen 2011). OUs appealed to hospi- tals for reducing unnecessary admis- sions and also the low cost of triaging patients from the emergency room (ER) (Roberts 1997, Graff 1997). Almost 30 years aſter their in- troduction, OUs are once again the subject of an ongoing public discus- sion (Feng 2012, Baugh 2013, Wright 2013, Sheehy 2013). Recent reports have indicated that patients in OUs are admitted for extended periods of time (Feng 2012). e proportion of patients’ admissions to OUs is increas- ing, and the Centers for Medicare and Medicaid Services have held public hearings in an attempt to understand the reasons behind this trend (Feng 2012). ere is also a wide variation in the way OUs are operating (Sekhri 2009). Moreover, since the time of earlier studies, more advanced im- aging procedures have come into use to triage chest pain patients in the ER Original Research ABSTRACT Background: Recent studies cast doubt about the economic efficiency of observation units (OUs). Objective: We aimed to reexamine the cost savings of OUs com- pared with inpatient care. Methods: Claims for 15,851 patients who were admitted to inpatient or OUs between January 2009 and December 2012 following emer- gency room (ER) visits for chest pain were retrospectively examined. The two groups were compared for total cost of episode, length of stay (LOS), and utilization rates of diagnostic procedures, including stan- dard exercise and echocardiography stress tests, myocardial perfusion imaging (MPI), coronary computed tomography angiography (CCTA), and computed tomography (CT) chest scans. Total costs of care and LOS were adjusted for age, gender, risk scores, and comorbidities using quantile regression. Results: More than 37% of the sample was admitted to inpatient units (n=5,890) vs 62.7% to OUs (n=9,961). Patients admitted to in- patient units had more comorbidities and longer LOS during their ER visit (median 1.5 adjusted days; 10th percentile=1, 90th percentile=3) vs. median 21 adjusted hours for OUs (20, 23). The adjusted median cost of OUs was $5,411 ($4,652, $7,157) vs. $6,946 for inpatient admis- sion ($5,978, $18,683). The estimated adjusted cost saving of OUs was $1,535 (95% CI=$1,206, $1,411) compared with inpatient admission. About 37% of patients admitted to OUs stayed longer than 24 hours. Compared with patients admitted to inpatient units, patients in OUs also received more MPI (35.8% vs. 31.5%), CT scans (13.2% vs. 10.4%), standard exercise test (45.6% vs. 33.8%) and echocardiography stress test (8% vs. 3.4%). Conclusion: Despite the increased proportion of patients exceed- ing the 24-hour LOS and the increased utilization of advanced imaging procedures, OUs are still less costly compared with inpatient admission. Keywords: Observation units; inpatient; costs; length of stay; diag- nostics; imaging
Transcript of Revisiting the Economic Efficiencies of Observation Units · 46 MANAGED CARE / MARCH 2015...

46 MANAGED CARE / MARCH 2015
Revisiting the Economic Efficiencies Of Observation UnitsIbrahim M Abbass, RPh, PhD,1 Trudy M. Krause, DrPH, CPHQ,1 Salim S. Virani MD, PhD,3,4 J. Michael Swint, PhD,1,2 Wenyaw Chan, PhD,1 and Luisa Franzini, PhD1
1University of Texas School of Public Health, Division of Management, Policy and Community Health, Houston, Texas2University of Texas School of Medicine, Center for Clinical Research and Evidence-Based Medicine, Houston, Texas3Health Policy, Quality & Informatics Program, Michael E. DeBakey Veterans Affairs Medical Center HSR&D, Houston, Texas 4Center for Innovations; Section of Cardiovascular Research, Dept. of Internal Medicine, Baylor College of Medicine, Houston, Texas
INTRODUCTIONSince their inception in the 1980s, chest pain observation units (OUs) have been widely accepted as provid-ing care of equivalent quality to inpa-tient settings but at a lower cost (Ga-spoz 1998, Sayre 1994, Roberts 1997, Graff 1997, Wright 2013). A recent study reported that one third of U.S. hospitals have dedicated OUs within their facilities (Venkatesh 2011). The estimated annual cost savings to the U.S. health care system, if all U.S. hos-pitals adopted OUs for conditions that require short stay, has been estimated to be $3.1 billion (Baugh 2012).
The proliferation of chest pain OUs was mainly driven by studies con-ducted in the 1990s and early 2000s that found them to be cost-effective (Gaspoz 1998, Sayre 1994, Roberts 1997, Graff 1997, Goodacre 2004). In the case of chest pain, no significant differences in cardiac outcomes were noticed between patients admitted to OUs or inpatient care (Abbass 2014, Cullen 2011). OUs appealed to hospi-tals for reducing unnecessary admis-sions and also the low cost of triaging patients from the emergency room (ER) (Roberts 1997, Graff 1997).
Almost 30 years after their in-troduction, OUs are once again the subject of an ongoing public discus-sion (Feng 2012, Baugh 2013, Wright 2013, Sheehy 2013). Recent reports have indicated that patients in OUs are admitted for extended periods of time (Feng 2012). The proportion of patients’ admissions to OUs is increas-
ing, and the Centers for Medicare and Medicaid Services have held public hearings in an attempt to understand the reasons behind this trend (Feng 2012). There is also a wide variation
in the way OUs are operating (Sekhri 2009). Moreover, since the time of earlier studies, more advanced im-aging procedures have come into use to triage chest pain patients in the ER
Original Research
ABSTRACTBackground: Recent studies cast doubt about the economic
efficiency of observation units (OUs). Objective: We aimed to reexamine the cost savings of OUs com
pared with inpatient care.Methods: Claims for 15,851 patients who were admitted to inpatient
or OUs between January 2009 and December 2012 following emergency room (ER) visits for chest pain were retrospectively examined. The two groups were compared for total cost of episode, length of stay (LOS), and utilization rates of diagnostic procedures, including standard exercise and echocardiography stress tests, myo cardial perfusion imaging (MPI), coronary computed tomography angiography (CCTA), and computed tomography (CT) chest scans. Total costs of care and LOS were adjusted for age, gender, risk scores, and comorbidities using quantile regression.
Results: More than 37% of the sample was admitted to inpatient units (n=5,890) vs 62.7% to OUs (n=9,961). Patients admitted to inpatient units had more comorbidities and longer LOS during their ER visit (median 1.5 adjusted days; 10th percentile=1, 90th percentile=3) vs. median 21 adjusted hours for OUs (20, 23). The adjusted median cost of OUs was $5,411 ($4,652, $7,157) vs. $6,946 for inpatient admission ($5,978, $18,683). The estimated adjusted cost saving of OUs was $1,535 (95% CI=$1,206, $1,411) compared with inpatient admission. About 37% of patients admitted to OUs stayed longer than 24 hours. Compared with patients admitted to inpatient units, patients in OUs also received more MPI (35.8% vs. 31.5%), CT scans (13.2% vs. 10.4%), standard exercise test (45.6% vs. 33.8%) and echocardiography stress test (8% vs. 3.4%).
Conclusion: Despite the increased proportion of patients exceeding the 24hour LOS and the increased utilization of advanced imaging procedures, OUs are still less costly compared with inpatient admission.
Keywords: Observation units; inpatient; costs; length of stay; diagnostics; imaging

MARCH 2015 / MANAGED CARE 47
Economic Efficiencies of Observation Units
(Johnson 2007, Stillman 2007, Ladapo 2008, Rubinshtein 2007, Hein 2009). National surveys have documented a 368% increase in the utilization of ad-vanced imaging procedures for chest pain patients in the ER between 1999 and 2008 (Bhuiya 2010).
These new developments cast doubt about the current economic efficiencies of OUs and their appro-priateness of care. Given these fac-tors, we reexamined the cost savings of OUs from the payer’s perspective. We used claims data to compare the costs and utilization rates of imaging procedures for patients who had ob-servation services versus those admit-ted to inpatient setting.
METHODSStudy Design and Data Sources In this study, we retrospectively evaluated ER visits by patients with nonspecific chest pain (ICD-9 codes 768.5, 786.50, and 786.59). We used BlueCross BlueShield of Texas (BCBS-TX) claims data from January 2009 to December 2012 to extract the study population. At the time of the study, BCBS-TX was the third-largest pri-vate health insurance provider in the state, covering about 3 million en-rollees in a given year. Patients with plans other than preferred provider organization (PPO) and PPO+ were excluded from the study due to a lack of comprehensive claims data. We identified inpatient admission using
the bill type code (bill type=11X) while we defined observation services per the Medicare Claims Processing Manual (CMS 2013).
SamplingPatients 18–65 years of age with 1 year of continuous enrollment prior to their ER visit were included in the study. Claims incurred in the preindex period were used to identify patients’ comorbidities and calculate their risk scores. We excluded patients with a history of ER visits for non specific chest pain because such patients would likely have a different course of treatment. As the primary purpose of this study is to compare solely the costs of inpatient and observation ser-vices, we excluded patients who were directly discharged home following their ER visits, died, or had both inpa-tient and observation services during the same episode.
Cost of CareWe examined the costs of care from the payer’s perspective, where cost is defined as the total allowed amount paid by the insurers to providers for the rendered services. The allowed amount represents the actual contrac-tual agreed amount between BCBS-TX and health care providers which is different from hospital charges. For the purpose of this study, the chest pain episode of care was set to start from the day of the ER visit and con-tinued until the discharge date from observation/inpatient units. In cases where discharge dates were missing, the episode of care was ended when
there was a day gap between the last day medical services/procedures ob-served and the next incurred medical services/procedures. All costs were adjusted for inflation using the Medi-cal Services Price Index for 2012.
Length of Stay and Observation HoursLength of stay (LOS) for inpatient admission was calculated using the number of service units associated with room and board revenue codes. The duration of observation hours was calculated using the number of service units associated with the G0378 CPT code in facility claims. The median of both lengths of stay and observation hours were then ad-justed for differences in demographic characteristics, risk scores, cardio-vascular risk factors, and year of visit using quantile regression.
Risk StratificationTo account for baseline differences in prior comorbidities and burden of illness, we used 2 approaches. First, we calculated a risk score for each patient that represents the burden of illness (Halling 2006). We used the Johns Hopkins software for Adjusted Clinical Group (ACG) to calculate the risk scores (Weiner 2011). The mean risk score for the sample population is calibrated to 1; patients who had risk scores >1 have higher illness bur-den compared with the population mean. Second, we adjusted for spe-cific cardio vascular risk factors that directly influence providers’ decisions as to whether to discharge or admit or utilize diagnostic procedures (Table 1; see page 52A for comorbidities and ICD-9 codes). Year-to-year variation in protocol development, technol-ogy adoption, and practice patterns was controlled for using dummy variables for the year of the ER visit (2009 through 2012). Finally, we clas-sified patients into three groups based on their diagnosis at discharge; the
Funding source: NoneConflict disclosure: No conflicts to reportCorresponding author:Ibrahim M Abbass, RPh, PhDAdjunct Assistant ProfessorUniversity of Texas School of Public Health1200 Hermann Pressler StreetHouston, TX 77030Telephone: 8326618556Email: [email protected]: Abbass conduced this research while at University of Texas but is now employed by Comprehensive Health Insights, a Humana company.
Jesa
da2u
| D
ream
stim
e.co
m

48 MANAGED CARE / MARCH 2015
Economic Efficiencies of Observation Units
groups included patients with (1) ill-defined diagnoses (ICD-9 codes 788.xx-799.xx), (2) circulatory diag-noses (ICD-9 codes 390.xx-459.xx), and (3) all other noncirculatory di-agnoses. Diagnosis at discharge and use of ambulance services were used to adjust for the urgency of patients’ conditions.
Statistical Analyses We used chi-square test and t-test to evaluate the baseline differences between observation and inpatient units. The utilization of different di-agnostic tests and procedures was summarized for each group. The cost for each group was summed and compared across the two groups. We used quantile regression to examine the difference in costs and LOS be-tween the two groups. Boot strapping, with 10,000 replications, was used to calculate the 95% confidence inter-vals (CI) around the estimates. To
further validate our findings and to account for potential indication bias, we developed a logit model using ob-servation (vs. inpatient) admission as the dependent variables and con-ducted 1-to-1 propensity matching with a caliper of 0.05. The matching was performed using PSMatch SAS macro (Coca-Perraillon 2007) and was based on patients’ demographics, risk scores, comorbidities, utilization of ambulance services, year of visit, and diagnosis at discharge.
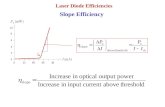
RESULTSStudy PopulationThe figure (see page 52A) depicts the methodology we employed to extract the final study sample. There were 152,856 patient visits to the ER for which the primary complaint was nonspecific chest pain. We excluded 30,491 patient visits for not meeting the continuous enrollment criterion and 52,644 for having a history of ER
visits due to non specific chest pain. Also, we excluded 37 patients who died during their ER episodes, 53,709 visits where patients were directly dis-charged home, and 124 patient visits involving both inpatient and observa-tion services. Thus, the final sample included 15,851 patients, of whom 5,890 patients were admitted to in-patient units while 9,961 patients were admitted to OUs.
Baseline Demographics In Table 1, we compared the baseline clinical characteristics and risk factors of patients across the two groups. The average age of the study population was 51 years, with older patients being admitted to inpatient care. The over-all median risk was relatively simi-lar across the two groups, although patients admitted to inpatient units had higher prevalence of comorbidi-ties compared with patients admit-ted to the OUs. Patients admitted to in patient units were more likely to have circulatory diagnoses (15.5% vs. 1.3%) and other noncirculatory diagnoses (10.3% vs. 1.5%) compared with those in OUs.
Table 1 also depicts the utilization trend of observation services between 2009 and 2012. As illustrated, the uti-lization of OUs for non specific chest pain patients increased from 19.4% in 2009 to 31.2% in 2012.
Cost of ER Episode by Pattern of CareThe median unadjusted cost for in-patient admission (10th and 90th percentiles) was $7,674 ($4,038, $23,939) vs. $ 5,467 ($3,409, $10,008) for OUs. The adjusted median cost of OUs was $5,411 ($4,652, $7,157) vs. $6,946 ($5,978, $18,683). The es-timated median cost saving of OUs, after adjusting for differences in base-line characteristics, risk scores, and diagnosis at discharge using quan-tile regression (Table 2, page 52B), was $1,308 (95% CI, $1,206–$1,411)
KEy POINTSWhat is already known on this subject?• Evidence of observation unit (OU) cost savings come from studies
conducted in the 1990s and early 2000s. • Since then, expensive imaging and other diagnostic procedures have
come into use to triage patients from OUs, and patients are spending more time in OUs.
What this study adds• OUs still are less costly than inpatient admission despite the longer
length of stay and increased use of advanced imaging in OUs. In this study, the difference in the adjusted median costs of OU patients and those treated as inpatients was $1,535.
• The saving margin of OUs is declining compared to historical values. Compared with previous studies, historical data, the economic efficiencies of OUs have diminished from being 2 times less costly than inpatient care to only 1.4 times less costly.
Takeaways • Patients in OUs had higher utilization of diagnostic and imaging
procedures compared with the inpatient group even though they had fewer comorbidities.
• More than one third of patients in OUs stayed >24 hours under observation.
• Despite current trends, OUs remain less costly than inpatient care.

MARCH 2015 / MANAGED CARE 49
Economic Efficiencies of Observation Units
compared with inpatient units (Table 3). The total cost of episode was sta-tistically significantly associated with
older age, male, the presence of isch-emic heart diseases ($200); diseases of arteries, arterioles, and capillaries
($261); and the use of ambulance to reach ER ($1,801). This coefficient of ER reflects both the cost of using the ambulance (median of $352) and the urgency of the case and subsequent resource utilization. Table 2 (online appendix) also demonstrates a consis-tent, increasing trend of the cost of ER episode from 2009 to 2012. This trend could be a result of technology adop-tion, practice patterns, and protocol development. Additionally, patients who ended up with circulatory di-agnoses or noncirculatory diagnoses had significantly higher median costs ($11,443 and $4,035, respectively) compared with patients who ended up with ill-defined diagnoses, which include nonspecific chest pain.
Diagnostic Tests and Procedures Used During ER EpisodesTable 4 illustrates the utilization of a variety of diagnostic tests and proce-dures during the ER episode for the two groups. The most utilized tests were the standard exercise stress tests (45.6% for OUs vs. 33.8% for the in-patient group), followed by MPI (35.8% for observation vs. 31.5% for in patient), and CT noncoronary scans (13.2% for observation vs. 10.4% for inpatient). Echocardiography stress test and CCTA were the least utilized diagnostics in both populations. Ex-cept for CCTA (P=.38), patients ad-mitted to OUs utilized more standard exercise and echocardiography stress tests, CT chest, and MPI (P<.001). The results of chi-square tests in the matched population demonstrate that patients in OUs had more echo-cardiography stress tests and CT chest (P<.001) but not MPI (P=.20).
LOS and Observation Hours The unadjusted median LOS for pa-tients admitted to inpatient units was 2 days, with 25.4% of patients hav-ing an LOS >2 days. Patients in OUs stayed under observation a median of 22 hours before being discharged (5th
TABLE 1 Clinical characteristics of patients prior to emergency room (ER) visit (using 1-year claims data)
Inpatient(n=5,890)
Observation(n=9,961) Pc
Age (mean±STD) 51.1±9.1 50.5±8.7 <.001
Gender (% female) 3,016 (51.2) 5,664 (56.9) <.001
Risk score 0.80±1.54 0.98±1.75 <.001
Number of patients with comorbidities (%)a
Chronic rheumatic heart disease 119 (2.0) 79 (0.8) <.001
Hypertensive disease 4,155 (70.5) 5,423 (54.4) <.001
Ischemic heart disease 2,059 (35.0) 1,656 (16.6) <.001
Diseases of pulmonary circulation 179 (3.0) 163 (1.6) <.001
Other forms of heart diseaseb 2,074 (35.2) 1,938 (19.5) <.001
Cerebrovascular disease 424 (7.2) 514 (5.2) <.001
Diseases of arteries, arterioles, and capillaries
493 (8.4) 441 (4.4) <.001
Diseases of veins and lymphatics, and other diseases of circulatory system
768 (13.0) 902 (9.1) <.001
Diabetes mellitus 1,693 (28.7) 1,960 (19.7) <.001
Dyslipidemia 3,641 (61.8) 4,615 (46.3) <.001
Diseases of the digestive system 3,076 (52.2) 4,218 (42.3) <.001
Mental disorders 3,025 (51.4) 3,499 (35.1) <.001
Diseases of the respiratory system 3,406 (57.8) 5,312 (53.3) <.001
Coronary artery bypass graft 79 (1.3) 79 (0.8) <.001
Percutaneous transluminal coronary angioplasty
448 (7.6) 415 (4.2) <.001
Used ambulance to reach ER 1,433 (24.3) 1,556 (15.6) <.001
ER visit in 2009 1,508 (25.6) 1,937 (19.4) <.001
ER visit in 2010 1,308 (22.2) 2,305 (23.1) .18
ER visit in 2011 1,353 (23.0) 2,607 (26.2) <.001
ER visit in 2012 1,721 (29.2) 3,112 (31.2) .01
Diagnosis at discharge: illdefined 4,374 (74.3) 9,677 (97.1) <.001
Diagnosis at discharge: circulatory 912 (15.5) 130 (1.3) <.001
Diagnosis at discharge: others 604 (10.3) 154 (1.5) <.001a Percentages are the proportion of identified comorbidities over the total number of
patient visits in each group.b Other heart diseases include pericarditis, endocarditis, cardiomyopathy, conduction
disorders, dysrhythmia, heart failure, and complications of heart diseases.c Student’s t test was used to test mean differences for continuous variables, and chisquare
test was used to test differences for categorical variable.

50 MANAGED CARE / MARCH 2015
Economic Efficiencies of Observation Units
percentile, 6 hours; 95th percentile, 49 hours). About 37.3% of patients admitted to the OUs exceeded the rec-ommended 24-hour window for ob-servation. When adjusted for demo-graphic, risk scores, cardio vascular risk factors, and year of visit, the me-dian LOS for inpatient admission was 1.5 days compared with a median of 21 hours for patients in OUs. In real-ity, we cannot tell from claims data the number of hours patients spent in the inpatient units, and it is more likely for patients staying in inpatient units 1.5 days to be billed for 2 days.
DISCUSSIONOur study took a comprehensive ap-proach in examining the costs of ob-servation services and inpatient care following an ER admission for non-specific chest pain patients. We found that the cost associated with OU ser-vices is consistently lower compared with the cost associated with inpatient admission for the study population. This finding concurs with previous randomized clinical trial (RCT) stud-ies that found OUs to be less costly compared with inpatient admission (Sayre 1994, Gaspoz 1994, Roberts 1997). Second, patients who had ob-servation services received higher proportion of diagnostic procedures even though they had lower preva-lence of comorbidities and cardio-vascular risk. This high utilization of diagnostics procedures did not dis-appear in the matched population. This rise in diagnostic procedures has added more costs to patients receiv-ing observation services. Nonethe-less, this increase in diagnostics did not render OUs more expensive than inpatient admission. Third, the uti-lization of observation services has consistently increased between 2009 and 2012 as did the cost of both inpa-tient admission and observation ser-vices. Prior studies have documented the increased use of OUs in Medicare population (Feng 2012).
The high utilization of advanced imaging procedures in the observa-tion group compared with inpatient defies the original purpose of OUs when they were initially established in 1990s. At that time, OUs represented a cost-saving healthcare delivery model where patients were observed for a longer period of time, allowing physi-cians to conduct a thorough medical history and a physical examination with accelerated protocols using an array of low-cost procedures, such as serial biomarkers/ECG tests (Gaspoz 1998, Sayre 1994, Roberts 1997, Graff 1997). This process aided the physi-cian in making a decision to admit or discharge patients from the ER (Gaspoz 1998, Sayre 1994, Roberts 1997, Graff 1997). Today, however, care has shifted toward adopting
more technologies, and hospitals are proposing incorporating advanced imaging procedures in OUs as part of their standard care (Miller 2014). This increase in diagnostic procedure rates was also coupled with an increase in observation hours, where more than one third of patients stayed longer than 24 hours. Korley and colleagues found that ER visits that had CT or MRI scans were held 126 minutes longer (Korley 2010). Therefore, the proliferation of advanced imaging procedures also might have contrib-uted to the unexplained increase in the observation hours (Feng 2012).
Graff and colleagues (Graff 1997) summarized the cost difference be-tween OUs and inpatient ward for studies conducted in 1990s (Sayre 1994, Roberts 1997, Farkouh 1998).
TABLE 3Median inpatient and observation services costs (with 10th and 90th percentiles)
Inpatient(n=5,890)
Observation(n= 9,961)
Unadjusted costs $7,674 ($4,038, $23,939)
$5,467 ($3,409, $10,008)
Adjusted costsa $6,946 ($5,978, $18,683)
$5,411 ($4,652, $7,157)
Estimated cost saving of observation units
$1,308 (95% CI, $1,206–$1,411)
a Cost was adjusted for patients’ demographics, baseline characteristics, risk score, and diagnosis at discharge.
TABLE 4Major diagnostic procedures used during the ER episodea
Inpatient(n=5,890)
Observation(n=9,961)
P
Standard exercise stress test (%) 1,990 (33.8) 4,541 (45.6) <.001
Echocardiography stress test (%) 198 (3.4) 795 (8.0) <.001
Computed tomography noncoronary chest scans (%)
612 (10.4) 1,311 (13.2) <.001
Coronary computed tomography angiography (%)
47 (0.8) 93 (0.9) .38
Myocardial perfusion imaging (%) 1,857 (31.5) 3,570 (35.8) <.001a Patients could have multiple tests.

MARCH 2015 / MANAGED CARE 51
Economic Efficiencies of Observation Units
The costs of OUs were estimated to be in the range of $1,915 to $2,581 with an average of $2,139, while inpatient admissions were estimated to range from $4,180 to $6,418, with an aver-age of $4,798 when adjusted for infla-tion using the Medical Services Price Index for 2012. Inpatient admissions were consistently more than 2 times (average, 2.2) higher than the costs of OUs (Sayre 1994, Gaspoz 1994, Far-kouh 1998). Our findings, however, indicate that inpatient admission costs were 1.4 times higher than the costs of OUs. Several reasons could explain this reduction in cost difference be-tween observation and inpatient ad-mission. First, when earlier studies were conducted, patients were triaged using protocols that included mainly an array of low-cost tests and pro-cedures (Roberts 1997, Graff 1997). In our study, however, we have seen that a large portion of patients had myocardial perfusion imaging and CT scans. Many of the studies that evaluated the cost- effectiveness of OUs did not incorporate MPI, CCTA, or CT scans as part of their protocols (Roberts 1997, Goodacre 2004). Fur-thermore, our results, and other more recent studies also indicate that a large proportion of patients admitted to OUs have longer LOS versus what was initially allowed (24–48 hours), which might explain the increase in the cost of observation (Feng 2012). Likewise, the utilization rate of some diagnos-tics was higher for patients in OUs even though they had lower cardio-vascular risk factors compared with the inpatient group. This high use of imaging procedures could be re-lated to the original triaging purpose of OUs, where tests and procedures are heavily utilized so physicians can make a decision to admit or discharge patients. Finally, the cost estimates de-rived in prior studies were measured at individual hospitals or a handful of participating ERs, which had a large variation in patients’ disposition, in-
clusion, and exclusion criteria, which might explain the differences in the costs between inpatient and observa-tion admission (Roberts 1997, Graff 1997, Sekhri 2009, Baugh 2013).
Our study also found that patients with more comorbidities were more likely to be admitted to inpatient units. To adjust for that, we con-ducted two types of analysis. First, we calculated the median adjusted costs for each group, taking into ac-count the prevalence of risk factors, using quantile regression analysis. The differences between the groups regressed around the population me-dian, but the differences between the two groups remained significant. Sec-ond, we performed 1-on-1 propensity matching and compared patients ad-mitted to OUs or inpatient settings. After propensity score matching, the difference of the cost between the two groups persisted and was supportive of our initial findings. Both methods produced similar results, with an es-timated cost difference between ob-servation and inpatient admissions of $1,308 using quantile regression and $1,437 using propensity matching.
The results of this study do not discard inpatient care as a viable option for directly admitting some patients following their ER visits. In another study with a similar cohort, we compared the 1-year outcomes of patients admitted with observation and inpatient units (Abbass 2014). In that study, we could not match 11% of inpatient cohort to OUs, as they were sicker and had higher comorbidities. The findings also suggested that 89% of patients admitted to inpatient units could have been admitted to OUs and would have had similar outcomes. We also found that patients admitted to OUs were 79% more likely to have revascularization procedures com-pared with the inpatient group. This trend in revascularization procedures could be explained by the higher utili-zation of imaging procedures we ob-
served in this study as also reported by Shrei bati and colleagues (Abbass 2014, Shreibati 2011). The 1-year costs associated with OUs, however, were similar to the costs of inpatient care (Abbass 2011).
The current health policy debate re-garding OUs focuses on the extended observation hours and the appropri-ate payment model of observation services. However, what is not fully addressed in the current debate is a discussion about the purpose of ob-servation status and the intensity and the appropriateness of the resources utilized for patients in OUs compared to an alternative healthcare delivery model such as inpatient care.
LimitationsOur study has several limitations. First, our definition of an ER event is not all-encompassing. Some claims from office visits or subsequent care in other settings that could have occurred the next day after ER dis-charge date could have been included in our analyses. However, when we checked the costs of evaluation and management, about 98% of the costs incurred were due to inpatient, emer-gency room visits, and consultation, while the rest were due to specialist and office-based visits. This indicated that there was very little chance our analyses included services that oc-curred outside the ER event. Second, we used the claims for patients with PPO and PPO+ coverage, thus the results could potentially be differ-ent for patients with fee-for-service or health maintenance organization (HMO) coverage. Third, patterns of care and diagnostic procedures are more likely to change from a hospital to another. Given the data we had, we were not able to control for hospital characteristics because we had a de-identified database. Finally, we limi-ted this study to patient dispositions following ER visits owing to chest pain only; therefore, the results can-

52 MANAGED CARE / MARCH 2015
Economic Efficiencies of Observation Units
not be extended to other conditions. Nonetheless, chest pain is cited as the leading cause of ER visits, observa-tion, and short inpatient admissions (Wright 2013, Sheehy 2013).
CONCLUSIONObservation units cost less compared with inpatient admission, despite the increased LOS and utilization of ad-vanced imaging procedures in OUs. The findings of this study suggest that the costs associated with observation services have increased substantially compared with estimates derived from studies conducted to 1990s due to the longer LOS and increased uti-lization of advanced imaging. Still, OUs are a cost-saving tool and have the potential to drive down the costs of health care if the current trends of diagnostic procedures utilization could be reversed.
REFERENCESAbbass IM, Virani SS, Michael Swint J, et
al. One-year outcomes associated with using observation services in triaging patients with nonspecific chest pain. Clin Cardiol. 2014(3):591–596.
Baugh CW, Schuur JD. Observation care—high-value care or a cost-shifting loophole? N Engl J Med. 2013;369:302–305. Erratum in: N Engl J Med. 2013;369:1476.
Baugh CW, Venkatesh AK, Hilton JA, et al. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31:2314–2323.
Bhuiya FA, Pitts SR, McCaig LF. Emergency department visits for chest pain and abdominal pain: United States, 1999–2008. NCHS Data Brief. 2010:1-8.
CMS (Centers for Medicare and Medicaid Services). Medicare Claims Processing Manual: Including Inpatient Hospital Part B and OPPS (Pub. 100-04). www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R2845CP.pdf. Accessed Feb. 24, 2015.
Coca-Perraillon M. Local and global opti-mal propensity score matching. SAS Global Forum. www.biostat.umn.edu/~will/6470stuff/Class25-12/SAS%20matching%202007.pdf. Ac-cessed Feb. 24, 2015.
Cullen MW, Reeder GS, Farkouh ME, et al. Outcomes in patients with chest pain evaluated in a chest pain unit:
the chest pain evaluation in the emer-gency room study cohort. Am Heart J. 2011;161:871–877.
Farkouh ME, Smars PA, Reeder GS, et al. A clinical trial of a chest-pain observation unit for patients with unstable angina. Chest Pain Evaluation in the Emer-gency Room (CHEER) Investigators. N Engl J Med. 1998;339:1882–1888.
Feng Z, Wright B, Mor V. Sharp rise in Medi-care enrollees being held in hospitals for observation raises concerns about causes and consequences. Health Aff (Millwood). 2012;31:1251–1259.
Gaspoz JM, Lee TH, Weinstein MC, et al. Cost-effectiveness of a new short-stay unit to “rule out” acute myocardial infarction in low risk patients. J Am Coll Cardiol. 1994;24:1249–1259.
Goodacre S, Nicholl J, Dixon S, et al. Ran-domised controlled trial and economic evaluation of a chest pain observation unit compared with routine care. BMJ. 2004;328:254.
Graff LG, Dallara J, Ross MA, et al. Impact on the care of the emergency depart-ment chest pain patient from the chest pain evaluation registry (CHEPER) study. Am J Cardiol. 1997;80:563–568.
Halling A, Fridh G, Ovhed I. Validating the Johns Hopkins ACG Case-Mix System of the elderly in Swedish primary health care. BMC Public Health. 2006;6:171.
Hein PA, Romano VC, Lembcke A, et al. Initial experience with a chest pain protocol using 320-slice volume MDCT. Eur Radiol. 2009;19:1148–1155.
Johnson TR, Nikolaou K, Wintersperger BJ, et al. ECG-gated 64-MDCT angio-graphy in the differential diagnosis of acute chest pain. AJR Am J Roentgenol. 2007;188:76–82.
Korley FK, Pham JC, Kirsch TD. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998–2007. JAMA. 2010;304:1465–1471.
Ladapo JA, Hoffmann U, Bamberg F, et al. Cost-effectiveness of coronary MDCT in the triage of patients with acute chest pain. AJR Am J Roentgenol. 2008;191:455–463.
Miller CD, Case LD, Little WC, et al. Stress CMR reduces revascularization, hospi-tal readmission, and recurrent cardiac testing in intermediate-risk patients with acute chest pain. JACC Cardiovasc Imaging. 2013;6:785–794.
Roberts RR, Zalenski RJ, Mensah EK, et al. Costs of an emergency department-based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial. JAMA. 1997;278:1670–1676.
Rubinshtein R, Halon DA, Gaspar T, et al. Usefulness of 64-slice cardiac computed tomographic angiography for diagnos-ing acute coronary syndromes and predicting clinical outcome in emer-
gency department patients with chest pain of uncertain origin. Circulation. 2007;115:1762–1768.
Sayre MR, Bender AL, Dey CC, et al. Evalu-ating chest pain patients in an emer-gency department rapid diagnostic and treatment center is cost-effective. Acad Emerg Med. 1994;1:A45.
Sekhri N. Rapid Access Chest Pain Clinics: Characteristics and Outcomes of Patients from Six Centres [dissertation]. London: Queen Mary University of London; 2009. https://qmro.qmul.ac.uk/xmlui/handle/123456789/592. Accessed Feb. 24, 2015.
Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: charac-teristics of patients with “observation status at an academic medical center. JAMA Intern Med. 2013;173:1991–1998.
Shreibati JB, Baker LC, Hlatky MA. Associa-tion of coronary CT angiography or stress testing with subsequent utiliza-tion and spending among Medicare beneficiaries. JAMA. 2011;306:2128–2136.
Stillman AE, Oudkerk M, Ackerman M, et al; North American Society of Cardiac Imaging; European Society of Cardiac Radiology. Use of multidetector com-puted tomography for the assessment of acute chest pain: a consensus statement of the North American Society of Car-diac Imaging and the European Society of Cardiac Radiology. Int J Cardiovasc Imaging. 2007;23:415–427.
Venkatesh AK, Geisler BP, Gibson Chambers JJ, et al. Use of observation care in US emergency departments, 2001 to 2008. PLoS One. 2011;6(9):e24326. Erratum in: PLoS One. 2012;7(1).
Weiner JP, ed. The Johns Hopkins ACG(r) System Technical Reference Guide. Version 10.0. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health; 2011.
Wright S. Hospitals’ Use of Observation Stays and Short Inpatient Stays for Medicare Beneficiaries. Washington, DC: U.S. Department of Health and Human Services, Office of Inspec-tor General. OEI-02-12-00040. 2013. https://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Feb. 24, 2015.

MARCH 2015 / MANAGED CARE 52A
Economic Efficiencies of Observation Units
APPENDIX
Disease Codes
Current myocardial infarction ICD9=410.xx
Congestive heart failure ICD9=428.xx
Stroke ICD9=430.xx, 431.xx, 432.xx, 434.xx, 435.xx, 436.xx
Cardiac arrest ICD9=427.5x
Chronic rheumatic heart disease ICD9=393.xx–398.xx
Hypertensive disease ICD9=401.xx–405.xx
Ischemic heart disease ICD9=410.xx–414.xx
Diseases of pulmonary circulation ICD9=415.xx–417.xx
Cerebrovascular disease ICD9=430.xx–438.xx
Diseases of arteries, arterioles, and capillaries ICD9=440.xx–448.xx
Diseases of veins and lymphatics, and other diseases of circulatory system
ICD9=451.xx–459.xx
Diabetes mellitus ICD9=250.xx
Dyslipidemia ICD9=272.xx
Coronary artery bypass graft CPT=33510–33519, 33521–33523, 33533–33536
Percutaneous transluminal coronary angioplasty CPT=92980–92984
Mental disorders ICD9=290.xx–319.xx
Digestive disorders ICD9=520.xx–579.xx
Respiratory disorders ICD9= 460.xx–519.xx
FIGUREDetermination of fi nal study sample
69,721 patient visits
Final sample included 15,851 patient visits
30,491 patient visits were excluded for not having 12 months of continuous
enrollment prior to the visit
52,644 patient visits were excluded for having a history of ER visits related
to nonspecifi c chest pain
37 patients died during their visits, 53,709 visits resulting in home discharge were
excluded, and 124 patient visits with both inpatient and observation claims were excluded
152,856 chest pain complaints seen in the ER
122,365 patient visits

52B MANAGED CARE / MARCH 2015
Economic Efficiencies of Observation Units
TABLE 2 Coefficient estimates of quantile regression with median cost difference as the point estimate
ParameterMedian cost
difference ($)a
95% confidence intervalb
PLower limit
($) Upper limit
($)
Observation vs. inpatient -1,308b -1,411 -1,206 <.001
Age 6 2 9 .002
Gender (females are the reference gender) 84 20 148 .01
Risk scores 29 10 48 .002
Chronic rheumatic heart diseases -326 -810 157 .19
Hypertensive disease -33 -101 35 .34
Ischemic heart diseases 200 74 326 .002
Diseases of pulmonary circulation -157 -471 158 .33
Other forms of heart diseasec -36 -134 61 .47
Cerebrovascular disease -8 -172 156 .93
Diseases of arteries, arterioles, and capillaries 260 58 464 .01
Diseases of veins and lymphatics, and other diseases of circulatory system
128 -2 257 .05
Diabetes mellitus 46 -43 134 .31
Dyslipidemia -35 -107 36 .34
Cardiac revascularization -69 -270 132 .50
Diseases of the digestive system 15 -49 79 .65
Mental disorders -30 -93 34 .37
Diseases of the respiratory system 43 -19 105 .17
Used ambulance to reach ER 1,801 1,651 1,950 <.001
Year of ER visit (2009 vs. 2012) -1,040 -1,143 -938 <.001
Year of ER visit (2010 vs. 2012) -690 -769 -612 <.001
Year of ER visit (2011 vs. 2012) -309 -384 -235 <.001
Diagnosis at discharge
Circulatory vs illdefined diagnosis 11,443 10,605 12,280 <.001
Others vs illdefined diagnosis 4,033 3,496 4,570 <.001
Intercept 6,635 6,423 6,847 <.001a Negative number indicates less cost incurred. b Confidence intervals were calculated using the interior algorithm with 10,000 bootstrapping replications.c Other heart diseases include pericarditis, endocarditis, cardiomyopathy, conduction disorders, dysrhythmia, heart failure, and complications of heart diseases.