
Revised Perinatal Hospital Standards 6 - IN.gov of Care Chart Key E Essential requirement for level...
28
2015 Revisions approved by the IPQIC Governing Council June 16, 2015 Revised Indiana Perinatal Hospital Standards
Transcript of Revised Perinatal Hospital Standards 6 - IN.gov of Care Chart Key E Essential requirement for level...

2015
RevisionsapprovedbytheIPQICGoverningCouncilJune16,2015
RevisedIndianaPerinatalHospitalStandards
RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page2
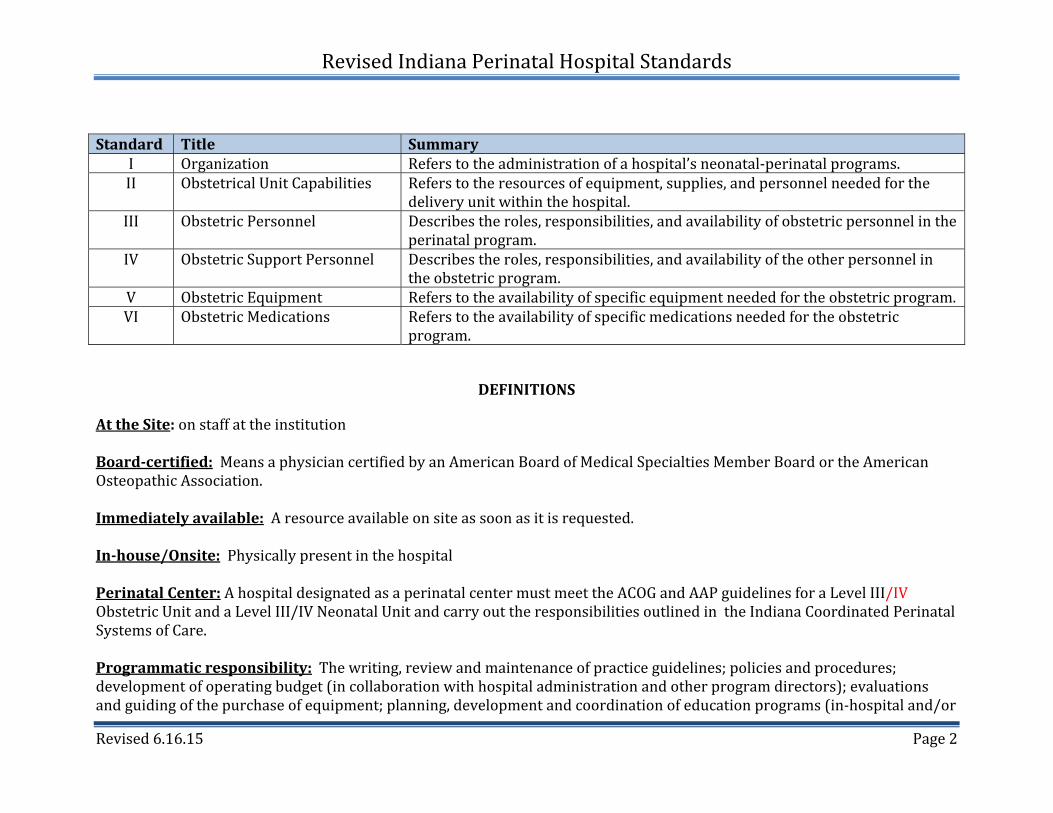
Standard Title SummaryI Organization Referstotheadministrationofahospital’sneonatal‐perinatalprograms.II ObstetricalUnitCapabilities Referstotheresourcesofequipment,supplies,andpersonnelneededforthe
deliveryunitwithinthehospital.III ObstetricPersonnel Describestheroles,responsibilities,andavailabilityofobstetricpersonnelinthe
perinatalprogram.IV ObstetricSupportPersonnel Describestheroles,responsibilities,andavailabilityoftheotherpersonnelin
theobstetricprogram.V ObstetricEquipment Referstotheavailabilityofspecificequipmentneededfortheobstetricprogram.VI ObstetricMedications Referstotheavailabilityofspecificmedicationsneededfortheobstetric
program.
DEFINITIONS
AttheSite:onstaffattheinstitutionBoard‐certified:MeansaphysiciancertifiedbyanAmericanBoardofMedicalSpecialtiesMemberBoardortheAmericanOsteopathicAssociation.Immediatelyavailable:Aresourceavailableonsiteassoonasitisrequested.In‐house/Onsite:PhysicallypresentinthehospitalPerinatalCenter:AhospitaldesignatedasaperinatalcentermustmeettheACOGandAAPguidelinesforaLevelIII/IVObstetricUnitandaLevelIII/IVNeonatalUnitandcarryouttheresponsibilitiesoutlinedintheIndianaCoordinatedPerinatalSystemsofCare.Programmaticresponsibility:Thewriting,reviewandmaintenanceofpracticeguidelines;policiesandprocedures;developmentofoperatingbudget(incollaborationwithhospitaladministrationandotherprogramdirectors);evaluationsandguidingofthepurchaseofequipment;planning,developmentandcoordinationofeducationprograms(in‐hospitaland/or

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page3
outreachasapplicable);participationintheevaluationofperinatalcare;andparticipationofperinatalqualityimprovementandpatientsafetyactivities.Readilyavailable:Aresourceforconsultsandassistanceavailablewithinashorttimeafteritisrequested.30minutes:In‐housewithinthirty(30)minutes.(Exceptionsmayoccurforcircumstancesbeyondanindividual’scontrolsuchasextraordinaryweatherortrafficimpediments).
LevelsofCareChartKey
E EssentialrequirementforlevelofperinatalcenterO OptionalrequirementforlevelofperinatalcenterNA NotApplicable

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page4
OBSTETRICALDEFINITIONS
LevelI
LevelIhospitalshaveperinatalprogramsthatprovidebasiccaretopregnantwomenandinfants,asdescribedbythesestandardsandasstatedinIndianaAdministrativeCode(IAC)Title410:Article15.LevelIfacilities(basiccare)providecaretowomenwhoarelowriskandareexpectedtohaveanuncomplicatedbirth.Thesehospitalsprovidedeliveryroomandnormalnewborncareforstableinfants≥350/7weeksgestation.LevelIfacilitieshavethecapabilitytoperformroutineintrapartumandpostpartumcarethatisanticipatedtobeuncomplicated.Maternitycareproviders,midwives,familyphysicians,orobstetrician–gynecologistsshouldbeavailabletoattendallbirths. Thesehospitalsdonotacceptmaternaltransportsfromhospitalswithobstetricalservices.LevelIILevelIIobstetricalserviceshaveperinatalprogramsthatprovidespecialtycaretopregnantwomenandinfants,asdescribedbythesestandards.LevelIIfacilities(specialtycare)providecaretoappropriatehigh‐riskpregnantwomen,bothadmittedandtransferredtothefacility.InadditiontothecapabilitiesofaLevelI(basiccare)facility,LevelIIfacilitiesshouldhavetheinfrastructureforcontinuousavailabilityofadequatenumbersofRNswhohavedemonstratedcompetenceinthecareofobstetricpatients(womenandfetuses).Thesehospitalsprovidedeliveryroomandacutespecializedcareforinfants≥1,500gramsAND≥320/7weeksgestation.Maternalcareislimitedtotermandpretermgestationsthatarematernalriskappropriate.AlthoughmidwivesandfamilyphysiciansmaypracticeinLevelIIfacilities,anattendingobstetrician–gynecologistshouldbeavailableatalltimes.Aboardcertifiedobstetricianhasresponsibilityforprogrammaticmanagementofobstetricalservices.Thesehospitalsmayreceivematernalreferralswithintheguidelinesoftheirlevel.LevelIII
LevelIIIhospitalshaveobstetricalprogramsthatprovidesubspecialtycareforpregnantwomenandinfants,asdescribedbythesestandards.DesignationofLevelIIIshouldbebasedonthedemonstratedexperienceandcapabilityofthefacilitytoprovidecomprehensivemanagementofseverematernalandfetalcomplications. Thesehospitalsprovideacutedeliveryroomandneonatalintensivecareunit(NICU)careforhigh‐riskmothersandinfants<1,500gramsOR<320/7weeksgestation.

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page5
Maternalcarespanstherangeofnormaltermgestationcaretothemanagementofcomplexmaternalcomplicationsandprematurity.Thedirectorofthematernal–fetalmedicineserviceshouldbeaboard‐certifiedmaternal–fetalmedicinesubspecialist.Aboard‐certifiedobstetrician–gynecologistwithspecialinterestandexperienceinobstetriccareshoulddirectobstetricservices. LevelIIIobstetricalhospitalsacceptriskappropriatematernaltransports.Inacceptingmaternaltransportsthelevelofneonatalcarerequiredforananticipateddeliveryandcareoftheneonatemustbeinplace.
LevelIV
LevelIVfacilities(regionalperinatalhealthcarecenters)includethecapabilitiesofLevelI,LevelII,andLevelIIIfacilitieswithadditionalcapabilitiesandconsiderableexperienceinthecareofthemostcomplexandcriticallyillpregnantwomenthroughoutantepartum,intrapartum,andpostpartumcare.InadditiontohavingICUcareonsiteforobstetricpatients,aLevelIVfacilitymusthaveevidenceofamaternal–fetalmedicinecareteamthathastheexpertisetoassumeresponsibilityforpregnantwomenandwomeninthepostpartumperiodwhoareincriticalconditionorhavecomplexmedicalconditions.Amaternal–fetalmedicineteammemberwithfullprivilegesisavailableatalltimesforon‐siteconsultationandmanagement.Theteamshouldbeledbyaboard‐certifiedmaternal–fetalmedicinesubspecialistwithexpertiseincriticalcareobstetrics.Thedirectorofobstetricservicesisaboard‐certifiedmaternal–fetalmedicinesubspecialistoraboard‐certifiedobstetrician–gynecologistwithexpertiseincriticalcareobstetrics.Inacceptingmaternaltransportsthelevelofneonatalcarerequiredforananticipateddeliveryandcareoftheneonatemustbeinplace.

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page6
STANDARDI.ORGANIZATION‐GOVERNINGBOARDRESPONSIBILITIES1.1Thehospital’sBoardofDirectors,administration,andmedicalandnursingstaffsshalldemonstratecommitmenttoitsspecificlevelperinatalcenterdesignationandtothecareofperinatalpatients.ThiscommitmentshallbedemonstratedbyaBoardresolutionthat:
a) ThehospitalagreestomeettheIndianaPerinatalSystemStandardsforitsspecificlevelofdesignationthroughits
commitmenttothefinancial,human,andphysicalresourcesandtotheinfrastructurethatisnecessarytosupportthehospital’slevelofcaredesignation.
b) ThehospitalagreestoconductinternalauditingandattestationusingscreeningformsprovidedbytheIndianaStateDepartmentofHealth(ISDH).OncetheISDHformiscompleted,itistobesignedbytheCEOtoverifythatinformationsubmittedistrueandaccurate.
c) Thehospitalassuresthatallperinatalpatientsshallreceivemedicalcarecommensuratewiththelevelofthehospital’sdesignation.
d) Thehospitalagreestoberesponsibleforcredentialing,licensingandtrainingofallneonatalandobstetricalstaffbasedonthehospital’sdesignatedlevelofcare.Thehospitalisalsoresponsibleforensuringthatallhealthcareworkersmaintaincurrentlicenses,registrationorcertification,andkeepdocumentationofthisinformationwiththeabilitytohavethematerialavailablewithinareasonableamountoftime.410IAC15‐1.4‐1
e) Thehospitalagreestohavewrittenmedicalstaffpoliciesandproceduretoaddressemergentneonatalandobstetricalemergencies,initiatingtreatmentandreferringwhenappropriate.Thehospitalwillbeabletoprovideimmediatelifesavingmeasuresandhavetheappropriatestaffreadilyavailabletocareforemergentneonatalandobstetricpatientneeds,includingtimelyassessment,stabilization,andtreatmentpriortotransfer.Transfersshouldbearrangedwhenneededalongwithcopiesofthepatients’recordsandtreatmentsprovidedtotheacceptingfacility410IAC15‐1.4‐1

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page7
STANDARDII.OBSTETRICALUNITCAPABILITIES I II III IV2.1Thehospitalshalldemonstrateitscapabilityofprovidinguncomplicatedandcomplicatedobstetricalcarethroughwrittenstandards,protocols,guidelinesandtrainingincludingthefollowing:
a) Managingunexpectedobstetricalandneonatalproblems. E E E Eb) Providingfetalmonitoring,includinginternalscalpelectrodemonitoring. E E E Ec) Initiatinganemergentcesareandeliverywithinatimeintervalthatbest
incorporatesmaternalandfetalrisksandbenefitswiththeprovisionofemergencycare.
E E E E
d) Selectingandmanagingobstetricalpatientsatamaternalrisklevelappropriatetoitscapability. E E E E
e) Providingcriticalcareservicesappropriateforobstetricalpatients,asdemonstratedbyhavingacriticalcareunitandaboard‐certifiedcriticalcarespecialist,readilyavailableatalltimes.
NA NA E E
f) Assuringavailabilityofanesthesia,radiology,ultrasound,laboratory,andbloodbankservicesatalltimes E E E E
g) Determiningthelevelofcompetenceandqualificationsrequiredforstafftoassumeclinicalresponsibilityforneonatalresuscitation24hoursadayand7daysaweek.
E E E E
h) Initiatingmaternaltransportstoanappropriatelevel. E E E Ei) Havingawrittenplanforacceptinglevelbasedmaternaltransports O E E Ej) Havingwrittenplanforconsultationandtransferarrangements. E E E Ek) Havingprotocolsandcapabilitiesformassivetransfusion,emergency
releaseofbloodproducts(beforefullcompatibilitytestingiscomplete)andmanagementofmultiplecomponenttherapy.
E E E E
2.2Thematernityservicehasaccesstothehospital’slaboratoryservicesincluding24‐hourcapabilitytoprovidebloodgroup,Rhtype,cross‐matching,antibodytestingandbasicemergencylaboratoryevaluations,andeitherABO‐Rh‐specificorO‐Rh‐negativebloodandfreshfrozenplasmaandcryoprecipitateatthefacilityatalltimes.
E E E E
2.3HospitalshallfollowcurrentCDC/ACOGrecommendationsregardinginductionoflabor,GroupBstreptococci(GBS)treatment,andHIVtreatment. E E E E
2.4Thehospitalshallhavegeneticdiagnosticandcounselingservicesorpolicyfor O E E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page8
STANDARDII.OBSTETRICALUNITCAPABILITIES I II III IVconsultationreferralsfortheseservicesinplace.
2.5Thehospitalshallhavealaboratorycapableofperformingfetallungmaturitytests. O E E E
2.6Thehospitalshallhaveafullrangeofinvasivematernalmonitoringavailabletothedeliveryarea,includingequipmentforcentralvenouspressureandarterialpressuremonitoring.
O O E E
2.7Thehospitalshallhavespecialequipmentneededtoaccommodatethecareandservicesneededforobesewomen. O E E E
2.8ThehospitalshallhaveappropriateequipmentandpersonnelavailableonsitetoventilateandmonitorwomeninlaboranddeliveryuntilsafelytransferredtoanICU
NA NA E E
2.9ThehospitalICUcollaboratesactivelywiththeMFMcareteaminthemanagementofallpregnantwomenandwomeninthepostpartumperiodwhoareincriticalconditionorhavecomplexmedicalconditions.ThehospitalICUco‐managesICUadmittedobstetricpatientswiththeMFMteam.
NA NA E E
2.10Hospitalsofferingatrialoflaborforpatientswithapriorcesareandeliverymusthaveimmediatelyavailableappropriatefacilitiesandpersonnelwiththecapacityforanesthesia,cesareansection,andneonatalresuscitationcapabilityduringthetrialoflabor.
E E E E
STANDARDIII.OBSTETRICPERSONNEL I II III IV3.1Ataminimum,eachdeliveryhospitalmusthavethefollowingprimarydeliveryprovidersavailabletoattendalldeliverieswhenapatientisinactivelabor:
a) Obstetricprovider(OB‐GYN,SurgeonorFamilyPracticephysicianwithadditionaltraininginobstetrics)withappropriatetrainingandprivilegestoperformemergencycesareandeliveryshouldbeavailabletoattendalldeliveries.
E NA NA NA
b) Aproviderboard‐certifiedorboardeligibleinobstetrics/gynecologyormaternal‐fetalmedicineavailableatalltimes NA E E E
c) Aproviderboard‐certifiedorboardeligibleinobstetrics/gynecologyor NA NA E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page9
STANDARDIII.OBSTETRICPERSONNEL I II III IVmaternal‐fetalmedicineonsiteatalltimes
3.2Aprovider(orproviders)board‐certifiedorboardeligibleinmaternal‐fetalmedicineshallbe:
a) Availableforconsultationon‐site,byphoneorbytelemedicineasneeded. E E NA NAb) Availableatalltimesonsite,byphoneorbytelemedicinewithinpatient
privileges NA O E NA
c)Availableatalltimesforonsiteconsultationandmanagement NA NA O1 E3.3Aproviderboard‐certifiedinobstetrics/gynecologywithexperienceand
interestinobstetricsshallbeamemberofthemedicalstaffandhaveresponsibilityforprogrammaticmanagementofobstetricalservices.
O E E NA
3.4Aproviderboard‐certifiedinmaternal‐fetalmedicineorboard‐certifiedinobstetrics/gynecologywithexpertiseincriticalcareobstetrics,shallbeamemberofthemedicalstaffandhaveresponsibilityforprogrammaticmanagementofhigh‐riskobstetricalservices.
NA O O2 E
3.5Aboard‐certifiednurse‐midwifewithobstetricalprivilegesmaybeamemberoftheobstetricalstaffincollaborationwithalicensedphysicianwithobstetricalprivileges.
0 0 0 O
3.6MedicalandSurgicalConsultantservicesmustbeavailablecommensuratewiththelevelofcareprovided.a) Establishedagreementwithahigher‐levelreceivinghospitalfortimely
transport,includingdeterminationofconditionsnecessitatingconsultationandreferral
E NA NA NA
b) MedicalandSurgicalconsultantsavailabletostabilize NA E E Ec) Fullcomplementofsubspecialistsavailableforinpatientconsultation
includingcriticalcare,generalsurgery,infectiousdisease,hematology,cardiology,nephrology,neurology,andneonatology.
NA NA E E
d) Adultmedicalandsurgicalspecialtyandsub‐specialtyconsultantsimmediatelyavailableatalltimesincludingthoseindicatedinLevelIIIandadvancedneurosurgeryorcardiacsurgery.
NA NA NA E
1ExpectedforhospitalswishingtobedesignatedasaPerinatalCenter2ExpectedforhospitalswishingtobedesignatedasaPerinatalCenter

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page10
STANDARDIII.OBSTETRICPERSONNEL I II III IV3.7Anesthesiaserviceshouldmeettheneedsofthepatientsserved,withinthe
scopeoftheserviceoffered,inaccordancewithacceptablestandardsofpractice,andunderthedirectionofaqualifiedphysician.
E E E E
a) Anesthesiaservicesshouldbeavailabletoprovidelaboranalgesiaandsurgicalanesthesia.
E E E E
b) Aproviderboard‐certifiedorboardeligibleinanesthesiologywithspecialtrainingorexperienceinobstetricsshallbereadilyavailableforconsultation.
O E NA NA
c) Aproviderboard‐certifiedorboardeligibleinanesthesiologywithspecialtrainingorexperienceinobstetricsshallbeavailableatalltimesonsite. O O E E
3.8Aproviderboard‐certifiedinanesthesiologyshallbeamemberofthemedicalstaffandhaveresponsibilityforprogrammaticmanagementofanesthesiaservices.
E E E E
3.9Thehospitalshallhaveappropriatelyqualifiedmedicalstaffavailabletoperformandinterpretobstetricultrasonographyatalltimes. E E E E
3.10Thehospitalshallhaveappropriatelyqualifiedmedicalstafftoperformandinterpretcomputedtomographyscans,magneticresonanceimagingwithinterpretationsformaternalandfetalassessment
NA E E E
3.11Thehospitalshallhaveappropriatelyqualifiedmedicalstafftoperformbasicinterventionalradiology,maternalechocardiography,computedtomography,magneticresonanceimagingandnuclearmedicineimagingwithinterpretation,detailedobstetricultrasonographyandfetalassessmentincludingDopplerstudiesavailableatalltimes.
O O E E
3.12Thehospitalshallhaveappropriatelyqualifiednursingpersonnelinadequatenumberstomeettheneedsofeachpatientinaccordancewiththecaresettingincluding:
E E E E
a) Aregisterednursewithdemonstratedtrainingandexperienceintheassessment,evaluationandcareofpatientsinlaborpresentatalldeliveries. E E E E
b) Aregisterednurseskilledintherecognitionandnursingmanagementofthecomplicationsoflaboranddeliveryreadilyavailableifneededtothelaboranddeliveryunitatalltimes.
E E E E
RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page11
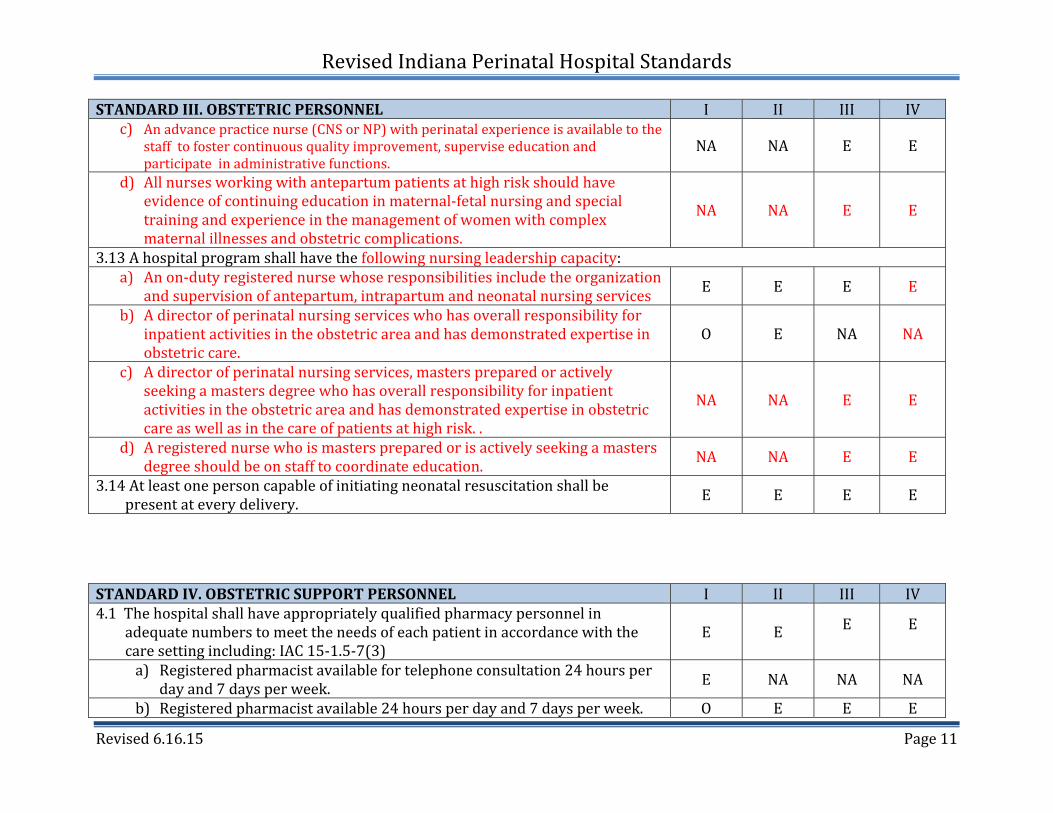
STANDARDIII.OBSTETRICPERSONNEL I II III IVc) Anadvancepracticenurse(CNSorNP)withperinatalexperienceisavailabletothe
stafftofostercontinuousqualityimprovement,superviseeducationandparticipateinadministrativefunctions.
NA NA E E
d) Allnursesworkingwithantepartumpatientsathighriskshouldhaveevidenceofcontinuingeducationinmaternal‐fetalnursingandspecialtrainingandexperienceinthemanagementofwomenwithcomplexmaternalillnessesandobstetriccomplications.
NA NA E E
3.13Ahospitalprogramshallhavethefollowingnursingleadershipcapacity:a) Anon‐dutyregisterednursewhoseresponsibilitiesincludetheorganization
andsupervisionofantepartum,intrapartumandneonatalnursingservices E E E E
b) Adirectorofperinatalnursingserviceswhohasoverallresponsibilityforinpatientactivitiesintheobstetricareaandhasdemonstratedexpertiseinobstetriccare.
O E NA NA
c) Adirectorofperinatalnursingservices,masterspreparedoractivelyseekingamastersdegreewhohasoverallresponsibilityforinpatientactivitiesintheobstetricareaandhasdemonstratedexpertiseinobstetriccareaswellasinthecareofpatientsathighrisk..
NA NA E E
d) Aregisterednursewhoismasterspreparedorisactivelyseekingamastersdegreeshouldbeonstafftocoordinateeducation. NA NA E E
3.14Atleastonepersoncapableofinitiatingneonatalresuscitationshallbepresentateverydelivery. E E E E
STANDARDIV.OBSTETRICSUPPORTPERSONNEL I II III IV4.1Thehospitalshallhaveappropriatelyqualifiedpharmacypersonnelin
adequatenumberstomeettheneedsofeachpatientinaccordancewiththecaresettingincluding:IAC15‐1.5‐7(3)
E E E E
a) Registeredpharmacistavailablefortelephoneconsultation24hoursperdayand7daysperweek. E NA NA NA
b) Registeredpharmacistavailable24hoursperdayand7daysperweek. O E E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page12
STANDARDIV.OBSTETRICSUPPORTPERSONNEL I II III IVc) Registeredpharmacistwithexperienceinperinatal/neonatal
pharmacologyavailable24hoursperdayand7daysperweek. NA O E E
4.2The hospital shall have at least one registered dietitian or nutritionist who has special training in perinatal nutrition and can plan diets that meet the special needs of both women and neonates at high risk
O E E E
4.3ThehospitalshallprovidelactationsupportperAWHONNandILCArecommendation:a) LevelI1.3FTEper1000deliveriesperyear E NA NA NAb) LevelII1.6FTEper1000deliveriesperyear NA E NA NAc) LevelIII/IV1.9FTEsper1000deliveries NA NA E E
4.4ThehospitalshallhavealicensedsocialworkerorRNCaseManagerwithexperienceinpsychosocialassessmentandinterventionwithwomenandtheirfamiliesreadilyavailabletotheperinatalservice.
E E E E
4.5Thehospitalshallhaveatleastonestaffmemberwithexpertiseinbereavementresponsibleforthehospital’sbereavementactivities,includingasystemicapproachtoensuringthatindividualsinneedreceivetheappropriateservices.
OE
E
E
4.6Aregisterednurseshallsuperviselicensedpracticalnursesandotherlicensedpatientcarestaffwhodemonstrateknowledgeandclinicalcompetenceinthenursingcareofwomen,fetuses,andnewbornsduringlabor,delivery,andthepostpartumandneonatalperiods.
E E E E
4.7Bloodbanktechniciansshallbeimmediatelyavailable24hoursaday. O E E E
STANDARDV.OBSTETRICEQUIPMENT I II III IV5.1Thehospitalshallhaveequipmentforperforminginterventionalradiology
servicesforobstetricalpatients. O O E E
5.2Thehospitalwillhavethefollowingequipmentavailableandthecapabilitytouseasindicated.:a) Non‐stressandstresstesting E E E Eb) Ultrasonography E E E Ec) UltrasonographywithDopplerCapability O O E Ed) Portableobstetricultrasonographyequipment,withtheservicesof O E E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page13
STANDARDV.OBSTETRICEQUIPMENT I II III IVappropriatesupportstaff,shallbeavailableinthedeliveryarea
e) ComputedTomography O E E Ef) MagneticResonanceImaging NA O E Eg) NuclearMedicineImaging NA O E Eh) Amniocentesis O E E Ei) Cardioversion/defibrillationcapabilityformothers E E E Ej) Resuscitationequipmentformothers E E E Ek) Adultbagandmasksystemscapableofdeliveringacontrolled
concentrationofoxygen E E E E
l) Orotrachealtubes,endotrachealtubesinarangeofsizesforadultintubation E E E E
m) Wallsuctionandaspirationequipment E E E En) Laryngoscopes E E E Eo) Bloodpressurecuffsinfullrangeofsizes,formanualandmachineuse E E E Ep) Pulseoximeter E E E Eq) Arterialbloodgasmachine E E E Er) Fiberopticscopesforawakeintubation E E E Es) Arteriallinekits NA O E Et) Centralvenouslinekits NA O E Eu) Invasivehemodynamicmonitoringequipment NA NA E Ev) Adultechocardiographyequipment NA NA E Ew) Individualoxygen,airO2blendedandhumidifiedcapability,andsuction
outlets E E E E
x) Emergencycallsystem E E E E
STANDARDVI.OBSTETRICMEDICATIONS I II III IV6.1Allemergencyresuscitationmedicationsandequipmentneededtoinitiateand
maintainresuscitationshallbepresentinthedeliveryareainaccordancewithAdvancedCardiacLifeSupport(ACLS),NeonatalResuscitationProgram.
E E E E
6.2Thefollowingmedicationsshallbeinthedeliveryareaorimmediatelyavailabletothedeliveryarea:

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page14
STANDARDVI.OBSTETRICMEDICATIONS I II III IVa) Oxytocin(Pitocin) E E E Eb) Methylergonovine(Methergine) E E E Ec)15‐methylprostaglandinF2(Prostin) E E E Ed)Misoprostol E E E Ee)Carboprosttromethamine(Hemabate) E E E Ef)Narcotics E E E Eg)Antibiotics E E E Eh)Magnesiumsulfate E E E Ei)Naloxone E E E E
j)Lorazepam E E E E
NEONATALSECTION‐DEFINITIONS THESESTANDARDSREFLECTTHEREVISEDAAPPOLICYSTATEMENTONLEVELSOFNEONATALCARE20123
LevelIHospitalshaveneonatalprogramsthatprovideabasiclevelofcaretoinfantswhoarelowrisk,asdescribedbythesestandards.Thesehospitalsprovidenormalnewborncareforinfants≥350/7weeksgestationwhoarephysiologicallystable.Theymusthavethecapabilitiestoperformneonatalresuscitationateverydeliveryandtoevaluateandprovideroutinepostnatalcareforhealthynewborninfants.LevelIhospitalsmustbeabletostabilizenewborninfantswhoarelessthan35weeksofgestationorwhoareilluntiltheycanbetransferredtoafacilityatwhichspecialtyneonatalcareisprovided.Boardcertifiedpediatriciansorfamilyphysicianswithprivilegesfornewbornresuscitationsupervisetheseunits.Theseneonatalunitsdonotprovidepediatricsubspecialtyorneonatalsurgicalspecialtyservices.Thesehospitalsdonotreceiveprimaryinfantormaternalreferrals.
3TheAAPCommitteeonFetusandNewbornsissuedthePolicyStatementonLevelsofNeonatalCareonAugust27,2012.www.pediatrics.org/cgi/doi/10.1542/peds.2012‐1999PEDIATRICS(ISSNNumbers:Print,0031‐4005;Online,1098‐4275).

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page15
LevelIIHospitalshaveneonatalprogramsthatprovidespecialtycaretoinfants,asdescribedbythesestandards.Thesehospitalsmusthavetheabilitytoprovidecareforstableormoderatelyillinfants≥1,500gramsAND≥320/7weeksgestationwithproblemsthatareexpectedtoresolverapidlyandnotanticipatedtoneedsubspecialty‐levelservicesonanurgentbasis.Thesehospitalsmusthavetheabilitytoprovideassistedconventionalventilationorcontinuouspositiveairwaypressureorbothforbriefdurations,generallylessthan24hours.LevelIInurseriesmusthavetheabilitytostabilizeinfantsbornbefore32weeksgestationandweighinglessthan1500gramsuntiltransfertoaneonatalintensivecarefacility.LevelIInurseriesmusthaveequipmentandpersonnelcontinuouslyavailabletoprovideongoingcareaswellastoaddressemergencies.Thesehospitalsdonotreceiveprimaryinfanttransports.Thehospitalshallhaveawrittenplanforacceptingortransferringmothersorneonatesas“backtransports”forongoingconvalescentcare,includingcriteriaforacceptingthepatientandpatientinformationontherequiredcase.Theseneonatalunitsaresupervisedbyaboard‐certifiedpediatrician,andhaveprearrangedconsultativeagreementswithalevelIIIorIVcenter.LevelIII
Hospitalsprovidesubspecialtycareforinfantsasdescribedbythesestandards.ThesehospitalsprovideacuteandcomprehensiveNICUcareforinfantswhoarebornat<32weeksgestationand<1500gramsatbirth,orhavemedicalorsurgicalconditionsregardlessofgestationalageorweight.DesignationofLevelIIIcareshouldbebasedonclinicalexperienceasdemonstratedbylargepatientvolume,increasingcomplexityofcare,andavailabilityofpediatricmedicalsubspecialistsandpediatricsurgicalspecialists4.Pediatricsurgicalspecialists(includinganesthesiologistswithpediatricexperience)shouldperformallproceduresinnewborninfants.Pediatricophthalmologyservicesandanorganizedprogramforthemonitoring,treatment,andfollow‐upofretinopathyofprematurityshouldbereadilyavailableinLevelIIInurseries.TheneonatalunitsaresupervisedbyBoard‐certifiedneonatologistsandoffercontinuousavailabilityofneonatologists.Neonatalunitsprovidea4AccordingtotheAAPpolicystatement“Althoughlittledebateexistsontheneedforadvancedneonatalservicesforthemostimmatureandsurgicallycomplexneonates,ongoingcontroversiesexistregardingwhichfacilitiesarequalifiedtoprovidetheseservicesandwhatisthemostappropriatemeasureforsuchqualification.Theseissuesare,ingeneral,basedontheneedforcomparisonoffacilityexperience(measuredbypatientvolumeorcensus),location(inborn/outborndeliveries,regionalperinatalcenter,orchildren’shospital)orcase‐mix(includingstillbirths,deliveryroomdeaths,andcomplexcongenitalanomalies).”ThereisanexpectationthatthenextreviewoftheAAPLevelsofNeonatalCarepolicystatementwillindicateappropriatepatientvolumeforeachlevelofneonatalcare.TheAAPPolicyStatementonLevelsofNeonatalCare,August27,2012.www.pediatrics.org/cgi/doi/10.1542/peds.2012‐1999

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page16
fullrangeofrespiratorysupportthatmayincludeconventionalventilation,and/orinhalednitricoxide,and/orhigh‐frequencyventilationifsuitableequipmentandproperlytrainedpersonnelareavailable.Pediatricmedicalsubspecialtyservicesmaybeprovidedonsiteorconsultationmaybeprovidedatacloselyrelatedinstitutionwhichallowsforemergencytransportwithinareasonabletimebetweeninstitutions.Pediatricsurgicalandanesthesiologysubspecialistsmaybeonsiteoratacloselyrelatedinstitutiontoperformmajorsurgeries.Neonatalcarecapabilityincludesadvancedimaging,withinterpretationonanurgentbasisthatincludescomputedtomography,magneticresonanceimaging,andechocardiography.LevelIIIperinatalhospitalsacceptrisk‐appropriatematernalandneonataltransports.Thehospitalshallhaveawrittenplanforacceptingortransferringmothersorneonatesas“backtransports”forongoingconvalescentcare,whichincludescriteriaforacceptingthepatientandpatientinformationontherequiredcase.LevelIVHospitalsprovidecomprehensivesubspecialtyneonatalcareservices,asdescribedbythesestandards.ThesehospitalsprovideacuteNICUcareforinfantsofallbirthweightsandgestationalages.Inaddition,theneonatologistsassistinthemanagementoffetuseswhoareextremelyprematureorhavecomplexproblemsthatrendersignificantriskofpreterm,delivery,andpostnatalcomplications.TheneonatalunitsaresupervisedbyBoard‐certifiedneonatal‐perinatalsubspecialistsandoffercontinuousavailabilityofneonatologists.Advancedmodesofneonatalventilationandlife‐supportareprovided,includinghighfrequencyventilation,inhalednitricoxideand/orextracorporealmembraneoxygenation(ECMO).Theseneonatalunitsprovideafullrangeofmedicalpediatricsubspecialtyservices.Additionally,afullrangeofpediatricsubspecialtysurgicalservicesandpediatricanesthesiologistsareavailableatthesite,includingpediatriccardio‐thoracicopen‐heartsurgeryandpediatricneurosurgery.LevelIVperinatalhospitalsacceptmaternalandneonataltransports.Thesehospitalsfacilitatetransportandprovideoutreacheducation.STANDARDVII.NEONATALUNITCAPABILITIES I II III IV
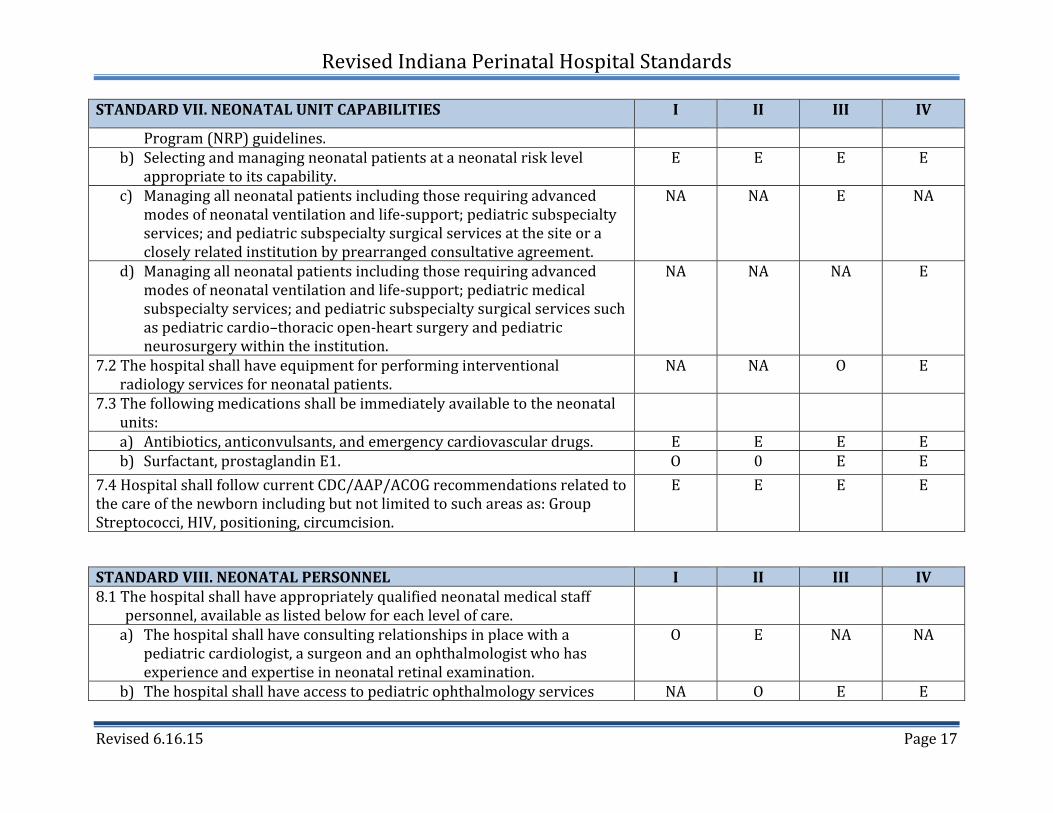
7.1Thehospitalshalldemonstrateitscapabilityofprovidingneonatalcarethroughwrittenstandards,protocols,guidelines,andtraining,thatincludethefollowing:
a) ProvidingresuscitationandstabilizationofunexpectedneonatalproblemsaccordingtothemostcurrentNeonatalResuscitation
E E E E
RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page17
STANDARDVII.NEONATALUNITCAPABILITIES I II III IV
Program(NRP)guidelines.b) Selectingandmanagingneonatalpatientsataneonatalrisklevel
appropriatetoitscapability.E E E E
c) Managingallneonatalpatientsincludingthoserequiringadvancedmodesofneonatalventilationandlife‐support;pediatricsubspecialtyservices;andpediatricsubspecialtysurgicalservicesatthesiteoracloselyrelatedinstitutionbyprearrangedconsultativeagreement.
NA NA E NA
d) Managingallneonatalpatientsincludingthoserequiringadvancedmodesofneonatalventilationandlife‐support;pediatricmedicalsubspecialtyservices;andpediatricsubspecialtysurgicalservicessuchaspediatriccardio–thoracicopen‐heartsurgeryandpediatricneurosurgerywithintheinstitution.
NA NA NA E
7.2Thehospitalshallhaveequipmentforperforminginterventionalradiologyservicesforneonatalpatients.
NA NA O E
7.3Thefollowingmedicationsshallbeimmediatelyavailabletotheneonatalunits:
a) Antibiotics,anticonvulsants,andemergencycardiovasculardrugs. E E E Eb) Surfactant,prostaglandinE1. O 0 E E
7.4HospitalshallfollowcurrentCDC/AAP/ACOGrecommendationsrelatedtothecareofthenewbornincludingbutnotlimitedtosuchareasas:GroupStreptococci,HIV,positioning,circumcision.
E E E E
STANDARDVIII.NEONATALPERSONNEL I II III IV8.1Thehospitalshallhaveappropriatelyqualifiedneonatalmedicalstaff
personnel,availableaslistedbelowforeachlevelofcare.
a) Thehospitalshallhaveconsultingrelationshipsinplacewithapediatriccardiologist,asurgeonandanophthalmologistwhohasexperienceandexpertiseinneonatalretinalexamination.
O E NA NA
b) Thehospitalshallhaveaccesstopediatricophthalmologyservices NA O E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page18
STANDARDVIII.NEONATALPERSONNEL I II III IVc) Thehospitalshallhaveavailabilitytoperformstatandroutinecardiac
echoandEEGs24hoursadayand7daysaweek,andavailableinterpretationforstatcardiacechowithin1hourandforroutinestudieswithin24hours.
NA O E E
d) Thehospitalshallhavepromptandreadilyavailableaccesstoafullrangeofpediatricmedicalsubspecialists,pediatricsurgicalspecialists,anesthesiologistswithpediatricexperience,andpediatricophthalmologistsatthesiteoratacloselyrelatedinstitutionbyprearrangedconsultativeagreement.
NA O E NA
e) Thehospitalshallmaintainafullrangeofpediatricmedicalsubspecialists,pediatricsurgicalsubspecialists,andanesthesiologistswithpediatricexperienceatthesite.
NA O O E
f) Thehospitalshallbelocatedwithinaninstitutionwiththecapabilitytoprovideon‐sitepediatricsurgicalcareofcomplexcongenitaloracquiredconditions.
NA NA NA E
8.2Aproviderboard‐certifiedinpediatricsorfamilymedicineshallbeamemberofthemedicalstaff,haveprivilegesforneonatalcare,andhaveresponsibilityforprogrammaticmanagementforneonatalunitservices.
E NA NA NA
8.3Aproviderboard‐certifiedinpediatricsorinneonatal‐perinatalmedicineshallbeamemberofthemedicalstaff,haveprivilegesforneonatalcare,andhaveresponsibilityforneonatalunitservices.
O E NA NA
8.4Aprovider(s)board‐certifiedinneonatal‐perinatalmedicineshallbeamemberofthemedicalstaffandhavefull‐timeresponsibilityforneonatalspecialcareorintensivecareunitservices.
NA O E E
8.5Thehospitalshallhaveprearrangedconsultativeagreementswithaboard‐certifiedneonatologist24hoursaday.
E E NA NA
8.6NeonatalResuscitationProgram(NRP)trainedprofessional(s)shallbeimmediatelyavailabletothedeliveryandneonatalunits.
E E E E
8.7Aproviderwhohascompletedpostgraduatepediatrictraining,anursepractitioner,familyphysicianorphysicianassistantwithprivilegesforneonatalcareappropriatetothelevelofthenurseryshallbeavailable
NA E NA NA

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page19
STANDARDVIII.NEONATALPERSONNEL I II III IVwhenaninfantrequiresLevelIIneonatalservicessuchasFiO2>40%,assistedventilation,orcardiovascularsupport.
8.8APediatricianwhohascompletedpediatricresidencytraining,anursepractitionerorphysicianassistantwithadequateNICUtrainingandexperience,withprivilegesforneonatalcareappropriatetothelevelofthenursery,shallbephysicallypresentin‐house24hoursadayandassignedtothedeliveryareaandneonatalunitsandnotsharedwithotherunitsinthehospital.
NA O E E
8.9Aboard‐certifiedprovideroranactivecandidateforboard‐certificationinneonatologyshallbeavailabletobepresentin‐housewithin30minutes.
NA O E E
8.10Thehospitalshallhave: a)Aprearrangedwrittenplanwithaneurodevelopmentalfollow‐upclinic
orneurodevelopmentalpractice.O O E NA
b)Aneurodevelopmentalfollow‐upclinicorpractice O O O E8.11Thehospitalshallhaveaprovideronthemedicalstaffwithprivilegesfor
providingcriticalinterventionalradiologyservicesforneonatalpatients.O O O E
8.12Thehospitalshallhaveappropriatelyqualifiedneonatalpersonnelinadequatenumberstomeettheneedsofeachpatientinaccordancewiththecaresetting:
a) Aregisterednursewithdemonstratedtrainingandexperienceintheassessment,evaluationandcareofnormalnewbornsatalltimes.
E E E E
b) Aregisterednurseskilledintherecognitionandnursingmanagementoftheneonatewithcomplicationsontheunitatalltimes.
NA E NA NA
c) Anadvancepracticenurse(CNSorNP)withperinatalexperienceisavailabletothestafftofostercontinuousqualityimprovement,superviseeducationandparticipateinadministrativefunctions.
NA NA E E
d) Allnursesworkingwithneonatesathighriskshouldhaveevidenceofcontinuingeducationinneonatalnursingandspecialtrainingandexperienceinthemanagementofneonateswithcomplex
NA NA E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page20
STANDARDVIII.NEONATALPERSONNEL I II III IVillnessesandneonatalcomplications
8.13Thehospitalshallhaverespiratorytherapistswhoare: a) Experiencedinthedeliveryofcontinuouspositiveairwaypressure
and/ormechanicalventilationorbothreadilyavailable.NA E E E
b) SkilledinneonatalventilatorcareandmanagementassignedtotheNICUandnotsharedwithotherunitswhenanypatientisreceivingassistedpositivepressureventilation,high‐frequencyventilation,and/orinhalednitricoxide24hoursaday.
NA NA E E
8.14Ahospitalprovidingneonatalsurgicalservicesshallhavenursesonstaffwithspecialexpertiseinperioperativemanagementofneonates.
NA NA E E
8.15ThehospitalshallprovidelactationsupportperAWHONNandILCArecommendation:a) LevelI1.3FTEper1000deliveriesperyear
b) LevelII1.6FTEper1000deliveriesperyear
c) LevelIIIandIV1.9FTEsper1000deliveries
E E E E
8.16Thehospitalshallhaveafull‐timeInternationalBoardCertifiedLactationConsultantwithexperienceinlactationsupportforthemotherofapreterminfant.
NA O E E
8.17ThehospitalshallhavealicensedsocialworkerorRNCaseManager,withexperienceinpsychosocialassessmentandinterventionwithwomenandtheirfamilieswhois:
a) Readilyavailable E E E Eb) Dedicatedtotheperinatalservice. O O E E
8.18ThehospitalshallhavePhysicalTherapistand/orOccupationalTherapist,withadditionalContinuingEducationUnitsintheareaofneonatalcare,asamemberoftheinterdisciplinarycareteam.
NA O E E
8.19ThehospitalshallhaveaSpeechTherapist,withadditionalContinuingEducationUnitsintheareaofneonatalcare,asamemberoftheinterdisciplinarycareteam.
NA O E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page21
STANDARDVIII.NEONATALPERSONNEL I II III IV8.20Thehospitalshallhavequalifiednursingleadershipinaccordancewith
thecaresetting:
a) Nursingcareshouldbeundertheleadershipofaregisterednurse E NA NA NAb) Nursingcareshouldbeundertheleadershipofaregisterednursewith
demonstratedexpertiseinobstetriccare,neonatalcareorboth O E NA NA
c) Nursingcareshouldbeundertheleadershipofaregisterednurse,masterspreparedoractivelyseekingamastersdegree,withexperienceandtraininginneonatalnursing,aswellasinthecareofpatientsathighrisk.
O O E E
8.21Aregisterednursewhohasbeeneducatedandmasterspreparedoractivelyseekingamastersdegree,shouldbeonstafftocoordinateeducation.
O O E E
8.22Ahospitalperinatalprogramshallhaveat least one registered dietitian or nutritionist who has special training in perinatal nutrition and can plan diets that meet the special needs of neonates at high risk
O O E E
8.23Thehospitalshallhaveappropriatelyqualifiedpharmacypersonnelinadequatenumberstomeettheneedsofeachpatientinaccordancewiththecaresettingincluding:IAC15‐1.5‐7(3)
E E E E
a)Registeredpharmacistavailablefortelephoneconsultation24hoursperdayand7daysperweek.
E NA NA NA
b)Registeredpharmacistavailable24hoursperdayand7daysperweek.
NA E E E
c)Ahospitalperinatalprogramshallhavepharmacy personnel with pediatric expertise who can work to continually review their systems and processes of medication administration to ensure that patient care policies are maintained.
O O E E
STANDARDIX.NEONATALSUPPORTPERSONNEL I II III IV9.1Portableultrasonographyfornewborns,withtheservicesofappropriate
supportstaff,shallbeavailabletotheneonatalunits.O E E E

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page22
9.2Computedtomography(CT)capability,withtheservicesofappropriatesupportstaff,shallbeavailableoncampus.
O O E E
9.3Magneticresonanceimaging(MRI)capability,withtheservicesofappropriatesupportstaff,shallbeavailableoncampus.
O O E E
9.4Neonatalechocardiographyequipmentandexperiencedtechnicianwithinterpretationbypediatriccardiologistshallbeimmediatelyavailable.
O O E E
9.5Thehospitalshallhaveapediatriccardiaccatheterizationlaboratoryandappropriatestaff.
O O O E
9.6Portablex‐rayequipment,withtheservicesofappropriatesupportstaff,shallbeavailabletotheneonatalunits.
E E E E
9.7Bloodbanktechniciansshallbepresentin‐house24hoursaday. O E E E
STANDARDX.NEONATALEQUIPMENT I II III IV10.1Thehospitalshallobtainandmaintaincurrentequipmentand
technology,asdescribedinthesestandards,tosupportoptimalneonatalcareforthelevelofcareofthehospitalsdesignation.
E E E E
10.2Thehospitalshallhaveallofthefollowingequipmentandsuppliesimmediatelyavailableforexistingpatientsandforthenextpotentialpatient:
a) pulseoximeterb) phototherapyunitc) Dopplerbloodpressureforneonatesd) cardioversion/defibrillationcapabilityforneonatese) resuscitationequipmentforneonatesf) individualoxygen,airO2blendedandhumidifiedcapability,and
suctionoutletsformothersandneonatesg) emergencycallsystemh) bowelbags
E E E E
a) O2analyzer b) stethoscope

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page23
STANDARDX.NEONATALEQUIPMENT I II III IVi) intravenousinfusionpumpswithappropriatedruglibraries j) radiantheatedbedindeliveryroomandavailableintheneonatal
units
k) oxygenhoodwithhumidity l) pediatricbagandmaskscapableofdeliveringacontrolled
concentrationofoxygentotheinfant
m) orotrachealtubes n) aspirationequipment o) laryngoscope p) umbilicalvesselcathetersandinsertiontray q) cardiacmonitor r) pulseoximeter
STANDARDXI.NEONATALMEDICATION I II III IV11.1Thefollowingmedicationsshallbeimmediatelyavailabletotheneonatal
units:
a)antibiotics,anticonvulsants,andemergencycardiovasculardrugs E E E E
b)surfactant,prostaglandinE1 O O E E
11.2Emergencymedications,aslistedintheNeonatalResuscitationProgramoftheAmericanAcademyofPediatrics/AmericanHeartAssociation(AAP/AHA),shallbeimmediatelyavailableinthedeliveryareaandneonatalunits
E E E E
JOINTSTANDARDSAPPLYUNIVERSALLY

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page24
STANDARDXII.LABORATORY12.1Theprogrammaticleadersoftheperinatalserviceinconjunctionwiththehospitallaboratoryleaderswillagreeon
processingandreportingtimestoensurethattheseareappropriateforsamplesdrawnfromobstetricandneonatalpatientswithspecificconsiderationfortheacuityofthepatientandtheintegrityofthesamples.
12.2Thehospitallaboratoryshalldemonstratethecapabilitytoimmediatelyreceiveprocessandreporturgent/emergentobstetricandneonatallaboratoryrequests.
12.3Thehospitallaboratoryshallhaveaprocessinplacetoreportcriticalresultstotheobstetricandneonatalservices.12.4ThehospitalshallhaveavailabletheequipmentandtrainedpersonneltoperformaPulseOximetryassessmentandnewbornhearingscreeningpriortodischargeonallinfantsbornatortransferredtotheinstitutionasrequiredbytheStateofIndianaUniversalNewbornHearingScreening,Diagnosis,andInterventionGuidelines.(410IAC3)
12.5Thehospitalshallhavemolecular,cytogenic,andbiochemicalgenetictestingavailableorwrittenpolicyforconsultationandreferralinplace.
12.6AllhospitalsperformingpointofcarelaboratorytestingwillfollowtherulesestablishedbyCLIAandIndianaAdministrativeCode.
STANDARDXIII.EDUCATION13.1Thehospitalshallhaveidentifiedminimumcompetenciesforobstetricalclinicalstaff,nototherwisecredentialed,thatare
assessedpriortoindependentpracticeandonaregularbasisthereafter.13.2Thehospitalshallprovidecontinuingeducationprogramsforphysicians,nurses,andancillarymembersoftheperinatal
teamconcerningthetreatmentandcareofobstetricalandneonatalpatients. Conductteamtraininginperinatalareastoteachstafftoworktogetherandcommunicateeffectively Providelactationandbreastfeedingeducationforallmembersoftheperinatalteam. Forhighriskeventssuchasshoulderdystocia,emergencycesareandelivery,maternalhemorrhageandneonatal
resuscitation,conductclinicaldrillstohelpstaffprepareforhighrisk,highcomplexityeventswithlowrateofoccurrence
Conductdrilldebriefingstoevaluateteamperformanceandidentifyareasforimprovementforhighriskevents Educatenurses,residents,nursemidwivesanddeliveringphysicianstousestandardizedterminologyto
communicateallcategoriesoffetalheartratemonitortracings. Identifyspecifictriggersforrespondingtochangesinthemother’s,fetus’sornewborn’svitalsignsandclinical

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page25
STANDARDXIII.EDUCATIONconditionanddevelopanduseprotocolsanddrillsforrespondingtochangessuchaspreeclampsia,hemorrhage,orneonatalshock.
13.3.Ahospitalthatacceptsmaternaland/orneonatalprimarytransportsshallprovidethefollowingtothereferringhospital/providers:a) Guidanceonindicationsforconsultationandreferralofpatientsathighrisk.b) Informationaboutalternativesourcesforspecializedcarenotprovidedbytheacceptinghospital.c) Guidanceonthepre‐transportstabilizationofpatients.d) Feedbackonthepre‐transportcareofpatients.e) Clearcommunicationbetweensendingandreceivingpersonnel.f) Oncethepatienthasreachedthereceivinghospital,informationregardingthepatient’scondition,andcaregiven
duringtransportshouldbesentbacktothereferringproviderandreferringhospitalstaff.g) Regularlyscheduledconferenceswithreferralandreceivinghospitalsthatmayincludethefollowingtopics:
Reviewofmajorperinatalconditions,theirmedicalandnursingmanagement. Reviewoffetalmonitoring,includingmaternal‐fetaloutcomes,towardagoalofstandardizingnomenclatureand
patientcare. Reviewofperinataloutcomesandcomplications. Reviewofpatientandreferringprovidersatisfactiondata,complaintsandcompliments.
h) Perinataloutreacheducationprovidedjointlybyneonatalandobstetricphysicians,nurses,APN’s,PA’sandotherperinatalstaff.Responsibilitieswouldinclude: Assessreferralhospitaleducationalneeds. Plancurricula. Teach,implementandevaluateprograms. Analyzeanduseperinataldata. Providepatientfollow‐uptoreferringcommunitypersonnel. Maintaininformativeworkingrelationshipswithcommunitypersonnelandoutreachteammembers.
13.4ThePerinatalteammember:
Acquiresknowledgeandexperiencesthatreflectcurrentevidencedbasedpracticeinordertomaintainskillsandcompetenceappropriateforhisorherspecialtyarea,role,andpracticesetting.
Participatesinandmaintainsprofessionalrecordsofeducationalactivitiesrequiredtoprovideevidenceofcompetency.

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page26
STANDARDXIII.EDUCATION Maintainslicensureandcertificationasmandatedbystatelicensingboards,healthcarefacilitiesandaccrediting
agencies. Maintainscertificationwithinthespecialtyareaofpracticeasappropriate,asamechanismtodemonstrate
specialknowledge. Participatesinlifelonglearning,includingeducationalactivitiesrelatedtoevidencebasedpractice,knowledge
acquisition,safetyandprofessionalissues. Hasknowledgeofrelevantpracticeparametersandguidelinesofotherorganizationsthatfocusonthedeliveryof
healthcareservicestowomenandnewborns.13.5Thehospitalshallhaveawrittenplanforassuringregisterednurse/patientratiosaspercurrentGuidelinesForPerinatal
Care,orAssociationofWomen’sHealth,Obstetric,andNeonatalNurses(AWHONN)nursepatientratios.
STANDARDXIV.PERFORMANCEIMPROVEMENT14.1Thehospitalshallhaveamultidisciplinarycontinuousqualityimprovementprogramforimprovingmaternaland
neonatalhealthoutcomesthathasinitiativestopromotepatientsafetyincludingsafemedicationpractices,UniversalProtocoltopreventproceduralerrors,andeducationalprogramstoimprovecommunicationandteamwork.
14.2Thehospitalstaffshallconductinternalperinatalcasereviewsthatincludeallmaternal,intrapartumfetalandneonataldeaths,andallmaternalneonataltransports.
14.3Thehospitalshallutilizeamultidisciplinaryforumtoconductperiodicperformancereviewsofperinatalprogram.Thisreviewshallincludeareviewoftrends,alldeaths,alltransfers,allverylowbirthweightinfants,problemidentificationandsolution,issuesidentifiedfromthequalitymanagementprocess,andsystemsissues.
STANDARDXV.POLICIESANDPROTOCOLS15.1Thehospitalshallhavewrittenpoliciesandprotocolsfortheinitialstabilizationandcontinuingcareofallobstetricaland
neonatalpatientsappropriatetothelevelofcarerenderedatitsfacility.15.2Thehospitalshallhaveobstetricalandneonatalresuscitationprotocols.15.3Thehospitalmedicalstaffcredentialingprocessshallincludedocumentationofcompetencytoperformobstetricaland
neonatalinvasiveproceduresappropriatetoitsdesignatedlevelofcare.15.4Thehospitalshallhaveawrittenplanforacceptingortransferringmothersorneonatesas“backtransports”forongoing
convalescentcare,includingcriteriaforacceptingthepatientandnecessarypatientinformation.
RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page27
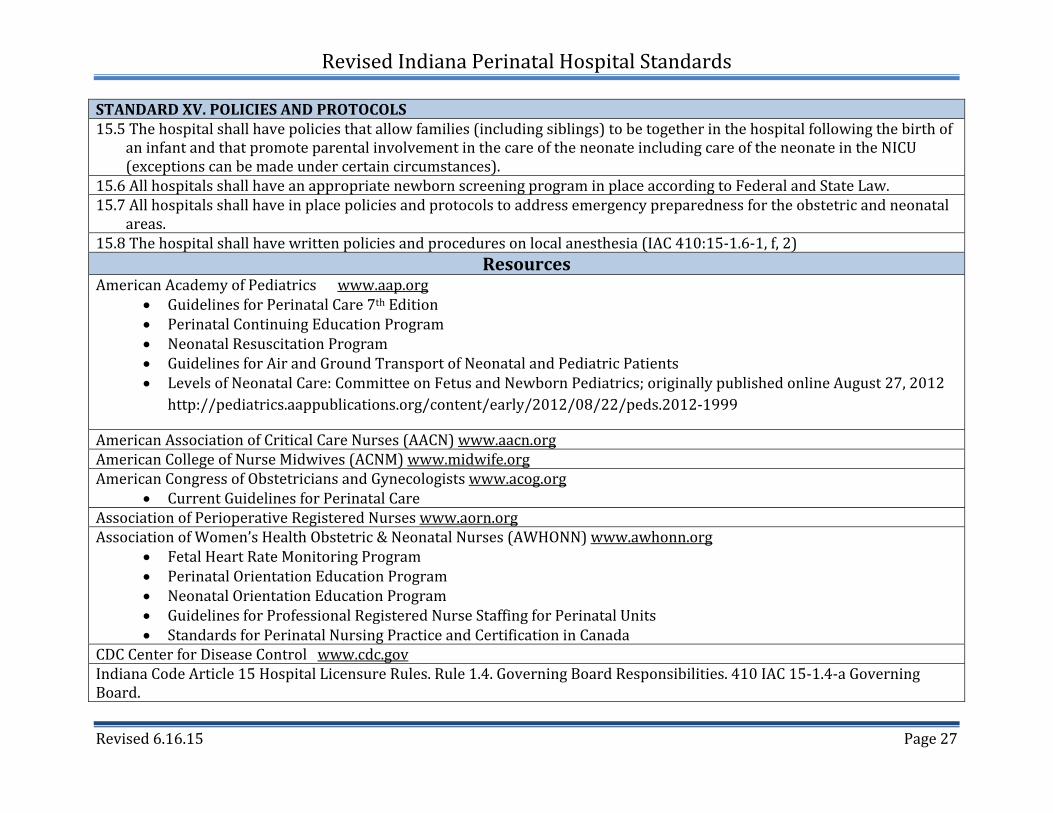
STANDARDXV.POLICIESANDPROTOCOLS15.5Thehospitalshallhavepoliciesthatallowfamilies(includingsiblings)tobetogetherinthehospitalfollowingthebirthof
aninfantandthatpromoteparentalinvolvementinthecareoftheneonateincludingcareoftheneonateintheNICU(exceptionscanbemadeundercertaincircumstances).
15.6AllhospitalsshallhaveanappropriatenewbornscreeningprograminplaceaccordingtoFederalandStateLaw.15.7Allhospitalsshallhaveinplacepoliciesandprotocolstoaddressemergencypreparednessfortheobstetricandneonatal
areas.15.8Thehospitalshallhavewrittenpoliciesandproceduresonlocalanesthesia(IAC410:15‐1.6‐1,f,2)
ResourcesAmericanAcademyofPediatricswww.aap.org
GuidelinesforPerinatalCare7thEdition PerinatalContinuingEducationProgram NeonatalResuscitationProgram GuidelinesforAirandGroundTransportofNeonatalandPediatricPatients LevelsofNeonatalCare:CommitteeonFetusandNewbornPediatrics;originallypublishedonlineAugust27,2012
http://pediatrics.aappublications.org/content/early/2012/08/22/peds.2012‐1999
AmericanAssociationofCriticalCareNurses(AACN)www.aacn.orgAmericanCollegeofNurseMidwives(ACNM)www.midwife.orgAmericanCongressofObstetriciansandGynecologistswww.acog.org
CurrentGuidelinesforPerinatalCareAssociationofPerioperativeRegisteredNurseswww.aorn.orgAssociationofWomen’sHealthObstetric&NeonatalNurses(AWHONN)www.awhonn.org
FetalHeartRateMonitoringProgram PerinatalOrientationEducationProgram NeonatalOrientationEducationProgram GuidelinesforProfessionalRegisteredNurseStaffingforPerinatalUnits StandardsforPerinatalNursingPracticeandCertificationinCanada
CDCCenterforDiseaseControlwww.cdc.govIndianaCodeArticle15HospitalLicensureRules.Rule1.4.GoverningBoardResponsibilities.410IAC15‐1.4‐aGoverningBoard.

RevisedIndianaPerinatalHospitalStandards
Revised6.16.15 Page28
STANDARDXV.POLICIESANDPROTOCOLSIndianaMothersMilkBankwww.immilkbank.orgIndianaPerinatalNetwork(IPN)www.indianaperinatal.orgIndianaStateDepartmentofHealth(ISDH)www.in.gov/isdhInternationalLactationConsultantsAssociation(ILCA)www.ilca.orgHealthstreamwww.healthstream.comMarchofDimeswww.marchofdimes.comNationalAssociationofNeonatalNurses(NANN)www.nann.orgNICHDEuniceKennedyShriverNationalInstituteofChildHealthandHumanDevelopmentwww.nih.gov/about/almanac/organization/nichd.htmOccupationalHealthandSafetyAdministration(OSHA)www.osha.govPeri‐factsUniversityofRochesterwww.urmc.rochester.edu/ob‐gyn/education/peri‐factsSugar&SafeCare,Temperature,Airway,BloodPressure,LabWork,EmotionalSupport(S.T.A.B.L.E.)Programwww.stableprogram.orgTheJointCommissionwww.jointcommission.org


















