
Paediatric Congenital Cardiac Services in England Service Standards

Review of Paediatric Cardiac Services in Scotland
National Services Division A Division of National Services Scotland
2006/2007

Review of Paediatric Cardiac Services in Scotland
Index Executive Summary 1 Introduction
1.1 Background to the review 1.2 Aim 1.3 Remit 1.4 Methodology
2. Literature review: Best Practice 2.1 Introduction 2.2 Paediatric cardiac surgery
2.2.1 Mortality rates in cardiac surgery for children 2.2.2 Hypoplastic left heart syndrome
2.3 Interventional cardiology 2.3.1 Procedures 2.3.2 Neonatal cardiology 2.3.3 Non-invasive imaging techniques 2.3.4 Mortality rates in interventional cardiology for children
2.4 Extracorporeal life support 2.5 Developmental progress 2.5.1 Development progress in children with congenital heart disease 2.5.2 Risk factors 2.6 Paediatric intensive care services 2.7 Paediatric heart transplantation 2.8 Paediatric heart-lung transplantation 2.9 Summary and Conclusions
3. Literature Review: Epidemiology 3.1 Definition 3.2 Risk factors 3.3 Classification of congenital heart defects
3.3.1 Acyanotic heart defects 3.3.2 Cyanotic heart defects
3.4 Incidence 3.4.1 Worldwide 3.4.2 Incidence in Scotland
3.5 Effect of termination on incidence at birth 3.6 Summary and Conclusions
4. Current Service for Residents of Scotland 4.1 Organisation of Scottish services
4.1.1 Nature of service level agreement 4.1.2 Cardiac surgery 4.1.3 Interventional cardiology 4.1.4 Neonatal cardiology
4.2 Activity 4.2.1 Paediatric Cardiac Surgery 4.2.2 Paediatric Interventional cardiology 4.3 Trends in age distribution and complexity 4.3.1 Activity trends and complexity 4.3.2 Neonates 4.3.3 Infants 4.4 Hypoplastic left heart syndrome 4.5 Summary and Conclusions – Assessed Needs
- 2 -

Review of Paediatric Cardiac Services in Scotland
5. Current issues 5.1 Overview 5.2 Hypoplastic left heart syndrome 5.3 Capacity 5.4 Northern Ireland activity
6. Quality & outcomes
6.1 Clinical outcomes 6.2 UK services and standards 6.3 Waiting times
7. Finance
7.1 Service funding methodology 7.2 Service funding since 1999 review 7.3 Future service funding
8. Fit against NSAG Criteria 9. Conclusions 10. Recommendations
- 3 -

Review of Paediatric Cardiac Services in Scotland
Executive summary
1. National Services Division (NSD) of National Services Scotland commissions designated national
specialist services and some national screening programmes at an all Scotland level. One of the required
outcomes of the 1999 Review of Paediatric Cardiac Surgery (PCS) was that NSD would assess the impact
on the service of the centralisation of paediatric cardiac surgery services for Scotland in Glasgow around 5
years after implementation. Both the Scottish Executive Health Department (SEHD) and National Services
Advisory Group (NSAG) have supported a minor NSD service review of PCS in 2006/2007.
2. As a “minor” service review the review took the form of a strategic stocktake to assess the extent to which
the service meets the needs of the children of Scotland, and is clinically and cost effective. The conclusions
and recommendations are set out below.
3. The annual need for interventional paediatric cardiology for residents of Scotland over the next 5-10
years is projected to be:
- 290 paediatric cardiac surgical procedures a year (including hypoplastic left heart surgery)
- 240 paediatric interventional cardiological procedures a year
- 65 neonatal cardiology episodes a year.
4. Current activity is consistent with assessed need although there remain a number of children on the
waiting list who have waited longer that the target waiting time of 16 weeks. All urgent cases receive surgery
or interventional cardiology without delay. No children assessed and ready for treatment are currently
waiting longer than 18 weeks (true waiting list). NSD is working with NHS GG&C to reduce waiting times for
all patients to within the target of 16 weeks by end December 2007, including those with ASC codes.
5. Mortality rates are consistently low and comparable with the best in the UK.
6. Surgery for hypoplastic left heart syndrome should be provided in Scotland from April 2008 as an integral
part of the service in Scotland.
7. Expenditure on the service in 2006/07 was £8.8 million. There has been considerable investment in the
service out of NSD’s general uplift over recent years in the light of new techniques, technologies, drugs, pay
increases and service pressures. (No additional top sliced funds were sought). Funding for current service
pressures and temporary additional funding to achieve waiting times targets, additional junior doctor cover,
and succession planning for consultant surgical staff have been found within NSD’s general uplift. The
service remains cost effective at average unit costs of £16,000.
8. The service continues to meet the criteria for designation.
- 4 -

Review of Paediatric Cardiac Services in Scotland
1. Introduction
1.1 Background to the review
Paediatric cardiac services in Scotland were reviewed by National Services Division (NSD) in 1999, when the
service was delivered from two sites (The Royal Hospital for Sick Children (RHSC) in Yorkhill, Glasgow and
RHSC, Edinburgh). The review arose mainly from the concern of clinicians providing the service about the
continuing viability of the two centres, and followed on from the Acute Services Review (Carter, 1997) which
identified a need for the centralisation of the service on one site in Scotland.
The remit of the 1999 review was stated as:
To assess whether any change was needed in the [then] current pattern of services in light of [then]
recent trends in care.
To consider the options for change.
To make recommendations on the future pattern of service delivery for paediatric cardiac surgery and
adult congenital heart surgery in Scotland.
One of the major conclusions of that review was that the surgical caseload should be centred on one site in
Scotland rather than the previous two sites. This led to the decision to concentrate cardiac surgery and
interventional cardiology for children in Glasgow from 2000/01. From April 2004, the service was extended to
provide also neonatal cardiology to provide specialist diagnostic tests (including some antenatally) and stabilise
infants prior to surgery.
1.2 Aim
The aim of the review was to assess the extent to which the current service reflected published best practice,
and continued to meet the needs of the children of Scotland clinically and cost effectively.The review draws from
current literature to seek to predict future trends in clinical care, and consideration is given to how the service
might adapt to support these changes. In conclusion, the review examines whether the service continues to fit
the criteria for national designation.
1.3 Remit
To review current provision of paediatric cardiac services for residents of Scotland in light of developments
in clinical care, quality standards and waiting time targets; and make recommendations to the National
Services Advisory Group (NSAG) on the future provision of services required to meet the needs of the
residents of Scotland for high quality, sustainable and cost effective care.
- 5 -

Review of Paediatric Cardiac Services in Scotland
1.4 Methodology
The review followed NSD's standard procedural guidelines for the conduct of a minor review and as such
was conducted internally, with input and participation from the service providers. The public health
consultant of NSD was designated to lead the review with the support of the multidisciplinary team of the
Division. A project manager, a project support officer and a commissioning manager from within the Division
undertook the bulk of the work and were responsible for the operational management of the review.
Data relating to the number of patients referred to and operated on were collected along with details of case
mix and trends in age and the severity of conditions. To enhance this data, meetings were held at Yorkhill
Hospital with the surgeons, cardiologists, intensivists, nursing staff and the general and finance managers
involved with paediatric cardiac services.
The final report has been prepared for consideration by NSAG in May 2007.
- 6 -

Review of Paediatric Cardiac Services in Scotland
2. Literature review: Best Practice
2.1 Introduction
Congenital heart defects are structural or functional anomalies in the heart that occur during fetal
development and are present at birth. Congenital heart disease is the most common congenital structural
malformation. The survival of children born with congenital heart disease has improved dramatically over
the past thirty years, improvements in diagnosis, medical and surgical management as well as anaesthetic
care have improved survival rates from 20% to 80% today (Knowles et al, 2005). This has led to a rapidly
increasing prevalence of congenital heart disease among adults; the British Cardiac Working Party on
grown up congenital heart disease (GUCH) estimated that in 2000 there were just fewer than 150,000
adults with GUCH in the UK. Of these, 11,500 had the most complex GUCH requiring lifelong supervision.
By 2010, it was estimated that over 185,000 adults in the UK would be living with GUCH with over 17,000
having the most complex form of the disease (Petersen et al, 2003).
2.2 Paediatric cardiac surgery Children with congenital heart disease may undergo either closed or open heart surgery. In a closed operation,
the heart and main blood vessels can be operated on while the heart is still beating. In open procedures, the
heart is opened and the blood flow to the child’s vital organs is supported by a heart-lung bypass machine.
Types of closed heart surgery include patent ductus arteriosus, coarcation of the aorta and Blalock-Taussig
Shunt (palliative procedure). Types of open heart procedure are listed in the table.
Types of open heart surgery Septal defects
Atrial septal defects (ASD)
Ventricular septal defects (VSD)
Atrioventricular septal defect (AVSD)
Defect causing obstruction to blood flow
Pulmonary stenosis
Aortic stenosis
Tetralogy of Fallot
Defects involving the great arteries
Transposition of the great arteries (arterial switch)
- 7 -
Review of Paediatric Cardiac Services in Scotland
Others
Hypoplastic left heart surgery
Aortic valve replacement
An observable trend is the rising proportion of younger children presenting for surgery. Surgical techniques
for repair of CHD continue to evolve and this is particularly evident in the treatment of hypoplastic left heart
syndrome (Van Doom, 2006). Advances in intensive care will be considered later.
2.2.1 Mortality rates for cardiac surgery in children
The Central Cardiac Audit Database (CCAD) was set up in 1996 to coordinate data collection activities.
Since the Bristol Inquiry, all paediatric cardiac centres in England, Scotland and Northern Ireland participate
in the paediatric cardiac surgery and congenital heart disease audit. Data has been collected from all 13 UK
tertiary congenital cardiac centres since April 2000. For the first five years, outcome analysis for surgical
and cardiac intervention treatment has been restricted to peri-operative (within 30 days of the procedure)
and one year survival. It is anticipated that data on long term survival and neurological outcome may be
available in the future.
Outcomes in the Scottish centre and other UK centres will be discussed in detail in section 6. In summary,
however, an analysis of national UK data of survival of children under 1 year after cardiac surgery between
April 1996 and March 2002 demonstrated that mortality in all UK centres fell from 12% to 4% (Aylin et al).
The reduction did not seem to be due to fewer high risk procedures. Improved quality of care may account
for the drop in mortality through new technologies or improved peri-operative and post-operative care (Aylin
et al).
2.2.2 Hypoplastic left heart syndrome
Hypoplastic left heart syndrome (HLHS) is a combination of congenital cardiac anomalies involving
hypoplasia of the ascending aorta, aortic valve atresia or stenosis, a small or absent left ventricle, and mitral
atresia or stenosis (Connor, 2004). The incidence of HLHS is 1 in 4000 to 6000 live births (Fyler, 1980).
However, the incidence may be higher that reported because some infants may die prior to diagnosis. Over
50% of known cases of HLHS are diagnosed prenatally in the UK. This allows considered decision making
prior to birth. However there is a lack of evidence that this early diagnosis confers a survival advantage
(Sullivan, 2002).
In utero, the fetus receives oxygen from the maternal blood. At birth, the baby may appear normal. This is
because the ductus arteriosus, which connects the pulmonary artery to the aorta, is still patent and
‘bypasses’ the defect. However, a few days after birth the ductus begins to close and the neonate may
suddenly present with cynaosis, breathlessness and shock. Once the diagnosis has been made, it is
- 8 -

Review of Paediatric Cardiac Services in Scotland
imperative to treat with prostaglandin to maintain ductal patency (Claxon-McKinney, 2001). Surgical
treatment is a staged procedure, detailed below.
Stage 1 - Norwood procedure
This is carried out during the first week of life. The aim is to establish blood flow from the right ventricle to
the aorta and to regulate pulmonary blood flow. The operation may be carried out using a modified Blalock-
Taussig shunt (with mortality rates ranging from 10-40%), or a recent technical modification which utilises a
right ventricle - pulmonary artery conduit. A randomised controlled trial is currently comparing these two
techniques (Slavik, 2006).
Stage 2 - Glenn procedure
This procedure is normally carried out at 5-6 months of age and carries a lower mortality risk that the
Norwood proecedure. Interstage mortality (death occurring between hospital discharge from first procedure
and admission for second procedure) ranges from 10-25%. Thielen (2005), however, reported that with daily
monitoring, this could be reduced from 16% to 0%.
Stage 3 - Fontan procedure
Usually carried out between 3 and 5 years of age.
Neurological complications have been reported for HLHS not only as a result of the surgery but also during
the pre- and post-operative period (Connor, 2004). The management of these children is extremely
challenging for surgeons, obstetricians, anaesthetists, intensivists and nursing staff alike.
Pre-operatively, the aim of management is to optimise systemic oxygen delivery and organ perfusion. This
will optimise the condition of the child prior to stage 1 surgery. Post-operatively, the child will have been
subjected to a long period of cardiopulmonary bypass and aortic cross clamping, with deep hypothermia
and in many cases, a period of circulatory arrest. These neonates therefore require intensive monitoring
with early action on any disturbance to their systemic oxygen delivery (Theillen, 2005).
Neonatal treatment for HLHS was examined by Connor (2004) who analysed hospital discharge records for
550 neonates (≤ 30 days) who were born with HLHS. The study found that 234 underwent the Norwood
procedure, 17 had heart transplants and 106 died in hospital with no surgical intervention. Those who died
were significantly more likely to have received care in hospitals identified as 'small' (less than 300 beds) or
'not a children's hospital). The mortality rate for the Norwood procedure was 32%, and for transplantation,
41%. Other centres are now quoting mortality rates of 20% (Theilen, 2005).
2.3 Interventional cardiology
Paediatric interventional cardiology is an expanding specialty with a range of mature, emerging and
investigative procedures and technologies. These procedures are performed most often for palliative or
definitive treatment purposes. Interventional catheterisation has largely replaced surgery as the standard
- 9 -

Review of Paediatric Cardiac Services in Scotland
treatment for pulmonary valve stenosis, initial treatment of aortic stenosis, treatment of pulmonary branch
stenosis, coarctation of the aorta, patent ductus arteriosus (after the neonatal period) and secundum atrial
septal defects. Technologies for percutaneous ventricular septal defects closure and percutaneous valve
replacement are under intense scrutiny and will enter mainstream practice soon. Additional technologies
are being assessed for use in single ventricle disease and the application of interventional treatments to the
foetus is being investigated. (Schneider et al, 2004). In addition, other groups have already established
cather-based procedures for the creation of Fontan communications and others have performed non
surgical pulmonary artery banding. The trend toward cather-mediated interventions looks set to continue
and some authors believe that surgical interventions will decline (Levi et al, 2003).
Haemodynamics and the anatomy of congenital heart disease are assessed by echocardiography alone in the
majority of patients. Consequently diagnostic catherterisations are primarily done to measure precise gradients
or visualize distal or convoluted structures (Rhodes, 2003).
2.3.1 Procedures These can be broadly divided into four categories comprising opening procedures, closing procedures, retrieval
procedures and electrophysiological procedures (Andrews et al, 2004).
Opening procedures Balloon dilation The commonest indications for balloon dilations are aortic and pulmonary vein stenosis. Complications
include regurgitation, balloon rupture with consequent removal difficulties and air embolus. The procedure is
generally safe and effective. Another indication includes atrial septostomy on Cyanotic CHD. This is a small
risk of cardiac rupture and surgery should be available on site.
Stenting An increasing range of stents are available. However they are normally reserved for older children due to the
limited potential for expansion and difficulties in removal. The three main indications include stenting branch
pulmonary arteries, stenting of coarctation and aterial duct stenting.
Radiofrequency perforation This is performed for pulmonary atresia. Closing procedures Patent Ductus Arteriosus (PDA) For those children who are over one year old, closure of PDA can be achieved by using coil devices. The choice
of device is influenced by the size and shape of the defect. This is usually a straightforward procedure.
- 10 -

Review of Paediatric Cardiac Services in Scotland
Atrial Septal Defect (ASD) Many secundum ASD are suitable for device closure. However, very large defects or primum defects may
require surgical closure.
Ventricular Septal Defect (VSD) This is a relatively recent advance. The vast majority of large defects or those requiring closure in infancy are
closed surgically. However there is debate about whether moderate defects could be closed using a device in
the catheter lab. The risks are higher than ASD due to the higher pressures in the ventricle. These may include
embolisation or complete heart block.
Closure of fenestrations A fenestration is created in children with a single ventricle to relieve pressure on the systemic circuit. In the
longer term this can lead to a right to left shunt. This can be closed by devices used in ASD management.
Embolisation of collaterals can also employ devices for closure. Retrieval procedures These may include baskets, snares and forceps to retrieve embolised line fragments
Electrophysiological procedures Radiofrequency ablation is used to manage tachyarrhythmias in middle to late childhood and may lead to a
complete cure. In the study by Tanel et al (1997) the overall final success rate for all diagnoses was 90%
and the incidence of serious complications was 1.2% (1 late death, 1 ventricular dysfunction, 1 complete
heart block, 1 cardiac perforation, and 1 cerebrovascular accident).
2.3.2 Neonatal cardiology. Since the cardiac service for children was centralised in Glasgow there has been a significant increase in
referrals of neonates, and pregnant women whose unborn babies have been found to have a possible
cardiac anomaly, for specialist cardiology assessment and for investigation and stabilization prior to cardiac
surgery. Depending on gestational age, many neonates require intensive ventilatory support for several
days during the assessment period at the end of which a decision may be made to proceed to surgery. In
some cases surgery may not be deemed appropriate.
2.3.3 Non-invasive imaging techniques The development of non-invasive techniques over the past 20 years has changed the way that cardiologists
investigate children prior to surgery. Techniques including echocardiography with Doppler, isotope imaging
studies and MRI have reduced the need for invasive investigations prior to surgery. Cardiac ultrasound
machines are becoming increasingly sophisticated. This may allow bedside diagnosis and avoid the need to
sedate infants (Richens, 2006). Continuing developments in medical technology and research are
- 11 -

Review of Paediatric Cardiac Services in Scotland
constantly expanding the range of imaging tests and diagnostic measures available. There is therefore a
need for clinicians to collaborate to determine the most appropriate choice of investigations. A consensus
statement (Fraser et al, 2006) recommends that experts in different modalities should collaborate and that
joint clinical services and diagnostic pathways should be developed for this patient group.
2.3.4 Mortality rates for paediatric interventional cardiology
Outcomes in the Scottish centre and other UK centres will be discussed in detail in section 6. In summary,
however, an analysis of national UK data of survival after therapeutic catheterisation procedures for
congenital heart disease in 1828 cases showed survival at 30 days was 99.1%, falling to 98.1% at one year
(Gibbs et al, 2004). In a 2005 study (Agnoletti et al) analysed 1022 interventional procedures performed
over eight years (excluding 260 procedures for atrial septostomy) to determine the risk factors for
complications and death. The findings indicated the incidence of complications was 4.1% with 0.4%
mortality (n=4) Identified predictors of risk included the level of technical challenge, the clinical condition of
the child, the level of training of the operator, operator error and breakdown of equipment
2.4 Extracorporeal life support (ECLS) in congenital heart disease (formerly known as Extracorporeal membrane oxygenation (ECMO))
ECLS is provided as a means of temporary life support to patients with cardiac or pulmonary failure. The
service at Yorkhill Hospital is nationally funded and is one of only four in the UK. The service provides a key
role in supporting the national cardiac service.
Cardiac patients make up 13% of total ECLS patients with an overall survival of 41% (Conrad et al, 1998).
As described by Salzer-Muhar et al (1999) the main considerations for the cardiologist in the context of
ECLS include:
screening for congenital heart disease prior to ECLS in newborn with respiratory symptoms
appraisal of surgical repair with special emphasis on detection of unknown residual defects
assessment of haemodynamics during post-operative ECLS
detection of complications during ECLS
consensus regarding initiation of ECLS. This includes pre-operative discussion with cardiac surgeons,
anaesthetists and intensive care specialists concerning the issues of post operative ECLS
outcome and rehabilitation after ECLS.
Chaturvedi et al (2004) examined factors which affect outcome for children supported by ECLS after
paediatric open heart surgery. Factors which may enhance survival include the identification of hearts with
reversible ventricular dysfunction, initiation for reactive pulmonary hypertension and cannulation in the
operating room rather than intensive care. This may be due to early effective support preventing prolonged
hypoperfusion and the avoidance of catastrophic cardiac arrest. Adverse survival factors included serious
- 12 -

Review of Paediatric Cardiac Services in Scotland
mechanical ECMO circuit problems, renal support, residual lesions and inability to wean off ECLS.
2.5 Developmental progress
There has been a significant decline in both mortality and severe morbidity in children who have had
surgery for congenital heart defects; and research has focused on the developmental progress of this cohort
of children. Additional research has looked at the factors which may predict or influence development.
2.5.1 Developmental progress in children with congenital heart disease
Studies have identified a number of developmental issues in children who have undergone surgical
correction of a heart defect. These include lower mean IQs, mild language delays and motor difficulties.
Other neurological sequelae include muscle tone changes, behavioural difficulties and cranial nerve
changes (Limperopoulos et al, 2002). Limperopoulos et al studied the prevalence of functional limitations
and burden of care of young children with congenital heart defects. 138 infants who were assessed pre and
post operatively, and again at 12 to 18 months after surgery. The results showed that only 21% were
functioning within their expected age range. Moderate disability was noted in 37% with severe disability in
6% (Limperopoulos et al, 2001). Medical risk factors, socioeconomic factors and parental stress can all
contribute to these observations. This research suggests that although severe impairments are rare, mild to
moderate impairments are highly prevalent. Further research is required into the longer term outcomes in
later school and adulthood - as mortality rates drop, there is an increasing need to consider these factors
which may affect the developmental potential of the child in later life.
2.5.2 Risk factors
Causes contributing to neurological development sequelae are multifactorial and involve a complex
interaction of preoperative, perioperative and postoperative events. Preoperative factors may include
chronic hypoxia, acidosis, poor nutrition and inadequate cerebral perfusion. Intraoperative procedures such
as cardiopulmonary bypass and deep hypothermic arrest have also been associated with poorer outcomes,
caused by cerebral side-effects due to micro-embolism during bypass. Postoperative factors may include
cardiac arrest or infections (Majnemer et al, 1999) A shorter duration of core cooling time before deep
hypothermic circulatory arrest (specifically less than 20 minutes) has also been associated with higher
developmental scores. In addition, longer exposure to deep hypothermia (>50-60 minutes), particularly
during neonatal surgery, has been linked to greater morbidity rates (Limperopoulos et al, 2002).
Daliento et al, 2006 suggest that unnecessary disruption of the attachement between mother and child
during hospitalisation may have a negative impact on health and that the period of separation between child
and parents should be limited to the duration of to the surgical event.
2.6 Paediatric cardiac intensive care services The management of children both pre and post operatively has great impact on the eventual outcome. Over
the past few decades the importance of paediatric cardiac intensive care (PCIC) has become apparent.
- 13 -

Review of Paediatric Cardiac Services in Scotland
Chang (2000) describes developments which may have an impact on PCIC in the coming years. These
include:
Emergence of new patient populations
The survival of children with previously lethal lesions has increased the case complexity. Recent research
on fetal cardiac surgery suggests that ongoing care for these patients after birth may be increasingly
required in the future.
New methods for the treatment of pulmonary hypertension in cardiac patients
Nitric oxide, used as a pulmonary vasodilator, has been useful in the post operative management of cardiac
patients, leading to a reduction in the utilisation of ECLS ( Chang, 2000) A number of other therapies aimed
at reducing pulmonary vascular resistance, such as dilutional and modified ultra-filtration to remove
circulating vasoconstrictor endothelin-1 (ibid) are also being investigated.
Other innovations
New techniques for mechanical ventilation may allow better post op management to optimise right heart
dynamics. Expanding research into single ventricle physiology and utilisation of gaseous agents may allow
better control of pulmonary vascular resistance in post op neonates (ibid).
Advances in the treatment of heart failure
Drug therapy has progressed to allow better management of heart failure as well as immuno-suppression
post transplant. Ventricular assisted devices as well as extracorporeal membrane oxygenation are also
being progressed.
Improved non-invasive imaging of critically ill paediatric cardiac patients
Transthoracic as well as transoesophageal echocardiography have allowed better pre- and post- procedure
assessment of patients' cardiac status, providing more clinical information on which to base treatment
decision and assess outcomes.
New techniques in paediatric cardiac surgery
The understanding of the impact of cardiopulmonary bypass on the brain of the child has led to a focus on
protective techniques. The use of robotics and biomaterial may enhance outcomes further in the future. A
Herma Heart Report (Herma Heart Centre 2005) describes, for example, the ability of a cerebral near-
infrared spectroscopy (CNIS) monitor to detect potential and occurring brain compromise before or during
its occurrence, alerting the operator to the need to intervene to prevent the potential long-term effects of
hypoxia.
Use of computer technology and intensive care monitoring
Continuous monitoring of relevant serum chemistry, e.g. serum lactate may allow the development of
‘medical intelligent’ systems with feedback loops to make decisions about adjusting electrolyte imbalances.
Telemedicine links to other hospitals is already part of mainstream practice. In the future links to patient’s
- 14 -

Review of Paediatric Cardiac Services in Scotland
homes and a global network of paediatric intensive care could allow the development of research,
guidelines and audit.
Cost
The high cost of this care should ensure that there is a focus on prognosis, severity of illness and outcome.
2.7 Paediatric heart transplantation Heart transplant is an established treatment option for infants and children with end-stage heart failure or
complex congenital cardiac defects. According to the International Society for Heart and Lung
Transplantation (ISHLT) Registry, over the last 20 years nearly 4000 infants and children have received a
heart transplant (Mendeloff, 2002). In the UK 159 paediatric heart transplants were carried out between 1
July 1995 and 31 December 2001 (Anyanwu et al, 2002).
One of the differences between cardiac transplantation in adults and children is in the indications for the
operation. In children less than 12 months of age, congenital defects account for about 75% of those listed,
with hypoplastic left heart syndrome being the most common defect. In the one to ten year age group
slightly over 50% have cardiomyopathy and approximately 37% have congenital heart disease and in
adolescents the main indication is cardiomyopathy at 64% with congenital disease accounting for 26%. In
2001 for paediatric patients overall cardiomyopathy accounted for 54% of registrations and congenital
disease for 40% (Colombani et al, 2003 and Kichuk-Chrisant, 2002).
Graft survival rates are slightly lower for patients under one year of age. There is an 86% survival at three
months compared to 88% in all other age groups. Overall paediatric patient survival at three months ranges
from 85% to 92 % and at five years a survival range from 63% to 74% (Colombani et al, 2003). These
survival rates are slightly better than for older patient groups and most likely are a result of the benefits of
younger donor grafts with less risk of coronary disease. Boucek et al (2001) explain the higher three-month
mortality in patients less than 12 months of age as most likely being a result of abnormally complex
anatomy and physiology and the fact that these infants may have to wait for a lengthy period of time in a
very poor condition.
2.8 Paediatric heart-lung transplantation Primary pulmonary hypertension (PPH) and pulmonary hypertension associated with Eisenmenger's
syndrome/congenital heart disease have been the main indications for heart-lung transplantation in adults.
Despite the widespread use of bilateral lung transplantation, CF remains the third most common diagnosis
among heart-lung recipients (Trulock et al 2003). The number of paediatric patients being registered for
heart-lung transplantation in the UK has remained fairly consistent over the last decade. In 2001, 25
patients were added to the waiting list but only six transplants were performed (Colombani et al, 2003).
- 15 -
Review of Paediatric Cardiac Services in Scotland
Congenital abnormalities of the heart and/or lung are the leading indication for heart-lung transplantation in
young children and cystic fibrosis is the leading cause in 11 to 17 year olds (Boucek et al 2001).
2.9 Summary and conclusions of literature review
Current practice in the Scottish service is consistent with published literature on best practice in both cardiac
surgery and interventional cardiology.
Outcomes in hypoplastic left heart syndrome have improved markedly internationally and techniques are now
established. Most international centres similar in size to the Scottish service provide this treatment option. This
would suggest that it is now time to consider developing the capacity to undertake this surgery in Scotland.
- 16 -

Review of Paediatric Cardiac Services in Scotland
3. Literature review: Epidemiology
3.1 Definition
Congenital heart disease, as defined by Mitchell et al (1971) is a gross structural abnormality of the heart or
intrathoracic great vessels that is of actual or potential functional significance. There are eight common
lesions, which account for 85% of all cases. They are:
ventricular septal defect (VSD)
patent ductus arteriosus(PDA)
atrial septal defect (ASD)
pulmonary valve stenosis
aortic valve stenosis
coarctation of the aorta
tetralogy of Fallot
transposition of great arteries.
The remaining 15% account for a variety of more rare and complex lesions. Congenital heart disease as a
whole occurs with an equal frequency in males and females but some lesions such as aortic stenosis,
coarctation of the aorta are more common in males, while patent ductus arteriosus and atrial septal defects
are more common in females
http://www.pediatriconcall.com/FORDOCTOR/DiseasesandCondition/congenital_heart.asp)
3.2 Risk factors
Only 8% of all congenital (i.e. present at birth) heart defects are known to be associated with single mutant
gene or chromosome abnormalities, the remaining 92% are thought to be due to various environmental
factors including diabetes, alcohol consumption, maternal progesterone use, certain viruses and other
teratogens (Woolfe et al, 1995). Although at present only a small proportion of cases currently have
identifiable gene markers, ongoing research into developmental biology, genetic and paediatric cardiology
is likely to provide more secure grounds for genetic counselling and intervention in future (Winlaw et al,
2005).
As children with congenital heart defects are now surviving to have children of their own, the incidence of
mothers with congenital defects having affected children is 2.5-18%, and the incidence of fathers with CHD
having affected children is 1.5-3.0%. (Perloff et al, 2001) Both figures are higher than for the general
population, often quoted as 0.8% or 8 per 1000 live births (Review of Paediatric Cardiac Surgery Services
in Scotland, NSD, 1999). Rarely, more than one child in the same family may have a congenital defect. The
reason the risk is relatively modest is that most congenital defects are a result of multiple gene defects
and/or interaction between multiple or single gene defects and fetal environment. (Winlaw et al, 2005).
- 17 -
Review of Paediatric Cardiac Services in Scotland
About 5% of patients with congenital defects have chromosomal abnormalities. These include Down’s
syndrome, Trisomy 18 and Turner’s syndrome. Genetic tests are available in only a few instance and most
causes are heterogeneous. In addition, different types of congenital defects can result from the same
chromosomal alteration or from mutations in the same gene. Further studies are required to predict the
clinical expression of specific mutations (Goldmutz et al, 2001). It has been estimated that up to 10-20% of
all children with congenital heart defects will require a heart transplant at some point in their lives
(Mendeloff, 2002).
3.3 Classification of congenital heart defects
Congenital heart defects can be broadly classified into acyanotic (75% of all defects) and cyanotic (25% of
all defects).
3.3.1 Acyanotic heart defects
An acyanotic heart defect is a group of structural congenital heart defects which can be subdivided into two
groups, depending on whether there is shunting of the blood from the left vasculature to the right (left to
right shunt) or no shunting at all.
Left to right shunting heart defects includes ventricular septal defect (VSD) which account for 30% of all
congenital heart defects, persistent ductus arteriosus (PDA), atrial septal defects (ASD) and atrioventricular
septal defects (AVSD).
Acyanotic defects without shunting include pulmonary stenosis, aortic stenosis and coarctation of the aorta.
3.3.2 Cyanotic heart defects
Cyanotic heart defect is a group-type of congenital heart defects. The patient appears blue (cyanotic) due to
deoxygenated blood bypassing the lungs and entering the systemic circulation. This can be caused by right-
to-left or bidirectional shunting, or malposition of the great arteries.
Defects in this group include:
transposition of the great vessels
Hypoplastic left heart syndrome (HLHS)
Pulmonary atresia (PA)
Tetralogy of Fallot (ToF) – 10% of CHD
Tricuspid atresia
Truncus arteriosus
- 18 -
Review of Paediatric Cardiac Services in Scotland
3.4 Incidence 3.4.1 Worldwide At approximately 8 per 1000 live births, congenital heart disease is the leading non-infectious cause of
death in neonates (Winlaw et all, 2005). However, as noted by Hoffman & Kaplan (2002), significant
variation exists in reported incidence between studies. They conclude that this is probably due to variations
in the ability to detect trivial lesions between centres in the studies – for example small VSD. The incidence
of severe cardiac lesions which require medical intervention is stable at 2.5-3 cases per 1000 live births
while the moderate forms of cardiac lesions account for another 3 per 1000 live births.
Minor forms of cardiac defects may not attract or require medical intervention however, one third of all
children born with congenital heart disease will need surgical or catheter based intervention during the first
year of life (Winlaw et al, 2005).
3.4.2 Incidence in Scotland
The reported incidence rates for Scotland have, in recent years, varied from 8.29 to 11.02 cases per 1000 live
births i.e. around 450-600 children a year. Table 1 (source ISD) illustrates the Scottish rates of detected
congenital anomalies for the ten year period 1995-2004. Taking termination rates into account (Table 2, ISD)
results in only a marginal change in incidence, ranging from 8.38 cases per 1000 live births in 1998 to 11.24 in
2004.
The number of live births in Scotland from 2001-2006 (GRO, 2007) were:
Year Live births
2000 53,076 2001 52,527 2002 51,270 2003 52,432 2004 53,957 2005 54,386 2006 55,690
3.5 Effect of termination on the incidence at birth
The 2003 Health Technology Assessment Report (NHS Quality Improvement Scotland, 2003)
recommended that each pregnant woman in Scotland should be offered an ultrasound scan in both the first
and second trimesters of pregnancy. However, this service is not universally available in Scotland at
present.
There is evidence of the efficacy of first trimester scans in detecting major congenital heart disease. Rasiah
et al (2006) carried out a systematic review of existing evidence and found that positive first trimester scans
- 19 -
Review of Paediatric Cardiac Services in Scotland
- 20 -
diagnosed major defects with high accuracy (specificity approaching 100%). When negative, first trimester
ultrasound scan diagnosed fetuses with a normal heart with reasonable accuracy (sensitivity around 85%).
However, many of the articles related to ultrasounds were carried out in specialised and experienced
centres.
Germanakisl et al (2006) looked at the factors which may influence the decision to terminate a pregnancy
and modelled the impact on a population. The most important factor was found to be the availability and
performance of antenatal sonography and this was found to be variable. In addition, the stage of pregnancy
and the severity of the defect were found to affect the decision to terminate the pregnancy. The authors
anticipated a 15% reduction in the most severe forms of congenital heart disease if fetal cardiac screening
was universally available.
The Scottish figures suggest little impact at present but if second trimester screening becomes widely
available this may lead to some impact on birth incidence, particularly of the most severe forms of the
disease.
3.6 Summary of conclusions on epidemiology literature review - Future trends
Although the number of adults with congenital heart disease is rising as more children receive better
treatment and survive to adulthood, there remains a degree of uncertainty as to the accurate measure of
incidence (Hoffman & Kaplan, 2002). The 1999 NSD review of the service settled on a figure of 8 per 1000
live births as a reasonable representative average during the 1990s and noted that the incidence of
congenital heart disease had remained fairly constant over time and across different populations. According
to the 2003 Report of the Paediatric and Congenital Cardiac Services Review Group (Department of Health
2003), no increase in the number of new cases of congenital heart disease was predicted. This was
supported by evidence from Scottish, Swedish and Dutch studies. However, ISD figures in table 1 show that
reported incidence in Scotland had increased to 11 per 1000 population in 2004 (593 children). A small
forecast increase in the birthrate over the next 10-15 years means that the overall incidence of congenital
heart disease is likely to continue to rise gradually.
In addition, advances in treatment such as those mentioned in this report are likely to mean that more
children are likely to be suitable for some form of surgery or interventional procedure. Other diagnostic/fetal
cardiology advances also mean that more conditions are detectable before birth, allowing for choice on
whether to proceed with a pregnancy and/or optimal planning for delivery and neonatal care.
Activity data from the Scottish centre seems to support the prediction of a steady but small rise in the overall
numbers.

Review of Paediatric Cardiac Services in Scotland
Table 1: Singletons born in Scotland & detected1 with congenital anomaliesa at birth or during infancy2 rates per 1,000 births by anomaly and year : 1995 - 2004
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Anomalies of the heart & circulatory system 8.59 9.04 8.82 8.29 9.59 10.35 9.96 8.39 10.27 11.02
Heart 5.19 5.27 5.33 4.35 4.42 5.28 5.38 4.75 5.83 6.37
Circulatory System 4.81 4.40 4.28 3.65 4.33 4.21 4.22 4.10 4.30 5.13
a see codes used for definition of congenital anomalies
1 Anomalies have been located from the diagnostic summaries contained within the linked source data comprising profiles of
neonatal and inpatient hospital discharge records, stillbirth notifications, Scottish birth record and death registrations
2 All Infants followed up from birth for period of one year to allow detection of anomalies from hospital inpatient records or
General Register Office death registrations
Table 2: Singletons born in Scotland & detected1 with congenital anomaliesa at birth, during infancy2,
or aborted3
because of pre-natal diagnosis rates per 1,000 births by anomaly and year : 1995 - 2004
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Anomalies of the heart & circulatory system 8.66 9.08 8.87 8.38 9.62 10.50 10.06 8.53 10.39 11.24
Heart 5.26 5.30 5.38 4.44 4.46 5.42 5.48 4.90 5.95 6.59
Circulatory System 4.81 4.40 4.28 3.65 4.33 4.23 4.22 4.10 4.30 5.13
a see codes used for definition of congenital anomalies
1 Anomalies have been located from the diagnostic summaries contained within the linked source data comprising profiles of
neonatal and inpatient hospital discharge records, stillbirth notifications, Scottish birth record and death registrations
2 All Infants followed up from birth for period of one year to allow detection of anomalies from hospital inpatient records or
General Register Office death registrations
3 Refers to therapeutic abortions notified in accordance with the Abortion Act 1967.
Figures from ISD, NSS Scotland
- 21 -
Review of Paediatric Cardiac Services in Scotland
4. Current Service for Residents of Scotland
4.1 Organisation of Scottish services Following the NSD review of paediatric cardiac surgery services in 1999, paediatric cardiac surgery and
interventional cardiology services were centralised on one site in Glasgow. Since then Yorkhill has been the
national designated centre for paediatric cardiac services in Scotland (see section 5 for further background
information and current service structure). Non-invasive cardiac investigation also takes place at the Sick
Children’s Hospital in Edinburgh which has cardiology inpatient beds, and provides outpatient clinics. A
network of cardiologists across Scotland provide care close to home supported by outreach clinics provided
from the two main centres in Edinburgh and Glasgow.
Consultants from Edinburgh and Glasgow meet weekly to discuss patients who may require surgical or
catheter intervention. Cardiologists from Edinburgh travel to Glasgow to undertake catheter procedures and
participate in on-call. Outreach clinics are provided by consultants from both units to patients throughout
Scotland. In addition, telemedicine facilities are available in some locations throughout Scotland. The
network enables two-way transmissions of live videos, still images and echocardiography. This enables
remote assessment of the child and can influence decisions to treat locally or transfer. There are now
seven paediatric cardiologists in Scotland (Richens, 2006).
4.1.1 Nature of service level agreement
The national cardiac surgery and interventional cardiology service is currently funded by way of a cost and
volume service agreement, under which the service providers receive a fixed monthly sum together with an
amount based on the actual activity achieved, up to a maximum indicative level of activity. The service
provides detailed activity information to NSD as specified in the agreement, and is required to demonstrate
that it meets all other specified levels and standards in quality, effectiveness, audit, etc. NSD meets with the
service providers at least twice yearly to discuss both general activity and specific developments, and is
required by SEHD to conduct regular reviews of the service to ensure that it continues to meet the criteria
for designation and continues to fulfil its requirements in these areas. Neonatal cardiology was included in
the single service level agreement from 2004/05.
The service covers direct inpatient services from admission for heart surgery, neonatal cardiology or
interventional cardiology, (for elective cases up to two days prior to operation is covered, and for emergency
cases an in-patient stay begins on the day of the procedure) up to discharge or transfer from post-operative
ward, and includes all surgery, interventional cardiology and intensive therapy. In addition the service
provides facilities for pre-operative outpatient assessment and post-operative review. There are also some
specific exclusions, such as cardiology, diagnostic and imaging activities such as angiography and cardiac
catheterisation carried out prior to the definitive admission for cardiac surgery, which define the entry point
to the nationally designated service.
- 22 -

Review of Paediatric Cardiac Services in Scotland
4.1.2 Cardiac surgery
The service is designed to provide all open and closed cardiac surgery for children in Scotland up to and
including the age of 16 years, for all congenital and acquired heart disease, with the exception of surgery of
HLHS, currently provided from Birmingham Children's Hospital, and heart/heart & lung transplantation, provided
from Freeman Hospital, Newcastle.
Some additional surgical work is undertaken outwith the national designation, such as surgery provided to
children who are not Scottish residents. Currently, the service level agreement between NSD and the surgical
service is for 265 post-operative discharges. The current indicative levels of activity are as follows:
Closed simple 37 Closed complex 60 Open simple 11 Open intermediate 80 Open complex 77 TOTAL 265 = =
4.1.3 Interventional cardiology
Interventional cardiology was included in national designation from 2001, reflecting the need to have cardiac
surgery back up on site for interventional cardiology. A joint service level agreement is in place and NSD
receives activity returns and annual reports from the integrated service.
The agreement between NSD and the service currently indicates an activity level of 200 procedures. The main
cost drivers are identified below with indicative numbers for each procedure. Although this is not an exhaustive
list of the procedures which may be carried out by the interventional cardiology team under national designation,
it does identify the most usual procedures.
Balloon dilatation 50Electrophysiology 3Coil occlusion 25Device occlusion 42Pacemaker 11Stent 24Atrial Septostomy 12Ablation 10Other 23TOTAL 200
4.1.4 Neonatal cardiology
The service provides for assessment, investigation and stabilisation prior to cardiac surgery. This may
include detailed fetal scanning and intensive ventilatory support in the neonatal period. If the cardiac defect
is identified antenatally the mother may be delivered at the Queen Mother’s Hospital (QMH).
- 23 -
Review of Paediatric Cardiac Services in Scotland
The indicative level of activity for the neonatal cardiology component of the service is for 65 procedures per
year. Of these it can be expected that 33 women will be delivered at QMH and 32 will be delivered at the
referral hospital but transferred soon after delivery. The current service level agreement does not define
indicative activity by procedure, but according to the 2005/06 annual report of the service, 25% (n = 17) of
admissions (n = 67) were for surgical management of patent ductus arteriosus, and 42% presented with
cyanotic congenital heart disease, many requiring subsequent surgical intervention.
4.2 Activity
435 children were treated for congenital heart disease in the Scottish service in 2006/07. Some children
require more than one surgical and / or interventional procedure in the course of their life. A total of 530
procedures were carried out in 2006/07. The average number of procedures per child over the last 6 years
has been 1.2. Details of the 2006/07 caseload are set out in Appendix B.
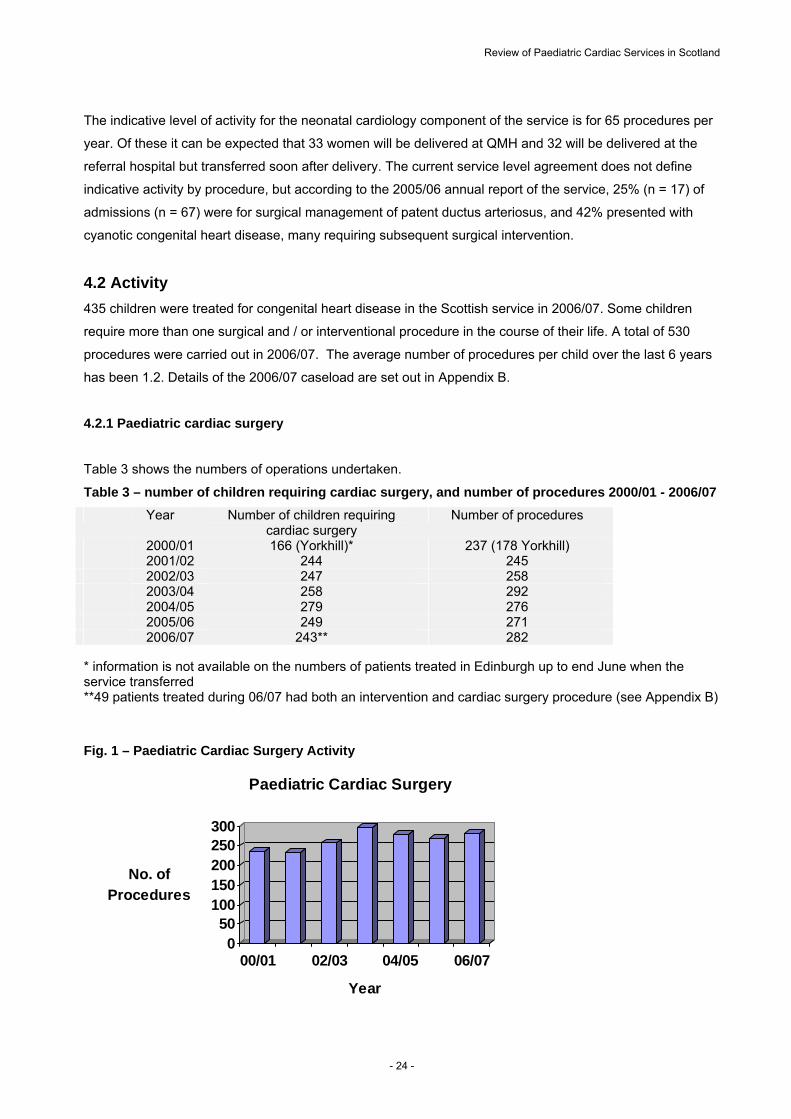
4.2.1 Paediatric cardiac surgery
Table 3 shows the numbers of operations undertaken.
Table 3 – number of children requiring cardiac surgery, and number of procedures 2000/01 - 2006/07
Year Number of children requiring cardiac surgery
Number of procedures
2000/01 166 (Yorkhill)* 237 (178 Yorkhill) 2001/02 244 245 2002/03 247 258 2003/04 258 292 2004/05 279 276 2005/06 249 271 2006/07 243** 282 * information is not available on the numbers of patients treated in Edinburgh up to end June when the service transferred **49 patients treated during 06/07 had both an intervention and cardiac surgery procedure (see Appendix B)
Fig. 1 – Paediatric Cardiac Surgery Activity
050
100150200250300
No. of
Procedures
00/01 02/03 04/05 06/07
Year
Paediatric Cardiac Surgery
- 24 -
Review of Paediatric Cardiac Services in Scotland
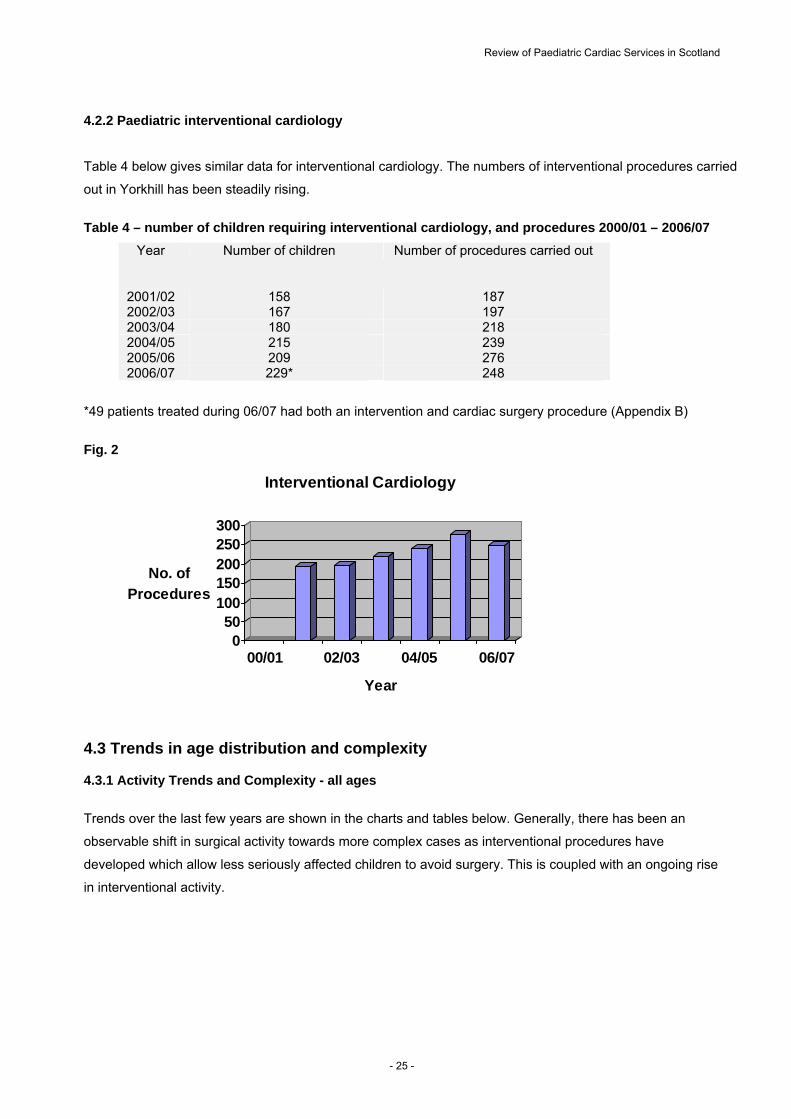
4.2.2 Paediatric interventional cardiology
Table 4 below gives similar data for interventional cardiology. The numbers of interventional procedures carried
out in Yorkhill has been steadily rising.
Table 4 – number of children requiring interventional cardiology, and procedures 2000/01 – 2006/07
Year Number of children Number of procedures carried out
2001/02 158 187 2002/03 167 197 2003/04 180 218 2004/05 215 239 2005/06 209 276 2006/07 229* 248
*49 patients treated during 06/07 had both an intervention and cardiac surgery procedure (Appendix B)
Fig. 2
050
100150200250300
No. of
Procedures
00/01 02/03 04/05 06/07
Year
Interventional Cardiology
4.3 Trends in age distribution and complexity 4.3.1 Activity Trends and Complexity - all ages
Trends over the last few years are shown in the charts and tables below. Generally, there has been an
observable shift in surgical activity towards more complex cases as interventional procedures have
developed which allow less seriously affected children to avoid surgery. This is coupled with an ongoing rise
in interventional activity.
- 25 -
Review of Paediatric Cardiac Services in Scotland
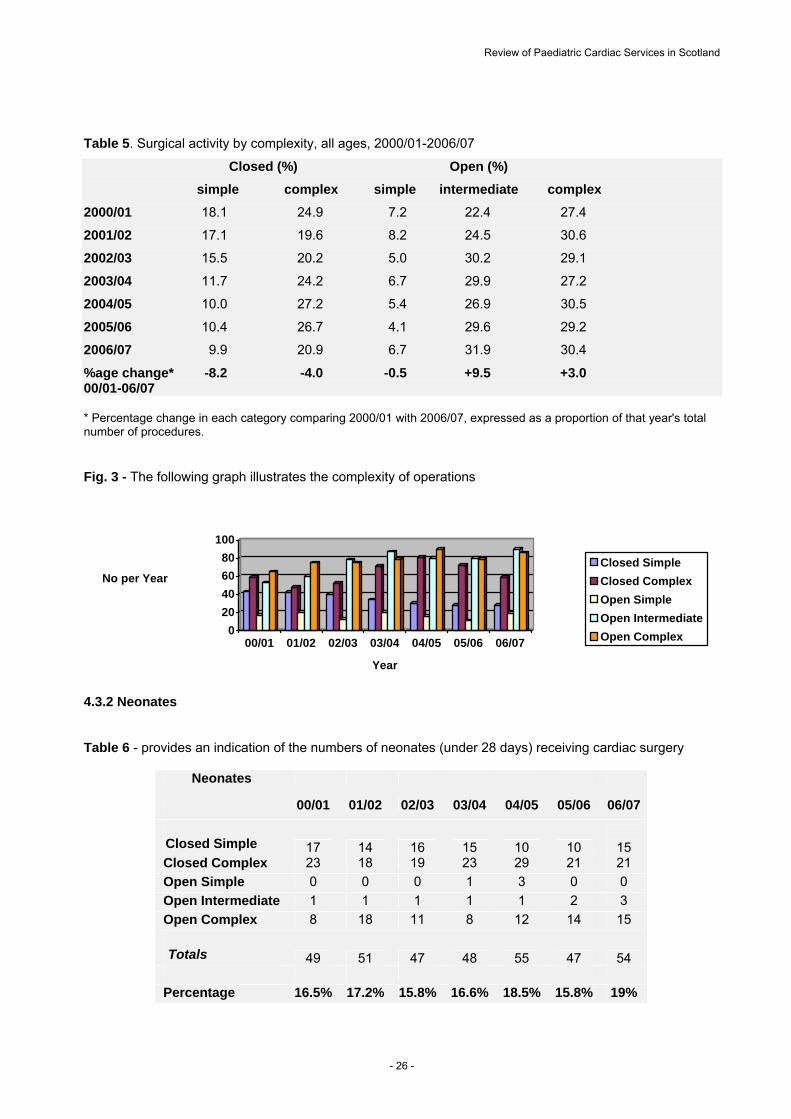
Table 5. Surgical activity by complexity, all ages, 2000/01-2006/07
Closed (%) Open (%)
simple complex simple intermediate complex
2000/01 18.1 24.9 7.2 22.4 27.4
2001/02 17.1 19.6 8.2 24.5 30.6
2002/03 15.5 20.2 5.0 30.2 29.1
2003/04 11.7 24.2 6.7 29.9 27.2
2004/05 10.0 27.2 5.4 26.9 30.5
2005/06 10.4 26.7 4.1 29.6 29.2
2006/07 9.9 20.9 6.7 31.9 30.4
%age change* -8.2 -4.0 -0.5 +9.5 +3.0 00/01-06/07 * Percentage change in each category comparing 2000/01 with 2006/07, expressed as a proportion of that year's total number of procedures. Fig. 3 - The following graph illustrates the complexity of operations
0
20
40
60
80
100
No per Year
00/01 01/02 02/03 03/04 04/05 05/06 06/07
Year
Closed Simple
Closed Complex
Open Simple
Open Intermediate
Open Complex
4.3.2 Neonates Table 6 - provides an indication of the numbers of neonates (under 28 days) receiving cardiac surgery
Neonates
00/01 01/02 02/03 03/04 04/05 05/06 06/07
Closed Simple 17 14 16 15 10 10
15 Closed Complex 23 18 19 23 29 21 21
Open Simple 0 0 0 1 3 0 0
Open Intermediate 1 1 1 1 1 2 3
Open Complex 8 18 11 8 12 14 15
Totals 49 51 47 48 55 47 54
Percentage 16.5% 17.2% 15.8% 16.6% 18.5% 15.8% 19%
- 26 -

Review of Paediatric Cardiac Services in Scotland
Fig. 4 - shows that neonates have remained at around 16% of the caseload
0.0%
5.0%
10.0%
15.0%
20.0%
% of Neonates
00/01 01/02 02/03 03/04 04/05 05/06 06/07
Year
Neonates
4.3.3 Infants Until 2006/07, infants made up around 15 - 20% of the caseload. The reason for the change in 2006/07 has not yet been investigated. Table 7
Infant < 1 Year
00/01 01/02 02/03 03/04 04/05 05/06 06/07
Closed Simple 16 17 18 13 16 15 10
Closed Complex 21 17 19 29 25 30 21
Open Simple 1 3 1 1 3 2 1
Open Intermediate 18 15 16 26 31 22 34
Open Complex 22 18 19 26 26 23 18
Totals 78 70 73 95 101 92 84
Percentage 15.3% 13.8% 14.3% 18.7% 19.8% 18.1% 28%
Fig. 5
0.0%5.0%
10.0%15.0%20.0%25.0%30.0%
% of Infant <1 Year
00/01 01/02 02/03 03/04 04/05 05/06 06/07
Year
Infant <1 Year
- 27 -

Review of Paediatric Cardiac Services in Scotland
4.4 Hypoplastic Left Heart Syndrome
Hypoplastic left heart disease occurs in less than 2/10,000 births
http://www.nlm.nih.gov/medlineplus/ency/article/001106.htm. The table below shows the number of cases
expected in Scotland according to birth rates over the last six years.
Table 8
Year Live births Expected no. of children with HLHS
2001 52,527 11 2002 51,270 10 2003 52,432 10 2004 53,957 11 2005 54,386 11 2006 55,690 11
This condition is corrected by staged surgical procedures at a few days old, 4-6 months and 18 months to 3
years old. Scottish children have been referred to Birmingham over the past few years. Table 9 shows 5
children who have been treated in Birmingham together with PICU use and cost.
Table 9 - Birmingham Children's Hospitals Cardiac Surgery / Cardiology Procedures 2005/06
NHS Board
HRG Code
Activity - Spells Breakdown of Charge
Day
Case Inpatient Totals
PICU Bed Days Standard
Tariff Top Up
Excess Bed Days
PICU Totals
A&A E41 0 2 2 1 9,180 6,334 4,121 2,214
21,849
D&G E03 0 1 1 1 9,787 6,753
- 2,214
18,754
Glasgow E41 0 2 2 2 9,180 6,334
- 4,428
19,943
Grampian E41 0 1 1 1 4,590 3,167
- 2,214
9,971
Lanarkshire E03 0 1 1 1 9,787 6,753
- 2,214
18,754
Totals 0 7 7 6 42,524 29,342 4,121 13,285 89,272
Notes. HRG codes - E03: Cardiac Valve Procedures
E41: Other Cardiothoracic or Circulatory Procedures <19 Individual patient information is no longer provided
The number of children treated at Birmingham is less than predicted – possible explanations include coding
issues, termination of pregnancy for this condition, the choice of families to allow the child to die without
further treatment, or neonates not being referred for a variety of other reasons. Elliot (2004) reported a
similar effect in a UK study; although surgery for HLHS was readily available, only 47 first stage procedures
were performed in the year of analysis and of these, 20% were referred from outwith the UK. According to
the birthrate and incidence of HLHS, the expected number of incident cases that year was 382.
- 28 -

Review of Paediatric Cardiac Services in Scotland
4.5 Summary and Conclusions - Assessed Future Needs
The current level of interventional cardiology activity in the service level agreement requires revision in the
light of current trends. In 2006/07, numbers were as follows:
Procedure indicative actual
Cardiac surgery 265 282
Interventional cardiology 200 248
Neonatal cardiology 65 65
This review concludes that, in the light of population projections of need and actual trends in activity over
the last few years, the activity levels for the Service Agreement in 2007/08 and future years should be:
- 275 cardiac surgical procedures a year (rising to 290 a year including hypoplastic left heart)
- 240 interventional cardiology procedures a year (recognising that some of these are joint
procedures with surgery)
- 65 neonatal cardiology interventions a year.
- 29 -
Review of Paediatric Cardiac Services in Scotland
5. Current issues within the service 5.1 Overview
During the course of the review a meeting was held between clinical and managerial staff from Yorkhill and
the review team form National Services Division. The aim of this was to discuss and document the issues
which currently affect the service and the proposals being developed or implemented to deal with them.
Issues which were identified included service-specific issues and wider issues which were affecting this and
other specialities.
5.2 Hypoplastic left heart surgery
Neonates with HLHS are currently referred to Birmingham and, on occasions, to Guy's Hospital in London
due to capacity issues at Birmingham. Babies who are diagnosed pre-natally are normally delivered at the
Queen Mother's Hospital in Glasgow and subsequently transferred to Birmingham (or Guy's) for treatment.
They are sometimes referred back to Yorkhill PICU or ward for further supportive care post-operatively. All
prenatally diagnosed babies should be discussed with the cardiac team at Yorkhill to inform clinical
management and transfer decisions. The Yorkhill unit is currently working on plans for a formal reiteration of
the need for units to seek their guidance on pre-natally detected cases, which represent around 50% of the
total. Post-natal cases should also always be discussed with the team.
There is a need to consider whether babies still need to travel to Birmingham for this condition. When the
decision was taken some ten years ago for all Scottish children with hypoplastic left heart to go to
Birmingham it was because at that time both the surgery and post surgical care in intensive care were at the
boundaries of medical techniques. Now however experience has been built up in a range of increasingly
complex procedures and the procedure used in hypoplastic left heart is within the scope of the complexity of
surgery now undertaken at Yorkhill.
There would be benefits for families in reducing the need for travel to Birmingham in the first few days after
birth and the disruption this causes to the family. NSD therefore considers that a programme of work should
now be put in hand to train staff and develop the capability to provide this element of cardiac surgery at
Yorkhill in future. The return of the service to Scotland is, however, dependent on a proposal which is
currently being developed, which must ensure that the unit at Yorkhill is fully prepared to offer a service that
is both clinically effective and equivalent to the English alternative. With this aim, the Yorkhill cardiac team
have documented an explicit set of objectives to enable the return of surgery for HLHS to Glasgow. Early
indications suggest that the repatriation of this part of the service could be achieved within current resource;
but as a specific development or future plan this would be looked at in detail once a fully detailed and costed
proposal was available.
The rationale behind the change is the desire to offer a comprehensive cardiac surgery programme and
minimise travel and inconvenience for families.
- 30 -
Review of Paediatric Cardiac Services in Scotland
This review recommends that hypoplastic left heart surgery should be provided in Scotland from 1 April
2008.
5.3 Capacity
There are a number of issues affecting the ability of the service to fulfil the demands placed on it. These are
related to staffing, intensive care provision and theatre time.
Staffing
There are currently three surgeons who operate on children with congenital heart disease at Yorkhill. These
surgeons also have a commitment to the adult cardiac surgery service. The key issues which require to be
considered are:
Succession planning for consultants - it may be necessary for any new consultant to work alongside
experienced colleagues to ensure a proper and safe handover of the clinical workload.
Clarity about when a new consultant will assume responsibility for the workload.
Standards which require to be kept in mind when planning the service: requirements to operate on a
minimum number of cases per year and have at least two surgeons with experience in open heart
surgery on infants.
NSD has agreed additional funding for 2-3 years for a 4th consultant cardiac surgeon to work alongside
existing consultants to provide succession planning.
In common with many other specialities, there are implications of Government policy on working time and
modernising medical careers (MMC) concerning the availability of junior doctors to cover service
commitments after August 2007. In addition, junior doctors may, in future, be less experienced when they
are appointed to cardiac services and require higher levels of supervision. This issue will be progressed
jointly by NSD and Yorkhill, as in future a solution may prove workable in conjunction with other services. In
the meantime NSD has agreed additional funding for a further junior doctor as a consequence of MMC.
Theatre availability
NSD is currently funding, on a non-recurring basis, a Friday theatre session to ease waiting list and
emergency pressures. Yorkhill management have agreed a theatre utilisation policy to ensure maximum
capacity usage throughout the week. This, plus the appointment of a fourth surgeon, will enable the service
to meet waiting time targets. The service has been asked to include data on theatre utilisation in future
annual reports.
- 31 -

Review of Paediatric Cardiac Services in Scotland
5.4 Northern Ireland Activity
NHS Greater Glasgow and Clyde has responded to a request from the NHS in Northern Ireland and has
formally expressed an interest in providing paediatric cardiac services for Northern Ireland (NI). The NI
activity has been estimated at 80 cardiac surgery cases per year with some of the more complex patients
currently treated in Birmingham. In addition, there is one interventional catheter session per week.
NSD understands that negotiations are continuing between the Health Departments in Northern Ireland and
Scotland, and NHS Greater Glasgow and Clyde.
Clearly, to avoid any detriment to the children of Scotland, such a development would need to be fully
funded and resourced by the NHS in Northern Ireland..
- 32 -
Review of Paediatric Cardiac Services in Scotland
Section 6 Outcomes & quality
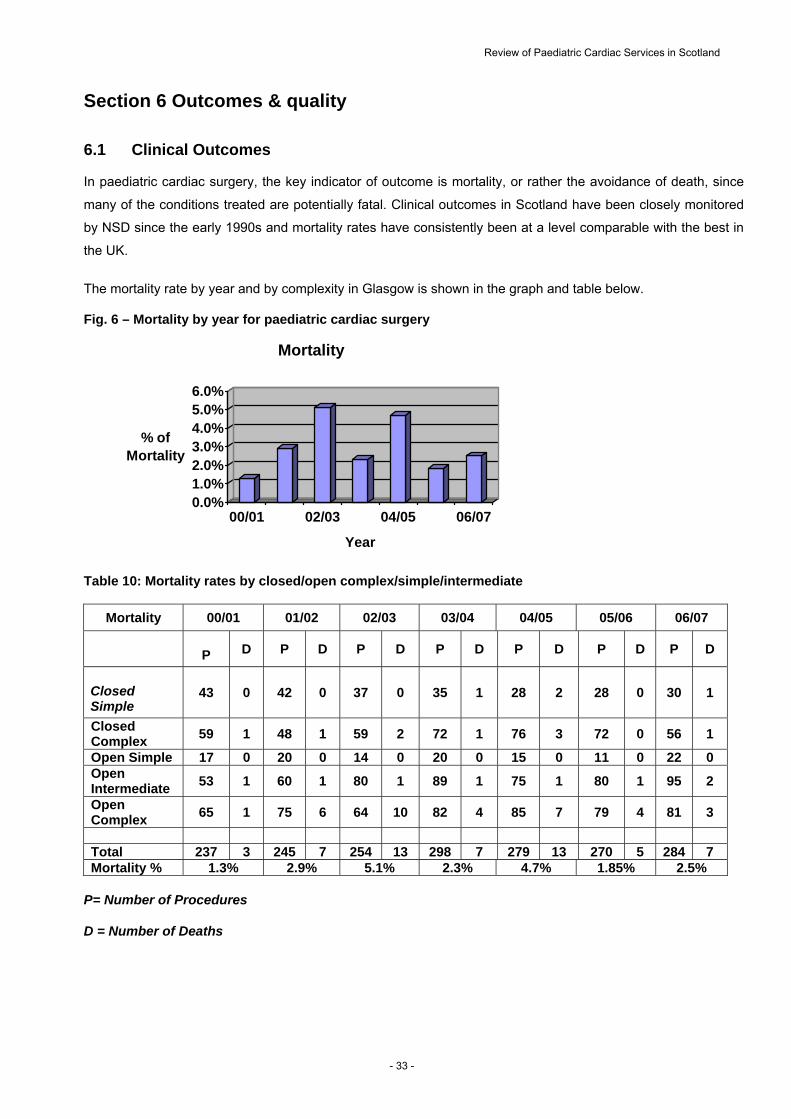
6.1 Clinical Outcomes In paediatric cardiac surgery, the key indicator of outcome is mortality, or rather the avoidance of death, since
many of the conditions treated are potentially fatal. Clinical outcomes in Scotland have been closely monitored
by NSD since the early 1990s and mortality rates have consistently been at a level comparable with the best in
the UK.
The mortality rate by year and by complexity in Glasgow is shown in the graph and table below. Fig. 6 – Mortality by year for paediatric cardiac surgery
0.0%1.0%2.0%3.0%4.0%5.0%6.0%
% of Mortality
00/01 02/03 04/05 06/07
Year
Mortality
Table 10: Mortality rates by closed/open complex/simple/intermediate
Mortality 00/01 01/02 02/03 03/04 04/05 05/06 06/07
P D P D P D P D P D P D P D
Closed Simple
43 0 42 0 37 0 35 1 28 2 28 0 30 1
Closed Complex
59 1 48 1 59 2 72 1 76 3 72 0 56 1
Open Simple 17 0 20 0 14 0 20 0 15 0 11 0 22 0 Open Intermediate
53 1 60 1 80 1 89 1 75 1 80 1 95 2
Open Complex
65 1 75 6 64 10 82 4 85 7 79 4 81 3
Total 237 3 245 7 254 13 298 7 279 13 270 5 284 7 Mortality % 1.3% 2.9% 5.1% 2.3% 4.7% 1.85% 2.5%
P= Number of Procedures
D = Number of Deaths
- 33 -

Review of Paediatric Cardiac Services in Scotland
6.2 UK services & standards The most recent comparable UK figures available at present are 2001/02 although updated figures are due
to be published on 1 June 2007. The 2001/02 figures show that overall performance of the Scottish service
and performance in relation to specific procedures compares favourably with the rest of the UK.
Table 11 Mortality (all ages) – UK comparisons 2001/02 Cardiac Surgery Interventional cardiology Royal Hospital for Sick Children, Glasgow
2.9%
0%
UK average
4.1%
0.9%
Published studies have a demonstrated a link between volume and outcome in paediatric cardiac surgery.
As the trend towards interventional and minimally invasive procedures began to take over from open heart
surgery in the 1990s, clinicians in Scotland actively sought to centralise the service on one site.
This led to the decision to centralise the service in Glasgow in 2000 into a single unit performing some 270
surgical procedures a year. While there is no firm evidence on the minimum number of procedures required
to maintain clinical expertise, the figure of 300 a year is broadly accepted in literature. The Scottish service
is close to this number and continues to demonstrate outcomes consistent with the best in the UK.
The review of paediatric and congenital cardiac services carried out in England, Wales and Northern Ireland
in response to the Kennedy report (2001) on the Bristol service, set out guidance on service standards for
children with cardiac conditions and requirements to maintain high quality services (Department of Health,
2003). The Government accepted all of the recommendations with one exception, which was the
recommendation that centres should carry out a minimum of 300 operations per year. The evidence for a
volume/outcome relationship based on this number is not conclusive as the Central Cardiac Database and
subsequent publications do not indicate any discernable difference in survival between the 13 UK centres,
though it should be noted that confidence intervals for the smaller centres were wide and limited the ability
to accurately assess or detect any underperformance in one year of data (Gibbs et al, 2004).
The other recommended standards related explicitly to the following areas:
Clinical team leadership with shared responsibility
Evaluation of clinical practice with dissemination of key lessons
Provision of a child centred environment
Information and consent
The patient journey from screening, assessment and diagnosis
Medical and surgical care
Discharge and going home
- 34 -

Review of Paediatric Cardiac Services in Scotland
Growing up and transition to adult services
Support to parents and families
These have been acted upon in the Scottish service and NSD continues to monitor performance against UK
clinical standards.
6.3 Waiting times
At end March 2007, 49 patients were waiting on the surgical waiting list and 45 patients were on the
catheter waiting list for interventional cardiology. The charts below show the progress in reducing the
waiting list for both surgery and interventional cardiology.
Figs. 7 and 8
74
6669 71 71
78 81 7984
78
67
59 6168
63
5562
57 5952
57 5754
70 67
59
5158 61
5559 60 60
5255
49
0
10
20
30
40
50
60
70
80
90
04 04 04 04 04 04 04 04 04 05 05 05 05 05 05 05 05 05 05 05 05 06 06 06 06 06 06 06 06 06 06 06 06 07 07 07
Surgical Waiting List : Running Total (2004 to 2007)
4 1
52 54 57 55
6 6 6 7 706 2 6 4
7973
6 7
8 5 8 2 8 3 8 278
736 9
746 6
596 7
78 7874
78
6 357
4 64 0
4 452
4 3 4 5
0
10
20
30
40
50
60
70
80
90
Apr
May Jun
Jul
Aug Sep Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep Oct
Nov
Dec Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep Oct
Nov
Dec Jan
Feb
Mar
04 04 04 04 04 04 04 04 04 05 05 05 05 05 05 05 05 05 05 05 05 06 06 06 06 06 06 06 06 06 06 06 06 07 07 07
Cath Waiting List : Month End Running Total
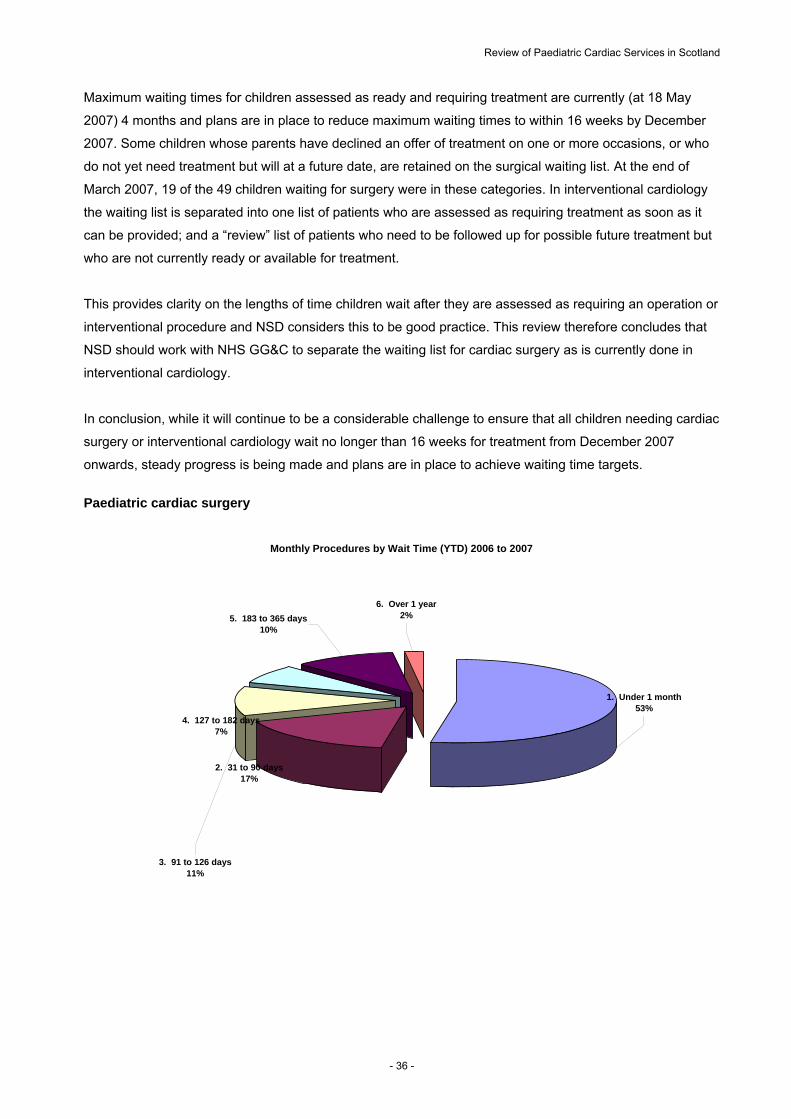
There remain a number of children on the waiting list who have waited longer that the target waiting time of
16 weeks. All urgent cases receive surgery or interventional cardiology without delay. In 2006/07, 53% of
children received surgery within 1 month; 80% within 4 months.
- 35 -
Review of Paediatric Cardiac Services in Scotland
Maximum waiting times for children assessed as ready and requiring treatment are currently (at 18 May
2007) 4 months and plans are in place to reduce maximum waiting times to within 16 weeks by December
2007. Some children whose parents have declined an offer of treatment on one or more occasions, or who
do not yet need treatment but will at a future date, are retained on the surgical waiting list. At the end of
March 2007, 19 of the 49 children waiting for surgery were in these categories. In interventional cardiology
the waiting list is separated into one list of patients who are assessed as requiring treatment as soon as it
can be provided; and a “review” list of patients who need to be followed up for possible future treatment but
who are not currently ready or available for treatment.
This provides clarity on the lengths of time children wait after they are assessed as requiring an operation or
interventional procedure and NSD considers this to be good practice. This review therefore concludes that
NSD should work with NHS GG&C to separate the waiting list for cardiac surgery as is currently done in
interventional cardiology.
In conclusion, while it will continue to be a considerable challenge to ensure that all children needing cardiac
surgery or interventional cardiology wait no longer than 16 weeks for treatment from December 2007
onwards, steady progress is being made and plans are in place to achieve waiting time targets.
Paediatric cardiac surgery
Monthly Procedures by Wait Time (YTD) 2006 to 2007
6. Over 1 year2%
4. 127 to 182 days7%
3. 91 to 126 days11%
2. 31 to 90 days17%
5. 183 to 365 days10%
1. Under 1 month53%
- 36 -
Review of Paediatric Cardiac Services in Scotland
7. Finance
7.1 Service Funding Methodology
Section 4 “Current Service for Residents of Scotland” outlined the current commissioning arrangements for
paediatric cardiac services. In summary NSD have three components of service delivery within the service
level agreement with NHS Greater Glasgow & Clyde, these are:
Paediatric Cardiac Surgery (PCS), Activity 265, Value £6.2 million
Interventional Cardiology (IC), Activity 200, Value £1.6 million
Neonatal Cardiology (NC), Activity 65, Value £0.5 million
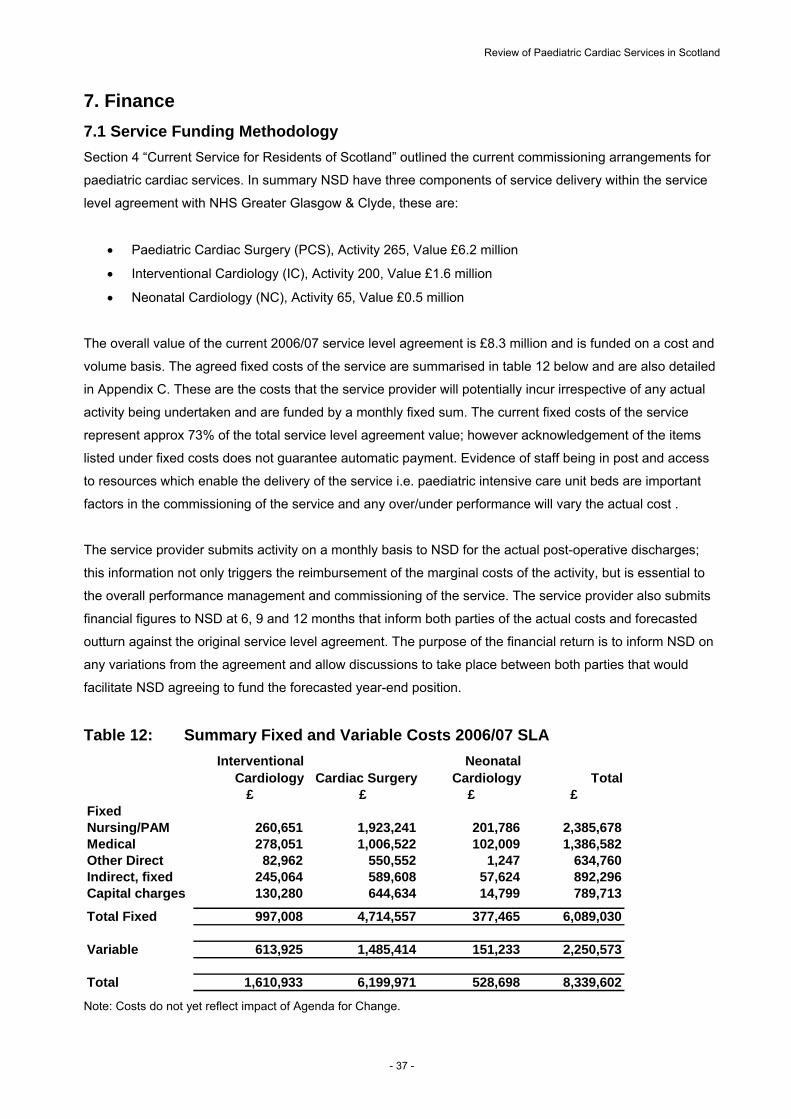
The overall value of the current 2006/07 service level agreement is £8.3 million and is funded on a cost and
volume basis. The agreed fixed costs of the service are summarised in table 12 below and are also detailed
in Appendix C. These are the costs that the service provider will potentially incur irrespective of any actual
activity being undertaken and are funded by a monthly fixed sum. The current fixed costs of the service
represent approx 73% of the total service level agreement value; however acknowledgement of the items
listed under fixed costs does not guarantee automatic payment. Evidence of staff being in post and access
to resources which enable the delivery of the service i.e. paediatric intensive care unit beds are important
factors in the commissioning of the service and any over/under performance will vary the actual cost .
The service provider submits activity on a monthly basis to NSD for the actual post-operative discharges;
this information not only triggers the reimbursement of the marginal costs of the activity, but is essential to
the overall performance management and commissioning of the service. The service provider also submits
financial figures to NSD at 6, 9 and 12 months that inform both parties of the actual costs and forecasted
outturn against the original service level agreement. The purpose of the financial return is to inform NSD on
any variations from the agreement and allow discussions to take place between both parties that would
facilitate NSD agreeing to fund the forecasted year-end position.
Table 12: Summary Fixed and Variable Costs 2006/07 SLA
Interventional Cardiology Cardiac Surgery
Neonatal Cardiology Total
£ £ £ £FixedNursing/PAM 260,651 1,923,241 201,786 2,385,678Medical 278,051 1,006,522 102,009 1,386,582Other Direct 82,962 550,552 1,247 634,760Indirect, fixed 245,064 589,608 57,624 892,296Capital charges 130,280 644,634 14,799 789,713
Total Fixed 997,008 4,714,557 377,465 6,089,030
Variable 613,925 1,485,414 151,233 2,250,573
Total 1,610,933 6,199,971 528,698 8,339,602
Note: Costs do not yet reflect impact of Agenda for Change.
- 37 -
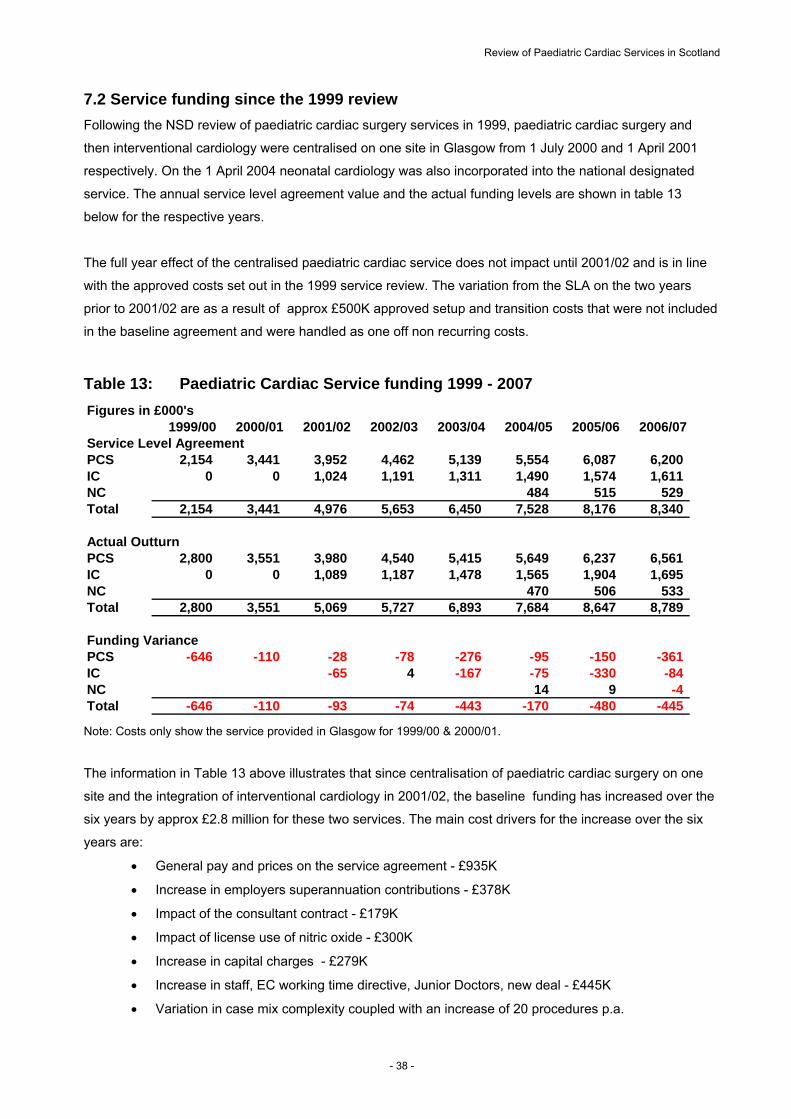
Review of Paediatric Cardiac Services in Scotland
7.2 Service funding since the 1999 review
Following the NSD review of paediatric cardiac surgery services in 1999, paediatric cardiac surgery and
then interventional cardiology were centralised on one site in Glasgow from 1 July 2000 and 1 April 2001
respectively. On the 1 April 2004 neonatal cardiology was also incorporated into the national designated
service. The annual service level agreement value and the actual funding levels are shown in table 13
below for the respective years.
The full year effect of the centralised paediatric cardiac service does not impact until 2001/02 and is in line
with the approved costs set out in the 1999 service review. The variation from the SLA on the two years
prior to 2001/02 are as a result of approx £500K approved setup and transition costs that were not included
in the baseline agreement and were handled as one off non recurring costs.
Table 13: Paediatric Cardiac Service funding 1999 - 2007
Figures in £000's1999/00 2000/01 2001/02 2002/03 2003/04 2004/05 2005/06 2006/07
Service Level AgreementPCS 2,154 3,441 3,952 4,462 5,139 5,554 6,087 6,200IC 0 0 1,024 1,191 1,311 1,490 1,574 1,611NC 484 515 529Total 2,154 3,441 4,976 5,653 6,450 7,528 8,176 8,340
Actual OutturnPCS 2,800 3,551 3,980 4,540 5,415 5,649 6,237 6,561IC 0 0 1,089 1,187 1,478 1,565 1,904 1,695NC 470 506 533Total 2,800 3,551 5,069 5,727 6,893 7,684 8,647 8,789
Funding VariancePCS -646 -110 -28 -78 -276 -95 -150 -361
-65 -167 -75 -330 -84 -4
-646 -110 -93 -74 -443 -170 -480 -445
IC 4NC 14 9Total Note: Costs only show the service provided in Glasgow for 1999/00 & 2000/01.
The information in Table 13 above illustrates that since centralisation of paediatric cardiac surgery on one
site and the integration of interventional cardiology in 2001/02, the baseline funding has increased over the
six years by approx £2.8 million for these two services. The main cost drivers for the increase over the six
years are:
General pay and prices on the service agreement - £935K
Increase in employers superannuation contributions - £378K
Impact of the consultant contract - £179K
Impact of license use of nitric oxide - £300K
Increase in capital charges - £279K
Increase in staff, EC working time directive, Junior Doctors, new deal - £445K
Variation in case mix complexity coupled with an increase of 20 procedures p.a.
- 38 -

Review of Paediatric Cardiac Services in Scotland
The cost of funding the pressures and developments have been met and absorbed from the general uplift
on the overall NSD baseline apart from an additional allocation specifically to meet the costs related to
employer’s superannuation agreements.
The information in Table 13 also illustrates the additional funding allocated to the service over and above
the baseline service agreement value. It should be noted that some of the pressures and developments
highlighted to NSD during a financial year will, if agreed be incorporated in the following years baseline
agreement value. However looking at the information provided in Table 13 in conjunction with the activity
data that is provided in Table 14 below it can be seen that a major cost driver has been the substantial
increase in activity especially over the last three years. The 2006/07 figures show 65 post-operative
discharges over the baseline activity agreement and further analysing the variable costs shown in Appendix
D, it can be seen that the financial impact of the increase in activity coupled with the variation to the case
mix complexity accounts for £248,385. Two other cost pressures make up the remainder of the £197K
overspend. The first one has been discussed in section 5 “Current issues within the service” NSD is
currently funding £112K on a non-recurring basis, a Friday theatre session to ease waiting list and
emergency pressures and the last cost pressure funded in 2006/07 is cardiac nursing posts, £85K.
Table 14: Paediatric Cardiac Service activity 1999 - 2007
Figures in post-operative discharges1999/00 2000/01 2001/02 2002/03 2003/04 2004/05 2005/06 2006/07
Service Level AgreementPCS 180 247 270 270 265 265 265 265IC 0 0 175 175 200 200 200 200NC 65 65 65Total 180 247 445 445 465 530 530 530
Actual OutturnPCS 149 237 234 258 292 276 271 282IC 0 0 187 197 218 239 276 248NC 58 61 65Total 149 237 421 455 510 573 608 595
Activity VariancePCS 31 10 36 12IC 0 0NC 7 4 0Total 31 10 24
-27 -11 -6 -17 -12 -22 -18 -39 -76 -48
-10 -45 -43 -78 -65
- 39 -

Review of Paediatric Cardiac Services in Scotland
7.3 Future service funding
There are a number of service issues, pressures and recommendations coming out of the review that have
a financial impact on the service agreement going forward. Some of the issues are costs that are currently
being absorbed into the actual funding of the service, a summary of these are listed below:
Increase in activity levels and rebasing case mix complexity from 2007/08
o 275 cardiac surgical procedures a year, estimated additional cost £125K
o 240 interventional procedures a year, estimated additional cost £61K
o 65 neonatal procedures a year, no additional cost
Hypoplastic left heart surgery service currently funded by NSD and provided in Birmingham at an
approx cost of £89K. Recommendation to provide within Glasgow service from 1 April 2008. No
additional cost estimated.
Succession planning for consultant cardiac consultant - NSD have agreed additional funding for 3
years for a 4th consultant to work alongside existing consultants, estimated costs already included
within 2007/08 plan, estimated additional cost £150K.
Nursing posts previously funded by the British Heart Foundation - NSD agreed in 2005/06 to
include in our service agreement the cost of these posts once the soft funding finished. An
addendum in the 2006/07 financial year was issued to cover the £85K and the baseline for 2007/08
has been adjusted to reflect the cost associated with the posts.
Modernising medical careers – proposals submitted by Glasgow concerning the availability of junior
doctors to cover service commitments after August 2007 are estimated at £85K recurring (£40K in
2007/08).
No service issues, pressures and recommendations coming out of this review will require the request to top
slice additional funds from NHS Boards.
- 40 -

Review of Paediatric Cardiac Services in Scotland
8. Fit against NSAG Criteria
Every 3-5 years NSD is required by SEHD and NHS Boards to review whether each designated national
specialist service continues to meet the criteria for designation. In summary, the criteria for designation as a
national specialist service are:
Need for service is low in terms of volume of cases, and/or is unpredictable, uneven
Clinical effectiveness is proven
The service is cost effective
Individual unit costs of treatment are high as a result of a need for expensive equipment or a highly
skilled clinical team
The service can only be clinically, or cost, effectively delivered on one or very few sites
The service is small in scale
In paediatric cardiac services the number of children requiring medical intervention each year is low -
around 400-450 a year. Both cardiac surgery and interventional cardiology in children involve techniques of
proven clinical effectiveness. (Survival rates exceed 95% and most children receiving treatment survive into
adulthood.)
The service requires concentration of clinical expertise and both highly skilled multidisciplinary team and
specialist equipment that can only be clinically and cost effectively, sustained on a single site in Scotland.
Unit costs are around £16,000 on average per procedure although complex cardiac surgery is considerably
more expensive, and some interventional cardiology is less expensive.
In conclusion, the service continues to fit the criteria for national designation.
9. Conclusions
9.1 The number of children likely to require cardiac surgery or interventional cardiology is likely to increase
over the next 5 years in proportion to the increasing birth rate. Current numbers are around 400-450
children each year.
9.2 In the early 1990s treatment involved conventional heart surgery and some 450 operations were
required a year, but as interventional techniques developed, there was a drop in the numbers needing
surgery, and an increase in complexity. The numbers of operations required has been stable at around 270
a year for around 5 years. A small increase is expected in future in line with the increasing birthrate.
- 41 -

Review of Paediatric Cardiac Services in Scotland
9.3 There has been an increase in the number of interventional cardiology procedures – and a recent
development has been joint interventional cardiology and cardiac surgery for some complex cases.
9.4 Using population projections and past experience as the basis on which to predict future need, the
number of operations required in the next five years is 275 a year; and the of interventional cardiology
procedures required is 240. The number of admissions for specialist cardiology and neonatology in the
neonatal cardiology service is expected to remain at 65.
9.5 Maximum waiting times for children assessed and ready for treatment are currently 4 months and the
increases in activity noted above, and the planned investment in PICU from 2007/08, should ensure that the
16 week target in December 2007 should be achieved and sustained.
9.6 Clinical outcomes are comparable with the rest of the UK.
There are improvements in survival for children with even the most complex cardiac disease.
There is a need to focus on measuring and improving long-term morbidity.
Surgical advances in the treatment of hypoplastic left heart syndrome have led to dramatic
improvements in survival and the surgery is now within the scope of complexity of the Scottish
service.
9.7 The service continues to fit the criteria for designation.
- 42 -

Review of Paediatric Cardiac Services in Scotland
10. Recommendations
10.1 NSD should increase activity levels in the service agreement to:
- 275 cardiac surgical procedures a year (290 including hypoplastic left heart syndrome)
- 240 interventional cardiology procedures a year (recognising that some of these are joint
procedures with surgery)
- maintain number of neonatal cardiology admissions at 65 a year.
10.2 The surgical waiting list should only be used for patients for whom diagnostic tests are complete and
the patient requires surgery imminently. NHS GG&C should maintain a separate list of patients who will
need surgery at a planned future date, or who need a planned future review to assess whether surgery is
required; or who have turned down an invitation for treatment but who continue to need followed up.
10.3 Hypoplastic left heart surgery should be provided in Glasgow for Scottish residents in future. A
structured programme of staff training should be put in place with a view to providing surgery in Glasgow
from 1 April 2008.
10.4 A fourth cardiac surgeon consultant should be appointed as soon as possible to provide succession
planning and continuity of the service (funding has been provided by NSD).
10.5 Since the service continues to fit the criteria for designation, it should continue to be commissioned
nationally as a national specialist service.
- 43 -
Review of Paediatric Cardiac Services in Scotland
References Appendix A
Andrews RE, Tulloh RMR (2004) Interventional cardiac catheterisation in congenital heart disease. Archives of Diseases in Childhood 2004; 89:1168-1173 Anyanwu AC, Rogers CA and Murday AJ (2002) Intrathoracic organ transplantation in the United Kingdom 1995-99: results from the UK cardiothoracic transplant audit Heart, 87 (5) pp 449 – 454 Aylin P, Bottle A, Jarman B and Elliott P (2004) Paediatric Cardiac Surgical Mortality in England after Bristol: descriptive analysis of hospital episode statistics 1991-2002. British Medical Journal 2004; 321: 825 Boucek MM (2001) The Registry of the International Society for Heart and Lung Transplantation: fourth official paediatric report 2000 The Journal of Heart and Lung Transplantation 20 (1) pp39 - 52 British Association of Paediatric Surgeons (2002) Paediatric Surgery: Standards of Care. British Association of Paediatric Surgeons, London, May 2002. Chang A (2000) Paediatric cardiac intensive care: current state of the art and beyond the millennium. Current Opinion in Paediatrics 2000:12:238-246 Chaturvedi R, Macrae D, Brown K L , Schindler M, Smith E C, Davis K B, Cohen G, Tsang V, Elliott M, De Leval M, Gallivan S and Goldman A P (2004) Cardiac ECMO for biventricular hearts after paediatric open heart surgery Heart 2004;90:545-551 Colombani PM et al (2003) Paediatric Transplantation American Journal of Transplantation Supplement Vol 3 Supp 4 pp 53 – 63 Conrad SA, Rycust PR (1998) Extracorporeal Life Support. American Society for Artificial Internal Organs Journal 1998;44:848-52. Department of Health (2003) Paediatric and Congenital Cardiac Services review Report. Department of Health Media Centre 2003/0519. December 2003. Daliento L, Mapelli D, Volpe B: “Measurement if Cognitive Outcome and Quality if Life in Congenital heart disease”. Heart 2006;92:569-574. Dietrich H, Buhrer C, Grimmer I, Dittrich S, Abdul-Khaliq H, Lange P E. (2003) Neurodevelopment at 1 Year of age in infants with Congenital Heart Disease; Heart 2003; 89:436-441 Elliot, M. 'A European perspective on the management of hypoplastic left heart syndrome' Cardiol. Young 2004:14 (suppl. 1) pp 41-46 Fraser A G, Buser P T, Bax J J, Dassen W R, Nihoyannopoulos P, Schwitter J, Knuuti J M, Höher M, Bengel F and Szatmária; (2006) The future of cardiovascular imaging and non-invasive diagnosis; A joint statement from the European Association of Echocardiography, the Working Groups on Cardiovascular Magnetic Resonance, Computers in Cardiology, and Nuclear Cardiology, of the European Society of Cardiology, the European Association of Nuclear Medicine, and the Association for European Paediatric Cardiology”; European Heart Journal Volume 27, Number 14, p.1750-1753 Fyler DC (1980). Report of the New England Regional Infant Cardiac Program. Paediatrics 1980; 65 (suppl):375-461 Germanakis I, Sifakis S. (2006). The Impact of Fetal Echocardiography on the Prevalence of Liveborn Congenital Heart Disease. Pediatr Cardiol; 2006 27:464-472. Gibbs JL, Monro JL, Cunningham D, Rickards A; (2004) Survival after surgery or therapeutic catheterisation for congenital heart disease in children in the United Kingdom: analysis of the central cardiac audit database for 2000-1. British Medical Journal 2004; 328: 611
- 44 -

Review of Paediatric Cardiac Services in Scotland
Goldmutz E. 2001. The Epidemiology and genetics of congenital heart disease. Clin Perinatol. 2001 Mar; 27(1):1-10 Hoffman, J. I. E., Kaplan, S. (2002). The Incidence of Congenital Heart Disease FACC Journal Am Coll Cardiol, 2002; 39:1890-1900 Kennedy (2001) Learning from Bristol: The report of the Public Inquiry into children’s heart surgery at the Bristol Royal Infirmary 1984-1995. Command Paper: CM 5207 July 2001 Kichuk-Chrisant MR (2002) Children are not small adults: some differences between paediatric and adult cardiac transplantation Current Opinion in Cardiology 17(2) pp 152 - 159 Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C (2005) Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis Health Technology Assessment 2005;9(44) Limperopoulos C, Majnemer A, Shvell M, , Rosenblatt B, Rohlicek C Tchervenkov C, Darwish H. Functional Limitations in Young Children with Congenital Heart Defects After Cardiac Surgery. Pediatrics;Dec 2001;108,6: pages 1325-1331. Limperopoulos C, Majnemer A, Shvell M, Rohlicek C, Rosenblatt B, Tchervenkov C, Darwish H. Predictors of developmental disabilities after open heart surgery in young children with congenital heart disease. Journal of pediatrics; 2002.Volume 141, no 1 – pages 51-58. Levi D S, Alejos J C, Moore J W (2003). Future of interventional cardiology in paediatrics. Current Opinion in Cardiology” 2003;18:79-90 Majnemer A,: Developmental Progress of Children with Congenital Heart Defects requiring open heart surgery: Seminary in Pediatric Neurology, vol 6, No 1 (March), 1999:pp12-19 Mendeloff E N (2002). The history of paediatric heart and lung transplantation Paediatric Transplantation 6(4); pp 270 - 279 Mitchell SC, Korones SB, Berendes HW. (1971)Congenital heart disease in 56,109 births. Incidence and natural history. Circulation. 1971; 43:323–332 National Services Division (1999) Review of paediatric cardiac surgery services in Scotland. National Services Division, January 1999. Noonan J A. (2004). A History of Paediatric Specialties: The Development of Paediatric Cardiology; Paediatric Research; Vol 56 No 2 2004 298-306. Perloff JK, Warnes CA (2001). Challenges posed by adults with repaired congenital heart disease; Circulation 2001 May 29; 103(21):2637-43 Petersen S, Peto V and Rayner M (2003) Congenital Heart Disease Statistics. British Heart Foundation Health Promotion Research Group, Department of Public Health, University of Oxford Rasiah S, Publicover M, Ewer A.K., Khan K.S., Kilby M.D., Zamoras J: (2006). A Systematic review of the accuracy of first-trimester ultrasound examination for detecting major congenital heart disease: Ultrasound in Obstet Gynecol 2006; 28:110-116
Rhodes J F, Lane G K, Tuzcu E M, Latson L A; Invasive Echocardiography: “The use of Catheter Imaging by the Interventional Cardiologist. Catheterization and Cardiovascular Interventions” 59:277-290(2003)
Richens T (2006) The Development of Paediatric Cardiac Services in Scotland. SMJ 2006: 51 (2)
- 45 -
Review of Paediatric Cardiac Services in Scotland
Royal College of Paediatric and Child Health (2004). Commissioning Tertiary Services and Specialised Services for Children and Young People. RCPCH, London, March 2004 Winlaw D S, Sholler G F and Harvey R P (2005) Progress and challenges in the genetics of congenital heart disease; Medical Journal of Australia. 7th February 2005, Vol 182 (3):100-101 Salzer-Muhar U, Marx N, Wimmer M (1999) “Pediatric Cardiac Extracorporeal Membrane Oxygenation in Congenital Heart Disease”: The Cardiologist’s view. Artificial Organs 1999; 23(11):995-1000 Schneider D J, Kevi D S, Serwacki M J, Moore S D, Moore J W. “Overview of interventional paediatric cardiology in 2004”; Minerva Pediatr 2004;56:1-28
Tanel RE, Walsh EP, Triedman JK, Epstein MR, Bergau DM, Saul JP (1997) Five-year experience with radiofrequency catheter ablation: implications for management of arrhythmias in paediatric and young adult patients. Journal of Paediatrics 1997 Dec; 131(6):878-87
Trulock EP et al (2003) The registry of the international society for heart and lung transplantation: twentieth official adult lung and heart-lung transplant report 2003 The Journal of Heart and Lung Transplantation 22 (6) pp 625 – 635 Woolfe et al, 1995
Wren C, Richmond S, Donaldson L (2000) Temporal variability in birth prevalence of cardiovascular malformations Heart 2000;83:414–19.
http://en.wikipedia.org/wiki/Congenital
http://www.nhlbi.nih.gov/health/dci/Disease/chd/chd_diagnosis.html
www.isdscotland.org/isd/info
- 46 -
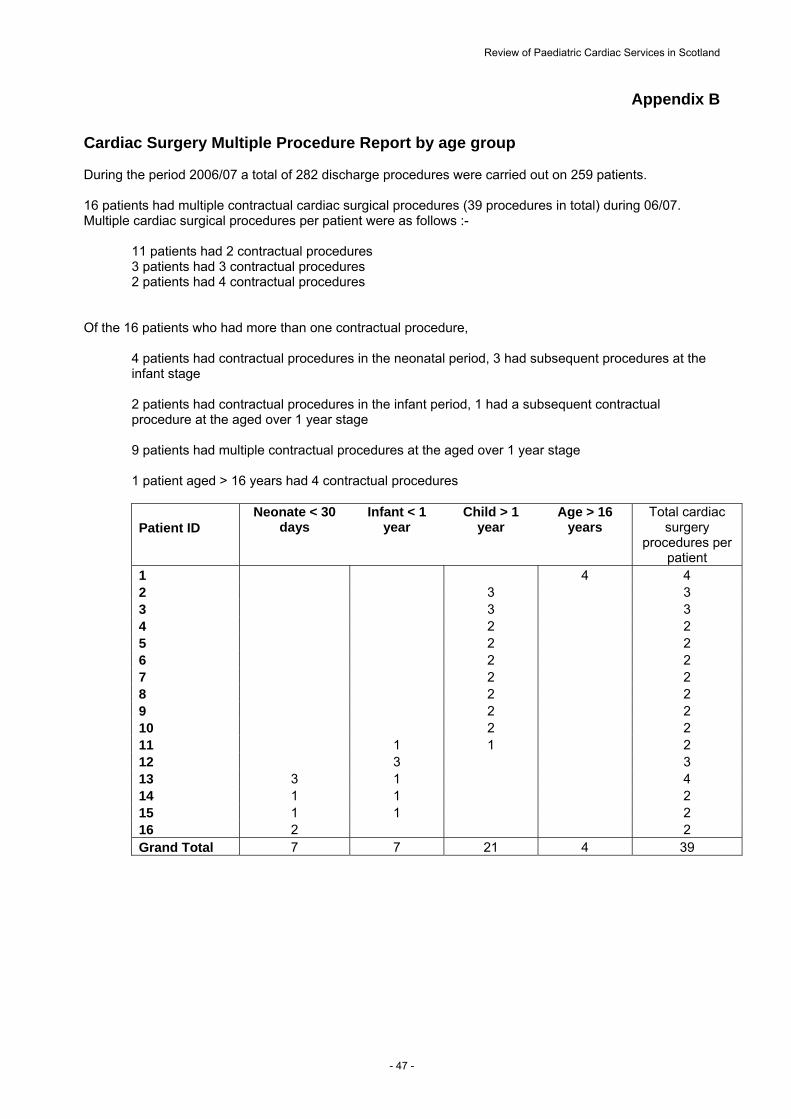
Review of Paediatric Cardiac Services in Scotland
Appendix B
Cardiac Surgery Multiple Procedure Report by age group During the period 2006/07 a total of 282 discharge procedures were carried out on 259 patients. 16 patients had multiple contractual cardiac surgical procedures (39 procedures in total) during 06/07. Multiple cardiac surgical procedures per patient were as follows :- 11 patients had 2 contractual procedures 3 patients had 3 contractual procedures 2 patients had 4 contractual procedures Of the 16 patients who had more than one contractual procedure,
4 patients had contractual procedures in the neonatal period, 3 had subsequent procedures at the infant stage 2 patients had contractual procedures in the infant period, 1 had a subsequent contractual procedure at the aged over 1 year stage 9 patients had multiple contractual procedures at the aged over 1 year stage 1 patient aged > 16 years had 4 contractual procedures
Patient ID Neonate < 30
days Infant < 1
year Child > 1
year Age > 16
years Total cardiac
surgery procedures per
patient 1 4 4 2 3 3 3 3 3 4 2 2 5 2 2 6 2 2 7 2 2 8 2 2 9 2 2 10 2 2 11 1 1 2 12 3 3 13 3 1 4 14 1 1 2 15 1 1 2 16 2 2 Grand Total 7 7 21 4 39
- 47 -
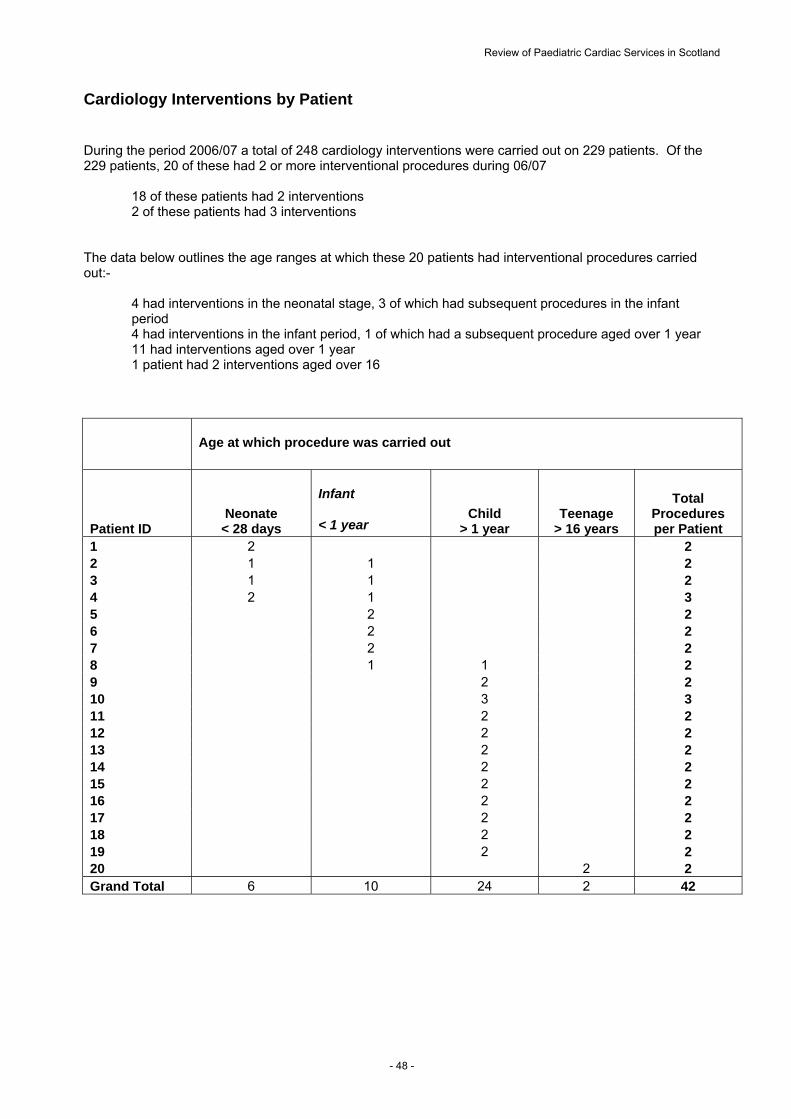
Review of Paediatric Cardiac Services in Scotland
Cardiology Interventions by Patient During the period 2006/07 a total of 248 cardiology interventions were carried out on 229 patients. Of the 229 patients, 20 of these had 2 or more interventional procedures during 06/07
18 of these patients had 2 interventions 2 of these patients had 3 interventions
The data below outlines the age ranges at which these 20 patients had interventional procedures carried out:-
4 had interventions in the neonatal stage, 3 of which had subsequent procedures in the infant period
4 had interventions in the infant period, 1 of which had a subsequent procedure aged over 1 year 11 had interventions aged over 1 year 1 patient had 2 interventions aged over 16
Age at which procedure was carried out
Patient ID Neonate
< 28 days
Infant
< 1 year Child
> 1 year Teenage
> 16 years
Total Procedures per Patient
1 2 2 2 1 1 2 3 1 1 2 4 2 1 3 5 2 2 6 2 2 7 2 2 8 1 1 2 9 2 2 10 3 3 11 2 2 12 2 2 13 2 2 14 2 2 15 2 2 16 2 2 17 2 2 18 2 2 19 2 2 20 2 2 Grand Total 6 10 24 2 42
- 48 -

Review of Paediatric Cardiac Services in Scotland
Appendix C
Paediatric Cardiac ServicesCardiac Surgery - Interventional Cardiology - Neonatal CardiologyFunded Profile 2006/07
Interventional Cardiology Cardiac Surgery
Neonatal Cardiology Total
2006/07 2006/07 2006/07 2006/07£ £ £ £
DIRECT, Fixed
NURSINGWard 2AGrade I 0 40,394 0 40,394Grade G 5,808 47,590 0 53,399Grade F 8,145 79,277 0 87,422Grade E 42,037 218,868 0 260,906Grade D 30,304 58,035 0 88,338Other 13,273 38,694 0 51,966Total Ward 2A 99,567 482,858 0 582,424
Cardiology Dept.Grade G 25,763 0 0 25,763Grade E 59,981 0 0 59,981MTO 5 10,781 0 0 10,781MTO 4 2,777 0 0 2,777MTO 3 51,207 0 0 51,207MTO 2 9,178 0 0 9,178Aide 1,397 0 0 1,397Total Cardiology Dept. 161,084 0 0 161,084
Intensive Care Grade H 0 8,915 0 8,915Grade G 0 104,448 0 104,448Grade F 0 183,839 0 183,839Grade E 0 704,447 0 704,447Grade D 0 109,742 0 109,742Grade C 0 967 0MTO 5 0 9,546 0 9,546Total Intensive Care Unit 0 1,121,904 0 1,121,904
TheatresGrade I 0 3,766 0 3,766Grade H 0 3,567 0 3,567Grade G 0 8,247 0 8,247Grade F 0 11,842 0 11,842Grade E 0 209,390 0 209,390Grade D 0 72,763 0 72,763Grade A 0 8,905 0 8,905Total Theatres 0 318,479 0 318,479
Midwifery SalariesGrade I 0 0 4,741 4,741Grade H 0 0 699 699Grade G 0 0 45,137 45,137Grade F 0 0 58,335 58,335Grade E/F 0 0 53,455 53,455Grade E 0 0 21,113 21,113Grade D 0 0 3,742 3,742Other 0 0 14,564 14,564Total Midwifery Salaries 0 0 201,786 201,786
967
TOTAL NURSING/PAM 260,651 1,923,241 201,786 2,385,678
- 49 -
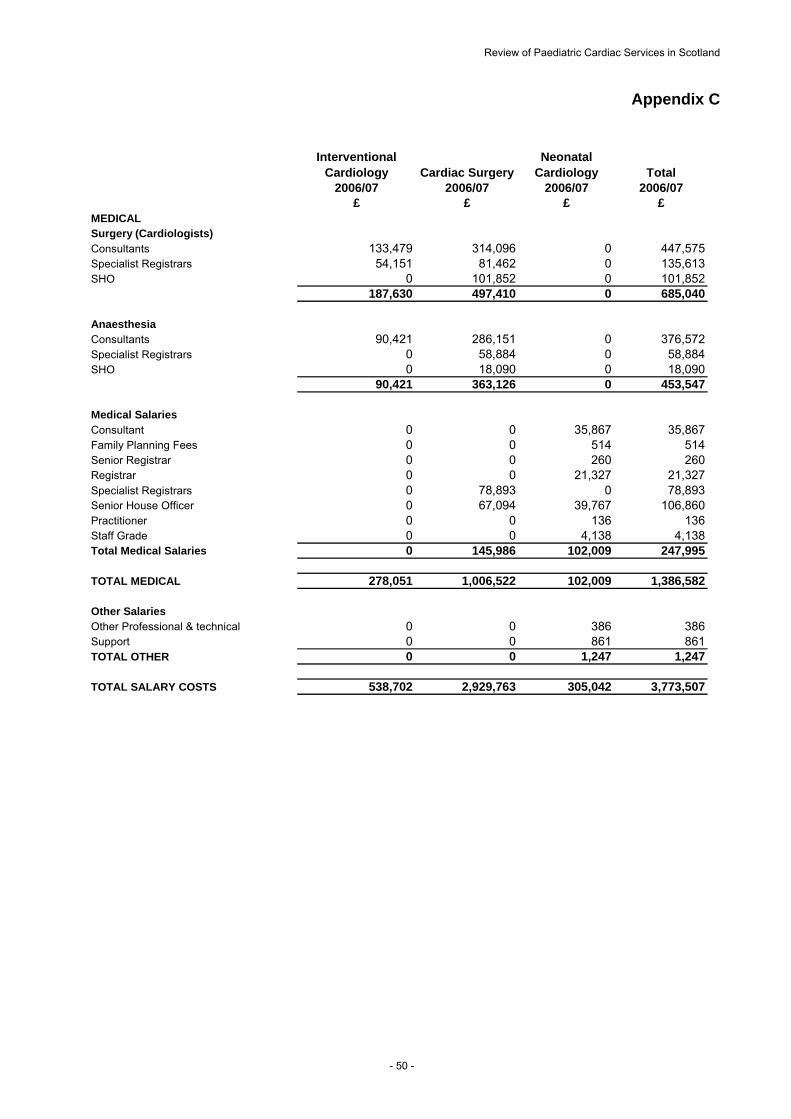
Review of Paediatric Cardiac Services in Scotland
Appendix C
Interventional Cardiology Cardiac Surgery
Neonatal Cardiology Total
2006/07 2006/07 2006/07 2006/07£ £ £ £
MEDICALSurgery (Cardiologists) Consultants 133,479 314,096 0 447,575Specialist Registrars 54,151 81,462 0 135,613SHO 0 101,852 0 101,852
187,630 497,410 0 685,040
AnaesthesiaConsultants 90,421 286,151 0 376,572Specialist Registrars 0 58,884 0 58,884SHO 0 18,090 0 18,090
90,421 363,126 0 453,547
Medical SalariesConsultant 0 0 35,867 35,867Family Planning Fees 0 0 514 514Senior Registrar 0 0 260 260Registrar 0 0 21,327 21,327Specialist Registrars 0 78,893 0 78,893Senior House Officer 0 67,094 39,767 106,860Practitioner 0 0 136 136Staff Grade 0 0 4,138 4,138Total Medical Salaries 0 145,986 102,009 247,995
TOTAL MEDICAL 278,051 1,006,522 102,009 1,386,582
Other SalariesOther Professional & technical 0 0 386 386Support 0 0 861 861TOTAL OTHER 0 0 1,247 1,247
TOTAL SALARY COSTS 538,702 2,929,763 305,042 3,773,507
- 50 -

Review of Paediatric Cardiac Services in Scotland
Appendix C
Interventional Cardiology Cardiac Surgery
Neonatal Cardiology Total
2006/07 2006/07 2006/07 2006/07£ £ £ £
OTHERDirect ward/cardiology dept 41,783 0 0 41,783Direct ward/theatre costs 0 2,922 0 2,922Pharmacy 5,075 55,440 0 60,515Bacteriology 17,194 10,413 0 27,607Haematology 6,967 14,524 0 21,491Biochemistry 3,372 28,517 0 31,889Physiotherapy 0 40,444 0 40,444Pain Control Service 0 89 0Dietetics 0 6,877 0 6,877EEG 0 5,893 0 5,893Cardiac Investigation 0 109,805 0 109,805Radiology 8,570 63,212 0 71,783Perfusionists 0 184,511 0 184,511Biochem/Cath Lab Technicians 0 27,904 0 27,904TOTAL OTHER 82,962 550,552 0 633,513
TOTAL DIRECT, Fixed 621,664 3,480,315 305,042 4,407,020
DIRECT, VariablePharmacy 368,740 0 0 368,740Ward 2A 19,921 69,551 0 89,472Cardiology Dept 194,672 0 0 194,672ICU 0 811,765 0 811,765Theatres 0 444,327 0 444,327Bacteriology 5,218 4,847 0 10,065Haematology 1,178 3,508 0 4,686Biochemistry 2,036 8,077 0 10,113EEG 0 181 0 181Cardiac Investigation 0 49,139 0 49,139Radiology 2,706 27,165 0 29,871Blood Gas Consumables 0 29,862 0 29,862Travel and training 0 0 1,840 1,840Other 0 0 1,998 1,998Equipment 0 0 7,551 7,551Drugs 0 0 11,100 11,100Dressings 0 0 855 855Instruments & Sundries 0 0 14,596 14,596CSSD/TSSU charges 0 0 1,058 1,058TOTAL DIRECT/Variable 594,471 1,448,421 38,998 2,081,891
TOTAL DIRECT 1,216,135 4,928,736 344,039 6,488,911
INDIRECT, FixedClerical/ward clerk/ess 0 4,528 0 4,528Theatre Orderlies 0 8,316 0 8,316Hotel Costs 0 56,318 0 56,318Medical Secretarial 18,873 34,318 0 53,191Database Audit Admin 0 16,045 0 16,045Database Audit Admin/DP 39,855 20,672 0 60,527Equipment maintenance 19,217 0 0 19,217General Overheads 167,119 449,412 0 616,531Clinical Support 0 0 9,987 9,987AHP Support 0 0 3,132 3,132Labs and X-Ray Support 0 0 38,339 38,339Ancillary Support 0 0 6,166 6,166Capital Charges 130,280 644,634 14,799 789,713TOTAL INDIRECT/Fixed 375,344 1,234,242 72,423 1,682,009
INDIRECT, VariableHotel Costs 19,454 36,993 0 56,446Clinical Support 0 0 22,589 22,589AHP Support 0 0 49,884 49,884Labs and X-Ray Support 0 0 10,246 10,246Ancillary Support 0 0 29,516 29,516TOTAL INDIRECT/Variable 19,454 36,993 112,236 168,682
89
- 51 -

Review of Paediatric Cardiac Services in Scotland
- 52 -
Appendix C
Interventional
Cardiology Cardiac SurgeryNeonatal
Cardiology TotalSummary Funded Profile 2006/07 2006/07 2006/07 2006/07
£ £ £ £FixedNursing/PAM 260,651 1,923,241 201,786 2,385,678Medical 278,051 1,006,522 102,009 1,386,582Other Direct 82,962 550,552 1,247 634,760Indirect, fixed 245,064 589,608 57,624 892,296Capital charges 130,280 644,634 14,799 789,713Total 997,008 4,714,557 377,465 6,089,030
Variable 613,925 1,485,414 151,233 2,250,573
Total 1,610,933 6,199,971 528,698 8,339,602
Analysis of Variable Costs06/07 06/07
Variable Total Cost/Case Cases V.C.
Interventional CardiologyBalloon Dilation 1,315 50 65,760EP 1,873 3 5,619Coil Occlusion 1,272 25 31,801Device Occlusion 7,765 42 326,122Pacemaker 6,811 11 74,924Stent 2,637 24 63,278Atrial Septostomy 597 12 7,164Ablation 2,928 10 29,284Other 434 23 9,973TOTAL 200 613,925
Cardiac SurgeryClosed simple 1,750 37 64,750Closed complex 3,166 60 189,960Open simple 5,224 11 57,464Open intermediate 7,158 80 572,640Open complex 7,800 77 600,600TOTAL 265 1,485,414
Neonatal CardiologyPharmacy 2,327 65 151,233TOTAL 65 151,233

Review of Paediatric Cardiac Services in Scotland
- 53 -
Yorkhill DivisionClinical Board of Anaesthesia and Surgery
Appendix D Monitoring of activity and costs: 2006/07
CARDIAC SURGERY
variable
Full Year Year-to-date Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total
ActivityClosed simple 4 1 3 1 1 3 2 5 1 4 2 1 28Closed complex 4 10 1 3 0 4 4 2 4 15 7 5 59Open simple 4 0 3 2 2 3 2 0 1 1 1 0 19Open intermediate 7 13 12 6 8 5 5 9 7 6 7 5 90Open complex 7 4 7 9 6 7 7 6 12 8 5 8 86Total cases 26 28 26 21 17 22 20 22 25 34 22 19 282
37 3760 6011 1180 8077 77
265 265
Variable costs £ £ £ £ £ £ £ £ £ £ £ £ £ £ £Closed simple 7,000 1,750 5,250 1,750 1,750 5,250 3,500 8,750 1,750 7,000 3,500 1,750 49,000Closed complex 12,664 31,660 3,166 9,498 0 12,664 12,664 6,332 12,664 47,490 22,162 15,830 186,794Open simple 20,896 0 15,672 10,448 10,448 15,672 10,448 0 5,224 5,224 5,224 0 99,256Open intermediate 50,106 93,054 85,896 42,948 57,264 35,790 35,790 64,422 50,106 42,948 50,106 35,790 644,220Open complex 54,600 31,200 54,600 70,200 46,800 54,600 54,600 46,800 93,600 62,400 39,000 62,400 670,800Total cost £ 145,266 £ 157,664 £ 164,584 £ 134,844 £ 116,262 £ 123,976 £ 117,002 £ 126,304 £ 163,344 £ 165,062 £ 119,992 £ 115,770 £ 1,650,070
CARDIOLOGY
64,750 64,750189,960 189,96057,464 57,464
572,640 572,640600,600 600,600
£ 1,485,414 £ 1,485,414
Full Year Year-to-date Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total
ActivityBalloon dilatation 9 5 11 4 9 14 11 3 4 5 8 5 88EP 0 0 0 0 0 0 0Coil occlusion 2 0 2 2 1 2 1 1 3 2 1 17Device occlusion 3 7 6 4 7 3 6 2 1 6 45Pacemaker 2 0 2 1 1 1 4 1 1 2 1 0 16Stent 1 0 1 2 2 2 2 1 2 0 13Atrial Septostomy 2 1 0 0 2 1 1 2 1 1 5 1 17Ablation 1 2 1 1 0 2 2 1 1 2 1 0 14Others 1 0 6 2 2 7 2 1 1 6 2 8 38Total cases 21 15 29 16 24 32 23 16 11 20 20 21 248
50 503 3
25 2542 4211 1124 2412 1210 1023 23
200 200
Variable costs £ £ £ £ £ £ £ £ £ £ £ £ £ £ £Balloon dilatation 11,835 6,575 14,465 5,260 11,835 18,410 14,465 3,945 5,260 6,575 10,520 6,575 115,720EP 0 0 0 0 0 0 0 0 0 0 0 0 0Coil occlusion 2,544 0 2,544 2,544 1,272 2,544 1,272 1,272 3,816 2,544 0 1,272 21,624Device occlusion 23,295 54,355 46,590 31,060 54,355 23,295 0 46,590 0 15,530 7,765 46,590 349,425Pacemaker 13,620 0 13,620 6,810 6,810 6,810 27,240 6,810 6,810 13,620 6,810 0 108,960Stent 2,636 0 2,636 5,272 5,272 5,272 5,272 2,636 0 0 5,272 0 34,268Atrial Septostomy 1,194 597 0 0 1,194 597 597 1,194 597 597 2,985 597 10,149Ablation 2,929 5,858 2,929 2,929 0 5,858 5,858 2,929 2,929 5,858 2,929 0 41,006Others 434 0 2,604 868 868 3,038 868 434 434 2,604 868 3,472 16,492Total cost £ 58,487 £ 67,385 £ 85,388 £ 54,743 £ 81,606 £ 65,824 £ 55,572 £ 65,810 £ 19,846 £ 47,328 £ 37,149 £ 58,506 £ 697,644
Grand Total £ 2,099,329 £ 2,099,329 £ 203,753 £ 225,049 £ 249,972 £ 189,587 £ 197,868 £ 189,800 £ 172,574 £ 192,114 £ 183,190 £ 212,390 £ 157,141 £ 174,276 £ 2,347,714
Actual
Actual
65,750 65,7505,625 5,625
31,800 31,800326,130 326,13074,910 74,91063,264 63,2647,164 7,164
29,290 29,2909,982 9,982
£ 613,915 £ 613,915
Agreement
Agreement


















