
REVIEW OF LITERATURE Introduction -...
23
Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 9 REVIEW OF LITERATURE Introduction International Diabetes federation has estimated that, in the year 2025, 330 million people worldwide will be affected by diabetes mellitus (Zimmet P 2001) and it’s believed that India will be the Diabetic Capital of the world. If these predictions come true, it would create a major burden on the worlds’ healthcare budget for diabetes, which is predicted to bounce from 5% to 40%. Diabetic patients fall mainly into two categories: type 1 and type 2 diabetes (DeFronzo RA 2004). Type 1 diabetes (T1D) is a disease resulting from a cell-mediated autoimmune attack against pancreatic insulin-producing β-cells. It is characterized by insulin insufficiency, blood glucose dysregulation, persistent hyperglycemia, and long-term complications. According to its process of development, islet-specific autoimmunity leads to β-cell damage which in turn results in insulin insufficiency. There are three conventional therapeutic options used for treating T1D which are currently available: insulin therapy, cell-based therapy and immunotherapy (Powers 2008.). Insulin therapy is typically the most common and widely used therapy to treat T1D. The discovery of insulin revolutionized T1D therapy and made this incurable and debilitating disease manageable, saving thousands of lives since its discovery nearly one century ago. However, insulin therapy for treatment of T1D is passive in nature and does not directly address the cause of the disease. It is now well established that the risk of diabetic complications is dependant on the degree of glycemic control in diabetic patients. Clinical trials such as the Diabetes Control and Complications Trial (DCCT) (Group 1993), the UK prospective Diabetes Study (UKPDS) (Group 1998), and Kumamato study (Ohkubo Y 1995) have demonstrated that tight glycemic control achieved with intensive insulin regimens can reduce the risk of developing or progressing retinopathy, nephropathy or neuropathy in patients with all types of diabetes. However, the Third National Health and Nutrition Examination Survey (NHANES III) showed that only 50% of diabetics have been able to achieve Hba1C level of less than 7%; therefore, the only way to ensure the long term health of diabetic patients is to maintain constant normoglycemia. Despite intensive insulin therapy, however, most individuals with type 1 diabetes are unable to maintain a blood glucose level in the normal range at all times. Moreover, intensive glycemic control with insulin therapy is associated with an increased incidence of hypoglycemia, which is the major barrier to the implementation of intensive treatment from the perspective of both physicians and patients.
Transcript of REVIEW OF LITERATURE Introduction -...

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 9
REVIEW OF LITERATURE Introduction
International Diabetes federation has estimated that, in the year 2025, 330 million people
worldwide will be affected by diabetes mellitus (Zimmet P 2001) and it’s believed that India
will be the Diabetic Capital of the world. If these predictions come true, it would create a
major burden on the worlds’ healthcare budget for diabetes, which is predicted to bounce
from 5% to 40%.
Diabetic patients fall mainly into two categories: type 1 and type 2 diabetes (DeFronzo RA
2004). Type 1 diabetes (T1D) is a disease resulting from a cell-mediated autoimmune attack
against pancreatic insulin-producing β-cells. It is characterized by insulin insufficiency, blood
glucose dysregulation, persistent hyperglycemia, and long-term complications. According to
its process of development, islet-specific autoimmunity leads to β-cell damage which in turn
results in insulin insufficiency. There are three conventional therapeutic options used for
treating T1D which are currently available: insulin therapy, cell-based therapy and
immunotherapy (Powers 2008.). Insulin therapy is typically the most common and widely
used therapy to treat T1D. The discovery of insulin revolutionized T1D therapy and made
this incurable and debilitating disease manageable, saving thousands of lives since its
discovery nearly one century ago. However, insulin therapy for treatment of T1D is passive
in nature and does not directly address the cause of the disease. It is now well established
that the risk of diabetic complications is dependant on the degree of glycemic control in
diabetic patients. Clinical trials such as the Diabetes Control and Complications Trial
(DCCT) (Group 1993), the UK prospective Diabetes Study (UKPDS) (Group 1998), and
Kumamato study (Ohkubo Y 1995) have demonstrated that tight glycemic control achieved
with intensive insulin regimens can reduce the risk of developing or progressing retinopathy,
nephropathy or neuropathy in patients with all types of diabetes. However, the Third
National Health and Nutrition Examination Survey (NHANES III) showed that only 50% of
diabetics have been able to achieve Hba1C level of less than 7%; therefore, the only way to
ensure the long term health of diabetic patients is to maintain constant normoglycemia.
Despite intensive insulin therapy, however, most individuals with type 1 diabetes are unable
to maintain a blood glucose level in the normal range at all times. Moreover, intensive
glycemic control with insulin therapy is associated with an increased incidence of
hypoglycemia, which is the major barrier to the implementation of intensive treatment from
the perspective of both physicians and patients.

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 10
Type 2 diabetes presents a more complex etiology that affects 95% of the diabetic patients.
The pathology occurs mainly at adult ages and is often associated with genetic
predisposition as well as obesity due to an unbalanced diet and a sedentary lifestyle
(Zimmet P 2001; DeFronzo RA 2004). The disease progresses from insulin resistance to
glucose intolerance and subsequently β-cell death by apoptotic mechanisms. Type 2
diabetes is treated initially by oral hypoglycemic agents, and typically with adjunct insulin
therapy in the later stages of the disease. Indeed, it is now well accepted that the β-cell
mass is decreased by about 50% in type 2 diabetes (Donath 2004). Replacing the missing
cells could be a means to treat the insulin delivery malfunction of this form of the disease.
Although a higher percentage of diabetic patients are classified as type 2 diabetics, the
increase in incidence of T1D has been surprisingly high in the recent decade (Onkamo 1999;
Wild 2004). In some countries, such as the UK and China, the increase in the incidence rate
has reached over 70% per year in children aged less than 14 years (Devendra 2004),
pushing for more fundamentally curative solutions to be intensively investigated.
(Limbert 2008)
The successes achieved over the last few decades by the transplantation of whole pancreas
and isolated islets suggest that diabetes can be cured by the replenishment of deficient β-
cells. The mature pancreas has two functional compartments: the exocrine portion (99%),
including acinar and duct cells, implicated in nutrient digestion to facilitate absorption in the
gut, and the endocrine portion (1%), including the islets of Langerhans. Islets are composed
of four cell types that synthesize and secrete distinct peptidic hormones: insulin (β-cells),

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 11
glucagon (α-cells), somatostatin (δ-cells), and pancreatic polypeptide (PP-cells). β-cells
represent approximately 60–80% of the whole islet.
Figure I: Human pancreas and islets in culture.
a. Pancreas and islet transplantation
It seems logical that replacement of the islet tissue itself offers a better approach than simply
replacing insulin that has been lost. However, whole pancreas transplantation still faces
technical obstacles such as immune rejection, appropriate blood supply to the allograft and
the risk of activating the digestive enzymes of the exocrine portion. Interestingly, islet
transplantation partially overcomes some of these problems, although this technology is still
far from being a successful alternative. In this sense, several obstacles remain, such as the
diabetogenic effects of some immunosuppressants (Roche E 2005), the establishment of an
appropriate immunosuppressive therapy (Ryan EA 2005), and the scarcity of human donor
pancreas (Roche E 2005).
The clinical trial known as the Edmonton Protocol tried to solve some of these issues by
introducing key important variants (Shapiro AM 2000), such as intraportal infusion of a
correct number of freshly isolated islets, and the use of non-diabetogenic
immunosuppressive agents. Following this protocol, insulin independence with tight
glycemic control was achieved in patients for up to 1year. The longest (over 11 years) case
of insulin independence after allogeneic islet transplantation was recently reported (Berney

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 12
2009), and several such cases in the near future will reach the symbolic 10-year mark. More
than 500 type 1 diabetics in more than 50 institutions have undergone islet transplantation
by using the Edmonton protocol, to cure their disease; however, the clinical benefit of this
protocol can be provided only to a small minority of patients (only 31% and 10% of patients
remained insulin independent at 2 years and 5 years respectively) and recipient immune
response limits implant survival to 3–5 years, indicating that improvements are still
necessary (Robertson 2004; Ryan EA 2005). Moreover, the number of islets required to
achieve independence from insulin injections is very high and resources of human donor
organs to provide islet grafts are limited. About 850,000 (11,000 islet equivalent/kg body
weight) islets are required to achieve successful transplantation outcomes with the
Edmonton protocol.
Figure II: Cadaveric islet transplantation in the hepatic portal vein. Adapted from Nature Reviews.
At present, the only suitable source of human islets for clinical use is from pancreases of
heart-beating, brain-dead donors. This type of organ donor is rare, so current protocols for
human islet transplantation are unlikely to make a widespread therapeutic impact on T1DM,
with 105 potential recipients in the UK and 106 in the USA. This clinical need is therefore
driving research into alternative sources of functionally competent, insulin-secreting β-cells
as substitutes for donor islets in transplantation therapy. Although still highly experimental,

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 13
various cellular sources for physiologically regulated insulin production have been proposed
including stem cells, xenogenic islets, cells grown in vitro from mature islets, and cells
“transdifferentiated” from various cell sources.
b. Alternative sources of islets from mammalian and non mammalian hosts (xenotransplantation)
Mammalian source: Using islets of Langerhans from other species is an obvious way of
providing the large amounts of functional tissue required for transplantation therapy of
diabetes. Pigs have been particularly attractive as a potential islet source because:
(i) Western countries have pre-existing facilities for high-throughput breeding (have
large litters, which grow quickly to adult size), rearing and slaughtering of pigs
(porcine pancreas as a byproduct of pork production was a source of insulin for
treating T1DM for many years before recombinant human insulin became widely
available);
(ii) display regulated insulin secretion similar to that of humans;
(iii) high islet yields can be obtained from porcine pancreas using techniques similar
to those for human islet isolation; and
(iv) pigs are amenable to genetic modification to make human insulin or to protect
against immune assault.
Clinical trials performed, most notably by Groth et al (Groth, Korsgren et al. 1994), in which
fetal porcine islets were infused into the portal vein or in the renal capsule of diabetic
patients, did not reverse diabetes, but resulted in detectable porcine C peptide levels.
Valdes-Gonzalez et al reported a series of patients given a mixture of neonatal porcine islets
and Sertoli cells within abdominal subcutaneous membrane sheaths. In that report, a few
patients achieved temporary insulin independence with no immunosuppression (Valdes-
Gonzalez, Dorantes et al. 2005).
Two important impediments have however restricted the widespread use of pig islets in
humans. First, the hyperimmune response to xenografts has proved difficult to avoid.
Numerous attempts to hide the transplanted xenografts from the host immune system by
islet encapsulation have largely failed to maintain islet viability and insulin secretory
responses over prolonged periods required of transplanted islets. Progress that may
overcome the first problem has been made. Humans rapidly reject pig tissue (hyperacute
rejection) because of higher titer antibodies against galactose α(1,3)galactose, a
carbohydrate residue expressed on porcine cells. With advances in animal cloning, a
genetically modified pig that does not express the residue is under investigation (Kolber-

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 14
Simonds, Lai et al. 2004). In a proof-of-concept study, T-cell targeted immunosuppressive
therapy enabled the use of unmodified pig islets to reverse experimental diabetes in non-
human primates for prolonged periods (Hering, Wijkstrom et al. 2006).
Second, the demonstration that porcine endogenous retroviral (PERV) sequences in the
porcine DNA may become activated on xenotransplantation. Van der Laan et al (van der
Laan, Lockey et al. 2000) raised the possibility of novel viral infections in humans receiving
porcine islet implants. However, recent work has suggested that the potential threat of
PERVs to xenotransplant recipients may have been over-estimated, because prolonged
immunosuppression and exposure to porcine islet xenografts caused no detectable
transmission of PERVs in vitro or in vivo studies (Denner, Specke et al. 2008; Irgang, Laue
et al. 2008).
Non-mammalian source: Teleost fish islet tissue has emerged as an intriguing alternative
to the use of islet tissue from mammalian pancreases. The islet tissue, called Brockman
bodies (BBs), is anatomically distinct from the pancreatic exocrine tissue and can be easily
identified and isolated. Islets harvested from Nile tilapia (Oreochromis niloticus), when
transplanted into streptozotocin-diabetic nude mice, produce long-term normoglycemia and
achieve mammalian-like glucose tolerance profiles. Unlike the porcine islets, BBs function
immediately after transplantation; thus, their rejection can be assessed on the basis of loss
of function as well as other parameters (Wright, Pohajdak et al. 2004). Additionally, tilapia
are potentially ideal xenogeneic donors because of markedly lower donor production costs,
minimal islet procurement costs, and possibly decreased xenozoonotic potential relative to
mammalian donors. Tilapia islets appear to be appropriately glucose responsive with high
insulin output, can be cryopreserved, and are much more resistant to hypoxia than
mammalian islets (Wright and Pohajdak 2001). Further more, tilapia BBs are also devoid of
alpha-gal expression, and may offer an alternative to swine as a donor species for islet
xenotransplantation (Leventhal, Sun et al. 2004).
The commercial and clinical potential of pig islets and tilapia BBs, as source of transplant
material for treating T1DM seems likely to drive larger, more rigorous and more carefully
controlled clinical trials, and the outcome of those trials will determine whether these
xenogenic islets are a realistic functional substitute for human islets. The concept of islet
xenografts has been around for many years without making much progress, but recent
events suggest that this is an area worth watching.

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 15
c. Regeneration of β-cell mass through expansion of β-cells and transdifferentiation of ductal cells and Islet neogenesis from stem cells.
The adult endocrine pancreas has for a long time been considered a quiescent cell
population. Recent studies have shown that, like most tissues, β-cell mass is dynamically
regulated (Bonner-Weir 2000; Butler 2003). The interplay of cell expansion and reduction
mechanisms determines the amount of the β-cell mass. Expansion can occur through β-cell
hypertrophy, proliferation (self-replication) and neogenesis (differentiation of progenitor cells
into new β-cells). Conversely, reduction can result from β-cell atrophy, death, or loss of
phenotypic stability (Lipsett 2006). Thus, the development of strategies to avoid β-cell mass
reduction or to enhance β-cell mass expansion, both in vivo and in vitro, could prove a
promising option for cell-based therapy of type 1 and type 2 diabetes. Regeneration of β-cell mass: β-cells are most abundant lineage in the islets, and are
generally believed to undergo slow, continual turnover in the adult pancreas. The β-cell
mass increases during pre- and neonatal life as well in pregnancy and obesity in humans
and rodents, but the rate of proliferation declines dramatically with age (Bouwens L 2005).
The origin(s) of these new β-cells is important when considering how to expand the β-cell
mass in or ex vivo. Recent lineage tracing studies in mice suggest that, under most
circumstances including acute pancreatic regeneration, new β-cells arise by a slow but
uniform self-renewal of existing β-cells (Dor 2004; Teta 2007). A recent study of β-cell
proliferation suggested that, unlike rodent β-cells, adult human β-cells are largely non-
proliferative in vitro (Parnaud 2008), although this has been questioned by another study that
suggested the de-differentiation of human β-cells into proliferative ‘progenitor’ cells in vitro
(Russ 2008). β-cells of cultured islets can dedifferentiate, expand and can then be directed
to redifferentiate back toward a β-cell phenotype. The change resembles the process of
epithelial-mesenchymal transition (EMT) (Gershengorn, Hardikar et al. 2004). As the cells
expand from cultured human islet preparations, they develop a serpiginous appeareance
and express nestin and mesenchymal marker vimentin, but not islet hormones (Zulewski
2001; Linning, Tai et al. 2004). However, they are not completely mesenchymal, because
they continue to express endodermal proteins such as amylase, carbonic anhydrase II and
albumin (Linning, Tai et al. 2004). Multiple passages were achieved in all the studies
suggesting that the β-cells were capable of self-renewal. A variety of maneuvers were used
to force redifferentiation, including serum free media, nicotinamide, glucagon like-peptide1
(GLP-1)/exendin-4, activin A, betacellulin, hepatocyte growth factor, Ly294002 (an inhibitor
of PI3-kinase), and aggregation of cells, which led to the expression of an assortment of islet
Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 16
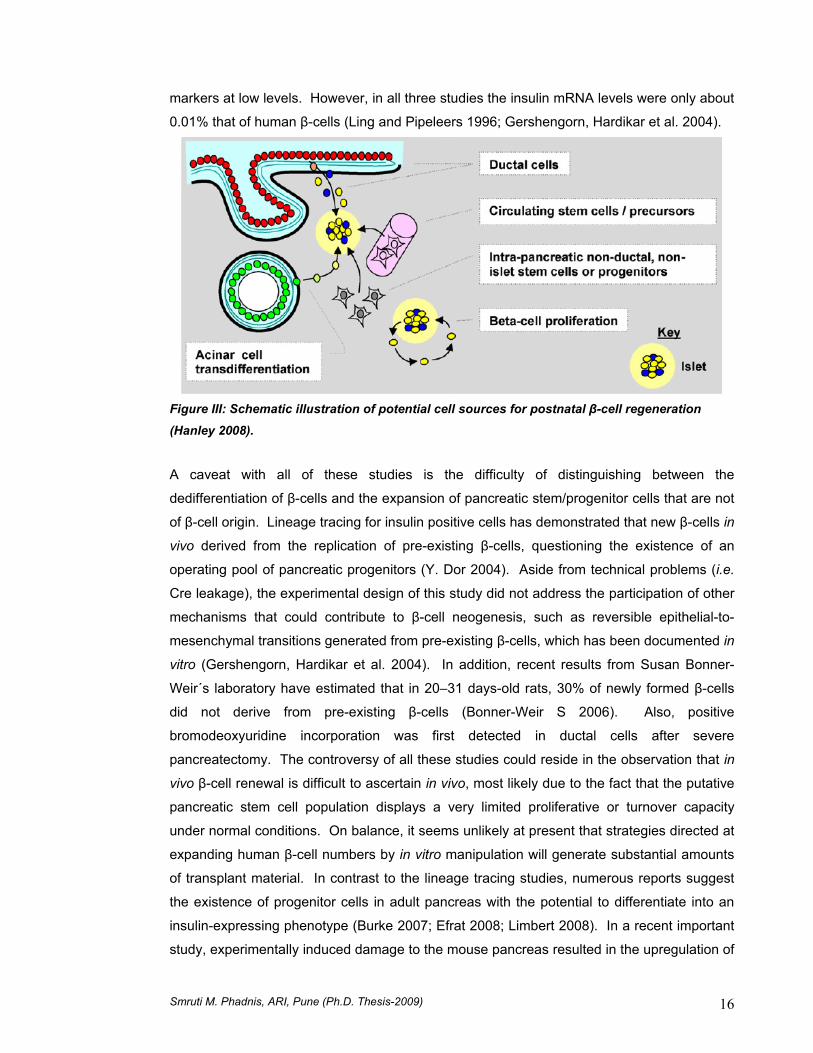
markers at low levels. However, in all three studies the insulin mRNA levels were only about
0.01% that of human β-cells (Ling and Pipeleers 1996; Gershengorn, Hardikar et al. 2004).
Figure III: Schematic illustration of potential cell sources for postnatal β-cell regeneration
(Hanley 2008).
A caveat with all of these studies is the difficulty of distinguishing between the
dedifferentiation of β-cells and the expansion of pancreatic stem/progenitor cells that are not
of β-cell origin. Lineage tracing for insulin positive cells has demonstrated that new β-cells in
vivo derived from the replication of pre-existing β-cells, questioning the existence of an
operating pool of pancreatic progenitors (Y. Dor 2004). Aside from technical problems (i.e.
Cre leakage), the experimental design of this study did not address the participation of other
mechanisms that could contribute to β-cell neogenesis, such as reversible epithelial-to-
mesenchymal transitions generated from pre-existing β-cells, which has been documented in
vitro (Gershengorn, Hardikar et al. 2004). In addition, recent results from Susan Bonner-
Weir´s laboratory have estimated that in 20–31 days-old rats, 30% of newly formed β-cells
did not derive from pre-existing β-cells (Bonner-Weir S 2006). Also, positive
bromodeoxyuridine incorporation was first detected in ductal cells after severe
pancreatectomy. The controversy of all these studies could reside in the observation that in
vivo β-cell renewal is difficult to ascertain in vivo, most likely due to the fact that the putative
pancreatic stem cell population displays a very limited proliferative or turnover capacity
under normal conditions. On balance, it seems unlikely at present that strategies directed at
expanding human β-cell numbers by in vitro manipulation will generate substantial amounts
of transplant material. In contrast to the lineage tracing studies, numerous reports suggest
the existence of progenitor cells in adult pancreas with the potential to differentiate into an
insulin-expressing phenotype (Burke 2007; Efrat 2008; Limbert 2008). In a recent important
study, experimentally induced damage to the mouse pancreas resulted in the upregulation of

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 17
progenitor cells with the capacity to differentiate into different islet endocrine cells, indicative
of the existence of multipotent pancreatic progenitor cells (Xu 2008). Putative progenitor
cells have been localized previously to the exocrine pancreas (Zhao 2007; Efrat 2008), to
pancreatic ducts (Bonner-Weir S 2000; Yatoh 2007) and to endocrine islets (Zulewski 2001;
Davani, Ikonomou et al. 2007), suggesting a widespread distribution throughout the
pancreas. The prospect of isolating, expanding, and differentiating adult pancreatic
progenitor cells to a β-cell phenotype has obvious therapeutic potential, but at present, the
precise identity of these cells remains elusive. Few studies have employed lineage-tracing
techniques to demonstrate progenitor to β-cell progression, and the ex vivo proliferative
capacity of progenitor populations isolated from human pancreas remains to be
demonstrated.
Islet neogenesis from the ductal epithelium: Islet neogenesis, the budding of new islets
from pancreatic stem/progenitor cells located in or near ducts has long been assumed to be
an active process in the postnatal pancreas. Ninety percent partial pancreatectomy is a well
established murine model, in which regeneration occurs by two pathways: replication of
preexisting endocrine or exocrine cells, and proliferation of ductules and their subsequent
differentiation into whole new lobes of pancreas that become indistinguishable from pre-
existing ones. As the duct cells replicate, they transiently express the protein Pdx-1, a
transcription factor expressed widely in the embryonic pancreatic progenitors, but by birth
restricted to β and δ cells. Pancreatic ductal epithelial cells with rapid replication, transiently
assume a less differentiated, and less restricted, phenotype that can redifferentiate into new
islets and acini (Bonner-Weir, Toschi et al. 2004). Such plasticity results in the possibility of
abundant multipotent progenitors in adult pancreatic ducts that participate in natural renewal,
a process that could be enhanced by pharmacological intervention. Several in vitro studies
have also shown that insulin-producing cells can be generated from adult pancreatic ductal
tissues (Bonner-Weir 2000; Noguchi 2003). Bonner-Weir et al. cultured human adult ductal
tissue with matrigel and observed the formation of islet like buds consisting of cytokeratin 19
(CK-19) positive duct cells and insulin positive cells (Bonner-Weir 2000). Gao et al. showed
that serum-free media, supplemented with nicotinamide along with matrigel were absolute
requirements for differentiation (Gao, Ustinov et al. 2003). Using human islet preparations
that include both duct and acinar cells, Suarez-Pinzon et al. reported a doubling of β-cells
after 4 weeks of treatment with combination of epidermal growth factor (EGF) and gastrin
(Suarez-Pinzon, Lakey et al. 2005; Suarez-Pinzon, Yan et al. 2005). They also observed
increases in the number of cells expressing the duct marker CK-19 and the transcription
factor PDX-1, suggesting that the increase in β-cell number was due to activation of
neogenesis from the pancreatic ducts. Although these studies support the idea that duct

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 18
cells can serve as progenitor cells, conclusive evidence for this supposition will require
lineage tracing.
Assessment of 83 human islet grafts transplanted using the Edmonton Protocol since 1999
was reported (Street 2004). A significant positive correlation was observed between the
number of islet progenitor (ductal-epithelial) cells transplanted and long term metabolic
success as assessed by intravenous glucose tolerance test at approximately 2 years post
transplantation. The data showed that the presence of ductal cells in clinical islet
transplantation may improve the long term metabolic outcome.
Stem cells as a source of substitute β-cells: Stem cells are undifferentiated cells capable
of sustained proliferation ‘self-renewal’ and, when induced, differentiation by means of
asymmetric cell division. Stem cells that are able to differentiate into all embryonic cell types
(including trophectoderm) and adult cell types are termed totipotent. In mammals, only the
fertilized egg and cells of the early blastomere are known to be totipotent. Embryonic stem
cells (ESCs), derived from the blastocysts’ inner cell mass, and embryonic germ (EG) cells,
derived from the germinal ridge of early fetal tissue, are capable of forming any type of tissue
in the adult and are therefore termed pluripotent. Observations of the regenerative potential
of adult tissues have led to the concept of adult stem cells. In general, adult stem cells
appear to be multipotent, but restricted in their ability to differentiate into cell types of a single
tissue (Wagers, Sherwood et al. 2002). It has been suggested, however, that pluripotent
stem cells may be present in adult bone marrow (Jiang 2002).
Figure IV: Sources of Stem cells.
Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 19
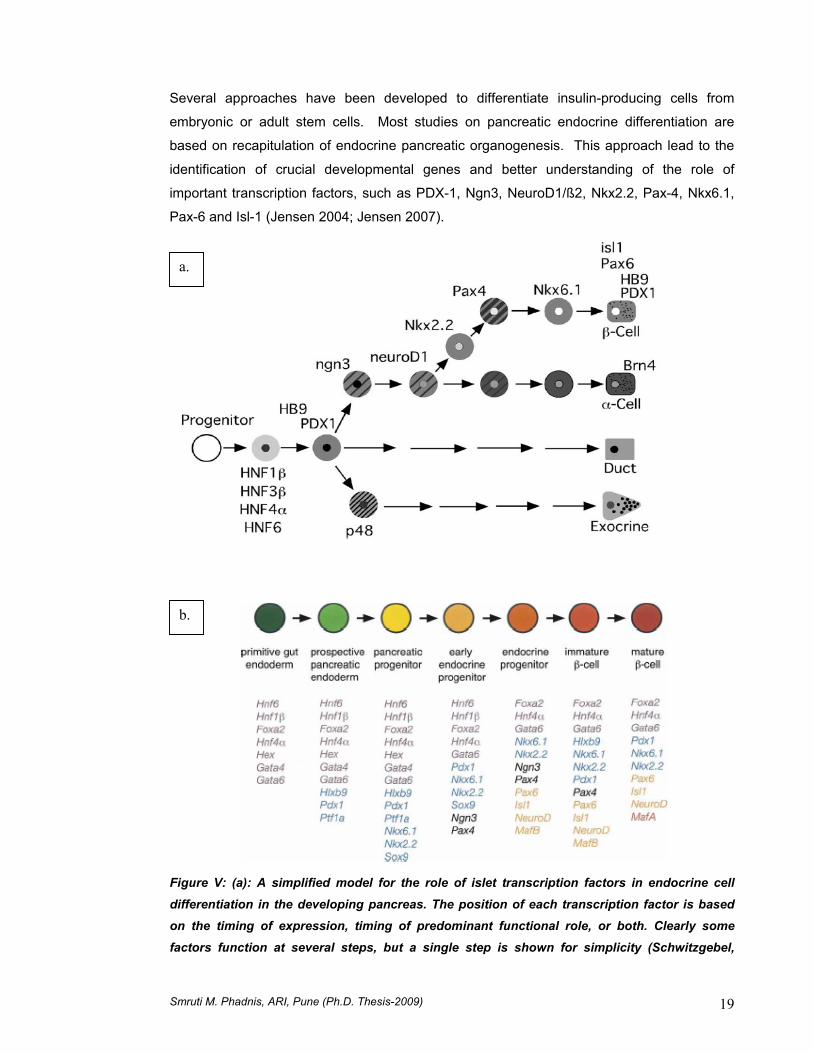
Several approaches have been developed to differentiate insulin-producing cells from
embryonic or adult stem cells. Most studies on pancreatic endocrine differentiation are
based on recapitulation of endocrine pancreatic organogenesis. This approach lead to the
identification of crucial developmental genes and better understanding of the role of
important transcription factors, such as PDX-1, Ngn3, NeuroD1/ß2, Nkx2.2, Pax-4, Nkx6.1,
Pax-6 and Isl-1 (Jensen 2004; Jensen 2007).
Figure V: (a): A simplified model for the role of islet transcription factors in endocrine cell
differentiation in the developing pancreas. The position of each transcription factor is based on the timing of expression, timing of predominant functional role, or both. Clearly some
factors function at several steps, but a single step is shown for simplicity (Schwitzgebel,
a.
b.

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 20
Scheel et al. 2000). (b): Transcription factor profile during stages of β-cell formation from endodermal derivatives. Factors initially expressed at a particular stage are colour-coded as
follows: gut endoderm (purple), pancreatic endoderm progenitor (blue), early endocrine progenitor (black), endocrine progenitor (orange), β-cell (red) (Oliver-Krasinski 2008).
The model shown in figure Va clearly reduces the complicated relationships between the
islet transcription factors to an overly simplistic outline, and it provides a starting point for
thinking about how the gene expression program evolves as cells move from multipotent
endodermal progenitors to mature pancreatic cells. The model also provides testable
hypotheses regarding the relative positions of individual transcription factors within the
different lineages (Wilson 2003). The insights into the mechanisms that control the
generation of pancreatic cells during development can eventually be applicable to the
development of strategies for tissue regeneration and for replacing the β-cells either by stem
cell sources, ES cells, or adult pancreatic tissue in diabetic individuals.
Insulin presence in the final cell population does not mean that the differentiation protocol
has been completed. In addition to hormone production, the resulting cell also has to
express functional groups of proteins that are necessary to mimic correct β-cell function and
reverse diabetes in transplanted animal models. These groups of proteins include the
glucose-sensing machinery, the exocytotic apparatus, and the insulin processing pathway.
The glucose-sensing machinery is responsible for the detection of extracellular glucose
changes and transmits this information to the secretory and insulin biosynthetic pathways
(Prentki 1996). This sensing system uses key metabolic pathways that present some
special features in pancreatic β-cells. Glucose enters in the β-cell through the glucose
transporter GLUT1 (humans) or GLUT2 (rodents), and is quickly metabolized by glucokinase
(GK), entering the glycolytic pathway and yielding pyruvate (Prentki 1996; Rolland,
Winderickx et al. 2001). This metabolite fuels mitochondria, increasing the activity of the
Krebs cycle and favoring the rise of ATP levels, which immediately produces the closure of
the ATP-dependent potassium channels (KATP) located on the plasma membrane. The
resulting depolarization contributes to the opening of voltage-dependent L-type calcium
channels and allows extracellular Ca2+ to enter and activate specific sensors of the secretory
vesicles (Yang, Larsson et al. 1999; Henquin 2000). Lastly, insulin, as many secreted
proteins in eukaryotic cells, results from a complex processing pathway which starts at the
rough endoplasmic reticulum (RER) and ends at the Golgi complex. Translation of insulin
mRNA yields prepro-insulin, which is sequentially, cleaved by endoproteinases PC1 and
PC2 to give pro-insulin first and mature insulin + C-peptide second, before packaging into
secretory vesicles. In the secretory granule, 6 insulin molecules are coordinated by a Zn

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 21
atom, which is evidenced under microscopy by DTZ staining. Although substantial progress
has been made in this field over the last 6 years, the definite protocol to in vitro production of
functional β-cells is still to be found. Moreover, additional problems need to be solved
before finding a clinical application of this technology, mainly concerning immune rejection
and tumor formation.
Figure VI: Signal transduction in b-cell: b-cells have complex mechanisms to enable them to respond to multiple external cues (nutrient and non-nutrient) and secrete the appropriate
amount of insulin to maintain blood glucose within a narrow range (5–8 mM). Briefly, glucose is transported into b-cells on the high capacity GLUT2 transporter and metabolised within the
cell, generating ATP which binds to ATP-sensitive K+-channels (KATP), leading to closure of the channels. The consequent inhibition of K+ efflux leads to b-cell plasma membrane depolarisation and opening of voltage-operated Ca2+ channels. Extracellular Ca2+ enters b-
cells resulting in elevations in intracellular Ca2+, activation of Ca2+-sensitive downstream signalling pathways and initiation of insulin secretion. Insulin secretion is also stimulated by
ligands such as acetylcholine (ACh) and cholecystokinin (CCK) acting at cell surface receptors linked to IP3 and DAG generation and those such as glucose-dependent insulinotropic peptide
(GIP) and glucagon, which elevate intracellular cyclic AMP (Jones, Courtney et al. 2008).
Embryonic stem cells: Embryonic stem cells (ESC) are highly proliferative and pluripotent
cells which have recently received much more attention in the field of cell-based therapy.
Derived from the inner cell mass of the early developing embryo, ESCs are capable of
undergoing multilineage differentiation into highly specialized cells representing all three
germinal layers (Raikwar and Zavazava 2009). Owing to their properties of self-renewal and
pluripotency, ESCs hold great potential to be an unlimited source for targeted therapies and

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 22
regenerative medicine especially for T1D. Soria et al. (Soria, Andreu et al. 2000; Soria,
Roche et al. 2000) reported the first successful generation of insulin-producing cells from
mouse ESCs in 2000. They developed an insulin-secreting cell clone from undifferentiated
ESCs using a cell-trapping system and found that these cells were able to restore
normoglycemia and normal body weight following implantation in STZ-induced diabetic mice.
In the following year, Lumelsky et al. (Lumelsky, Blondel et al. 2001) described the
generation of insulin secreting structures similar to pancreatic islets from mouse ESCs
through a five-step protocol. Several approaches have been used to obtain enriched
populations: selection by manipulating culture conditions (Lumelsky, Blondel et al. 2001;
Hori, Rulifson et al. 2002; Kahan, Jacobson et al. 2003; Segev, Fishman et al. 2004);
overexpression of key transcription factors such as paired box gene 4 (Pax4) and the
pancreatic and duodenal homeobox factor-1 (PDX-1) (Blyszczuk, Czyz et al. 2003;
Blyszczuk, Asbrand et al. 2004; Miyazaki, Yamato et al. 2004); and cell trapping with
antibiotic resistance driven by the Nkx6.1 or insulin promoter to select cells (Soria, Roche et
al. 2000; Leon-Quinto, Jones et al. 2004). In particular, the selection of ES cells expressing
nestin, an intermediate filament protein thought to be a marker of neuronal stem cells, has
been used to obtain insulin-producing cells efficiently in several articles (Lumelsky, Blondel
et al. 2001; Hori, Rulifson et al. 2002; Blyszczuk, Asbrand et al. 2004; Miyazaki, Yamato et
al. 2004). Despite reports that ESCs can be differentiated into cells capable of insulin
expression; there is considerable controversy as to whether the data is sufficiently robust to
infer successful β-cell differentiation. It is worth noting that many of the insulin-positive cells
in ESC cultures may be the product of insulin uptake from culture medium instead of
endogenous synthesis (Rajagopal, Anderson et al. 2003; Hansson, Tonning et al. 2004).
During last few years, the procedures for β-cell-like differentiation from ESCs in vitro are
getting more feasible and controllable (Shi 2005), and in vitro derivations of functional
insulin-producing cells from human ESCs has been reported from many research institutes
by formation of early stages of endoderm differentiation (D'Amour, Bang et al. 2006; Jiang,
Au et al. 2007; Jiang 2007; Kroon, Martinson et al. 2008). Despite significant improvements
in the currently available ES cell differentiation protocols, the final yield of IPCs are still very
low (≤1% of the final heterogeneous cell population). Thus, for ES cells to become a
potential source of IPCs that can be used clinically, significantly improved and novel
protocols need to be developed. In addition, the amount of insulin produced by each IPC
compared to that produced by a single islet appears to be less than a tenth of matured
functional islets and also has low glucose responsiveness. Also there is an urgent need to
develop new feeder-free human ES cell lines. The currently available human ES cell lines
have been generated and cultivated on mouse embryonic feeders and require serum of

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 23
bovine origin, which poses a significant risk in terms of zoonotic transmission of viral
diseases. Thus, it is highly desirable to optimize feeder-free and serum-free cultivation of
human ES cells. Nevertheless, even with success in differentiating ESCs into β-cells, a
persistent concern of ESC transplantation is the oncogenic potential of the undifferentiated
ESCs, and the risks of malignant transformation must be carefully considered prior to its
clinical application. In addition, the issue of the immunogenicity of β-cells differentiated from
allogeneic ESCs remains unresolved. The ethical issue is another major obstacle to the
clinical use of ES cells.
Adult Stem cells: Adult stem cells (ASCs) found within tissues of the adult organism could
serve as an alternative to ESCs for the generation of insulin-producing cells. Although they
possess a limited proliferation potential as well as commitment to specific cell fates, ASCs
offer the advantage of autologous transplantation, thereby circumventing the immune
rejection dilemma. Recent data support the plasticity of these cells to differentiate to
alternative cell fates beyond those derived from their natural body niches. This means that a
broad spectrum of ASCs could be differentiated in vitro or in vivo to insulin-producing cells.
Figure VII: Schematic diagram representing an overview of reported in vitro results of tissue
and organ differentiation capacity (Limbert 2008).
Adult stem cells from the endoderm precursors: intestine, liver, and pancreas During embryonic development, the pancreas initially is separated into two independent
buds, the dorsal and ventral buds, which eventually fuse. The ventral primordium develops
from the endoderm of the hepatic diverticulum, whereas the dorsal primordium derives from

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 24
the duodenum. When the fusion process occurs, the ventral anlage will result in the head of
the pancreas and the dorsal in the tail (Wells 1999; Wells 2000; Hammerman 2006). The
liver (including extrahepatic biliary system) and ventral pancreas arise from the same region
of the ventral foregut endoderm (Zaret 2008). Thus, the pancreas, gut, fetal liver and gall
bladder share a common embryonic origin, and most likely precursor cells of these organs
share many phenotypical and functional traits that make them interesting candidates to
generate insulin-secreting cells (Sahu 2009; Sahu 2009).
The intestinal epithelium contains active stem cells located in the crypts that allow gut
renewal each 28–40 hrs. Among the 4 cell types present in the differentiated gut epithelium,
the GLP-1 secreting L cells have an endocrine phenotype, expressing molecules that are
involved in glucose sensing and regulated secretion similar to β-cells (Schuit 2001).
Therefore, these cells could be candidates that through minimal engineering can become β-
cell surrogates. Intestinal crypts can be isolated from rodents and humans from a biopsy
and cultured under specific conditions. Cells derived from these cultures are capable of
expressing insulin after transfection with Pdx-1 and exposed to betacellulin. Similar results
have been obtained after a double transfection with the transcription factors Pdx-1 and Isl1
(Kojima 2002; Yoshida 2002). Although the resulting cells displayed several pancreatic β-
cell markers, they were unable to secrete insulin in a glucose-regulated manner.
There is now a growing body of evidence to suggest that it may be possible to induce the
conversion of liver cells (hepatocytes, intra-/extrahepatic biliary epithelial cells and gall
bladder epithelium) to pancreatic lineages. Transdifferentiation has been demonstrated in a
number of models including: overexpression of pancreas and duodenal homeobox gene 1
(pdx1) in liver cells (Ferber 2000). However, vectors with Pdx-1 resulted in high rates of
hepatoxicity which was not due to the residual infective potential of the viral vector itself.
Instead, it seemed that Pdx-1 expression was more likely implicated in the development of
these hepatic alterations through the induction of differentiating exocrine tissue (Kojima
2003). The presence of exocrine proteases, such as trypsin, could cause the self-
destruction of hepatic cells, affecting at the same time newly-formed hepatic insulin-
producing cells. These complications were not observed when cells were reprogrammed
using NeuroD delivering vectors (Kojima 2003). Sumazaki et al. (Sumazaki 2004)
demonstrated the conversion of the developing biliary system to pancreatic tissue in Hes1
null mice. Unfortunately, use of the common bile duct as a source of tissue for the
generation of β-cells is precluded, as it is essential for normal liver function. While the
common bile duct may not be useful as a source of pancreatic β-cells, the gall bladder may
offer an alternative starting material. Recent studies have demonstrated that gall bladder
Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 25
(Sahu 2009), as well as human biliary duct epithelial cells contain endocrine pancreatic
hormone-producing cells. Recently it has also been shown that intrahepatic biliary epithelial
cells can be expanded and converted to β-like cells (Nagaya 2009).
On the other hand, pancreatic tissue has been extensively studied in order to find
regeneration pathways as well as precursors that could be managed in vivo and in vitro for
tissue repair. In this context, several mechanisms have been proposed: (a) neogenesis from
pancreatic ductal/islet stem cells, (b) replication of existing β-cells and (c) transdifferentiation
of pancreatic exocrine cells/precursors. These have been discussed earlier in the chapter.
Insulin-producing cells from ectoderm precursors: Pancreatic β-cells of endodermal
origin share many common features with ectoderm-derived neurons, including transcription
factors, biosynthetic enzymes, as well as proteins of the secretory pathway and metabolism.
Although adult β-cells are phenotypically and functionally different from neurons, some
common molecular mechanisms could be remodeled to bioengineer neuronal precursors to
insulin-producing cells (Hori 2005). Indeed, hypothalamic neurons display the ability to
express insulin II gene, although molecular modifications will be required to increase the
amount of insulin produced and to achieve correct pro-hormone processing. In this context,
it has been reported that cultured neuronal stem cells can generate insulin-producing
surrogates, expressing phenotypical markers and displaying functional responses typical of
pancreatic β-cells (Burns 2005; Hori 2005). Although nestin expression has been
considered a neuroectoderm marker, it has been previously proposed that nestin-positive
cells in the adult pancreas could be endocrine precursors. However, transgenic mouse
technology has evidenced that nestin is expressed in endothelial cells of islet vasculature
(Treutelaar 2003). Mesenchymal cells derived from islets in vitro have the ability of
expressing nestin as well (Gershengorn, Hardikar et al. 2004). It has also been shown that
the replicating cells in expanded adult islets were mostly endocrine, displaying transient
nestin expression and rapid de-differentiation in non-defined cell culture medium (Lardon
2002; Selander 2002). Altogether, the data seem to indicate that nestin expression is not
limited exclusively to ectodermal- derived tissues and could be a candidate marker for islet
precursors.
Insulin-producing cells from mesoderm precursors: bone marrow, peripheral blood cells, umbilical cord blood cells and Adipocytes: Bone marrow is an important source
of easily accessible adult stem cells, and bone marrow transplantation (BMT) is considered
to be a potential treatment of autoimmune type 1 diabetes. However, there is a great debate
on the issue of the fate of transplanted bone marrow stem cells. Ianus et al. (Ianus, Holz et

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 26
al. 2003) showed that mouse bone marrow-derived cells can differentiate into pancreatic
endocrine β-cells with glucose-dependent and incretin-enhanced insulin secretion when
transplanted into lethally irradiated mice. They transplanted genetically labeled marrow
using CRE-LoxP-GFP system, and showed that up to 3% of recipient islet cells co-
expressed GFP-Insulin-Glut2. However subsequent reports did not find any evidence of
differentiation of the similar BMCs into β-cells (Choi, Uchino et al. 2003; Lechner, Yang et al.
2004; Mathews, Hanson et al. 2004; Taneera, Rosengren et al. 2006). Though these
studies support homing of donor bone marrow cells within the pancreas, it is believed that
BMCs help in proliferation of endogenous resident cells to bring about reconstitution of the
target organ (Hess, Li et al. 2003; Ende, Chen et al. 2004; Banerjee, Kumar et al. 2005; Lee,
Seo et al. 2006; Hasegawa, Ogihara et al. 2007). Hess et al. (Hess, Li et al. 2003) reported
that transplantation of c-kit positive mouse bone marrow-derived stem cells initiated
endogenous pancreatic regeneration and improved blood glucose level in streptozocin (STZ)
induced diabetic mice via enhanced endothelial proliferation by donor cells. In a similar
study, Lee et al. (Lee, Seo et al. 2006) demonstrated that transplanted MSCs from human
bone marrow lowered blood glucose levels in diabetic immunodeficient mice by promoting
repair of mouse pancreatic islets.
Lately, co-transplantation of syngeneic BMCs and syngeneic or allogeneic MSCs into
diabetic mice resulted in rapid recovery of blood glucose and serum insulin levels
accompanied with efficient tissue regeneration (Urbán 2008). Researchers suggested that
two aspects operate parallelly and synergistically in this model. First, BMCs and MSCs
induce the regeneration of recipient derived pancreatic insulin-secreting cells. Second,
MSCs inhibit T cell mediated immune responses against newly formed β-cells. Their work
offers a novel potential therapeutic protocol for type 1 diabetes. On the other hand, studies
illustrated that when cultured in vitro, bone marrow derived-cells obtained from mice (Tang,
Cao et al. 2004) and rats (Oh SH 2004) could be differentiated into insulin-producing cells.
Multi-potent adult progenitor cells (MAPCs) or MSCs within bone marrow are intriguing
candidates that can give rise to insulin positive cells. In 2002, Jiang et al. (Jiang 2002)
proposed the existence of pluripotent MSCs derived from adult marrow. Chen et al. (Chen,
Jiang et al. 2004) and Wu et al. (Wu 2007) isolated MSCs from rat bone marrow, and
successfully induced their differentiation into islet-like cells. Moreover, transplantation of
these islet-like cells could alleviate the hyperglycaemia in diabetic rats. Subsequently, Choi
et al. (Chen, Jiang et al. 2004; Choi, Shin et al. 2005) proved that treatment of rat pancreatic
extract can differentiate rat marrow mesenchymal cells into insulin-producing cells in vitro.
Genetic manipulations followed by exposure to specific growth and differentiating factors
have been shown to promote in vitro differentiation of BMCs into insulin-expressing cells

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 27
(Moriscot, de Fraipont et al. 2005). Transfer of human insulin gene into human BMCs
(hBMCs) generated insulin-producing cell for more than 3 weeks (Lu, Wang et al. 2006). It
was also demonstrated that forced expression of PDX-1, a master regulator of pancreas
development, in hBMCs successfully allowed for expression of pro-endocrine genes such as
neurogenin3 (NGN3) as well as downstream genes such as the glucose sensing enzyme
glucokinase, glucose transporter (GLUT2), and pancreatic hormones; glucagon and insulin.
Recently, two studies (Karnieli, Izhar-Prato et al. 2007; Li, Zhang et al. 2007) have presented
evidence that pancreatic duodenal homeobox-1 (PDX-1) gene-modified human bone
marrow-derived MSCs can be induced to differentiate into functional insulin-producing cells.
However, these differentiated hBMCs do not show efficient glucose stimulated insulin
secretion (GSIS). Nonetheless, animals that were rendered diabetic using β-cell specific
toxin (STZ) showed normal glucose concentration for over a month after transplantation with
these cells (Karnieli, Izhar-Prato et al. 2007; Li, Zhang et al. 2007). Though these studies
have helped us immensely in understanding the differentiation of BMCs into endocrine
pancreatic lineage, the use of viral vectors limit them from use in cell replacement therapy
for diabetes (Hasbrouck NC 2008). Non transformed murine (Chen, Jiang et al. 2004; Tang,
Cao et al. 2004) and human (D'Ippolito, Diabira et al. 2004; Sun, Chen et al. 2007) BMCs
when treated with growth factors, demonstrated that these cells have the potential to
differentiate into the pancreatic lineage. However manipulation of culture conditions induced
low levels of insulin in vitro (Tang, Cao et al. 2004; Chen, Jiang et al. 2004; Choi, Shin et al.
2005). In addition, Sun et al. (Sun, Chen et al. 2007) demonstrated that bone marrow
derived MSCs from diabetic patients can differentiate into IPCs under appropriate conditions
in vitro. Their results provide the direct evidence for the feasibility of using patient’s own BM-
MSCs as a source of IPCs for β-cell replacement therapy.
MSCs from human bone marrow and adipose tissue represent very similar cell populations
with comparable phenotypes (Zuk 2002; De Ugarte 2003; Lee 2004; Dicker 2005). Thus,
MSCs with the potential to adopt a pancreatic endocrine phenotype could also exist in
human adipose tissue. Timper et al. (Timper 2006) isolated human adipose tissue-derived
MSCs and expanded them in basic fibroblast growth factor (bFGF) containing culture
medium. Proliferating MSCs expressed the stem cell markers nestin, ABCG2, SCF, Thy-1
as well as the pancreatic endocrine transcription factor Isl-1 mRNA. When subjected to
defined differentiation medium, a down-regulation of ABCG2 and an up-regulation of
transcription factors Isl-1, Ipf-1 and Ngn3 were observed together with induction of the islet
genes insulin, glucagon and somatostatin. Murine adipose tissue-derived stem cells (ASCs)
with and without PDX-1 transfection, have recently been shown to efficiently differentiate into
pancreatic hormone-expressing islet-like cell aggregates (Chandra 2009; Kajiyama,

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 28
Hamazaki et al. 2009). Consequently, autologous adipose tissue-derived MSCs could be an
alternative source of pancreatic β-cells.
Human umbilical cord blood (hUCB) is another source of stem cells with the potential to
develop into insulin-producing cells. hUCB-derived MNC population have recently been
shown to contain a subset of "pancreas-committed" cells that have the potential to
differentiate into insulin-producing cells in vivo (Parekh, Joglekar et al. 2009).
Transplantation of hUCB cells resulted in the improvement of blood glucose levels and
survival rate in type 2 diabetic mice (Ende 2004). Furthermore, a regression of glomerular
hypertrophy and tubular dilatation, common complications attributed to diabetes, was
observed in hUCB treated mice. In another study (Ende 2004), transplantation of hUCB cells
into type 1 diabetic mice led to a dose-dependent reduction in blood glucose levels and the
degree of autoimmune insulitis. A recent report (Yoshida 2005) has focused on the in vivo
capacity of hUCB-derived cells to generate insulin-producing cells. Following transplantation
of hUCB cells into NOD-SCID, IPCs of human origin were found in recipient pancreatic
islets. Double FISH analysis using species-specific probes further indicated that HUCB cells
can give rise to insulin-producing cells by fusion-dependent and –independent mechanisms.
The number of hUCB cells that transdifferentiated and the rate of such an event are critical
aspects. The proportion of hUCB-derived insulin-producing cells per total number of islet
cells (Yoshida 2005) was less than in the case of BM-derived insulin-producing cells (Ianus,
Holz et al. 2003). However, under diabetic conditions, the demand for the neogenesis of
insulin-producing cells might increase and the rate of hUCB cell differentiation could become
higher in order to compensate for the regeneration of β-cell mass. On the other hand, the
stem cell type in hUCB responsible for generation of insulin-producing cells remains unclear.
Since MSCs have been identified in the cord blood (Bieback 2004) and hUCB-derived USSC
(unrestricted somatic stem cell) share most of the cell markers and properties with MAPCs
(Koblas 2005), it should be considered that MSCs may take part in the differentiation of
hUCB cells towards a β-cell phenotype.
In addition to hUCB, the Wharton’s jelly of the human umbilical cord is rich in mesenchymal
stem cells (UC-MSCs) that fulfil the criteria for MSCs (Kadam, Tiwari et al. 2009). Recently,
Chao et al. (Chao, Chao et al. 2008) successfully differentiated UCMSCs into mature ICCs,
and these ICCs possess insulin-producing ability in vitro and in vivo. Moreover, they
indicated that UC-MSCs seem to be the preferential source of stem cells to convert into
IPCs, because of the large potential donor pool, its rapid availability, no risk of discomfort for
the donor, and low risk of rejection.

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 29
Human monocytes isolated from peripheral blood can be reprogrammed to endoderm
precursors by exposure to interleukin-3 and macrophagecolony stimulating factor, and
further differentiated to insulin-producing cells by the addition of EGF, hepatocyte growth
factor (HGF) and nicotinamide (Ruhnke, Ungefroren et al. 2005). Transplantation of the
resulting cells under the kidney capsule of experimental-diabetic mice led to the restoration
of normoglycaemia over a short period of time before immunological implant rejection.
Although promising, the circulating pluripotential cell has not been identified, the C-peptide
content is very low, and, for unknown reasons this protocol seems to work only in 2/3 of the
blood samples obtained. In any case, more solid animal models need to be developed in
order to test the long term potential of these cells in correcting hyperglycemia.
Induced pluripotent stem cells: A breakthrough in the field of somatic cell reprogramming
came from the laboratory of Yamanaka, who reported the induction of pluripotent stem cells
from mouse embryonic and adult fibroblast cultures by defined factors (Takahashi and
Yamanaka 2006). Starting with 24 candidate factors for pluripotency, they identified 4 that
are necessary and sufficient for somatic reprogramming to pluripotency. Analysis of factors
led to the conclusion that Oct3/4 (i.e. Oct4), Sox2, Klf4, and c-Myc are indispensable for
pluripotency. The authors also report that the majority, but not all, of the clones, named
induced pluripotent stem (iPS) cells, derived from the transduced cultures actually attained
pluripotency in vivo, when transplanted into nude mice. In addition, when gene expression
patterns were analyzed between iPS and ES cells, some differences were noted, suggesting
the necessity for the involvement of additional factors in somatic reprogramming. Recently, human iPS cells with disease genotypes have been generated as a tool for human
disease modeling (Dimos, Rodolfa et al. 2008; Park, Arora et al. 2008; Ebert, Yu et al. 2009).
iPS cells have also been generated from fibroblasts obtained from type 1 diabetic patients
(Maehr, Chen et al. 2009). Differentiation of diabetic iPS cells to β-like cells is relevant not
only for the long term possibility of autologous cell replacement therapy, but also for disease
modeling. These model systems may be useful for testing of preventative and therapeutic
strategies.
d. Potential sites for islet transplantation. Islet transplantation into the portal vein is the current clinical practice. However, it has now
been recognized that this implantation site has several characteristics that can hamper islet
engraftment and survival, such as low oxygen tension, an active innate immune system, and
the provocation of an inflammatory response (IBMIR). In addition to this, the increase of
portal pressure, risk of bleeding, risk of portal vein thrombosis, along with the embolization of

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 30
the pancreatic tissue into the portal system, limits the number of repeated islet transplants
needed to maintain the islet mass required to produce adequate levels of insulin, mainly due
to important technical complications. These factors result in the loss of many transplanted
islets, mainly during the first hours or days after transplantation, which could in part explain
the necessity for the transplantation of islets from multiple pancreas donors to cure type 1
diabetes. This eventually increases the burden on the limited pool of donor organs.
Therefore, an alternative anatomical site for islet transplantation that offers maximum
engraftment, efficacious use of produced insulin, and maximum patient safety is urgently
needed. However, many of the experimentally tested sites have no clinical applicability,
leaving the liver, for the time being, as the most feasible site for pancreatic islet
transplantation in humans.
The bladder submucosa and testis via the vas deferens might represent alternative sites
for pancreatic islet transplantation (PIT). The latter route may benefit from the
immunoprivileged and special trophic conditions of the testis (Burgos, Gomez et al. 2006).
The pancreas itself can be considered as an alternative implantation site and minimal or
suboptimal number of free or immunoisolated islets, if transplanted elsewhere, may be
sufficient to prevent hyperglycemia in the recipient (Stagner 2007). Primary human fetal
pancreatic tissue fragments were transplanted into SCID mice at three transplantation sites:
mammary fat pad, subcutaneous flank region, and kidney capsule. The authors
demonstrated that transplantation of primary human fetal pancreatic fragments under the
kidney capsule reproducibly resulted in greater than 85% (106/124) engraftment while
maintaining a three dimensional tissue architecture (Ai, Todorov et al. 2007). Presence of
thymic tissue beneath the autologous renal capsule facilitated the engraftment of minor-
mismatched islets, and such grafts achieved results similar to autologous islet transplants
(Kumagai 2002). Therefore, the ability to create vascularized islet grafts may provide a
strategy for successful islet transplantation across allogeneic and potentially across
xenogeneic barriers. The gastric submucosa represents a potential islet engraftment site
because of its easy accessibility by endoscopy (Caiazzo 2007). Omentum also is
speculated to be an alternative site for islet transplants in humans, but poor vasculature of
omentum in mice makes it undesirable for experimental purposes. The mouse epididymal fat pad, however, is a well-vascularized and thin veil of tissue connected to the epididymis
with many properties similar to that of the human greater omentum. Thus it may serve as a
useful site for islet implantation because it is easily accessible, the grafts may be easily
removed without damage to other organs, and it allows for the use of scaffold delivery
devices to be used to enhance islet engraftment. However the epididymal fat pad does not
have a portal drainage system unlike the omental site (Chen 2007). This site could

Smruti M. Phadnis, ARI, Pune (Ph.D. Thesis-2009) 31
constitute an interesting alternative for experimental studies in large mammals and,
eventually, for clinical application. Bone Marrow is widely distributed, protected, and has
well-vascularized microenvironment capable of sustaining independent cell grafts.
Pancreatic islet isografts and allografts were implanted into the bone marrow tissue of the
tibial bone of non-diabetic rats. Although these studies do not prove that the bone marrow is
a more suitable site than the liver for the implantation of islets, the presence of engrafted
islets staining positive for insulin and glucagon, without evident signs of apoptosis or
rejection when no immunosuppression was used, is encouraging (Salazar-Banuelos 2008).
Although the rest of the sites have a huge potential in experimental diabetes, they would
require a lot of clinical investigations along with other primary concerns. Eventually, the liver
will most likely be replaced by a site that allows long-term survival of islets from a single
donor to reverse type 1 diabetes. However, till date, the liver still seems to be the most
suitable site for islet transplantation in humans.
e. Objectives and scope of the present study: Since human bone marrow can be used for syngenic and allogeneic transplantation settings,
we designed the study to explore the potential of human bone marrow derived mesenchymal
cells to differentiate into functional, hormone producing islet like cell clusters without any
genetic intervention.
Objectives:
To identify, isolate and characterize mesenchymal stem cells (MSCs) from human
bone marrow (BM).
To assess the multilineage potential of human bone marrow derived mesenchymal
cells (hBMCs) in vitro under the influence of specific differentiation cocktails and
tissue/organ extracts.
To study in vitro differentiation of these hBMCs into insulin-producing islet-like cell
aggregates (ICAs) along with their gene profiling to assess early markers in islet
differentiation pathway.
To assess the functionality of differentiated ICAs in vitro and in vivo following
transplantation in immuno-incompetent as well as immuno-competent mice.


















