
Review Article Proposing a new algorithm for ...
9
775 Review Article Proposing a new algorithm for premanipulative testing in physical therapy practice Brent Harper, PT, DPT, DSc, OCS, FAAOMPT 1)* , Daniel Miner, PT, DPT, NCS 2) , Harrison Vaughan, PT, DPT, OCS 3) 1) Crean College of Health and Behavior Sciences, Chapman University: 9401 Jeronimo Road, Irvine, CA 92618, USA 2) Department of Physical Therapy, Waldron College of Health and Human Services, Radford University, USA 3) PhysioFit, USA Abstract. In the field of physical therapy, there is debate as to the clinical utility of premanipulative vascular assessments. Cervical artery dysfunction (CAD) risk assessment involves a multi-system approach to differentiate between spontaneous versus mechanical events. The purposes of this inductive analysis of the literature are to dis- cuss the link between cervical spine manipulation (CSM) and CAD, to examine the literature on premanipulative vascular tests, and to suggest an optimal sequence of premanipulative testing based on the differentiation of a spon- taneous versus mechanical vascular event. Knowing what premanipulative vascular tests assess and the associated clinical application facilitates an evidence-informed decision for clinical application of vascular assessment before CSM. Key words: Manipulation, Algorithm, Cervical (This article was submitted Jun. 18, 2020, and was accepted Aug. 4, 2020) INTRODUCTION Traditionally, vertebrobasilar insufficiency (VBI) has been considered the most concerning risk factor for an adverse event during cervical spine manipulation (CSM) 1, 2) . The majority of investigations of CSM adverse events have focused on VBI, specifically injury to the vertebral artery (VA) 3–6) . Another vascular concern reported in the literature involves internal carotid artery (ICA) dissection 4, 7–11) which would indicate an immediate need for medical referral 12) . The purposes of this clinical perspectives manuscript are to discuss the link between cervical spine manipulation (CSM) and cervical artery dysfunction (CAD), to examine premanipulative vascular tests in the literature, and to suggest an optimal sequence of premanipulative testing based on the differentiation of a spontaneous versus mechanical vascular event. METHODS A non-comprehensive inductive analysis of the literature addressing links between CSM and CAD and a review of pre- manipulative vascular tests in order to propose a new algorithm for premanipulative testing in physical therapy. The answers to this question were determined through the following 5-step process: a literature search was conducted in order to identify information; copies of articles were identified through the literature search and obtained; a synopses of each article was writ- ten in order to capture any information pertaining to the purpose of the study, the research design, sources and kinds of data, data collection and analysis, results, and conclusions. Any manual therapy safety options used to screen patients with neck J. Phys. Ther. Sci. 32: 775–783, 2020 *Corresponding author. Brent Harper (E-mail: [email protected]) ©2020 The Society of Physical Therapy Science. Published by IPEC Inc. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial No Deriva- tives (by-nc-nd) License. (CC-BY-NC-ND 4.0: https://creativecommons.org/licenses/by-nc-nd/4.0/)
Transcript of Review Article Proposing a new algorithm for ...
775
Review Article
Proposing a new algorithm for premanipulative testing in physical therapy practice
Brent Harper, PT, DPT, DSc, OCS, FAAOMPT1)*, Daniel Miner, PT, DPT, NCS2), Harrison Vaughan, PT, DPT, OCS3)
1) Crean College of Health and Behavior Sciences, Chapman University: 9401 Jeronimo Road, Irvine, CA 92618, USA
2) Department of Physical Therapy, Waldron College of Health and Human Services, Radford University, USA
3) PhysioFit, USA
Abstract. In thefieldofphysical therapy, there isdebateas to theclinicalutilityofpremanipulativevascularassessments.Cervicalarterydysfunction(CAD)riskassessmentinvolvesamulti-systemapproachtodifferentiatebetweenspontaneousversusmechanicalevents.Thepurposesofthisinductiveanalysisoftheliteraturearetodis-cussthelinkbetweencervicalspinemanipulation(CSM)andCAD,toexaminetheliteratureonpremanipulativevasculartests,andtosuggestanoptimalsequenceofpremanipulativetestingbasedonthedifferentiationofaspon-taneousversusmechanicalvascularevent.Knowingwhatpremanipulativevasculartestsassessandtheassociatedclinicalapplicationfacilitatesanevidence-informeddecisionforclinicalapplicationofvascularassessmentbeforeCSM.Key words:Manipulation,Algorithm,Cervical
(This article was submitted Jun. 18, 2020, and was accepted Aug. 4, 2020)
INTRODUCTION
Traditionally,vertebrobasilarinsufficiency(VBI)hasbeenconsideredthemostconcerningriskfactorforanadverseeventduringcervicalspinemanipulation(CSM)1, 2).ThemajorityofinvestigationsofCSMadverseeventshavefocusedonVBI,specificallyinjurytothevertebralartery(VA)3–6).Anothervascularconcernreportedintheliteratureinvolvesinternalcarotidartery(ICA)dissection4, 7–11)whichwouldindicateanimmediateneedformedicalreferral12).Thepurposesofthisclinicalperspectivesmanuscriptaretodiscussthelinkbetweencervicalspinemanipulation(CSM)andcervicalarterydysfunction(CAD),toexaminepremanipulativevasculartestsintheliterature,andtosuggestanoptimalsequenceofpremanipulativetestingbasedonthedifferentiationofaspontaneousversusmechanicalvascularevent.
METHODS
Anon-comprehensiveinductiveanalysisoftheliteratureaddressinglinksbetweenCSMandCADandareviewofpre-manipulativevasculartestsinordertoproposeanewalgorithmforpremanipulativetestinginphysicaltherapy.Theanswerstothisquestionweredeterminedthroughthefollowing5-stepprocess:aliteraturesearchwasconductedinordertoidentifyinformation;copiesofarticleswereidentifiedthroughtheliteraturesearchandobtained;asynopsesofeacharticlewaswrit-teninordertocaptureanyinformationpertainingtothepurposeofthestudy,theresearchdesign,sourcesandkindsofdata,datacollectionandanalysis,results,andconclusions.Anymanualtherapysafetyoptionsusedtoscreenpatientswithneck
J. Phys. Ther. Sci. 32: 775–783, 2020
*Correspondingauthor.BrentHarper(E-mail:[email protected])©2020TheSocietyofPhysicalTherapyScience.PublishedbyIPECInc.
Thisisanopen-accessarticledistributedunderthetermsoftheCreativeCommonsAttributionNon-CommercialNoDeriva-tives(by-nc-nd)License.(CC-BY-NC-ND4.0:https://creativecommons.org/licenses/by-nc-nd/4.0/)
The Journal of Physical Therapy Science

J. Phys. Ther. Sci. Vol. 32, No. 11, 2020 776
painwasnotedoneachsynopsis.MEDLINEandCINHALsearchtermsincluded“classify”,“candidates”,“manipulation”,“uppercervicalspinemanipulation”,“clinicaldecisionmaking”,“clinicalreasoning”,“evidence-basedmedicine”,“predic-tiverule”,and“clinicalpredictionrule”.Allarticlesweresearched,butonlyEnglishlanguagearticleswereobtainedbecauseEnglishabstractsofnon-Englisharticlesindicatedirrelevance.Allyearsweresearchedwith,emphasiswasplacedonarticlespublishedwithinthelastten-years.Referencearticlesfromreviewedjournalsgarneredadditionalarticles.
RESULTS
Intheirdiscussionofvascularinsufficiencies,Kerryetal.13)andKerry&Taylor14)proposedarevisionofthenomencla-ture,suggestingthetermcervical artery dysfunction (CAD)sinceitencompassespotentialcomplicationsofallarteriesinthecervico-cranialregion.Theauthorsidentifiedinherentrisksfromaglobalhemodynamicperspectiveratherthanstructuralorpathological,ashistoricallycategorized.Kerryetal.13)definedCADas:thecompletenessofthearterialanatomy(e.g.,thevertebrobasilarsystem,theinternalcarotidarteries,andtheCircleofWillis),andtherangeofpathologiesthatthemanualtherapistmayencounter (e.g., localdissection,atheroscleroticevents,vessel injury,non-ischaemic[sic]events, ischemicevents).
ThisdefinitionofCADistheInternationalFrameworkforExaminationoftheCervicalRegionstandardasadoptedbytheInternationalFederationofOrthopaedicManualPhysicalTherapists(IFOMPT)foridentificationofvascularinvolvementbeforeorthopedicmanualtherapyintervention15).IFOMPTdoesnotdiscouragemechanicalvascularpatencyassessments,andtheAustralianPhysiotherapyAssociation(APA)16)protocolincludesevaluationforvascularsymptomswhileperformingmechanicalmovementsthatstressvascularpatency.
Neurovascular structurescanbecompromisedbothexternallyand internally, resulting in symptoms.CADsymptomsfromextrinsicormechanicalfactors,inwhichanatomicalstructuresplayarole,includingosteophytes,skeletalanomalies,muscularentrapment,fibrousbands,andnerveentrapment,maycompromiseneurovascularstructures.Excessivemechani-calforces,likecervicalspinerotationandhyperextensionorCSM,arealsoextrinsiccauseswhichmayresultinmechanicalarterialdissection17).IntrinsicCADsymptomsrelatetothepathologyofthearteryitself,anarrowingofthelumen.Intrinsicfactorsincludeatherosclerosis,aneurysms,thrombosis,andemboli,anyofwhichmayresultinspontaneousarterialdissec-tion17, 18).
TheincidenceofmechanicalarterialdissectionsduetoanextrinsicfactorsuchasCSMrangesfrom1in9,000to1in10millionwithinherentunder-reporting,makingtheactualincidencechallengingtocalculateaccurately19–24).Theincidenceofspontaneousarterialdissectionduetointrinsicfactorsis1to1.5per100,000people19–24).Thus,aspontaneousarterialdissectioneventisprobablymoreprevalentthanthoseassociatedwithCSMorvertebralarterytestinglikedeKleyn’s,pre-manipulativeholdsorcervicalrotation19–24).Consequently,thereappeartobeotherfactorsinvolvedinarterialcompromisebesidesthebiomechanicalforcesassociatedwithCSMorvertebralarterytesting17, 20, 21, 25).Theseotherfactorsfocusonvari-ousmedicalco-morbidities,resultinginturbulenceinthearteries,specificallyatherosclerosis,hypertension,ordiabetesmel-litus18, 26, 27).Spontaneousarterialdissectionsappeartoberelatedtoco-morbiditiesthataffectvasculature,primarilyICAs,aswellastheVAs.TheICAsaffectedbyvascularturbulenceissuesaremorelikelytopresentwithsignsandsymptoms.Itisnosurprise,then,thatICAdissectionratesarenearlydoubletheratesofVAdissection28).Giventhevariouscorticalandsubcorticalregionsthesevesselssupply,clinicalsigns,andsymptomsassociatedwithICAdissectiondiffersignificantlyfromthoseassociatedwithVAdissection.AfulldescriptionofICAsymptomsisbeyondthispaper’sscope,butinitialsignsofICAdisruptionareoftenseenbytestingeyefunctions17,29).Thecriticalelementregardingmechanicalextrinsicandintrinsictestingisthatbiomechanicalarterialtestingwillnotassistinidentifyingthoseatriskofspontaneousarterialdissection.Infact,theactualperformanceofabiomechanicaltestonsomeoneatriskforintrinsicpathologymayenableaspontaneouseventtooccurmorereadily17).
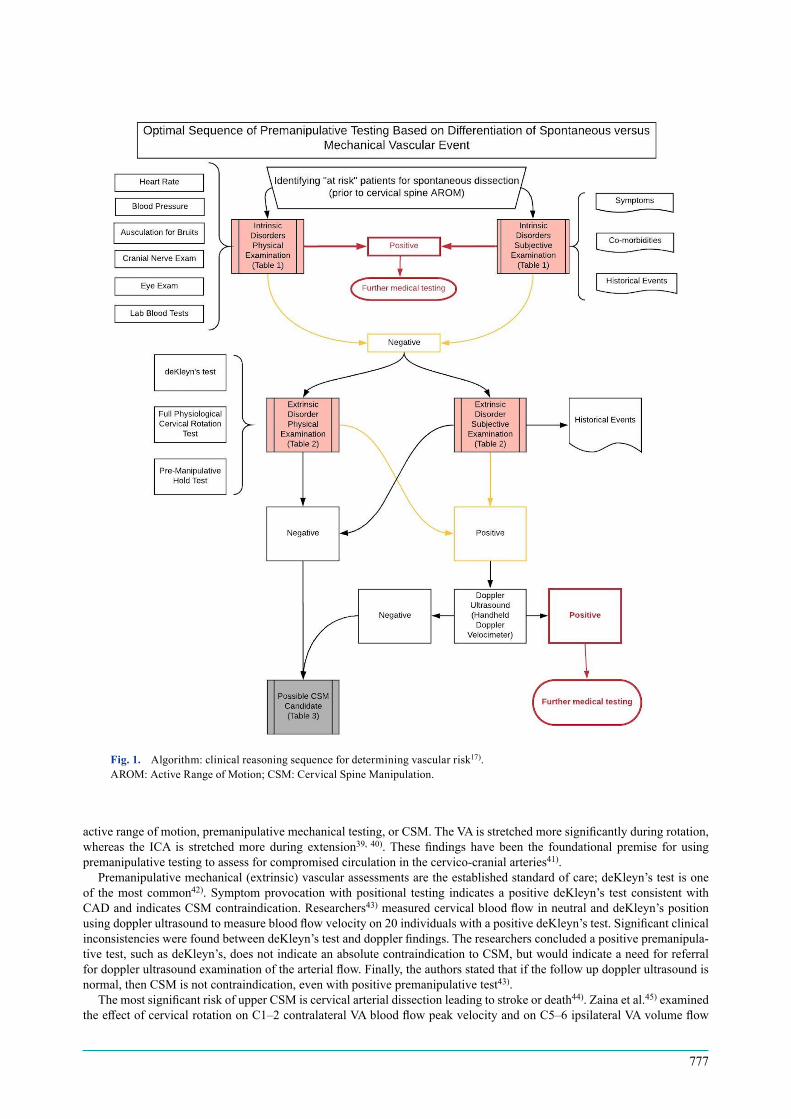
Cliniciansmustbeabletoeffectivelyscreenforandruleoutconcernforvascularcompromisebeforeanymechanicalevaluationofthecervicalspine.Theabilitytoeffectivelyscreenforvascularcomplicationthreatsisessentialtounderstand-ingtheunderlyingriskfactorswhichmaypredisposeanindividualtocervicalarterydissection(Fig.1)17).
TheICAsprovide80–89%ofbloodflowtothebrainandgiverisetothemiddleandanteriorcerebralarteries.TheVAsjointoformthebasilararteryandcontribute11–20%ofcerebralbloodflowtotheposteriorcirculationofthebrain30, 31).ThecourseoftheVAvariesandismorelikelytobeanomalousinindividualswithcongenitaldeformitiesofthecranio-cervical junctionorwithahistoryof traumainvolvingatlantoaxialsubluxation32, 33).Upto20%of thepopulationhasanormal anatomical variation of some type.Theoretically, anomalies of theVA, or any artery,may alter hemodynamicsby increased turbulence,whichmaypredispose the individual toaneurysms, thus increasing the risk forcerebrovascularaccident(CVA)17, 27).Despiteanatomicalvariations,theirimpactontheriskofVAdissectionisunknown34, 35).
TheVApassesthroughfourdistinctanatomicalzones.Inzone3,theVApassesthroughthetransverseforamenofC1andmakesasharpturnhorizontallyacrossitbeforepiercingthroughtheduramater.Fiftypercentofcervicalrotationoccurswithinzone3attheatlantoaxial(AA)jointbetweenC1andC2,causingthemostsignificantimpactontheVAasitmaybe“tethered”atvariouspoints11, 34, 35).Therefore,thetortuouscourseoftheVAinzone3correlateswiththelocationmostfrequentlyatriskfromCSM36–38).
TheanatomicalcourseoftheVAanditspotentialvulnerabilityatfixationpointsmightaffectbloodflowduringcervical
777
activerangeofmotion,premanipulativemechanicaltesting,orCSM.TheVAisstretchedmoresignificantlyduringrotation,whereas the ICA is stretchedmore during extension39, 40).Thesefindings have been the foundational premise for usingpremanipulativetestingtoassessforcompromisedcirculationinthecervico-cranialarteries41).
Premanipulativemechanical(extrinsic)vascularassessmentsaretheestablishedstandardofcare;deKleyn’stestisoneof themostcommon42).Symptomprovocationwithpositional testing indicatesapositivedeKleyn’s testconsistentwithCADandindicatesCSMcontraindication.Researchers43)measuredcervicalbloodflowinneutralanddeKleyn’spositionusingdopplerultrasoundtomeasurebloodflowvelocityon20individualswithapositivedeKleyn’stest.SignificantclinicalinconsistencieswerefoundbetweendeKleyn’stestanddopplerfindings.Theresearchersconcludedapositivepremanipula-tivetest,suchasdeKleyn’s,doesnotindicateanabsolutecontraindicationtoCSM,butwouldindicateaneedforreferralfordopplerultrasoundexaminationofthearterialflow.Finally,theauthorsstatedthatifthefollowupdopplerultrasoundisnormal,thenCSMisnotcontraindication,evenwithpositivepremanipulativetest43).
ThemostsignificantriskofupperCSMiscervicalarterialdissectionleadingtostrokeordeath44).Zainaetal.45)examinedtheeffectofcervicalrotationonC1–2contralateralVAbloodflowpeakvelocityandonC5–6ipsilateralVAvolumeflow
Fig. 1. Algorithm:clinicalreasoningsequencefordeterminingvascularrisk17).AROM:ActiveRangeofMotion;CSM:CervicalSpineManipulation.

J. Phys. Ther. Sci. Vol. 32, No. 11, 2020 778
rate,andwhethertherewasacumulativebloodflow.Twentyparticipantswereexaminedwithultrasounddopplerinaseatedpositionwithheadneutral,at45degrees,andinendrangecervicalrotation.Noneof theparticipantsweresymptomaticduringtesting,andnosignificantdifferenceswerefoundat45degreesorend-rangerotationsinthebloodflowparametersofpeakvelocityatC1–2andvolumeflowrateatC5–6.Repetitionoftherotationalpositioningdidnothaveacumulativeeffect,demonstratingthatcumulativepremanipulativetestingdidnotharmtheVAsinthoseparticipants45).Furthermore,Erhardtetal.46)assessedhaemodynamicsonhealthyadultsatC1–2andfoundnodeletreiouseffectstoVAbloodflowwhencomparinghigh-velocitylowamplitude(HLVT)thrusttechniquetopremanipulativeholds.
SpecificbloodflowturbulenceassessmentssuchasdopplerultrasonographyhavedemonstratedthatspontaneouschangesinVAandICAbloodflow16, 47, 48)arenotalwaysdirectlyrelatedtoCSMmechanicalforces,butmaybeintrinsicallybased.Atpresent,therearenodefinitivefindingsrelatingbloodflowchangestoCSMandliteratureismixed;severalstudiesshowareductionincontralateralbloodflowduringcervicalrotation49–53),whileothersshownobloodflowchanges54–57).Onestudy58)usedMRItoassessbloodflowofhealthyindividualsduringvariousnon-manipulativeproceduressuchasend-rangecervicalrotation,uppercervicalrotation,orfirmaxialdistractionandfoundnoalterationsinbloodflowandconcludeditunlikelythatend-rangeneckrotationanddistractionpositionsarehazardoustothecerebralcirculation.Furthermore,theauthorssuggestedspecificsegmentallylocalizedtechniquesposednohigherrisktocerebralcirculationthanthemechanicalpositions tested58).Other research59) on healthy, asymptomatic patientswith decreased bloodflow inVAs and ICAs, asconfirmedbymagneticresonanceangiography,hadnegativepositionaltestsforCADduringmechanicalendrangerotationtesting.Theresultsofthesestudiescallintoquestiontheutilityofmechanicalvascularassessmentprocedures.Thomasetal.59)hypothesizedthatcompromisedbloodflowinonearteryisnaturallycompensatedforbycollateralflowthroughthearterialCircleofWillis,whichhelpstomitigateanysymptomswhichmayhaveresultedfromdecreasedcirculation.Thisevidencemaysuggestthatindividualswhoexperienceend-rangecervicalrotationsymptomsmaynothaveCAD,butmayhavedysfunctionmoreproximally(intrinsic)intheintracranialcirculationoftheCircleofWillis59).
Furthermore,Symons&Westaway27)arguethatbiomechanicalvertebralarterialtests,likedeKleyn’s,andmanualinter-ventions,likeCSM,maynotdisruptvertebralarterybloodflowfortworeasons.First,mostpeoplehavefourmajorarteriesthatsupply theCircleofWillis,allowingcollateralreflexivevascularcompensationforanybrainperfusiondeficits.TheauthorsprovideevidencethatcompensatorybloodflowoccurswithoutresultinginanincidentofVBI,evenwhen100%ofthevertebralarteryisoccluded.Second,theauthorsreportthatCSMistoofast,occurringat200milliseconds,ifperformedcorrectly inmid-rangeandnotatend-range tension,whichdoesnotstress theneurovascularstructures likeaprolongedstretch.Therefore,CSMproceduresaretoofasttocausearterialdamageifperformedintheproperrangeofmotion.TheauthorsconcludethatifCSMinducesVBIsignsandsymptoms,itdoessoonlyinthepresenceofotherfactorslikewhenaspontaneouseventisalreadyinprogress27).
Eventhoughpremanipulativemechanicalvascularassessmentsaretaughtinentry-levelphysicaltherapyprograms,theycontinuetobechallengedandquestionedasobjectiveclinicaltests.Duetoreducedsensitivity11, 13, 14, 48, 60),thesetestsareas-sociatedwithahighrateoffalsenegatives6)andhavepoorabilitytodiscriminatebetweenindividualswithorwithoutarterialpathology.Evidence-informedpracticeindicatesthatclinicianscannotrelysolelyonsymptomprovocationwithmechanicalvascularassessmentstodefinitivelyruleoutcervicalarterydysfunctionduetothepoordiagnosticaccuracyofthesetests3, 60).
Insummary,oneofthefirstclinicaltestsforcervicalarterialdysfunctionwasdescribedbydeKlyneover50-yearsagoandcontinuestobecommonlyused4)eventhoughconcernsrelatedtodiagnosticaccuracyhavepreventeditsintegrationintoclinicalpredictionrules.Bloodflow45, 54, 57, 58), VA61, 62),andICA61)strainstudiesfoundacompletelackofconstructvalidityforpremanipulativevascularscreeningtests.Theliteraturefailstosupporttheabilityofpremanipulativeteststoidentify,throughpositiveornegativetestfindings,individualsatriskforapost-CSMvascularevent3,5,11,13,39,63),toprovideanyusefuladditionaldiagnosticinformation64);andhasidentifiedahighfrequencyoffalsenegativeVAtests65).Manyauthorsadviseagainstusingmechanicalvascularteststoassessvascularpatency,primarilywhenathoroughhistoryidentifiessignsandsymptomsconsistentwithCAD13, 60, 64).Finally,theevidencesuggeststhatactiverangeofmotionputsmorestrainontheICAthanCSM61).
Limitationsincludedlackofaccesstonon-publishedprofessionalconferencesandthepossibilitythatsomenon-Englishprofessionalwritingsintheformofbooksandjournalarticlesmighthavebeenrelevanttothesubjectstudiedinthispaper.
DISCUSSION
TheAustralianPhysiotherapyAssociation(APA)VAprotocol16)recommendsconductingactiverangeofmotion(AROM)andpositionalvascularpatencytestwhensymptomsofVBI/CADareunclearonpatientswithavaguesubjectivehistoryforpotentialVBI/CADsymptoms.IntheUnitedStates,vascularscreeningremainscommonpracticepriortoCSM.Despitethecurrentresearch,IFOMPT15)doesnotspecificallydiscouragemechanicalvascularpatencyassessments.ICAvascularcompromise is associatedwith spontaneousarterialdissection; thus, assessments forovert symptomsor thepresenceofvaguesignsandsymptomsassociatedwithICAischemiaisvital,inconjunctionwithathoroughhistoryofco-morbiditiesandevents(Tables1and 3)beforeanymechanicalstressisplacedintheregion17),suchasvascularscreeningormechanicalstressors(AROM),
DespitethelackofsupportformechanicalvascularassessmentsforCAD,thereremainssomeclinicalvalueinprema-nipulativescreeningtests.Thekeytounderstandingtheirclinicalvalueisinacknowledgingthatmechanicaltestscannot

779
identifyriskforspontaneousCADand,aspreviouslystated,maycauseavascularevent. If therearenoriskfactors forvasculardiseaseandnegativenon-vascularpatencyscreeningtests(likeheartrate,bloodpressure,bruits)forsystem-widespontaneousvascularcompromise,thenthereisminimalriskofprovokingavasculareventthroughtheuseofmechanicalvascularscreens.Ontheotherhand,ifpositiveriskfactorsareidentifiedforaspontaneouseventoriftheclinicianisunsure,theclinicianwouldbeunwisetoattemptprovocationthroughmechanicaltesting.Therefore,mechanicalpremanipulativetestsarenotemployedwhentheclinicianhasanysuspicionthataspontaneousvasculareventisimminentorhighlyprob-able13, 17, 66),butmaybeusefultoassessanindividual’sphysicalandemotionaltoleranceintherangeinwhichtheCSMwilloccur17).
Itistheopinionoftheauthorsthatthecurrentevidencedoesnotsupporttheutilityofroutinelyperformingpremanipula-tivescreens,suchasdeKlyne’s, to identifyCAD.Presently,basedon thecurrentmedico-legalconstraintsgoverning theprofession,premanipulativescreensshouldbedone,whenappropriate,formedico-legalpurposesduetothesocietalpercep-tionoftherisksforadverseevents,eventhoughtheevidencedoesnotsupportthetests,untilwhichtimetheexpectationsofexcludingmechanicalpremanipulativetestingbecomes“standard”practice17).
Thisclinicalusefulnessofthisstudyisinitsemphasisontheorderofoperationsforsafelyscreeningforspontaneousarterial dissectionprior toAROM, and in the recommendation that vascular screening tests arenot useful for assessingvascularpatency,butmightbeusefulafterclearanceforspontaneousdissection(Table1)toassessanindividual’smechani-calandemotionaltolerancewithintherangeCSMwilloccur.ThisalgorithmisintendedtoaddtoAPA16)andIFOMPT15) premanipulativeCADguidelines (Fig.1)and isbasedon intrinsicversusextrinsicdisorders.Screening for spontaneoushemodynamicCADinvolvesacombinationofassessingforco-morbidities,investigatingpatienthistoricalevents,evalu-atingsubjectivecomplaints,andprovidingappropriatephysicalexaminationprocedures11, 13, 14, 17, 67).Oncespontaneousvascular sequelaeevents (intrinsicdisorders) (Table1)havebeenscreenedasnegative forvascularco-morbidities, thenpremanipulativescreeningformechanicalarterialcompromise(extrinsicdisorders)(Table2)canbeperformed,nottoassessarterialpatencyintermsofVBI/CAD,buttoevaluateforpotentialintolerancetomechanicalforceswhichmayoccurduringCSM17)(Table3).
Table 1.Optimalsequenceofpremanipulativeassessment(intrinsic)11, 13, 14, 17, 67)
Spontaneousarterialdissection(intrinsicdisorder)
History–Subjectiveexam/SE
1.Symptoms:5Ds(Diplopia,Dizziness,DropAttacks,Dysarthria,&Dysphagia),3Ns(Nausea,Nystagmus,&Numbness),Headache,Ataxia
2.Co-Morbidities(Anythingthatincreasesturbulence):Atherosclerosis,Hypertension(HTN),DiabetesMellitus(DM),historyofmigraine,geneticdefects(e.g.,increasedlevelsofaminoacidhomocysteinecreatingfragilityofthearterialwalls)
3.HistoricalEventsa)Asuddenonsetofseveresharpposteriorcervicalandoccipitalpain.b)Ahistoryofsmoking(especiallylong-standinghistory).c)Episodicdizzinessorvertigolastinggreaterthanoneminuteinisolationorwithpre-manipulativescreeningtest.d)Previoushistoryofischemicattacks.e)Ahistoryoftrauma(especiallyifitincludedwhiplashthatinvolvedaflexion-distrac-tion-and-rotationforce).
Tests&Measures–Objectiveexam (Physicalexam/PE)
HeartRate(HR),BloodPressure(BP),Auscultationforbruits,cranialnerveexamination,generaleyeexamination,labbloodtests(aminoacidhomocysteinelevels).
Table 2.Optimalsequenceofpremanipulativeassessment(extrinsic)11, 13, 14, 17, 67)
Mechanicalarterialcompromise(extrinsicdisorder)History–Subjectiveexam/SE 1.HistoricalEvents
a)Asuddenonsetofseveresharpposteriorcervicalandoccipitalpain.b)Ahistoryofsmoking(especiallylong-standinghistory).c)Episodicdizzinessorvertigolastinggreaterthanoneminuteinisolationorwithpre-manipulativescreeningtest.d)Previoushistoryofischemicattacks.e)Ahistoryoftrauma(especiallyifitincludedwhiplashthatinvolvedaflexion-distrac-tion-and-rotationforce).
Tests&Measures–Objectiveexam(Physicalexam/PE)
deKleyn’stest,FullPhysiologicalCervicalRotationtest,Pre-ManipulativeHold(PMH)test,HandheldDopplerVelocimeter.
J. Phys. Ther. Sci. Vol. 32, No. 11, 2020 780
FundingNone.
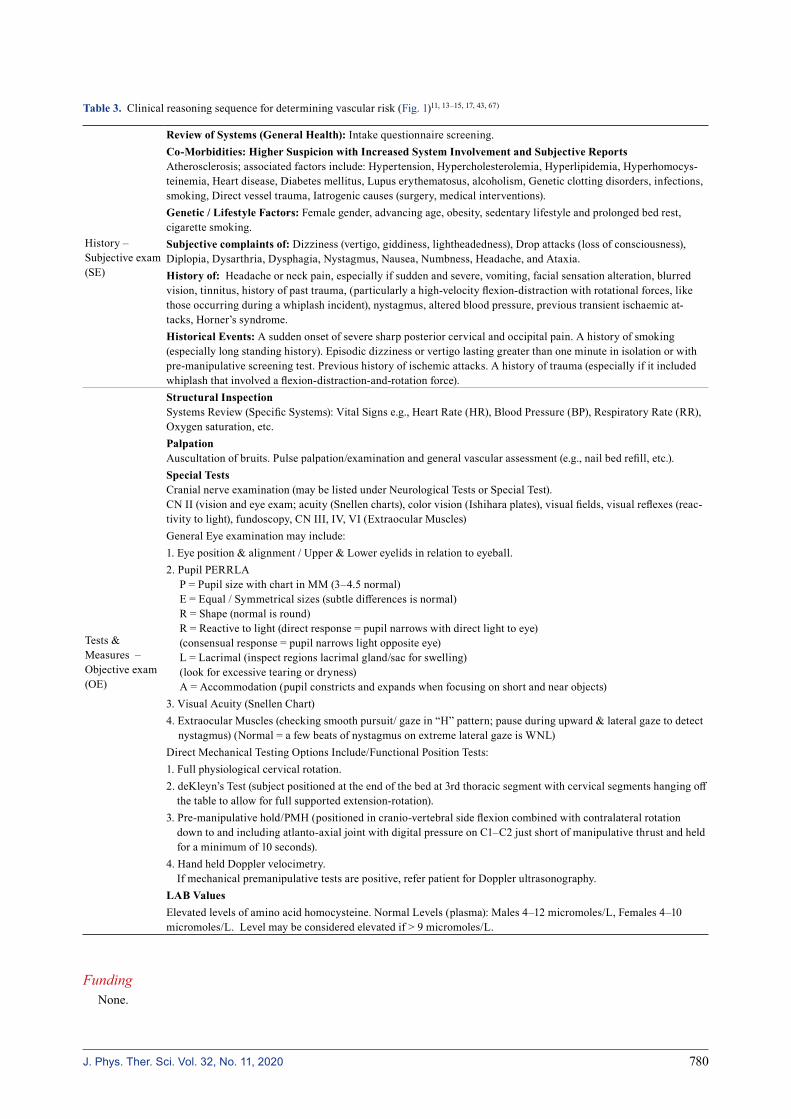
Table 3.Clinicalreasoningsequencefordeterminingvascularrisk(Fig.1)11, 13–15, 17, 43, 67)
History– Subjectiveexam(SE)
Review of Systems (General Health):Intakequestionnairescreening.Co-Morbidities: Higher Suspicion with Increased System Involvement and Subjective ReportsAtherosclerosis;associatedfactorsinclude:Hypertension,Hypercholesterolemia,Hyperlipidemia,Hyperhomocys-teinemia,Heartdisease,Diabetesmellitus,Lupuserythematosus,alcoholism,Geneticclottingdisorders,infections,smoking,Directvesseltrauma,Iatrogeniccauses(surgery,medicalinterventions).Genetic / Lifestyle Factors:Femalegender,advancingage,obesity,sedentarylifestyleandprolongedbedrest,cigarettesmoking.Subjective complaints of:Dizziness(vertigo,giddiness,lightheadedness),Dropattacks(lossofconsciousness),Diplopia,Dysarthria,Dysphagia,Nystagmus,Nausea,Numbness,Headache,andAtaxia.History of:Headacheorneckpain,especiallyifsuddenandsevere,vomiting,facialsensationalteration,blurredvision,tinnitus,historyofpasttrauma,(particularlyahigh-velocityflexion-distractionwithrotationalforces,likethoseoccurringduringawhiplashincident),nystagmus,alteredbloodpressure,previoustransientischaemicat-tacks,Horner’ssyndrome.Historical Events:Asuddenonsetofseveresharpposteriorcervicalandoccipitalpain.Ahistoryofsmoking(especiallylongstandinghistory).Episodicdizzinessorvertigolastinggreaterthanoneminuteinisolationorwithpre-manipulativescreeningtest.Previoushistoryofischemicattacks.Ahistoryoftrauma(especiallyifitincludedwhiplashthatinvolvedaflexion-distraction-and-rotationforce).
Tests& Measures–Objectiveexam(OE)
Structural InspectionSystemsReview(SpecificSystems):VitalSignse.g.,HeartRate(HR),BloodPressure(BP),RespiratoryRate(RR),Oxygensaturation,etc.PalpationAuscultationofbruits.Pulsepalpation/examinationandgeneralvascularassessment(e.g.,nailbedrefill,etc.).Special TestsCranialnerveexamination(maybelistedunderNeurologicalTestsorSpecialTest).CNII(visionandeyeexam;acuity(Snellencharts),colorvision(Ishiharaplates),visualfields,visualreflexes(reac-tivitytolight),fundoscopy,CNIII,IV,VI(ExtraocularMuscles)GeneralEyeexaminationmayinclude:1.Eyeposition&alignment/Upper&Lowereyelidsinrelationtoeyeball.2.PupilPERRLA
P=PupilsizewithchartinMM(3–4.5normal) E=Equal/Symmetricalsizes(subtledifferencesisnormal) R=Shape(normalisround) R=Reactivetolight(directresponse=pupilnarrowswithdirectlighttoeye) (consensualresponse=pupilnarrowslightoppositeeye) L=Lacrimal(inspectregionslacrimalgland/sacforswelling) (lookforexcessivetearingordryness) A=Accommodation(pupilconstrictsandexpandswhenfocusingonshortandnearobjects)
3.VisualAcuity(SnellenChart)4.ExtraocularMuscles(checkingsmoothpursuit/gazein“H”pattern;pauseduringupward&lateralgazetodetectnystagmus)(Normal=afewbeatsofnystagmusonextremelateralgazeisWNL)
DirectMechanicalTestingOptionsInclude/FunctionalPositionTests:1.Fullphysiologicalcervicalrotation.2.deKleyn’sTest(subjectpositionedattheendofthebedat3rdthoracicsegmentwithcervicalsegmentshangingoffthetabletoallowforfullsupportedextension-rotation).
3.Pre-manipulativehold/PMH(positionedincranio-vertebralsideflexioncombinedwithcontralateralrotationdowntoandincludingatlanto-axialjointwithdigitalpressureonC1–C2justshortofmanipulativethrustandheldforaminimumof10seconds).
4.HandheldDopplervelocimetry. Ifmechanicalpremanipulativetestsarepositive,referpatientforDopplerultrasonography.
LAB ValuesElevatedlevelsofaminoacidhomocysteine.NormalLevels(plasma):Males4–12micromoles/L,Females4–10micromoles/L.Levelmaybeconsideredelevatedif>9micromoles/L.
781
Conflict of interest
Theauthorshavenoconflictofintereststodisclose.
REFERENCES
1) CarlessoLC,GrossAR,SantaguidaPL,etal.:Adverseeventsassociatedwiththeuseofcervicalmanipulationandmobilizationforthetreatmentofneckpaininadults:asystematicreview.ManTher,2010,15:434–444.[Medline] [CrossRef]
2) ChungCL,CôtéP,SternP,etal.:Theassociationbetweencervicalspinemanipulationandcarotidarterydissection:asystematicreviewoftheliterature.JManipulativePhysiolTher,2015,38:672–676.[Medline] [CrossRef]
3) DiFabioRP:Manipulationofthecervicalspine:risksandbenefits.PhysTher,1999,79:50–65.[Medline]4) GrantR:Vertebralarterytesting—theAustralianPhysiotherapyAssociationProtocolafter6years.ManTher,1996,1:149–153.[Medline] [CrossRef]5) HaldemanS,KohlbeckFJ,McGregorM:Unpredictabilityofcerebrovascularischemiaassociatedwithcervicalspinemanipulationtherapy:areviewofsixty-
fourcasesaftercervicalspinemanipulation.Spine,2002,27:49–55.[Medline] [CrossRef]6) HanelineMT,CroftAC,FrishbergBM:Associationofinternalcarotidarterydissectionandchiropracticmanipulation.Neurologist,2003,9:35–44.[Medline]
[CrossRef]7) BeattyRA:Dissectinghematomaoftheinternalcarotidarteryfollowingchiropracticcervicalmanipulation.JTrauma,1977,17:248–249.[Medline] [Cross-
Ref]8) HamannG,FelberS,HaasA,etal.:Cervicocephalicarterydissectionsduetochiropracticmanipulations.Lancet,1993,341:764–765.[Medline] [CrossRef]9) LynessSS,WagmanAD:Neurologicaldeficitfollowingcervicalmanipulation.SurgNeurol,1974,2:121–124.[Medline]10) PetersM,BohlJ,ThömkeF,etal.:Dissectionoftheinternalcarotidarteryafterchiropracticmanipulationoftheneck.Neurology,1995,45:2284–2286.
[Medline] [CrossRef]11) TaylorAJ,KerryR:Neckpainandheadacheasaresultofinternalcarotidarterydissection:implicationsformanualtherapists.ManTher,2005,10:73–77.
[Medline] [CrossRef]12) WillettGM,WachholtzNA:Apatientwithinternalcarotidarterydissection.PhysTher,2011,91:1266–1274.[Medline] [CrossRef]13) KerryR,TaylorAJ,MitchellJ,etal.:Manualtherapyandcervicalarterialdysfunction,directionsforthefuture:aclinicalperspective.JManualManipTher,
2008,16:39–48.[Medline] [CrossRef]14) KerryR,TaylorAJ:Cervicalarterialdysfunction:knowledgeandreasoningformanualphysicaltherapists.JOrthopSportsPhysTher,2009,39:378–387.
[Medline] [CrossRef]15) RushtonA,RivettD,CarlessoL,etal.:InternationalframeworkforexaminationofthecervicalregionforpotentialofCervicalArterialDysfunctionpriorto
OrthopaedicManualTherapyintervention.ManTher,2014,19:222–228.[Medline] [CrossRef]16) MagareyME,RebbeckT,CoughlanB,etal.:Pre-manipulativetestingofthecervicalspinereview,revisionandnewclinicalguidelines.ManTher,2004,9:
95–108.[Medline] [CrossRef]17) HarperB:Clinicalreasoningforuppercervicalspinemanipulation:modifiedextensiveliteraturereview.(Doctoraldissertation).OlaGrimsbyInstitute,Salt
LakeCity,UT.2008.18) MitchellJ:Vertebralarteryatherosclerosis:ariskfactorintheuseofmanipulativetherapy?PhysiotherResInt,2002,7:122–135.[Medline] [CrossRef]19) CassidyJD,BoyleE,CôtéP,etal.:Riskofvertebrobasilarstrokeandchiropracticcare:resultsofapopulation-basedcase-controlandcase-crossoverstudy.
Spine,2008,33:S176–S183.[Medline] [CrossRef]20) HartRG,EastonJD:Dissectionsofcervicalandcerebralarteries.NeurolClin,1983,1:155–182.[Medline] [CrossRef]21) LeeVH,BrownRDJr,MandrekarJN,etal.:Incidenceandoutcomeofcervicalarterydissection:apopulation-basedstudy.Neurology,2006,67:1809–1812.
[Medline] [CrossRef]22) MurphyDR:Currentunderstandingoftherelationshipbetweencervicalmanipulationandstroke:whatdoesitmeanforthechiropracticprofession?Chiropr
Osteopat,2010,18:22.[Medline] [CrossRef]23) RothwellDM,BondySJ,WilliamsJI:Chiropracticmanipulationandstroke:apopulation-basedcase-controlstudy.Stroke,2001,32:1054–1060.[Medline]
[CrossRef]24) WhedonJM,SongY,MackenzieTA,etal.:RiskofstrokeafterchiropracticspinalmanipulationinmedicareBbeneficiariesaged66to99yearswithneck
pain.JManipulativePhysiolTher,2015,38:93–101.[Medline] [CrossRef]25) SchievinkWI,MokriB,WhisnantJP:Internalcarotidarterydissectioninacommunity.Rochester,Minnesota,1987–1992.Stroke,1993,24:1678–1680.
[Medline] [CrossRef]26) RosnerAL:Spontaneouscervicalarterydissectionsandimplicationsforhomocysteine.JManipulativePhysiolTher,2004,27:124–132.[Medline] [Cross-
Ref]27) SymonsBP,WestawayM:Virchow’striadandspinalmanipulativetherapyofthecervicalspine.JCanChiroprAssoc,2001,45:225–231.28) BillerJ,SaccoRL,AlbuquerqueFC,etal.AmericanHeartAssociationStrokeCouncil:Cervicalarterialdissectionsandassociationwithcervicalmanipula-
tivetherapy:astatementforhealthcareprofessionalsfromtheAmericanheartassociation/Americanstrokeassociation.Stroke,2014,45:3155–3174.[Medline] [CrossRef]
29) ChaibiA,RussellMB:Arisk-benefitassessmentstrategytoexcludecervicalarterydissectioninspinalmanual-therapy:acomprehensivereview.AnnMed,2019,51:118–127.[Medline] [CrossRef]
30) GrieveGP:Commonvertebraljointproblems.NewYork:ChurchillLivingstoneInc,1981.31) CaillietR:Headandfacepainsyndromes,1sted.Philadelphia:F.A.DavisCompany,1992.32) YamazakiM,OkawaA,FuruyaT,etal.:Anomalousvertebralarteriesintheextra-andintraosseousregionsofthecraniovertebraljunctionvisualizedby
J. Phys. Ther. Sci. Vol. 32, No. 11, 2020 782
3-dimensionalcomputedtomographicangiography:analysisof100consecutivesurgicalcasesandreviewoftheliterature.Spine,2012,37:E1389–E1397.[Medline] [CrossRef]
33) VaněkP,BradáčO,deLacyP,etal.:VertebralarteryandosseousanomaliescharacteristicatthecraniocervicaljunctiondiagnosedbyCTand3DCTangiog-raphyinnormalCzechpopulation:analysisof511consecutivepatients.NeurosurgRev,2017,40:369–376.[Medline] [CrossRef]
34) JohnsonCP,HowT,ScraggsM,etal.:Abiomechanicalstudyofthehumanvertebralarterywithimplicationsforfatalarterialinjury.ForensicSciInt,2000,109:169–182.[Medline] [CrossRef]
35) MacchiC,GiannelliF,CecchiF,etal.:TheinnerdiameterofhumanintracranialvertebralarterybycolorDopplermethod.ItalJAnatEmbryol,1996,101:81–87.[Medline]
36) FrumkinLR,BalohRW:Wallenberg’ssyndromefollowingneckmanipulation.Neurology,1990,40:611–615.[Medline] [CrossRef]37) GeorgeB,LaurianC:Vertebro-basilarischaemiawiththrombosisofthevertebralartery:reportoftwocaseswithembolism.JNeurolNeurosurgPsychiatry,
1982,45:91–93.[Medline] [CrossRef]38) SimE,SchwarzN,Biowski-FaschingI,etal.:Color-codedDuplexsonographyofvertebralarteries.11casesofbluntcervicalspineinjury.ActaOrthopScand,
1993,64:133–137.[Medline] [CrossRef]39) RivettDA,SharplesKJ,MilburnPD:Effectofpremanipulativetestsonvertebralarteryandinternalcarotidarterybloodflow:apilotstudy.JManipulative
PhysiolTher,1999,22:368–375.[Medline] [CrossRef]40) ScheelP,RugeC,SchöningM:Flowvelocityandflowvolumemeasurementsintheextracranialcarotidandvertebralarteriesinhealthyadults:referencedata
andtheeffectsofage.UltrasoundMedBiol,2000,26:1261–1266.[Medline] [CrossRef]41) BarkerS,KessonM,AshmoreJ,etal.:Professionalissue.Guidanceforpre-manipulativetestingofthecervicalspine.ManTher,2000,5:37–40.[Medline]
[CrossRef]42) MageeD:Orthopaedicphysicalassessment,5thed.St.Louis:SaundersElsevier,2008.43) LichtPB,ChristensenHW,Høilund-CarlsenPF:Istherearoleforpremanipulativetestingbeforecervicalmanipulation?JManipulativePhysiolTher,2000,
23:175–179.[Medline] [CrossRef]44) MileyML,WellikKE,WingerchukDM,etal.:Doescervicalmanipulativetherapycausevertebralarterydissectionandstroke?Neurologist,2008,14:66–73.
[Medline] [CrossRef]45) ZainaC,GrantR,JohnsonC,etal.:Theeffectofcervicalrotationonbloodflowinthecontralateralvertebralartery.ManTher,2003,8:103–109.[Medline]
[CrossRef]46) ErhardtJW,WindsorBA,KerryR,etal.:Theimmediateeffectofatlanto-axialhighvelocitythrusttechniquesonbloodflowinthevertebralartery:Arandom-
izedcontrolledtrial.ManTher,2015,20:614–622.[Medline] [CrossRef]47) HerzogW,LeonardTR,SymonsB,etal.:Vertebralarterystrainsduringhigh-speed,lowamplitudecervicalspinalmanipulation.JElectromyogrKinesiol,
2012,22:740–746.[Medline] [CrossRef]48) RivettD,ShirleyD,MagareyM,etal.:APAclinicalguidelinesforassessingvertebrobasilarinsufficiencyinthemanagementofcervicalspinedisorders,2006.
https://www.scribd.com/doc/90011859/APA-VBI-Guidelines(AccessedMay27,2015)49) ArnoldC,BourassaR,LangerT,etal.:Dopplerstudiesevaluatingtheeffectofaphysicaltherapyscreeningprotocolonvertebralarterybloodflow.ManTher,
2004,9:13–21.[Medline] [CrossRef]50) LichtPB,ChristensenHW,HøjgaardP,etal.:Triplexultrasoundofvertebralarteryflowduringcervicalrotation.JManipulativePhysiolTher,1998,21:27–31.
[Medline]51) LiYK,ZhangYK,LuCM,etal.:Changesandimplicationsofbloodflowvelocityofthevertebralarteryduringrotationandextensionofthehead.JManipula-
tivePhysiolTher,1999,22:91–95.[Medline] [CrossRef]52) MitchellJ,KeeneD,DysonC,etal.:Iscervicalspinerotation,asusedinthestandardvertebrobasilarinsufficiencytest,associatedwithameasureablechange
inintracranialvertebralarterybloodflow?ManTher,2004,9:220–227.[Medline] [CrossRef]53) RossitiS,VolkmannR:Changesofbloodflowvelocityindicatingmechanicalcompressionofthevertebralarteriesduringrotationoftheheadinthenormal
humanmeasuredwithtranscranialDopplersonography.ArqNeuropsiquiatr,1995,53:26–33.[Medline] [CrossRef]54) BowlerN,ShamleyD,DaviesR:Theeffectofasimulatedmanipulationpositiononinternalcarotidandvertebralarterybloodflowinhealthyindividuals.Man
Ther,2011,16:87–93.[Medline] [CrossRef]55) HaynesM,MilneN:Colorduplexsonographicfindingsinhumanvertebralarteriesduringcervicalrotation.JClinUltrasound,2001,29:14–24.[Medline]
[CrossRef]56) QuesneleJJ,TrianoJJ,NoseworthyMD,etal.:Changesinvertebralarterybloodflowfollowingvariousheadpositionsandcervicalspinemanipulation.J
ManipulativePhysiolTher,2014,37:22–31.[Medline] [CrossRef]57) ThielH,WallaceK,DonatJ,etal.:Effectofvariousheadandneckpositionsonvertebralarterybloodflow.ClinBiomech(Bristol,Avon),1994,9:105–110.
[Medline] [CrossRef]58) ThomasLC,RivettDA,BatemanG,etal.:Effectofselectedmanualtherapyinterventionsformechanicalneckpainonvertebralandinternalcarotidarterial
bloodflowandcerebralinflow.PhysTher,2013,93:1563–1574.[Medline] [CrossRef]59) ThomasLC,McLeodLR,OsmotherlyPG,etal.:Theeffectofend-rangecervicalrotationonvertebralandinternalcarotidarterialbloodflowandcerebral
inflow:asubanalysisofanMRIstudy.ManTher,2015,20:475–480.[Medline] [CrossRef]60) ChildsJD,FlynnTW,FritzJM,etal.:Screeningforvertebrobasilarinsufficiencyinpatientswithneckpain:manualtherapydecision-makinginthepresence
ofuncertainty.JOrthopSportsPhysTher,2005,35:300–306.[Medline] [CrossRef]61) HerzogW,TangC,LeonardT:Internalcarotidarterystrainsduringhigh-speed,low-amplitudespinalmanipulationsoftheneck.JManipulativePhysiolTher,
2015,38:664–671.[Medline] [CrossRef]62) WuestS,SymonsB,LeonardT,etal.:Preliminaryreport:biomechanicsofvertebralarterysegmentsC1–C6duringcervicalspinalmanipulation.JManipula-
tivePhysiolTher,2010,33:273–278.[Medline] [CrossRef]63) CôtéP,KreitzBG,CassidyJD,etal.:Thevalidityoftheextension-rotationtestasaclinicalscreeningprocedurebeforeneckmanipulation:asecondaryanaly-
sis.JManipulativePhysiolTher,1996,19:159–164.[Medline]
783
64) ThielH,RixG:Isittimetostopfunctionalpre-manipulationtestingofthecervicalspine?ManTher,2005,10:154–158.[Medline] [CrossRef]65) DunningJ,ButtsR,JuntillaU:Pre-manipulativetestingpriortocervicalmanipulation:timetoabandontheVBItest?2015.https://osteopractor.wordpress.
com/2015/01/08/pre-manipulative-testing-prior-to-cervical-manipulation-time-to-abandon-the-vbi-test/.66) SymonsBP,LeonardT,HerzogW:Internalforcessustainedbythevertebralarteryduringspinalmanipulativetherapy.JManipulativePhysiolTher,2002,25:
504–510.[Medline] [CrossRef]67) TaylorAJ,KerryR:A“systembased”approachtoriskassessmentofthecervicalspinepriortomanualtherapy.IntJOsteopathMed,2010,13:85–93.[Cross-
Ref]


















