
Review Article Osteosarcoma -...
13
Osteosarcoma Abstract Osteosarcoma, the most common bone sarcoma, affects approximately 560 children and adolescents annually in the United States. The incidence of new diagnoses peaks in the second decade of life. Twenty percent of patients present with clinically detectable metastases, with micrometastases presumed to be present in many of the remaining patients. Treatment typically includes preoperative chemotherapy, surgical resection, and postoperative chemotherapy. Limb-salvage procedures with wide surgical margins are the mainstay of surgical intervention. Advances in chemotherapy protocols have led to a 5-year survival rate of 60% to 78%. Among the goals of future treatment regimens are improved chemotherapeutic agents with higher specificity and lower toxicity. O steosarcoma, the most com- mon bone sarcoma, is charac- terized by production of both osteoid and bone by malignant spindle cells. The disease affects approximately 560 children and adolescents each year in the United States. 1 The inci- dence of osteosarcoma peaks in the second decade of life during periods of rapid bone turnover, such as the adolescent growth spurt. 2,3 Osteosar- coma most commonly develops at sites of rapid bone turnover, such as the distal femur, proximal tibia, and proximal humerus. 3,4 Most cases of osteosarcoma are spo- radic, with relatively few associated with known inherited defects in cell cycle regulation. Even so, approxi- mately 70% of osteosarcoma tumor specimens demonstrate a chromosomal abnormality. 2 Genetic predisposition commonly involves mutations in tumor-suppressor genes or in DNA helicases. Tumor-suppressor genes normally regulate the cell cycle; mu- tations will result in uncontrolled cell proliferation as seen in Li-Fraumeni syndrome, involving the p53 gene, or retinoblastoma, involving the RB1 gene. 2,5 DNA helicases unwind double-stranded DNA for replication and alteration of these genes, as seen in the BLM and RECQL4 genes, re- sulting in Bloom syndrome and Rothmund-Thomson syndrome, re- spectively. 2,5 More than 85% of osteosarcoma cases are categorized as primary os- teosarcoma, a de novo disease process of bone. 6 Osteosarcoma is subcate- gorized, based on clinical, radio- graphic, and histologic features, into intramedullary subtypes (ie, conven- tional, telangiectatic, low-grade in- tramedullary, small-cell) and surface subtypes (ie, parosteal, periosteal, high-grade surface). Patient Evaluation History and Physical Examination Individuals with osteosarcoma usu- ally present with nonspecific symp- toms, most commonly new-onset, strain-related pain of several months’ Patrick J. Messerschmitt, MD Ryan M. Garcia, MD Fadi W. Abdul-Karim, MD Edward M. Greenfield, MD Patrick J. Getty, MD Dr. Messerschmitt is Resident, Department of Orthopaedic Surgery, University Hospitals Case Medical Center, Case Western Reserve University, Cleveland, OH. Dr. Garcia is Resident, Department of Orthopaedic Surgery, University Hospitals Case Medical Center, Case Western Reserve University. Dr. Abdul-Karim is Professor, Department of Pathology, University Hospitals Case Medical Center, Case Western Reserve University. Dr. Greenfield is Professor and Director of Orthopaedic Research, Department of Orthopaedic Surgery, University Hospitals Case Medical Center, Case Western Reserve University. Dr. Getty is Assistant Professor and Director of Graduate Orthopaedic Education, Department of Orthopaedic Surgery, University Hospitals Case Medical Center, Case Western Reserve University, Director of Musculoskeletal Oncology, Ireland Cancer Center, Cleveland, OH, and Medical Director, Department of Orthopaedic Oncology, Louis Stokes VA Hospital of Cleveland, Cleveland, OH. Reprint requests: Dr. Messerschmitt, Department of Orthopaedic Surgery, University Hospitals Case Medical Center, Case Western Reserve University, 6th Floor Hanna House, 11100 Euclid Avenue, Cleveland, OH 44106. J Am Acad Orthop Surg 2009;17: 515-527 Copyright 2009 by the American Academy of Orthopaedic Surgeons. Review Article August 2009, Vol 17, No 8 515
Transcript of Review Article Osteosarcoma -...

Osteosarcoma
Abstract
Osteosarcoma, the most common bone sarcoma, affectsapproximately 560 children and adolescents annually in the UnitedStates. The incidence of new diagnoses peaks in the seconddecade of life. Twenty percent of patients present with clinicallydetectable metastases, with micrometastases presumed to bepresent in many of the remaining patients. Treatment typicallyincludes preoperative chemotherapy, surgical resection, andpostoperative chemotherapy. Limb-salvage procedures with widesurgical margins are the mainstay of surgical intervention.Advances in chemotherapy protocols have led to a 5-year survivalrate of 60% to 78%. Among the goals of future treatment regimensare improved chemotherapeutic agents with higher specificity andlower toxicity.
Osteosarcoma, the most com-mon bone sarcoma, is charac-
terized by production of both osteoidand bone by malignant spindle cells.The disease affects approximately560 children and adolescents eachyear in the United States.1 The inci-dence of osteosarcoma peaks in thesecond decade of life during periodsof rapid bone turnover, such as theadolescent growth spurt.2,3 Osteosar-coma most commonly develops atsites of rapid bone turnover, such asthe distal femur, proximal tibia, andproximal humerus.3,4
Most cases of osteosarcoma are spo-radic, with relatively few associatedwith known inherited defects in cellcycle regulation. Even so, approxi-mately 70% of osteosarcoma tumorspecimens demonstrate a chromosomalabnormality.2 Genetic predispositioncommonly involves mutations intumor-suppressor genes or in DNAhelicases. Tumor-suppressor genesnormally regulate the cell cycle; mu-tations will result in uncontrolled cellproliferation as seen in Li-Fraumenisyndrome, involving the p53 gene,
or retinoblastoma, involving theRB1 gene.2,5 DNA helicases unwinddouble-stranded DNA for replicationand alteration of these genes, as seenin the BLM and RECQL4 genes, re-sulting in Bloom syndrome andRothmund-Thomson syndrome, re-spectively.2,5
More than 85% of osteosarcomacases are categorized as primary os-teosarcoma, a de novo disease processof bone.6 Osteosarcoma is subcate-gorized, based on clinical, radio-graphic, and histologic features, intointramedullary subtypes (ie, conven-tional, telangiectatic, low-grade in-tramedullary, small-cell) and surfacesubtypes (ie, parosteal, periosteal,high-grade surface).
Patient Evaluation
History and PhysicalExaminationIndividuals with osteosarcoma usu-ally present with nonspecific symp-toms, most commonly new-onset,strain-related pain of several months’
Patrick J. Messerschmitt, MD
Ryan M. Garcia, MD
Fadi W. Abdul-Karim, MD
Edward M. Greenfield, MD
Patrick J. Getty, MD
Dr. Messerschmitt is Resident,Department of Orthopaedic Surgery,University Hospitals Case MedicalCenter, Case Western ReserveUniversity, Cleveland, OH.Dr. Garcia is Resident, Departmentof Orthopaedic Surgery, UniversityHospitals Case Medical Center,Case Western Reserve University.Dr. Abdul-Karim is Professor,Department of Pathology, UniversityHospitals Case Medical Center,Case Western Reserve University.Dr. Greenfield is Professor andDirector of Orthopaedic Research,Department of Orthopaedic Surgery,University Hospitals Case MedicalCenter, Case Western ReserveUniversity. Dr. Getty is AssistantProfessor and Director of GraduateOrthopaedic Education, Departmentof Orthopaedic Surgery, UniversityHospitals Case Medical Center,Case Western Reserve University,Director of MusculoskeletalOncology, Ireland Cancer Center,Cleveland, OH, and MedicalDirector, Department of OrthopaedicOncology, Louis Stokes VA Hospitalof Cleveland, Cleveland, OH.
Reprint requests: Dr. Messerschmitt,Department of Orthopaedic Surgery,University Hospitals Case MedicalCenter, Case Western ReserveUniversity, 6th Floor Hanna House,11100 Euclid Avenue, Cleveland,OH 44106.
J Am Acad Orthop Surg 2009;17:515-527
Copyright 2009 by the AmericanAcademy of Orthopaedic Surgeons.
Review Article
August 2009, Vol 17, No 8 515

duration.7 This pain may disruptsleep. On examination, a visible orpalpable mass in the affected area,decreased joint motion, or localizedwarmth or erythema may be present.Approximately 5% to 10% of undi-agnosed patients with osteosarcomapresent with a pathologic fracture.8
Late signs of the disease include
weight loss, fever, and general mal-aise.
ImagingAt least two orthogonal radiographicviews are required of any suspectedbone lesion. Radiographs classicallydemonstrate an aggressive bone le-sion arising from the metaphysis of
the distal femur, proximal tibia, orproximal humerus.4 Less commonsites for osteosarcoma include thepelvis, the spine, and the craniofacialbones. The lesion typically has ill-defined borders, osteoblastic and/orosteolytic features, and an associatedsoft-tissue mass (Figure 1).
Advanced imaging is warranted inthe setting of osteosarcoma. MRI isthe primary mode of evaluation andcan clearly demonstrate the extent oftumor invasion of the surroundingsoft tissues, neurovascular involve-ment, extent of bone marrow re-placement, and presence of discon-tinuous metastases (ie, skip lesions)(Figure 2). Local anatomy is bestdemonstrated on axial images. Thesecan be used to assess the possibilityof limb salvage. CT is not essential,but it may be helpful in demonstrat-ing cortical integrity, the presence offracture, neurovascular involvement,and mineralization.
BiopsyThe diagnosis of osteosarcoma requirestissue biopsy to provide histopathologicexamination of the lesion, so as to con-firm the clinical and radiographic im-pression (Figure 3). The biopsy siteshould be selected with considerationfor definitive tumor resection. Tumorresection must include the biopsy tractalong with the tumor mass because thetract could be contaminated with tumorcells.
Osteosarcoma Subtypesand Characteristics
Intramedullary
ConventionalConventional, or “classic,” osteosar-coma is the most prevalent variant
AP (A) and lateral (B) radiographs of the knee demonstrating commonradiographic features of conventional osteosarcoma: metaphyseal region ofthe distal femur (arrow), lytic and blastic bone lesion with ill-defined borders(arrowhead), and associated expansion into the soft tissues (arrowhead).C, Lateral photograph of a gross specimen revealing the mass replacingmarrow and extending into soft tissue (arrow). D, High-powerphotomicrograph demonstrating malignant mesenchymal cells withpleomorphic nuclei and osteoid (hematoxylin-eosin, original magnification×200).
Figure 1
None of the following authors or a member of their immediate families has received anything of value from or owns stock in acommercial company or institution related directly or indirectly to the subject of this article: Dr. Messerschmitt, Dr. Garcia, Dr. Abdul-Karim, Dr. Greenfield, and Dr. Getty.
Osteosarcoma
516 Journal of the American Academy of Orthopaedic Surgeons

(constituting 80% of all osteosar-coma cases) and primarily affectspersons in the first or second decadeof life.3 Conventional osteosarcomais typically high-grade and originatesin the intramedullary cavity. Plain ra-diographs demonstrate an osteolyticand/or osteoblastic bone lesion withcortical destruction (Figure 1, A andB). The metaphysis of long bones isthe primary site in >80% of cases,but tumors may also arise in the di-aphysis of long bones or the axialskeleton4 (Figure 1, C).
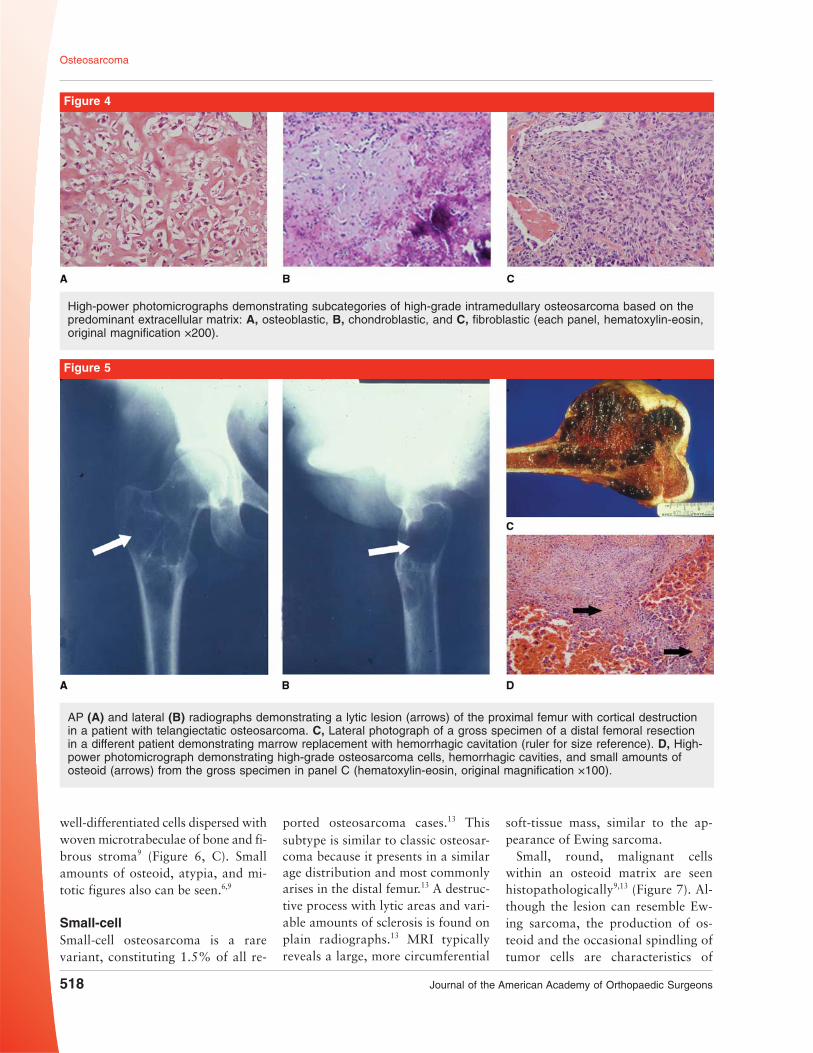
Histopathologic examination dem-onstrates malignant mesenchymalcells, spindle to polyhedral in shape,with pleomorphic nuclei and occa-sional mitotic figures6,9 (Figure 1, D).Evidence of bone or osteoid produc-tion on histopathologic evaluation iscrucial for diagnosis.9 The WorldHealth Organization further subcate-gorizes high-grade intramedullaryosteosarcoma based on the predomi-nant extracellular matrix produced
by the tumor: osteoblastic (boneand/or osteoid, 50% of cases), chon-droblastic (high-grade hyaline carti-lage, 25% of cases), or fibroblastic(high-grade spindle cells, 25% ofcases)6 (Figure 4).
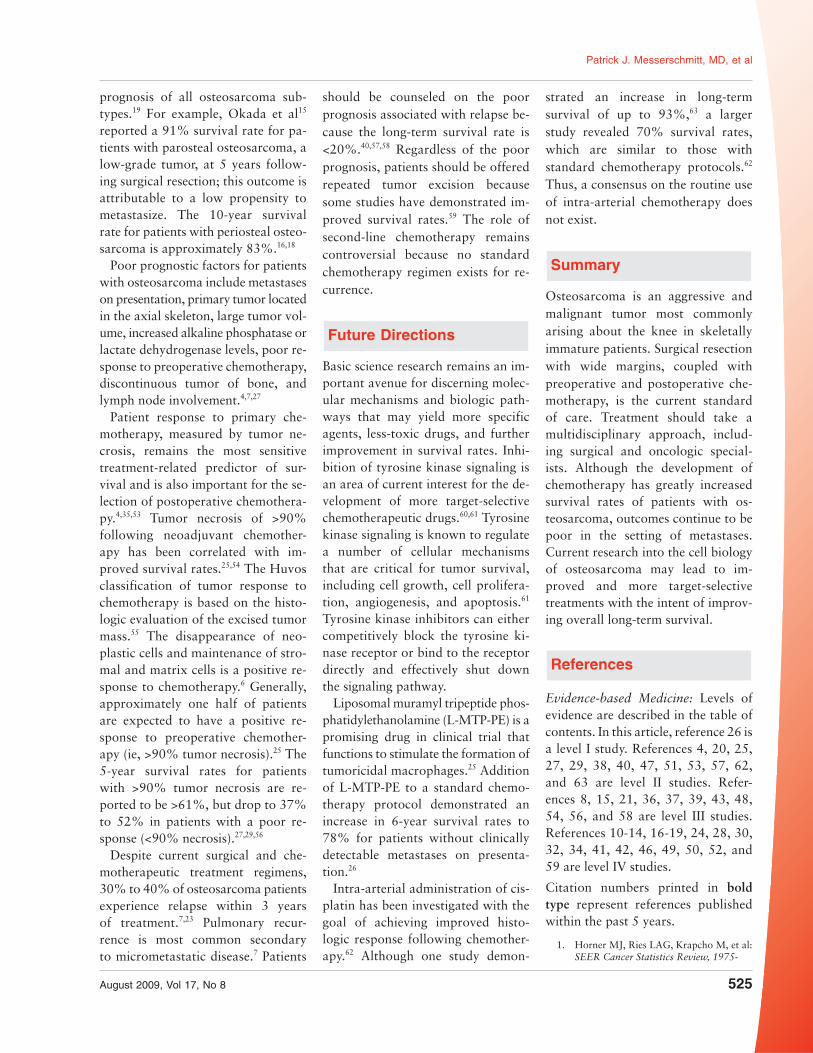
TelangiectaticTelangiectatic osteosarcoma ac-counts for <4% of all osteosarcomacases, most of which arise in childrenand adolescents.6 Twenty-five per-cent of patients with telangiectaticosteosarcoma present with a patho-logic fracture.10 Radiographic imag-ing demonstrates an eccentric andosteolytic lesion expanding or dis-rupting the metaphyseal surface ofthe distal femur or proximal tibia;the lesion may resemble an aneurys-mal bone cyst11 (Figure 5). The lesionis composed of multiple blood-filledsinusoids, which can be easily de-tected as high signal intensity on T2-weighted MRI scans.
Histopathologic examination reveals
the tumor to be composed of multipledilated hemorrhagic cavities, smallamounts of osteoid, and high-grade os-teosarcoma cells, found within thesepta6,9 (Figure 5, D). Foci of giant cellsare occasionally found.9 The overallhistologic appearance may mimicthat of an aneurysmal bone cyst;however, the septa of telangiectaticosteosarcoma will clearly demon-strate high-grade sarcoma cells.
Low-gradeLow-grade intramedullary osteosar-coma constitutes 1% to 2% of all os-teosarcomas and generally affects in-dividuals in the third or fourthdecade.6,12 Lesions commonly involvethe femur and tibia about the knee.12
Radiographic examination revealsa relatively unaggressive-appearinglytic, mixed lytic-blastic, or blasticprocess–appearing fibro-osseous le-sion with varying amounts of septalossification and sclerosis12 (Figure 6,A). The tumor can resemble fibrousdysplasia, but MRI or CT will usu-ally demonstrate cortical violation.12
Histologic evaluation demonstrates
Coronal T2-weighted short tau inversion recovery MRI scan (A) and axialT1-weighted postgadolinium MRI scan with fat saturation (B) demonstratingconventional osteosarcoma of the distal femur with epiphyseal involvement ina 10-year-old patient. Axial slices are helpful in identifying neurovascularinvolvement.
Figure 2
Axial CT scan of the distal femurduring CT-guided core needlebiopsy in a patient with suspectedosteosarcoma. Extraosseouslocation of the core needle isrequired to avoid cortical violationand subsequent predisposition tofracture.
Figure 3
Patrick J. Messerschmitt, MD, et al
August 2009, Vol 17, No 8 517
well-differentiated cells dispersed withwoven microtrabeculae of bone and fi-brous stroma9 (Figure 6, C). Smallamounts of osteoid, atypia, and mi-totic figures also can be seen.6,9
Small-cellSmall-cell osteosarcoma is a rarevariant, constituting 1.5% of all re-
ported osteosarcoma cases.13 Thissubtype is similar to classic osteosar-coma because it presents in a similarage distribution and most commonlyarises in the distal femur.13 A destruc-tive process with lytic areas and vari-able amounts of sclerosis is found onplain radiographs.13 MRI typicallyreveals a large, more circumferential
soft-tissue mass, similar to the ap-pearance of Ewing sarcoma.
Small, round, malignant cellswithin an osteoid matrix are seenhistopathologically9,13 (Figure 7). Al-though the lesion can resemble Ew-ing sarcoma, the production of os-teoid and the occasional spindling oftumor cells are characteristics of
High-power photomicrographs demonstrating subcategories of high-grade intramedullary osteosarcoma based on thepredominant extracellular matrix: A, osteoblastic, B, chondroblastic, and C, fibroblastic (each panel, hematoxylin-eosin,original magnification ×200).
Figure 4
AP (A) and lateral (B) radiographs demonstrating a lytic lesion (arrows) of the proximal femur with cortical destructionin a patient with telangiectatic osteosarcoma. C, Lateral photograph of a gross specimen of a distal femoral resectionin a different patient demonstrating marrow replacement with hemorrhagic cavitation (ruler for size reference). D, High-power photomicrograph demonstrating high-grade osteosarcoma cells, hemorrhagic cavities, and small amounts ofosteoid (arrows) from the gross specimen in panel C (hematoxylin-eosin, original magnification ×100).
Figure 5
Osteosarcoma
518 Journal of the American Academy of Orthopaedic Surgeons

small-cell osteosarcoma.9 Similar toEwing sarcoma, small-cell osteosar-coma stains positive for CD99.9 Dis-tinguishing small-cell osteosarcomafrom Ewing sarcoma or malignantlymphoma can be difficult based onhistology alone; thus, diagnosis ne-cessitates ancillary studies.
SurfaceParostealSurface osteosarcomas arise on thesurface of long bones, sparing themedullary canal.9,14 The peak inci-dence is during the third decade oflife, and the disease affects more fe-males than males.9,14,15 Parosteal os-teosarcoma, the most common juxta-cortical variety, constitutes 1% to6% of all osteosarcoma cases.6,9,14
Parosteal osteosarcomas arise fromthe outer surface of metaphysealbone, and radiographic analysis clas-sically shows a densely ossified andlobulated mass on the posterior as-pect of the distal femur, with sparingof the medullary cavity15 (Figure 8, Athrough C). Large tumors may encir-cle the bone. Parosteal osteosarcomais slow-growing.
Parosteal osteosarcoma demonstratesa low-grade, well-differentiated fi-brous stroma with osseous componentson histopathologic examination6,9
(Figure 8, D). The presence of bonytrabeculae with a parallel orientationand a “pulled steel wool” pattern iscommon.9 Approximately 25% to30% of these tumors will show anadditional cartilaginous differentia-tion cap (Figure 8, E).9
PeriostealPeriosteal osteosarcoma constitutes1% to 2% of all osteosarcoma cas-es.6,16 This juxtacortical tumor ismore aggressive than the parostealvariant. Radiographic imaging re-veals a radiolucent mass, usuallysparing the medullary cavity; themass commonly is located on theproximal tibia or distal femur.16-18 Asunburst appearance or a Codmantriangle is commonly seen with peri-osteal osteosarcoma17 (Figure 9, A).Histopathologic evaluation demon-strates an intermediate-grade tumorthat contains a mostly cartilaginousmatrix with areas of calcification9
(Figure 9, B). Generally, small amountsof osteoid are seen.17
High-gradeHigh-grade surface osteosarcomaconstitutes <1% of all osteosarco-mas.6 This surface tumor typicallyarises on the femur or tibia; radio-graphic analysis shows a surface le-sion with partial mineralization andtumor extension into the surround-ing soft tissues.19 Disruption of theunderlying cortex is often evident.Histologic examination reveals high-grade spindle cells with atypia and
AP radiograph (A) and coronal section of a gross specimen (B) of the distal femur demonstrating a fibro-osseouslesion with cortical violation in a patient with low-grade intramedullary osteosarcoma. C, Low-power photomicrographrevealing well-differentiated cells dispersed among woven bone trabeculae and small amounts of osteoid (hematoxylin-eosin, original magnification ×40).
Figure 6
High-power photomicrographdemonstrating small, round, bluecells with osteoid in a patient withmalignant small-cell osteosarcoma(hematoxylin-eosin, originalmagnification ×400).
Figure 7
Patrick J. Messerschmitt, MD, et al
August 2009, Vol 17, No 8 519

varying amounts of osteoid.9,19 Histo-logically, the appearance is similar tothat of conventional osteosarcoma.
Laboratory Tests
Laboratory tests are not diagnosticfor osteosarcoma but are helpfulonce a diagnosis has been estab-lished. Baseline laboratory valuesshould be obtained to assess organfunction before the initiation of pre-operative chemotherapy. These in-clude complete blood count with dif-ferential, basic metabolic panel,
renal and liver function values, andurinalysis. Baseline cardiac functionwith echocardiography should be es-tablished before doxorubicin therapyis begun. Alkaline phosphatase andlactate dehydrogenase levels can beobtained to assess for increased os-teoblastic and osteoclastic activity,respectively; elevated levels are asso-ciated with a poorer prognosis.7,20,21
Staging
The National Comprehensive CancerNetwork recommends plain radio-
graphs, MRI scan of the extremity,CT scan of the chest, and bone scan(with or without positron-emissiontomography [PET] scan) in the pa-tient with suspected osteosarcoma.22
CT scan of the chest is more sensitivethan chest radiography in detectingpulmonary metastasis and should beperformed in all patients with os-teosarcoma. Chest CT is useful inevaluating for pulmonary metastasesand serves as a baseline study withwhich to follow response to chemo-therapy or to evaluate future relapse.Pulmonary metastases will appear as
A, Lateral radiograph demonstrating a densely ossified and lobulated bone lesion on the posterior aspect of the distalfemur in a patient with parosteal osteosarcoma. Axial radiograph (B) and axial section (C) of a gross specimen of thedistal femur demonstrating a highly lobulated bone lesion with sparing of the medullary canal. D, High-power photomi-crograph demonstrating well-differentiated fibrous stroma and bony trabeculae with a parallel orientation and a “pulledsteel wool” pattern (hematoxylin-eosin, original magnification ×100). E, High-power photomicrograph demonstrating well-differentiated fibrous stroma and a cartilaginous cap (hematoxylin-eosin, original magnification ×100).
Figure 8
Osteosarcoma
520 Journal of the American Academy of Orthopaedic Surgeons

small, round, dense nodules, oftenwith central calcification.23 Meta-static nodules commonly arise in theperiphery of the lungs but may alsooccur centrally.23
Radionuclide bone scan with tech-netium Tc-99 methylene diphospho-nate scintigraphy will reveal in-creased metabolic activity at the siteof tumor and is useful in detectingdiscontinuous tumor and distant me-tastases. Abnormal findings on bonescan warrant further imaging withplain radiographs. Advanced imag-ing such as CT and MRI is necessarywhen discontinuous tumor or distantmetastases require further character-ization.
PET has not been used frequentlyto evaluate osteosarcoma. Interest inthe use of PET scans both for stagingosteosarcoma and monitoring treat-ment is increasing. The ultimate util-ity of PET remains to be determined.
The Enneking system for stagingmalignant bone tumors, includingosteosarcoma, is the most recognizedmethod.24 This system establishes tu-mor grade (ie, low, high), site or ex-tension (ie, intracompartmental, ex-tracompartmental), and the presence
or absence of metastases (Table 1).Most patients with osteosarcoma arestaged as Enneking IIB.23 An alterna-tive method for staging malignantbone tumors was established by theAmerican Joint Committee on Can-cer; it assesses tumor size (≤8 cm or>8 cm), lymph node involvement,and distant metastases.22
The spread of osteosarcoma cellsto distant sites usually occurs he-matogenously. Metastases are clini-cally detectable in approximately20% of patients on initial presenta-tion.4,25,26 Compared with patientswith localized disease, patients withmetastatic disease are more likely tohave axial-located tumors, large tu-mors, or a longer history of symp-toms.4 The most common site of me-tastases (80% to 85%) is the lungs4,27
(Figure 10); metastases to bone is thesecond most common course.4 Dis-tant bone lesions and sites of discon-tinuous tumor can occur in 1% to10% of patients with other metasta-ses.4,27,28 Rare sites of metastases in-cludes the liver, lymph nodes, centralnervous system, adrenal glands, mus-cle, and skin.27
Treatment
A multidisciplinary approach isneeded in the treatment of patientswith osteosarcoma, including surgi-cal and oncologic specialists. Forpatients without metastatic disease,survival rates surpass 70% whena multidisciplinary approach isused.3,4,26,29 For high-grade osteosar-coma, treatment consists of preoper-ative (ie, neoadjuvant) chemother-apy, wide surgical resection, andpostoperative chemotherapy (ie, ad-juvant). Patients without clinicallydetectable metastases are presumedto have micrometastases and are
A, AP section of a gross specimen (top) and AP radiograph (bottom) of the proximal femur demonstrating a radiolucentbone lesion in a patient with periosteal osteosarcoma. A sunburst appearance is appreciable. B, High-powerphotomicrograph demonstrating a high-grade tumor with cartilaginous components and small amounts of osteoid(hematoxylin-eosin, original magnification ×100).
Figure 9
Table 1
Enneking System for StagingMalignant Bone Tumors24
Stage Grade Site
IA Low IntracorticalIB Low ExtracorticalIIA High IntracorticalIIB High ExtracorticalIII Any Metastases
Patrick J. Messerschmitt, MD, et al
August 2009, Vol 17, No 8 521

treated with preoperative and post-operative chemotherapy.3 Patientswith parosteal osteosarcoma or low-grade intramedullary osteosarcomaare treated with wide surgical resec-tion; chemotherapy is reserved forcases of high-grade transformation.3
Periosteal osteosarcoma may betreated with preoperative chemother-apy similar to that used for conven-tional osteosarcoma30 or with intra-arterial chemotherapy.22
ChemotherapyThe primary goal of preoperative che-motherapy is to treat detectable me-tastases or presumed micrometastases.Chemotherapy may also decrease thesize of the primary tumor by reducingits neovascularity, thus making limb-salvage surgery technically more feasi-ble by promoting tumor demarcationfrom surrounding tissues.31-33 The
chemotherapeutic agents that aremost effective in the treatment ofosteosarcoma include doxorubicin,cisplatin, methotrexate, and ifos-famide.3,23,26,29 Combining multipledrugs serves to avoid chemoresis-tance and to increase the degree oftumor necrosis.34 The National Can-cer Institute supports ongoing coop-erative trial groups consisting of re-searchers, physicians, and cancercenters to explore new chemothera-peutic agents, groups in which allchildren with osteosarcoma may beenrolled.35
Surgical resection of the primary os-teosarcoma is generally performed 3 to4 weeks after the last dose of preoper-ative chemotherapy. Delaying surgicalresection from the time of diagnosis hasnot been shown to adversely affect pa-tient survival.4 Postoperative chemo-therapy is begun 2 weeks after surgi-cal resection, provided that thesurgical wound has completelyhealed. The postoperative chemo-therapeutic regimen is typically thesame as the preoperative regimenwhen tumor necrosis is found to be≥90% at the time of surgery.
Poor responders to preoperativechemotherapy, defined as those with<90% tumor necrosis at the time ofsurgery, may still benefit from post-operative chemotherapy.36 In these
cases, a salvage therapeutic regimenis attempted with an increased doseof chemotherapy, an increased lengthof chemotherapy, or a change in che-motherapeutic agents. However, nei-ther changing chemotherapy drugsnor increasing the dose in salvage at-tempts has been shown to improvesurvival in poor responders to preop-erative chemotherapy.29,37 The role ofradiation therapy in the treatment ofosteosarcoma is limited to palliationbecause this neoplasm is highly resis-tant to radiation.
SurgerySurgical resection of all clinically de-tectable tumor, including metastases,is the cornerstone of treatment of os-teosarcoma. The two primary surgi-cal options are tumor excision withlimb salvage, and amputation. Surgi-cal margins in excision should en-compass resection of tumor, pseudo-capsule, and a cuff of normal tissueen bloc (Table 2). Axial images onMRI or CT scan are helpful in creat-ing a surgical plan and in delineatingthe extent of the tumor as well as in-volvement of the neurovascularstructures.
The current treatment recommen-dation for detectable metastases is toexcise as many lesions as technicallyfeasible following surgical treatment
Axial CT scans of the chest demonstrating multiple sites of pulmonary metastases (arrows) in a 10-year-old patient withconventional osteosarcoma at the midthoracic level (A) and the low thoracic level (B). C, Gross lung tissue specimenwith metastatic nodules.
Figure 10
Table 2
Surgical Margins for TumorResection
Type Plane of Dissection
Intralesional Within lesionMarginal Within reactive zoneWide Through normal tissue,
beyond reactive zoneRadical Extracompartmental
Osteosarcoma
522 Journal of the American Academy of Orthopaedic Surgeons

of the primary tumor. Long-term sur-vival has a fivefold increase withcomplete resection of both primaryand metastatic sites compared withexcision of the primary tumoralone.27 The survival rate for patientswith a solitary lung metastasis can beas high as 75% when both the pri-mary tumor and solitary lung noduleare adequately resected.27,38
Prior to the emergence of limb-salvage surgery in the 1970s, am-putation of the affected limb wasconsidered the definitive surgical in-tervention. Amputation remains theindicated treatment when resectionto disease-free margins leaves a non-functional limb. Better local controlmay be achieved with amputationcompared with limb-salvage surgerywhen extensive contamination isfound at the time of biopsy.
When deciding between amputa-tion and limb-salvage surgery, it isimportant to consider postoperativelimb function, potential complica-tions, emotional impact, and differ-ences in oncologic outcomes. In casesin which a prosthesis functions betterthan the salvaged limb, amputationshould be discussed. Studies haveshown that patients adapt equallywell psychologically whether theyundergo an amputation or a limb-salvage procedure.7,39 Most impor-tant, no significant difference existsbetween the survival rates for ampu-tation and limb-salvage surgery.31,40,41
The emergence of limb-salvage sur-gery as an option for patients withosteosarcoma is attributable to theuse of preoperative chemotherapyand to advancements in musculoskel-etal imaging, prosthetic implant de-sign, and surgical technique. Limb-salvage surgery is possible for >85%of appendicular osteosarcoma.31 Thegoal of limb salvage is to preserve afunctioning limb without increasingthe risk of tumor recurrence. A vari-ety of reconstructions can be usedfor limb salvage, including arthrode-
sis, prosthetic implantation, osteoar-ticular allografting, and an allograft/prosthetic composite. Absolute andrelative contraindications for limb-salvage surgery include the inabilityto obtain wide surgical margins, neu-rovascular involvement, and patho-logic fracture.8 The rate of surgicalsite tumor recurrence is 4% to 6%for both limb salvage and amputa-tion.29,40
Following intra-articular resection,several surgical options to reconstructthe deficient joint are available: en-doprosthesis, allograft-prosthetic com-posite, osteoarticular allograft, and ar-throdesis. An endoprosthesis may beused to reconstruct an articular joint;this has the advantage of providing im-mediate skeletal stability and inherentjoint stability (Figure 11). A recentstudy of patients at a mean follow-upof 15 years demonstrated that revisionsurgery for endoprosthetic reconstruc-tion was necessitated most commonlyby mechanical failure (18% of patients)and infection (11% of patients).42 Anallograft-prosthetic composite maybe used to provide immediate struc-tural stability while allowing for thepotential biologic benefits of al-lograft bone. An osteoarticular al-lograft can be used to reconstruct thejoint surface using both native andallograft soft-tissue attachments tocreate adequate stability. Failurerates of osteoarticular allografts canbe high, with fractures occurring in17% to 20% of cases.43,44 Osteoartic-ular allograft failure can involvenonunion and infection as well, typi-cally occurring within 3 years of re-construction.44 Arthrodesis is a via-ble and durable option and can becompleted with autograft and/or al-lograft bone and internal fixation.
Limb reconstruction can be challeng-ing in the skeletally immature patient,for whom the goal is creating a func-tional limb while avoiding limb-lengthdiscrepancy. Most osteosarcomas affectthe metaphyseal region, and surgical re-
section often damages or removes thephysis.45 To counteract limb-lengthdiscrepancy, bone lengthening can beaccomplished with an extendible en-doprosthesis. The endoprosthesis al-lows interval lengthening of the limb,mimicking the growth pace of thecontralateral limb. The endoprosthe-sis can be adjusted surgically whenthe length discrepancy reaches 1 to 2cm.45 However, the device often re-quires multiple surgical interventionsand may introduce increased risk ofinfection or mechanical failure of theimplant.
Rotationplasty is an option for theyoung child who is skeletally immatureand in whom the tumor involves thedistal femur or proximal tibia.31,45
This procedure involves intercalaryresection of the tumor about theknee and 180° rotation of the distalleg, creating a new knee joint fromthe prior ankle joint, enabling activeknee motion. Rotationplasty is donewith all autologous tissue, whichmay lead to decreased postoperativeinfection and mechanical problems.45
A prosthesis is worn at the knee forambulation, and gait analyses dem-onstrate improved kinematics in pa-tients treated with rotationplastycompared with above-knee amputa-tion.46 However, rotationplasty istechnically demanding, and not allfamilies are willing to accept the fi-nal cosmetic appearance.
Complications following limb re-construction include wound compli-cations, infection, mechanical con-struct failure, and nonunion. Thereported incidence of wound compli-cations is 4% to 38%, with dehis-cence, delayed healing, skin graftnecrosis, and flap necrosis all poten-tially occurring.45 The overall infec-tion risk following limb reconstruc-tion is approximately 11%, evenwith intraoperative and postopera-tive prophylaxis therapy.47 Loss ofinternal fixation, prosthesis failure,and joint instability are potential
Patrick J. Messerschmitt, MD, et al
August 2009, Vol 17, No 8 523

modes of mechanical failure.45 Non-union of the reconstruction is possi-ble, particularly with osteoarticularallografts and postoperative chemo-therapy.48 Prior radiation therapy isan additional risk factor for periop-erative complications with limb re-construction.45
Prognosis
Prior to the introduction of chemo-therapy, when amputation was theprimary treatment for patients with
osteosarcoma, the predicted long-term survival rate was 10% to20%.23,49,50 Dismal survival rateswere presumably attributable to pul-monary metastatic disease, whetherobvious or occult.
Survival rates dramatically increasedduring the 1970s and 1980s with theevolution of chemotherapy. In onestudy, adjuvant therapy, in conjunctionwith surgical resection, resulted in im-proved long-term survival rates of 60%to 65%.20 Currently, long-term survivalrates are 60% to 78% for patients with
localized osteosarcoma.4,26,51 Despitethe use of chemotherapy, the ex-pected 10-year survival rate declinessignificantly to 20% to 30% in pa-tients with clinically detectable me-tastases.4,27,52 Most of the nonsurviv-ing patients ultimately die because ofrespiratory failure caused by themetastatic burden.7 Excluding high-grade surface osteosarcoma, whichhas a similar prognosis to that ofconventional osteosarcoma, the sur-face, or parosteal and periosteal, os-teosarcoma variants have the best
Intraoperative photographs demonstrating limb-salvage surgery with endoprosthetic reconstruction in a 10-year-oldpatient with conventional osteosarcoma of the distal femur. A, The prior site and tract of tissue biopsy are excised withthe tumor mass. B, Neurovascular structures are identified and marked with vessel loops to aid in preservingpostoperative limb function. C, The tumor mass is excised en bloc with wide surgical margins. D, The endoprostheticimplant is sized based on preoperative imaging studies and intraoperative measurements. E, Preservation of theextensor mechanism helps to optimize postoperative limb function.
Figure 11
Osteosarcoma
524 Journal of the American Academy of Orthopaedic Surgeons
prognosis of all osteosarcoma sub-types.19 For example, Okada et al15
reported a 91% survival rate for pa-tients with parosteal osteosarcoma, alow-grade tumor, at 5 years follow-ing surgical resection; this outcome isattributable to a low propensity tometastasize. The 10-year survivalrate for patients with periosteal osteo-sarcoma is approximately 83%.16,18
Poor prognostic factors for patientswith osteosarcoma include metastaseson presentation, primary tumor locatedin the axial skeleton, large tumor vol-ume, increased alkaline phosphatase orlactate dehydrogenase levels, poor re-sponse to preoperative chemotherapy,discontinuous tumor of bone, andlymph node involvement.4,7,27
Patient response to primary che-motherapy, measured by tumor ne-crosis, remains the most sensitivetreatment-related predictor of sur-vival and is also important for the se-lection of postoperative chemothera-py.4,35,53 Tumor necrosis of >90%following neoadjuvant chemother-apy has been correlated with im-proved survival rates.25,54 The Huvosclassification of tumor response tochemotherapy is based on the histo-logic evaluation of the excised tumormass.55 The disappearance of neo-plastic cells and maintenance of stro-mal and matrix cells is a positive re-sponse to chemotherapy.6 Generally,approximately one half of patientsare expected to have a positive re-sponse to preoperative chemother-apy (ie, >90% tumor necrosis).25 The5-year survival rates for patientswith >90% tumor necrosis are re-ported to be >61%, but drop to 37%to 52% in patients with a poor re-sponse (<90% necrosis).27,29,56
Despite current surgical and che-motherapeutic treatment regimens,30% to 40% of osteosarcoma patientsexperience relapse within 3 yearsof treatment.7,23 Pulmonary recur-rence is most common secondaryto micrometastatic disease.7 Patients
should be counseled on the poorprognosis associated with relapse be-cause the long-term survival rate is<20%.40,57,58 Regardless of the poorprognosis, patients should be offeredrepeated tumor excision becausesome studies have demonstrated im-proved survival rates.59 The role ofsecond-line chemotherapy remainscontroversial because no standardchemotherapy regimen exists for re-currence.
Future Directions
Basic science research remains an im-portant avenue for discerning molec-ular mechanisms and biologic path-ways that may yield more specificagents, less-toxic drugs, and furtherimprovement in survival rates. Inhi-bition of tyrosine kinase signaling isan area of current interest for the de-velopment of more target-selectivechemotherapeutic drugs.60,61 Tyrosinekinase signaling is known to regulatea number of cellular mechanismsthat are critical for tumor survival,including cell growth, cell prolifera-tion, angiogenesis, and apoptosis.61
Tyrosine kinase inhibitors can eithercompetitively block the tyrosine ki-nase receptor or bind to the receptordirectly and effectively shut downthe signaling pathway.
Liposomal muramyl tripeptide phos-phatidylethanolamine (L-MTP-PE) is apromising drug in clinical trial thatfunctions to stimulate the formation oftumoricidal macrophages.25 Additionof L-MTP-PE to a standard chemo-therapy protocol demonstrated anincrease in 6-year survival rates to78% for patients without clinicallydetectable metastases on presenta-tion.26
Intra-arterial administration of cis-platin has been investigated with thegoal of achieving improved histo-logic response following chemother-apy.62 Although one study demon-
strated an increase in long-termsurvival of up to 93%,63 a largerstudy revealed 70% survival rates,which are similar to those withstandard chemotherapy protocols.62
Thus, a consensus on the routine useof intra-arterial chemotherapy doesnot exist.
Summary
Osteosarcoma is an aggressive andmalignant tumor most commonlyarising about the knee in skeletallyimmature patients. Surgical resectionwith wide margins, coupled withpreoperative and postoperative che-motherapy, is the current standardof care. Treatment should take amultidisciplinary approach, includ-ing surgical and oncologic special-ists. Although the development ofchemotherapy has greatly increasedsurvival rates of patients with os-teosarcoma, outcomes continue to bepoor in the setting of metastases.Current research into the cell biologyof osteosarcoma may lead to im-proved and more target-selectivetreatments with the intent of improv-ing overall long-term survival.
References
Evidence-based Medicine: Levels ofevidence are described in the table ofcontents. In this article, reference 26 isa level I study. References 4, 20, 25,27, 29, 38, 40, 47, 51, 53, 57, 62,and 63 are level II studies. Refer-ences 8, 15, 21, 36, 37, 39, 43, 48,54, 56, and 58 are level III studies.References 10-14, 16-19, 24, 28, 30,32, 34, 41, 42, 46, 49, 50, 52, and59 are level IV studies.
Citation numbers printed in boldtype represent references publishedwithin the past 5 years.
1. Horner MJ, Ries LAG, Krapcho M, et al:SEER Cancer Statistics Review, 1975-
Patrick J. Messerschmitt, MD, et al
August 2009, Vol 17, No 8 525

2006. Bethesda, MD, National CancerInstitute. Available at: http://seer.cancer.gov/csr/1975_2006. Accessed May 15,2009.
2. Hayden JB, Hoang BH: Osteosarcoma:Basic science and clinical implications.Orthop Clin North Am 2006;37:1-7.
3. Carrle D, Bielack SS: Current strategiesof chemotherapy in osteosarcoma. IntOrthop 2006;30:445-451.
4. Bielack SS, Kempf-Bielack B, Delling G,et al: Prognostic factors in high-gradeosteosarcoma of the extremities or trunk:An analysis of 1,702 patients treated onneoadjuvant cooperative osteosarcomastudy group protocols. J Clin Oncol2002;20:776-790.
5. Wang LL: Biology of osteogenicsarcoma. Cancer J 2005;11:294-305.
6. Fletcher CD, Unni KK, Mertens F, eds:World Health OrganizationClassification of Tumours: Pathologyand Genetics of Tumours of Soft Tissueand Bone. Lyon, France, IARC Press,2002, pp 227-232, 264-285.
7. Meyers PA, Gorlick R: Osteosarcoma.Pediatr Clin North Am 1997;44:973-989.
8. Scully SP, Ghert MA, Zurakowski D,Thompson RC, Gebhardt MC:Pathologic fracture in osteosarcoma:Prognostic importance and treatmentimplications. J Bone Joint Surg Am2002;84:49-57.
9. Klein MJ, Siegal GP: Osteosarcoma:Anatomic and histologic variants. Am JClin Pathol 2006;125:555-581.
10. Mervak TR, Unni KK, Pritchard DJ,McLeod RA: Telangiectaticosteosarcoma. Clin Orthop Relat Res1991;270:135-139.
11. Murphey MD, wan Jaovisidha S, TempleHT, Gannon FH, Jelinek JS, MalawerMM: Telangiectatic osteosarcoma:Radiologic-pathologic comparison.Radiology 2003;229:545-553.
12. Andresen KJ, Sundaram M, Unni KK,Sim FH: Imaging features of low-gradecentral osteosarcoma of the long bonesand pelvis. Skeletal Radiol 2004;33:373-379.
13. Nakajima H, Sim FH, Bond JR, UnniKK: Small cell osteosarcoma of bone:Review of 72 cases. Cancer 1997;79:2095-2106.
14. Temple HT, Scully SP, O’Keefe RJ,Katapurum S, Mankin HJ: Clinicaloutcome of 38 patients withjuxtacortical osteosarcoma. Clin OrthopRelat Res 2000;373:208-217.
15. Okada K, Frassica FJ, Sim FH, BeaboutJW, Bond JR, Unni KK: Parostealosteosarcoma: A clinicopathological
study. J Bone Joint Surg Am 1994;76:366-378.
16. Rose PS, Dickey ID, Wenger DE, UnniKK, Sim FH: Periosteal osteosarcoma:Long-term outcome and risk of laterecurrence. Clin Orthop Relat Res 2006;453:314-317.
17. Ritts GD, Pritchard DJ, Unni KK,Beabout JW, Eckardt JJ: Periostealosteosarcoma. Clin Orthop Relat Res1987;219:299-307.
18. Grimer RJ, Bielack S, Flege S, et al:Periosteal osteosarcoma: A Europeanreview of outcome. Eur J Cancer 2005;41:2806-2811.
19. Okada K, Unni KK, Swee RG, Sim FH:High grade surface osteosarcoma: Aclinicopathologic study of 46 cases.Cancer 1999;85:1044-1054.
20. Link MP, Goorin AM, Horowitz M,et al: Adjuvant chemotherapy of high-grade osteosarcoma of the extremity:Updated results of the Multi-InstitutionalOsteosarcoma Study. Clin Orthop RelatRes 1991;270:8-14.
21. Bacci G, Longhi A, Versari M, MercuriM, Briccoli A, Picci P: Prognostic factorsfor osteosarcoma of the extremitytreated with neoadjuvant chemotherapy:15-year experience in 789 patientstreated at a single institution. Cancer2006;106:1154-1161.
22. National Comprehensive CancerNetwork: NCCN Clinical PracticeGuidelines in Oncology: Bone Cancer.National Comprehensive CancerNetwork, 2009, version 1, p 14. FortWashington, PA, NationalComprehensive Cancer Network.Available at: http://www.nccn.org/professionals/physician_gls/PDF/bone.pdf. Accessed May 15, 2009.
23. Longhi A, Errani C, De Paolis M,Mercuri M, Bacci G: Primary boneosteosarcoma in the pediatric age: Stateof the art. Cancer Treat Rev 2006;32:423-436.
24. Enneking WF, Spanier SS, GoodmanMA: A system for the surgical staging ofmusculoskeletal sarcoma. Clin OrthopRelat Res 1980;153:106-120.
25. Meyers PA, Schwartz CL, Krailo M,et al: Osteosarcoma: A randomized,prospective trial of the addition ofifosfamide and/or muramyl tripeptide tocisplatin, doxorubicin, and high-dosemethotrexate. J Clin Oncol 2005;23:2004-2011.
26. Meyers PA, Schwartz CL, Krailo M,et al: Osteosarcoma: The addition ofmuramyl tripeptide to chemotherapyimproves overall survival: A report fromthe Children’s Oncology Group. J ClinOncol 2008;26:633-638.
27. Kager L, Zoubek A, Pötschger U, et al:
Primary metastatic osteosarcoma:Presentation and outcome of patientstreated on neoadjuvant CooperativeOsteosarcoma Study Group protocols.J Clin Oncol 2003;21:2011-2018.
28. Kager L, Zoubek A, Kastner U, et al:Skip metastases in osteosarcoma:Experience of the CooperativeOsteosarcoma Study Group. J ClinOncol 2006;24:1535-1541.
29. Ferrari S, Smeland S, Mercuri M, et al:Neoadjuvant chemotherapy with high-dose ifosfamide, high-dose methotrexate,cisplatin, and doxorubicin for patientswith localized osteosarcoma of theextremity: A joint study by the Italianand Scandinavian Sarcoma Groups.J Clin Oncol 2005;23:8845-8852.
30. Revell MP, Deshmukh N, Grimer RJ,Carter SR, Tillman RM: Periostealosteosarcoma: A review of 17 cases withmean follow-up of 52 months. Sarcoma2002;6:123-130.
31. Grimer RJ: Surgical options for childrenwith osteosarcoma. Lancet Oncol 2005;6:85-92.
32. Smith J, Heelan RT, Huvos AG, et al:Radiographic changes in primaryosteogenic sarcoma following intensivechemotherapy: Radiological-pathologicalcorrelation in 63 patients. Radiology1982;143:355-360.
33. Hosalkar HS, Dormans JP: Limb sparingsurgery for pediatric musculoskeletaltumors. Pediatr Blood Cancer 2004;42:295-310.
34. Bacci G, Ferrari S, Bertoni F, et al:Histologic response of high-gradenonmetastatic osteosarcoma of theextremity to chemotherapy. Clin OrthopRelat Res 2001;386:186-196.
35. National Cancer Institute: Clinical trials.Bethesda, MD, National CancerInstitute, 2009. Available at: http://www.cancer.gov/clinicaltrials. AccessedMay 15, 2009.
36. Meyers PA, Heller G, Healey J, et al:Chemotherapy for nonmetastaticosteogenic sarcoma: The MemorialSloan-Kettering experience. J Clin Oncol1992;10:5-15.
37. Smeland S, Müller C, Alvegard TA, et al:Scandinavian Sarcoma GroupOsteosarcoma Study SSG VIII:Prognostic factors for outcome and therole of replacement salvagechemotherapy for poor histologicalresponders. Eur J Cancer 2003;39:488-494.
38. Harris MB, Gieser P, Goorin AM, et al:Treatment of metastatic osteosarcoma atdiagnosis: A Pediatric Oncology GroupStudy. J Clin Oncol 1998;16:3641-3648.
39. Rougraff BT, Simon MA, Kneisl JS,Greenberg DB, Mankin HJ: Limb
Osteosarcoma
526 Journal of the American Academy of Orthopaedic Surgeons

salvage compared with amputation forosteosarcoma of the distal end of thefemur: A long-term oncological,functional, and quality-of-life study.J Bone Joint Surg Am 1994;76:649-656.
40. Bacci G, Ferrari S, Lari S, et al:Osteosarcoma of the limb: Amputationor limb salvage in patients treated byneoadjuvant chemotherapy. J Bone JointSurg Br 2002;84:88-92.
41. Simon MA, Aschliman MA, Thomas N,Mankin HJ: Limb-salvage treatmentversus amputation for osteosarcoma ofthe distal end of the femur. J Bone JointSurg Am 1986;68:1331-1337.
42. Jeys LM, Kulkarni A, Grimer RJ, CarterSR, Tillman RM, Abudu A:Endoprosthetic reconstruction for thetreatment of musculoskeletal tumors ofthe appendicular skeleton and pelvis.J Bone Joint Surg Am 2008;90:1265-1271.
43. Sorger JI, Hornicek FJ, Zavatta M, et al:Allograft fractures revisited. Clin OrthopRelat Res 2001;382:66-74.
44. Mankin HJ, Springfield DS, GebhardtMC, Tomford WW: Current status ofallografting for bone tumors.Orthopedics 1992;15:1147-1154.
45. Nichter LS, Menendez LR:Reconstructive considerations for limbsalvage surgery. Orthop Clin North Am1993;24:511-521.
46. Fuchs B, Kotajarvi BR, Kaufman KR,Sim FH: Functional outcome of patientswith rotationplasty about the knee. ClinOrthop Relat Res 2003;415:52-58.
47. Jeys LM, Grimer RJ, Carter SR, TillmanRM: Periprosthetic infection in patientstreated for an orthopaedic oncologicalcondition. J Bone Joint Surg Am 2005;87:842-849.
48. Hazan EJ, Hornicek FJ, Tomford W,Gebhardt MC, Mankin HJ: The effect of
adjuvant chemotherapy on osteoarticularallografts. Clin Orthop Relat Res 2001;385:176-181.
49. Gaffney R, Unni KK, Sim FH, SlezakJM, Esther RJ, Bolander ME: Follow-upstudy of long-term survivors ofosteosarcoma in the prechemotherapyera. Hum Pathol 2006;37:1009-1014.
50. Dahlin DC, Coventry MB: Osteogenicsarcoma: A study of six hundred cases.J Bone Joint Surg Am 1967;49:101-110.
51. Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients withnonmetastatic osteosarcoma of theextremity treated at the istitutoortopedico rizzoli according to theistituto ortopedico rizzoli/osteosarcoma-2 protocol: An updatedreport. J Clin Oncol 2000;18:4016-4027.
52. Bacci G, Rocca M, Salone M, et al: Highgrade osteosarcoma of the extremitieswith lung metastases at presentation:Treatment with neoadjuvantchemotherapy and simultaneousresection of primary and metastaticlesions. J Surg Oncol 2008;98:415-420.
53. Provisor AJ, Ettinger LJ, Nachman JB,et al: Treatment of nonmetastaticosteosarcoma of the extremity withpreoperative and postoperativechemotherapy: A report from theChildren’s Cancer Group. J Clin Oncol1997;15:76-84.
54. Meyers PA, Heller G, Healy JH, et al:Osteogenic sarcoma with clinicallydetectable metastasis at initialpresentation. J Clin Oncol 1993;11:449-453.
55. Huvos AG: Bone Tumors: Diagnosis,Treatment, and Prognosis, ed 2.Philadelphia, PA, WB Saunders, 1991,pp 122-128.
56. Bacci G, Bertoni F, Longhi A, et al:Neoadjuvant chemotherapy for high-
grade central osteosarcoma of theextremity: Histologic response topreoperative chemotherapy correlateswith histologic subtype of the tumor.Cancer 2003;97:3068-3075.
57. Kempf-Bielack B, Bielack SS, Jürgens H,et al: Osteosarcoma relapse aftercombined modality therapy: An analysisof unselected patients in the CooperativeOsteosarcoma Study Group (COSS).J Clin Oncol 2005;23:559-568.
58. Ferrari S, Briccoli A, Mercuri M, et al:Postrelapse survival in osteosarcoma ofthe extremities: Prognostic factors forlong-term survival. J Clin Oncol 2003;21:710-715.
59. Hawkins DS, Arndt CA: Pattern ofdisease recurrence and prognostic factorsin patients with osteosarcoma treatedwith contemporary chemotherapy.Cancer 2003;98:2447-2456.
60. Hughes DP, Thomas DG, Giordano TJ,McDonagh KT, Baker LH: EssentialerbB family phosphorylation inosteosarcoma as a target for CI-1033inhibition. Pediatr Blood Cancer 2006;46:614-623.
61. Messerschmitt PJ, Rettew AN,Brookover RE, Garcia RM, Getty PJ,Greenfield EM: Specific tyrosine kinaseinhibitors regulate human osteosarcomacells in vitro. Clin Orthop Relat Res2008;466:2168-2175.
62. Bacci G, Ferrari S, Tienghi A, et al: Acomparison of methods of loco-regionalchemotherapy combined with systemicchemotherapy as neo-adjuvant treatmentof osteosarcoma of the extremity. Eur JSurg Oncol 2001;27:98-104.
63. Wilkins RM, Cullen JW, Camozzi AB,Jamroz BA, Odom L: Improved survivalin primary nonmetastatic pediatricosteosarcoma of the extremity. ClinOrthop Relat Res 2005;438:128-136.
Patrick J. Messerschmitt, MD, et al
August 2009, Vol 17, No 8 527


















