Review Article False-positive uptake on radioiodine whole-body ...
24
Introduction Differentiated thyroid cancer (DTC) is a favor- able malignant tumor, and is associated with a lower risk of death, compared with most other malignancies [1]. Radioiodine has been used for more than five decades for diagnosis and treatment of patients with DTC, with reliance on the fact that trapping, organification, and stor- age of iodine is more prominent in functioning thyroid tissues than other tissues [2, 3]. In par- ticular, on the molecular level, enhanced ex- pression of sodium-iodide symporter (NIS) is a key mechanism of radioiodine uptake in func- tioning thyroid tissues [4-6]. Radioiodine whole- body scintigraphy (WBS) is an integral part of detection of NIS expression in patients suffering from recurrent or metastatic thyroid cancer and in selection of patients who might benefit from radioiodine therapy [7-9]. Precise interpretation of radioiodine WBS can result in avoidance of futile exposure to high-dose radioiodine and lead patients to optimal management of thyroid cancer, as well as other non-thyroidal disease. A considerable number of cases of unexpected radioiodine uptake have been reported. Al- though the mechanism is not fully understood, it can be categorized as follows: 1) functional NIS expression (in normal tissues, including thymus, breast, salivary glands, and gastrointestinal tract, or various benign and malignant tumors), 2) metabolism of radioiodinated thyroid hor- mone, 3) retention of radioiodinated body fluids (saliva, tears, blood, urine, exudate, transudate, gastric and mucosal secretions, etc.) associated with or without structural change, 4) retention and uptake of radioiodine in inflamed tissue, 5) contamination by physiologic secretions, and 6) unknown. The experienced nuclear medicine physician can differentiate malignant from physiologic radioiodine uptake; however, some findings may remain ambiguous. The first step in evaluation of a patient with suspected resid- ual or recurrent thyroid cancer is correlation of normal or abnormal scintigraphic findings with Am J Nucl Med Mol Imaging 2012;2(3):362-385 www.ajnmmi.us /ISSN:2160-8407/ajnmmi1205003 Review Article False-positive uptake on radioiodine whole-body scintigraphy: physiologic and pathologic variants unrelated to thyroid cancer Jong-Ryool Oh, Byeong-Cheol Ahn Department of Nuclear Medicine, Kyungpook National University School of Medicine and Hospital, Daegu, South Korea Received May 17, 2012; accepted June 22, 2012; Epub July 10, 2012; Published July 30, 2012 Abstract: Radioiodine whole-body scintigraphy (WBS), which takes advantage of the high avidity of radioiodine in the functioning thyroid tissues, has been used for detection of differentiated thyroid cancer. Radioiodine is a sensitive marker for detection of thyroid cancer; however, radioiodine uptake is not specific for thyroid tissue. It can also be seen in healthy tissue, including thymus, breast, liver, and gastrointestinal tract, or in benign diseases, such as cysts and inflammation, or in a variety of benign and malignant non-thyroidal tumors, which could be mistaken for thyroid cancer. In order to accurately interpret radioiodine scintigraphy results, one must be familiar with the normal physiol- ogic distribution of the tracer and frequently encountered physiologic and pathologic variants of radioiodine uptake. This article will provide a systematic overview of potential false-positive uptake of radioiodine in the whole body and illustrate how such unexpected findings can be appropriately evaluated. Keywords: Differentiated thyroid cancer, radioiodine, I-131, I-123, whole-body scintigraphy, false-positive, physiologic uptake, pathologic uptake
Transcript of Review Article False-positive uptake on radioiodine whole-body ...
Introduction Differentiated thyroid cancer (DTC) is a favor-able malignant tumor, and is associated with a lower risk of death, compared with most other malignancies [1]. Radioiodine has been used for more than five decades for diagnosis and treatment of patients with DTC, with reliance on the fact that trapping, organification, and stor-age of iodine is more prominent in functioning thyroid tissues than other tissues [2, 3]. In par-ticular, on the molecular level, enhanced ex-pression of sodium-iodide symporter (NIS) is a key mechanism of radioiodine uptake in func-tioning thyroid tissues [4-6]. Radioiodine whole-body scintigraphy (WBS) is an integral part of detection of NIS expression in patients suffering from recurrent or metastatic thyroid cancer and in selection of patients who might benefit from radioiodine therapy [7-9]. Precise interpretation of radioiodine WBS can result in avoidance of futile exposure to high-dose radioiodine and lead patients to optimal management of thyroid
cancer, as well as other non-thyroidal disease. A considerable number of cases of unexpected radioiodine uptake have been reported. Al-though the mechanism is not fully understood, it can be categorized as follows: 1) functional NIS expression (in normal tissues, including thymus, breast, salivary glands, and gastrointestinal tract, or various benign and malignant tumors), 2) metabolism of radioiodinated thyroid hor-mone, 3) retention of radioiodinated body fluids (saliva, tears, blood, urine, exudate, transudate, gastric and mucosal secretions, etc.) associated with or without structural change, 4) retention and uptake of radioiodine in inflamed tissue, 5) contamination by physiologic secretions, and 6) unknown. The experienced nuclear medicine physician can differentiate malignant from physiologic radioiodine uptake; however, some findings may remain ambiguous. The first step in evaluation of a patient with suspected resid-ual or recurrent thyroid cancer is correlation of normal or abnormal scintigraphic findings with
Am J Nucl Med Mol Imaging 2012;2(3):362-385 www.ajnmmi.us /ISSN:2160-8407/ajnmmi1205003
Review Article False-positive uptake on radioiodine whole-body scintigraphy: physiologic and pathologic variants unrelated to thyroid cancer Jong-Ryool Oh, Byeong-Cheol Ahn Department of Nuclear Medicine, Kyungpook National University School of Medicine and Hospital, Daegu, South Korea Received May 17, 2012; accepted June 22, 2012; Epub July 10, 2012; Published July 30, 2012 Abstract: Radioiodine whole-body scintigraphy (WBS), which takes advantage of the high avidity of radioiodine in the functioning thyroid tissues, has been used for detection of differentiated thyroid cancer. Radioiodine is a sensitive marker for detection of thyroid cancer; however, radioiodine uptake is not specific for thyroid tissue. It can also be seen in healthy tissue, including thymus, breast, liver, and gastrointestinal tract, or in benign diseases, such as cysts and inflammation, or in a variety of benign and malignant non-thyroidal tumors, which could be mistaken for thyroid cancer. In order to accurately interpret radioiodine scintigraphy results, one must be familiar with the normal physiol-ogic distribution of the tracer and frequently encountered physiologic and pathologic variants of radioiodine uptake. This article will provide a systematic overview of potential false-positive uptake of radioiodine in the whole body and illustrate how such unexpected findings can be appropriately evaluated. Keywords: Differentiated thyroid cancer, radioiodine, I-131, I-123, whole-body scintigraphy, false-positive, physiologic uptake, pathologic uptake
False-positive uptakes on radioiodine scintigraphy
363 Am J Nucl Med Mol Imaging 2012;2(3):362-385
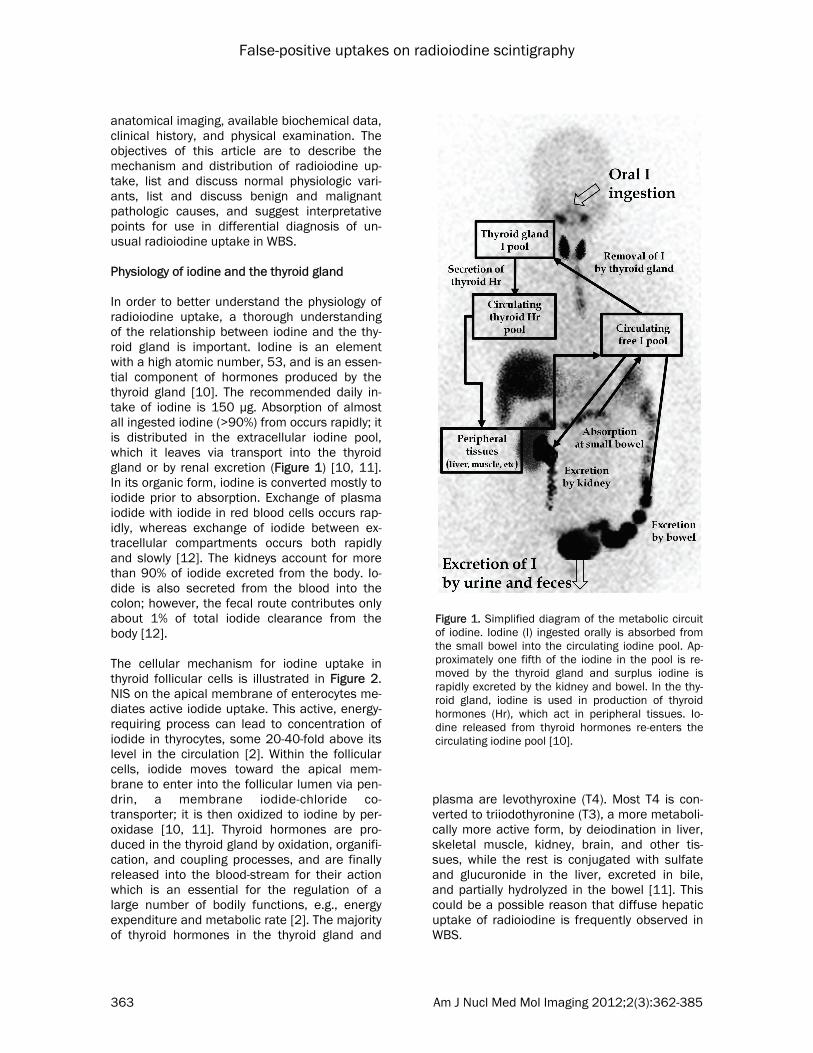
anatomical imaging, available biochemical data, clinical history, and physical examination. The objectives of this article are to describe the mechanism and distribution of radioiodine up-take, list and discuss normal physiologic vari-ants, list and discuss benign and malignant pathologic causes, and suggest interpretative points for use in differential diagnosis of un-usual radioiodine uptake in WBS. Physiology of iodine and the thyroid gland In order to better understand the physiology of radioiodine uptake, a thorough understanding of the relationship between iodine and the thy-roid gland is important. Iodine is an element with a high atomic number, 53, and is an essen-tial component of hormones produced by the thyroid gland [10]. The recommended daily in-take of iodine is 150 μg. Absorption of almost all ingested iodine (>90%) from occurs rapidly; it is distributed in the extracellular iodine pool, which it leaves via transport into the thyroid gland or by renal excretion (Figure 1) [10, 11]. In its organic form, iodine is converted mostly to iodide prior to absorption. Exchange of plasma iodide with iodide in red blood cells occurs rap-idly, whereas exchange of iodide between ex-tracellular compartments occurs both rapidly and slowly [12]. The kidneys account for more than 90% of iodide excreted from the body. Io-dide is also secreted from the blood into the colon; however, the fecal route contributes only about 1% of total iodide clearance from the body [12]. The cellular mechanism for iodine uptake in thyroid follicular cells is illustrated in Figure 2. NIS on the apical membrane of enterocytes me-diates active iodide uptake. This active, energy-requiring process can lead to concentration of iodide in thyrocytes, some 20-40-fold above its level in the circulation [2]. Within the follicular cells, iodide moves toward the apical mem-brane to enter into the follicular lumen via pen-drin, a membrane iodide-chloride co-transporter; it is then oxidized to iodine by per-oxidase [10, 11]. Thyroid hormones are pro-duced in the thyroid gland by oxidation, organifi-cation, and coupling processes, and are finally released into the blood-stream for their action which is an essential for the regulation of a large number of bodily functions, e.g., energy expenditure and metabolic rate [2]. The majority of thyroid hormones in the thyroid gland and
plasma are levothyroxine (T4). Most T4 is con-verted to triiodothyronine (T3), a more metaboli-cally more active form, by deiodination in liver, skeletal muscle, kidney, brain, and other tis-sues, while the rest is conjugated with sulfate and glucuronide in the liver, excreted in bile, and partially hydrolyzed in the bowel [11]. This could be a possible reason that diffuse hepatic uptake of radioiodine is frequently observed in WBS.
Figure 1. Simplified diagram of the metabolic circuit of iodine. Iodine (I) ingested orally is absorbed from the small bowel into the circulating iodine pool. Ap-proximately one fifth of the iodine in the pool is re-moved by the thyroid gland and surplus iodine is rapidly excreted by the kidney and bowel. In the thy-roid gland, iodine is used in production of thyroid hormones (Hr), which act in peripheral tissues. Io-dine released from thyroid hormones re-enters the circulating iodine pool [10].

False-positive uptakes on radioiodine scintigraphy
364 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Properties of radioiodines Iodine-131 I-131 is produced in a nuclear reactor by neu-tron bombardment of natural tellurium (Te-127) and decays by beta emission to xenon-133 (Xe-133), with a half-life of 8.02 days; it also emits gamma emissions (Table 1). It most often (89% of the time) expends its 971 keV of decay en-ergy by transforming into the stable Xe-131, in two steps; gamma decay rapidly following after beta decay. Beta particles with a maximal en-ergy of 606 keV (89% abundance, others 248–807 keV) and 364 keV gamma rays (81% abun-dance, others 723 keV) are the primary emis-sions of I-131 decay. I-131 is administered orally with activities of 1–5 mCi or less. As a result of data suggesting that stunning
(decreased uptake of the therapeutic dose of I-131 by the residual functioning thy-roid tissue or tumor due to cell death or dysfunction caused by the activity ad-ministered for diagnostic imaging) is less likely at the lower activity range, many prefer a range of 1–2 mCi. However, a higher rate of detection of iodine concen-trating tissues has been reported with higher dos-ages [13]. Iodine-123 I-123 is produced in a cyclo-tron by proton irradiation of enriched Xe-124 in a cap-sule. Decay of I-123 to Te-123 occurs by electron cap-ture, with a half-life of 13.22 hours and gamma radiation is emitted with predominant energies of 159 keV (the gamma ray primarily used for imaging) and 127 keV. Compared with I-131, I-123 is mainly a gamma emitter with a high counting rate, and provides a higher lesion-to -background s ignal , thereby improving the sensi-tivity and quality of imaging.
With the same administered activity, I-123 deliv-ers an absorbed radiation dose that is approxi-mately one-fifth that of I-131 to the thyroid tis-sue, thereby lessening the likelihood of stunning from imaging. I-123 is administered orally with activities of 0.4–5.0 mCi, which may allow avoidance of stunning [13, 14]. Iodine-124 I-124 is a proton-rich isotope of iodine produced in a cyclotron by numerous nuclear reactions; it decays to Te-124 with a half-life of 4.18 days. Its modes of decay include: 74.4% electron cap-ture and 25.6% positron emission. It emits gamma radiation with energies of 511 and 602 keV [15]. I-124 is administered intravenously with activities of 0.5–2.0 mCi for detection of metastatic lesions or assessment of the radia-
Figure 2. Cellular mechanism for iodine uptake in thyroid follicular cells. This process commences with uptake of iodide from the capillary into follicular cells of the thyroid gland. This process occurs against chemical and electrical gradients via sodium iodide symporter (NIS) located in the basal membrane of follicular cells. Increased intracellular sodium is pumped out by the action of Na+/K+ ATPase. The iodide within the follicular cell moves toward the apical membrane to enter into the follicular lumen and is then oxidized to iodine by peroxidase. Organification of the iodine follows oxidation by iodination of tyro-sine residues present within the thyroglobulin (TG) molecule, and the iodine stays in the follicle until it is released into the circulation as thyroid hormones. Thyroid stimulating hormone (TSH) activates the follicular cell via TSH recep-tor (TSH-R) and increases the expression of NIS and the TG [10].

False-positive uptakes on radioiodine scintigraphy
365 Am J Nucl Med Mol Imaging 2012;2(3):362-385
tion dose related to I-131 therapy. Compared to radioiodine gamma scintigraphy, significantly greater sensitivity and spatial resolution can be achieved using I-124 positron emission tomo-graphy, leading to improved detection of resid-ual or recurrent thyroid cancer. And, it can be used for patient-specific radiation dosimetry for radioiodine treatment [16]. Iodine-125 I-125, which is produced in nuclear reactor by neutron capture in irradiated xenon gas (Xe-124), disintegrates by electron capture via the excited level of 35 keV of Te-125 into the ground state of Te-125. It also emits x-rays and Auger electrons, as well as gamma rays. Be-cause of its relatively long half-life (59.39 days), I-125 is preferred for radioimmunoassay or other in vitro assays, and brachytherapy for sev-eral solid tumors, including brain tumor, pros-tate cancer, and head and neck cancer [17-20]. Owing to its low gamma energy, I-125 is not suitable for whole-body gamma camera imag-ing. Several authors reported regarding the treatment of hyperthyroidism using I-125 in 1970's, however, this was not the case in clini-cal practice [21]. Physiologic radioiodine uptake Ectopic thyroid tissue Ectopic thyroid tissue is the result of a failure of
migration of the thyroid gland, which begins at embryonic day 24. An endodermal diverticulum from the median plate of the floor of the pharyn-geal gut is formed; this diverticulum then de-scends in the midline, from the foramen cecum to the final location of the thyroid gland, anteri-orly to the pre-trachea and larynx [22]. The in-nate ability to trap iodine and produce thy-roglobulin is shared by ectopic thyroid tissues and normal thyroid tissues, observance of ec-topic thyroid tissues in radioiodine WBS is a common false-positive finding [10, 23, 24]. They are frequently found as a lingual, sublin-gual thyroid, thyroglossal duct cyst, intratracheal and mediastinal thyroid. They can also be lo-cated in both supra- and subdiaphragmatic or-gans, including lung, heart (struma cordis), ad-renal glands, gallbladder, duodenum, ovary (struma ovarii), pancreas and intestine [22]. Simultaneous presentation of two ectopic foci, such as lingual and perihyoid, or lingual and porta hepatis can occur [22, 25]. Recognition of the location and nature of ectopic thyroid tissue can minimize misinterpretation as metastatic disease. Non-thyroidal tissue Although the abilities to trap iodine and produce thyroglobulin are unique features of thyroid tis-sues, physiological uptake of radioiodine can also be observed in a variety of non-thyroidal tissues (Figure 3 and 4). Two main causes of uptake include functional NIS expression and
Table 1. Properties of radioiodines (iodine isotopes) I-131 I-123 I-124 I-125 Production Nuclear reactor Cyclotron Cyclotron Nuclear reactor
Decay mode β- decay Electron capture β+ decay Electron capture
Physical half life 8.02 days 13.22 hours 4.18 days 59.39 days
Gamma energy (keV) 364 159 511 35
β energy (keV) 606 (maximum) - - -
Typical administered activity, mCi (MBq)
Imaging: 1-5 (37-185) Treatment: 30-200 (1,110-7,400)
0.4-5 (15-185) (19-74) -
Advantages - Low costs - Availability for treat-ment
- Good image quality - No stunning effect
- Suitability for positron emission tomography - Superiority for do-simetry
- Availability for in vitro assays - Availability for brachytherapy
Disadvantages - Poor image quality - Stunning effect - Necessity of radiation safety for caregivers
- High costs - Relatively short half life
- High costs - Limited for use in whole-body imaging

False-positive uptakes on radioiodine scintigraphy
366 Am J Nucl Med Mol Imaging 2012;2(3):362-385
metabolism related to or the retention of ex-creted iodine. Expression of NIS in salivary and lacrimal glands, stomach, choroid plexus, ciliary body of the eye, skin, placenta, lactating mam-
mary gland, thymus, and, to a lesser extent, the prostate, ovary, adrenal gland, lung, and heart has been demonstrated [4, 6]. Liver is regarded as the major organ for metabo-lism of radioiodinated thy-roglobulin released from functioning thyroid tissues [26]. Retention of radioio-dine can occur as a result of structural or functional changes in any part of the body located along the route of radioiodine excre-tion or blood pooling (Table 2). Breast is the one of major organs expressing NIS. Iodine accumulation in the lactating breast has been recognized for 60 years and is now regarded as a usual finding in postpar-tum patients [27]. Once the NIS gene was cloned and become available for study, expression of NIS on the basolateral mem-brane of alveolar cells in mammary glands and marked induction during lactation were demon-strated [28, 29]. Bakheet et al. [30] conducted an analysis of patterns of radioiodine uptake in lac-tating breasts on 20 ra-dioiodine scintigraphic images. They identified four patterns of uptake: "full" (most common), "focal", "crescent", and "irregular". Uptake was asymmetric in 60% (left > right in 45%, right > left in 15%), symmetric in 25%, and unilateral in 15% of cases. Recognition of
those patterns and clinical history is helpful to interpretation of breast uptake on radioiodine scintigraphy (Figure 5). However, breast uptake that presents with an atypical pattern and/or is
Figure 3. Schematic presentation of the locations of physiologic uptake and possible sources of contamination of radioiodine whole-body scan (WBS) [10].
Figure 4. Physiologic uptakes of radioiodine in the whole body; A - planar scinti-graphy, B - SPECT/CT. Radioiodine uptakes in nasal secretion (1), parotid gland (2), dental prosthesis (3), remnant thyroglossal duct (4), remnant thyroid tissue (5), liver (6), and colon (7) are observed. The Hybrid SPECT/CT imaging helps recognize the exact localization of the radioiodine uptakes.

False-positive uptakes on radioiodine scintigraphy
367 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Table 2. Physiologic radioiodine uptake Region Mechanism of radioiodine uptake Reference Head and Neck
Ectasia Common carotids Blood stasis and reverse flow [48] Parotid gland duct Retention of saliva [54] Epiphora Retention of tear due to nasolacrimal duct obstruction [55] Nasolacrimal sac cyst Passive diffusion and retention of tear [130] Thyroglossal duct Functional NIS expression [131] Prosthetic denture Unclear, retention of saliva [56]
Chest Breast
Non-feeding Functional NIS expression [31, 132] Feeding Lactation of radioiodine, enhanced functional NIS expression [133-135] Hyperprolactinemia Enhanced functional NIS expression in breast tissue caused by prolactinoma in the
pituitary gland [32]
Thymus Functional NIS expression and iodine concentration in Hassall’s bodies [33-39, 136] Respiratory tract The use of local aerosol medication because of the chronic pulmonary disease [57] Esophageal retention Retention of saliva and/or refluxed gastric juice
Achalasia [137] Zenker’s diverticulum [138-140] Epiphrenic diverticulum [141] Esophageal scarring + post-radiation scarring [142]
Thoracic aortic aneurysm Retention of radioiodine in blood pool [49] Pectus excavatum Displaced cardiac blood pool by deformity [51] Hiatal hernia Functional NIS expression and gastric secretion [143, 144] Cysts Passive diffusion (or partially active transport) and retention of radioiodine Pleuropericardial cyst [145] Bronchogenic cyst [112, 146] Thymic cyst [147] Breast cyst [148]
Abdomen and pelvis Liver Absorption of radioiodinated thyroglobulin released from functioning thyroid tissue
[26], delayed hepatic excretion and functional NIS expression in the intrahepatic bile ducts [42]
[26, 42]
Gallbladder and biliary tract Delayed hepatic excretion and functional NIS expression in the gallbladder mucosa and bile ducts
[42, 62, 63, 66]
Stomach Gastric volvulus Retention of gastric secretions [64] Intestine
Meckel’s diverticulum Functional NIS expression [60] Colonic scar Unclear, appendectomy before 31 years ago [67] Appendix Retention of intestinal secretions [69]
Pelvocalyceal diverticulum or dilation
Retention of urine [61, 70]
Ectopic kidney Physiologic urine activity and/or urine retention [65, 149] Uterus and vagina Retention of menstrual blood [52, 53] Gestational sac Iodine transport from mother to fetus
Functional NIS expression in placenta [45]
Cysts Passive diffusion (or partially active transport) and retention of radioiodine Hepatic cyst [75-77] Renal cyst [71, 72, 74, 78]
Ovarian endometriosis cyst [73] Epithelial cyst in mesentery [79] Others Bone marrow Unclear, patient's athletic activities [80] Dilated greater saphenous vein Blood stasis and reverse flow [50] Sebaceous cyst Passive diffusion and retention of radioiodine: can be complicated by infection [100, 150] Contamination Tears Artificial eye [82, 149] Saliva Chewing tobacco and gum, lips [87, 91, 94] Nasal secretion Nose-ring sign [86]
Vomitus [27] Milk [93, 95]
Sweat Handkerchief sign, helmet sign, necklace sign [81, 83-85, 89-91, 97]
Urine [88]
False-positive uptakes on radioiodine scintigraphy
368 Am J Nucl Med Mol Imaging 2012;2(3):362-385
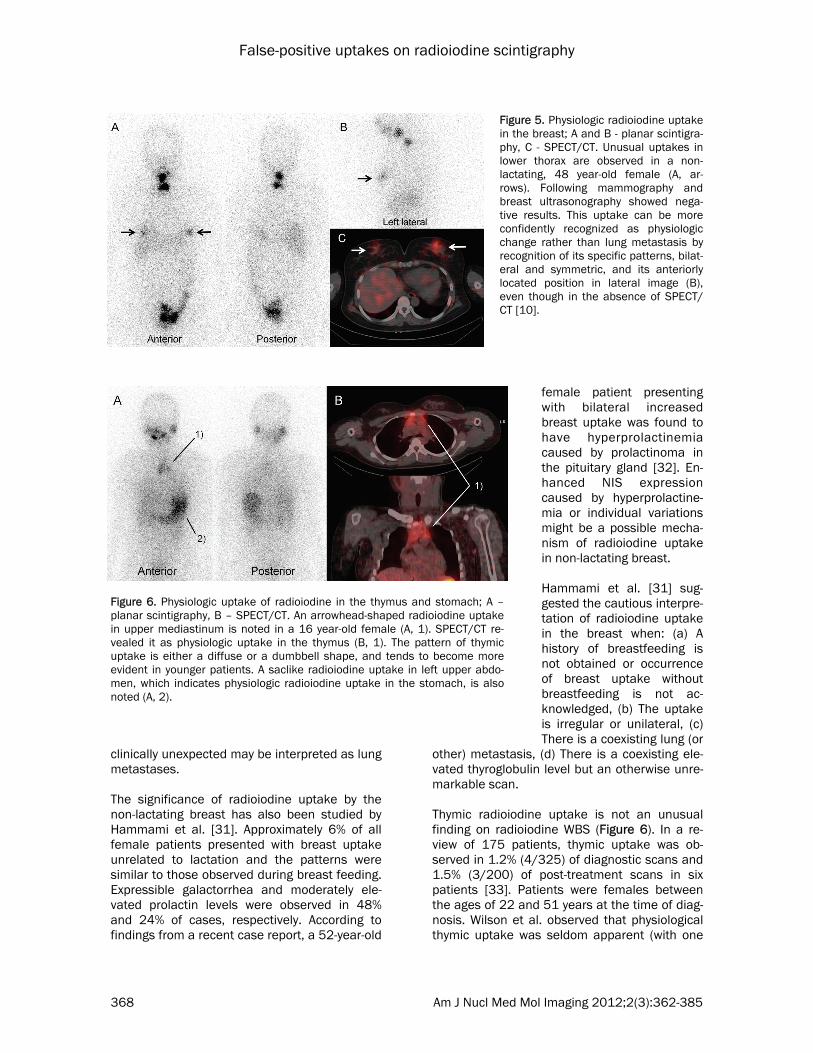
clinically unexpected may be interpreted as lung metastases. The significance of radioiodine uptake by the non-lactating breast has also been studied by Hammami et al. [31]. Approximately 6% of all female patients presented with breast uptake unrelated to lactation and the patterns were similar to those observed during breast feeding. Expressible galactorrhea and moderately ele-vated prolactin levels were observed in 48% and 24% of cases, respectively. According to findings from a recent case report, a 52-year-old
female patient presenting with bilateral increased breast uptake was found to have hyperprolactinemia caused by prolactinoma in the pituitary gland [32]. En-hanced NIS expression caused by hyperprolactine-mia or individual variations might be a possible mecha-nism of radioiodine uptake in non-lactating breast. Hammami et al. [31] sug-gested the cautious interpre-tation of radioiodine uptake in the breast when: (a) A history of breastfeeding is not obtained or occurrence of breast uptake without breastfeeding is not ac-knowledged, (b) The uptake is irregular or unilateral, (c) There is a coexisting lung (or
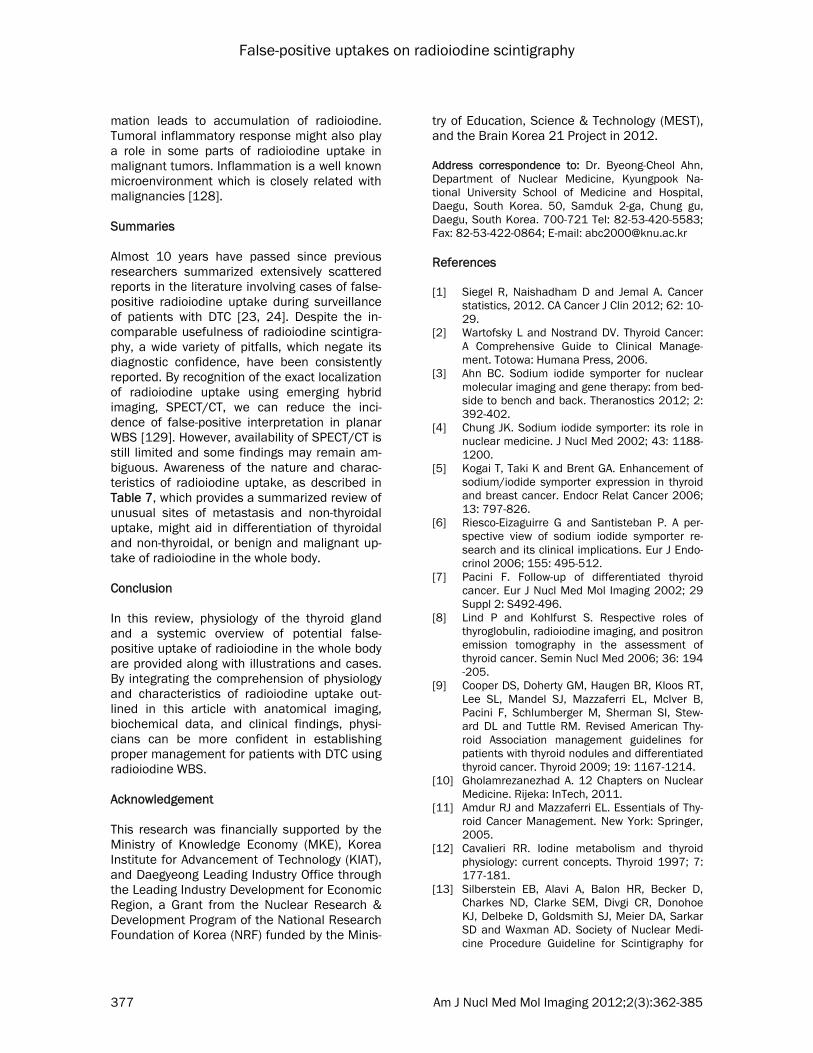
other) metastasis, (d) There is a coexisting ele-vated thyroglobulin level but an otherwise unre-markable scan. Thymic radioiodine uptake is not an unusual finding on radioiodine WBS (Figure 6). In a re-view of 175 patients, thymic uptake was ob-served in 1.2% (4/325) of diagnostic scans and 1.5% (3/200) of post-treatment scans in six patients [33]. Patients were females between the ages of 22 and 51 years at the time of diag-nosis. Wilson et al. observed that physiological thymic uptake was seldom apparent (with one
Figure 5. Physiologic radioiodine uptake in the breast; A and B - planar scintigra-phy, C - SPECT/CT. Unusual uptakes in lower thorax are observed in a non-lactating, 48 year-old female (A, ar-rows). Following mammography and breast ultrasonography showed nega-tive results. This uptake can be more confidently recognized as physiologic change rather than lung metastasis by recognition of its specific patterns, bilat-eral and symmetric, and its anteriorly located position in lateral image (B), even though in the absence of SPECT/CT [10].
Figure 6. Physiologic uptake of radioiodine in the thymus and stomach; A – planar scintigraphy, B – SPECT/CT. An arrowhead-shaped radioiodine uptake in upper mediastinum is noted in a 16 year-old female (A, 1). SPECT/CT re-vealed it as physiologic uptake in the thymus (B, 1). The pattern of thymic uptake is either a diffuse or a dumbbell shape, and tends to become more evident in younger patients. A saclike radioiodine uptake in left upper abdo-men, which indicates physiologic radioiodine uptake in the stomach, is also noted (A, 2).

False-positive uptakes on radioiodine scintigraphy
369 Am J Nucl Med Mol Imaging 2012;2(3):362-385
exception; the youngest) on the scan performed at 3-4 days but was clearly observed on the 7-day scan [34]. The pattern of uptake showed either a diffuse or a dumbbell shape. Overall consensus is that thymic uptake tends to be-come more evident on delayed imaging, with a therapeutic dose, in younger patients, and with less residual or metastatic thyroid tissues [33-39]. The mechanism of radioiodine uptake by the thymus is not yet fully understood. Autoradiogra-phy performed by Verminglio et al. [35] revealed localization of iodine uptake in the thymus to Hassall’s bodies, which are constituted by epithelial cells resembling keratinocytes. They suggested that this finding reflects the struc-tural similarity between cystic Hassall’s bodies and thyroid follicles. Although a capability of transport and concentration of iodine is weaker in the thymus, compared with that presented in the thyroid gland, the presence of NIS is a proven mechanism of radioiodine uptake in the thymus [40]. Following findings reported by Michigishi et al. [36] will be helpful in differentiating physiologic from malignant mediastinal uptake: (a) uptake that becomes more prominent with repeated treatment, (b) requirement of higher than usual iodine doses in order to visualize the area, (c) a young age, (d) a large thymus on CT, and (e) a low serum thyroglobulin level. Diffuse hepatic uptake of radioiodine is also a common finding on radioiodine WBS. Several authors have suggested that diffuse uptake of radioiodine by the liver is related to residual thyroid tissue or recurrent or persistent metas-tasis [26, 41]. According to Chung et al. [26], whose study included a large population, be-cause the liver is the major organ for the me-tabolism of thyroid hormones, this finding was explained by accumulation of radioiodinated thyroid hormones in patients with remnant thy-roid tissues. In patients without thyroid rem-nant, radioiodinated thyroglobulin released from functioning cancer tissue is regarded as the cause of diffuse hepatic uptake of radioiodine. However, other investigators have stated that diffuse hepatic uptake is a benign finding with-out clinical importance [42-44]. Tatar et al. [44] reported no significant association between liver uptake and uptake in the thyroid bed, the dose of radioiodine administered for ablation
therapy, thyroglobulin levels, age, stage of dis-ease, presence of local or distant metastases, recurrence, or survival. A more recent study of a larger population conducted by Omur et al [42] also revealed no correlation of hepatic uptake with serum thyroglobulin levels, thyroid remnant score, and presence of local or distant metas-tatic foci. Instead, of particular interest, hepatic uptake showed positive correlation with admin-istered doses of RAI, increased hepatic en-zymes, and hepatosteatosis. This finding sup-ports the concept that the presence of multiple metabolic factors is related to diffuse hepatic radioiodine uptake. They suggested that associ-ated changes in lipoproteins and hepatic en-zymes might have contributed to increased he-patic uptake in patients with hepatosteatosis. The increase of hepatic enzymes is an indica-tion that delayed action of deiodinase may re-sult in delayed excretion of iodine taken up by hepatocytes and consequent higher liver reten-tion. NIS can also contribute to hepatic radioio-dine uptake through mediation of active trans-port in association with iodine in intrahepatic bile ducts. Studies of physiologic radioiodine uptake in the liver are summarized in Table 3. Obviously, he-patic visualization tends to occur more fre-quently in post-therapy scanning, compared with diagnostic scanning, and delayed scanning (8-10 days), compared with early scanning (4-5 days). According to our observations, in studies where an early scan was performed, hepatic visualization appears to be associated with functioning thyroid tissues, whereas it was not in studies performed using a delayed scan (Table 3). This discrepancy may be owing to differences in biological characteristics for trap-ping or excretion of radioiodine in remnant thy-roid tissue, metastatic thyroid tissue, and liver with passage of time. The gestational sac can also be a site of radioio-dine accumulation [45]. Although the molecular mechanisms of iodine transport from mother to fetus are not clear, iodide and small amounts of thyroid hormones are transferred through the placenta from mother to fetus. Functional NIS expression in normal human placenta, preferen-tially in cytotrophoblastic cells, can also be a cause of radioiodine uptake in the gestational sac [46, 47]. Physiologic dilatation of the vessel, gut, duct, and ureter, regardless of the presence of ob-

False-positive uptakes on radioiodine scintigraphy
370 Am J Nucl Med Mol Imaging 2012;2(3):362-385
struction, causes retention of body fluid contain-ing radioiodine. Vascular dilatation of common carotids [48], thoracic aorta [49], and greater saphenous vein [50] have been reported. Dis-placed blood pool activity associated with pec-tus excavatum can also be misinterpreted as abnormal radioiodine uptake in the chest [51]. Menstruation history, even in young patients who have not yet reached menarche, should be considered in evaluation of unusual pelvic up-take of radioiodine [52, 53]. Retention of tears, saliva, gastric juice, bronchial secretion, bile, intestinal secretion, and urine can be related to a specific disease or clinical situation, such as epiphora, use of aerosol, achalasia, diverticu-lum, hiatal hernia, gastric volvulus, and ectopic
kidney (Figure 7) [48, 54-70]. Meckel’s diver-ticulum has an additional mechanism of radioio-dine uptake via NIS, which is originally ex-pressed in gastric mucosa. Various cystic structures, including the nasolac-rimal sac, pleuropericardial, bronchogenic, thymic, breast, hepatic, renal, ovarian, epithelial and sebaceous cysts are also known to show false-positive findings on radioiodine WBS (Figure 8) [71-79]. Entry of radioiodine into cysts occurs via passive diffusion or partially active transport; then, due to the slow exchange of water and chemical elements between the cysts and their surrounding extracellular/extravascular environment, it becomes trapped
Table 3. Review of diffuse hepatic uptake of radioiodine Reference Diagnostic scan Post-treatment scan Correlation with
residual or metastatic thyroid tissue
Incidence of hepatic visu-alization
Dose mCi (MBq), scanning time
Incidence of hepatic visuali-zation
Dose mCi (GBq), scanning time (mean)
Ziessman et al. (1987) [41]
22.0% (9/41) 2-10 (74-370), 48 hours
74.7% (14/19) 30-200 (1.1-7.4), 3-7 days
Yes
Rosenbaum et al. (1988) [43]
13.2% (5/38) 10 (370), 72 hours 52.2% (15/29) 80-150 (3.0-5.6), 7 days
Not always
Chung et al. (1997) [26]
22.7% (65/300)
2-10 (74-370), 48 hours
72.0%, (580/806)
30-200 (1.1-7.4), 3-5 days
Yes
Tatar et al. (2001) [44]
0% (0/118) 2-5 (74-185), 72 hours
96.4% (135/141)
30-200 (1.1-7.4), 3-21 (8.3) days
No
Omur et al. (2009) [42]
NA NA 96.5% (863/894)
75-200 (2.8-7.4), 6-13 (10) days
No
NA, not assessed. All scans were performed with I-131
Figure 7. Physiologic uptake of radioiodine in the gallbladder and intestines; A – planar scintigra-phy, B – SPECT/CT. Focal and segmental uptakes in right upper and left abdomen are noted (A, 1-2). SPECT/CT revealed them as physiologic uptakes unrelated to metastatic disease in gallbladder (1) and intestines (2). Secretion and retention of radioiodinated body fluid along the biliary tract and intestines can be causes of those unexpected uptakes of ra-dioiodine.

False-positive uptakes on radioiodine scintigraphy
371 Am J Nucl Med Mol Imaging 2012;2(3):362-385
within the cysts. Although the mechanism is unclear, diffuse radioiodine uptake in bone mar-row (bilateral femur and tibia) of patients in-volved in heavy running activity has also been reported [80]. Contamination by physiological secretion External contamination by physiological or pathological body secretions or excretions can result in positive radioiodine uptake, which mimics metastatic involvement of DTC (Table 2) [23, 24, 27, 81-97]. Sweat, breast milk, urine, vomitus and nasal, tracheobronchial, lacrimal, salivary secretions and feces contain radioio-dine and their contamination on hair, skin, or clothing can be misinterpreted as metastasis of thyroid cancer (Figure 3 and 9). Any focus of radioiodine uptake that cannot be explained by physiological or pathological causation must also be suspected as arising from contamina-tion by secretions. Fortunately, contamination is usually easily recognized by its pattern; acquisi-tion of images should be performed after re-moval of the contamination using decontami-nating procedures or removal of stained cloth-ing. However, unusual patterns of contamina-tion might occur and suspicion of the uptake as contamination would be difficult. Patients' peculiar physical characteristics or odd habits produce extraordinary patterns of con-tamination. Careful preparation of patients, in-cluding image acquisition in a clean gown after showering, can help to minimize false-positive scanning results due to contamination. Con-tamination is almost always superficial [23, 24],
therefore, use of lateral and/or oblique views to give a third dimension to the scan may aid in identification of the contamination. In addition, use of the single photon emission computed tomography (SPECT) image alone or the SPECT image fused with the anatomical image, which provides detailed information on the anatomic location of uptake sites, can be the best way to
Figure 8. Physiologic uptake of ra-dioiodine in a simple cyst of the right kidney; A – planar scintigraphy, B – SPECT/CT, C – abdominal CT. Focal tracer uptake is noted at the right side of the abdomen (A, arrows). SPECT/CT (B) and abdominal CT (C) images revealed it as physiologic radioiodine uptake in a simple cyst of the right kidney. Communication be-tween the cyst and the urinary tract, or secretion of radioiodine by the lining epithelium of the cyst can be causes of radioiodine uptake in the cystic structure.
Figure 9. Contamination of radioiodine by hair in two patients (A-B and C-D). Unexpected radioiodine up-takes in the outside (A) and on (C) the skull are ob-served (arrows). On the additional image after rolling up the hair (B and D), the uptakes were moved up-ward (arrows). The change or disappearance of up-take on additional image after rolling up the hair, showering, or removal of stained clothing can help to differentiate unusual uptake by the radioiodine con-tamination from pathologic condition. Note: Delayed scan of second patient (D) was performed 7 days after initial scan (C). S, scalp; O, oral cavity [10].

False-positive uptakes on radioiodine scintigraphy
372 Am J Nucl Med Mol Imaging 2012;2(3):362-385
accurately determine that contamination is the reason for the uptake. Pathologic radioiodine uptake: non-tumoral dis-ease Inflammation, which can be caused by any harmful stimuli, such as infection, trauma, or infarction, is the major cause of non-tumoral pathologic radioiodine uptake (Table 4, Figure
10). Inflamed tissues suffer a cascade of bio-logical events, including increased blood flow and capillary permeability. Increased permeabil-ity can result in an abundance of cells in tissue or vessels, and stasis of radioiodinated blood can also occur due to an increase in the con-centration of cells within blood. Mediator molecules also alter blood vessels in order to permit migration of leukocytes outside
Table 4. Pathologic uptake unrelated to tumor Region Mechanism of radioiodine uptake Reference Head and Neck
Inflammation Increased perfusion and vasodilatation, and enhanced capil-lary permeability
Folliculitis in scalp [151] Sialoadenitis [152, 153] Sinusitis [149, 154] Dacryocysitis [149] Mucocele Accumulation of inflammatory exudates and mucous secreted
by the hypertrophied glands and mucinous cells
Frontal sinus mucocele [101, 102] Laryngocele [155, 156] Trauma Increased perfusion and vasodilatation, and enhanced capil-
lary permeability
Subdural hematoma [157] Tracheostomy site [158, 159] Cranial metallic suture [160, 161]
Chest Inflammation Increased perfusion and vasodilatation, and enhanced capil-
lary permeability
Acute respiratory infection + accumulation of tracheobronchial secretions in the airway [103, 162] Pulmonary tuberculosis + accumulation of tracheobronchial secretions in the dam-
aged lung region [105]
Rheumatoid lung disease [163] Pulmonary aspergilloma + the endotoxins or enzymes released locally by the fungus,
which cause cellular damage to the inner lining of the fungus ball cavity
[164, 165]
Bronchiectasis Accumulation of bronchial secretions [104, 166] Myocardial infarction Increased perfusion and vasodilatation, and enhanced capil-
lary permeability [168]
Pericardial and pleural effu-sion
Pathologic transudates or exudates [169-172]
Chest wall after needle bi-opsy
Increased perfusion and vasodilatation, and enhanced capil-lary permeability by the tissue trauma
[173]
Abdomen and pelvis Cholecystitis Inflammatory reaction and retention of radioiodine in the leu-
kocytes/ bile retention/ mucinous secretion [100, 106]
Others Rheumatoid arthritis during acupuncture treatment
Increased perfusion and vasodilatation, and enhanced capil-lary permeability
[174]
Post-traumatic superficial scabs
Inflammatory reaction after trauma and retention of radioio-dine in the leukocytes of post-traumatic clots
[99]

False-positive uptakes on radioiodine scintigraphy
373 Am J Nucl Med Mol Imaging 2012;2(3):362-385
of the vessels into the tissue. As part of their bactericidal effect, leukocytes are known to in-duce iodide organification by means of a mye-loperoxidase [98]. Therefore, retention of ra-dioiodine in leukocytes of posttraumatic clots or tissues may also explain various reports of false-positive uptake in sites of inflammation (Figure 11) [99, 100]. Secretion of mucin containing iodide salts has also been suggested as another possible mechanism of iodine accumulation associated with chronic inflammatory conditions in bron-chus, gallbladder, or mucocele [101-106]. Pathologic radioiodine uptake: benign tumor Although the mechanism is not fully understood, unexpected radioiodine uptakes in diverse be-nign tumors having different histopathologic natures has been reported (Table 5). Functional NIS expression in parotid tumors, such as Warthin’s tumor or oncocytoma, breast fi-broadenoma (Figure 12), ectopic thyroid tis-sues, such as struma cordis and struma ovarii, other types of ovarian tumors, and teratoma has been suggested [107-115]. Using immuno-histochemical staining, Berger et al. [116] dem-onstrated the presence of high levels of func-tionally active NIS protein not only in normal breast tissue but also in a benign fibroade-noma. However, in a case of cystic meso-thelioma [117], results of immunohistochemical staining did not indicate the presence of NIS
Figure 10. Pathologic uptake of ra-dioiodine in a pulmonary fungus ball; A – planar scintigraphy, B – chest CT. Intense tracer uptake which is consid-ered as solitary pulmonary metastasis is observed in left lower lung field (A, arrows). Following chest CT revealed about 1.7 cm-sized cavitary lesion containing non-enhancing mural nod-ule (B, arrows). These findings sug-gested a pulmonary fungus ball rather than metastasis. This patient was clini-cally diagnosis to have pulmonary as-pergilloma based on radiologic fea-tures coupled with serologic evidence of precipitating antibodies to Aspergil-lus species [164].
Figure 11. Pathologic uptake of radioiodine in a su-perficial scab; A, B, and C – planar scintigraphy, D – photograph. Localized uptake of radioiodine is ob-served in left lower leg (A and B, arrows). On the lat-eral view, the uptake is considered to be located in anterior superficial portion of left lower leg (C, arrow). This finding suggests that the unusual uptake might not be related to skeletal metastasis. On physical examination, a superficial scab in the healing process of skin wound was detected in the shin of left leg (D, arrow). Iodine organification by leukocytes as part of their bactericidal effect can be the cause of unex-pected radioiodine uptake in posttraumatic clots or tissues [10].

False-positive uptakes on radioiodine scintigraphy
374 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Figure 12. Pathologic radioiodine uptake in benign fibroadenoma of the breast; A – planar scintigraphy, B – MR mam-mography. Post-therapy scintigraphy, performed 4 days after a second course of I-131 treatment, showed mild iodine uptake in the former thyroid bed as well as focal dystrophic radioiodine uptake in the region of the right breast (A, arrow). MR mammography showed a lesion in the right breast measuring 1 cm in diameter with slow, and at the bor-ders pronounced rise of signal intensity over time. No other focal breast lesions were detected. The figure shows the substraction image after and before contrast media injection, clearly demonstrating the contrast enhanced focal lesion in the right breast (B, arrow). Following histopathological examination revealed that the lesion was a benign fibroadenoma showing marked NIS-specific immunoreactivity. Adapted from ref. [116], with permission from Elsevier.
Table 5. Pathologic uptake related to benign tumor Region Mechanism of radioiodine uptake Reference Head and Neck
Meningioma Brain edema or high vascularity [118, 119] Cavernous angioma Unclear, possibly high vascularity [120] Warthin’s tumor Active transport in salivary glands [107-109] Oncocytoma of the parotid gland Increased vascularity, capillary permeability, and active I-
131 transport [110]
Osteoid osteoma of nasal bone Unclear, possibly high vascularity [125] Chest
Breast fibroadenoma Functional NIS expression [116] Cystic mesothelioma Passive diffusion and retention of radioiodine [117]
Struma cordis Functional NIS expression [115] Abdomen and pelvis Hepatic hemangioma Intravascular blood pooling and transcapillary escape of
iodine with interstitial retention [122]
Neurilemoma Unclear [175] Littoral cell angioma of spleen Prolonged pooling of I-131-laden blood within abnormal
cardiovascular structures [121]
Uterine myoma Unclear [176] Benign ovarian tumor
Struma ovarii Functional NIS expression [111, 177] Mucinous cystadenoma Functional NIS expression and fluid retention [112] Serous cystadenofibroma Functional NIS expression and fluid retention [114]
Rectal wall teratoma Functional NIS expression [178] Others Vertebral hemangioma Intravascular blood pooling and transcapillary escape of
iodine with interstitial retention [123, 124]

False-positive uptakes on radioiodine scintigraphy
375 Am J Nucl Med Mol Imaging 2012;2(3):362-385
expression. It can be speculated that passive diffusion alone might be a mechanism of ra-dioiodine uptake in certain benign tumors. Because meningioma with or without brain edema [118, 119], cavernous angioma [120], littoral cell angioma [121], hepatic [122] and vertebral [123, 124] hemangiomas, and osteoid osteoma [125] share the property that presents high vascularity, it can also be regarded as an-other mechanism of radioiodine uptake in a variety of benign tumors. Pathologic radioiodine uptake: malignant tumor Radioiodine accumulation has been reported in a variety of cancers, either primary or metasta-sis, involving the following organs: lung (adenocarcinoma, squamous cell carcinoma, large and small cell carcinoma, and bron-
chioloalveolar cell carcinoma), breast, stomach and cervix (adenocarcinoma), retroperitoneum (malignant fibrous histiocytoma), and liver and bone (metastatic adenocarcinoma) (Table 6). Expression of NIS is known to occur in more than 80% of breast cancer tissue, although the fraction of tumors that functionally concentrate iodine is likely to be much lower than that in thyroid cancer [29, 126]. NIS has also been reported in cancers involving bladder, cervix, oropharynx, colon, lung, pancreas, prostate, skin, stomach, ovary, and endometrium [127]. Of particular interest, absence of NIS was ob-served in normal lung alveolar tissue, yet posi-tive NIS expression was observed in approxi-mately two thirds of lung adenocarcinomas and squamous cell carcinomas [127]. This suggests that a cellular or subcellular change in iodine affinity as a consequence of malignant transfor-
Table 6. Pathologic uptake related to non-thyroidal malignant tumor Region Mechanism of radioiodine uptake Reference Chest
Primary lung cancer Functional NIS expression and tumoral inflamma-tory change
Adenocarcinoma [179-181] Squamous cell carcinoma [182]
Large cell carcinoma [183] Small cell carcinoma [184]
Bronchioloalveolar cell carcinoma + glandular secretion by mucinous lesion [185] Metastatic lung carcinoma Functional NIS expression and tumoral inflamma-
tory change
Cervical adenocarcinoma [186] Struma ovarii [187] Breast cancer Functional NIS expression and tumoral inflamma-
tory change [126, 188]
Abdomen and pelvis Metastatic hepatic tumor Functional NIS expression and tumoral inflamma-
tory change
Gastric adenocarcinoma [189] Struma ovarii [190-192] Malignant fibrous histiocytoma in
retroperitoneum Unclear, tumoral inflammatory process [193]
Malignant struma ovarii Functional NIS expression and tumoral inflamma-tory change
Ovarian tumor [194, 195] Peritoneal seeding [191, 196]
Others Metastatic bone tumor Functional NIS expression and tumoral inflamma-
tory change
Lung adenocarcinoma [180] Digestive adenocarcinoma [189, 197]

False-positive uptakes on radioiodine scintigraphy
376 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Table 7. Differential diagnosis according to the location and nature of radioiodine uptake Location Nature Differential diagnosis Additional findings Upper head Diffuse Perspiration in scalp or wig
Focal Brain or skull metastasis from thyroid cancer Not uncommon Eye metastasis from thyroid cancer Very uncommon [198, 199] Meningioma Half-lunar shaped Hematoma Crescent shaped Cavernous angioma Metallic suture Multiple in rows
Lower head Diffuse Physiologic accumulation of saliva Focal Skull metastasis from thyroid cancer Not uncommon
Salivary gland metastasis from thyroid cancer Very uncommon [199, 200] Mucocele and sinusitis Sialoadenitis Unilateral or bilateral Benign salivary tumors More localized than sialoadenitis Ectopic thyroid tissue Midline Various ductal retention and cysts
Outside of the body
Contamination to hair
Neck Diffuse Large amounts of remnant thyroid tissue Focal Metastatic lymph node and/or remnant thyroid tissue Common, single or multiple
Ectopic thyroid tissue and thyroglossal duct Midline Tracheostomy site Anterior, midline Contamination in necklace or scarf
Lung Diffuse Metastasis from thyroid cancer Not uncommon Pleural effusion Unilateral or bilateral: erect or decubitus view is
helpful Inflammatory lung disease Diffuse or perihilar distribution
Focal Metastasis from thyroid cancer Not uncommon Bronchiectasis Nodular, branching or perihilar distribution Inflammatory granuloma Primary or metastatic lung malignancy
Mediasti-num
Diffuse Physiologic thymic uptake Diffuse or dumbbell-shaped Pericardial effusion Halo-like uptake
Linear Esophageal retention Delayed imaging after water ingestion is helpful. Aortic aneurism Tracheal secretion Branching uptake
Focal Metastatic lymph node from thyroid cancer Not uncommon Ectopic thyroid tissue Esophageal diverticulum
Breast Diffuse Lactating or non-lactating breast Bilateral or unilateral Hyperprolactinemia Intense and relatively well localized
Focal Metastasis from thyroid cancer Very uncommon [201-203] Cysts or benign tumors Primary breast malignancy
Liver Diffuse Indicator of the presence of functioning thyroid tissue or hepatic dysfunction or hepatosteatosis
Focal Metastasis from thyroid cancer Uncommon [204-207] Cyst or hemangioma Biliary retention with/without stone Normal or inflamed gallbladder Metastasis from other malignancies
Kidney Focal Metastasis from thyroid cancer Uncommon [208-210] Cysts Urine retention Unilateral and bilateral Ectopic kidney
Gastrointes-tinal tract
Diffuse or seg-mental
Physiologic uptake
Focal Physiologic uptake Meckel’s diverticulum Colonic metastasis from struma ovarii Extremely uncommon [211]
Uterus Focal Metastasis from thyroid cancer Extremely uncommon [212] Menstruation Intrauterine device Myoma
Ovary Focal Struma ovarii Cysts or benign tumors
Bone Diffuse Increased physical activity Bilateral, long bones Focal Metastasis from thyroid cancer Not uncommon, single or multifocal
Osteoid osteoma Hemangioma Vertebra
Extremities Diffuse Inflammatory disease Focal Skin or soft tissue metastasis from thyroid cancer Uncommon [199, 213]
Trauma, superficial scab Contamination
Multiple sites
Multifocal Metastases from thyroid cancer or struma ovarii Not uncommon Metastases from other malignancies (lung, cervical or gastric cancer)
False-positive uptakes on radioiodine scintigraphy
377 Am J Nucl Med Mol Imaging 2012;2(3):362-385
mation leads to accumulation of radioiodine. Tumoral inflammatory response might also play a role in some parts of radioiodine uptake in malignant tumors. Inflammation is a well known microenvironment which is closely related with malignancies [128]. Summaries Almost 10 years have passed since previous researchers summarized extensively scattered reports in the literature involving cases of false-positive radioiodine uptake during surveillance of patients with DTC [23, 24]. Despite the in-comparable usefulness of radioiodine scintigra-phy, a wide variety of pitfalls, which negate its diagnostic confidence, have been consistently reported. By recognition of the exact localization of radioiodine uptake using emerging hybrid imaging, SPECT/CT, we can reduce the inci-dence of false-positive interpretation in planar WBS [129]. However, availability of SPECT/CT is still limited and some findings may remain am-biguous. Awareness of the nature and charac-teristics of radioiodine uptake, as described in Table 7, which provides a summarized review of unusual sites of metastasis and non-thyroidal uptake, might aid in differentiation of thyroidal and non-thyroidal, or benign and malignant up-take of radioiodine in the whole body. Conclusion In this review, physiology of the thyroid gland and a systemic overview of potential false-positive uptake of radioiodine in the whole body are provided along with illustrations and cases. By integrating the comprehension of physiology and characteristics of radioiodine uptake out-lined in this article with anatomical imaging, biochemical data, and clinical findings, physi-cians can be more confident in establishing proper management for patients with DTC using radioiodine WBS. Acknowledgement This research was financially supported by the Ministry of Knowledge Economy (MKE), Korea Institute for Advancement of Technology (KIAT), and Daegyeong Leading Industry Office through the Leading Industry Development for Economic Region, a Grant from the Nuclear Research & Development Program of the National Research Foundation of Korea (NRF) funded by the Minis-
try of Education, Science & Technology (MEST), and the Brain Korea 21 Project in 2012. Address correspondence to: Dr. Byeong-Cheol Ahn, Department of Nuclear Medicine, Kyungpook Na-tional University School of Medicine and Hospital, Daegu, South Korea. 50, Samduk 2-ga, Chung gu, Daegu, South Korea. 700-721 Tel: 82-53-420-5583; Fax: 82-53-422-0864; E-mail: [email protected] References [1] Siegel R, Naishadham D and Jemal A. Cancer
statistics, 2012. CA Cancer J Clin 2012; 62: 10-29.
[2] Wartofsky L and Nostrand DV. Thyroid Cancer: A Comprehensive Guide to Clinical Manage-ment. Totowa: Humana Press, 2006.
[3] Ahn BC. Sodium iodide symporter for nuclear molecular imaging and gene therapy: from bed-side to bench and back. Theranostics 2012; 2: 392-402.
[4] Chung JK. Sodium iodide symporter: its role in nuclear medicine. J Nucl Med 2002; 43: 1188-1200.
[5] Kogai T, Taki K and Brent GA. Enhancement of sodium/iodide symporter expression in thyroid and breast cancer. Endocr Relat Cancer 2006; 13: 797-826.
[6] Riesco-Eizaguirre G and Santisteban P. A per-spective view of sodium iodide symporter re-search and its clinical implications. Eur J Endo-crinol 2006; 155: 495-512.
[7] Pacini F. Follow-up of differentiated thyroid cancer. Eur J Nucl Med Mol Imaging 2002; 29 Suppl 2: S492-496.
[8] Lind P and Kohlfurst S. Respective roles of thyroglobulin, radioiodine imaging, and positron emission tomography in the assessment of thyroid cancer. Semin Nucl Med 2006; 36: 194-205.
[9] Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Stew-ard DL and Tuttle RM. Revised American Thy-roid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009; 19: 1167-1214.
[10] Gholamrezanezhad A. 12 Chapters on Nuclear Medicine. Rijeka: InTech, 2011.
[11] Amdur RJ and Mazzaferri EL. Essentials of Thy-roid Cancer Management. New York: Springer, 2005.
[12] Cavalieri RR. Iodine metabolism and thyroid physiology: current concepts. Thyroid 1997; 7: 177-181.
[13] Silberstein EB, Alavi A, Balon HR, Becker D, Charkes ND, Clarke SEM, Divgi CR, Donohoe KJ, Delbeke D, Goldsmith SJ, Meier DA, Sarkar SD and Waxman AD. Society of Nuclear Medi-cine Procedure Guideline for Scintigraphy for

False-positive uptakes on radioiodine scintigraphy
378 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Differentiated Papillary and Follicular Thyroid Cancer. 2006.
[14] Ma C, Kuang A, Xie J and Ma T. Possible expla-nations for patients with discordant findings of serum thyroglobulin and 131I whole-body scan-ning. J Nucl Med 2005; 46: 1473-1480.
[15] Rault E, Vandenberghe S, Van Holen R, De Beenhouwer J, Staelens S and Lemahieu I. Comparison of image quality of different iodine isotopes (I-123, I-124, and I-131). Cancer Bio-ther Radiopharm 2007; 22: 423-430.
[16] Lubberink M, Abdul Fatah S, Brans B, Hoekstra OS and Teule GJ. The role of (124)I-PET in diag-nosis and treatment of thyroid carcinoma. Q J Nucl Med Mol Imaging 2008; 52: 30-36.
[17] Bodei L, Kassis AI, Adelstein SJ and Mariani G. Radionuclide therapy with iodine-125 and other auger-electron-emitting radionuclides: experi-mental models and clinical applications. Can-cer Biother Radiopharm 2003; 18: 861-877.
[18] Peiffert D. [Insterstitial brachytherapy of local-ised prostate cancer using iodine 125 perma-nent implants]. Cancer Radiother 2005; 9: 388-393.
[19] Jiang P, Jiang Y, Wang JJ, Meng N, Ran W, Qu A and Yang R. Percutaneous ultrasonography-guided permanent iodine-125 implantation as salvage therapy for recurrent head and neck carcimonas. Cancer Biother Radiopharm 2011; 26: 753-757.
[20] Schwarz SB, Thon N, Nikolajek K, Niyazi M, Tonn JC, Belka C and Kreth FW. Iodine-125 brachytherapy for brain tumours - a review. Radiat Oncol 2012; 7: 30.
[21] Iagaru A and McDougall IR. Treatment of thyro-toxicosis. J Nucl Med 2007; 48: 379-389.
[22] Noussios G, Anagnostis P, Goulis DG, Lappas D and Natsis K. Ectopic thyroid tissue: anatomi-cal, clinical, and surgical implications of a rare entity. Eur J Endocrinol 2011; 165: 375-382.
[23] Shapiro B, Rufini V, Jarwan A, Geatti O, Kearfott KJ, Fig LM, Kirkwood ID and Gross MD. Arti-facts, anatomical and physiological variants, and unrelated diseases that might cause false-positive whole-body 131-I scans in patients with thyroid cancer. Semin Nucl Med 2000; 30: 115-132.
[24] Carlisle MR, Lu C and McDougall IR. The inter-pretation of 131I scans in the evaluation of thyroid cancer, with an emphasis on false posi-tive findings. Nucl Med Commun 2003; 24: 715-735.
[25] Chong A, Jeong SY, Kwon SY, Seo YS, Ha JM, Oh JR, Bom HS, Song HC and Min JJ. Dual lin-gual thyroid mimicking mono-ectopic thyroid in the anterior view of Tc-99m sodium pertech-netate thyroid scan. Nucl Med Mol Imaging 2008; 42: 485-486.
[26] Chung JK, Lee YJ, Jeong JM, Lee DS, Lee MC, Cho BY and Koh CS. Clinical significance of hepatic visualization on iodine-131 whole-body scan in patients with thyroid carcinoma. J Nucl
Med 1997; 38: 1191-1195. [27] Honour AJ, Myant NB and Rowlands EN. Secre-
tion of radioiodine in digestive juices and milk in man. Clin Sci 1952; 11: 449-462.
[28] Cho JY, Leveille R, Kao R, Rousset B, Parlow AF, Burak WE, Jr., Mazzaferri EL and Jhiang SM. Hormonal regulation of radioiodide uptake ac-tivity and Na+/I- symporter expression in mam-mary glands. J Clin Endocrinol Metab 2000; 85: 2936-2943.
[29] Tazebay UH, Wapnir IL, Levy O, Dohan O, Zuck-ier LS, Zhao QH, Deng HF, Amenta PS, Fineberg S, Pestell RG and Carrasco N. The mammary gland iodide transporter is expressed during lactation and in breast cancer. Nat Med 2000; 6: 871-878.
[30] Bakheet SM and Hammami MM. Patterns of radioiodine uptake by the lactating breast. Eur J Nucl Med 1994; 21: 604-608.
[31] Hammami MM and Bakheet S. Radioiodine breast uptake in nonbreastfeeding women: clinical and scintigraphic characteristics. J Nucl Med 1996; 37: 26-31.
[32] Hu LH, Wang SJ and Liu RS. Hyperprolactine-mia-related 131I Uptake in Nonlactating Breasts. Clin Nucl Med 2012; 37: e57-58.
[33] Davidson J and McDougall IR. How frequently is the thymus seen on whole-body iodine-131 diagnostic and post-treatment scans? Eur J Nucl Med 2000; 27: 425-430.
[34] Wilson LM, Barrington SF, Morrison ID, Kettle AG, O'Doherty MJ and Coakley AJ. Therapeutic implications of thymic uptake of radioiodine in thyroid carcinoma. Eur J Nucl Med 1998; 25: 622-628.
[35] Vermiglio F, Baudin E, Travagli JP, Caillou B, Fragu P, Ricard M and Schlumberger M. Iodine concentration by the thymus in thyroid carci-noma. J Nucl Med 1996; 37: 1830-1831.
[36] Michigishi T, Mizukami Y, Shuke N, Yokoyama K, Noguchi M, Watanabe Y, Matsui O, Aburano T, Tonami N and Hisada K. Visualization of the thymus with therapeutic doses of radioiodine in patients with thyroid cancer. Eur J Nucl Med 1993; 20: 75-79.
[37] Mello ME, Flamini RC, Corbo R and Mamede M. Radioiodine concentration by the thymus in differentiated thyroid carcinoma: report of five cases. Arq Bras Endocrinol Metabol 2009; 53: 874-879.
[38] Meller J and Becker W. The human sodium-iodine symporter (NIS) as a key for specific thymic iodine-131 uptake. Eur J Nucl Med 2000; 27: 473-474.
[39] Connolly LP and Connolly SA. Thymic uptake of radiopharmaceuticals. Clin Nucl Med 2003; 28: 648-651.
[40] Spitzweg C, Joba W, Eisenmenger W and Heu-felder AE. Analysis of human sodium iodide symporter gene expression in extrathyroidal tissues and cloning of its complementary de-oxyribonucleic acids from salivary gland, mam-

False-positive uptakes on radioiodine scintigraphy
379 Am J Nucl Med Mol Imaging 2012;2(3):362-385
mary gland, and gastric mucosa. J Clin Endocri-nol Metab 1998; 83: 1746-1751.
[41] Ziessman HA, Bahar H, Fahey FH and Dubi-ansky V. Hepatic visualization on iodine-131 whole-body thyroid cancer scans. J Nucl Med 1987; 28: 1408-1411.
[42] Omur O, Akgun A, Ozcan Z, Sen C and OzkiIic H. Clinical implications of diffuse hepatic uptake observed in postablative and post-therapeutic I-131 scans. Clin Nucl Med 2009; 34: 11-14.
[43] Rosenbaum RC, Johnston GS and Valente WA. Frequency of hepatic visualization during I-131 imaging for metastatic thyroid carcinoma. Clin Nucl Med 1988; 13: 657-660.
[44] Tatar FA, Morita E, Ituarte PH, Cavalieri RR, Duh QY, Price DC, Siperstein AE and Clark OH. Asso-ciation between residual thyroid carcinoma and diffuse hepatic uptake of 131I following ra-dioiodine ablation in postoperative total thyroi-dectomy patients. World J Surg 2001; 25: 718-722.
[45] Nishiyama Y, Yamamoto Y, Takahashi K, Na-kano S, Satoh K, Takashima H, Ohkawa M and Tanabe M. False-positive iodine-131 whole-body imaging due to gestational sac. Clin Nucl Med 1998; 23: 535-536.
[46] Di Cosmo C, Fanelli G, Tonacchera M, Ferrarini E, Dimida A, Agretti P, De Marco G, Vitti P, Pinchera A, Bevilacqua G, Naccarato AG and Viacava P. The sodium-iodide symporter expres-sion in placental tissue at different gestational age: an immunohistochemical study. Clin Endo-crinol (Oxf) 2006; 65: 544-548.
[47] Mitchell AM, Manley SW, Morris JC, Powell KA, Bergert ER and Mortimer RH. Sodium iodide symporter (NIS) gene expression in human placenta. Placenta 2001; 22: 256-258.
[48] Giuffrida D, Garofalo MR, Cacciaguerra G, Freni V, Ippolito A, Regalbuto C, Santonocito MG and Belfiore A. False positive 131I total body scan due to an ectasia of the common carotidis. J Endocrinol Invest 1993; 16: 207-211.
[49] Mena Bares LM, Vallejo Casas JA, Moreno Or-tega E, del Real Nunez R, Maza Muret FR and Latre Romero JM. I-131 visualization of thoracic aortic aneurysm after radioiodine administra-tion for thyroid carcinoma. Clin Nucl Med 2008; 33: 553-554.
[50] Varoglu E, Yildirim M, Bayrakdar R, Kantarci AM and Uslu H. Radioiodine pooling in dilated greater saphenous vein mimicking contamina-tion. Clin Nucl Med 2003; 28: 866-868.
[51] Muherji S, Ziessman HA, Earll JM and Keyes JW Jr. False-positive iodine-131 whole body scan due to pectus excavatum. Clin Nucl Med 1988; 13: 207-208.
[52] Mattern M and Staab E. I-131 localization in hematocolpos: a differential diagnosis consid-eration for pelvic I-131 uptake. Clin Nucl Med 2007; 32: 659-660.
[53] Rachinsky I and Driedger A. Iodine-131 uptake in a menstruating uterus: value of SPECT/CT in
distinguishing benign and metastatic iodine-positive lesions. Thyroid 2007; 17: 901-902.
[54] Wolff H, Breda DJ, Da Silva N and Hartmann AA. False-positive I-131 deposition in a parotid gland duct ectasia. Clin Nucl Med 1998; 23: 257-259.
[55] Yuoness S, Rachinsky I, Driedger AA and Belho-cine TZ. Differentiated thyroid cancer with epiphora: detection of nasolacrimal duct ob-struction on I-131 SPECT/CT. Clin Nucl Med 2011; 36: 1149-1152.
[56] Shin-Loong TC, Ki W and Sing-Fai L. False-Positive 131I Uptake in Fixed Prosthetic Den-ture. Clin Nucl Med 2012; 37: e64-66.
[57] Kienast O, Hofmann M, Ozer S, Dobrozemsky G, Dudczak R and Kurtaran A. Retention of iodine-131 in respiratory tract in a patient with papil-lary thyroid carcinoma after radionuclide ther-apy: a rare false-positive finding. Thyroid 2003; 13: 509-510.
[58] Nair N, Basu S and Pakhale H. Unusual uptake of radioiodine in the chest in a patient with thyroid carcinoma. Br J Radiol 2004; 77: 63-67.
[59] Knapska-Kucharska M and Makarewicz J. A case of iodine-131 retention in the esophagus mimicking a mediastinal metastasis in a pa-tient with follicular thyroid carcinoma after gas-tric volume reduction operation. Clin Nucl Med 2011; 36: 817-818.
[60] Caplan RH, Gundersen GA, Abellera RM and Kisken WA. Uptake of iodine-131 by a Meckel's diverticulum mimicking metastatic thyroid can-cer. Clin Nucl Med 1987; 12: 760-762.
[61] Bakheet SM, Hammami MM and Powe J. False-positive radioiodine uptake in the abdomen and the pelvis: radioiodine retention in the kid-neys and review of the literature. Clin Nucl Med 1996; 21: 932-937.
[62] You DL, Tzen KY, Chen JF, Kao PF and Tsai MF. False-positive whole-body iodine-131 scan due to intrahepatic duct dilatation. J Nucl Med 1997; 38: 1977-1979.
[63] Carlisle M, Cortes A and McDougall IR. Uptake of I-131 in the biliary tract: a potential cause of a false-positive result of scintiscan. Clin Nucl Med 1998; 23: 524-527.
[64] Zucker RJ, Bradley YC, Toney MO and Bridwell RS. Gastric volvulus detected with iodine-131 whole-body imaging. Clin Nucl Med 2000; 25: 303-305.
[65] Attard M, Marozzi P, Gambino L, Janni F, Salice P, Ficola U and Giuffrida D. False-positive re-sults of an iodine-131 whole-body scan caused by an ectopic kidney. Clin Nucl Med 2001; 26: 271-273.
[66] Seok JW, Kim SJ, Kim IJ, Kim YS and Kim YK. Normal gallbladder visualization during post-ablative iodine-131 scan of thyroid cancer. J Korean Med Sci 2005; 20: 521-523.
[67] Sioka C, Dimakopoulos N, Kouraklis G, Kotsa-lou I and Zouboulidis A. False-positive whole-

False-positive uptakes on radioiodine scintigraphy
380 Am J Nucl Med Mol Imaging 2012;2(3):362-385
body scan after I-131 therapy in a patient with intestinal scar. Clin Nucl Med 2006; 31: 232-233.
[68] De la Riva Perez PA, Castro Montano J, Iglesias Jerez R, Lopez Munoz N, Gil Martinez EM and Rodriguez de Quesada B. [Atypical uptake of gallbladder as cause of False-positive iodine-131 in post-surgical removal scanning of thy-roid remains]. Rev Esp Med Nucl 2007; 26: 52-53.
[69] Borkar S, Grewal R and Schoder H. I-131 up-take demonstrated in the appendix on a post-treatment scan in a patient with thyroid cancer. Clin Nucl Med 2008; 33: 551-552.
[70] Husmann L, Scheffel H, Stumpe K, Schmid S, Alkadhi H and Goerres GW. Pyelocaliceal diver-ticulum as a rare pitfall in I-131 post-therapy scanning. Clin Nucl Med 2010; 35: 443-444.
[71] Giuffrida D, Fornito MC, Pellegriti G, Regalbuto C and Vigneri G. False positive 131I total body scan due to bilateral polycystic renal disease. J Endocrinol Invest 1997; 20: 342-344.
[72] Wen C, Iuanow E, Oates E, Lee SL and Perrone R. Post-therapy iodine-131 localization in un-suspected large renal cyst: possible mecha-nisms. J Nucl Med 1998; 39: 2158-2161.
[73] Lungo M, Tenenbaum F, Chaumerliac P, Vons C, Mirat A, Beuzen F, Luton JP and Richard B. [Ovarian endometriosis cyst with iodine 131 uptake : first case of false positive in the follow up for differentiated thyroid carcinoma]. Ann Endocrinol (Paris) 2000; 61: 147-150.
[74] Letaief B, Boughattas S, Guezguez M, Hassine H and Essabbah H. Abdominal uptake of I-131 revealing a renal cyst. Clin Nucl Med 2001; 26: 255-256.
[75] Okuyama C, Ushijima Y, Kikkawa M, Yamagami T, Nakamura T, Kobayashi K, Hirota T and Ni-shimura T. False-positive I-131 accumulation in a liver cyst in a patient with thyroid carcinoma. Clin Nucl Med 2001; 26: 198-201.
[76] Gunawardana DH, Pitman AG and Lichtenstein M. Benign hepatic cyst mimicking a functional thyroid carcinoma metastasis on whole-body I-131 imaging. Clin Nucl Med 2003; 28: 527-528.
[77] Omur O, Ozbek SS, Akgun A, Yazici B, Mutlu-koca N and Ozcan Z. False-positive I-131 accu-mulation in a hepatic hydatid cyst. Clin Nucl Med 2007; 32: 930-932.
[78] Kraft O, Sirucek P, Mrhac L and Havel M. I-131 false positive uptake in a huge parapelvic renal cyst. Nucl Med Rev Cent East Eur 2011; 14: 36-37.
[79] Bural GG, Peel RL and Mountz JM. Benign epithelial cyst mimicking thyroid cancer metas-tasis: a false-positive finding on post-therapy I-131 scan. Clin Nucl Med 2012; 37: 88-90.
[80] Bohnen NI and Charron M. Isolated lower ex-tremity I-131 bone marrow uptake in a runner. Clin Nucl Med 2001; 26: 163-164.
[81] Ash L, Bybel B, Neumann D and Beebe W. The
helmet sign: Physiologic radioactive accumula-tion after 131I therapy--a case report. J Nucl Med Technol 2004; 32: 164-165.
[82] Bakheet SM, Hammami MM, Hemidan A, Powe JE and Bajaafar F. Radioiodine secretion in tears. J Nucl Med 1998; 39: 1452-1454.
[83] Beaulieu S, Djang D and Minoshima S. False-positive "necklace sign" on whole-body thyroid cancer survey--a case report. J Nucl Med Tech-nol 2005; 33: 42-43.
[84] Bhargava P and Choi WS. Artifactual I-131 ac-tivity in the hairs after thyroid remnant ablation. Thyroid 2006; 16: 1187-1189.
[85] Camponovo EJ, Goyer PF, Silverman ED, Kistler AM and Yudt WM. Axillary iodine-131 accumula-tion due to perspiration. Clin Nucl Med 1989; 14: 762-763.
[86] Dick C, Mudun A and Alazraki NP. False-positive I-131 images mimicking thyroid cancer metas-tasis. The nose ring sign. Clin Nucl Med 1995; 20: 876-877.
[87] Gritters LS, Wissing J, Gross MD and Shapiro B. Extensive salivary contamination due to concur-rent use of chewing tobacco during I-131 ra-dioablative therapy. Clin Nucl Med 1993; 18: 115-117.
[88] Ibis E, Wilson CR, Collier BD, Akansel G, Isitman AT and Yoss RG. Iodine-131 contamination from thyroid cancer patients. J Nucl Med 1992; 33: 2110-2115.
[89] Joyce WT and Cowan RJ. A potential false-positive posttherapy radioiodine scan secon-dary to I-131 excretion in perspiration. Clin Nucl Med 1995; 20: 368-369.
[90] Ozcan Kara P, Sari O, Gedik GK, Kocak I and Kaya B. An interesting contamination artifact appearing in I-(131) whole-body imaging after ablative therapy. Rev Esp Med Nucl 2011; 30: 36-37.
[91] Ozguven M, Ilgan S, Arslan N, Karacalioglu AO, Yuksel D and Dundar S. Unusual patterns of I-131 contamination. Ann Nucl Med 2004; 18: 271-274.
[92] Pochis WT, Krasnow AZ, Isitman AT, Cerletty JM, Kir KM, Hellman RS and Collier BD. The radio-active handkerchief sign. A contamination arti-fact in I-131 imaging for metastatic thyroid carcinoma. Clin Nucl Med 1990; 15: 491-494.
[93] Robinson PS, Barker P, Campbell A, Henson P, Surveyor I and Young PR. Iodine-131 in breast milk following therapy for thyroid carcinoma. J Nucl Med 1994; 35: 1797-1801.
[94] Roman MR, Larcos G and Devadas M. Lick your lips: a case of salivary contamination after I-131 therapy for thyroid carcinoma. Clin Nucl Med 2002; 27: 462.
[95] Rubow S and Klopper J. Excretion of radioio-dine in human milk following a therapeutic dose of I-131. Eur J Nucl Med 1988; 14: 632-633.
[96] Schechter D, Krausz Y, Moshe S, Rubinstein R and Chisin R. Radioiodine hot hand sign. Clin

False-positive uptakes on radioiodine scintigraphy
381 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Nucl Med 1998; 23: 378-379. [97] Zakavi SR and Kakhki VD. Exercise-induced
radio-iodine accumulation in scalp and hair during admission of 131I therapy for thyroid cancer. Thyroid 2006; 16: 1185-1186.
[98] Klebanoff SJ and Hamon CB. Role of myeloper-oxidase-mediated antimicrobial systems in intact leukocytes. J Reticuloendothel Soc 1972; 12: 170-196.
[99] Regalbuto C, Buscema M, Arena S, Vigneri R, Squatrito S and Pezzino V. False-positive find-ings on (131)I whole-body scans because of posttraumatic superficial scabs. J Nucl Med 2002; 43: 207-209.
[100] Brucker-Davis F, Reynolds JC, Skarulis MC, Fraker DL, Alexander HR, Weintraub BD and Robbins J. False-positive iodine-131 whole-body scans due to cholecystitis and sebaceous cyst. J Nucl Med 1996; 37: 1690-1693.
[101] Matheja P, Lerch H, Schmid KW, Kuwert T and Schober O. Frontal sinus mucocele mimicking a metastasis of papillary thyroid carcinoma. J Nucl Med 1997; 38: 1022-1024.
[102] Duque JJ, Miguel MB, Ruiz E, Castillo L, Claver M, Rubio MJ, Calvo JI, Rodriguez A, Zamora B and Casado C. False-positive I-131 whole-body scan in follicular thyroid carcinoma caused by frontal sinus mucocele. Clin Nucl Med 2000; 25: 137-138.
[103] Bakheet SM, Hammami MM and Powe J. Ra-dioiodine bronchogram in acute respiratory tract infection. Clin Nucl Med 1997; 22: 308-309.
[104] Jong I, Taubman K and Schlicht S. Bronchiecta-sis simulating pulmonary metastases on iodine-131 scintigraphy in well-differentiated thyroid carcinoma. Clin Nucl Med 2005; 30: 688-689.
[105] Picolos MK, Habra M, Safdar A and Sarlis NJ. Inactive pulmonary tuberculosis mimicking metastasis from papillary thyroid carcinoma in diagnostic radioiodine whole-body scintigraphy. Thyroid 2005; 15: 1105-1106.
[106] McEwan LM and Fong W. Unusual extrathy-roidal iodine accumulation in a post-ablative I-131 scan. Australas Radiol 2001; 45: 512-513.
[107] Ilgan S, Narin Y, Arslan N, Aksu A and Bayhan H. Warthin's tumor and I-131 body scan. Clin Nucl Med 1999; 24: 721-722.
[108] Caglar M, Tuncel M and Usubutun A. Increased uptake on I-131 whole-body scintigraphy in Warthin tumor despite false-negative Tc-99m pertechnetate salivary gland scintigraphy. Clin Nucl Med 2003; 28: 945-946.
[109] Gekeler J, Luers JC, Krohn T and Beutner D. False positive findings in F-18 FDG PET and whole body scans with I-131 in Warthin tumor of the parotid gland. Clin Nucl Med 2010; 35: 105-106.
[110] Broekhuizen-de Gast H, van Isselt H, Roef M and Lam M. Oncocytoma of the parotid gland causing false-positive result on I-131 whole-
body scintigraphy. Clin Nucl Med 2011; 36: 701-703.
[111] Macdonald W and Armstrong J. Benign struma ovarii in a patient with invasive papillary thyroid cancer: detection with I-131 SPECT-CT. Clin Nucl Med 2007; 32: 380-382.
[112] Agriantonis DJ, Hall L and Wilson MA. Pitfalls of I-131 whole body scan interpretation: broncho-genic cyst and mucinous cystadenoma. Clin Nucl Med 2008; 33: 325-327.
[113] Qiu ZL, Xu YH, Song HJ and Luo QY. Unusual (1)(3)(1)I uptake in a benign mucinous cystade-noma of the ovary in a patient with papillary thyroid cancer. Clin Nucl Med 2010; 35: 965-966.
[114] Flug J, Lameka K, Lee R, Katz DS, Sung WW and Yung E. False-positive I-131 uptake by an ovarian serous cystadenofibroma. Clin Nucl Med 2012; 37: 178-180.
[115] Rieser GD, Ober KP, Cowan RJ and Cordell AR. Radioiodide imaging of struma cordis. Clin Nucl Med 1988; 13: 421-422.
[116] Berger F, Unterholzner S, Diebold J, Kne-sewitsch P, Hahn K and Spitzweg C. Mammary radioiodine accumulation due to functional sodium iodide symporter expression in a benign fibroadenoma. Biochem Biophys Res Commun 2006; 349: 1258-1263.
[117] de Keizer B, Arsos G, Smit JW, Lam MG, Rinkes IH, Goldschmeding R and van Isselt JW. I-131 accumulation in a benign cystic mesothelioma in a patient with follicular thyroid cancer. Thy-roid 2008; 18: 369-371.
[118] Schmidt M, Scheidhauer K, Urbannek V, Luyken C, Friese M, Voth E and Schicha H. [Metastasizing follicular thyroid carcinoma with intracranial iodine 131 uptake in brain edema due to a frontal meningioma]. Nuklearmedizin 2000; 39: 38-39.
[119] Sinha P, Conrad GR and Holzhauer M. Inciden-tal detection of a falx meningioma on post-therapy radioiodide whole-body imaging. Clin Nucl Med 2002; 27: 916-917.
[120] Bulzico D, Vaisman F, Cordeiro de Noronha Pessoa CH and Corbo R. Cavernous angioma mimicking a differentiated thyroid carcinoma brain metastasis. Clin Nucl Med 2011; 36: 62-63.
[121] Mohan V, Jones RC, Drake AJ, 3rd, Daly PL and Shakir KM. Littoral cell angioma presenting as metastatic thyroid carcinoma to the spleen. Thyroid 2005; 15: 170-175.
[122] Karyagar S, Uyanik E, Mulazimoglu M and Karyagar SS. Uptake of (131)I on a post thyroid ablation whole body scan, due to cavernous liver hemangioma, mimicking metastases. Hell J Nucl Med 2009; 12: 177-178.
[123] Laguna R, Silva F, Vazquez-Selles J, Orduna E and Flores C. Vertebral hemangioma mimicking a metastatic bone lesion in well-differentiated thyroid carcinoma. Clin Nucl Med 2000; 25: 611-613.

False-positive uptakes on radioiodine scintigraphy
382 Am J Nucl Med Mol Imaging 2012;2(3):362-385
[124] Khan S, Dunn J, Strickland N and Al-Nahhas A. Iodine-123 uptake in vertebral haemangiomas in a patient with papillary thyroid carcinoma. Nucl Med Rev Cent East Eur 2008; 11: 30-33.
[125] Rachinsky I, Shelef I, Agranovich S and Lants-berg S. Is osteoid osteoma an iodophilic le-sion?: pathologically proved osteoid osteoma of nasal bone first seen on whole-body iodine-131 scan. Clin Nucl Med 2003; 28: 696-698.
[126] Wapnir IL, Goris M, Yudd A, Dohan O, Adelman D, Nowels K and Carrasco N. The Na+/I- sym-porter mediates iodide uptake in breast cancer metastases and can be selectively down-regulated in the thyroid. Clin Cancer Res 2004; 10: 4294-4302.
[127] Wapnir IL, van de Rijn M, Nowels K, Amenta PS, Walton K, Montgomery K, Greco RS, Dohan O and Carrasco N. Immunohistochemical profile of the sodium/iodide symporter in thyroid, breast, and other carcinomas using high den-sity tissue microarrays and conventional sec-tions. J Clin Endocrinol Metab 2003; 88: 1880-1888.
[128] Mantovani A, Allavena P, Sica A and Balkwill F. Cancer-related inflammation. Nature 2008; 454: 436-444.
[129] Oh JR, Byun BH, Hong SP, Chong A, Kim J, Yoo SW, Kang SR, Kim DY, Song HC, Bom HS and Min JJ. Comparison of (1)(3)(1)I whole-body imaging, (1)(3)(1)I SPECT/CT, and (1)F-FDG PET/CT in the detection of metastatic thyroid cancer. Eur J Nucl Med Mol Imaging 2011; 38: 1459-1468.
[130] Mulazimoglu M, Koca S, Tamam MO, Uyanik E and Ozpacaci T. False-positive findings in post-treatment iodine-131 whole-body scintigraphy in a nasolacrimal sac cyst, confirmed with SPECT/CT and MRI. Clin Nucl Med 2011; 36: 805-807.
[131] Feuerstein IM and Harbert JC. Hypertrophied thyroid tissue in a thyroglossal duct remnant. Clin Nucl Med 1986; 11: 135.
[132] Perros P, Mallick UK and Fenwick JD. Radioio-dine uptake in normal female breasts and liver of a patient with differentiated thyroid cancer imaged by whole body scanning. Thyroid 2003; 13: 511.
[133] Welcsh PL and Mankoff DA. Taking up iodide in breast tissue. Nature 2000; 406: 688-689.
[134] Hsiao E, Huynh T, Mansberg R, Bautovich G and Roach P. Diagnostic I-123 scintigraphy to as-sess potential breast uptake of I-131 before radioiodine therapy in a postpartum woman with thyroid cancer. Clin Nucl Med 2004; 29: 498-501.
[135] Sinha A, Bradley KM, Steatham J and Weaver A. Asymmetric breast uptake of radioiodine in a patient with thyroid malignancy: metastases or not? J R Soc Med 2008; 101: 319-320.
[136] Lin EC. Iodine-131 uptake in thymic hyperplasia with atypical computed tomographic features. Clin Nucl Med 2000; 25: 375.
[137] Ozdemir A, Gungor F, Ozugur S, Cubuk M, Boz A and Karayalcin B. Abnormal iodine-131 uptake in the mediastinum caused by achalasia. Clin Nucl Med 1998; 23: 706-707.
[138] Boulahdour H, Meignan M, Melliere D, Braga F and Galle P. False-positive I-131 scan induced by Zenker's diverticulum. Clin Nucl Med 1992; 17: 243-244.
[139] Song HC, Kim SM, Heo YJ and Bom HS. Reten-tion of iodine-131 in a thoracic esophageal diverticulum mimicking metastatic thyroid can-cer. Clin Nucl Med 2002; 27: 896-897.
[140] Rashid K, Johns W, Chasse K, Walker M and Gupta SM. Esophageal diverticulum presenting as metastatic thyroid mass on iodine-131 scin-tigraphy. Clin Nucl Med 2006; 31: 405-408.
[141] Nguyen BD and Roarke MC. Epiphrenic diver-ticulum: potential pitfall in thyroid cancer iodine-131 scintigraphy. Clin Nucl Med 2005; 30: 631-632.
[142] Schuster DM and Alazraki N. Esophageal scar-ring causing false-positive uptake on I-131 whole-body imaging. Clin Nucl Med 1998; 23: 334.
[143] Freeman M, Roach P, Robinson B and Shields M. Hiatal hernia in iodine-131 scintigraphy: a potential cause of false-positive midline tho-racic uptake. Clin Nucl Med 2003; 28: 709-710.
[144] Ceylan Gunay E and Erdogan A. Mediastinal radioiodine uptake due to hiatal hernia: a false-positive reason in 131I scan. Rev Esp Med Nucl 2010; 29: 95.
[145] Francese C, Schlumberger M, Travagli JP, Vera P, Caillou B and Parmentier C. Iodine 131 up-take in a pleuropericardial cyst: case report of a false-positive radioiodine total body scan result in a patient with a thyroid cancer. Eur J Nucl Med 1991; 18: 779-780.
[146] Lejeune M, Heron C, Tenenbaum F, Sarfati PO, Louvel A, Luton JP and Richard B. [Iodine 131 uptake by a bronchogenic cyst in a patient with differentiated carcinoma of the thyroid gland]. Presse Med 2000; 29: 1345-1347.
[147] Kayano D, Michigishi T, Ichiyanagi K, Inaki A and Kinuya S. I-131 uptake in a thymic cyst. Clin Nucl Med 2010; 35: 438-439.
[148] Serafini A, Sfakianakis G, Georgiou M and Mor-ris J. Breast cyst simulating metastases on iodine-131 imaging in thyroid carcinoma. J Nucl Med 1998; 39: 1910-1912.
[149] Bakheet SM and Hammami MM. False-positive radioiodine whole-body scan in thyroid cancer patients due to unrelated pathology. Clin Nucl Med 1994; 19: 325-329.
[150] Turoglu HT, Naddaf S, Young I and Abdel-Dayem HM. Infected sebaceous cyst. A cause for false-positive total-body I-123 metastatic survey for thyroid cancer. Clin Nucl Med 1996; 21: 887.
[151] Kinuya S, Yokoyama K, Michigishi T and Tonami N. I-131 accumulation in folliculitis of the scalp.
False-positive uptakes on radioiodine scintigraphy
383 Am J Nucl Med Mol Imaging 2012;2(3):362-385
Clin Nucl Med 1996; 21: 807-808. [152] Kolla IS, Alazraki NP and Watts NB. Sialadenitis
mimicking metastatic thyroid carcinoma. Clin Nucl Med 1989; 14: 564-566.
[153] Carlisle MR and McDougall IR. Dramatic parotid uptake of I-131 on a diagnostic whole-body scan. Clin Nucl Med 2000; 25: 895-897.
[154] Bakheet SM, Hammami MM, Powe J and Lars-son S. Radioiodine uptake in the head and neck. Endocr Pract 2000; 6: 37-41.
[155] Schmidt M, Dietlein M, Schroder U and Schicha H. False-positive uptake of I-131 in a laryngo-cele mimicking thyroid remnant after thyroidec-tomy for papillary thyroid carcinoma. Clin Nucl Med 2006; 31: 716-717.
[156] Niepomniszcze H and Schere D. How to distin-guish between radioiodine accumulation in a laryngocele from a radioiodine-concentrating thyroid remnant after thyroidectomy for papil-lary carcinoma. Thyroid 2004; 14: 867-868.
[157] Ong SC, Eng DN, Sundram FX and Chan LL. A novel case of false-positive I-131 whole-body scan in thyroid carcinoma caused by subdural hematoma. Clin Nucl Med 2004; 29: 164-166.
[158] Ain KB and Shih WJ. False-positive I-131 up-take at a tracheostomy site. Discernment with Tl-201 imaging. Clin Nucl Med 1994; 19: 619-621.
[159] Vallejo Casas JA, Mena Bares ML, Galvez Mo-reno MA and Latre Romero JM. [Tracheostomy cannula as a cause of false positive result on the whole-body scan with (131)I in the follow-up of differentiated thyroid cancer]. Rev Esp Med Nucl 2011; 30: 384-385.
[160] Modoni S, Martino G, Guerra M and Frusciante V. Unusual radioiodine uptake caused by metal-lic sutures in the skull in a patient with thyroid cancer. Clin Nucl Med 2000; 25: 1053-1054.
[161] Campenni A, Minutoli F, Pecorella GR and Bal-dari S. Unusual radioiodine uptake in a patient with thyroid cancer and cranial metallic clips. Nuklearmedizin 2002; 41: N89-N90.
[162] Bakheet SM, Powe J and Hammami MM. Ra-dioiodine uptake in the chest. J Nucl Med 1997; 38: 984-986.
[163] Bakheet SM, Hammami MM and Powe J. Ra-dioiodine uptake in rheumatoid arthritis-associated lung disease mimicking thyroid can-cer metastases. Clin Nucl Med 1998; 23: 319-320.
[164] Ahn BC, Lee SW, Lee J and Kim C. Pulmonary aspergilloma mimicking metastasis from papil-lary thyroid cancer. Thyroid 2011; 21: 555-558.
[165] Pina JS, Meyer CA, Billingsley JL, Matlock JP, Horan MP and Knodel DH. Inflammatory dis-eases of the lung causing false-positive 131io-dine whole body scans in the evaluation of papillary thyroid carcinoma. Two case reports. Chest 1996; 110: 565-567.
[166] Song HC, Heo YJ, Kim SM and Bom HS. Iodine-131 uptake in focal bronchiectasis mimicking metastatic thyroid cancer. Clin Nucl Med 2003;
28: 351-352. [167] Mason DT, Frye RL and Wagner HN, Jr. Radio-
isotope scanning of the precordial distribution of iodide in patients with myocardial infarction. Circulation 1961; 24: 1338-1341.
[168] Dreyfuss F, Ben-Porath M and Menczel J. Ra-dioiodine uptake by the infarcted heart. Am J Cardiol 1960; 6: 237-245.
[169] Geatti O, Shapiro B, Orsolon PG, Mirolo R and Di Donna A. An unusual false-positive scan in a patient with pericardial effusion. Clin Nucl Med 1994; 19: 678-682.
[170] Lopez Aznar D, Garcia Sanchis L, Rivas San-chez A, Alonso Monfort J, Hervas Benito I and Mateo Navarro A. [Pericardial effusion as a possible cause of false positives in I-131 ra-dionuclide scans]. Rev Esp Med Nucl 1998; 17: 158-161.
[171] Maslack MM and Wilson CA. Iodine-131 accu-mulation in a pericardial effusion. J Nucl Med 1987; 28: 133.
[172] Mitchell G, Pratt BE, Vini L, McCready VR and Harmer CL. False positive 131I whole body scans in thyroid cancer. Br J Radiol 2000; 73: 627-635.
[173] Naddaf SY, Akisik MF, Omar WS, Young I and Abdel-Dayem HM. I-123 uptake in the chest wall after needle biopsy of a pulmonary nodule. A cause for false-positive I-123 uptake. Clin Nucl Med 1997; 22: 572-573.
[174] Otsuka N, Fukunaga M, Morita K, Ono S, Nagai K, Katagiri M, Harada T and Morita R. Iodine-131 uptake in a patient with thyroid cancer and rheumatoid arthritis during acupuncture treat-ment. Clin Nucl Med 1990; 15: 29-31.
[175] Wang PW, Chen HY, Li CH and Chen WJ. Uptake of I-131 by an abdominal neurilemoma mimick-ing metastatic thyroid carcinoma. Clin Nucl Med 1993; 18: 964-966.
[176] Hirata K, Shiga T, Kubota KC, Okamoto S, Kamibayashi T and Tamaki N. Radioiodine ther-apy for thyroid cancer depicted uterine leio-myoma. Clin Nucl Med 2009; 34: 180-181.
[177] Deandreis D, Lumbroso J, Al Ghuzlan A, Baudin E, Schlumberger M and Leboulleux S. Abnormal pelvic uptake on post-therapeutic radioiodine (131I) whole-body scan. Eur J Nucl Med Mol Imaging 2011; 38: 1957.
[178] Lakshmanan M, Reynolds JC, Del Vecchio S, Merino MJ, Norton JA and Robbins J. Pelvic radioiodine uptake in a rectal wall teratoma after thyroidectomy for papillary carcinoma. J Nucl Med 1992; 33: 1848-1850.
[179] Fernandez-Ulloa M, Maxon HR, Mehta S and Sholiton LJ. Iodine 131 uptake by primary lung adenocarcinoma. Misinterpretation of 131I scan. JAMA 1976; 236: 857-858.
[180] Langsteger W, Lind P, Koltringer P, Beham A and Eber O. Misinterpretation of iodine uptake in papillary thyroid carcinoma and primary lung adenocarcinoma. J Cancer Res Clin Oncol 1990; 116: 8-12.
False-positive uptakes on radioiodine scintigraphy
384 Am J Nucl Med Mol Imaging 2012;2(3):362-385
[181] Langsteger W, Koltringer P, Wolf G, Eber B, Semlitsch G and Eber O. False-positive radioio-dine uptake in lung carcinoma. J Nucl Med 1994; 35: 2056-2057.
[182] Misaki T, Takeuchi R, Miyamoto S, Kasagi K, Matsui Y and Konishi J. Radioiodine uptake by squamous-cell carcinoma of the lung. J Nucl Med 1994; 35: 474-475.
[183] Acosta J, Chitkara R, Khan F, Azueta V and Sil-ver L. Radioactive iodine uptake by a large cell undifferentiated bronchogenic carcinoma. Clin Nucl Med 1982; 7: 368-369.
[184] Haubold-Reuter BG, Landolt U and von Schul-thess GK. Bronchogenic carcinoma mimicking metastatic thyroid carcinoma. J Nucl Med 1993; 34: 809-811.
[185] Malhotra G, Nair N, Menon H, Gujral S, Abhy-ankar A, Baghel NS, Awasare S, Nabar SJ, Abhy-ankar S and Kand PG. Bronchoalveolar carci-noma of lung masquerading as iodine avid metastasis in a patient with minimally invasive follicular carcinoma of thyroid. Clin Nucl Med 2008; 33: 26-29.
[186] Sohn MH, Kim MW, Lim ST, Lee NR, Song EK and Yim CY. Radioiodine uptake by metastatic nonthyroidal adenocarcinoma of the lung in a patient with papillary thyroid carcinoma. Clin Nucl Med 2005; 30: 269-270.
[187] Ruel IF, Fierrard H, Vercellino L, Bernard L, Hin-die E, Duron F and Toubert ME. Pulmonary me-tastasis of struma ovarii: a case report. Clin Nucl Med 2010; 35: 692-694.
[188] Eskin BA. Iodine and mammary cancer. Adv Exp Med Biol 1977; 91: 293-304.
[189] Wu SY, Kollin J, Coodley E, Lockyer T, Lyons KP, Moran E, Parker LN and Yu AC. I-131 total-body scan: localization of disseminated gastric ade-nocarcinoma. Case report and survey of the literature. J Nucl Med 1984; 25: 1204-1209.
[190] Konez O, Hanelin LG, Jenison EL, Goyal M and Randolph W. Functioning liver metastases on an I-131 whole-body scan: a case of malignant struma ovarii. Clin Nucl Med 2000; 25: 465-496.
[191] Cherng SC, Wang YF, Fan YM, Chen CY, Yuan YN and Cheng CY. Malignant struma ovarii with peritoneal implants and pelvic structures and liver metastases demonstrated by I-131 SPECT and low-dose CT. Clin Nucl Med 2005; 30: 797-798.
[192] McDougall IR. Metastatic struma ovarii: the burden of truth. Clin Nucl Med 2006; 31: 321-324.
[193] Acar E, Akgun A, Kocacelebi K, Kumanlioglu K and Tuncyurek M. I-131 uptake in malignant fibrous histiocytoma. Clin Nucl Med 2007; 32: 580-581.
[194] Lim ST, Jeong HJ, Chung MJ, Yim CY and Sohn MH. Malignant struma ovarii demonstrated on post-therapy radioiodine scan after total thyroi-dectomy for papillary thyroid cancer. Clin Nucl Med 2008; 33: 429-431.
[195] Kraft O, Mrhac L, Sirucek P, Dvorackova J, Chmelova J, Graf P and Sevcik L. I-131 uptake in an ovarian tumor: differential diagnosis for abdominal I-131 uptake. Clin Nucl Med 2009; 34: 390-392.
[196] McGill JF, Sturgeon C and Angelos P. Metastatic struma ovarii treated with total thyroidectomy and radioiodine ablation. Endocr Pract 2009; 15: 167-173.
[197] Ajmi S, Ben Ali K, Ben Fredj M, Ghannouchi N, Khalifa M and Letaief A. Tc-99m and I-131 uptake in widespread bone metastases from undetectable digestive adenocarcinoma. Clin Nucl Med 2011; 36: 1020-1022.
[198] Huang IC, Chou FF, Liu RT, Tung SC, Chen JF, Kuo MC, Hsieh CJ and Wang PW. Long-term outcomes of distant metastasis from differenti-ated thyroid carcinoma. Clin Endocrinol (Oxf) 2012; 76: 439-447.
[199] Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lum-broso JD, De Vathaire F and Schlumberger M. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab 2006; 91: 2892-2899.
[200] Seifert G, Hennings K and Caselitz J. Metastatic tumors to the parotid and submandibular glands--analysis and differential diagnosis of 108 cases. Pathol Res Pract 1986; 181: 684-692.
[201] Chisholm RC, Chung EB, Tuckson W, Khan T and White JE. Follicular carcinoma of the thy-roid with metastasis to the breast. J Natl Med Assoc 1980; 72: 1101-1104.
[202] Cristallini EG, Ascani S, Nati S, Liberati F and Farabi R. Breast metastasis of thyroid follicular carcinoma. Acta Oncol 1994; 33: 71-73.
[203] Fiche M, Cassagnau E, Aillet G, Bailly J, Chupin M, Classe JM and Bodic MF. [Breast metastasis from a "tall cell variant" of papillary thyroid car-cinoma]. Ann Pathol 1998; 18: 130-132.
[204] Kouso H, Ikegami T, Ezaki T, Ishida T, Aimitsu S, Fujihara M and Mori M. Liver metastasis from thyroid carcinoma 32 years after resection of the primary tumor: report of a case. Surg Today 2005; 35: 480-482.
[205] Shah DH and Samuel AM. Metastasis to the liver in well-differentiated carcinoma of the thyroid. Thyroid 1996; 6: 607-611.
[206] Casara D, Busnardo B and Cimitan M. Liver metastases from differentiated thyroid carci-noma. J Nucl Med Allied Sci 1981; 25: 53-54.
[207] Atmaram SH, Ganatra RD, Sharma SM and Ramanna L. Functioning metastases in liver from thyroid carcinoma: case report. J Nucl Med 1975; 16: 919-921.
[208] Oh JR, Lim JH, Jeong SY, Heo SH, Chong A and Min JJ. Simultaneous uptake of I-131 and F-18 FDG by a renal metastasis of thyroid papillary cancer. Clin Nucl Med 2011; 36: 798-799.

False-positive uptakes on radioiodine scintigraphy
385 Am J Nucl Med Mol Imaging 2012;2(3):362-385
[209] Liou MJ, Lin JD, Chung MH, Liau CT and Hsueh C. Renal metastasis from papillary thyroid mi-crocarcinoma. Acta Otolaryngol 2005; 125: 438-442.
[210] Cheon M, Choi JY, Kim HK, Chung J-H, Ko YH, Kim YE, Choi D, Lee K-H and Kim B-T. Renal metastasis from follicular thyroid carcinoma diagnosed by I-131 whole-body scan mimicking renal cell carcinoma on contrast-enhanced computed tomography. Nucl Med Mol Imaging 2011; 45: 72-75.
[211] Yang CW, Liang WY, Lin JK, Chiou TJ, Lee CH and Jiang JK. Colonic metastasis from a papil-lary thyroid carcinoma arising in struma ovarii. Int J Colorectal Dis 2010; 25: 913-914.
[212] Benbassat CA, Mechlis-Frish S and Hirsch D. Clinicopathological characteristics and long-term outcome in patients with distant metasta-ses from differentiated thyroid cancer. World J Surg 2006; 30: 1088-1095.
[213] Caobelli F, Paghera B, Panarotto MB, Camoni L and Giubbini R. Two distant muscular metasta-ses from papillary carcinoma of the thyroid demonstrated by 18F-FDG PET/CT and con-firmed by biopsy. Nucl Med Mol Imaging 2011; 45: 324-325.