Review articlejpp.krakow.pl/journal/archive/04_14/pdf/157_04_14_article.pdf · and methods of...
13
INTRODUCTION Stem cell biology is one of the most challenging and exciting fields of modern science, and at the same time one of the most controversial. Attitudes toward stem cell research have changed significantly in recent decades as a result of the complexity of the subject. This complexity is reflected in the diversity of hypotheses and methods of analysis using various cell lines, laboratory animals, and human tissue samples. Stem cell research has accelerated even more vigorously since the first population of tumor-initiating cells, also known as cancer stem cells (CSCs), was identified in human leukemia (1). According to the CSCs hypothesis, a small self-renewing population of cells within hematologic cancers or solid tumors plays a critical role in cancer initiation, progression, and metastasis (2). Despite the significant progress to date, the nature of many biological processes which account for CSC properties still remains unclear. There are several pertinent topics currently under active investigation including the molecular pathways regulating CSCs functions, the role of the CSC’s niche and its “plasticity” characteristics, specific CSCs biomarkers in all cancer types, ideal marker(s) and ideal assay(s) for CSC markers, variable frequency of CSCs between tumors, instability of the CSC’s phenotype, the existence of multiple CSC pools within individual tumors, the nature of metastatic CSCs, the resistance of CSCs to cytotoxic chemotherapy and low-dose radiation treatment, and the prognostic significance of CSCs. More details about the biological properties of CSCs can be found in the comprehensive review published by Visvader et al. (3). Scientific attention is also currently focused on the discovery and development of novel drugs that can selectively target and destroy CSCs. In the face of these challenges, many biopharmaceutical companies around the globe are investing in new anti-CSC drug programs. Numerous anti-CSC compounds have already entered human clinical trials, and some have successfully completed different phases of testing (4-6). Since it is beyond the scope of this review to cover the detailed evaluation of each anti-CSC drug candidate we will highlight only the most important properties of anti-CSC drugs and discuss how these properties relate to the drug development process. THERAPEUTIC APPROACHES TO TARGET CANCER STEM CELLS The different types of anti-cancer stem cells therapeutics and their characteristics The majority of anti-CSC drugs can be divided into three major groups: the first group of therapeutic biologics includes monoclonal antibodies, human vaccines, cellular immunotherapeutics, therapeutic peptides, and microRNA- based therapeutics (7-12). The second group of therapeutics JOURNAL OF PHYSIOLOGY AND PHARMACOLOGY 2014, 65, 2, 157-169 www.jpp.krakow.pl Review article I. SKIDAN 1 , S.C.J. STEINIGER 2 IN VIVO MODELS FOR CANCER STEM CELL RESEARCH: A PRACTICAL GUIDE FOR FREQUENTLY USED ANIMAL MODELS AND AVAILABLE BIOMARKERS 1 Pharmapt, Inc., Chelsea, MA 02150, USA; 2 Institute of Pharmaceutical Technology, Johann Wolfgang Goethe University, Frankfurt/Main, Germany The identification of a rare population of cancer stem cells whose presence in tumors is believed to determine their growth and metastatic activity, has provided a novel approach for targeted anti-cancer therapy. At the in vivo stage of the development of new therapeutic approaches for killing cancer stem cells, the most significant issues are the appropriate choice of rational animal models that offer the option to select animal species, strains and substrains, essential techniques for the inoculation of tumors, and methods of tumor detection in animals. The identification and validation of various types of cancer stem cell markers, which could serve as potential marker(s) of therapeutic efficacy of applied drugs, is a considerable challenge. The aim of this review is to provide a guide for the in vivo study of novel therapeutics that target cancer stem cells. This review describes frequently used mouse solid tumor models and evaluates their usefulness for cancer stem cell research. The classification of existing compounds that are used in today’s experimental anti-cancer stem cell therapy and examples of exploratory first-in-human studies using these compounds for selective elimination of cancer stem cells will also be discussed. Finally, this review will examine the current status of available cancer stem cell markers, and highlight several important cancer stem cell properties that are still not well understood, but could influence the anti-cancer drug development process. Key words: cancer stem cells, tumor models, patient-derived xenograft, immunodeficient mice, humanized mice, biomarkers
Transcript of Review articlejpp.krakow.pl/journal/archive/04_14/pdf/157_04_14_article.pdf · and methods of...

INTRODUCTION
Stem cell biology is one of the most challenging and excitingfields of modern science, and at the same time one of the mostcontroversial. Attitudes toward stem cell research have changedsignificantly in recent decades as a result of the complexity of thesubject. This complexity is reflected in the diversity of hypothesesand methods of analysis using various cell lines, laboratoryanimals, and human tissue samples. Stem cell research hasaccelerated even more vigorously since the first population oftumor-initiating cells, also known as cancer stem cells (CSCs),was identified in human leukemia (1). According to the CSCshypothesis, a small self-renewing population of cells withinhematologic cancers or solid tumors plays a critical role in cancerinitiation, progression, and metastasis (2). Despite the significantprogress to date, the nature of many biological processes whichaccount for CSC properties still remains unclear. There are severalpertinent topics currently under active investigation including themolecular pathways regulating CSCs functions, the role of theCSC’s niche and its “plasticity” characteristics, specific CSCsbiomarkers in all cancer types, ideal marker(s) and ideal assay(s)for CSC markers, variable frequency of CSCs between tumors,instability of the CSC’s phenotype, the existence of multiple CSCpools within individual tumors, the nature of metastatic CSCs, theresistance of CSCs to cytotoxic chemotherapy and low-doseradiation treatment, and the prognostic significance of CSCs.
More details about the biological properties of CSCs can be foundin the comprehensive review published by Visvader et al. (3).Scientific attention is also currently focused on the discovery anddevelopment of novel drugs that can selectively target and destroyCSCs. In the face of these challenges, many biopharmaceuticalcompanies around the globe are investing in new anti-CSC drugprograms. Numerous anti-CSC compounds have already enteredhuman clinical trials, and some have successfully completeddifferent phases of testing (4-6). Since it is beyond the scope ofthis review to cover the detailed evaluation of each anti-CSC drugcandidate we will highlight only the most important properties ofanti-CSC drugs and discuss how these properties relate to the drugdevelopment process.
THERAPEUTIC APPROACHES TO TARGET CANCER STEM CELLS
The different types of anti-cancer stem cells therapeutics andtheir characteristics
The majority of anti-CSC drugs can be divided into threemajor groups: the first group of therapeutic biologics includesmonoclonal antibodies, human vaccines, cellularimmunotherapeutics, therapeutic peptides, and microRNA-based therapeutics (7-12). The second group of therapeutics
JOURNAL OF PHYSIOLOGY AND PHARMACOLOGY 2014, 65, 2, 157-169www.jpp.krakow.pl
Review article
I. SKIDAN1, S.C.J. STEINIGER2
IN VIVO MODELS FOR CANCER STEM CELL RESEARCH: A PRACTICAL GUIDEFOR FREQUENTLY USED ANIMAL MODELS AND AVAILABLE BIOMARKERS
1Pharmapt, Inc., Chelsea, MA 02150, USA; 2Institute of Pharmaceutical Technology, Johann Wolfgang Goethe University, Frankfurt/Main, Germany
The identification of a rare population of cancer stem cells whose presence in tumors is believed to determine theirgrowth and metastatic activity, has provided a novel approach for targeted anti-cancer therapy. At the in vivo stage ofthe development of new therapeutic approaches for killing cancer stem cells, the most significant issues are theappropriate choice of rational animal models that offer the option to select animal species, strains and substrains,essential techniques for the inoculation of tumors, and methods of tumor detection in animals. The identification andvalidation of various types of cancer stem cell markers, which could serve as potential marker(s) of therapeutic efficacyof applied drugs, is a considerable challenge. The aim of this review is to provide a guide for the in vivo study of noveltherapeutics that target cancer stem cells. This review describes frequently used mouse solid tumor models and evaluatestheir usefulness for cancer stem cell research. The classification of existing compounds that are used in today’sexperimental anti-cancer stem cell therapy and examples of exploratory first-in-human studies using these compoundsfor selective elimination of cancer stem cells will also be discussed. Finally, this review will examine the current statusof available cancer stem cell markers, and highlight several important cancer stem cell properties that are still not wellunderstood, but could influence the anti-cancer drug development process.
K e y w o r d s : cancer stem cells, tumor models, patient-derived xenograft, immunodeficient mice, humanized mice, biomarkers

that target CSC is small molecules (13-15), and the third ischemical compounds that not specifically designed for useagainst CSCs, but which have recently been found to have anti-CSC properties (16-22).
The complex pharmacokinetic behaviour, various modes ofactions, and toxicity of therapeutic biologics are mainlydetermined by their various physicochemical properties. Forexample, therapeutic monoclonal antibodies (mAbs), the mostcommon type of biologics, do not readily cross cell membranesdue to their large size, usually resulting in low tumor tissuepenetration. However, mAbs interact with a wide range ofextracellular signaling molecules and cell-surface proteinstriggering various events involved in cancer cell death. Thepresence of two identical antigen-binding sites in mAbs offers anexceedingly high selectivity and binding affinity for the intendedtarget tumor cell antigens, including CSCs antigens. In addition,one of mAbs’ important modes of action is their interaction withthe immune system. An example is the immune-mediated cellkilling mechanisms, which include induction of phagocytosis,complement activation, antibody-dependent cell-mediatedcytotoxicity, target gene-modified T cells, and activation of T cells through inhibition of T cell inhibitory receptors andantibody-mediated cross presentation of antigen to DC-cells(23). Some biologics such as RNA-based therapeutics can haveoff-target effects (24, 25) and typically require special deliverysystems for efficient transport to the target cells (26). Anothertype of biologic is therapeutic vaccines. The specific immuneresponses caused by vaccines are often weak due to the lack of
co-stimulatory signals and specificity to antigens (27). Ingeneral, biologics are sensitive to temperature changes,susceptible to microbial contamination, and easily degrade in thegastrointestinal (GI)-tract before reaching the systemiccirculation. Furthermore, such therapeutics are often difficultand expensive to manufacture (28, 29).
In contrast to biologics, the common characteristics of smallmolecules include a low molecular weight, rapid entry intosystemic circulation through blood capillaries, usually a shorthalf-life, poor selectivity, and typically a lack of high specificity.However, current data are ambiguous and biased toward certaintarget classes, most prominently human G-protein-coupledreceptors and kinases, specifically tyrosine kinases (30). Unlikemany biologics, small molecules readily diffuse across cellmembranes and reach intracellular targets. However, they areoften limited to protein targets due to small binding pockets withwhich they can bind and alter the rates of specific intracellularsignaling pathways (31). A major safety concern with smallmolecules is toxicity to different organs and systems where theypotentially accumulate. Additionally, the therapeuticapplicability of small molecules is often limited by their lowaqueous solubility. Because of this, they require stable aqueousformulations for the intravenous administration. In case of oraladministrations, special delivery systems are needed to maintain,enhance, or facilitate small molecule absorption from the GI-tract (30, 31).
As mentioned above, the third group may include a varietyof chemical compounds alone and in combinations with drugs
158
Drugs * Reference
Monoclonal Antibodies:OMP-21M18, (Demcizumab - anti-DLL4 humanized monoclonal antibody) [NCT01189968] **RO5429083 (Anti-CD44 recombinant human monoclonal antibody) [NCT01358903]OMP-18R5 (Vantictumab - human monoclonal antibody (anti-Frizzled) [125]AVE1642 (The insulin-like growth factor-I receptor (IGF-IR) monoclonal antibody) [126]MT110 (EpCAM/CD3-bispecific antibody) [20]
Human Vaccines and Cellular Immunotherapeutics, Peptides, MicroRNA-based Therapeutics:
CD40 ligand and IL-2-expressing tumor cells vaccine [NCT00458679]DC-vaccine006 [NCT01334047]Dendritic cell based therapy targeting CSCs in glioblastoma [NCT00846456]Peptides [7]MicroRNA-21 [8]MicroRNA-34a [9]
Small Molecule Therapeutics:Reparixin [NCT01861054]MK-0752 [NCT00645333]GDC-0449 (Vismodegib) [10]IPI-926 [NCT01255800]RO4929097 [11]VS-5584 [12]
Other Therapeutics and their Combination against CSC: Metformin, the drug that is normally used to treat people with diabetes [NCT01440127]Gemcitabine plus Paclitaxel and novel GDC-0449 [NCT01088815]Paclitaxel plus hyaluronic acid [13]Gemcitabine plus novel CHK1 inhibitor (PF-00477736) [14]Salinomycin [15]All-trans retinoic acids stealth liposomes [16]Stealth liposomal Daunorubicin plus Tamoxifen [17]Polymeric nanoparticle formulation of Curcumin (Curcumin, a polyphenolic compound derived fromthe popular Indian spice turmeric) [18]Amide-functionalized multiwalled carbon nanotubes for eradication of triple-negative breast CSCs [19]
* Listed therapeutics with anti-CSC properties are examples of the literature findings and not a complete list. ** ClinicalTrials.gov is a registry and results database ofpublicly and privately supported clinical studies of human participants conducted around the world ClinicalTrials.gov records are linked, via NCT number, to publications.
Table 1. Anti-CSC therapeutics and their combinations, dosage forms and delivery systems in preclinical and clinical studies (7-20,125, 126).

159
Markers Source Animal model Drugs Reference
* Listed references are examples of the literature findings and not a complete list.
Melanoma chemoresistancemediator (ABCB5). Markerexpression by ABCB5+:Nestin, TIE1, CD144, CD31,and BMPR1A.
CD133 does not mark tumor-propagating cells (TPC) inPtc+/- tumors. TPC in Ptc+/-medulloblastoma is containedwithin the GNP-like Math1-GFP+ population andexpresses CD15.
Pancreatic CSCs isolated fromKrasG12D mice express highlevels of stem cell markers(CD133, CD44, CD24 andESA) and transcription factors(Nanog and Oct-4).
CD44high, CD24high,EpCAMhigh
Unsegregated, ABCB5+, orABCB5- clinical patient-derivedmelanoma cells, or ABCB5+ orABCB5- cells isolated fromprimary ABCB5+ patient-derivedxenografts.
Human medulloblastoma tissuesamples.
Pancreatic CSCs isolated fromKrasG12D mice.
Primary colorectal tumor-initiating cells (TICs) from one40 year-old male colorectalcancer patient (stage 4). Colontumor xenografts derived fromhuman CRC line HT-29 cells inNOD/SCID mice.
Tumorigenicity studies:melanoma cells were injecteds.c. into NOD/SCID mice.Malignant-melanoma-initiatingcells targeting experiments:melanoma cells werexenografted s.c. into Balb/cnude mice.
Tumor cells were isolated fromPtc+/- mice and immediatelystereotaxically implanted intothe cerebellum of SCID-beigehosts.
The KrasG12D mice developspontaneous tumors in thepancreas, and it truly resemblesthe growth of human pancreaticcancers.
Cells were injected s.c. intoNOD/SCID mice. HumanPBMCs isolated from freshwhole blood of a healthy donorwere mixed with TICs andmixture was s.c. injected intoNOD/SCID mouse.
Animals. wereinjected i.p. with anti-ABCB5 monoclonalantibody.
-
Resveratrol
EpCAM/CD3-bispecific antibodycalled MT110.
[80]
[69]
[116]
[20]
Table 2A. Animal models of cancer and CSC markers in preclinical CSC research (16, 17, 20, 21, 69, 73, 80, 86, 87, 89, 103-105,116, 117).
Markers Source Animal model Drugs Reference
* Listed references are examples of the literature findings and not a complete list.
Breast cancer stem cells wereidentified with theCD44+/CD24 phenotype andcharacterized with properties:resistant to cytotoxic agent,stronger capability ofproliferation, and strongercapability of differentiation.
Breast cancer stem cells wereidentified with theCD44+/CD24 .
CD34+
ALDH activity:ALDEFLUOR assay andseparation of the ALDH-positive population.
Human breast cancer cell lines:MCF-7 and MDA-MB-231 cells.
Human breast cancer MCF-7 cellline.
Human fibrosarcoma HT1080cell line.
Human breast cancer cell lines:HCC1954, MDA-MB-453, andSUM159 cells.
The cancer relapse model wassuccessfully established byxenografting breast cancer stemcells into NOD/SCID mice.
Cancer cells were injected s.c.into nude mice.
Human tumor xenograftscontaining a human vascularbed in nude mice by s.c. co-implantation of matrigel-embedded human endothelialcells, human mesenchymalstem cells as a source of muralcells and HT1080 humanfibrosarcoma cells.
Cancer cells were implanted inhumanized cleared fat pads ofNOD/SCID mice. Sorted cellswere injected in the heart leftventricle for induction ofmetastasis.
All-trans retinoic acidstealth liposomes.
Stealth liposomaldaunorubicin plustamoxifen.
-
-
[16]
[17]
[89]
[87]

160
Markers Source Animal model Drugs Reference
* Listed references are examples of the literature findings and not a complete list.
CD44+CD24+ESA+
CD133+
A2B5, c-kit, CD44, CD49B,CD49D, CD49f, CD54,CD133, CD166, E-cadherin,HNK-1, L1CAM, MCAM, N-cadherin, and p75.
Sca1 + cells from Kras;p53-flox tumors are lung tumor-propagating cells.
Human pancreaticadenocarcinoma tissue samples.
Human glioma tissue samples.Tumor specimen used (T4121)was a recurrent glioblastomamultiforme (GBM) diagnosed ina 26 year old male.
Human melanoma tissuesamples.
Primary adenocarcinomas weredissected from the lungs of Krasmice, dissociated into single cellsuspensions and transplantedintratracheally (IT) into recipientmice. Secondary tumors formedin recipient mice four to eightmonths after IT transplant cells.
Sorted cells and suspended inRPMI/Matrigel mixturefollowed by injection s.c. intoNOD/SCID mice. In separateexperiments, a medianlaparotomy was done, andsorted cells were injected intothe tail of the pancreas.
Cancer cells were transientlypassaged as xenografts in nudemice. Labeled cancer stem cellsand non-stem tumor cells (fromT4121) were mixed at a10%:90% ratio and transplantedinto the cortex of a nude mouse.
Sorted cancer cells wereinjected s.c. into NOD/SCIDand NOD/SCID IL2R null mice.
Lox-Stop-Lox-KrasG12D andLox-Stop-Lox-KrasG12D;p53fl/fl
mice were anesthetized and IVcatheter was inserted into thetrachea. A 50µL cell suspensionwas pipetted into the catheterand the mouse inhaled the cellsuspension.
-
-
-
-
[73]
[103]
[104]
[105]
Table 2B. Animal models of cancer and CSC markers in preclinical CSC research (16, 17, 20, 21, 69, 73, 80, 86, 87, 89, 103-105,116, 117).
Markers Source Animal model Drugs Reference
* Listed references are examples of the literature findings and not a complete list.
CD44 +
GANT-61 inhibited cancerstem cell tumor growth whichwas associated with up-regulation of DR4 and DR5expression, and suppression ofGli1, Gli2, Bcl-2, CCND2 andZeb1 expression.
For the in vitro repopulationstudy, Hoechst 33342/PI–stained cells were sorted intoPI–/live, SP, and non-SPgroups.
Human tongue squamous cellcarcinoma CAL 27 cell line.
Human pancreatic tumor tissuesamples.
Murine mammary carcinoma4T1 cell line and murineneuroblastoma NXS2 cell line.
Tumor cells were s.c. implantedinto nude mice
Tumor cells were s.c. implantedin humanized NOD/SCID/IL2Rgamma(null) mice. Sorted cellswere injected i.v for inductionof metastasis.
Hoechst 33342/PI–stained cellswere sorted into PI–/live, SP,and non-SP groups, and 4T1cells were injectedorthotopically into themammary fat pad of BALB/cmice. Sorted PI–/live NXS2 SPand non-SP cells were injectedi.v. into the tail vein of A/Jmice.
RO5429083 is a novelfunctional monoclonalantibody, that targetsa glycosylated,conformationdependent epitope ofCD44.
GANT-61 - Glitranscription factorinhibitor) regulatesstem cellcharacteristics andtumor growth.
4T1 and NXS2 SPcells exhibitedincreased resistance tochemotherapy, and4T1 SP cells alsoshowed an increasedability to effluxDoxorubicin.
[21]
[117]
[86]

from the first or second group or well-known drugs at noveldosage forms and drug delivery systems such as polymericmicelles, liposomes, nanoparticle drug carriers etc. Because ofthe diversity of drugs, their possible combinations, dosage formsand delivery systems in the third group, it is difficult to makegeneralizations about them. Obviously, the third group mayinclude some common characteristics of the first and secondgroup. However, compounds of the third group may differ intheir biodistribution, toxicity and efficacy. Examples of differenttypes of drugs, which represent all three groups, can be found inTable 1 and Table 2.
Drug delivery targeting cancer stem cells
It is well-known that the accumulation of macromoleculardrugs within a tumors is predominantly a result of ”leaky”microvasculature and impaired lymphatic support, known as theenhanced permeability and retention (EPR) effect (32, 33). Thisabnormality allows various types of anti-cancer drugs, alone orin association with polymeric delivery systems such asnanoparticles, to exhibit selectivity of action (34). In thiscontext, we have previously reported that micelles preparedfrom conjugates of polyethylene glycol (PEG) and diacyllipids,such as phosphatidylethanolamine (PE) can be used for anefficient solubilization of poorly soluble substances and providesaqueous stability to the micelles (35-37). Small size of PEG-PE-micelles facilitates their “passive” targeting into tumors via theEPR effect. In contrast, active targeting of drugs can be achievedusing various specific ligands attached to nanoparticle surfaces(33, 35-38). Therefore, certain drug delivery platforms fortargeting CSCs, such as polymeric nanoparticle formulation ofcurcumin (18), triblock polymeric micelles with doxorubicin(39), lipid nanocapsules functionalized with a monoclonalantibody (40), all-trans retinoic acid stealth liposomes (16),poly(benzylglutamate)-hyaluronan polymerosomes withdoxorubicin (41), paclitaxel-hyaluronan bioconjugate (42) makeit one of the promising approaches in anti-CSC therapy. Moreexamples of strategies for passive or active CSC targeting can befound elsewhere (43).
In summary, modern drug delivery technologies which havebeen designed to dose drugs continually for prolonged timeperiods and in a controlled fashion have a high potential forenhancing accumulation of drug in tumors. However, even afterthese drugs reach therapeutic levels in tumors, it may not beenough for them to act specifically on one particular targetedtype of cell - for example, to selectively seek and destroy CSCs.While current efforts are focused on passive or active targetingof tumors, where many drugs have extracellular and/orintracellular compartments as their site of action, much less isknown about efficient and selective therapies that target CSCspreferentially.
GENERAL PRINCIPLES OF ANTI-CANCER STEM CELLDRUG DEVELOPMENT
Traditionally, the preclinical drug development processmeets several critical experimental requirements. These include:the availability of prospective drug candidates in large enoughquantities for comprehensive in vitro analysis, and the ability toidentify potential drug targets (e.g. these targets can be outsidethe cell, inside the cell, or on the cell surface) that arespecifically involved in a particular metabolic or signalingpathway. Another requirement is the accessibility of suitableclinically relevant animal models for in vivo studies. The animalmodels must have a histotype for the evaluation of modes ofaction, quantitative pharmacology studies (e.g. pharma- and
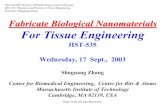
toxicokinetics), toxicity, and efficacy studies, and accessibilityof suitable biomarkers that can serve as marker(s) of efficacy.One of the most distinctive characteristics of in vivo efficacystudies for the identification of potent anti-CSC drugs is thatthey usually consist of two steps. The first step in this approachis to administer drugs into the tumor-bearing animals for theinhibition of malignant ascites production or inhibition of solidtumor growth and/or metastasis. Researchers then use othertypes of in vivo assays to confirm the stem cell behaviors of self-renewal and their long-term repopulating ability. The diagram inFig. 1 shows a typical in vivo study for the identification of ahighly selective anti-CSC drug.
In preclinical studies, the anti-tumor effectiveness of theapplied drugs can be evaluated by direct caliper measurement oftumor size, calculation of visible surface metastasis, or Kaplan-Meier survival analysis of animals harboring varioushematological and solid tumors. Alternatively, tumor growth andmetastasis can be visualized in live animals using X-ray,ultrasound, CT, SPECT, PET, MRI, and other in vivo imagingmodalities to detect green fluorescent protein- and luciferase-expressing tumor models. However, in some cases an in vivoanti-cancer therapy may be considered efficacious based on thesignificant reduction of primary tumor size and metastasis, butthere is still a high risk that after treatment the cancer couldrelapse due to the survival of sufficient number of CSCs. Inaddition, many traditional cytostatic or cytotoxic and even novelmolecularly-targeted drugs may be highly toxic to healthy cells,including normal stem cells. Therefore, new anti-CSCs drugs arestill urgently needed.
Tumor microenvironment and cancer stem cell markers inpreclinical cancer stem cell research
It has been shown that solid tumors are a complex mix ofphenotypically and functionally heterogeneous neoplastic cellsincluding cancer cells, CSCs, and various normal stromal cellsand bioactive molecules (e.g. cytokines and chemokines) thatsurround tumor cells, also referred to as the tumormicroenvironment (44). Interestingly, normal stem cells andCSC share common features that include activation of the samemolecular pathways that regulate their stemness and their abilityto self-renew. For example, many cell surface markers such asEpCAM, CD24, CD44, and CD133 that currently are associatedwith CSCs were also found in normal stem cells in the tissue-of-origin (45-48). Due to the similarities between CSCs and normalstem cells, the majority of current therapies that target CSCs arenot selective exclusively to CSC, they may also eliminatenormal stem cells. On the other hand, one of the differencesbetween normal stem cells and CSC is their degree ofdependence on the stem cell niche, a specializedmicroenvironment in which stem cells reside (49). Thus, themicroenvironment seems to be of crucial importance for primarytumor growth as well as metastasis formation (50).
The interactions between cellular components of the stromaand the factors that they express during cancer initiation andprogression are critically important. For example, the chemokinestroma-derived factor (SDF-1/CXCL12) is of particular interestbecause the binding of this ligand to chemokine receptorCXCR4 in CSCs is implicated in tumor proliferation, survival,and metastasis (51). Indeed, CXCL12 contributes to tumorimmunosuppression through recruiting of specific immune cellpopulations, enhances tumor neovascularization, and mediatestumor cell migration, adhesion, and invasion. In fact, variouscomponents of the tumor microenvironment including cancer-associated fibroblasts, endothelial cells, pericytes, cancer cells,and immune inflammatory cells have a direct influence on CSCproperties (2, 44, 52). On the other hand, using the same
161

chemokine receptors to get into the bone marrow, CSCs may usethe normal hematopoietic stem cell microenvironment or“niche” which houses hematopoietic stem cells in the bonemarrow to their advantage (53). It is therefore obvious that theunderstanding of the specific diversity of cell morphology andmolecular profiling reveals the similarities and differencesbetween CSCs and other cell types in the tumor stroma, andunderstanding their mechanisms of interaction will provide newpotential targets for specific anti-CSC therapeutic intervention.
One way to enhance the efficacy and reduce the unwantedeffects of anti-cancer drugs is to selectively target CSCs. In orderto do this it is necessary to distinguish CSCs from other stromalcomponents of the tumor. Distinct and specific markers,including molecules that are on the cell surface, cell signalingmolecules (5, 6, 54-60) and differential expression of miRNAsin CSCs (61) can be used for this purpose. Although theprognostic value of CSC-associated markers is still under activeinvestigation, many researchers believe that specific geneexpression by CSCs may be able to predict clinical outcomes.More details about the current state of CSC biomarkers, CSCdetection in patients, and discussion about future perspectivesfor the development of prognostic and predictive CSCbiomarkers for routine clinical use can be found elsewhere (3,54-56, 62-65).
It is important to emphasize that CSCs can also bedistinguished from the bulk-tumor population by othercharacteristics such as high expression of cytoprotectiveenzymes, for instance, aldehyde dehydrogenase 1 (ALDH1)(66), ATP-binding cassette (ABC) transport proteins (4) orthymosin β4 (Tβ4), a small acidic actin binding peptide (67).
As mentioned earlier, the sorted subsets of CSCs can be usedin both, in vitro clonogenic and in vivo tumorigenic assays tocharacterize CSCs. For example, in one in vivo tumorigenicassay where CSCs were sorted by CD133 expression it wasfound that 1 in 262 CD133+ cells had colon tumor formationcapacity in immunodeficient mice, while only 1 in 57,000unsorted tumor cells could form a tumor (68). Other researchershave identified CSCs in the most commonly used animal modelof medulloblastoma (MB), the Patched mutant Ptc+/– mice. CSCswere propagated not by CD133+ cells but by cells expressingmarkers Math1+ and CD15+ (CD15+ -known as SSEA-1 or LeX).As a result, MB tumors from Ptc+/– mice were propagated byorthotopic transplantation of 300,000 unsorted and 300,000CD15+ Ptc+/– MB sorted cells, and not by 300,000 CD15- cells(69). In these experiments the most common method used toidentify CSC population is fluorescence-activated cell sorting(FACS). An overview of phenotypes of CSC markers in variouscancer types (animal models) is provided in Table 2.
162
Fig. 1. Diagram of recommended steps in the developmental strategy for anti-CSC therapeutics in solid tumor models: (1) the selectionof clinically relevant animal tumor models (e.g. animals, tumor material for inoculation into animals, implantation site, methods oftumor detection, maximum tumor size, endpoints for euthanasia etc.), (2) the administration of anti-CSC compounds to animals (e.g.dose, formulation, frequency, duration etc.), (3) analysis of tumor samples, (4) In vivo repopulation to assess CSCs properties, (5)comparative analysis of tumor samples.CSC: cancer stem cells; RT-PCR: reverse transcriptase - polymerase chain reaction; IHC: immunohistochemistry; MTT: (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide] assay.

In recent decades, numerous therapeutic strategies foreradicating CSCs have been proposed. Some of the mostpromising approaches target cell surface marker(s) (e.g. CD33,CD44, CD90, CD133, CD166 and EpCAM etc.) (3, 55) and cellsignal cascade(s) (e.g. Notch, Hedgehog, Wnt, NF-κB etc.) (4,55). While other strategies are based on the targeting of specificmicroenvironments in solid tumors that form a permissive“niche” for the CSC (e.g. CXCL12/CXCR4, VEGF/VEGFR,weakly acid pH etc.) (3, 51, 55), metabolic activity of CSCs (e.g.ALDH1 etc.) (55, 66) or drug efflux transporters that are the“guardians” of the stem cell population (e.g. ATP-bindingcassette (ABC) drug transporters)) (55, 70). Also, DNA repairmechanisms (e.g. CSCs use a network of activated DNA repairmechanisms to remove different types of DNA damage) (52, 71),and detoxifying enzymes that are responsible for the chemo-andradiation therapy resistance of CSCs can be considered (55, 56).
General characteristic of laboratory rodents and tumormaterial for the induction of tumor growth in rats and mice
Traditionally, there are three sources of tumor material usedfor the induction of tumor growth in laboratory rodents. Tomodel and reproduce the variability of response of specifictumor types, researchers use stable, immortalized cancer celllines, of which there are currently more than 1000 commerciallyavailable (70). The biggest disadvantage of using immortalizedcancer cell lines is that they do not represent all of the biologicaland genomic properties of primary tumors (71, 72). In somestudies, researchers may also use cancer cells isolated fromprimary tumors grown in vivo or primary patient tissue samples,which can be inoculated as single-cell suspensions or surgicallyresected human tumor fragment(s). Heterotransplantation ofhuman tumor material into immunodeficient rodents is alsoknown as human tumor xenografts. Notably, rodent xenograftmodels are critical for certain types of in vivo studies because ofthe difficulty in routinely obtaining primary human tumors fromparticular organs, especially the pancreas (73). Rapidengraftment of human tumor material from patient primarysolid-tumor tissue at low passage is known as a patient-derivedtumor xenograft (PDX). Currently, the inbred/outbred nudeathymic mice that are T-cell deficient and suffer from a lack ofcell-mediated immunity (74) and B-cell-deficient and T-cell-deficient severe combined immunodeficient (SCID) mice (74,75) are widely used as xenograft hosts. In addition to the firsttwo strains, human tumor xenografts can be successfullypropagated in non-obese diabetic/severe combinedimmunodeficient (NOD/SCID) mice that are B-cell-deficientand T-cell-deficient plus they are defective in DC-cell activity,and macrophages and natural killer (NK) cell activity. Also,these mice do not have a complement hemolytic activity due tothe lack of the complement protein C5 (76). In contrast, theBUB/BnJ strain of mice is reported to have high serumcomplement hemolytic activity (77). It has been shown thatNOD/SCID mice are an excellent model system to study theengraftment and mobilization of human peripheral blood stemcells (78) and appear to be more receptive for growingexperimental leukemias and solid tumors (79, 80). Notably, thenude mice have intact innate immunity and they do not have adefect in T-cell precursors. Therefore, the chances of asuccessful transplantation of primary tumor cell into nude micein some cases can be as low as <5% (81). In certain SCID micehave been reports of “leakiness”, meaning they have the abilityto generate a small number of functional B and T cell clones(82). However, some adult SCID mice, specifically in theBALB/cBy and C57BL/6J genetic backgrounds have a highcapacity for developing these clones and on the low end is theC3H/HeJ background (74). This should be taken into account
when choosing immunodeficient animals for experiments. Sometypes of human tumor cells grow quite well in the basic nude andSCID mice, while others grow unacceptably slow with poortumor “take”. For better engraftment of peripheral-bloodmononuclear cells (PBMC) as well as human cancer cell lines,cancer cells isolated from primary tumors grown in vivo orpatient-derived tissue, NSG mice (NOD-scid IL2Rgammanull)that are lacking mature T cells, B cells, NK cells, complement,and are defective in DC-cells and macrophages, and are deficientin cytokine signaling, can be successfully used for long or short-term in vivo experiments (83). Athymic nude rat that are T-celldeficient and show depleted cell populations in thymus-dependent areas of peripheral lymphoid organs are useful in thestudy of graft rejection in immunocompromised hosts since theycan accept major histocompatibility complex mismatched organallografts or xenografts for several months. Also, it has beenshown that some human tumor cell lines grow well in such rats(84). It is believed that various immunodeficient strains havelymphoid tissue alterations, such as partial or total depletion ofthe thymus, spleen, and lymph nodes and that may hide potentialtoxic effects of applied anti-CSC drugs. This factor should betaken into account in designing in vivo experiments. Any newtherapeutics, including anti-CSC drugs need to be tested in bothnormal and immunocompromised preclinical animal models.Therefore, the strains of mice and rats that researchers finallychoose for in vivo studies will depend on the immunologic statusand other characteristics, for instance, the type of therapeutics,duration of experiment, and tumor microenvironment that bestfits with the aim of the study.
Examples of transplantable animal tumors in cancer stem cellresearch
For many years, laboratory animals have played a criticaland necessary role in the anti-cancer drug development process.Despite that, however, no animal models can be referred to as“ideal model” that can fully recapitulate the genetic, epigenetic,and immune system complexity found in human cancer patients.In preclinical CSC research, there are now a variety oftransplantable animal tumors which can be placedheterotopically (e.g. subcutaneous (s.c.), intraperitoneal (i.p.),and intramuscular (i.m.) administration of tumor cells intoanimals)) or orthotopically (i.e. into the organ of origin) insyngeneic (i.e. same species, genetically identical), allogeneic(i.e. same species, genetically different) or xenogeneic (i.e.different species and genetics)) host systems. Table 2 providesoverviews of different host species, methods of inoculation oftumor cells, types of cancer for investigation and types of tumorsthat express proteins that can be important for CSC detection.More details about the types of transplantable tumor models thatapplicable for CSC research can be found in the reviewpublished by Talmadge (85). Moreover, for in vivo tumorigenicassays with sorted CSC populations, the model that belongs tothe heterotopic group is particularly useful. By the intravenous(i.v.) or intracardiac (i.c.) administration of tumor cells,experimental metastasis in lungs and/or liver (by i.v.) or in bone,muscle, lung, and soft tissue (by i.c.) can be induced and studiedor analyzed (15, 86, 87).
By leveraging lessons learned through testing andimplementation of various models, the primary goal of thisreview is to provide practical solutions regarding thedevelopment of rational models for CSC-research, and highlightthe advantages and disadvantages of each approach. Forexample, the s.c. inoculation of single-cell suspension(s) ortumor fragment(s) is still one of the more common techniquesfor the induction of tumor growth in heterotopic models forefficacy studies of novel anti-CSC candidates. The benefits of
163

s.c. tumors are the simplicity of tumor inoculation,reproducibility and repeatability of experiments, andaccessibility for direct tumor size measurements. The large s.c.space in rodents allows for continuous growth of the tumor,which can measure from approximately 50 mm3 up to 1500 mm3.This is beneficial for CSC research, especially when a largeamount of tumor mass is needed for the isolation and molecularcharacterization of CSCs.
One drawback of the s.c. models is that it may not provideaccurate information on the specific microenvironment (or“niche”) to support growth of CSC and may not represent the“true side” of human tumors. One possibility to overcome thisproblem is to s.c. administer the tumor cells suspended in thebasement membrane matrix proteins CultrexBME or Matrigel(88). Tumor cells can also be co-injected with human fibroblasts,matrigel-embedded human endothelial cells, humanmesenchymal stem cells, or other types of stromal cells that insome way mimic in vivo extracellular microenvironments. Thiswill allow CSC to achieve sustainable tumor development, andenable the tumor to grow more rapidly (89). Table 2 showsseveral examples of s.c. models that are applicable in CSC-research. In addition, s.c. implantation of cells isolated fromfreshly dissociated human tumor tissues or small piece(s) ofsurgically resected human tumors into immunocompromisedanimals is often an initial step in the establishment of patient-derived xenografts (PDXs). The experimental benefit of s.c.PDXs is that they may maintain many aspects of the humanmicroenvironment for several weeks, which offers a moreaccurate simulation of cancer cell behavior in patients.Moreover, orthotopic PDXs with organ-specificmicroenvironments for CSC might serve as an excellent sourcefor the identification and validation of CSC-related markers withhighly predictive potential for therapy. Unfortunately, it has beenshown that after 2–3 passages the human microenvironment insuch tumors can be substituted with elements of murine tumorstroma (90, 91). In the context of human tumor xenograftscontaining co-implanted matrigel-embedded human endothelialcells, endothelial cells have also been rapidly substituted by theirmurine counterparts, and by day 16 post-implantation humanCD34-positive cells were almost undetectable in intratumoralvessels (89).
As noted above, s.c. models are a valuable tool, but they arelimited by the lack of blood supply and lymphatic drainage thatare so vastly different than those of the orthotopic site (92).Thus, s.c models cannot truly reproduce the patterns ofdevelopment of distant metastasis often seen in cancer patients,for example, in sinonasal cancers (93). Importantly, theorthotopic model has all of the elements of themicroenvironment that help maintain the CSC phenotype in asubset of cells, essential not only for primary tumor growth, butalso in mediating tissue invasion and metastasis (94). It ispossible that different organs that consist of epithelial tissue,such as the liver, kidneys, lungs, pancreas, and colon, harbordifferent microenvironments with distinct endothelial or stromalcell types and extracellular matrix components that promote orinhibit tumor growth (95). The authors suggested that the tumorinitiation and maintenance at the primary site of disease ormetastatic dissemination would depend on the interaction ofCSCs with a particular niche. Recently, an orthotopic metastaticmurine model for head and neck squamous cell carcinoma(HNSCC) using GFP-labeled cells and FACS for generation of apure metastatic cell line has been developed (96). Moreover, thismodel also allowed the authors to identify a number of genesthat may have an important role in metastasis in HNSCC,possibly through the induction of the epithelial-to-mesenchymaltransition and formation of CSCs. Other authors suggested thatCD44-positive CSC-like cells have enhanced ability for
metastasis. Some researchers previously described thedevelopment of an orthotopic mouse model, in which anorthotopic implantation of CD44-positive subpopulation oftumor cells into the mammary gland (97) or into the cecal wall(98) of immunocompromised animals yielded local tumors, aswell as distant metastasis in lungs or liver. Research also showsthat in addition to genetic and epigenetic complexity anddiversity, tumor cell plasticity may contribute to phenotypic andfunctional heterogeneity (2, 44, 52, 54, 64, 65, 99). Interestingly,CSC model of heterogeneity may apply more readily to early-stage rather than to advanced tumors due to the dominant clonesthat probably drive tumor progression (3). Also, advancedtumors often have some evidence of necrosis and bleeding thatmay have a significant impact on the quality of tumor samplesfor analysis.
The superiority of orthotopic xenograft models is due to thesite-specific microenvironment in the host organ that closelymimics clinical pathology. However, orthotopic tumors inanimal experiments grow much faster than in cancer patients andhence can be, at least hypothetically, more sensitive to targetedanti-CSC drugs. Therefore, preclinical in vivo data may notalways translate well to the clinic. More information describingthe translation of novel anticancer drugs into the clinic andhighlighting the challenges, limitations and where there is a needfor improvements can be found in (100-102).
As mentioned earlier, a CSC population may be confirmedby preferential tumor formation from cells directly isolated fromprimary tumors in drug-treated and untreated (control) animals.This requires the sacrifice of the animal to assess the treatment’seffect on both CSCs and other types of cancer cell populations.Also, site-specific tumor growth in orthotopic models limits thereal time evaluation of the efficacy of novel anti-CSC drugcandidates in living rodents. Alternatively, to evaluate thepotential of CSCs in direct comparison to non-CSCs in the samemicroenvironment, researchers have recently developedtechniques to use different fluorescent proteins for labeling oftumor cells to monitor their behavior over time using intravitalmicroscopy (103).
The challenge of designing in vivo orthotopic modelexperiments is to develop sustainable growth of transplantedtumors. The initial engraftment rate with implantation of tumormaterial in immunocompromised mice has been shown to be aslow as <5% (81), 20% (66) or 25% (73). In fact, many CSCresults are derived from xenotransplantation experiments inwhich human cancer cells are grown in immunodeficientanimals with different genetic backgrounds. Therefore, toincrease the percentage of tumor “take,” the rational selection ofthe appropriate strains of rodents is necessary for success. Forexample, a group of authors showed that using the PDXmelanoma model significantly increased the detectablefrequency of CSCs through some modifications inxenotransplantation assays. In their study, the CSCs were morelikely to be detected in more highly immunocompromised micesuch as NOD/SCID/IL2Rgammanull mice (104). Other in vivostudies have shown that the genotype of tumor samples must betaken into account in the targeting of CSCs. For example, usingorthotopic (intratracheal transplant) models of the most commonform of human lung cancer, researchers found that lungadenocarcinomas of differing genotypes have CSCs with distinctmarkers that therefore require different strategies for isolation ofCSCs from each model (105).
Other things to consider when using orthotopic models forCSC research include site-specific variation in response totherapy and accurate analysis of tumor growth and metastasis.Also, these models are labor-intensive and time-consuming, andsome procedures require specialized training. Some animalmodels, especially PDXs, can cost tens of thousands of dollars
164

per study, and therefore are not widely used in routine in vivolaboratory practices. Furthermore, the vast majority of internalorthotopic models provide only a small amount of tumor massfor analysis, which may be critical for the isolation of these rarepopulations of CSCs. The only exceptions to this are certainbreast cancer models transplanted into a mammary gland fat pad,whose tumors are relatively superficial and accessible for routinetumor-size measurements, and, more importantly, are availablefor the collection of large amounts of tumor tissue. More detailsabout models’ strengths, weaknesses, applicability, andtranslation to human cancer in the context of anti-cancer drugdiscovery can be found here (100, 106, 107).
It has long been recognized that the host immune status andthe tumor microenvironment play a crucial role during tumordevelopment in both animals and humans. Sinceimmunocompromised rodents fail to functionally replicate theimmune system characteristics that are present in humans, it canbe assumed that such conditions may permit growth of tumors inrodents that would never occur in human patients. In addition,for some biologics such as humanized mAbs, the host immunesystem is needed to fully realize their anti-tumor potential,especially when the intact host immune system is required forthe antibody-dependent cellular cytotoxicity (ADCC). To furtherexplore the role of ADCC in anti-HER2/neu antibody therapy,researchers used Balb/c mice inoculated s.c. with neu-expressingTUBO breast carcinoma cells which are cells derived fromBALB-neuT transgenic mice) (108). These researchers haveclearly demonstrated that an activation of innate immunity andT-cells that was initiated by antibody treatment is necessary forsignificant tumor suppression. Furthermore, the possibility oftargeting CSCs in DC cell-based vaccination, using anorthotopic (intracranial) 9L tumor in adult F344 Fisher rats hasbeen explored (109). DC-based vaccination using CSC antigenselicited antigen-specific T-cell responses against CSCs. Becauseof the immune response required for the host (rodents) to realizethe maximum therapeutic potential of particular types of drugs incancer treatment, numerous experimental approaches have beendeveloped and studied in preclinical practice. For example, thetransfer of a functional human immune system, for instance,human PBMC (via i.v. or intrasplenic injections) to mice withsevere combined immunodeficiency is a useful way to make“humanized mice” (110). Notably, humanized mice can beengineered by the engraftment of components of the humanimmune system not only from blood (110) or human bonemarrow (111), but also by engraftment of primary human fetallymph nodes (112). Alternatively, human fetal liver and thymusfragments can be implanted in some cases, under the renalcapsule in adult SCID mice (113-115). Moreover, i.padministration of human haematopoietic stem cells into newbornor adult immunodeficient recipients usually resulted in very lowengraftment (114).
One group of researchers have reported that humanized anti-CD44 antibody RO5429083 can effectively target the CSCpopulation in CAL-27 human xenografts in humanized micewhile boosting the number of NK cells, and thus may synergizewith drugs that work via ADCC such as Cetuximab (116). Inanother study, humanized NOD/SCID/IL2Rgammanull mice wereused to examine the effects of GANT-61 (Gli transcription factorinhibitor) on CSC’s tumor growth (117). Humanized mice servenot only for tumor grafting and testing of various anti-CSCdrugs, but also allow researchers to study and manipulate theimmune response in advanced cancer therapy (118). To explorethe efficiency of anti-CSC drug treatments on tumor growth,researchers also used animal models in which tumor material orprimary human tissue were transplanted orthotopically into thehumanized cleared mammary fat pad of NOD/SCID mice,without cultivation in vitro (66). The humanized orthotopic
mammary fat pad mouse model was first developed byKuperwasser et al. (119) in which both the stromal and epithelialcomponents of the reconstructed mammary gland are of humanorigin. Injection of immortalized human breast fibroblastsresulted in creation of a ‘humanized’ stroma that consist about15% human fibroblasts after 8 weeks. This type of model iscloser to the human tumor and more suitable for stem cell studiescompared with s.c. injection. In addition, Stewart et al., (120)found that mammary fat pad xenografts recapitulated inter-andintratumor heterogeneity of primary serous ovarian cancer(CD133+), as assessed by histology, surface immunophenotype,and expression of p53, WT1, and CK7. Alternatively, cancer-initiating cells can be injected orthotopically either under therenal capsule, ovarian bursa, or peritoneum of NOD/SCID orNSG mice (68, 120). Interestingly, some authors suggested thatthe mammary fat pad might provide a microenvironment moresimilar to that of human serous ovarian cancer than “morerelevant” sites such as peritoneal cavity (120).
In contrast, researchers have proposed that the CSC conceptcan be applied to syngenic tumor models that would providealternative approaches for the in-depth characterization of CSCsin an immunocompetent tumor microenvironment, and for theunderstanding of complex behaviors in the interaction betweenanti-CSC drugs and the host’s immune system (86). In addition,syngenic animal models have the advantage of being widelyavailable for preclinical studies and allowing researchers toavoid legal and ethical issues related to the sourcing of humantissue samples.
Targeted gene disruption in rodents is a powerful tool forgenerating an entirely new type of models for the development ofnovel anti-cancer drugs. This technology opens up the possibilityof in vivo CSC research utilizing genetically engineered mousemodels (GEMM) that include transgenic models, i.e. introductionof gene sequences into the mouse genome, or gene knock-out/knock-in models in which endogenous mouse genes aredeleted and/or modified (69, 121, 122). These GEMM modelswould most likely be able to more accurately mimic the cancer-related disparities in humans (123). Today, GEMMs arebecoming an important tool in the preclinical development ofanti-CSC drugs. Recent research using GEMMs include theexamination of the molecular mechanisms by which resveratrolinhibits stem cell characteristics of pancreatic CSCs derived fromhuman primary tumors in KrasG12D transgenic mice (116),identification of cells initiating human melanomas usingNOD/SCID/IL2Rgammanull chain knock-out mice (80), orevaluation of prominin-1/CD133 as a biomarker for stem cellsand early progenitors in mouse small intestine, using transgenicProm1/CD133 knock-in mice (124).
CONCLUSION
Preclinical animal research is an excellent instrument for thebetter understanding of biology, genetics, immunology,pharmacology, and other Life Science disciplines in novelinvestigative situations. In the context of in vivo cancer stem cellresearch, the robust understanding of rodent physiology,possible genetic variability in rodents strains and the effect thismay have on the observed phenotype differences, types andmethods of induction of experimental tumors as well asbehavioral and molecular biomarkers in translational animalmodels are critically important for the development of rational invivo models for anti-CSC drug testing. In addition to this, adeeper understanding of pharmacological properties of varioustypes of anti-cancer drugs, and modern technologies which canincrease the selectivity of drugs for their intended targets mayultimately lead to a greater understanding of the CSC biology
165

and thus, ultimately help improving the development ofpredictive biomarkers and targeted therapeutic strategies for theeradication of CSCs.
Abbreviations: CSC: cancer stem cell; DC: dendritic cells;NK: natural killer cells; PBMC: peripheral blood mononuclearcells; mAbs: monoclonal antibodies; ADCC: antibody-dependent cellular cytotoxicity; GI-tract: gastrointestinal tract;EPR-effect: enhanced permeability and retention effect; ABC:ATP-binding cassette; MB: medulloblastoma; PDX: patient-derived xenograft; GEMM: genetically engineered mousemodels; SCID mice: severe combined immunodeficient mice.
Conflict of interests: None declared.
REFERENCES
1. Lapidot T, Sirard C, Vormoor J, et al. A cell initiating humanacute myeloid leukaemia after transplantation into SCIDmice. Nature 1994; 367: 645-648.
2. Magee JA, Piskounova E, Morrison SJ. Cancer stem cells:impact, heterogeneity, and uncertainty. Cancer Cell 2012;21: 283-296.
3. Visvader JE, Lindeman GJ. Cancer stem cells: current statusand evolving complexities. Cell Stem Cell 2012; 10: 717-728.
4. Diaz A, Leon K. Therapeutic approaches to target cancerstem cells. Cancers (Basel) 2011; 3: 3331-3352.
5. Zhou BB, Zhang H, Damelin M, Geles KG, Grindley JC,Dirks PB. Tumour-initiating cells: challenges andopportunities for anticancer drug discovery. Nat Rev DrugDiscov 2009; 8: 806-823.
6. Naujokat C. Targeting Human Cancer Stem Cells withMonoclonal Antibodies. J Clin Cell Immunol 2012; S5: 007.
7. Perlstein B, Finniss SA, Miller C, et al. TRAIL conjugatedto nanoparticles exhibits increased anti-tumor activities inglioma cells and glioma stem cells in vitro and in vivo. NeuroOncol 2013; 15: 29-40.
8. Zhou L, Yang ZX, Song WJ, et al. MicroRNA-21 regulatesthe migration and invasion of a stem-like population inhepatocellular carcinoma. Int J Oncol 2013; 43: 661-669.
9. Liu C, Kelnar K, Liu B, et al. The microRNA miR-34ainhibits prostate cancer stem cells and metastasis by directlyrepressing CD44. Nat Med 2011; 17: 211-215.
10. Singh BN, Fu J, Srivastava RK, Shankar S. Hedgehogsignaling antagonist GDC-0449 (Vismodegib) inhibitspancreatic cancer stem cell characteristics: molecularmechanisms. PLoS One 2011; 6: e27306.
11. Luistro L, He W, Smith M, et al. Preclinical profile of apotent gamma-secretase inhibitor targeting notch signalingwith in vivo efficacy and pharmacodynamic properties.Cancer Res 2009; 69: 7672-7680.
12. Hart S, Novotny-Diermayr V, Goh KC, et al. VS-5584, anovel and highly selective PI3K/mTOR kinase inhibitor forthe treatment of cancer. Mol Cancer Ther 2013; 12: 151-161.
13. Lee H, Kim JB, Park SY, Kim SS, Kim H. Combinationeffect of paclitaxel and hyaluronic acid on cancer stem-like side population cells. J Biomed Nanotechnol 2013; 9:299-302.
14. Fang DD, Cao J, Jani JP, et al. Combined gemcitabine andCHK1 inhibitor treatment induces apoptosis resistance incancer stem cell-like cells enriched with tumor spheroidsfrom a non-small cell lung cancer cell line. Front Med 2013;7: 462-476.
15. Gupta PB, Onder TT, Jiang G, et al. Identification ofselective inhibitors of cancer stem cells by high-throughputscreening. Cell 2009; 138: 645-659.
16. Li RJ, Ying X, Zhang Y, et al. All-trans retinoic acidstealth liposomes prevent the relapse of breast cancerarising from the cancer stem cells. J Control Release 2011;149: 281-291.
17. Guo J, Zhou J, Ying X, et al. Effects of stealth liposomaldaunorubicin plus tamoxifen on the breast cancer and cancerstem cells. J Pharm Pharm Sci 2010; 13: 136-151.
18. Lim KJ, Bisht S, Bar EE, Maitra A, Eberhart CG. Apolymeric nanoparticle formulation of curcumin inhibitsgrowth, clonogenicity and stem-like fraction in malignantbrain tumors. Cancer Biol Ther 2011; 11: 464-473.
19. Burke AR, Singh RN, Carroll DL, et al. The resistance ofbreast cancer stem cells to conventional hyperthermia andtheir sensitivity to nanoparticle-mediated photothermaltherapy. Biomaterials 2012; 33: 2961-2970.
20. Herrmann I, Baeuerle PA, Friedrich M, et al. Highlyefficient elimination of colorectal tumor-initiating cells byan EpCAM/CD3-bispecific antibody engaging human Tcells. PLoS One 2010; 5: e13474.
21. Perez, A, Neskey DM, Wen J, et al. Targeting CD44 in headand neck squamous cell carcinoma (HNSCC) with a newhumanized antibody RO5429083. Cancer Res 2012; 72(Suppl. 1): abstract 2521. doi: 10.1158/1538-7445.AM2012-2521
22. Korbut E, Ptak-Belowska A, Brzozowski T. Mechanismspromoting physiological cells progression intotumorigenesis. J Physiol Pharmacol 2012; 63: 565-570.
23. Scott AM, Allison JP, Wolchok JD. Monoclonal antibodiesin cancer therapy. Cancer Immun 2012; 12: 14.
24. Burnett JC, Rossi JJ. RNA-based therapeutics: currentprogress and future prospects. Chem Biol 2012; 19: 60-71.
25. Jackson AL. Linsley PS. Recognizing and avoiding siRNAoff-target effects for target identification and therapeuticapplication. Nat Rev Drug Discov 2010; 9: 57-67.
26. Seth S, Johns R, Templin MV. Delivery and biodistributionof siRNA for cancer therapy: challenges and futureprospects. Ther Deliv 2012; 3: 245-261.
27. Zaks TZ, Rosenberg SA. Immunization with a peptideepitope (p369-377) from HER-2/neu leads to peptide-specific cytotoxic T lymphocytes that fail to recognize HER-2/neu+ tumors. Cancer Res 1998; 58: 4902-4908.
28. Sahr RN. The Biologics Price Competition and InnovationAct: Innovation Must Come Before Price Competition 2(Boston College Intellectual Prop. & Tech. Forum 2009).http://bciptf.org/?s=The+biologics+price+competition+and+innovation+act%3A+Innovation+must+come+before+price+competition
29. Materials at http://foundation.aarp.org.30. Kruger FA, Overington JP. Global analysis of small
molecule binding to related protein targets. PLoS ComputBiol 2012; 8: e1002333.
31. Hoelder S, Clarke PA, Workman P. Discovery of smallmolecule cancer drugs: successes, challenges andopportunities. Mol Oncol 2012; 6: 155-176.
32. Matsumura Y, Maeda H. A new concept for macromoleculartherapeutics in cancer chemotherapy: mechanism oftumoritropic accumulation of proteins and the antitumoragent smancs. Cancer Res 1986; 46: 6387-6392.
33. Torchilin V. Tumor delivery of macromolecular drugs basedon the EPR effect. Adv Drug Deliv Rev 2011; 63: 131-135.
34. Steiniger SC, Kreuter J, Khalansky AS, et al. Chemotherapyof glioblastoma in rats using doxorubicin-loadednanoparticles. Int J Cancer 2004; 109: 759-767.
35. Skidan I, Miao B, Thekkedath RV, Dholakia P, Degterev A,Torchilin V. In vitro cytotoxicity of novel pro-apoptoticagent DM-PIT-1 in PEG-PE-based micelles alone and incombination with TRAIL. Drug Deliv 2009; 16: 45-51.
166

36. Skidan I, Dholakia P, Torchilin V. Photodynamic therapy ofexperimental B-16 melanoma in mice with tumor-targeted5,10,15,20-tetraphenylporphin-loaded PEG-PE micelles.J Drug Target 2008; 16: 486-493.
37. Miao B, Skidan I, Yang J, et al. Small molecule inhibition ofphosphatidylinositol-3,4,5-triphosphate (PIP3) binding topleckstrin homology domains. Proc Natl Acad Sci USA2010; 107: 20126-20131.
38. Zamboni WC, Torchilin V, Patri AK, et al. Best practices incancer nanotechnology: perspective from NCInanotechnology alliance. Clin Cancer Res 2012; 18: 3229-3241.
39. Kim TH, Mount CW, Gombotz WR, Pun SH. The deliveryof doxorubicin to 3-D multicellular spheroids and tumors ina murine xenograft model using tumor-penetrating triblockpolymeric micelles. Biomaterials 2010; 31: 7386-7397.
40. Bourseau-Guilmain E, Bejaud J, Griveau A, et al.Development and characterization of immuno-nanocarrierstargeting the cancer stem cell marker AC133. Int J Pharm2012; 423: 93-101.
41. Upadhyay KK, Bhatt AN, Mishra AK, et al. The intracellulardrug delivery and anti tumor activity of doxorubicin loadedpoly(gamma-benzyl L-glutamate)-b-hyaluronanpolymersomes. Biomaterials 2010; 31: 2882-2892.
42. Banzato A, Bobisse S, Rondina M, et al. A paclitaxel-hyaluronan bioconjugate targeting ovarian cancer affords apotent in vivo therapeutic activity. Clin Cancer Res 2008; 14:3598-3606.
43. Vinogradov S, Wei X. Cancer stem cells and drug resistance:the potential of nanomedicine. Nanomedicine (Lond) 2012;7: 597-615.
44. Sounni NE, Noel A. Targeting the tumor microenvironmentfor cancer therapy. Clin Chem 2013; 59: 85-93.
45. Mizrak D, Brittan M, Alison M. CD133: molecule of themoment. J Pathol 2008; 214: 3-9.
46. Gires O, Klein CA, Baeuerle PA. On the abundance of EpCAMon cancer stem cells. Nature Rev Cancer 2009; 9: 143.
47. Williams K, Motiani K, Giridhar PV, Kasper S. CD44integrates signaling in normal stem cell, cancer stem cell and(pre)metastatic niches. Exp Biol Med (Maywood) 2013;238: 324-338. Epub 2013/04/20.
48. Sano A, Kato H, Sakurai S, et al. CD24 expression is a novelprognostic factor in esophageal squamous cell carcinoma.Ann Surg Oncol 2009; 16: 506-514.
49. Li L, Neaves WB. Normal stem cells and cancer stem cells:the niche matters. Cancer Res 2006; 66: 4553-4557.
50. Borovski T, De Sousa EM, Vermeulen L, Medema JP.Cancer stem cell niche: the place to be. Cancer Res 2011; 71:634-639.
51. Kryczek I, Wei S, Keller E, Liu R, Zou W. Stroma-derivedfactor (SDF-1/CXCL12) and human tumor pathogenesis.Am J Physiol Cell Physiol 2007; 292: C987-C995.
52. Hanahan D, Weinberg RA. Hallmarks of cancer: the nextgeneration. Cell 2011; 144: 646-674.
53. Shiozawa Y, Taichman RS. Cancer stem cells and the bonemarrow microenvironment. Bonekey Rep 2012; 2012: 48.
54. Keysar SB, Jimeno A. More than markers: biologicalsignificance of cancer stem cell-defining molecules. MolCancer Ther 2010; 9: 2450-2457.
55. Chen K, Huang YH, Chen JL. Understanding and targetingcancer stem cells: therapeutic implications and challenges.Acta Pharmacol Sin 2013; 34: 732-740.
56. Madka V, Rao CV. Cancer stem cell markers as potentialtargets for epithelial cancers. Indian J Exp Biol 2011; 49:826-835.
57. Han ME, Oh SO. Gastric stem cells and gastric cancer stemcells. Anat Cell Biol 2013; 46: 8-18.
58. Riether C, Schurch C, Ochsenbein AF. From “magic bullets”to specific cancer immunotherapy. Swiss Med Wkly 2013;143: w13734. doi: 10.4414/smw.2013.13734.
59. Hill RP, Perris R. “Destemming” cancer stem cells. J NatCancer Inst 2007; 99: 1435-1440.
60. Tu LC, Foltz G, Lin E, Hood L, Tian Q. Targeting stem cells-clinical implications for cancer therapy. Curr Stem Cell ResTher 2009; 4: 147-153.
61. Liu C, Tang DG. MicroRNA regulation of cancer stem cells.Cancer Res 2011; 71: 5950-5954.
62. Klonisch T, Wiechec E, Hombach-Klonisch S, et al. Cancerstem cell markers in common cancers - therapeuticimplications. Trends Mol Med 2008; 14:450-460.
63. Rasheed ZA, Kowalski J, Smith BD, Matsui W. Concisereview: Emerging concepts in clinical targeting of cancerstem cells. Stem Cells 2011; 29: 883-887.
64. Li F, Tiede B, Massague J, Kang Y. Beyond tumorigenesis:cancer stem cells in metastasis. Cell Res 2007; 17: 3-14.
65. Ponnusamy MP, Batra SK. Ovarian cancer: emergingconcept on cancer stem cells. J Ovarian Res 2008; 1: 4.
66. Ginestier C, Hur MH, Charafe-Jauffret E, et al. ALDH1 is amarker of normal and malignant human mammary stem cellsand a predictor of poor clinical outcome. Cell Stem Cell2007; 1: 555-567.
67. Steiniger SC, Coppinger JA, Kruger JA, Yates J, Janda KD.Quantitative mass spectrometry identifies drug targets incancer stem cell-containing side population. Stem Cells2008; 26: 3037-3046.
68. O’Brien CA, Pollett A, Gallinger S, Dick JE. A human coloncancer cell capable of initiating tumour growth inimmunodeficient mice. Nature 2007; 445: 106-110.
69. Read TA, Fogarty MP, Markant SL, et al. Identification ofCD15 as a marker for tumor-propagating cells in a mousemodel of medulloblastoma. Cancer Cell 2009; 15: 135-147.
70. Barretina J, Caponigro G, Stransky N, et al. The Cancer CellLine Encyclopedia enables predictive modelling ofanticancer drug sensitivity. Nature 2012; 483: 603-607.
71. Neve RM, Chin K, Fridlyand J, et al. A collection of breastcancer cell lines for the study of functionally distinct cancersubtypes. Cancer Cell 2006; 10: 515-527.
72. Charafe-Jauffret E, Ginestier C, Monville F, et al. Geneexpression profiling of breast cell lines identifies potentialnew basal markers. Oncogene 2006; 25: 2273-2284.
73. Li C, Heidt DG, Dalerba P, et al. Identification of pancreaticcancer stem cells. Cancer Res 2007; 67: 1030-1037.
74. Bosma MJ, Carroll AM. The SCID mouse mutant:definition, characterization, and potential uses. Annu RevImmunol 1991; 9: 323-350.
75. Ito M, Hiramatsu H, Kobayashi K, et al.NOD/SCID/gamma(c)(null) mouse: an excellent recipientmouse model for engraftment of human cells. Blood 2002;100: 3175-3182.
76. Shultz LD, Schweitzer PA, Christianson SW, et al. Multipledefects in innate and adaptive immunologic function inNOD/LtSz-scid mice. J Immunol 1995; 154: 180-191.
77. Ong GL, Baker AE, Mattes MJ. Analysis of highcomplement levels in Mus hortulanus and BUB mice.J Immunol Methods 1992; 154: 37-45.
78. van der Loo JC, Hanenberg H, Cooper RJ, Luo FY, LazaridisEN, Williams DA. Nonobese diabetic/severe combinedimmunodeficiency (NOD/SCID) mouse as a model systemto study the engraftment and mobilization of humanperipheral blood stem cells. Blood 1998; 92: 2556-2570.
79. Lock RB, Liem N, Farnsworth ML, et al. The nonobesediabetic/severe combined immunodeficient (NOD/SCID)mouse model of childhood acute lymphoblastic leukemia
167

reveals intrinsic differences in biologic characteristics atdiagnosis and relapse. Blood 2002; 99: 4100-4108.
80. Schatton T, Murphy GF, Frank NY, et al. Identification ofcells initiating human melanomas. Nature 2008; 451: 345-349.
81. Pretlow TG, Wolman SR, Micale MA, et al. Xenografts ofprimary human prostatic carcinoma. J Nat Cancer Inst 1993;85: 394-398.
82. Bosma MJ. B and T cell leakiness in the scid mouse mutant.Immunodefic Rev 1992; 3: 261-276.
83. Shultz LD, Lyons BL, Burzenski LM, et al. Humanlymphoid and myeloid cell development in NOD/LtSz-scidIL2R gamma null mice engrafted with mobilized humanhemopoietic stem cells. J Immunol 2005; 174: 6477-6489.
84. Rolstad B. The athymic nude rat: an animal experimentalmodel to reveal novel aspects of innate immune responses?Immunol Rev 2001; 184: 136-144.
85. Talmadge JE, Singh RK, Fidler IJ, Raz A. Murine models toevaluate novel and conventional therapeutic strategies forcancer. Am J Pathol 2007; 170: 793-804.
86. Kruger JA, Kaplan CD, Luo Y, et al. Characterization ofstem cell-like cancer cells in immune-competent mice.Blood 2006; 108: 3906-3912.
87. Charafe-Jauffret E, Ginestier C, Iovino F, et al. Breast cancercell lines contain functional cancer stem cells withmetastatic capacity and a distinct molecular signature.Cancer Res 2009; 69: 1302-1313.
88. Fridman R, Benton G, Aranoutova I, Kleinman HK, BonfilRD. Increased initiation and growth of tumor cell lines,cancer stem cells and biopsy material in mice usingbasement membrane matrix protein (Cultrex or Matrigel) co-injection. Nat Protoc 2012; 7: 1138-144.
89. Alonso-Camino V, Santos-Valle P, Ispizua MC, Sanz L,Alvarez-Vallina L. Engineered human tumor xenografts withfunctional human vascular networks. Microvasc Res 2011;81: 18-25.
90. Decaudin D. Primary human tumor xenografted models(‘tumorgrafts’) for good management of patients withcancer. Anticancer Drugs 2011; 22: 827-841.
91. Moro M, Bertolini G, Tortoreto M, Pastorino U, Sozzi G, RozL. Patient-derived xenografts of non small cell lung cancer:resurgence of an old model for investigation of modernconcepts of tailored therapy and cancer stem cells. J BiomedBiotechnol 2012; 2012: 568567.
92. Kim S, Park YW, Schiff BA, et al. An orthotopic model ofanaplastic thyroid carcinoma in athymic nude mice. ClinCancer Res 2005; 11: 1713-1721.
93. Gelbard A, Kupferman ME, Jasser SA, et al. An orthotopicmurine model of sinonasal malignancy. Clin Cancer Res2008; 14: 7348-7357.
94. Le NH, Franken P, Fodde R. Tumour-stroma interactions incolorectal cancer: converging on beta-catenin activation andcancer stemness. Br J Cancer 2008; 98: 1886-1893.
95. Penchev VR, Rasheed ZA, Maitra A, Matsui W.Heterogeneity and targeting of pancreatic cancer stem cells.Clin Cancer Res 2012; 18: 4277-4284.
96. Masood R, Hochstim C, Cervenka B, et al. A novelorthotopic mouse model of head and neck cancer and lymphnode metastasis. Oncogenesis 2013; 2: e68.
97. Yae T, Tsuchihashi K, Ishimoto T, et al. Alternative splicingof CD44 mRNA by ESRP1 enhances lung colonization ofmetastatic cancer cell. Nat Commun 2012; 3: 883. doi:10.1038/ncomms1892
98. Du L, Rao G, Wang H, et al. CD44-positive cancer stem cellsexpressing cellular prion protein contribute to metastaticcapacity in colorectal cancer. Cancer Res 2013; 73: 2682-2694.
99. La Porta CA. Thoughts about cancer stem cells in solidtumors. World J Stem Cells 2012; 4: 17-20.
100. Ruggeri BA, Camp F. Miknyoczki S. Animal models ofdisease: pre-clinical animal models of cancer and theirapplications and utility in drug Discovery. BiochemPharmacol 2013; 87: 150-161.
101. van der Worp HB, Howells DW, Sena ES, et al. Cananimal models of disease reliably inform human studies?PLoS Med 2010; 7: e1000245. doi:10.1371/journal.pmed.1000245.
102. Francipane MG, Chandler J, Lagasse E. Cancer stem cells:a moving target. Curr Pathobiol Rep 2013; 1: 111-118.
103. Lathia JD, Gallagher J, Myers JT, et al. Direct in vivoevidence for tumor propagation by glioblastoma cancerstem cells. PloS One 2011; 6: e24807. doi:10.1371/journal.pone.0024807.
104. Quintana E, Shackleton M, Sabel MS, Fullen DR, JohnsonTM, Morrison SJ. Efficient tumour formation by singlehuman melanoma cells. Nature 2008; 456: 593-598.
105. Curtis SJ, Sinkevicius KW, Li D, et al. Primary tumorgenotype is an important determinant in identification oflung cancer propagating cells. Cell Stem Cell 2010; 7: 127-133.
106. Cheng L, Ramesh AV, Flesken-Nikitin A, Choi J, NikitinAY. Mouse models for cancer stem cell research. ToxicolPathol 2010; 38: 62-71.
107. Valent P, Bonnet D, De Maria R, et al. Cancer stem celldefinitions and terminology: the devil is in the details. NatRev Cancer 2012; 12: 767-775.
108. Park S, Jiang Z, Mortenson ED, et al. The therapeuticeffect of anti-HER2/neu antibody depends on both innateand adaptive immunity. Cancer Cell 2010; 18: 160-170.
109. Xu Q, Liu G, Yuan X, et al. Antigen-specific T-cellresponse from dendritic cell vaccination using cancerstem-like cell-associated antigens. Stem Cells 2009; 27:1734-1740.
110. Mosier DE, Gulizia RJ, Baird SM, Wilson DB. Transfer ofa functional human immune system to mice with severecombined immunodeficiency. Nature 1988; 335: 256-259.
111. Lapidot T, Pflumio F, Doedens M, Murdoch B, WilliamsDE, Dick JE. Cytokine stimulation of multilineagehematopoiesis from immature human cells engrafted inSCID mice. Science 1992; 255: 1137-1141.
112. Shih CC, Hu J, Arber D, LeBon T, Forman SJ.Transplantation and growth characteristics of human fetallymph node in immunodeficient mice. Exp Hematol 2000;28: 1046-1053.
113. McCune JM, Namikawa R, Kaneshima H, Shultz LD,Lieberman M, Weissman IL. The SCID-hu mouse: murinemodel for the analysis of human hematolymphoiddifferentiation and function. Science 1988; 241: 1632-1639.
114. Shultz LD, Brehm MA, Garcia-Martinez JV, Greiner DL.Humanized mice for immune system investigation:progress, promise and challenges. Nature Rev Immunol2012; 12: 786-798.
115. Brehm MA, Shultz LD, Greiner DL. Humanized mousemodels to study human diseases. Curr Opin EndocrinolDiabetes Obes 2010; 17: 120-125.
116. Shankar S, Nall D, Tang SN, et al. Resveratrol inhibitspancreatic cancer stem cell characteristics in human andKrasG12D transgenic mice by inhibiting pluripotencymaintaining factors and epithelial-mesenchymal transition.PloS One 2011; 6: e16530.
117. Fu J, Rodova M, Roy SK, et al. GANT-61 inhibitspancreatic cancer stem cell growth in vitro and inNOD/SCID/IL2R gamma null mice xenograft. CancerLett 2013; 330: 22-32.
168

118. Wege AK, Ernst W, Eckl J, et al. Humanized tumor mice—a new model to study and manipulate the immune responsein advanced cancer therapy. Int J Cancer 2011; 129: 2194-2206.
119. Kuperwasser C, Chavarria T, Wu M, et al. Reconstructionof functionally normal and malignant human breast tissuesin mice. Proc Nat Acad Sci USA 2004; 101: 4966-4971.
120. Stewart JM, Shaw PA, Gedye C, Bernardini MQ, Neel BG,Ailles LE. Phenotypic heterogeneity and instability ofhuman ovarian tumor-initiating cells. Proc Nat Acad SciUSA 2011; 108: 6468-6473.
121. Doyle A, McGarry MP, Lee NA, Lee JJ. The constructionof transgenic and gene knockout/knockin mouse models ofhuman disease. Transgenic Res 2012; 21: 327-349.
122. Wolfer DP, Crusio WE, Lipp HP. Knockout mice: simplesolutions to the problems of genetic background andflanking genes. Trends Neurosci 2002; 25: 336-340.
123. Politi K, Pao W. How genetically engineered mouse tumormodels provide insights into human cancers. J Clin Oncol2011; 29: 2273-2281.
124. Snippert HJ, van Es JH, van den Born M, et al. Prominin-1/CD133 marks stem cells and early progenitors in mousesmall intestine. Gastroenterology 2009; 136: 2187-2194.
125. Gurney A, Axelrod F, Bond CJ, et al. Wnt pathwayinhibition via the targeting of Frizzled receptors results indecreased growth and tumorigenicity of human tumors.Proc Nat Acad Sci USA 2012; 109: 11717-11722.
126. Dallas NA, Xia L, Fan F, et al. Chemoresistant colorectalcancer cells, the cancer stem cell phenotype, and increasedsensitivity to insulin-like growth factor-I receptorinhibition. Cancer Res 2009; 69: 1951-1957.
R e c e i v e d : September 6, 2013A c c e p t e d : January 24, 2014
Author’s address: Dr. Sebastian C.J. Steiniger, Institute ofPharmaceutical Pharmacology, Johann Wolfgang GoetheUniversity, 9 Max von Laue Street, Frankfurt/Main, GermanyE-mail: [email protected]
169