Review Adipose tissue significance with special emphasis ... · PDF filemolecular mediators of...
16
Vol. 1 Issue 3, pp: (25-40), December 2016. Available online at: http://www.prudentjournals.org/IRJC Review Adipose tissue significance with special emphasis on its role in regulating immune functions in mammals M. K. Vidya 1 , Girish Kumar 1 , Madiajagan Bagath 2 , Govindan Krishnan 2 , R.K. Veeranna 2 , K.K. Sunil Kumar 1 , Veerasamy Sejian 2* and Raghavendra Bhatta 2 1 Veterinary College, Karnataka Veterinary Animal and Fisheries Sciences University, Hebbal, Bangalore-560024, India. 2 ICAR-National Institute of Animal Nutrition and Physiology, Adugodi, Bangalore-560030, India *Corresponding Author. E-mail: [email protected] Received 23 July, 2016; Accepted 13 November, 2016. Abstract This review attempts to cover the implication of the adipose tissue in controlling immune functions with emphasis on the structure and properties of adipose tissue, adipokines produced by adipose tissue, immune cells in adipose tissue and molecular mediators of adipose tissue inflammation. Adipose tissue (AT) in mammals is a complex, multi-depot, anatomically dissectible discrete structure with high metabolic activity. Both excess and deficiency of adipose tissue affect the normal homeostasis of the body. The AT comprises of two types of adipocytes, white adipocytes which store lipids whereas brown adipocytes which oxidize these lipids to produce heat. Further, to serving as a fat depot, AT also serves as endocrine adipose organ producing many bioactive molecules, called adipokines. These adipokines include leptin, adiponectin, visfatin, apelin, vaspin, omentin, resistin, hepacidin, monocyte chemoattractant protein (MCP), interleukin 6 (IL-6), tumor necrosis factor (TNF-α), plasminogen activator inhibitor (PAI-1) and other cytokines. Leptin is by far the most important endocrine parameter produced which regulates feed intake and considered as nutritional signal in mammals. In addition, leptin also was also found to be associated with controlling puberty, immunity, and autoimmune disorders. Adiponectin was found to be another noteworthy molecule produced from AT which increases fatty acid oxidation and reduces the synthesis of glucose in the liver. Further, adiponectin was found to have an anti-diabetic, anti-inflammatory and anti-atherogenic effect. A strong interplay between AT and immunity was established in mammals. Recently it was established that AT plays a huge role in controlling the immune functions in mammals through its close association with lymphoid organs; secreting inflammatory cytokines and adipokines; and through its anti-microbial and phagocytic activities. The involvement of AT in controlling immunity and autoimmune disorder was reported to be a significant breakthrough in cancer biology. Hence, it may be concluded that apart from acting as a fat depot to control energy metabolism, AT was also found to be associated with several other important biological functions signifying its role as an important endocrine organ in mammals. Keywords: Adipose tissue, Auto-immune disorder, Leptin, Adipokines, Immunity, Interleukins. International Research Journal of Chemistry Article Number: PRJA13407592 Copyright ©2016 Author(s) retain the copyright of this article Author(s) agree that this article remain permanently open access under the terms of the Creative Commons Attribution 4.0 International License.
Transcript of Review Adipose tissue significance with special emphasis ... · PDF filemolecular mediators of...

Vol. 1 Issue 3, pp: (25-40), December 2016. Available online at: http://www.prudentjournals.org/IRJC
Review
Adipose tissue significance with special emphasis on
its role in regulating immune functions in mammals M. K. Vidya1, Girish Kumar1, Madiajagan Bagath2, Govindan Krishnan2, R.K.
Veeranna2, K.K. Sunil Kumar1, Veerasamy Sejian2* and Raghavendra Bhatta2
1Veterinary College, Karnataka Veterinary Animal and Fisheries Sciences University, Hebbal,
Bangalore-560024, India.
2ICAR-National Institute of Animal Nutrition and Physiology, Adugodi, Bangalore-560030, India
*Corresponding Author. E-mail: [email protected]
Received 23 July, 2016; Accepted 13 November, 2016.
Abstract
This review attempts to cover the implication of the adipose tissue in controlling immune functions with
emphasis on the structure and properties of adipose tissue, adipokines produced by adipose tissue,
immune cells in adipose tissue and molecular mediators of adipose tissue inflammation. Adipose tissue
(AT) in mammals is a complex, multi-depot, anatomically dissectible discrete structure with high
metabolic activity. Both excess and deficiency of adipose tissue affect the normal homeostasis of the
body. The AT comprises of two types of adipocytes, white adipocytes which store lipids whereas brown
adipocytes which oxidize these lipids to produce heat. Further, to serving as a fat depot, AT also serves
as endocrine adipose organ producing many bioactive molecules, called adipokines. These adipokines
include leptin, adiponectin, visfatin, apelin, vaspin, omentin, resistin, hepacidin, monocyte
chemoattractant protein (MCP), interleukin 6 (IL-6), tumor necrosis factor (TNF-α), plasminogen activator
inhibitor (PAI-1) and other cytokines. Leptin is by far the most important endocrine parameter produced
which regulates feed intake and considered as nutritional signal in mammals. In addition, leptin also was
also found to be associated with controlling puberty, immunity, and autoimmune disorders. Adiponectin
was found to be another noteworthy molecule produced from AT which increases fatty acid oxidation
and reduces the synthesis of glucose in the liver. Further, adiponectin was found to have an anti-diabetic,
anti-inflammatory and anti-atherogenic effect. A strong interplay between AT and immunity was
established in mammals. Recently it was established that AT plays a huge role in controlling the immune
functions in mammals through its close association with lymphoid organs; secreting inflammatory
cytokines and adipokines; and through its anti-microbial and phagocytic activities. The involvement of
AT in controlling immunity and autoimmune disorder was reported to be a significant breakthrough in
cancer biology. Hence, it may be concluded that apart from acting as a fat depot to control energy
metabolism, AT was also found to be associated with several other important biological functions
signifying its role as an important endocrine organ in mammals.
Keywords: Adipose tissue, Auto-immune disorder, Leptin, Adipokines, Immunity, Interleukins.
International Research Journal of Chemistry Article Number: PRJA13407592 Copyright ©2016 Author(s) retain the copyright of this article Author(s) agree that this article remain permanently open access under the terms of the Creative Commons
Attribution 4.0 International License.

Introduction
Anatomically adipose tissue (AT) is a
complex structure comprising two types of
adipocytes, white and brown, each of which
differs in their anatomy and physiology. White
adipocytes store lipids whereas brown
adipocytes oxidize these lipids to produce heat
(non-shivering thermogenesis).
Until very recently, AT was thought to be a mere
fat storage sink. However, the discovery of leptin
sheds new light on the involvement of AT in
immunity. Apparently, the endocrine adipose
organ produces many bioactive molecules, called
adipokines. These adipokines include leptin,
adiponectin, visfatin, apelin, vaspin, omentin,
resistin, hepacidin, which regulate metabolism
and possess immunoregulatory properties1.
Among these adipokines, leptin and adiponectin
are the most important. Increased or altered
production of these factors in obesity may lead to
insulin resistance and metabolic syndrome 2.
Excess and deficiency of AT, both affect the
normal homeostasis of the body. Excess of AT
predisposes an individual to inflammation,
autoimmune diseases, and cancer. Obesity, the
hallmark of the metabolic syndrome, which takes
its origin to the expansion of AT in the body, is a
heterogenous disorder leading to insulin
resistance and type 2 diabetes mellitus (DM2).
Obesity is characterized by chronic, low-grade
inflammation with increased infiltration of immune
cells to the AT, especially visceral adipose tissue
(VAT) and switching of macrophages towards a
pro-inflammatory phenotype.
In a new research area called
immunometabolism, the role of immune cells of
the AT in the initiation and progression of
inflammation has been highlighted. Indeed, AT is
now considered an active immune organ with a
key role in metabolic homeostasis. Adipose
tissue contains many types of resident immune
cells3. There is infiltration of many other pro-
inflammatory and anti-inflammatory cells in
obesity. The pro-inflammatory cells include
macrophages, neutrophils, mast cells, CD8+ T
cells and B cells; whose number directly
correlates to the extent of inflammatory response.
Particularly, the AT macrophages (ATM) are
increased during obesity-induced inflammation.
In contrary, the anti-inflammatory cells like
eosinophils, regulatory T cells (Tregs), helper T
cells (Th2) cells and CD4+ T cells are negatively
correlated. Along with innate immune cells, T
cells and B cells also regulate insulin resistance
through the expression of cytokines on their cell
surface. Hence, both adaptive and innate
immune cells’ role has been implicated in the
inflammatory process of obesity. Although AT
was originally thought to have associated only
with fat storage and energy metabolism, the latest
information suggests its involvement in multiple
functions4,5. Hence, an attempt has been made in
this review to collate and synthesize information
pertaining to various biomolecules synthesized
and about the multifaceted functions of AT. This
review attempts to cover the implication of the
adipose tissue in controlling immune functions
with emphasis on the structure and properties of
adipose tissue, adipokines produced by adipose
tissue, immune cells in adipose tissue and
molecular mediators of adipose tissue
inflammation.
Structure and salient properties of adipose
tissue
Adipose tissue of mammals is a complex,
multi depot, anatomically dissectible discrete
structure with a high metabolic activity. It
comprises of two types of adipocytes, white and
brown, each of which differs both in their anatomy
and physiology. White adipocytes store lipids,
whereas brown adipocytes oxidize these lipids to
produce heat (non-shivering thermogenesis).
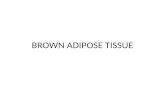
Uncoupling protein (UCP1) is a mitochondrial
protein, which is found only in brown adipocytes
to burn the lipids6. Fig. 1 describes the white and
brown fat cells.
Vidya et al 26

Fig. 1 describing the white and brown fat cells
Besides adipocytes, the AT produces bioactive
adipokines like leptin, adiponectin, visfatin,
apelin, vaspin, omentin, resistin, hepacidin3.
Further, the AT also produces important
cytokines like monocyte chemoattractant protein-
1 (MCP-1), interleukin 6 (IL-6), tumor necrosis
factor (TNF-α) and plasminogen activator
inhibitor (PAI-1)7. The adipose tissue also
contains connective tissue matrix, nerve tissue,
stromal vascular cells, and immune cells.
Together, these components function as an
integrated unit which contributes to the
inflammatory status of the body8.
White adipocytes are spherical, unilocular
adipocytes with a diameter of 40μ to 160μm
(lean, mammary subcutaneous) and 30μm to
100μm (lean, visceral perirenal). They are
surrounded by a distinct basal membrane and
have elongated and thin mitochondria with
randomly oriented cristae whereas, brown
adipocytes are polygonal in shape with a variable
diameter (15μ to 50μm). Unlike unilocular white
adipocytes which store the triglycerides as a
single lipid droplet, brown adipocytes are
multilocular wherein the triglycerides are present
in the form of multiple small vacuoles9. The brown
adipocytes have a large and numerous numbers
of mitochondria in the cytoplasm10. Furthermore,
in comparison to white adipocytes, brown
adipocytes are supplied with a denser blood
supply and nerve supply. Brown adipocytes are
present in all the Subcutaneous Adipose Tissue
(SCAT) and VAT depots. Their numbers are more
in young ones. Adipose tissue is diffused in the
body superficially and deeply as SCAT and VAT,
respectively11
Table 1: Physiological differences between VAT and SCAT
Properties VAT SCAT
Inflammatory and immune cells More Less
Large adipocytes More Less
Glucocorticoid and androgen receptors More Less
Transdifferentiation capacity Low High
Metabolic activity highly active Low
Lipolysis more sensitive Less
Insulin resistance More Less
Capaticity to generate Free Fatty Acids (FFA) More Less
Capacity to uptake glucose More Less
Sensitivity to adrenergic stimulation More Less
27 Int. Res. J. Chem.

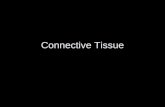
Fig.2. Role of adipose tissue in controlling different biological functions in mammals 4,12,13
There are regional variations in the adipose
tissue receptors density, affinity and signal
transduction11. Receptors of adipose tissue are
activated by three types of signals (i) endocrine
hormones in circulation; (ii) Paracrine mechanism
adipokines; (iii) nerve impulses from Central
Nervous System (CNS). The four kinds of
receptors in AT are (i) Glucocorticoid receptors,
(ii) Androgen receptors (iii) Estrogen receptors
(iv) Adrenergic receptors White and brown
adipocytes are often found intermingled with one
another. The relative amount of white, brown and
mixed regions are genetically determined and
depends on age, sex, environmental temperature
ADIPONECTINN
RESISTIN
VISFATIN
ADIPSIN
APELIN
Nutritional Cue Haematoposis Puberty Immunity
Anti-Diabetic Anti-Inflammatory Anti-Atherogenic
Diabetic Inflammatory Anti-Atherogenic
Glucose Chemotaxis Auto Immune Disorder
Obesity
Adipocyte Differentiation Complement Activation
Adipocyte Differentiation
ADIPOKINES CYTOKINES RESIDENT IMMUNE CELLS
INSULIN RESISTANCE & IMMUNITY
LEPTIN
ADIPOSE TISSUE
WHITE ADIPOSE TISSUE BROWN ADIPOSE TISSUE
LIPID STORAGE NON-SHIVERING THERMOGENESIS
ENDOCINE ADIPOSE ORGAN
Vidya et al 28
and nutritional status10. Fig. 2 describes the role
of adipose tissue in controlling different biological
functions in mammals.
Different adipokines produced by
Adipose tissue
Adipokines are the bioactive peptides
produced by the endocrine adipose organ which
regulates systemic metabolism and also possess
immunoregulatory properties1. These adipokines
include leptin, adiponectin, visfatin, apelin,
vaspin, omentin, resistin, hepcidin and few more.
Leptin
Leptin, the so-called “satiety hormone”
encoded by an obese (ob) gene in murines or
LEP gene located on chromosome 7 in humans;
was discovered in 1994 in the white adipose
tissue (WAT)14. This discovery hypothesized that
WAT takes part in immunity apart from its
paradigm of fat storing status15. The primary
function of leptin is to regulate fat stores by
inhibiting hunger which is in contrary to the effect
of “the hunger hormone” Ghrelin.
Leptin is a non-glycosylated peptide
hormone of 16 kDa, consisting 167 amino acids
belongs class-I cytokine superfamily. Besides
being mainly produced by WAT, leptin is also
produced by BAT, placenta, ovaries, skeletal
muscle, bone marrow16.
Leptin and its receptors
Leptin contains four antiparallel α-helices
which are interconnected. The structure and
function of leptin and its receptors closely
resembles the long-chain helical cytokines17.
When a molecule of leptin binds to its receptor, a
tetrameric complex is formed. The leptin receptor
forms homodimer to which two molecules of
leptin binds. Interestingly, it is the tetrameric
complex of ligand and receptor which induces
activation of the receptor through conformational
change and not mere the dimerization of the
receptor18. The leptin receptors (LEP-R or CD295
or OB-R) encoded by gene ‘ob’ are expressed in
the arcuate nucleus of the hypothalamus. The
leptin receptor (OB-R) has an extracellular
domain of 840-amino-acid with the signal
transducing component gp-130, which is in
common with IL-619.
Regulation of production of leptin
Leptin is found in circulation in both bound
form in association with plasma proteins and OB-
Re (leptin receptor subtype), and biologically
active free form. The levels of leptin in blood
follow the diurnal rhythm and are gender-
dependent which is slightly higher in females than
in males20. The circulating leptin levels varying
exponentially with WAT mass reflects the relative
amount of fat stored21. Increase in pro-
inflammatory cytokines like tumor necrosis factor
α (TNF-α) and IL-1, Insulin, inflammatory stimuli
like lipopolysaccharide (LPS) and turpentine
causes an acute increase in leptin expression22;
in obesity. So it also conveys that low leptin level
results in the depressed immune system with the
onset of starvation23.
Effects of leptin and its role in immunity
It stimulates satiety by promoting synthesis of α-
Melanocyte Stimulating Hormone (MSH), a
hunger suppressant24. Accumulation of fat in non-
adipose tissue in the body results in lipotoxicity
which can be prevented by stimulating fatty acid
oxidation and glucose uptake through the action
of leptin on hypothalamus25. Serum level of leptin
is increased during pregnancy whereas during
lactation an immune-reactive leptin is found,
which is transferred to the young ones through
milk3. The level of leptin controls the onset of
puberty26. Leptin deficiency is associated with
increased susceptibility to pro-inflammatory
stimuli like bacterial endotoxins and viral
infections27. Added to that, there is reduced
inflammation in models of autoimmune disease28.
Leptin has shown direct effects in both
innate and adaptive immunity. Leptin has a
pleiotropic role in innate immune cells i.e.,
antigen presenting cells (APCs) like dendritic
cells (DCs), macrophages/monocytes, and
neutrophils and natural killer (NK) cells. It
promotes the survivability and maturation of DCs.
It increases the proliferative and phagocytic
capacity of macrophages and monocytes. It also
promotes infiltration of macrophage into the
wound site29. Leptin role in adaptive immunity is
29 Int. Res. J. Chem.

to promote longevity of naive T cells by protecting
them from apoptosis, and also the production of
IFN-γ and IL-2 are also enhanced. Switching of
cytokine production from T cell towards Th1
phenotype is attributed to leptin. Also, it activates
Th1 cells and IgG2a switching of B cells while
they inhibit Th2 cells through a reduction in the
class switching of IgG1. Leptin suppresses B cell
apoptosis and hence increase their survivability30.
Leptin also plays a role in autoimmune disorders.
Production of leptin is much higher in
osteoarthritic human cartilage than in normal
cartilage. Obese individuals are protected against
osteoarthritic degeneration of cartilage as they
have high circulating level of leptin31.
Adiponectin
Encoded by the gene Adiponectin, C1Q and
Collagen Domain Containing (ADIPOQ) which is
located on chromosome 3q27, adiponectin is a
244 amino acid polypeptide. Adiponectin has a
plasma half-life of 2.5 hours in humans32. Unlike
leptin, it can cross blood brain barrier on its own33.
There are two receptors for Adiponectin
through which it acts, ADIPOR1 and ADIPOR234.
This adipokine has a wide spectrum of biological
activities and is well known for its role in the
regulation of insulin sensitivity. In humans,
adiponectin levels are positively correlated with
insulin sensitivity and inversely related to the
degree of adiposity and obesity35. Adiponectin
increases fatty acid oxidation and reduces the
synthesis of glucose in the liver. In addition to its
inhibitory effect on the phagocytic activity of the
macrophages and the production of IL-6 and
TNFα, it also reduces B-cell lymphopoiesis and
decreases T-cell response. Thus, it has a
protective role against obesity2. It induces the
production of anti-inflammatory factors IL-10 and
IL-1RA (IL-1 receptor antagonist) by human
monocytes and APCs like macrophages and
dendritic cells2. Adiponectin has the anti-diabetic,
anti-inflammatory and anti-atherogenic effect to
protect the body during adverse conditions.
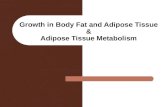
Fig. 3 describes the different types of inflammatory responses of adipose tissues in mammals.
Vidya et al 30

Resistin
Resistin is a dimeric polypeptide with a
molecular weight of 12 kDa containing 114 amino
acids. It belongs to the family of cysteine-rich C-
terminal domain proteins, also called as resistin-
like molecules (RELMs). They are predominantly
found in adipocytes in mice. In contrast,
macrophages are the important source of resistin
in humans along with adipocytes, muscle, and
pancreatic cells. This polypeptide molecule has
been implicated in representing an interesting role
in the regulation of inflammatory processes36.
Expression of resistin in serum can be
increased by pro-inflammatory cytokines IL-1, IL-6
and TNF, and by LPS stimulated macrophages in
humans whereas decreased by PPARγ agonists
(eg. pliaglitazone)10. Furthermore, cytokines like
IFNγ and leptin had no effect on its expression. As
found in rodents, expression of resistin is 15-fold
greater in SCAT than in VAT37.
Visfatin
Visfatin is a peptide hormone exhibiting its
function through endocrine, autocrine and
paracrine function. It is expressed preferentially in
white adipocytes of visceral adipose tissue and
has been identified in various tissues and organs
like brain, lung, kidney, spleen, and testis. It is also
produced by neutrophils. This adipokine mimics
the action of insulin by binding and activating the
insulin receptor thereby decreasing the insulin
resistance38. Interestingly, it does not
competitively inhibit insulin, indicating that the two
proteins bind to different sites on the insulin
receptor.
Adipsin
Adipsin, also called as complement factor
D or C3 convertase activator, is derived from
adipocyte differentiation-dependent serine
protease gene. It is expressed during adipocyte
differentiation and is a rate-limiting enzyme in the
alternative pathway of complement activation.
Adipsin is primarily found in adipocytes in mice
and in both adipocytes and monocytes-
macrophages in humans39. Further, adipsin is
required for the production of acylation stimulating
protein (ASP), a complement protein that affects
lipid and glucose metabolism by cleaving the
terminal arginine of C3a by carboxypeptidase B
(CbB)40. Decreased level of adipsin has been
reported in murines during obesity. However, in
humans increased adipsin level was reported with
adiposity, insulin resistance, dyslipidemia, and
cardiovascular disease40.
Apelin
It is a bioactive peptide produced in TNFα
stimulated adipose tissue. It is expressed during
adipocyte differentiation. Similar to insulin, plasma
and circulating apelin levels are increased in
obesity41.
Vaspin
Secretion of vaspin from AT is a
compensatory mechanism for the damage caused
by obesity and its complications. It is produced
from the VAT and is known to improve glucose
tolerance and insulin sensitivity in obese mice24. It
is believed that vaspin could be regarded as a new
link between obesity and related metabolic
disorders42.
Hepcidin
Being produced by liver, hepcidin is the
master regulator of iron homeostasis. It was later
identified as an adipokine that has a role in
mediation of antimicrobial immunity also43.
Synthesis of hepcidin depends on plasma iron
level, hypoxia and inflammatory stimuli. Induction
of hepcidin represents a component of the innate
immune response to acute infection, with the
potential to affect disease pathogenesis44.
Omentin
Omentin is also called as intelectin. It is
produced from omental AT (milky spots)45.
Through recognition of pathogens and bacterial
components it has acquired importance in innate
immune response against parasitic infection.
Further, the expression of omentin gene is altered
in obesity46.
Adipose tissue role in immunity (innate
and adaptive)
There are many other pieces of evidence
that signify the interplay between AT and
immunity47,48. Firstly, a close anatomical
interaction with lymphoid organs47. Secondly,
other than adipocytes, AT also secretes
31 Int. Res. J. Chem.

inflammatory cytokines and adipokines. Thirdly,
the AT exhibits anti-microbial and phagocytic
activity through adipose resident macrophages49.
Finally, excess adiposity activates a cascade of
events like ER stress and apoptosis of
adipocytes50. So, it is important to know how the
immune functions are carried out by AT.
Immunity is the protective mechanism of
the body that comprises of two different types –
innate and adaptive immunity. Activation of innate
immune system is induced by either pathogen
associated molecular patterns (PAMPs) from
pathogens or damage associated molecular
patterns (DAMPs) from dying cells, which are
recognized by pattern recognition receptors
(PRRs) of the host. The PRRs include toll-like
receptors (TLRs), nucleotide-binding
oligomerization domain (NOD)-like receptors
(NLRs), C-type lectin receptors (CLRs), and
retinoic acid–inducible gene (RIG)-I-like receptors
(RLRs). Subsequently, these signals lead to
activation of innate immune cells like
macrophages, dendritic cells (DCs), mast cells,
neutrophils, eosinophils and natural killer (NK)
cells51.
However, adaptive immune system is
different from the innate immune system in a way
that it is extremely specific against a particular
antigen. Adaptive immune mechanisms are
mediated by B or T lymphocytes, including many
subsets of T cell population like CD4+, CD8+ T,
and NK T (NKT) cells. These cells have highly
specific receptors on their surface called B cell
receptor (BCR) and T cell receptors (TCR), which
are equipped with the ability to recognize an
enormous number of antigens specifically52.
Immune cells in adipose tissue
Macrophages
Macrophages are the most abundantly
found leukocytes in AT53 and represent 5% of the
stromal vascular fraction in lean AT which
increases up to 25-30% in obese AT54. There are
two phenotypic states, M1 (classically activated)
and M2 (alternatively activated) macrophages
which reversibly switch among themselves
depending on the metabolic status of AT.
Normally, M2 phenotype macrophages present in
the AT helps to maintain the state of insulin
sensitivity through secretion of anti-inflammatory
cytokine IL-10. In contrary to M1 macrophages,
the pro-inflammatory M2 macrophages produce
IL-6 and TNF-α which are directly involved in local
and systemic inflammation and insulin
resistance55.
Dendritic cells
The DCs are professional antigen-
presenting cells that present antigen to T cells
through major histocompatibility complex (MHC)
II. Hence they are involved in both innate and
adaptive immunity56. They produce cytokines IL-
12 and IL-15 which are involved in inducing the
differentiation of naive T cells into Th1 T cells and
proliferation and activation of CD8 T cells and NK
cells, respectively57. Their circulating numbers are
increased in obesity and also have a role in the
aggregation of macrophages around the
adipocytes58.
Neutrophils
Neutrophils, the first leukocytes to arrive at
the site of inflammation, comprises of 1.5% of the
stromal vascular fraction of AT. The inflamed
adipocytes secrete neutrophil chemoattractant
protein, IL-859. Subsequently, through the
production of MCP-1 and other cytokines, the
neutrophils recruit the monocytes which
perpetuate the inflammation. In obese individuals,
elevated plasma myeloperoxidase level is
reported which is a neutrophil marker; indicative of
inflammation60,61.
Eosinophils
Eosinophils are the sentinels of WAT that
influences metabolic regulation and represent
about 5% of stromal vascular cells of AT which is
decreased in obesity62. They are produced in bone
marrow and then recruited into AT with the help of
IL-563. Primarily, these cells are more in lean
individuals and eosinophilia is linked with insulin
sensitivity. Their population is decreased in
obesity leading to insulin resistance. Mainly,
resident eosinophils of WAT are the primary
source of IL-4 and IL-13 which is required for
activation of M2 macrophages64.
Vidya et al 32

Mast cells
Mast cells are involved in the orchestration
of immune cells and activation of DCs thereby the
adaptive immunity65. There are two types of mast
cells, MT that express only tryptase and MCTC
which express both chymase and tryptase. MCTC
are the type of mast cells present in AT66. The
activated macrophages secrete a wide range of
pro- and anti-inflammatory cytokines (TNFα, IL-1β,
IL-6, IFNγ, TGF-β, IL-4 and IL-10). IL-6 and IFNγ
promote the inflammatory processes in the AT.
Accordingly, mast cells are accumulated in the
obese AT67.
T cells
The T cells are the important lymphocytes
of adaptive immunity. Further to macrophages,
both B and T lymphocytes are the other largest
groups of immune cells present in AT68. They are
produced in the bone marrow and maturation
takes place in thymus69. Based on their function,
they are divided into T helper cells (IFNγ-
producing Th1 cells, IL-4-producing Th2 cells, IL-
17-producing Th17 cells, and IL-10-producing
regulatory T cells) and cytotoxic T cells. T helper
cells bear CD4+ surface marker and MHC II
molecules on their surface through which they
present the antigen while cytotoxic T cells bear
CD8+ marker and MHC I molecule on their surface
for antigen recognition. The regulatory T cells bear
CD4+ marker on their surface70.
Th1
The Th1 cells are increased in obesity
while Th2 cells are reduced. Th1 cells secrete
IFNγ which directly helps in the polarization of M2
macrophages and thereby acts as a pro-
inflammatory immune cell68.
Tregs
Tregs are found in more numbers in lean
AT and they are reduced in obesity71. These
regulatory T cells are required by the AT to
maintain a normal anti-inflammatory state. Indeed,
they are involved in preventing the self-destructive
immune responses in AT. Further, they enroll
themselves in sustaining the macrophages in M2
state through secretion of IL-1071. Also, they
express peroxisome proliferator-activated
receptor gamma (PPARγ) factor which is crucial
for the anti-inflammatory function of Tregs72.
Cytotoxic T cells (CTLs)
The CTLs are the CD8+ T cell population.
Their numbers in circulation are increased by 3 to
4 fold in obesity. They increase the recruitment of
macrophages and expression of TNFα and IL-6
thereby promoting the inflammatory responses73.
Invariant natural killer T cells (iNKT)
The iNKT are a type of NK cells that
recognize antigen presented even by CD1d
antigen presenting molecules expressed by DCs,
macrophages, B cells and T cells74. Interestingly,
CD1d activated iNKT cells are known for their
ability to rapidly produce Th1 and Th2 cytokines.
These iNKT cells improve the insulin sensitivity.
Their numbers are more in murine and human AT
and are reversibly reduced in obesity75.
B-cells
B-cells are synthesized from the bone
marrow in an immature form which contains IgM
BCR. After being transported to various secondary
lymphoid organs like the spleen or lymph node, the
B cell undergoes complete maturation and
differentiates into other antibodies viz., IgA, IgD,
IgG, and IgE76. In lean animals, they provide
immunity against infection. However in obesity, B-
cells undergo functional changes and influence
the AT pathologically to develop insulin
resistance77. Furthermore, they also influence the
polarization of M2 to M1 macrophages and they
are involved in downregulation of Tregs78.
Cytokines secreted by adipose tissue
Cytokines are the hormonal messengers
involved in cell-mediated immunity. Obesity-
induced insulin resistance occurs in adipocytes,
hepatocytes, myocytes and β-cells whereas,
obesity-induced inflammation occur in the tissue-
infiltrating immune cells. Obesity-inflamed immune
cells produce cytokines that mediate the insulin
resistance and recruitment of other tissue-resident
immune cells. Cytokines can be grouped into two
functional types – pro-inflammatory (TNFα, IL-6,
IL-1 β, Plasminogen activator inhibitor-1 (PAI-1),
C-reactive protein, Monocyte chemoattractant
33 Int. Res. J. Chem.

protein (MCP-1) and anti-inflammatory cytokines
(IL-13, IL-4, IL-10)7.
Molecular mediators of AT inflammation
Lipids are the essential signaling moieties
in metabolic regulation79. Besides, they are also
required for enhancing the inflammatory gene
expression in AT80. There are many mechanisms
through which lipids carry out the inflammatory
functions. For example, (Toll Like Receptors)
TLRs, inflammasomes, nuclear receptors, cell
death, endoplasmic reticulum (ER) stress,
cytokines, and hypoxia.
The IKKβ/NFκB pathway
Nuclear factor-κB (NFκB) is a molecular
mediator of inflammation81. Resting cells have
NFκB bound to IκBα in the cytoplasm; so its
nuclear localization sequence (NLS) is
unexposed. Any stimuli like growth factors,
cytokines, and foreign pathogens activate the IKK
enzyme complex which phosphorylates Ser32 and
36 of IκBα inducing the proteasome-dependent
degradation of IκBα. It causes translocation of
NFκB into the nucleus finally leading to initiation of
the gene expression of various inflammatory
mediators like TNFα, IL-6, and MCP-1.
Jun N-terminal kinases (JNKs)
The Jun N-terminal kinase/stress-
activated protein kinases (JNK/ SAPKs) plays a
major role in insulin resistance through ER stress
pathway where it directly inhibits the insulin
signaling pathway and affects insulin-responsive
cells82.
Endoplasmic Reticulum Stress
The ER is the site for the synthesis, folding,
and secretion of the membrane and secretory
proteins. Acute shortage of proteins may lead to
accumulation of misfolded proteins and hence
disrupting the ER homeostasis. Finally, to maintain
ER homeostasis the unfolded protein response
(UPR) signaling pathway is activated83. This is a
potential mechanism in the pathologic
development of obesity and types 2 diabetes. The
stressors induce the activation of ER stress sensor
Inositol-requiring-enzyme 1α (IRE1α) or ER-
resilient eukaryotic translation inhibition factor 2α
(eIF2α) kinase PERK to cause the activation of
inflammatory signaling cascades, such as the JNK
and NF-κB pathways82.
Inflammasome pathway
The inflammasome is a high-molecular-
weight multimeric intracellular complex that plays
a major role in innate immunity84. There are four
classes of inflammasomes - the NLR family, pyrin
domain–containing 1 and 3 (NLRP1 and NLRP3),
CARD domain–containing 4 (NLRC4, also known
as IPAF), and absent in melanoma 2 (AIM2)
inflammasomes. This complex is activated by
(Danger Associated Molecular Patterns) DAMPs
or (Pathogen Asscociated Molecular Patterns)
PAMPs. Since excess adiposity mimics the
danger signals mediated by DAMPs or PAMPs,
inflammasome pathway has key role pathology of
obesity and insulin resistance85.
Peroxisome Proliferator-Activated Receptors
(PPAR)
The PPARα, PPARδ, and PPARγ nuclear
receptors are transcription factors which are
expressed by macrophages and adipocytes that
mediate the effects of fatty acids and their
derivatives on gene expression. Notably, these
nuclear receptors have a role in polarization of
macrophages towards M2 phenotype and hence
improve insulin sensitivity78. They interfere with the
activity of pro-inflammatory transcription factors
NF-κB, (Activator Proteins) AP-1, and (Signal
Transducers and Activators of Transcription)
STATs, and inhibit inflammatory gene expression.
Cell Death
Pathological apoptosis of cells releases
intracellular molecules known as damage-
associated molecular patterns (DAMPs) that
activate the innate and adaptive immune
systems86. In obesity, adipocytes may die by
apoptosis87 and/or by necrosis10 which signal for
the recruitment of immune cells or activate
inflammasomes via adipocyte-associated DAMPs.
Interplay between AT and immunity
Recently, there are many pieces of
evidence suggesting that there is a cross-talk
between metabolic and immune system86,87. This
cross-talk is mediated by adipokines, cytokines
and immune cells which are expressed by the AT.
Vidya et al 34

Excess deposition of adiposity causes
dysfunction, a disorder characterized by chronic
low-grade subclinical inflammation, leading to
insulin resistance and metabolic, type 2 diabetes
mellitus, cardiovascular disease (CVD),
dyslipidemia, hepatic steatosis, cancers,
respiratory infections and other infections. These
conditions may cause morbidity and sometimes
they may also result in mortality88.
Obesity increases the number and
activation levels of pro-inflammatory cells and thus
mimicking the signals elicited by bacterial
infection. Among various pro-inflammatory cells,
adipose tissue macrophages are highly increased
in obesity.
Role of AT in Cancer:
Mechanism linking obesity and cancer is
not clear however the association of obesity with
chronic inflammation cannot be denied89.
Accumulation of AT in individuals leads to obesity
over a period of time. This increase in the AT
causes chronic hyperinsulinaemia with alteration
in peptide and steroid hormones. This alteration is
postulated for the development of cancer90.
Obesity related hormones/growth factors plays
vital role in the cross talk between adipocytes,
macrophages, and epithelial cells during cancer.
Dysfunction of adipose tissue, obesity towards
growth factor signaling and chronic inflammation
might also contribute to cancer91.
In obesity, hypertrophy of adipocyte,
hyperplasia of AT, alter the regulations within the
ATs leading to adiposopathy which actually means
promotion of pathogenic adipocytes and AT
related disorders92. It has been estimated that 20%
of all cancers are caused by excess weight gain.
Some common cancers that have increased risk
of occurrence with increased adiposity are
prostate, colon, breast, endometrial and
pancreatic cancers93. Leptin synthesized from AT
plays a vital role in autoimmune disorder by
maintaining immune suppression in individuals by
maintain a balance between metabolism and
immunity. In vitro studies of leptin on cancer cells
are indicative of proliferation of various cancers
due to leptin. The general effects of leptin in cancer
research include proliferation, cell survival,
angiogenesis, and subsequent cancer
progression94.
Adiponectin is one of the only adipocyte-
secreted protein with beneficial effects on health.
When adiponectin is decreased with obesity,
known as hypoadiponectinemia, as the result of
increased secretion of other cytokines like TNFα,
its anti-disease properties are also decreased. As
the most prolific protein secreted by adipocytes,
adiponectin is anti-inflammatory, pro-apoptotic,
and anti-proliferative under normal
circumstances95. There are two ways the hormone
can effect cancer retardation: either directly on the
tumor cells as several cancer lines express
adiponectin receptors or through its insulin-
sensitizing effects. Either way, decreases in
adiponectin have been associated with breast,
endometrial, colon, esophageal, and liver cancer
among many others96.
Cytokines are another class of molecule
that have been heavily indicated in the induction
and pathogenesis of cancer. Cytokines are
primarily linked to the development of cancers by
way of their influence on inflammation, mainly
chronic low grade inflammation associated with
many diseases such as obesity, hence
inflammation is one of the major factors that links
obesity to the development of its associated co-
morbidities97. Further, Apelin produced and
secreted by adipocytes, had been demonstrated
to play a role in lymph node metastasis and
lymphangiogenesis via binding to its receptor in
lymphatic endothelial cells that activates ERK and
PI3K pathways, leading to cell proliferation,
migration, and cell survival98. In addition, studies
on visfatin, resistin, and chemerin shown that
these adipokines enhance the progression of
cancers, while omentin shown anti-cancerous
action97.
Conclusion
Apart from its usual involvement in energy
metabolism, AT was also found to control other
important biological functions in mammals through
secretion of specialized molecules called
adipokines. Among these adipokines, leptin and
adiponectin are the predominant ones involved in
controlling additional biological functions. Further,
35 Int. Res. J. Chem.

it was also established that AT plays a huge role
in controlling the immune functions in mammals. In
addition, AT was also found to be associated with
controlling immunity and autoimmune disorders in
mammals. All these findings signify the importance
of AT in controlling various immune functions in
mammals and the most noteworthy progress
made was to elucidate its role in cancer biology.
Future research efforts are necessary to further
understand the hidden intricacies of AT in
controlling all these biological functions.
Conflict of Interest Statement
The authors declare that there is no any conflict of
interest for this manuscript
Acknowledgement
The authors extend their sincere thanks to director
NIANP for giving permission for submitting this
manuscript.
References:
Trayhurn P and Wood IS. 2005. Signalling role of
adipose tissue: adipokines and inflammation in
obesity. Biochem. Soc. Trans., 33: 1078-1081.
Tilg H and Moschen AR. 2006. Adipocytokines:
mediators linking adipose tissue, inflammation and
immunity. Nature Rev. Immunol., 6: 772-783.
Schipper HS, B Prakken, E Kalkhoven and M Boes.
2012. Adipose tissue-resident immune cells: key
players in immunometabolism. Trends Endocrinol.
Metabol., 23: 407-415.
Freedland ES. 2004. Role of critical visceral adipose
tissue threshold in metabolic syndrome: implications
for controlling dietary carbohydrates. Nutr. Metabol., 1:
12-35.
Ouchi N, Kihara S, Arita Y, Maeda K, Kuriyama H,
Okamoto Y, Hotta K, Nishida M, Takahashi M,
Nakamura T. and Yamashita, S. 1999. Novel
modulator for endothelial adhesion molecules
adipocyte-derived plasma protein adiponectin.
Circulation., 100: 2473-2476.
Cannon B, Hedin A and Nedergaard J. 1982.
Exclusive occurrence of thermogenin antigen in brown
adipose tissue. FEBS Lett., 150: 129-132.
Coppack SW 2001. Pro-inflammatory cytokines and
adipose tissue. Proc. Nutr. Soc., 60: 349-356.
Kershaw EE and Flier JS. 2004. Adipose tissue as an
endocrine organ. J. Clinic. Endocrinol. Metabol., 89:
2548-2556.
Blanchette-Mackie EJ, Dwyer NK, Barber T, Coxey RA
Takeda T, Rondinone CM, Theodorakis JL,
Greenberg AS and Londos C. 1995. Perilipin is located
on the surface layer of intracellular lipid droplets in
adipocytes. J. Lipid Res., 36: 1211-1226.
Cinti S, 2009. Transdifferentiation properties of
adipocytes in the adipose organ. Am. J. Physiol.
Endocrinol. Metab., 297: E977-E986.
Rolfe EDL, Ong KK, Sleigh A, Dunger DB, Norris S A,
2015. Abdominal fat depots associated with insulin
resistance and metabolic syndrome risk factors in
black African young adults. BMC Public Health, 15:
1013
Joyner JM, Hutley LJ and Cameron DP 2000.
Glucocorticoid receptors in human preadipocytes:
regional and gender variations. J. Endocrinol., 166:
145-152.
Hellmer J, Marcus C, Sonnefeld T and Arner P. 1992.
Mechanisms for differences in lipolysis between
human subcutaneous and omental fat cells. J. Clin.
Endocrinol. Metab., 75: 15-20.
Rohner-Jeanrenaud F and Jeanrenaud B. 1996. The
discovery of leptin and its impact in the understanding
of obesity. European journal of endocrinology, 135:
649-650.
Zhang Y, Proenca R, Maffei M, Barone M, Leopold L
and Friedman JM. 1994. Positional cloning of the
mouse obese gene and its human homologue. Nature,
372: 425-432.
Bado A, Levasseur S, Attoub S, Kermorgant S,
Laigneau JP, Bortoluzzi MN, Moizo L, Lehy T and
Guerre-Millo M. 1998. The stomach is a source of
leptin. Nature, 394: 790-793.
Zhang F, Basinski MB, Beals JM, Briggs, SL, Churgay
LM, Clawson DK and DiMarchi RD. 1997. Crystal
structure of the obese protein leptin-E100. Nature,
387: 206-209.
Fong TM, Huang RR, Tota MR, Mao C, Smith T,
Varnerin J, Karpiyskiy VV, Krause JE and Van der
Ploeg LH. 1998. Localization of leptin binding domain
in the leptin receptor. Mol. Pharmacol., 53: 234-240.
Vidya et al 36

Baumann H, Symes AJ, Comeau MR, Morella KK,
Wang Y, Friend D, Ziegler SF, Fink JS and Gearing
DP 1994. Multiple regions within the cytoplasmic
domains of the leukemia inhibitory factor receptor and
gp130 cooperate in signal transduction in hepatic and
neuronal cells. Mol. Cell Biol., 14: 138-146.
Otero M, Lago Gomez R, C Dieguez, F Lago, J
Gomez-Reino and Gualillo O. 2006. Towards a pro-
inflammatory and immunomodulatory emerging role of
leptin. Rheumatology, 45: 944-950.
Madej T. 1998. Considerations in the use of lipid-
based drug products. J. Intraven. Nurs., 21: 326-329.
Sarraf P, Frederich RC, Turner EM, Ma G, Jaskowiak
NT, Rivet DJ, Flier JS and Lowell B. 1997. Multiple
cytokines and acute inflammation raise mouse leptin
levels: potential role in inflammatory anorexia. J. Exp.
Med., 185: 171-175.
Ozata M, Ozdemir IC and Licinio J. 1999. Human
leptin deficiency caused by a missense mutation:
multiple endocrine defects, decreased sympathetic
tone, and immune system dysfunction indicate new
targets for leptin action, greater central than peripheral
resistance to the effects of leptin, and spontaneous
correction of leptin-mediated defects. J. Clin.
Endocrinol. Metab., 84: 3686-3695.
Lago F, Dieguez C, Gómez-Reino J and Gualillo O
2007. Adipokines as emerging mediators of immune
response and inflammation. Nature Clinical Practice,
3: 716-724.
Minokoshi Y and Kahn BB. 2003. Role of AMP
activated protein kinase in leptininduced fatty acid
oxidation in muscle. Biochem. Soc. Trans., 31: 196-
201.
Garcia-Mayor RV, Andrade MA, Rios M, Lage M,
Dieguez C and Casanueva FF, 1997. Serum leptin
levels in normal children: Relationship to age, gender,
body mass index, pituitary-gonadal hormones, and
pubertal stage 1. J. Clin. Endocrinol. Metabol. 82(9):
2849-2855.
Takaya K, Ogawa Y, Isse N, Okazaki T, Satoh, N.,
Masuzaki H, Mori K and Tamura N. 1996. Molecular
cloning of rat leptin receptor isoform complementary
DNAs-identification of a missense mutation in Zucker
fatty (fa/fa) rats. Biochem. Biophys. Res. Commun.,
225: 75-83.
Fantuzzi G. 2005. Adipose tissue, adipokines, and
inflammation. J. Allergy Clin. Immunol., 115: 911-919.
Goren I, Kampfer H, Podda M, Pfeilschifter J and
Frank S. 2003. Leptin and wound inflammation in
diabetic ob/ob mice: differential regulation of
neutrophil and macrophage influx and a potential role
for the scab as a sink for inflammatory cells and
mediators. Diabetes, 52: 2821-2832.
Faggioni R, Feingold KR and Grunfeld C. 2001. Leptin
regulation of the immune response and the
immunodeficiency of malnutrition. FASEB J., 15:
2565-2571.
Dumond H, Presle N, Terlain B, Mainard D, Loeuille D,
Netter P and Pottie P. 2003. Evidence for a key role of
leptin in osteoarthritis. Arthritis & Rheumatism, 48(11):
3118-3129.
Yamauchi T, Iwabu M, Okada-Iwabu M and Kadowaki,
T. 2014. Adiponectin receptors: a review of their
structure, function and how they work. Best Pract. Res
Clin. Endocrinol. Metab., 28(1):15-23.
Dumond H, Presle N, Terlain B, Mainard D, Loeuille D,
Netter P and Pottie P. 2003. Evidence for a key role of
leptin in osteoarthritis. Arthritis & Rheumatism, 48(11):
3118-3129.
Hug C, Wang J, Ahmad NS, Bogan JS, Tsao TS and
Lodish HF. 2004. T-cadherin is a receptor for
hexameric and high-molecular-weight forms of
Acrp30/adiponectin. Proc. Natl. Acad. Sci. U.S.A.,
101(28): 10308-10313.
Arita Y, Kihara S, Ouchi N, Takahashi M, Maeda K,
Miyagawa J, Hotta K, Shimomura I, Nakamura T,
Miyaoka K, Kuriyama H, Nishida M, Yamashita S,
Okubo K, Matsubara K, Muraguchi M, Ohmoto Y,
Funahashi T, Matsuzawa Y. 1999. Paradoxical
decrease of an adipose-specific protein, adiponectin,
in obesity. Biochem Biophys Res Commun.,
257(1):79-83.
Holcomb IN, Kabakoff RC, Chan B, Baker TW, Gurney
A and Henzel W. 2000. FIZZ1, a novel cysteine-rich
secreted protein associated with pulmonary
inflammation, defines a new gene family. EMBO J., 19:
4046-4055.
Banerjee RR and Lazar MA. 2003. Resistin: molecular
history and prognosis. J. Mol. Med., 81: 218-226.
Fukuhara A, Matsuda M, Nishizawa M., Segawa K,
Tanaka M, Kishimoto K, Matsuki Y, Murakami M,
Ichisaka T, Murakami H. and Watanabe E. 2005.
37 Int. Res. J. Chem.
https://www.ncbi.nlm.nih.gov/pubmed/?term=Miyagawa%20J%5BAuthor%5D&cauthor=true&cauthor_uid=10092513
https://www.ncbi.nlm.nih.gov/pubmed/?term=Nakamura%20T%5BAuthor%5D&cauthor=true&cauthor_uid=10092513

Visfatin: a protein secreted by visceral fat that mimics
the effects of insulin. Science, 307: 426-30.
Gabrielsson BG, Johansson JM, Lonn M, Jernas M,
Olbers T and Peltonen M. 2003. High expression of
complement components in omental adipose tissue in
obese men. Obes. Res., 11: 699-708.
Liu Y, Gupta P, Lapointe M, Yotsapon T, Sarat S,
Cianflone K. 2014. Acylation stimulating protein,
component C3 and lipid metabolism in ketosis-prone
daiabetic subjects. Plos One 9(10): e109237.
Daviaud D, Boucher J, Gesta S, Dray C, Guigne C and
Quilliot D. 2006. TNFalpha up-regulates apelin
expression in human and mouse adipose tissue.
FASEB J., 20: 1528-1530.
Dimova R. and Tankova T. 2015. The role of vaspin in
the development of metabolic and glucose tolerance
disorders and atherosclerosis. BioMed Research
International. Article ID 823481, 7 pages.
Bekri S, Gual P, Anty R, Luciani N, Dahman M,
Ramesh, B, Iannelli A, Staccini–Myx A, Casanova D,
Amor IB. and Saint–Paul MC. 2006. Increased
adipose tissue expression of hepcidin in severe
obesity is independent from diabetes and NASH.
Gastroenterology, 131(3): 788-796.
Armitage AE, Eddowes LA, Gileadi U, Cole S,
Spottiswoode N, Selvakumar TA, Ho LP, Townsend
AR and Drakesmith H. 2011. Hepcidin regulation by
innate immune and infectious stimuli. Blood, 118:
4129-4139.
Schäffler A, Neumeier M, Herfarth H, Fürst A,
Schölmerich J and Büchler C. 2005. Genomic
structure of human omentin, a new adipocytokine
expressed in omental adipose tissue. Biochimica et
Biophysica Acta (BBA)-Gene Structure and
Expression, 1732: 96-102.
de Souza Batista CM, Yang RZ, Lee MJ, Glynn NM,
Yu DZ, Pray J, Ndubuizu K, Patil S, Schwartz A,
Kligman M. and Fried SK. 2007. Omentin plasma
levels and gene expression are decreased in obesity.
Diabetes, 56: 1655-1661.
Pond CM. 2003. Paracrine relationships between
adipose and lymphoid tissues: implications for the
mechanism of HIV-associated adipose redistribution
syndrome. Trends Immunol., 24: 13-18.
Matarese G and La Cava A. 2004. The intricate
interface between immune system and metabolism.
Trends Immunol., 25: 193-200.
Saillan-Barreau C, Cousin B, Andre M, Villena P,
Casteilla L and Penicaud L. 2003. Human adipose
cells as candidates in defense and tissue remodeling
phenomena. Biochem. Biophys. Res. Commun., 309:
502-505.
Xu H, Barnes GT, Yang Q, Tan G, Yang D, Chou CJ,
Sole J, Nichols A, Ross JA, Tartaglia LA and Chen H.
2003. Chronic inflammation in fat plays a crucial role
in the development of obesity-related insulin
resistance. J. Clin. Invest., 112: 1821-1830.
Mills KH, 2011. TLR-dependent T cell activation in
autoimmunity. Nature Rev. Immunol., 11: 807-822.
Janeway CA and Medzhitov R. 2002. Innate immune
recognition. Annu. Rev. Immunol., 20: 197-216.
Chawla A, Nguyen KD and Goh YP. 2011.
Macrophage-mediated inflammation in metabolic
disease. Nature Rev. Immunol., 11: 738-749.
Nishimura S, Manabe I, Naqasaki M, Eto K,
Yamashita, H., Ohsuqi M and Otsu M, 2009. CD8+
effector T cells contribute to macrophage recruitment
and adipose tissue inflammation in obesity. Nature
Med., 15: 914-920.
Wentworth JM, Naselli G, Brown WA, Doyle L,
Phipson B, Smyth GK, Wabitsch M, O’Brien PE and
Harrison LC. 2010. Pro-inflammatory
CD11cCCD206C adipose tissue macrophages are
associated with insulin resistance in human obesity.
Diabetes, 59: 1648-1656.
Wu L and Liu YJ. 2007. Development of dendritic-cell
lineages. Immunity, 26: 741-750.
Hashimoto D, Miller J and Merad M. 2011. Dendritic
cell and macrophage heterogeneity in vivo. Immunity,
35: 323-335.
Dominguez PM and Ardavin C. 2011. Differentiation
and function of mouse monocytederived dendritic cells
in steady state and inflammation. Immunol. Rev., 234:
90-104.
Gerhardt CC, Romero IA, Cancello R, Camoin L and
Strosberg AD. 2001. Chemokines control fat
accumulation and leptin secretion by cultured human
adipocytes. Mol. Cell Endocrinol., 175: 81-92.
Vidya et al 38

Talukdar S, Oh DY, Bandyopadhyay, G, Li D, Xu J,
McNelis J and Liu M, 2012. Neutrophils mediate
insulin resistance in mice fed a high-fat diet through
secreted elastase. Nature Med., 18: 1407-1412.
Andrade VL, Petruceli E and Belo VA. 2012.
Evaluation of plasmatic MMP-8, MMP-9, TIMP-1 and
MPO levels in obese and lean women. Clin. Biochem.,
45: 412-415.
Gleich GJ and Adolphson CR. 1986. The eosinophilic
leukocyte: structure and function. Adv Immunol.
39:177-253.
Molofsky AB, Nussbaum JC, Liang HE, Van Dyken SJ,
Cheng LE, Mohapatra A. Chawla, A. and Locksley,
R.M. 2013. Innate lymphoid type 2 cells sustain
visceral adipose tissue eosinophils and alternatively
activated macrophages. J. Exp. Med., 210: 535-549.
Wu D, Molofsky AB, Liang HE, RR Ricardo-Gonzalez,
HA Jouihan, JK Bando, A Chawla and RM Locksley,
2011. Eosinophils sustain adipose alternatively
activated macrophages associated with glucose
homeostasis. Science, 332: 243-247.
Gri G, Frossi B, D'Inca F, Betto E, Mion F, Sibilano R
and Pucillo C. 2012. Mast cell: an emerging partner in
immune interaction. Front. Immunol., 3: 120.
Xu JM, Shi GP. 2012. Emerging role of mast cells and
macrophages in cardiovascular and metabolic
diseases. Endocr. Rev., 33: 71-108.
Altintas MM, Nayer B and Walford EC, 2012. Leptin
deficiency-induced obesity affects the density of mast
cells in abdominal fat depots and lymph nodes in mice.
Lipids Health Dis., 11: 21.
Winer DA, Winer S, Shen L, Wadia PP, Paltser G,
Tsui, H. and Wu, P. 2011. B cells promote insulin
resistance through modulation of T cells and
production of pathogenic IgG antibodies. Nature Med.,
17: 610-617.
Koch, U. and Radtke, F. 2011. Mechanisms of T cell
development and transformation. Annu. Rev. Cell
Dev. Biol., 27: 539-562.
Oestreich, K.J. and Weinmann, A.S. 2012. Master
regulators or lineage-specifying. Changing views on
CD4+ T cell transcription factors. Nature Rev.
Immunol., 12: 799-804.
Feuerer, M., Herrero, L., Cipolletta, D., Naaz, A.,
Wong, J., Nayer, A., Lee, J., Goldfine, A.B., Benoist,
C. and Shoelson, S., 2009. Lean, but not obese, fat is
enriched for a unique population of regulatory T cells
that affect metabolic parameters. Nature Med., 15:
930-939.
Cipolletta, D., Feuerer, M., Li, A., Kamei, N., Lee, J.,
Shoelson, S.E., Benoist, C. and D. Mathis, 2012.
PPAR-g is a major driver of the accumulation and
phenotype of adipose tissue Treg cells. Nature, 486:
549-553.
Rausch, M.E., Weisberg, S., Vardhana, P. and
Tortoriello, D.V. 2008. Obesity in C57BL/6J mice is
characterized by adipose tissue hypoxia and cytotoxic
T-cell infiltration. Int. J. Obes., 32: 451-463.
Gumperz, JE, 2006. The ins and outs of CD1
molecules: bringing lipids under immunological
surveillance. Traffic, 7: 2-13.
Lynch L, Nowak M, Varghese B, Clark J, Hogan AE,
Toxavidis V, Balk SP, O’Shea D, O’Farrelly C and
Exley MA. 2012. Adipose tissue invariant NKT cells
protect against diet-induced obesity and metabolic
disorder through regulatory cytokine production.
Immunity, 37: 574-587.
LeBien TW and Tedder TF. 2008. B lymphocytes: how
they develop and function. Blood, 112: 1570-1580.
DeFuria J, Belkina AC, Jagannathan-Bogdan M,
Snyder-Cappione J, Carr JD, Nersesova YR,
Markham D, Strissel KJ, Watkins AA and Zhu M. 2013.
B cells promote inflammation in obesity and type 2
diabetes through regulation of T-cell function and an
inflammatory cytokine profile. PNAS, 110: 5133-5138.
Kang K., Reilly SM, Karabacak V, Gangl MR and
Fitzgerald K. 2008. Adipocyte-derived Th2 cytokines
and myeloid PPARdelta regulate macrophage
polarization and insulin sensitivity. Cell Metab., 7: 485-
495.
Dresner A, Laurent D, Marcucci M, Griffin ME and
Dufour S. 1999. Effects of free fatty acids on glucose
transport and IRS-1-associated phosphatidylinositol 3-
kinase activity. J. Clin. Invest., 103: 253-259.
Shi H, Kokoeva MV, Inouye K, Tzameli I, Yin H and
Flier JS. 2006. TLR4 links innate immunity and fatty
acid-induced insulin resistance. J. Clin. Invest., 116:
3015-3025.
Ghosh G, Wang VY, Huang DB and Fusco A. 2012.
NF-kappaB regulation: lessons from structures.
Immunol. Rev., 246: 36-58.
39 Int. Res. J. Chem.

Hotamisligil GS. 2010. Endoplasmic reticulum stress
and the inflammatory basis of metabolic disease. Cell,
140: 900-917.
Ron D and Walter P. 2007. Signal integration in the
endoplasmic reticulum unfolded protein response.
Nature Rev. Mol. Cell Biol., 8: 519-529.
Strowig T, Henao-Mejia J, Elinav E and Flavell R.
2012. Inflammasomes in health and disease. Nature,
481: 278-286.
Vandanmagsar B, Youm YH, Ravussin A, Galgani JE
and Stadler K. 2011. The NLRP3 inflammasome
instigates obesity-induced inflammation and insulin
resistance. Nature Med., 17: 179-188.
Rock KL. and Kono H. 2008. The inflammatory
response to cell death. Ann. Rev. Pathol., 3: 99–126.
Alkhouri N, Gornicka A, Berk MP, Thapaliya S and
Dixon LJ. 2010. Adipocyte apoptosis, a link between
obesity, insulin resistance, and hepatic steatosis. J.
Biol. Chem., 285: 3428-3438.
Flegal KM, Graubard BI, Williamson DF and Gail MH.
2007. Cause specific excess deaths associated with
underweight, overweight, and obesity. JAMA, 298:
2028-2037.
Hursting SD, Dunlap SM, Ford NA, Hursting MJ and
Lashinger LM. 2013. Calorie restriction and cancer
prevention: a mechanistic perspective. Cancer
Metab., 1(1):10. doi: 10.1186/2049-3002-1-10.
Calle EE and Kaaks R. 2004. Overweight, obesity and
cancer: epidemiological evidence and proposed
mechanisms. Nat. Rev. Cancer, 4: 579–591.
Harvey AE, Lashinger LM, and Hursting SD. 2011.
The growing challenge of obesity and cancer: an
inflammatory issue. Ann. N.Y. Acad. Sci. 2011, 45–52.
Booth A, Magnuson A, Fouts J and Foster M. 2015.
Adipose tissue, obesity and adipokines: role in cancer
promotion. Horm Mol Biol Clin Invest. 21: 57–74.
Rodriguez C, Freedland SJ, Deka A, Jacobs EJ,
McCullough ML, Patel AV, Thun MJ and Calle EE.
2007. Body mass index, weight change, and risk of
prostate cancer in the Cancer Prevention Study II
Nutrition Cohort. Cancer Epidemiol Biomarkers Prev.
16: 63–9.
Roberts DL, Dive C and Renehan AG. 2010. Biological
mechanisms linking obesity and cancer risk: new
perspectives. Ann Rev Med. 61: 301–16.
Dalamaga M, Diakopoulos KN and Mantzoros CS.
2012. The role of adiponectin in cancer: a review of
current evidence. Endocr Rev. 33: 547–94
Barb D, Williams CJ, Neuwirth AK and Mantzoros CS.
2007. Adiponectin in relation to malignancies: a review
of existing basic research and clinical evidence. Am J
Clin Nutr. 86: 858–66.
Taniguchi K and Karin M. 2014. IL-6 and related
cytokines as the critical lynchpins between
inflammation and cancer. Semin Immunol., 26: 54–74.
Berta J, Hoda MA, Laszlo V, Rozsas A, Garay T, Torok
S, Grusch M, Berger W, Paku S, Renyi-Vamos F,
Masri B, Tovari J, Groger M, Klepetko W, Hegedus B
and Dome B. 2014. Apelin promotes
lymphangiogenesis and lymph node metastasis.
Oncotarget. 5: 4426–37.
Vidya et al 40