Revealing humans’ sensorimotor functions with...
11
rstb.royalsocietypublishing.org Review Cite this article: Desmurget M, Sirigu A. 2015 Revealing humans’ sensorimotor functions with electrical cortical stimulation. Phil. Trans. R. Soc. B 370: 20140207. http://dx.doi.org/10.1098/rstb.2014.0207 Accepted: 13 March 2015 One contribution of 15 to a theme issue ‘Controlling brain activity to alter perception, behaviour and society’. Subject Areas: neuroscience Keywords: electrical stimulation, sensorimotor maps, somatotopy, homunculus, language, human Author for correspondence: Angela Sirigu e-mail: [email protected] Revealing humans’ sensorimotor functions with electrical cortical stimulation Michel Desmurget 1,2 and Angela Sirigu 1,2 1 Centre de Neuroscience Cognitive, CNRS, UMR 5229, 67 boulevard Pinel, Bron 69500, France 2 Universite ´ Claude Bernard, Lyon 1, 43 boulevard du 11 novembre 1918, Villeurbanne 69100, France Direct electrical stimulation (DES) of the human brain has been used by neurosurgeons for almost a century. Although this procedure serves only clini- cal purposes, it generates data that have a great scientific interest. Had DES not been employed, our comprehension of the organization of the sensorimotor systems involved in movement execution, language production, the emer- gence of action intentionality or the subjective feeling of movement awareness would have been greatly undermined. This does not mean, of course, that DES is a gold standard devoid of limitations and that other approaches are not of primary importance, including electrophysiology, modelling, neuroimaging or psychophysics in patients and healthy subjects. Rather, this indicates that the contribution of DES cannot be restricted, in humans, to the ubiquitous concepts of homunculus and somatotopy. DES is a fundamental tool in our attempt to understand the human brain because it represents a unique method for mapping sensorimotor pathways and inter- fering with the functioning of localized neural populations during the performance of well-defined behavioural tasks. 1. Electrical stimulation: a unique approach for probing brain functions One of the most important discoveries in modern neuroscience can indisputa- bly be attributed to Luigi Galvani, who showed that electrical stimulation of the sciatic nerve in a severed frog leg caused the attached muscle to contract [1]. This finding sparked a flurry of research activity that has persisted up to the present. In animals, the first systematic use of direct electrical stimulation (DES) was conducted by Gustav Fritsch and Eduard Hitzig in Germany [2] and David Ferrier in England [3]. These authors showed that stimulating the cerebral cortex of dogs and monkeys evoked topographically organized muscle contractions in the contralateral hemibody [4]. They also established that lesions of the regions from which a movement was evoked caused a deficit in the realization of this movement and even, sometimes, a total paralysis. In the following years, DES was progressively generalized to human patients with various levels of success and ethical concerns [5]. However, this technique only reached its apogee in the 1930s with the well-known work of Wilder Penfield [6]. Since then, the approach has remained roughly unchanged, beyond minor technical and procedural adaptations [7,8]. Of course, in humans, the unique raison d’e ˆtre of DES is (and has to be) clinical. If neurosurgeons now use this mapping procedure almost universally, it is with the purpose of identifying cerebral areas, resection of which could cause major functional deficits [9,10]. Consistent with this goal, it has been shown that the sur- gical use of DES dramatically reduces the occurrence of permanent post-operative sequelae in patients with brain tumours, while significantly improving long-term survival [11–15]. However, the pre-eminence of clinical goals is not inconsistent with the existence of fundamental inquiries. Obviously, the behavioural and neurophysiological observations collected in per-operative contexts can also be of major interest for fundamental research and, in particular, for understanding the organization of the human brain. & 2015 The Author(s) Published by the Royal Society. All rights reserved. on August 20, 2018 http://rstb.royalsocietypublishing.org/ Downloaded from
Transcript of Revealing humans’ sensorimotor functions with...

on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
rstb.royalsocietypublishing.org
ReviewCite this article: Desmurget M, Sirigu A.
2015 Revealing humans’ sensorimotor
functions with electrical cortical stimulation.
Phil. Trans. R. Soc. B 370: 20140207.
http://dx.doi.org/10.1098/rstb.2014.0207
Accepted: 13 March 2015
One contribution of 15 to a theme issue
‘Controlling brain activity to alter perception,
behaviour and society’.
Subject Areas:neuroscience
Keywords:electrical stimulation, sensorimotor maps,
somatotopy, homunculus, language, human
Author for correspondence:Angela Sirigu
e-mail: [email protected]
& 2015 The Author(s) Published by the Royal Society. All rights reserved.
Revealing humans’ sensorimotor functionswith electrical cortical stimulation
Michel Desmurget1,2 and Angela Sirigu1,2
1Centre de Neuroscience Cognitive, CNRS, UMR 5229, 67 boulevard Pinel, Bron 69500, France2Universite Claude Bernard, Lyon 1, 43 boulevard du 11 novembre 1918, Villeurbanne 69100, France
Direct electrical stimulation (DES) of the human brain has been used by
neurosurgeons for almost a century. Although this procedure serves only clini-
cal purposes, it generates data that have a great scientific interest. Had DES not
been employed, our comprehension of the organization of the sensorimotor
systems involved in movement execution, language production, the emer-
gence of action intentionality or the subjective feeling of movement
awareness would have been greatly undermined. This does not mean, of
course, that DES is a gold standard devoid of limitations and that other
approaches are not of primary importance, including electrophysiology,
modelling, neuroimaging or psychophysics in patients and healthy subjects.
Rather, this indicates that the contribution of DES cannot be restricted, in
humans, to the ubiquitous concepts of homunculus and somatotopy. DES is
a fundamental tool in our attempt to understand the human brain because it
represents a unique method for mapping sensorimotor pathways and inter-
fering with the functioning of localized neural populations during the
performance of well-defined behavioural tasks.
1. Electrical stimulation: a unique approach for probing brainfunctions
One of the most important discoveries in modern neuroscience can indisputa-
bly be attributed to Luigi Galvani, who showed that electrical stimulation of
the sciatic nerve in a severed frog leg caused the attached muscle to contract
[1]. This finding sparked a flurry of research activity that has persisted up to
the present. In animals, the first systematic use of direct electrical stimulation
(DES) was conducted by Gustav Fritsch and Eduard Hitzig in Germany [2]
and David Ferrier in England [3]. These authors showed that stimulating the
cerebral cortex of dogs and monkeys evoked topographically organized
muscle contractions in the contralateral hemibody [4]. They also established
that lesions of the regions from which a movement was evoked caused a deficit
in the realization of this movement and even, sometimes, a total paralysis. In
the following years, DES was progressively generalized to human patients
with various levels of success and ethical concerns [5]. However, this technique
only reached its apogee in the 1930s with the well-known work of Wilder
Penfield [6]. Since then, the approach has remained roughly unchanged,
beyond minor technical and procedural adaptations [7,8].
Of course, in humans, the unique raison d’etre of DES is (and has to be) clinical.
If neurosurgeons now use this mapping procedure almost universally, it is with
the purpose of identifying cerebral areas, resection of which could cause major
functional deficits [9,10]. Consistent with this goal, it has been shown that the sur-
gical use of DES dramatically reduces the occurrence of permanent post-operative
sequelae in patients with brain tumours, while significantly improving long-term
survival [11–15]. However, the pre-eminence of clinical goals is not inconsistent
with the existence of fundamental inquiries. Obviously, the behavioural and
neurophysiological observations collected in per-operative contexts can also be
of major interest for fundamental research and, in particular, for understanding
the organization of the human brain.

rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
2
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
Certainly, this does not mean that DES is devoid of
limitations. In particular, the range of questions it allows us
to address is strongly restricted by clinical demands and per-
operative constraints. This is why the results obtained with
this technique have to be interpreted in light of a more general
knowledge, generated by other approaches [16]. Consider, for
instance, neuroimaging (functional magnetic resonnance ima-
ging—fMRI, positron emission tomography—PET) and
electrophysiology (electro and magneto encephalography—
EEG, MEG). During the past three decades these methods
have obviously played a major role in improving our under-
standing of the sensorimotor organization of the human
brain. However, it should not be forgotten that they too bear
important limitations [17–19]. In particular, they do not
allow us to neatly determine whether a responsive area is
truly critical for the expression of an investigated function
and whether an activated region receives afferent information,
sends efferent signals to the muscles or subserves compu-
tational processing. DES opens a window to this type of
knowledge. Of course, nobody would seriously argue that
this technique recruits neural populations as autogenous pro-
cesses do. It should be evident that DES produces unnatural
patterns of cellular activation. However, such a limitation
does not, by any means, call into question the usefulness of
the method. Indeed, even if it relies on unnatural patterns of
neural activation, DES remains unparalleled in its ability to:
(i) drive descending pathways for identifying cortical regions
with outputs to motoneurons (e.g. [6,20]); (ii) elicit positive sen-
sorimotor effects through the recruitment of neural populations
associated with the expression of high- (e.g. motor intention;
e.g. [21,22]) or low-level (e.g. sensory feelings; e.g. [6,20]) func-
tions; (iii), elicit negative sensorimotor effects through
disruption of an endogenous neural activity involved in the
realization of an ongoing task (whether motor or cognitive;
e.g. [23,24]). It is true that interpretative biases related to a poss-
ible spread of the electrical current have always been a subject
of concern for researchers [25,26]. However, during the past
two decades solid evidence has been gathered, at least for the
high-intensity/high-frequency stimulation parameters typically
used in surgical protocols, that DES effects are typically
mediated by the cell population being stimulated [27–29]. In
other words, DES does not spread in a meaningless jumble.
It operates primarily at a local level and, doing so, offers an
invaluable way to investigate the anatomo-functional organiz-
ation of the human brain. Among the multiple elements
supporting this conclusion (see [27,28] for detailed reviews),
the most convincing evidence comes probably from the suc-
cessful use of DES for mapping brain functions in per-
operative contexts. If, as is sometimes claimed [26], DES effects
were reflective of an artificial spread of current at distant sites,
then this method should be ineffective at preventing post-oper-
ative deficits in neurosurgical contexts. As reported above, this
is clearly not what the clinical literature demonstrates [11–15].
This being said, in the present review, we will focus on the
specificity and fundamental importance of DES. At a first
level, we intend to show that if this technique had not been
exploited in the past decades, several of our pillar concepts
and much of our knowledge on the anatomo-functional
organization of the sensorimotor system would be dramati-
cally undermined. At a second level, we plan to emphasize
recent studies and technical developments to demonstrate
that DES remains a major approach for understanding
brain functions.
2. Mapping the sensorimotor systemAt a time when the theory of brain localization was still
strongly questioned [30,31], Penfield’s work proved ground
breaking. As is the rule (see above), this neurosurgeon used
DES for clinical reasons ‘to define the motor area of the hemi-
sphere so that an infiltrating tumour could be removed as
widely as possible without producing paralysis [and. . .] as a
preliminary to radical extirpation of an epileptogenic focus’
[6, p. 396]. However, using this approach he also reported
results of great fundamental interest. In particular, he was
the first to show, in humans, that functional specialization
existed not only across brain areas, but also within them.
In his main pioneering work, Penfield used DES in 163
patients, among whom 126 provided useful results [6]. He
observed that movements could be triggered from only a lim-
ited number of cortical regions, including the primary motor
cortex (M1), the primary somatosensory cortex (S1), the pre-
motor cortex (PM) and the supplementary motor area (SMA).
Sensations were mostly evoked from the same regions. It is
unclear, however, whether stimulations (and how many)
were performed in non-central regions including the prefrontal
or posterior parietal cortices. Penfield found that more move-
ments were triggered from the precentral gyrus, while more
body sensations were evoked from the post-central gyrus,
although sensory and motor responses were identified in
both of these two regions. He also reported that different corti-
cal loci triggered movements and sensations in different body
parts. These observations led to the key idea that sensorimotor
regions are somatotopically organized in such a way that each
part of the body is represented within a different cortical space
in the pre- and post-central gyri. To formalize this finding, Pen-
field introduced the now famous concept of the homunculus.
According to him, within the central area, ‘toes begin at the
top and the members follow in order as though representing
a man hung upside down, but that thumb is followed by the
head as though the head and neck were erect and not inverted
(. . .) The homunculus may be said to be both motor and sen-
sory as the sequence pattern is roughly the same, although
there are differences’ [6, pp. 431–432]. Most major biology text-
books still mention Penfield’s idea and display a version of his
drawing of the human homunculus (e.g. [32,33]).
The idea that M1 and S1 are somatotopically organized is
probably one of the very few proposals that have withstood
the test of time in modern neuroscience. The concept of
the homunculus has seen its general validity supported by
numerous neuroimaging and electrophysiological studies in
humans [34–41]. However, recent evidence has started to
suggest that this consensus may rely, when carefully con-
sidered, on a rather weak ground [42–45]. According to this
view, the concept of the homunculus would mainly be an
emerging artefact of inter-individual averaging. It would
have no validity at the intra-individual level, where major
organizational differences are observed. In other words, the
homunculus as we know it would not represent a biological rea-
lity but rather a statistical construct that ‘does not appear to
exist’ [44, p. 292]. The same kind of criticism has been raised
with respect to neuroimaging data which ‘can produce the illu-
sion of a localized process by emphasizing fortuitous regions of
overlap to the exclusion of the more widely distributed active
regions in the individual subjects’ [46, p. 197].
Clearly, these claims are consistent with the observa-
tion that the synoptic, regularly ordered sequence of body

rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
3
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
movements and sensations described by Penfield on the basis
of the responses he recorded [6] is almost never observed at
the individual level. Although initial evidence came from
electrophysiological studies in monkeys [47–49], recent data
have confirmed that this is also true in humans, where
sensory and motor maps are typically organized as an inter-
mingled mosaic of neural populations related to different
body parts [43,44,50,51]. Major violations of Penfield’s
regular ordering are commonly found. It happens, for
instance, that mouth and face responses are represented
above finger or leg responses [43]. Moreover, both monkeys
[52] and humans [44] exhibit large variations of the sensori-
motor cortical organization from individual to individual
and between hemispheres. More generally, recent data have
also suggested that the functional segregation between M1
and S1 might not be as strict as initially postulated by
Penfield [53]. In humans, in particular, it was found that
the hand ‘hot spot’, defined as the cortical area that evokes
hand or finger responses at the lowest electrical intensity,
was located in the post-central gyrus in a significant fraction
of subjects [54,55]. At a first level, this puzzling result high-
lights the necessity of considering Penfield’s anatomical
maps with caution. Indeed, 100 years ago, neuronavigation
tools were not available and localizing stimulation sites
was not easy. For instance, as acknowledged by Penfield &
Boldrey, there was a strong bias toward associating motor
response with M1 stimulation because ‘the Rolandic fissure
can hardly be recognized until after stimulation has identified
it’ [6, p. 398]. However, the idea that the hand hot spot
is commonly localized in S1 was recently contradicted by
clinical observations showing, in a large population of 165
patients, that motor responses were scarcely evoked from
the post-central gyrus [20]. This conclusion is consistent
with monkey data showing that the level of current required
to trigger overt movements is almost systematically lower in
M1 than S1 [56,57]. In fact, as shown by a study aiming at
comparing the output properties of these two regions, the
motor responses evoked from S1 are rare, weak and often
inhibitory [58]. Strikingly, in monkey experiments, the lowest
motor threshold is consistently identified in regions located
within the bank of the central sulcus for both M1 (Brodmann
area 4) and S1 (Brodmann area 3a). In humans, however,
these intrasulcal areas are not accessible and DES is only per-
formed over the convexity of the pre- and post-central gyri.
Together with the limited number of sites that can be stimu-
lated in each subject, this may explain why the hand hotspot
has sometimes been reported in S1 in humans.
The recent questioning of Penfield’s homunculus does not
seem surprising. In truth, what appears to be really puzzling
is the ubiquity of this schematic representation and how it
became so universally accepted. Indeed, looking at Penfield’s
own data, it seems quite clear that the nice arrangement of
body parts he described along the pre- and post-central gyri
is functionally deceitful, although, of course, graphically con-
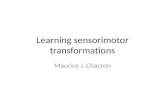
venient. This can be seen in figure 1 for a few representative
examples. The left side of the three first panels (figure 1a–c)
shows the individual stimulation sites identified as eloquent
by Penfield [6]. The right side displays the classical homunculus
he constructed from these data.
Figure 1a investigates the claim that an ordered somato-
topy exist for the fingers. Really, considering the actual
stimulation data, it seems hard to see any justification for
this hypothesis. Thumb contractions (coloured in blue), for
instance, are observed along the whole extent of the central
sulcus; they are not clustered in the medio-lateral region
and do not appear to be consistently medial with respect to
the responses recorded for other fingers, including the little
one (coloured in red). In fact, rather than observing indepen-
dent contractions for each finger, Penfield reported, in most
cases, motor responses that involved all fingers together
without individual segregation (black dots). Recently, this
combined activation has been reproduced in monkeys,
where microstimulation was found to trigger organized pat-
terns of finger synergies [60]. Also, data gathered in these
animals have clearly challenged the idea of a sequential rep-
resentation of each individual finger along a medio-lateral
axis going from the little finger to the thumb [49,61].
Figure 1b displays, on the same plot, upper limb (shoulder,
elbow, wrist, hand, undissociated by Penfield, coloured in red)
and finger responses (coloured in blue). Eloquent sites for these
two segments exhibit a major level of overlap and redundancy.
It is hard to figure out how Penfield went from these inter-
mingled responses to the nice sequential ordering presented
on the right panel, where upper limb representations are
located more medially than finger representations.
Data from the third panel (figure 1c) are even more dis-
concerting. They show face and neck representations.
Placing the neck above the face from these recordings really
seems questionable considering that all neck responses
except one are represented more laterally than face responses.
From a scientific point of view, the logic that led Penfield
to identify a precisely ordered homunculus on the basis of
his scattered data is hard to infer. However, a plausible
hypothesis might be that he got, at some point, the idea
of an inverted body map lined up over the cortical surface.
This map, drawn by Penfield himself in his pioneering work
[6], is shown on figure 1d. It implies, for instance, that the
neck should be represented more medially than the face.
Based on these remarks, it is tempting to speculate that
Penfield did not go from the data to the model, but was
rather biased toward forcing his clinical observations into
a predetermined map of representations.
In summary, DES has been a key approach for understand-
ing the organization of the primary sensorimotor regions. The
early work of Wilder Penfield, in particular, proved fundamen-
tal for establishing the central idea that brain functions are
localized and that the sensorimotor system is organized
somatotopically in such a way that specific cortical sites control
specific muscles. Nevertheless, Penfield also went too far in his
attempt to describe a nicely ordered map of sensorimotor
representations within the central regions. Both recent results
[42–44,50] and a re-evaluation of his original observations
show that sensorimotor representations are not organized in
a sequential rigidly ordered way, but rather in a mosaic of inter-
mingled representations where body parts overlap in multiple
non-contiguous areas. Such a fractured arrangement (a term
coined by Welker and his co-workers for describing the
somatosensory organization of the cerebellum [62]) has been
claimed to favour the production of complex motor responses
by making it easier to combine elemental body movements
within coordinated muscle synergies [59,61,63–65].
3. Mapping complex sensorimotor synergiesFrom the data above, it appears that DES typically evokes
simple meaningless movements in humans. Nevertheless,

thum
bin
dex
mid
dle
ring
little
all
diff
eren
t dig
its
neck
ver
sus
face
digi
ts v
ersu
s ar
m
Penf
ield
’s h
omun
culu
s
arm
digi
ts
neck
face
(a)
(b)
(c)
(d)
Figu
re1.
The
nice
lyor
dere
dho
mun
culu
sco
nstru
cted
byPe
nfiel
dis
notc
onsis
tent
with
the
indi
vidua
ldat
aac
tuall
yco
llecte
dby
this
neur
osur
geon
.(a)
(Lef
tpar
t.)Ev
oked
resp
onse
sid
entif
iedby
Penf
ield
fort
hedi
ffere
ntdi
gits;
(righ
tpar
t)co
rresp
ondi
ngho
mun
culu
s.(b
)(Le
ftpa
rt.)E
voke
dre
spon
ses
iden
tified
byPe
nfiel
dwe
rere
porte
don
the
sam
egr
aph
fort
hear
m(in
cludi
ngsh
ould
er,e
lbow
,wris
t,ha
nd;r
edco
lour
)an
dth
edi
gits
(blu
eco
lour
);(ri
ghts
ide)
corre
spon
ding
hom
uncu
lus.
(c)(L
eftp
art.)
Evok
edre
spon
sesi
dent
ified
byPe
nfiel
dwe
rere
porte
don
the
sam
egr
aph
fort
hefac
e(g
reen
colo
ur)a
ndth
ene
ck(re
dco
lour
);(ri
ghts
ide)
corre
spon
ding
hom
uncu
lus.
(d)(
Left
part.
)Pen
field
’sid
eaof
anin
verte
dho
mun
culu
s;(ri
ghts
ide)
corre
spon
ding
form
aliza
tion
ofth
isid
ea.A
dapt
edfro
m[6
,59]
,with
perm
ission
.
rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
4
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from

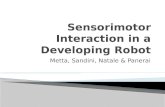
complex motor synergies in monkeys
reach-to-grasp
climbing/leaping
hand inlower space
manipulate in central space
defense
hand to mouth
chewing/licking
hand/mouth synergies in humans
hand-to-mouth movements
perioral exploration
(a) (b)
Figure 2. (a) Action zones in the precentral gyrus of the monkey where complex movements are evoked in response to long-train electrical stimulations (adaptedfrom [65], with permission). (b) Sites where complex hand/mouth synergies are evoked by electrical stimulation in the human precentral gyrus. The top panel of thefigure displays motor sites (black squares) evoking hand-to-mouth synergies resembling self-feeding, in which DES causes the closing hand to progressively approachthe opening mouth. The bottom panel of the figure displays multimodal sites (black squares) that evoke hand/arm actions when stimulated while receiving mouthsensory inputs. Adapted from [69], with permission.
rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
5
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
following cortical stimulation some studies have reported the
development of relatively complex, apparently purposeful
actions, including joint hand–mouth responses, coordinated
arm–eye–head aversive synergies and organized reach-to-
grasp gestures [6,22,43,66,67]. Unfortunately, when observed,
these movements were generally not described in detail.
Also, they were often said to be artefactual and reflective of
the unspecific recruitment, through current spread, of body
parts having contiguous cortical representations [43].
Technically, a reason why complex movements have not
been more commonly observed in response to DES could be
related to the tendency of clinicians (in humans) and exper-
imenters (in animals) to use short trains of stimulations.
As noted by Penfield & Welch [67, p. 310], for instance, it is
plausible that some of the simple motor responses they
found in their patients ‘would, with more prolonged stimu-
lations, have gone on to become more elaborate and to have
approached the full synergic employment of all extremities
and the trunk. The stimulating electrode has frequently been
removed at the first evidence of response, and thus the oppor-
tunity of producing more of the elaborate synergic responses
may have been missed’. Michael Graziano et al. were the first
to investigate this possibility in awake macaque monkeys
[68]. These authors stimulated the precentral gyrus using
stimulation trains of long duration. They found that some
motor responses that would have had the form of simple
muscle twitches in the context of short train stimulations,
unfolded into complex coordinated actions when the duration
of the stimulation lasted long enough. These actions included,
for instance, self-feeding movements in which the hand closed
into a grip while moving toward the opening mouth; reach-to-
grasp synergies in which the arm extended while the fingers
opened progressively; defensive gestures in which the facial
muscles squinted while the head turned sharply to one
side and the arm flung up; etc. Interestingly, as shown in
figure 2a, each of these categories of action was evoked from
different, well-localized, zones of the precentral gyrus.
Recently, Graziano’s pioneering observations were repro-
duced in New World monkeys and prosimian galagos by
John Kaas and his co-workers [70,71]. Also, they were gener-
alized to human subjects in a study aiming to investigate
whether hand–mouth synergies, a prominent example of
human behaviour with high ethological value, were rep-
resented as motor primitives in the precentral gyrus [69]. In
this study, electromyographic activity evoked by cortical
stimulation was recorded from the face and upper-limb
muscles in patients undergoing brain surgery. As shown in
figure 2b (top panel), this allowed identification of an inte-
grated motor primitive resembling self-feeding, in which
DES caused the closing hand to progressively approach the
opening mouth. Of course, not all responses evoked by
long train stimulations evolved into complex movements
and coordinated hand–mouth synergies intermingled with
simpler isolated movements over the whole surface of the
precentral gyrus. This anatomical dispersion contrasted
with the more clustered pattern found in monkeys (figure
2b). Two main hypotheses may account for this difference.
First, it is possible that this cortical region is differently orga-
nized in humans and monkeys [72,73]. Second, the
pioneering data reported by Graziano et al. in monkeys [68]
could be biased toward intra-individual variability (multiple
replications in few animals), while the data gathered in
humans could be rather slanted toward inter-individual
variability (few replications in multiple subjects).

rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
6
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
Notably, the true ethological nature of the complex syner-
gies evoked through DES was recently questioned by Cheney
and colleagues. In monkeys, these authors provided evidence
that postural synergies evoked through cortical stimulation
were not produced by natural patterns of EMG activity but
instead resulted from an unnatural co-contraction of numerous
‘hijacked’ muscles that forced the limb to an equilibrium point
[74,75]. However, the generality of these observations remains
debatable for at least three reasons. First, muscle hijacking was
not observed in several studies where evoked-EMG and kin-
ematic responses were found to be strikingly similar to the
responses seen in natural behaviours [60,68,76]. Second, the
non-teleonomic nature of the ‘hijacking’ hypothesis seems
hardly compatible with the repeated failure of DES to evoke
non-functional synergies where, for instance, the opening
hand would approach the closing mouth or the closing hand
would move away from the opening mouth [68,69]. Third,
beyond its ability to explain the emergence of postural equili-
bria, the ‘hijacking’ model cannot easily account for the
finesse and high functional specificity of some very complex
multi-segmental synergies. This includes, for instance, multi-
joint defensive postures specifically triggered from bimodal
neurons with tactile/visual receptive fields and made of the
following complementary elements (in Graziano’s terms): ‘a
facial grimmace, a squinting of the eye, a turning of the head
away from the side of the sensory receptive fields, a hunching
of the shoulders, a fast thrusting of the hand into the space
beside the head, and a turning of the hand such that the
palm faced outward, away from the head’ (fig. 4 in [77]).
Beyond these observations, it may be worth noting that
motor responses involving the coordinated recruitment of
distinct body segments were not the only type of complex
representation identified in the human precentral gyrus. Com-
bined recording of motor and somatosensory evoked potentials
revealed that this region also harbours motor-sensory represen-
tations where cross-signal integration is realized at specific
cortical sites that generate hand/arm actions while receiving
mouth sensory inputs. It is tempting to speculate that these
multimodal sites underlie the behavioural process of perioral
exploration. Indeed, they are shaped as a hardwired feedback
loop capable of binding oral sensory inputs with upper limb
motor commands or, in other words, capable of guiding hand
movements according to mouth sensations. This view is consist-
ent with a recent study on upper-limb reaching movements
showing, in humans and monkeys, that M1 contains fast feed-
back control loops integrating sensory and motor signals [78].
As shown in figure 2b (lower panel), complex hand–mouth sen-
sorimotor sites are not evenly distributed over the precentral
surface of the patients. They are clustered in the dorsal sector of
the precentral gyrus, where hand/arm movements are most
commonly represented.
In summary, using long trains of stimulation, researchers
and clinicians have provided convincing (although still
disputed) evidence that specific sensorimotor synergies with
a high ethological value are represented as integrated motor
primitives in the precentral gyrus. This cortical region cannot
be seen any more as a sort of keyboard, where segregated
populations of neurons can be recruited in a specific spatio-
temporal order to form complex symphonies of movements.
Overall, the use of DES reveals the complexity of primary
sensorimotor structures that can probably accommodate differ-
ent types of representations with various levels of complexity
[79]. This hypothesis fits well with the suggestion that
sensorimotor organization has been shaped by primate evol-
ution to optimize the production of ethologically relevant
behaviours while preserving the ability to learn new complex
synergies [64,65,70].
4. Mapping high-level functionsPer-operative mapping is not only useful for identifying brain
areas that evoke movements or sensations when stimulated.
This approach can also be used for probing the functional con-
tribution of a given cortical region. In this case, DES is applied
while the subject is performing a sensorimotor task such as
opening–closing the hand, reading or counting. The effect of
the stimulation on the ongoing behaviour is then evaluated.
In an alternative approach, the neurosurgeon can also interfere
with brain activity at rest and ask the patients to report the
thoughts or feelings they have experienced in response to
the stimulation.
To date, per-operative evaluations of high-level functions
have been mainly conducted for language mapping in awake
patients [80–83]. Based on this approach, large amounts of
data have been collected and used for producing probabilistic
maps of anatomo-functional correlations [13,20]. In other
words, using DES in large populations of patients, neurosur-
gical teams were able to associate specific cortical regions
with particular language disorders such as speech arrest
(cessation of speech output in the absence of evoked motor
response); dysarthria (improper articulation of speech);
anomia (inability to name objects while still being able to
speak or repeat sentences); alexia (inability to read while
still being able to spell words or write); receptive aphasia
(fluent but meaningless speech and inability to understand
simple sentences); expressive aphasia (impaired speech
production); etc.
Together with neuroimaging and lesion observations, these
per-operative results proved of major interest for improving
our understanding of the neural bases of language com-
prehension and production [84–88]. A striking example
concerns Broca’s area, the long-postulated role of which as a
speech output region remains debated in neuroimaging and
lesion studies [89–92]. A recent per-operative investigation
involving 165 patients provides an important, potentially deci-
sive, contribution to this issue [20]. As reported by the authors,
stimulation of Broca’s area only produces speech arrest in 4% of
the subjects, compared with 83% when the dorsal premotor
cortex (dPM) is targeted. The latter proportion is independent
of the localization of the tumour, i.e. of whether Broca’s area is
lesioned or not. Based on these results, it is tempting to suggest
that Broca’s area should no longer be considered a motor
region coordinating speech articulation but should rather be
viewed as a cognitive structure involved in high-level functions
such as verbal working memory, language comprehension or
lexical retrieval [20,93].
However, in the linguistic domain, the identification of
well-defined anatomo-functional correlations in response to
DES does not seem to be the norm. Indeed, a very striking
feature of per-operative evaluations of language abilities lies
in the wide distribution of functional sites across brain struc-
tures (figure 3). In contrast to the relatively circumscribed
networks that sometimes emerge from careful syntheses of
the lesion and neuroimaging literature (e.g. [90,94–96]), it
appears that highly specific aspects of language production

cortical sites for speech arrest [13] cortical sites for anomia [13]
cortical sites for alexia [13] cortical sites for speech arrest and anomia [20]
(a) (b)
(c) (d)
Figure 3. Language maps indicating, for the (left) dominant hemisphere, the cortical locations where DES induced speech dysfunctions in two large studies invol-ving, respectively, 250 [13] and 165 [20] consecutive patients with gliomas. (a) Brain sites inducing speech arrest per square centimetre of the cortical surface(reconstructed from [13]). (b) Brain sites inducing anomia per square centimetre of the cortical surface (reconstructed from [13]). (c) Brain sites inducingalexia per square centimetre of the cortical surface (reconstructed from [13]). (d ) Brain sites inducing speech arrest (red circles) and anomia (blue circles).Each individual circle represents a positive observation. Adapted from [20], with permission.
rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
7
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
can be impaired through stimulations delivered over very
different cortical zones. Anomia or alexia, for instance, is
consistently found after stimulation of wide (sometimes over-
lapping) regions in the frontal, temporal and parietal cortices
(figure 3). This high level of scattering is not totally surpris-
ing. It can have two main origins. On the one hand, it may
mirror the multiplicity of the neural processing required for
naming an object or reading a word [90]. On the other
hand, it may also reflect the existence of a tremendous level
of inter-individual variability in the localization of language
functional sites [13]. Obviously, part of this variability is
owing to the plastic changes that occur in brain organization
in response to slow-growing tumoural invasion [97].
Together with the existence of substantial differences in the
tasks being evaluated [98], these changes could explain
some of the above-mentioned discrepancies between DES,
acute lesion and neuroimaging studies.
This being said, language is far from being the only
high-level function open to per-operative evaluation [99].
Recently, this approach has been used to study, for instance,
visuo-spatial processing [100], action inhibition [23], move-
ment awareness [101,102] and sensorimotor intentionality
[103,104]. While reviewing the contribution made by DES
to all these fields would be beyond the scope of the present
paper, a brief focus on sensorimotor awareness and intention-
ality should help us provide another example of the unique
fruitfulness of this method.
Technically, sensorimotor intentionality has been very
difficult to address with classical electrophysiological, clinical
and neuroimaging tools given, in particular, the difficulty of
separating intentional and attentional processing [105,106].
Fortunately, DES does not have to deal with this ambiguity.
This was first shown by Penfield, who reported that some
frontal sites evoked a desire to move when stimulated [6].
Subsequent studies were able to confirm this observation,
but located the neural source of this desire on the frontal
medial wall, in a region encompassing the supplementary
and cingulate motor areas [22,107,108]. During stimulation,
the subjective experiences of the patients were characterized
by an uncontrollable urge to act. For instance, an epileptic
woman stimulated in the anterior cingulate sulcus at low
intensity through implanted intracerebral electrodes exhib-
ited ‘an irresistible urge to grasp something, resulting in
exploratory eye movements scanning both sides of the
visual field, and accompanied by a wandering arm move-
ment contralateral to the stimulation side. Then, after the
patient had visually localised a potential target, her left
hand moved towards the object to grasp it, as if mimicking
a spontaneous movement. This irrepressible need started
and ended with stimulation, and the patient was unable to
control it. Yet, the patient was aware of both her inability
to resist and of the movement she thus performed and
could describe very precisely’ [107, p. 265]. The same type
of urge was observed in another study, still in epileptic

rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
8
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
patients. In this case, however, the stimulation was located in
the supplementary motor area. This caused the participants
to experience an ‘urge to move the right leg inward’, an
‘urge to move the right thumb and finger’ or an ‘urge to
move the right arm away’ [22, p. 3661]. Although no movement
was evoked in response to these subjective feelings, overt
motor responses were observed when the intensity of the
stimulation was raised. For instance, a patient who reported
a ‘strong urge to raise the right elbow’ at 5 mA, experienced
a right-arm abduction at 6 mA [22, p. 3661].
Interestingly, the frontal medial wall is not the only cortical
area where intentional responses can be evoked. The emer-
gence of a subjective desire to move was also reported
following stimulation of the inferior parietal lobule [21]. In
this case, however, the subjective feelings reported by the sub-
jects were quite different from the ones observed after
stimulation of the supplementary and cingulate motor areas.
There was no dimension of urge or irrepressibility. Also, the
patients were unable to precisely describe the movements
they wanted to perform. When prompted to try, they either
said that they did not know or provided a very general descrip-
tion of their intentions in terms of action class. Representative
exchanges were as follows ([21]; electronic supplementary
material): (1) (Experimenter) Did you feel something? ; (Patient)Yes. . . It felt like I wanted to move my foot. Not sure how to explain;(E) Which foot? (P; showing the left leg): This one. (E) How did youwant to move it? ; (P): I don’t know, I just wanted to move it ; (2) (E)
Did you feel something? ; (P) I had a desire to do something ; (show-ing her chest) Here I have a desire to do. . . (E) In the chest? (P) Yes ;(E) And what did you feel? ; (P) Like a, like a will to move.
Another striking specificity of the parietal intentional sites
lies in the absence of motor response when the intensity of
the stimulation was increased. When a higher current was
used, the patients experienced illusory movements; they felt
that the movements they wanted to make at low intensity
had actually occurred in the absence of any overt or electro-
myographic motor response. A representative exchange was
as follows ([21]; electronic supplementary material). (5 mA)
(Experimenter) Did you move?; (Patient) No. I had a desire toroll my tongue. . . ; (E) To roll what? ; (P) To roll my tongue inmy mouth. (8 mA, same site) (E) Did you move? ; (P) Yes, yes,a corner of the mouth ; (E) Did you move the mouth? ; (P) Yes.
To account for this phenomenon, it was hypothesized that
higher currents did not simply prime a motor representation
to consciousness (giving rise to motor intention), but also
recruited the executive network responsible for movement
monitoring through forward modelling, a process that is
known to rely on posterior parietal computations [109,110].
In sharp contrast to the illusory movements evoked
through parietal stimulation, it was also found that actual
motor responses evoked by stimulating the dPM were not
consciously perceived by the patients. In other words,
although overt mouth and contralateral limb movements
were observed following stimulation of this region, the patients
firmly denied that they had moved [21]. This result highlights
clinical data showing that dPM is the most commonly lesioned
region in hemiplegic patients with anosognosia [111]. It also
echoes neuroimaging observations showing that the dPM is
important for comparing the actual and expected sensory sig-
nals [112]. It is tempting to speculate that when dPM is
prevented from performing its function, no error signal is gen-
erated in response to an unexpected muscle contraction, which
causes the ongoing movement to remain undetected [101].
Putting these observations together, a general model of
linking conscious motor intention and movement awareness
could be proposed that takes into account the functional
specificity of the parietal and frontal intentional regions
[103,104]. In brief, it was suggested that a general, unspecific
intention to act first emerges into consciousness within the
inferior parietal lobule. This intention is the neural signal
that triggers actual motor preparation. While the movement
is being planned, the cingulate and supplementary motor
regions exert inhibitory control over the motor output
regions. This is done to prevent an early, unwanted, release
of the motor command. Once the movement is ready, this
proactive inhibition is waived, which amounts to the emis-
sion of a ‘go’ signal that gives rise to a compulsive urge to
act. After movement onset, parietal control mechanisms
monitor action progression independently of sensory
inputs, through forward modelling. When an error is
detected that cannot be corrected through online control pro-
cesses (e.g. the arm does not move when it should), dPM
emits a warning signal that reaches consciousness. Of
course, this model is not only based on the outcomes of
DES studies but also on a large array of clinical, neuroima-
ging and electrophysiological data. However, DES was a
key method through which the material generated by each
of these approaches could be interpreted and aggregated [16].
5. Concluding remarksTo summarize, the data above show that DES has provided
a unique body of knowledge since its pioneering use by
Wilder Penfield, in humans, almost a century ago [6]. Had
this technique not been employed, our comprehension of
the organization of the sensorimotor systems involved in
movement execution, language production, the emergence
of action intentionality or the subjective feeling of movement
awareness would have been greatly undermined. This is not
to say, of course, that DES is a gold standard devoid
of limitations, nor to deny the major importance of other
clinical, eletrophysiological, modelling or neuroimaging
approaches [27]. This just means that DES represents a
unique way to map sensorimotor pathways and interfere
with the functioning of localized neural populations during
the performance of well-defined behavioural tasks. Recent
advances suggest that there is still a lot to learn from this
technique. In particular, many structures remain to be care-
fully investigated including, for instance, the cerebellum
[113]. Also, cortico-cortical connectivity continues to be a dif-
ficult challenge that DES could help to address in humans
[114,115]. Finally, the use of probabilistic maps taking into
account inter-individual variability to link structures and
functions will allow a better targeting, during per-operative
evaluations, of the functions that are at risk for a given
lesion. Such a ‘tailored’ approach will favour the develop-
ment of finer evaluation protocols and lead, potentially, to
a much better comprehension of the functional fine-grained
organization of the brain.
Authors’ contributions. Both authors contributed equally to the redactionof this review paper.
Competing interests. We declare we have no competing interests.
Funding. This work was funded by CNRS, the ‘Cortex’ Labex Programand the Agence Nationale de la Recherche (ANR-11BSV40271; ANR-12-BSV4001801) to A.S. and M.D.

9
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
References
rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
1. Galvani L. 1791 De viribus electricitatis in motumusculari commentarius. Bononiensi Sci. ArtiumInst. Acad. 7, 363 – 418.
2. Fritsch G, Hitzig E. 1870 Uber die elektrischeErregbarkeit des Grosshirns. Arch. Anat. Physiol.Wiss. Med. 37, 300 – 332.
3. Ferrier D. 1876 Functions of the brain. New York,NY: Putnam.
4. Taylor CS, Gross CG. 2003 Twitches versusmovements: a story of motor cortex.Neuroscientist 9, 332 – 342. (doi:10.1177/1073858403257037)
5. Zago S, Ferrucci R, Fregni F, Priori A. 2008Bartholow, Sciamanna, Alberti: pioneers in theelectrical stimulation of the exposed humancerebral cortex. Neuroscientist 14, 521 – 528.(doi:10.1177/1073858407311101)
6. Penfield W, Boldrey E. 1937 Somatic motor andsensory representation in the cerebral cortex ofman as studied by electrical stimulation. Brain60, 389 – 443. (doi:10.1093/brain/60.4.389)
7. Berger MS, Ojemann GA. 1992 Intraoperative brainmapping techniques in neuro-oncology. Stereotact.Funct. Neurosurg. 58, 153 – 161. (doi:10.1159/000098989)
8. Szelenyi A, Bello L, Duffau H, Fava E, Feigl GC,Galanda M, Neuloh G, Signorelli F, Sala F. 2010Intraoperative electrical stimulation in awakecraniotomy: methodological aspects of currentpractice. Neurosurg. Focus 28, E7. (doi:10.3171/2009.12.FOCUS09237)
9. Duffau H. 2005 Lessons from brain mapping insurgery for low-grade glioma: insights intoassociations between tumour and brain plasticity.Lancet Neurol. 4, 476 – 486. (doi:10.1016/S1474-4422(05)70140-X)
10. Sanai N, Berger MS. 2010 Intraoperative stimulationtechniques for functional pathway preservation andglioma resection. Neurosurg. Focus 28, E1. (doi:10.3171/2009.12.FOCUS09266)
11. Duffau H, Lopes M, Arthuis F, Bitar A, Sichez JP, VanEffenterre R, Capelle L. 2005 Contribution ofintraoperative electrical stimulations in surgery oflow grade gliomas: a comparative study betweentwo series without (1985 – 96) and with (1996 –2003) functional mapping in the same institution.J. Neurol. Neurosurg. Psychiatry 76, 845 – 851.(doi:10.1136/jnnp.2004.048520)
12. Duffau H, Moritz-Gasser S, Gatignol P. 2009Functional outcome after language mapping forinsular World Health Organization Grade II gliomasin the dominant hemisphere: experience with 24patients. Neurosurg. Focus 27, E7. (doi:10.3171/2009.5.FOCUS0938)
13. Sanai N, Mirzadeh Z, Berger MS. 2008 Functionaloutcome after language mapping for gliomaresection. N. Engl. J. Med. 358, 18 – 27. (doi:10.1056/NEJMoa067819)
14. Chang EF, Clark A, Smith JS, Polley MY, Chang SM,Barbaro NM, Parsa AT, McDermott MW, Berger MS.
2011 Functional mapping-guided resection of low-grade gliomas in eloquent areas of the brain:improvement of long-term survival. Clinical article.J. Neurosurg. 114, 566 – 573. (doi:10.3171/2010.6.JNS091246)
15. Sarubbo S et al. 2011 Awake surgery in low-gradegliomas harboring eloquent areas: 3-year meanfollow-up. Neurol. Sci. 32, 801 – 810. (doi:10.1007/s10072-011-0587-3)
16. Sirigu A, Mottolese C, Desmurget M. 2010 Responseto comment on ‘Movement intention after parietalcortex stimulation in humans’. Science 327, 1200.(doi:10.1126/science.1183758)
17. Logothetis NK. 2008 What we can do and what wecannot do with fMRI. Nature 453, 869 – 878.(doi:10.1038/nature06976)
18. Lio G, Boulinguez P. 2013 Greater robustness ofsecond order statistics than higher order statisticsalgorithms to distortions of the mixing matrix inblind source separation of human EEG: implicationsfor single-subject and group analyses. Neuroimage67, 137 – 152. (doi:10.1016/j.neuroimage.2012.11.015)
19. Sekihara K, Sahani M, Nagarajan SS. 2005Localization bias and spatial resolution of adaptiveand non-adaptive spatial filters for MEG sourcereconstruction. Neuroimage 25, 1056 – 1067.(doi:10.1016/j.neuroimage.2004.11.051)
20. Tate MC, Herbet G, Moritz-Gasser S, Tate JE, DuffauH. 2014 Probabilistic map of critical functionalregions of the human cerebral cortex: Broca’s arearevisited. Brain 137, 2773 – 2782. (doi:10.1093/brain/awu168)
21. Desmurget M, Reilly KT, Richard N, Szathmari A,Mottolese C, Sirigu A. 2009 Movement intentionafter parietal cortex stimulation in humans. Science324, 811 – 813. (doi:10.1126/science.1169896)
22. Fried I, Katz A, McCarthy G, Sass KJ, Williamson P,Spencer SS, Spencer DD. 1991 Functionalorganization of human supplementary motor cortexstudied by electrical stimulation. J. Neurosci. 11,3656 – 3666.
23. Filevich E, Kuhn S, Haggard P. 2012 Negative motorphenomena in cortical stimulation: implications forinhibitory control of human action. Cortex 48,1251 – 1261. (doi:10.1016/j.cortex.2012.04.014)
24. Luders HO, Dinner DS, Morris HH, Wyllie E, ComairYG. 1995 Cortical electrical stimulation in humans.The negative motor areas. Adv. Neurol. 67,115 – 129.
25. Strick PL. 2002 Stimulating research on motorcortex. Nat. Neurosci. 5, 714 – 715. (doi:10.1038/nn0802-714)
26. Borchers S, Himmelbach M, Logothetis N, KarnathHO. 2012 Direct electrical stimulation of humancortex—the gold standard for mapping brainfunctions? Nat. Rev. Neurosci. 13, 63 – 70. (doi:10.1038/nrn3140)
27. Desmurget M, Song Z, Mottolese C, Sirigu A. 2013Re-establishing the merits of electrical brain
stimulation. Trends Cogn. Sci. 17, 442 – 449. (doi:10.1016/j.tics.2013.07.002)
28. Histed MH, Ni AM, Maunsell JH. 2013 Insightsinto cortical mechanisms of behavior frommicrostimulation experiments. Prog. Neurobiol.103, 115 – 130. (doi:10.1016/j.pneurobio.2012.01.006)
29. Logothetis NK, Augath M, Murayama Y, Rauch A,Sultan F, Goense J, Oeltermann A, Merkle H. 2010The effects of electrical microstimulation on corticalsignal propagation. Nat. Neurosci. 13, 1283 – 1291.(doi:10.1038/nn.2631)
30. Finger S. 2010 Chapter 10: the birth of localizationtheory. Handb. Clin. Neurol. 95, 117 – 128. (doi:10.1016/S0072-9752(08)02110-6)
31. Tizard B. 1959 Theories of brain localization fromFlourens to Lashley. Med. Hist. 3, 132 – 145. (doi:10.1017/S0025727300024418)
32. Kandel ER, Schwartz JH, Jessell TM. 2000 Principlesof neural sciences (4th revised edition). New York,NY: McGraw-Hill.
33. Haines DE. 1997 Fundamental neuroscience.New York, NY: Churchill Livingston Inc.
34. Grafton ST, Woods RP, Mazziotta JC. 1993 Within-arm somatotopy in human motor areas determinedby positron emission tomography imaging ofcerebral blood flow. Exp. Brain Res. 95, 172 – 176.(doi:10.1007/BF00229666)
35. Lotze M, Erb M, Flor H, Huelsmann E, Godde B,Grodd W. 2000 fMRI evaluation of somatotopicrepresentation in human primary motor cortex.Neuroimage 11, 473 – 481. (doi:10.1006/nimg.2000.0556)
36. Plow EB, Arora P, Pline MA, Binenstock MT, Carey JR.2010 Within-limb somatotopy in primary motorcortex–revealed using fMRI. Cortex 46, 310 – 321.(doi:10.1016/j.cortex.2009.02.024)
37. Hlustik P, Solodkin A, Gullapalli RP, Noll DC, SmallSL. 2001 Somatotopy in human primary motor andsomatosensory hand representations revisited.Cereb. Cortex 11, 312 – 321. (doi:10.1093/cercor/11.4.312)
38. Alkadhi H, Crelier GR, Boendermaker SH, Golay X,Hepp-Reymond MC, Kollias SS. 2002 Reproducibilityof primary motor cortex somatotopy undercontrolled conditions. Am. J. Neuroradiol. 23,1524 – 1532.
39. Yang TT, Gallen CC, Schwartz BJ, Bloom FE. 1993Noninvasive somatosensory homunculus mapping inhumans by using a large-array biomagnetometer.Proc. Natl Acad. Sci. USA 90, 3098 – 3102. (doi:10.1073/pnas.90.7.3098)
40. Zeharia N, Hertz U, Flash T, Amedi A. 2012 Negativeblood oxygenation level dependent homunculusand somatotopic information in primary motorcortex and supplementary motor area. Proc. NatlAcad. Sci. USA 109, 18 565 – 18 570. (doi:10.1073/pnas.1119125109)
41. Nakamura A, Yamada T, Goto A, Kato T, Ito K,Abe Y, Kachi T, Kakigi R. 1998 Somatosensory

rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
10
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
homunculus as drawn by MEG. Neuroimage 7,377 – 386. (doi:10.1006/nimg.1998.0332)
42. Sanes JN, Schieber MH. 2001 Orderly somatotopy inprimary motor cortex: does it exist? Neuroimage 13,968 – 974. (doi:10.1006/nimg.2000.0733)
43. Branco DM et al. 2003 Functional variability of thehuman cortical motor map: electrical stimulationfindings in perirolandic epilepsy surgery. J. Clin.Neurophysiol. 20, 17 – 25. (doi:10.1097/00004691-200302000-00002)
44. Farrell DF, Burbank N, Lettich E, Ojemann GA. 2007Individual variation in human motor-sensory(rolandic) cortex. J. Clin. Neurophysiol. 24,286 – 293. (doi:10.1097/WNP.0b013e31803bb59a)
45. Graziano M. 2006 The organization of behavioralrepertoire in motor cortex. Annu. Rev. Neurosci.29, 105 – 134. (doi:10.1146/annurev.neuro.29.051605.112924)
46. Uttal WR. 2001 The new phrenology. Cambridge,MA: MIT press.
47. Gould 3rd HJ, Cusick CG, Pons TP, Kaas JH. 1986 Therelationship of corpus callosum connections toelectrical stimulation maps of motor, supplementarymotor, and the frontal eye fields in owl monkeys.J. Comp. Neurol. 247, 297 – 325. (doi:10.1002/cne.902470303)
48. Donoghue JP, Leibovic S, Sanes JN. 1992Organization of the forelimb area in squirrel monkeymotor cortex: representation of digit, wrist, andelbow muscles. Exp. Brain Res. 89, 1 – 19. (doi:10.1007/BF00228996)
49. Schieber MH, Hibbard LS. 1993 How somatotopic isthe motor cortex hand area? Science 261, 489 – 492.(doi:10.1126/science.8332915)
50. Meier JD, Aflalo TN, Kastner S, Graziano MS. 2008Complex organization of human primary motorcortex: a high-resolution fMRI study. J. Neurophysiol.100, 1800 – 1812. (doi:10.1152/jn.90531.2008)
51. Sanes JN, Donoghue JP, Thangaraj V, Edelman RR,Warach S. 1995 Shared neural substrates controllinghand movements in human motor cortex. Science268, 1775 – 1777. (doi:10.1126/science.7792606)
52. Nudo RJ, Jenkins WM, Merzenich MM, Prejean T,Grenda R. 1992 Neurophysiological correlates ofhand preference in primary motor cortex of adultsquirrel monkeys. J. Neurosci. 12, 2918 – 2947.
53. Matyas F, Sreenivasan V, Marbach F, Wacongne C,Barsy B, Mateo C, Aronoff R, Petersen CC. 2010Motor control by sensory cortex. Science 330,1240 – 1243. (doi:10.1126/science.1195797)
54. Nii Y, Uematsu S, Lesser RP, Gordon B. 1996 Doesthe central sulcus divide motor and sensoryfunctions? Cortical mapping of human hand areasas revealed by electrical stimulation throughsubdural grid electrodes. Neurology 46, 360 – 367.(doi:10.1212/WNL.46.2.360)
55. Haseeb A, Asano E, Juhasz C, Shah A, Sood S,Chugani HT. 2007 Young patients with focal seizuresmay have the primary motor area for the hand inthe postcentral gyrus. Epilepsy Res. 76, 131 – 139.(doi:10.1016/j.eplepsyres.2007.07.007)
56. Preuss TM, Stepniewska I, Kaas JH. 1996 Movementrepresentation in the dorsal and ventral premotor
areas of owl monkeys: a microstimulation study.J. Comp. Neurol. 371, 649 – 676. (doi:10.1002/(SICI)1096-9861(19960805)371:4,649::AID-CNE12.3.0.CO;2-E)
57. Fogassi L, Gallese V, Gentilucci M, Luppino G,Matelli M, Rizzolatti G. 1994 The fronto-parietalcortex of the prosimian Galago: patterns ofcytochrome oxidase activity and motor maps.Behav. Brain Res. 60, 91 – 113. (doi:10.1016/0166-4328(94)90067-1)
58. Widener GL, Cheney PD. 1997 Effects on muscleactivity from microstimuli applied to somatosensoryand motor cortex during voluntary movement inthe monkey. J. Neurophysiol. 77, 2446 – 2465.
59. Penfield W. 1954 Mechanisms of voluntary movement.Brain 77, 1 – 17. (doi:10.1093/brain/77.1.1)
60. Overduin SA, d’Avella A, Carmena JM, Bizzi E. 2012Microstimulation activates a handful of musclesynergies. Neuron 76, 1071 – 1077. (doi:10.1016/j.neuron.2012.10.018)
61. Schieber MH. 2001 Constraints on somatotopicorganization in the primary motor cortex.J. Neurophysiol. 86, 2125 – 2143.
62. Shambes GM, Gibson JM, Welker W. 1978 Fracturedsomatotopy in granule cell tactile areas of ratcerebellar hemispheres revealed by micromapping.Brain Behav. Evol. 15, 94 – 140. (doi:10.1159/000315982)
63. Rathelot JA, Strick PL. 2006 Muscle representationin the macaque motor cortex: an anatomicalperspective. Proc. Natl Acad. Sci. USA 103,8257 – 8262. (doi:10.1073/pnas.0602933103)
64. Rathelot JA, Strick PL. 2009 Subdivisions of primarymotor cortex based on cortico-motoneuronal cells.Proc. Natl Acad. Sci. USA 106, 918 – 923. (doi:10.1073/pnas.0808362106)
65. Graziano MS, Aflalo TN. 2007 Mapping behavioralrepertoire onto the cortex. Neuron 56, 239 – 251.(doi:10.1016/j.neuron.2007.09.013)
66. Foerster O. 1936 The motor cortex in man in light ofHughlings Jackson’s doctrines. Brain 59, 135 – 159.(doi:10.1093/brain/59.2.135)
67. Penfield W, Welch K. 1951 The supplementarymotor area of the cerebral cortex; a clinical andexperimental study. AMA Arch. Neurol. Psychiatry66, 289 – 317. (doi:10.1001/archneurpsyc.1951.02320090038004)
68. Graziano MS, Taylor CS, Moore T. 2002 Complexmovements evoked by microstimulation ofprecentral cortex. Neuron 34, 841 – 851. (doi:10.1016/S0896-6273(02)00698-0)
69. Desmurget M, Richard N, Harquel S, Baraduc P,Szathmari A, Mottolese C, Sirigu A. 2014 Neuralrepresentations of ethologically relevant hand/mouth synergies in the human precentral gyrus.Proc. Natl Acad. Sci. USA 111, 5718 – 5722. (doi:10.1073/pnas.1321909111)
70. Kaas JH, Gharbawie OA, Stepniewska I. 2013 Corticalnetworks for ethologically relevant behaviors inprimates. Am. J. Primatol. 75, 407 – 414. (doi:10.1002/ajp.22065)
71. Stepniewska I, Gharbawie OA, Burish MJ, Kaas JH.2014 Effects of muscimol inactivations of functional
domains in motor, premotor, and posterior parietalcortex on complex movements evoked by electricalstimulation. J. Neurophysiol. 111, 1100 – 1119.(doi:10.1152/jn.00491.2013)
72. Kaas JH. 2004 Evolution of somatosensory andmotor cortex in primates. Anat. Rec. 281A,1148 – 1156. (doi:10.1002/ar.a.20120)
73. Lemon RN. 2008 Descending pathways in motorcontrol. Annu. Rev. Neurosci. 31, 195 – 218. (doi:10.1146/annurev.neuro.31.060407.125547)
74. Griffin DM, Hudson HM, Belhaj-Saif A, Cheney PD.2011 Hijacking cortical motor output with repetitivemicrostimulation. J. Neurosci. 31, 13 088 – 13 096.(doi:10.1523/JNEUROSCI.6322-10.2011)
75. Griffin DM, Hudson HM, Belhaj-Saif A, Cheney PD.2014 EMG activation patterns associated with highfrequency, long-duration intracorticalmicrostimulation of primary motor cortex.J. Neurosci. 34, 1647 – 1656. (doi:10.1523/JNEUROSCI.3643-13.2014)
76. Graziano MS, Patel KT, Taylor CS. 2004 Mappingfrom motor cortex to biceps and triceps altered byelbow angle. J. Neurophysiol. 92, 395 – 407. (doi:10.1152/jn.01241.2003)
77. Graziano MS, Taylor CS, Moore T, Cooke DF. 2002 Thecortical control of movement revisited. Neuron 36,349 – 362. (doi:10.1016/S0896-6273(02)01003-6)
78. Pruszynski JA, Kurtzer I, Nashed JY, Omrani M,Brouwer B, Scott SH. 2011 Primary motor cortexunderlies multi-joint integration for fast feedbackcontrol. Nature 478, 387 – 390. (doi:10.1038/nature10436)
79. Reilly KT, Sirigu A. 2008 The motor cortex and itsrole in phantom limb phenomena. Neuroscientist14, 195 – 202. (doi:10.1177/1073858407309466)
80. Sanai N, Berger MS. 2012 Recent surgicalmanagement of gliomas. Adv. Exp. Med. Biol. 746,12 – 25. (doi:10.1007/978-1-4614-3146-6_2)
81. Talacchi A, Santini B, Casartelli M, Monti A, CapassoR, Miceli G. 2013 Awake surgery between art andscience. Part II: language and cognitive mapping.Funct. Neurol. 28, 223 – 239. (doi:10.11138/FNeur/2013.28.3.223)
82. Kilbride RD. 2013 Intraoperative functional corticalmapping of language. J. Clin. Neurophysiol. 30, 591 –596. (doi:10.1097/01.wnp.0000436900.48243.9f )
83. De Witte E, Marien P. 2013 The neurolinguisticapproach to awake surgery reviewed. Clin. Neurol.Neurosurg. 115, 127 – 145. (doi:10.1016/j.clineuro.2012.09.015)
84. Duffau H. 2008 The anatomo-functional connectivityof language revisited. New insights provided byelectrostimulation and tractography.Neuropsychologia 46, 927 – 934. (doi:10.1016/j.neuropsychologia.2007.10.025)
85. DeWitt I, Rauschecker JP. 2013 Wernicke’s arearevisited: parallel streams and word processing.Brain Lang. 127, 181 – 191. (doi:10.1016/j.bandl.2013.09.014)
86. Chang EF, Raygor KP, Berger MS. 2014Contemporary model of language organization: anoverview for neurosurgeons. J. Neurosurg. 122,250 – 261. (doi:10.3171/2014.10.JNS132647)

rstb.royalsocietypublishing.orgPhil.Trans.R.Soc.B
370:20140207
11
on August 20, 2018http://rstb.royalsocietypublishing.org/Downloaded from
87. Conant D, Bouchard KE, Chang EF. 2014 Speech mapin the human ventral sensory-motor cortex. Curr.Opin. Neurobiol. 24, 63 – 67. (doi:10.1016/j.conb.2013.08.015)
88. Specht K. 2014 Neuronal basis of speechcomprehension. Hear Res. 307, 121 – 135. (doi:10.1016/j.heares.2013.09.011)
89. Dronkers NF. 1996 A new brain region forcoordinating speech articulation. Nature 384,159 – 161. (doi:10.1038/384159a0)
90. Price CJ. 2012 A review and synthesis of the first 20years of PET and fMRI studies of heard speech,spoken language and reading. Neuroimage 62,816 – 847. (doi:10.1016/j.neuroimage.2012.04.062)
91. Hillis AE, Work M, Barker PB, Jacobs MA, Breese EL,Maurer K. 2004 Re-examining the brain regionscrucial for orchestrating speech articulation. Brain127, 1479 – 1487. (doi:10.1093/brain/awh172)
92. Wise RJ, Greene J, Buchel C, Scott SK. 1999Brain regions involved in articulation. Lancet 353,1057 – 1061. (doi:10.1016/S0140-6736(98)07491-1)
93. Tate MC, Herbet G, Moritz-Gasser S, Tate JE, DuffauH. 2014 Reply: probabilistic map of languageregions: challenge and implication. Brain 138, e338.(doi:10.1093/brain/awu253)
94. Hickok G, Poeppel D. 2007 The cortical organizationof speech processing. Nat. Rev. Neurosci. 8,393 – 402. (doi:10.1038/nrn2113)
95. Friederici AD. 2011 The brain basis of languageprocessing: from structure to function. Physiol. Rev. 91,1357 – 1392. (doi:10.1152/physrev.00006.2011)
96. Henseler I, Regenbrecht F, Obrig H. 2014 Lesioncorrelates of patholinguistic profiles in chronicaphasia: comparisons of syndrome-, modality- andsymptom-level assessment. Brain 137, 918 – 930.(doi:10.1093/brain/awt374)
97. Desmurget M, Bonnetblanc F, Duffau H. 2007Contrasting acute and slow-growing lesions: a newdoor to brain plasticity. Brain 130, 898 – 914.(doi:10.1093/brain/awl300)
98. Wu J, Lu J, Zhang H, Zhang J, Mao Y, Zhou L. 2014Probabilistic map of language regions: challengeand implication. Brain 138, e337. (doi:10.1093/brain/awu247)
99. Duffau H. 2010 Awake surgery for nonlanguagemapping. Neurosurgery 66, 523 – 528. (doi:10.1227/01.NEU.0000364996.97762.73)
100. Thiebaut de SM, Urbanski M, Duffau H, Volle E,Levy R, Dubois B, Bartolomeo P. 2005 Directevidence for a parietal – frontal pathway subservingspatial awareness in humans. Science 309,2226 – 2228. (doi:10.1126/science.1116251)
101. Carota F, Desmurget M, Sirigu A. 2010 Forwardmodeling mediates motor awareness. In Consciouswill and responsibility: a tribute to Benjamin Libet(eds L Nadel, W Sinnott-Armstrong), pp. 97 – 108.Oxford, UK: Oxford University Press.
102. Fridman EA, Desmurget M, Sirigu A. 2011 Fromconscious motor intention to movement awareness.In Characterizing consciousness: from cognitionto the clinic? (eds S Dehaene, Y Christen),pp. 191 – 198. Berlin, Germany: Springer.
103. Desmurget M, Sirigu A. 2009 A parietal – premotornetwork for movement intention and motorawareness. Trends Cogn. Sci. 13, 411 – 419. (doi:10.1016/j.tics.2009.08.001)
104. Desmurget M, Sirigu A. 2012 Conscious motorintention emerges in the inferior parietal lobule.Curr. Opin. Neurobiol. 22, 1004 – 1011. (doi:10.1016/j.conb.2012.06.006)
105. Andersen RA, Buneo CA. 2002 Intentional maps inposterior parietal cortex. Annu. Rev. Neurosci. 25, 189–220. (doi:10.1146/annurev.neuro.25.112701.142922)
106. Lau HC, Rogers RD, Haggard P, Passingham RE.2004 Attention to intention. Science 303,1208 – 1210. (doi:10.1126/science.1090973)
107. Kremer S, Chassagnon S, Hoffmann D, Benabid AL,Kahane P. 2001 The cingulate hidden hand.J. Neurol. Neurosurg. Psychiatry 70, 264 – 265.(doi:10.1136/jnnp.70.2.264)
108. Chassagnon S, Minotti L, Kremer S, Hoffmann D,Kahane P. 2008 Somatosensory, motor, and reaching/grasping responses to direct electrical stimulation ofthe human cingulate motor areas. J. Neurosurg. 109,593 – 604. (doi:10.3171/JNS/2008/109/10/0593)
109. Desmurget M, Grafton S. 2000 Forward modelingallows feedback control for fast reachingmovements. Trends Cogn. Sci. 4, 423 – 431. (doi:10.1016/S1364-6613(00)01537-0)
110. Sirigu A, Duhamel JR, Cohen L, Pillon B, Dubois B,Agid Y. 1996 The mental representation of handmovements after parietal cortex damage. Science273, 1564 – 1568. (doi:10.1126/science.273.5281.1564)
111. Berti A, Bottini G, Gandola M, Pia L, Smania N,Stracciari A, Castiglioni I, Vallar G, Paulesu E. 2005Shared cortical anatomy for motor awareness andmotor control. Science 309, 488 – 491. (doi:10.1126/science.1110625)
112. Christensen MS, Lundbye-Jensen J, Geertsen SS,Petersen TH, Paulson OB, Nielsen JB. 2007 Premotorcortex modulates somatosensory cortex duringvoluntary movements without proprioceptivefeedback. Nat. Neurosci. 10, 417 – 419. (doi:10.1038/nn1873)
113. Mottolese C, Richard N, Harquel S, Szathmari A,Sirigu A, Desmurget M. 2013 Mapping motorrepresentations in the human cerebellum. Brain136, 330 – 342. (doi:10.1093/brain/aws186)
114. Matsumoto R, Nair DR, LaPresto E, Bingaman W,Shibasaki H, Luders HO. 2007 Functionalconnectivity in human cortical motor system: acortico-cortical evoked potential study. Brain 130,181 – 197. (doi:10.1093/brain/awl257)
115. Matsumoto R, Nair DR, LaPresto E, Najm I,Bingaman W, Shibasaki H, Luders HO. 2004Functional connectivity in the human languagesystem: a cortico-cortical evoked potentialstudy. Brain 127, 2316 – 2330. (doi:10.1093/brain/awh246)