Acrylamide Grafting on Banana Fibres for Increased Water Absorbency and Retention

Occupational and Environmental Medicine 1994;51:205-21 1
Retention patterns of asbestos fibres in lung tissueamong asbestos cement workers
M Albin, F D Pooley, U Str6mberg, R Attewell, R Mitha, L Johansson, H Welinder
Department ofOccupational andEnvironmentalMedicineM AlbinR AttewellU StrombergH WelinderDepartment ofPathology, UniversityHospital S-221 85Lund, SwedenL JohanssonSchool of Engineering,University ofWales,College of Cardiff,WalesF D PooleyR MithaRequest for reprints to:Dr Maria Albin,Department of Occupationaland EnvironmentalMedicine, UniversityHospital, S-221 85 Lund,Sweden.
Accepted 28 June 1993
AbstractRetention patterns in lung tissue (deter-mined by transmission electron micro-scopy and energy dispersive spectro-metry) of chrysotile, tremolite, andcrocidolite fibres were analysed in 69dead asbestos cement workers and 96referents. There was an accumulation oftremolite with time of employment.Among workers who died within threeyears of the end of exposure, the 13 withhigh tremolite concentrations had a sig-nificantly longer duration of exposurethan seven in a low to intermediate cate-gory (medians 32 v 20 years; p = 0-018,one sided). Crocidolite showed similarpatterns of accumulation. In workerswho died more than three years after theend of exposure, there were no correla-tions between concentrations of amphi-bole fibres and time between the end ofexposure and death. Chrysotile concen-trations among workers who died shortlyafter the end of exposure were higherthan among the referents (median differ-ence in concentrations 13 million fibres(f)/g dry weight; p = 0'033, one sided). Noquantitative differences in exposure(duration or intensity) could be shownbetween workers with high and low tointermediate concentrations. Interest-ingly, all seven workers who had hada high intensity at the end of exposure(>2.5 f7ml), had low to intermediatechrysotile concentrations at death,whereas those with low exposure wereevenly distributed (31 subjects in bothconcentration categories); hence, therewas a dependence between last intensityof exposure and chrysotile concentration(p = 0-014). Among 14 workers with ahigh average intensity of exposure, boththose (n = 5) with high tissue concentra-tions of chrysotile and those (n = 10)with high tissue concentrations of tremo-lite fibres had more pronounced fibrosisthan those with low to intermediate con-centrations (median fibrosis grades forchrysotile: 2 v 1, p = 0-021; for tremolite:2 v 0-5, p = 0.012). Additionally, workerswho died shortly after the end of expo-sure with high concentrations ofchrysotile and crocidolite had smokedmore than those with low to intermediateconcentrations (medians for chrysotile 35v 15 pack-years, p = 0*030; for crocidolite37 v 15 pack-years, p = 0-012). The pre-sent data indicate that chrysotile has arelatively rapid turnover in human lungs,
whereas the amphiboles, tremolite andcrocidolite, have a slower turnover.Further, chrysotile retention may bedependent on dose rate. Chrysotile andcrocidolite deposition and retention maybe increased by tobacco smoking;chrysotile and tremolite by fibrosis.
(Occup Environ Med 1994;S1:205-21 1)
The persistence of mineral fibres in lung tis-sue is believed to be one of the major deter-minants for their ability to induce fibrosis andmalignancies,' and is thus crucial for evalua-tion of risk and preventive measures. Thispoint has, however, been contested by otherauthors, claiming that the fibres that passthrough the tissue might well be the causalagent.2
Animal data on retention of particularasbestos types have been reported in severalstudies,'6 indicating a faster elimination ofchrysotile than amphibole fibres, possibly dueto fragmentation of chrysotile (into shorterand thinner fibres) as opposed to simultane-ously administered amosite.7 Apart from fibretype, retention is determined by size, with afaster elimination for short fibres than forlong ones.8'0 Accordingly, Davis reportedthat the clearance after six months in rats was14% for long and 20% for short fibreamosite, compared with 55% for long and90% for short chrysotile."Human data are scarce. Analyses of min-
eral fibre concentrations in chrysotile minersand millers do, however, indicate a muchhigher retention of tremolite than ofchrysotile asbestos.'2 13 Only three studies,providing rough quantitative estimates of theclearance rates among humans, have beenpublished. The data were based on minersand millers (chrysotile and tremolite)," croci-dolite miners,'5 and on mesothelioma series(amosite and crocidolite) .6 Half times ofsome years to decades were reported. It isobvious, however, that the uncertainty ofthese estimates was considerable. Thus, morestudies of accumulation and elimination pat-terns are needed.We have studied retention patterns of as-
bestos fibres among asbestos cement workers.
Material and methodsMATERIALThe material consisted of lung tissue speci-mens preserved at the Lund UniversityHospital at necropsy examination of 75
205 on M
arch 4, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.3.205 on 1 March 1994. D
ownloaded from

Albin, Pooley, Stromberg, Attewell, Mitha, johansson, Welinder
asbestos cement workers and 96 controls.The workers were those (except one who wasexcluded as he was found to have been a con-tract worker) employed by an asbestoscement factory.'7 '9 Only the 69 workers withinformation on exposure were included in theanalysis. The controls were drawn from thesame hospital files, including all causes ofdeath, and chosen to match the workers forsex, age, and calendar year at death. Age(asbestos cement workers: median 68 years,referents: median 67 years), sex (five womenin each group), and calendar year of death(medians 1972 in both groups) were similaramong the asbestos cement workers finallyincluded and the referents.
EXPOSUREChrysotile was the major asbestos exposure.Tremolite is, however, known to be a com-
mon contaminant in commercial chrysotilequalities.20 Some amosite was used up to1956, crocidolite until 1966; both were usedintermittently. Dust measurements were
made from 1956 onwards; they reflect theconcentrations of all fibres, without informa-tion on the different components. Some fil-ters from dust sampling during the late 1960sare available. Preliminary data from determi-nation of fibre type in airborne dust, with an
analytical transmission electron microscope,have shown chrysotile and singular tremolitefibres (S Krantz, personal communication). Amore detailed description of available occupa-
tional hygiene data has been published in a
previous paper.The data on dust concentrations, produc-
tion, and dust control were used by an experi-enced industrial hygienist (HIW) to calculatetask specific exposure estimates (averageintensities; £'ml air) during five year periods.These were combined with the work historiesto obtain individual estimates of cumulativedose (f-years/ml), average intensity of expo-sure throughout employment, and lastobserved intensity.
Only workers performing milling, mixing,sawing, and polishing operations, or sweepingof the asbestos barn, were estimated to haveaverage intensities of exposure >2 fibres/ml.
Individual exposure estimates could not becalculated for six workers, due to missingwork histories. Among the remaining 69workers, mean duration of employment was18 (median 15) years, and mean timebetween the end of exposure and death 12years (median 10). The mean estimated aver-
age intensity of exposure was 1-7 (median1-2, range 0 0-7 3) f/ml, and the mean lastintensity of exposure 1-2 (median 1 0, range
0-0-6-1) f/ml.Data on smoking habits were obtained for
all but three workers (n = 66) by a postalinquiry sent to the next of kin. The accumu-
lated lifetime tobacco consumption was cal-culated as pack-years.
TISSUE ANALYSESDust extracts were prepared in a standardmanner. The analyses were performed with a
Philips 400T transmission electron micro-scope fitted with an Edax x ray analysis sys-tem at a magnification of 20 000. Fibrousparticles were identified, sized, and countedwithout restrictions as to minimum length.Mineral fibre concentrations were recorded asf/g of dried tissue.'9 21A histopathological grading of fibrosis was
made, as described earlier.'8
STATISTICSTabulation of chrysotile concentrationsamong the referents for different strata of tis-sue weights showed an inverse relationbetween tissue weight and chrysotile concen-tration (table 1). This finding was not con-founded by age or cumulative exposure. Astandardization curve was obtained throughlinear interpolation (linear extrapolation forsmall weights and constant extrapolation forlarge ones) between the points (medianweight, median concentration) in each class.No relation was found between sample weightand concentration of the amphibole fibres.
Chrysotile fibre concentrations among theexposed workers, measured both as observedand as residual concentrations from thestandardization curve, were dichotomised atthe 60th percentile (residual concentration22 x 106 f/g dry weight) into one group withlow to intermediate and one with a high con-centration. Similarly, the amphibole concen-trations were dichotomised (tremolite: 60thpercentile = 0-3 million, crocidolite: 60thpercentile = 4 million fig). The 60th per-centile was chosen to provide a sufficientnumber of observations, but still strictly posi-tive observations in the high concentrationcategory. There was no need for adjustment ofobserved concentrations ofthe amphibole fibres.The 69 workers with individual exposure
estimates were included in the analysis ofretention patterns. A maximum of three yearsbetween end of exposure and death wasassumed to exclude substantial elimination.Associations, among those who died withinthree years of end of employment, were inves-tigated between possible determinants (age atstart of employment, age at death, year ofemployment, duration of exposure, averageintensity of exposure throughout employ-ment, intensity at the end of exposure, timebetween the end of exposure and death,tobacco consumption, and grade of fibrosis)and fibre concentration. These results wereused to postulate to which concentrationcategory the others, who died more thanthree years after the end of employment,
Table 1 Chrysotile concentrations (medians) for differentstrata ofdry weights of lung tissue among 96 referents (192tissue samples)
Chrysotileconcentration
Thy weight (w (mng))Median ~~(fig dryInterval Median weight x 106) No
0<w 10 8 44 2610<w 20 15 31 7020 < w < 30 25 24 4030<w 40 35 21 17
w > 40 58 12 39
206 on M
arch 4, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.3.205 on 1 March 1994. D
ownloaded from

Retention patterns of asbestos fibres in lung tissue among asbestos cement workers
14
12
10o
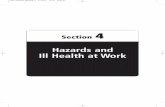
Dead S 3 y Onset of Estimated Observedfrom end of exposure category categoryexposure at end of at death(n = 20) exposure
Dead > 3 y from end of exposure (n = 49)
Figure 1 Modelfor the accumulation and elimination of tremolitefibres in lung tissuefrom 69 asbestos cement workers (medians are indicated within observed categories).
belonged when exposure ended. Subsequently, relations between the inferred elimination patterns (from the postulated categorat end of exposure to the observed category adeath) and the determinants mentioned, wereinvestigated among these workers (figs 1 an(2). Differences in the determinants werecompared by the Mann-Whitney test. On(sided tests were used for associations irwhich the alternative hypothesis was supported by data from other studies; howeverthe p values are two sided unless otherwise
stated. Also, the given confidence intervals(CIs) are based on the Mann-Whitney test.One of the reasons for analysing accumula-
tion and elimination patterns is the fact thatthe data are not satisfactorily described by thefollowing classic accumulation and elimina-tion model:
Fibre tissue concentration = A(averageintensity)[1-exp(-Btl)] exp(-Bt2), where t1 isduration of exposure, t2 is the time betweenend of exposure and death, and A and B arethe variables to be estimated. The model vari-able A multiplied by average intensity ofexposure corresponds to the steady stateconcentration under constant exposure, and
J the variable B is an elimination constant,related to clearance half life (T,,2 = ln2/B).The influences of last and average intensity
of exposure, on tissue concentrations (dicho-tomised at the 60th percentile) of chrysotileand tremolite at death were analysed bydichotomising the intensities at 2-5 f/ml intolow and high intensity groups. This limit waschosen to provide a sufficient number ofobservations in each group. The indepen-
- dence between intensity of exposure and- tissue concentration was examined byy Fisher's exact test (two sided). Differences inIt the determinants were first examined betweene the intensity groups, and then for the concen-
a tration categories within each intensity group.
e Possible confounding of observed associa-e tions between tobacco consumption and min-n eral fibre concentrations by age at death,- duration, and year of employment was exam-
ined by first dividing the data into two stratae (with the common stratum bound close to
Table 2 Associations between average intensity of exposure throughout employment, intensity at end of exposure, andconcentration category of chtysotile or tremolite fibres in lung tissue among 69 asbestos cement workers. Covariates not intable were not significant in any test
Chrysotile* TremoliteFibre concentration Fibre concentration
Lowto Low toHigh intermediate p Value High intermediate p Value
Average intensity>2-5 (median 4-3 (range 2-7-73)) f/ml air:
Subjects (n) 5 9 10 4Averageintensity(f/ml) 3-2 5 0 0-028t 3-8 5 0 0-32tFibrosis grade 2-0 1 0 0-021t 2-0 0-5 0-012tExposure time(y) 17 21 0.64t 25 9-7 0-066tTime to death (y) 3-7 10 0.38t 6-7 9-2 0-48t
<2-5 (median 1 0 (range 0 0-2-3)) f/ml air:Subjects (n) 26 29 0-551 20 35 0-0321
Average intensity (f/ml) 0 9 1-2 0-039t 1 0 1 0 0-94tFibrosis grade 1 0 1.0 0.29t 1-5 1 0 0-20tExposuretime(y) 16 12 027t 30 10 0-0015tTimetodeath(y) 9-8 13 0-62t 8-6 13 0.14t
Last intensity>2-5 (median 4-6 (range 2-7-6-1)) f/ml air:
Subjects (n) 0 7 - 4 3Average intensity (f/ml) - 5-0 - 5-0 5 0 0.48tFibrosis grade - 1 0 - 1-5 0 0064tExposure time(y) - 21 - 15 12 029tTime to death (y) - 9-7 - 10 4 0-72t
<2-5 (median 09 (range 0 0-23)) f/ml air:Subjects(n) 31 31 0-0141 26 36 0-46$
Average intensity (f/ml) 1.0 1-20 028t 1-2 1 0 0.15tFibrosis grade 1 0 1.0 0-78t 2-0 1.0 0-057tExposuretime(y) 17 12 0-22t 31 10 0-0003tTimeto death (y)§ 9-6 10 040t 9 13 0-027t
All Data values are medians; categories are high chrysotile median 61 (range 22 to 430), low to intermediate median 0-5 (range- 14 to 22), high tremolite median 1-5 (range 0-3 to 13), low to intermediate median 0-0 (range 00 to 0-2) f/g x 106.*Residual chrysotile concentrations as computed from a standardisation curve (see text).tMann-Whimey test for differences between the concentration categories.tFisher's exact test for independence between intensity and concentration categories (all 69 workers).§Time between cessation of exposure and death.
207
on March 4, 2021 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.51.3.205 on 1 M
arch 1994. Dow
nloaded from

Albin, Pooley, Stromberg, Attewell, Mitha, Johansson, Welinder
the median of the potential confounder), andthen calculating stratum specific median dif-ferences for the determinant between the cat-egories (and corresponding p values), as wellas a pooled p value.22 The observed influenceof grade of fibrosis on mineral fibre concen-trations by age and tobacco consumption wasexamined for possible confounding in thesame way.
Underlying cause of death, as coded by theNational Swedish Bureau of Statistics, wasgrouped into possibly asbestos related deaths(four groups: mesothelioma, lung cancer,fibrosis, colorectal cancer) and other causes.Differences in the fibre concentrationsbetween the other causes and each asbestosrelated group of deaths were assessed with theMann-Whitney test.
ResultsCHRYSOTILEThe 20 workers who had died within threeyears of the end of employment had higherchrysotile concentrations than the referents(n = 96; median difference in concentrations13 million f/g, p = 0-033, one sided).No differences in average, or last intensity,
or duration of exposure were found betweenthe nine workers with high and the 11workers with low to intermediate chrysotileconcentrations. The only determinant factorthat differed significantly between the twogroups was tobacco consumption. Workerswith high chrysotile concentrations had a twofold higher median tobacco consumptionthan workers with low to intermediate con-centrations (35 v 15 pack-years, p = 0 030).Stratification suggested, however, that thisrelation might be confounded by duration(and year) of employment.Two different classifications were made of
all workers with individual exposure estimates(n = 69). They were categorised as eitherhaving a high (>2 5 f/ml) or low ( 2 5 f/ml)last and average intensity of exposure (table2). There were no significant differences inthe other determinants between these highand low intensity groups.The association between last intensity and
category of tissue concentration was signifi-cant (p = 0-014); all workers with a high lastintensity of exposure had low to intermediatechrysotile concentrations in lung tissue. Nosuch relation was observed for average inten-sity. Within the group with a high averageintensity of exposure, grade of fibrosis washigher among those with high chrysotile con-centrations than among those with low tointermediate concentrations (p = 0-021). Strati-fication did not indicate that this finding wasconfounded by age or tobacco consumption.The results of the observed, unstandard-
ised, chrysotile concentrations were similar tothose obtained with the standardised concen-trations.
TREMOLITEAnalysis of tremolite concentrations in theworkers (n = 20) who had died within three
years of the end of exposure showed thatduration of exposure differed significantly,with a median of 32 years for workers in thehigh category (n = 13), and 20 years in thelow to intermediate category (p = 0-018, onesided; fig 1). In the low to intermediate cate-gory (n = 7), the upper limit of the 95% CIfor duration of exposure was 26 years. Thatlimit was used to postulate the concentrationcategory at the end of exposure for thoseliving >3 years after the end of exposure.
Tobacco consumption in the 20 workersdid not differ between the two tissue concen-tration categories (p = 0-24).Among workers living >3 years after end of
exposure, those employed for 26 years ormore were postulated to have belonged to thehigh category at the end of exposure, andthose with shorter durations as belonging tothe low to intermediate category. The timethat elapsed between the end of exposure anddeath among those postulated to havebelonged to the high concentration categoryat the end of exposure, was not significantlyassociated with observed concentration cate-gory of tremolite fibres at death (fig 1; high(n = 8), median 13 years, low to intermediate(n = 4) median 10 years, p = 0 67).Among workers postulated to have
belonged to the high category at end of expo-sure, those observed to be in the high concen-tration category at death, had significantlyhigher grades of fibrosis (medians 2-0 v 0-5;p = 0-014), than those in the low to inter-mediate category at death (with no indica-tions of confounding by age or tobaccoconsumption). They also had slightly, but sig-nificantly, higher average intensities of expo-sure (medians 1 0 v 0 6 f/ml; p = 0 011) thanthe others. This may indicate that intensityaffects tissue concentrations of tremolite,although this could not be shown in theanalysis of accumulation.The 10 workers postulated to have
belonged to the low to intermediate concen-tration category at the end of exposure, butfound to be in the high concentration cate-gory at death, tended to have a higher cumu-lative exposure (p = 0 055) than those 27workers both postulated and found to be inthe low to intermediate category.
Classification of all workers into high(>2-5 f/ml) and low groups of last andaverage intensity of exposure (table 2), didnot show any differences in the other deter-minants between the groups, except thatworkers with a high average intensity wereolder at the end of exposure than those with alow average intensity (p = 0-028).
Distributions of high and low to inter-mediate tremolite concentrations were com-pared for the intensity groups. There was asignificant association between average inten-sity and tremolite concentration (p = 0-032)but no such relation was seen for last inten-sity. Among workers with a low last intensityof exposure, those with high tremolite con-centrations in lung tissue had a longer dura-tion of exposure than those with lowconcentrations (p = 0 0003). Also, workers
208
on March 4, 2021 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.51.3.205 on 1 M
arch 1994. Dow
nloaded from

Retention patterns of asbestos fibres in lung tissue among asbestos cement workers
140r
:n = 12
A:
-1/~~~~~~~~~~~~~~~~~~~~~~~~~~~~1
Dead s 3 y Onset offrom end of exposureexposure(n = 17)
Estimatedcategoryat end ofexposure
Observedcategoryat death
Dead > 3 y from end of exposure (n = 52)
Figure 2 Model for the accumulation and elimination of crocidolite fibres in lung tissuefrom 69 asbestos cement workers (medians are indicated within observed categories).
with low concentrations had a longer timebetween the end of exposure and death thanthose with high concentrations (p = 0 027).Among workers with a high average inten-
sity of exposure, those with high tissue con-centrations had a higher grade of fibrosis(p = 0.012). Stratification indicated that agewas not a confounding factor in this context,whereas tobacco consumption might be.Among workers with a low average intensity,those with high concentrations had a longerduration of exposure (p = 0 0003).
CROCIDOLITECrocidolite use at the plant ended in 1966.Thus that year was regarded as the end ofexposure in the analyses of relations betweencategory of tissue concentration of crocidoliteand possible determinants. In the 17 personswho died within three years of end of expo-sure, longer durations of exposure were seenfor those in the high concentration category*(n = 9, median 32 years) compared withthose in the low to intermediate (n = 8,median 25, 95% CI one sided upper limit
Table 3 Mineralfibre concentrations (fig dry weight x 106) in lung tissuefrom 75asbestos cement workers by cause ofdeath
Tumour
Mesothelioma Lung Colorectal Fibrosis Other(n = 7) (n = 2) (n = 4) (n = 2) (n = 60)
Chrysotile:Observed 62t 16, 38 35 37, 86 43Residualt 14 5-1, 9-6 13 17, 64 15
Amphiboles 62** 16, 22 5 0 44, 90* 4-2Crocidolite 54** 1-9, 14 3-8 39, 69* 1-6Amosite 6-8 4-9, 6-2* 0-52 1-0, 17 0-18Tremolite 2.9** 1-2, 4-6* 0-25 2-2, 2-3* 0Anthophyllite 1-7* 0-85, 4-6* 0-38 0 95, 1-0 0
Totalfibres§ 211* 46, 141 43 132, 168 66
*p < 0-05; **p < 0-01 v deaths from other diseases (two sided, Mann-Whitney test).tGiven as medians for more than two observations.tResidual chrysotile concentrations as computed from a standardization curve (see text).SIncluding non-asbestos fibres.
= 29 years, p = 0-027; fig 2). Also, year ofonset of exposure differed (p = 0 0048)between the two tissue concentration cate-gories. All those in the high category hadstarted employment in the 1920s or 1930s,compared with four out of eight in the low tointermediate category.
Workers in the high category also had ahigher tobacco consumption than those in thelow category (medians 37 v 15 pack-years,p = 0-013); stratification did not indicateconfounding by age, or duration of employ-ment.Among workers who died more than three
years after the end of exposure, thoseemployed for 29 years or more were postu-lated to have belonged to the high category atthe end of exposure, and those with shorterdurations of employment as belonging to thelow to intermediate category. Time betweenthe end of exposure and death was similaramong workers assumed to have decreasedtheir tissue concentrations (from postulatedhigh to observed low to intermediate, n = 5),and workers believed to have been constantlyin the high category (n = 7, medians 5-6and 5-5 years, p = 0 87). Workers in theconstantly high category had a higheraverage intensity of exposure than those whohad changed category (medians 2-7 v 0-8,p = 0 028).Among workers assumed to have belonged
to the low to intermediate category at the endof exposure, those actually found in the highconcentration category at death (n = 14), hadsignificantly longer durations of employmentthan those observed in the low to inter-mediate category (n = 26; medians 11 v 3-8years, p = 0-0062).
AMOSITENo analyses of relations between amosite
F concentrations and possible determinantswere performed as only four workers had diedwithin three years from the end of exposure(with 1956 as the end point for possible expo-sure at the plant).
FIBRE CONCENTRATIONS AND CAUSE OF DEATHClassification of the asbestos cement workersby cause of death gave small numbers foreach asbestos related cause of death (pleuralmesothelioma seven; lung cancer two; lungfibrosis two). Colorectal cancer (n = 4) wasalso examined as a separate category, as arelation between exposure and mortality fromthis cancer was previously found in thecohort.17 Amphibole concentrations in work-ers who died of mesothelioma, lung cancer,or lung fibrosis, were generally higher thanamong workers who died from other causes(table 3). No such pattern was found forchrysotile. Fibre concentrations in workerswho died from colorectal cancer were similarto those among workers who died from otherdiseases.
DiscussionAny relation between intensity of exposure
6 P eL.J 3, 60th Percentile
LI < 60th Percentile
.Postulated categoriesObserved categories
And e
i
209 on M
arch 4, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.3.205 on 1 March 1994. D
ownloaded from

Albin, Pooley, Stromberg, Attewell, Mitha, Johansson, Welinder
and fibre concentrations in lung tissue arelikely to be obscured by several factors.Misclassification of exposure is a problem forthe early period, as no dust measurementswere performed before 1956. Even thereafter,difficulties remain, due to the use of differentmethods, and changes in the strategy formonitoring of dust concentrations. Further,the information on different work tasks per-formed by each worker is incomplete, and sois our information on the use of respirators(note that workers exposed to high concentra-tions of airborne dust are more likely to haveworn respirators). The two exposure variablesused-intensity and duration-are intercorre-lated, as exposure intensities declined withcalendar year of exposure. Thus, workerswith long durations generally also have higherestimated average intensities of exposure.This hampers the possibility of evaluating theexposure variables separately, and mightpartly also explain why cumulative dose didnot contribute more information than averageintensity and duration analysed separately.
Further, fibre type was not characterised inthe sampled dust. Use of crocidolite andamosite was intermittent at the plant, and ispoorly defined for each worker, both in termsof duration and intensity. The finding of astrong association between high concentra-tions of crocidolite and start of employmentin the 1920s and 1930s is useful as it indi-cates that exposure during these decadesmight be considered as an additional deter-minant of risk in further studies of relationsbetween exposure and response.Our material permitted only analyses with
crude methods to evaluate accumulation andelimination, without quantitative estimates ofclearance rates. The fact that those workersobserved in the high, but postulated to be inthe low to intermediate, concentration cate-gories of crocidolite and tremolite fibres,tended to have a higher exposure than theothers, indicates misclassification due to thestrict criteria for postulating that a workerbelonged to the high concentration categoryat the end of exposure. Application of a morecomplicated model to the data yielded highlyunstable estimates (results not presented).
Further, we could not account for thesample site in the lung, as this was usuallyunspecified. Estimates of the importance ofsample site vary between a factor of two andeight (generally, the highest concentrationsare found in the peripheral lower lobe2'-25;and FD Pooley, unpublished data). Clearly,the possible sources of errors already men-tioned imply that our results should be inter-preted with some caution.We found a negative relation between sam-
ple weight and chrysotile concentration. Partof the explanation might be that the dustfrom a heavy sample will be more dense andthus there will be an increased probability ofa covering effect. This would be most likelyto affect thin and short fibres, such aschrysotile.No relations indicating a continuous
increase in chrysotile concentrations in lung
tissue with increasing duration and intensityof exposure were found for workers who diedwithin three years of the end of exposure.The chrysotile fibres recovered from the lungsof these workers have a geometric meanlength of only 1 1 ,um, which is less than halfof the mean chrysotile length found amongtextile workers, and mean lengths for amphi-bole fibres in both groups.26 Thus, as shortfibre size is a determinant for a rapid clear-ance, a comparatively short retention ofchrysotile would be expected in this studyfrom the size data only. The lack of relationsbetween tissue concentration and duration oraverage intensity of exposure is also compati-ble with the observation that workers with ahigh last intensity seemed to have a fasterclearance than those with a low intensity.These findings are in accordance with a pre-vious report indicating an adaptive clearanceof chrysotile, possibly due to an enhancementof macrophage activity through the cytotoxi-city of chrysotile."4
Workers with a high average intensity ofexposure and high chrysotile or tremolitecounts in lung tissue had more pronouncedfibrosis than those with low to intermediateconcentrations. This might indicate animpaired clearance due to the fibrosis as theexposure was not significantly higher in thehigh concentration category, as analysed by acrude stratification. An impaired clearance infibrotic lungs has previously been suggestedby Timbrell.27
Indications of accumulation in lung tissuewith duration of exposure were seen fortremolite and crocidolite. No clear patternsindicating elimination after the end ofexposure were found. This is in accordancewith former findings, mainly from animalstudies,'-7 and among workers from chrysotiletextile and mining industries,28 that elimina-tion is slow for amphibole asbestos.
Interestingly, there were indications of anassociation between tobacco consumptionand high category of tissue concentrations ofchrysotile and crocidolite (but not tremolite).Stratification on the other time dependentdeterminants, however, indicated that theassociation found for chrysotile, might beconfounded by duration (and year) ofemployment. Thus the association we foundbetween tobacco consumption and chrysotileconcentrations should be interpreted withsome care.A causal association is, however, supported
by previous findings. In a series of cases oflung cancer, high tobacco consumption wasassociated with high total particle counts inlung tissue.29 Further, an increased accumula-tion of amosite fibres has been found in thebronchial walls of experimental animalsexposed to cigarette smoke.30 A positive asso-ciation between tobacco consumption andaccumulation of asbestos fibres might partlyexplain why smokers are more likely thannon-smokers to develop fibrosis3" and lungcancer32 when exposed.
Comparisons of fibre concentrations andcause of death displayed generally higher
210 on M
arch 4, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.51.3.205 on 1 March 1994. D
ownloaded from

Retention patterns of asbestos fibres in lung tissue among asbestos cement workers
amphibole concentrations for asbestos relateddiagnoses than other diseases, whereas thecomparisons were similar for chrysotile con-centrations. The results should be interpretedwith care due to the small numbers in eachgroup of asbestos related diagnoses. They are,however, in agreement with previous findingsmade among east London factory workers.
This study shows different kinetics foramphibole and chrysotile fibres in humanlung tissue. Amphibole fibre concentrationsincrease with duration of exposure, whereaschrysotile concentrations do not. Further-more, it supports a former finding of a pos-sible adaptive clearance of chrysotile. Also,we found indications of an impaired clear-ance among workers with fibrosis and work-ers with a high tobacco consumption. Theassociation between increased amphiboleconcentrations in lung tissue and death fromasbestos related causes suggests that workerswho died from these causes had a higheramphibole exposure or a poorer clearance ofthese fibres than the others. The findings thussupport the hypothesis that adverse effects areassociated rather with the fibres retained(amphiboles), than with the ones beingcleared (largely chrysotile).
This study was supported by grants from the Swedish WorkEnvironment Fund and from the Medical Faculty, LundUniversity. Lars Rylander, MSc, made the graphs. This isgratefully acknowledged.
1 Wagner JC. Mesothelioma and mineral fibers. Cancer1986;57:1905-1 1.
2 Doll R, Peto J. Asbestos. Effects on health of exposure toasbestos. A report to the Health and Safety Commission.London: HMSO 1985.
3 Wagner JC, Skidmore JW. Asbestos dust deposition andretention in rats. Ann N YAcad Sci 1965;132:77-86.
4 Wagner JC, Berry G, Skidmore JW, Timbrell V. Theeffects of inhalation of asbestos in rats. Br J Cancer1974;29:252-69.
5 Middleton AP, Beckett ST, Davis JMG. A study of theshort-term retention and clearance of inhaled asbestosusing UICC standard reference samples. In: WaltonWH, ed. Inhaled particles IV. Oxford: Pergamon Press,1977:247-57.
6 Wagner JC, Griffiths DM, Munday DE. Recent investiga-tions in animals and humans. In: Wagner JC, ed.Biological effects of chrysotile (Accomplishments inOncology. Vol 1. No 2). Philadelphia: Lippincott, 1986:,111-20.
7 Churg A, Wright JL, Gilks B, Depaoli L. Rapid short-term clearance of chrysotile compared with amositeasbestos in the guinea pig. Am Rev Respir Dis 1989;139:885-90.
8 Morgan A. Effect of length on the clearance of fibres fromthe lung and on body formation. In: Wagner JC, ed.Biological effects of mineral fibres. Lyon: IARC, 1980:vol1, 329-35. (IARC Sci Publ No 30).
9 Pooley FD, Clark NJ. A comparison of fibre dimensionsin chrysotile, crocidolite and amosite particles fromsamples of airborne dust and from post-mortem lungtissue specimens. In: Wagner JC, ed. Biological effects ofmineralfibres. Lyon: IARC, 1980: vol 1, 79-86. (IARCSci Publ No 30).
10 Davis JMG, Jones AD. Comparisons of the pathogenicityof long and short fibres of chrysolite asbestos in rats. Br_J Exp Pathol 1988;69:717-37.
11 Davis JMG. Mineral fibre carcinogenesis: experimentaldata relating to the importance of fibre type, size, depo-sition, dissolution and migration. In: Bignon J, Peto J,Saracci R, eds. Non-occupational exposure to mineralfibres. Lyon: IARC, 1989:33-45. (IARC Sci Publ No90).
12 Pooley FD. An examination of the fibrous mineral contentof asbestos lung tissue from the Canadian chrysotilemining industry. Environ Res 1976;12:281-98.
13 Rowlands N. Gibbs GW, McDonald AD. Asbestos fibresin the lungs of chrysotile miners and millers-a pre-liminary report. Ann Occup Hyg 1982;26:411-5.
14 Sebastien P. Begin R, Case BW, McDonald JC.Inhalation of chrysotile dust. In: Wagner JC, ed.Biological effects of chrysotile (Accomplishments inOncology. Vol 1. No 2). Philadelphia: Lippincott, 1986:19-29.
15 Du Toit RSJ. An estimate of the rate at which crocidoliteasbestos fibres are cleared from the lung. Ann OccupHyg 1991;35:433-8.
16 Berry G, Rogers AJ, Pooley FD. Mesotheliomas-asbestosexposure and lung burden. In: Bignon J, Peto J, SaracciR, eds. Non-occupational exposure to mineralfibres. Lyon:IARC, 1989:486-96. (IARC Sci Publ No 90).
17 Albin M, Jakobsson K, Attewell R, Johansson L, WelinderH. Mortality and cancer morbidity in cohorts ofasbestos cement workers and referents. Br J Ind Med1990;47:602-10.
18 Johansson L, Albin M, Jakobsson K, Welinder H,Ranstam J, Attewell R. Ferruginous bodies and pul-monary fibrosis in dead low to moderately exposedasbestos cement workers: histological examination. Br _7Ind Med 1987;44:550-8.
19 Albin M, Johansson L, Pooley FD, Jakobsson K, AttewellR, Mitha R. Mineral fibres, fibrosis, and asbestos bodiesin lung tissue from deceased asbestos cement workers.BrJ Ind Med 1990;47:767-74.
20- Addison J, Davies LST. Analysis of amphibole asbestos inchrysotile and other minerals. Ann Occup Hyg 1990;34:159-75.
21 Pooley FD, Clark NJ. Quantitative assessment of in-organic fibrous particulates in dust samples with ananalytical transmission electron microscope. Ann OccupHyg 1979;22:253-71.
22 Fisher RA. Statistical methods for research workers. 10th ed.Edinburgh: Oliver and Boyd, 1948.
23 Sebastien P, Fondimare A, Bignon J, Monchaux G,Desbordes J, Bonnaud G. Topographical distribution ofasbestos fibres in human lung in relation to occupa-tional and non-occupational exposure. In: Walton WH,ed. Inhaled particles IV. Edinburgh 1975. Part 2. Oxford:Pergamon Press, 1977:435-46.
24 Churg A, Wood P. Observations on the distribution ofasbestos fibers in human lungs. Environ Res 1983;31:374-80.
25 Morgan A, Holmes A. Distribution and characteristics ofamphibole asbestos fibres, measured with the lightmicroscope, in the left lung of an insulation worker. BrJ7Ind Med 1983;40:45-50.
26 Pooley FD, Mitha R. Fiber types, concentrations andcharacteristics found in lung tissues of chrysotile-exposed cases and controls. In: Wagner JC, ed.Biological effects of chrysotile. (Accomplishments inOncology. Vol 1. No 2). Philadelphia: Lippincott, 1986:1-11.
27 Timbrell V. Pulmonary deposition and retention of SouthAfrican amphibole fibres; identification of asbestosis-related measure of fibre concentration. In: Proceedings ofthe VIth International Pneumoconiosis Conference. Geneva:International Labour Office, 1984;2:997-1008.
28 Sebastien P, McDonald JC, McDonald AD, Case B,Harley R. Respiratory cancer in chrysotile textile andmining industries: exposure inferences from lung analy-sis. BrJ Ind Med 1989;46:180-7.
29 Churg A, Wiggs B. Mineral particles, mineral fibres, andlung cancer. Environ Res 1985;37:364-72.
30 McFadden D, Wright J, Wiggs B, Churg A. Cigarettesmoke increases the penetration of asbestos fibres intoairway walls. Am _7 Pathol 1986;123:95-9.
31 Kilburn KH, Lilis R, Anderson HA, Miller A, WarshawRH. Interaction of asbestos, age and cigarette smokingin producing radiographic evidence of diffuse pul-monary fibrosis. AmjMed 1986;80:377-81.
32 Saracci R. Asbestos and lung cancer: an analysis of theepidemiological evidence on the asbestos-smoking inter-action. Int3'Cancer 1977;20:323-31.
33 Wagner JC, Newhouse ML, Corrin B. Rossiter CE,Griffiths DM. Correlation between fibre content ofthe lung and disease in east London asbestos factoryworkers. BrJ Ind Med 1988;45:305-8.
211
on March 4, 2021 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.51.3.205 on 1 M
arch 1994. Dow
nloaded from