Results of therapeutic cranial irradiation in small cell lung cancer
5
In1 J. Radfalwn Oncology Bml Phys.. Vol. 14. pp. 455-459 O360-3016/M $3.00 t .OO Printed in the U.S.A. All rights rexned. Copyright 0 I Y88 Pergamon Journals Ltd. ?? Original Contribution RESULTS OF THERAPEUTIC CRANIAL IRRADIATION IN SMALL CELL LUNG CANCER JAMES CARMICHAEL, M.B., CH.B., JEFFREY M. CRANE, M.D., PAUL A. BUNN, M.D., ELI GLATSTEIN, M.D. AND DANIEL C. IHDE, M.D. NCI-Navy Medical Oncology and Radiation Oncology Branches, National Cancer Institute and Naval Hospital, and the Departments of Medicine and Radiology, Uniformed Services University of the Health Sciences, Bethesda. MD A large proportion of patients with small cell lung cancer develop intracranial metastases which are often severely disabling. The optimal radiotherapeutic program for treating these metastases is unknown. We therefore evalu- ated objective response rates, response duration, and survival after therapeutic cranial irradiation in 59 patients with proven brain metastases from small cell lung cancer. Objective responses to a variety of doses and schedules were observed in 37 (63%) patients. However, progression of intracranial disease after radiotherapy was common, with 24 responding patients having relapsed in the brain prior to death. The actuarial likelihood of remaining free of progressive brain tumor at 1 year was only 37% in complete and 0% in partial responders. Patients who received radiation doses of more than 40 Gy had longer response durations than those given lower doses, although patient selection could well explain this observation. Brain metastases presenting after initiation of systemic chemother- apy or occurring in conjunction with other sites of extrathoracic disease were associated with a poor prognosis. In patients who present with brain metastases as the sole site of metastatic disease, higher doses of cranial irradiation should be considered, in view of the high intracranial relapse rate associated with currently accepted dose and fractionation schedules. Small cell lung cancer, Brain metastases, Therapeutic cranial irradiation. INTRODUCTION Cerebral metastases, which are frequently severely dis- abling, are a common clinical manifestation of small cell lung cancer (SCLC).13 Approximately 10% of SCLC pa- tients present with brain metastases at the time of diag- nosis,5*‘4 and such metastases develop in an additional 20-25% of patients later in their clinical course, often simultaneously with progressive extracranial tumor. Some authors have suggested that there is no significant difference in median survival between SCLC patients with limited disease and those having brain metastases as the sole site of extensive stage disease at presentation.r6 However, the prognosis is extremely poor for patients with subsequent appearance of brain metastases, in whom systemic disease control is usually the predomi- nant factor affecting survival. With recent improvement in systemic therapy of SCLC, the question arises whether standard palliative doses of cranial irradiation which are customarily given are optimal. We therefore studied the therapeutic effects of cranial irradiation, in terms of both response rate and duration, in our SCLC patients in whom brain metastases were detected. METHODS AND MATERIALS The records of all patients with histologically con- firmed small cell lung cancer who were irradiated for pre- sumed brain metastases at the NCI-Navy Medical On- cology and Radiation Oncology Branches between No- vember 1977, and November 1983, were reviewed. All brain metastases were diagnosed on the basis of abnor- malities on computed tomographic (CT) and/or radio- nuclide brain scans. Details of brain imaging results in some of these patients have previously been reported.6 Patients were grouped according to whether their brain metastases were diagnosed at presentation or developed subsequently, whether the brain metastases were the sole site of extrathoracic metastatic disease or whether there Presented at the 74th Annual Meeting of the American Asso- ciation for Cancer Research, San Diego, CA, May 25, 1983. The opinions and assertions contained herein are the private Reprint requests to: Daniel C. Ihde, M.D., NCI-Navy Medi- cal Oncology Branch, Bldg. 8. Rm. 5 10 1, Naval Hospital, Bethesda, MD 208 14. views of the authors and are not to be construed as official or reflecting the views of the Department of the Navy or the De- partment of Defense. Accepted for publication 29 September 1987. 455
-
Upload
james-carmichael -
Category
Documents
-
view
214 -
download
2
Transcript of Results of therapeutic cranial irradiation in small cell lung cancer

In1 J. Radfalwn Oncology Bml Phys.. Vol. 14. pp. 455-459 O360-3016/M $3.00 t .OO
Printed in the U.S.A. All rights rexned. Copyright 0 I Y88 Pergamon Journals Ltd.
??Original Contribution
RESULTS OF THERAPEUTIC CRANIAL IRRADIATION IN SMALL CELL LUNG CANCER
JAMES CARMICHAEL, M.B., CH.B., JEFFREY M. CRANE, M.D., PAUL A. BUNN, M.D., ELI GLATSTEIN, M.D. AND DANIEL C. IHDE, M.D.
NCI-Navy Medical Oncology and Radiation Oncology Branches, National Cancer Institute and Naval Hospital, and the Departments of Medicine and Radiology, Uniformed Services University of the Health Sciences, Bethesda. MD
A large proportion of patients with small cell lung cancer develop intracranial metastases which are often severely disabling. The optimal radiotherapeutic program for treating these metastases is unknown. We therefore evalu- ated objective response rates, response duration, and survival after therapeutic cranial irradiation in 59 patients with proven brain metastases from small cell lung cancer. Objective responses to a variety of doses and schedules were observed in 37 (63%) patients. However, progression of intracranial disease after radiotherapy was common, with 24 responding patients having relapsed in the brain prior to death. The actuarial likelihood of remaining free of progressive brain tumor at 1 year was only 37% in complete and 0% in partial responders. Patients who received radiation doses of more than 40 Gy had longer response durations than those given lower doses, although patient selection could well explain this observation. Brain metastases presenting after initiation of systemic chemother- apy or occurring in conjunction with other sites of extrathoracic disease were associated with a poor prognosis. In patients who present with brain metastases as the sole site of metastatic disease, higher doses of cranial irradiation should be considered, in view of the high intracranial relapse rate associated with currently accepted dose and fractionation schedules.
Small cell lung cancer, Brain metastases, Therapeutic cranial irradiation.
INTRODUCTION
Cerebral metastases, which are frequently severely dis- abling, are a common clinical manifestation of small cell lung cancer (SCLC).13 Approximately 10% of SCLC pa- tients present with brain metastases at the time of diag- nosis,5*‘4 and such metastases develop in an additional 20-25% of patients later in their clinical course, often simultaneously with progressive extracranial tumor. Some authors have suggested that there is no significant difference in median survival between SCLC patients with limited disease and those having brain metastases as the sole site of extensive stage disease at presentation.r6 However, the prognosis is extremely poor for patients with subsequent appearance of brain metastases, in whom systemic disease control is usually the predomi- nant factor affecting survival. With recent improvement in systemic therapy of SCLC, the question arises whether standard palliative doses of cranial irradiation which are customarily given are optimal. We therefore studied the
therapeutic effects of cranial irradiation, in terms of both response rate and duration, in our SCLC patients in whom brain metastases were detected.
METHODS AND MATERIALS
The records of all patients with histologically con- firmed small cell lung cancer who were irradiated for pre- sumed brain metastases at the NCI-Navy Medical On- cology and Radiation Oncology Branches between No- vember 1977, and November 1983, were reviewed. All brain metastases were diagnosed on the basis of abnor- malities on computed tomographic (CT) and/or radio- nuclide brain scans. Details of brain imaging results in some of these patients have previously been reported.6 Patients were grouped according to whether their brain metastases were diagnosed at presentation or developed subsequently, whether the brain metastases were the sole site of extrathoracic metastatic disease or whether there
Presented at the 74th Annual Meeting of the American Asso- ciation for Cancer Research, San Diego, CA, May 25, 1983.
The opinions and assertions contained herein are the private
Reprint requests to: Daniel C. Ihde, M.D., NCI-Navy Medi- cal Oncology Branch, Bldg. 8. Rm. 5 10 1, Naval Hospital, Bethesda, MD 208 14.
views of the authors and are not to be construed as official or reflecting the views of the Department of the Navy or the De- partment of Defense.
Accepted for publication 29 September 1987.
455

456 1. J. Radiation Oncology 0 Biology 0 Physics March 1988. Volume 14. Number 3
were multiple extrathoracic metastatic sites, and whether or not the patients had symptoms relating to their brain metastases.
As previously described, all patients first underwent a detailed staging evaluation including radionuclide or CT brain scans or both and then received intensive induc- tion chemotherapy with either cyclophosphamide, doxo- rubicin, etoposide, and vincristine3 or cyclophospha- mide, methotrexate, and lomustine alternating with vin- &tine, doxorubicin, and procarbazine (CMC/VAP).4 Some patients with limited stage disease also received ir- radiation to the intrathoracic tumor as part of a random- ized trial.’ All patients with brain metastases at presenta- tion were given induction chemotherapy. However, sys- temic treatment of patients with delayed presentation of brain metastases was individualized according to the pa- tient’s performance status, disease extent, and response to prior or current systemic therapy.
Systemic corticosteroids were administered to all pa- tients receiving therapeutic cranial irradiation. Radia- tion dose and fractionation schedules were variable de- pending upon the patient’s performance and disease sta- tus; patients with poor performance status and with persistent systemic disease generally received shorter courses (12 weeks) and lower doses of radiation. Radia- tion was administered via a number of sources. Approxi-
Table 1. Characteristics of patients irradiated for brain metastases
Characteristics No.
Number of patients irradiated 61 Excluded patients* 2 Evaluable patients 59
Sex Male Female
Age in years, mean (range)
44 15
56.4 (34-70)
Time of diagnosis of brain metastases Presentation Delayed
Extent of extrathoracic disease Sole extrathoracic site Multiple extrathoracic sites
23 36
18 41
Symptomatic status Symptomatic Asymptomatic
39 20
Prior prophylactic cranial irradiation Yes No
11 48
Therapeutic radiation dose ~30 Gy 30-39.99 Gy 240 Gy
11 21 27
* 1 irradiated after surgical resection, 1 aspergilloma at au- topsy.
mately one-third of patients were treated using a “Co source, with the remainder treated using 4 MeV, 6 MeV, or 10 MeV linear accelerators. All patients received con- tinuous (not split course) radiotherapy. Dose per fraction ranged from 2 to 4 Gy. Forty Gy in 16 fractions of 2.5 Gy each over 4 weeks was the most frequently used treat- ment schedule, being given to 20 patients. Five addi- tional patients received 2.5 Gy fractions four times per week to total doses of 35-45 Gy.
Complete response to brain irradiation was defined as disappearance of signs and symptoms of brain metasta- ses and normalization of previously abnormal brain scans. Partial response represented improvement of signs and symptoms of brain metastases and brain scan evi- dence of a 50% reduction in the size of the brain tumor. In a few patients with brief partial responses, repeat im- aging studies were not performed. All other patients were considered non-responders, except that no attempt was made to assess response in patients dying within 8 weeks of the beginning of radiotherapy. This latter group was designated as having early death. Response duration was measured from the initiation of radiotherapy to the de- velopment of recurrent neurologic symptoms or worsen- ing or recurrence of abnormalities on brain imaging studies. Actuarial survival from the initiation of brain ra- diotherapy and duration of intracranial response to ther- apy were assessed by the product-limit method of Kaplan and Meier.’ In analyzing response duration, patients dying without evidence of progressive brain metastases were censored at the time of death.
RESULTS
Patient characteristics Sixty-one patients were diagnosed as having brain me-
tastases over this period. Two patients were considered ineligible for evaluation of the effects of radiotherapy. The first presented with a brain metastasis as his sole ex- trathoracic tumor site. He underwent surgical resection of his brain metastasis with postoperative radiotherapy to the brain, and then received CMC/VAP. He remains in apparent remission nearly 4 years later. The second patient presented with widespread metastatic disease and began therapy with CMC/VAP and whole brain irradia- tion for presumed metastatic disease. The patient ex- pired 6 weeks later, but at autopsy was found to have an aspergilloma in the brain.
Clinical characteristics of our patients are listed in Ta- ble 1. There were 44 men and 15 women with an average age of 56.4 years. Brain metastases were present at diag- nosis in 23 patients, and developed subsequently in an additional 36. The brain was the sole extrathoracic meta- static site in 18 cases and one of multiple sites in 4 1 pa- tients. Thirty-nine patients had symptoms relating to their metastases, whereas the remaining 20 were asymp- tomatic. The range of irradiation doses varied considera- bly as shown in Table 1. Nine of the 11 patients with

Therapeutic cranial irradiation in small cell lung cancer 0 J. CARMICHAEL et a/. 451
Table 2. Response to cranial irradiation
Time of brain metastases
Presentation Delayed All patients
No. patients
23 36 59
Complete response (%)
9 (39.1) 10 (27.8) 19 (32.2)
Partial response (%)
8 (34.8) 10 (27.8) 18 (30.5)
No response (%)
3(13.0) 4(11.1) 7(11.8)
Early death (%)
3 (13.0) 12 (33.3) 15 (25.4)
previous prophylactic cranial irradiation (PCI) received total doses of 30 Gy or less.
Response rate and duration Response rates to cranial irradiation according to the
time of presentation of brain metastases are given in Ta- ble 2. Thirty-seven patients (62.7%) achieved an objec- tive response to radiation, including 32.2% with a com- plete response, with higher response rates (73.9% vs. 55.6%) in patients treated for brain metastases at the time of presentation of SCLC. Fifteen patients died within 8 weeks and were not formally assessed for response; thus, the objective response rate was 84.0% in patients surviv- ing 2 months or longer.
Of the 37 patients who achieved an objective response, 24 developed recurrent or progressive tumor in the brain prior to death, including 8119 complete and 16/ 18 par- tial responders. Median actuarial response duration was 10 months for complete and 5 months for partial re- sponders (Fig. 1). The likelihood of remaining in re- sponse was 37% at 14 months in complete and 0% at 12 months in partial responders. However, these estimated relapse rates are likely to be underestimates, as autopsies including examination of the brain were performed in only two patients dying while still in response.
An attempt was made to relate response duration to dose of irradiation administered in patients surviving longer than 8 weeks. For this analysis, non-responding patients were assumed to have a response duration of zero. Actuarial median response duration was 0 months in four patients receiving less than 30 Gy, 5 months in 13 patients given 30-39.99 Gy, and 7 months in 2 1 patients given 40 Gy. In the six patients receiving more than 40 Gy, median response duration was 10 months.
Survival Data on survival from initiation of radiotherapy in
each patient subgroup are listed in Table 3. Patients pre- senting with brain metastases had much better survival than those with delayed development of metastases (me- dian survival 7 and 3 months, respectively). Therefore, survival in relation to other characteristics was deter- mined separately for patients with initial and delayed presentation of metastases. In both groups, patients whose brain metastases were the sole site of extrathoracic tumor appeared to live longer. As previously reported,6 there was no suggestion that the presence or absence of neurologic symptoms affected survival, presumably be-
cause extracranial tumor extent was the principal factor influencing life span in most patients. Radiation doses of 40 Gy or above were associated with better survival in patients with delayed brain metastases. However, it must be emphasized that the radiation dose and fractionation schedule employed were affected by the patients’ clinical status.
The 11 patients who received PC1 as part of their pri- mary management did uniformly poorly when treated for later brain metastases. Although four achieved an ob- jective response, the median survival of this group was less than 2 months, with 5 months maximum survival.
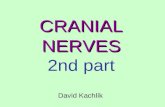
TOTAL FAIL -CR 19 8 _-__ pfq 18 16
I---- l
I
k I __
I .-_- _--, I I I
I I 1 I I 1 I 1 2 4 6 8 10 12 14 16
DURATION IN MONTHS
Fig. 1. Actuarial duration of response to cranial irradiation for patients with complete and partial response. Median response duration is 10 months for complete and 5 months for partial responders.

458 I. J. Radiation Oncology 0 Biology 0 Physics March 1988. Volume 14, Number 3
Table 3. Survival from initiation of brain irradiation
All patients
Extent of extrathoracic disease Sole site Multiple sites
Symptomatic status Symptomatic Asymptomatic
Therapeutic radiation dose ~30 Gy 30-39.99 Gy 240 Gy
Brain metastases at presentation
No. pts Survival, months
23 7 (l-18)*
11 9 (1-18) 12 5 (l-15)
13 9 (l-18) 10 5 (1.5-14.5)
1 1.5 (1.5) 7 9 (l-15)
15 7 (2-18)
Delayed brain metastases
No. pts Survival, months
36 3 (l-12)
7 4.5(1-12) 29 2 (1-12)
26 2 (1-12) 10 3 (1-12)
10 1 (l-3) 14 2 (l-12) 12 6 (2.5-12)
* Median survival (range of survival).
Median survival in patients without prior PC1 treated for and 54% of 39 patients failing to have neurologic symp- delayed brain metastases was 3 months. toms controlled at the time of death in the latter.
A second course of cranial irradiation was given to 12 of 24 initially responding patients who relapsed. Median survival of retreated patients was 3 months, although two patients lived 10 and 13 months from development of recurrent brain metastases. Median survival of relapsing patients not judged suitable for repeat irradiation was less than 1 month.
DISCUSSION
The probability of developing brain metastases in SCLC increases with increasing survival, with the actuar- ial probability of brain metastases rising to 60-80% for patients surviving more than 2 years.“,14 Many studies have shown that PC1 can decrease the incidence of cere- bral relapse. lo Overall, such prophylactic irradiation has failed to yield improved survival, and the benefit of re- duction in clinically detectable brain metastases has been principally confined to the select group of patients who achieve a complete clinical response to systemic chemo- therapy. ‘J Patients who fail to achieve a complete re- mission frequently relapse in the brain despite the ad- ministration of PCI,’ ‘*I5 presumably from a reseeding phenomenon.
Although none of these three reports defined the actu- arial durability of responses to brain irradiation or re- quired confirmation of response by improvement in brain imaging studies, our results are not dissimilar. In our study, 65% of the 37 patients who achieved an objec- tive response to therapeutic cranial irradiation had re- lapsed in the brain prior to death. The median duration of partial response was 5 months, with an estimated 100% of patients eventually progressing intracranially, and 63% of complete responders had relapsed by 10 months by actuarial analysis. Termination of intra- cranial tumor response in most of these patients is likely to be related to inadequacy of the radiotherapy program which was administered, but reseeding of the brain from persistent systemic cancer may well have occurred in some instances.
Surprisingly little information is available concerning the efficacy of therapeutic cranial irradiation in the treat- ment of established brain metastases in SCLC. In the re- port by Baglan et aL2 64% of 39 patients with proven brain metastases achieved complete palliation of neuro- logical symptoms for the remainder of their lives. These authors concluded that therapeutic irradiation con- trolled intracranial tumor as well as prophylactic irradia- tion. The reports of Cox et al.’ and Lucas et al. I2 are less sanguine, with brain metastases being a contributing cause of death in 45% of 40 patients in the former study
We believe this limited ability of cranial irradiation to achieve long-term control of overt brain metastases in SCLC actually strengthens the argument for manage- ment of metastases which might eventually become clin- ically detectable with early prophylactic rather than later therapeutic cranial irradiation, especially in limited stage patients who respond completely to systemic therapy. Because of lack of proven survival benefits and neuro- logic impairments sometimes observed in long-term sur- vivors of SCLC that may be partially attributed to PCI,’ however, we do not think an unequivocal recommenda- tion for its use is presently justified.
Despite these inadequacies of brain irradiation in con- trolling overtly metastatic SCLC, it remains true that this is a widely disseminated disease and treatment of brain metastases will have little effect on survival in most pa- tients. In contrast to the results of Lucas et al., I2 systemic disease was the predominant factor influencing survival in all our patients who survived more than 2 months. In some of our patients living less than 2 months, however,

Therapeutic cranial irradiation in small cell lung cancer 0 J. CARMICHAEL et al. 459
morbidity from central nervous system disease was a more significant problem. Therefore palliation for the short term is a reasonable goal of irradiation for most SCLC patients with brain metastases. It is only the occa- sional patient with prospects for more prolonged survival in whom the durability of therapeutic effects becomes relevant. In general, these patients include those who have brain metastases as the sole site of extrathoracic dis- ease at diagnosis and those with limited stage disease whose response to systemic therapy, particularly if a complete response, is terminated by the development of isolated intracranial tumor. The question that remains to be answered is whether higher doses of irradiation will provide better long-term control of brain metastases in these selected patients.
In agreement with the study of Lucas et a1.,12 we found that patients who received higher radiation doses lived longer, although it is highly likely that patient selection
was important in producing this correlation. Perhaps more importantly, we found that doses of irradiation above 40 Gy were associated with longer control of intra- cranial disease, although this observation is based on only six patients and could also be related to patient se- lection factors.
In conclusion, the irradiation schedules customarily used for treatment of brain metastases in SCLC are highly likely to fail to eradicate intracranial tumor in the occasional patient whose systemic cancer enters a dura- ble complete remission. In patients with brain metastases as the sole site of distant metastatic disease where rela- tively prolonged survival can sometimes result,16 it may be appropriate to consider treatment with higher radia- tion doses of more than 40 Gy. If further improvements in systemic therapy of SCLC occur, the efficacy of the cranial irradiation which is offered to these patients will assume increasing importance.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
Aroney, R.S., Aisner, J., Wesley, M.N., Whitacre, M.Y., Van Echo, D.A., Slawson, R.G., Wiernik, P.H.: Value of prophylactic cranial irradiation given at complete remis- sion in small cell lung carcinoma. Cancer Treat. Rep. 67: 675-682, 1983. Baglan, R.J., Marks, J.E.: Comparison of symptomatic and prophylactic irradiation of brain metastases from oat cell carcinoma of the lung. Cancer 47: 4 l-45, 198 1. Brower, M., Ihde, D.C., Johnston-Early, M., Bunn, P.A., Cohen, M.H., Carney, D.N., Makuch, R.W., Matthews, M.J., Radice, P.A., Minna, J.D.: Treatment of extensive stage small cell bronchogenic carcinoma. Amer. J. Med. 75: 993-1000,1983. Cohen, M.H., Ihde, DC., Bunn, P.A., Fossieck, B.E., Mat- thews, M.J., Shackney, SE., Johnston-Early, A., Makuch, R.W., Minna, J.D.: Cyclic alternating combination che- motherapy for small cell bronchogenic carcinoma. Cancer Treat. Rep. 63: 163-170, 1979. Cox, J.D., Komaki, R., Byhardt, R.W., Kun, L.E.: Results of whole-brain irradiation for metastases from small cell carcinoma of the lung. Cancer Treat. Rep. 64: 957-96 1, 1980. Crane, J.M., Nelson, M.J., Ihde, DC, Makuch, R.W., Glatstein, E., Zabell, A., Johnston-Early, A., Bates, H.R., Saini, N., Cohen, M.H., Bunn, P.A.: A comparison of computed tomography and radionuclide scanning for de- tection of brain metastases in small cell lung cancer. J. Clin. Oncol. 2: 1017-1024, 1984. Ihde, D.C., Bunn, P.A., Lichter, AS., Cohen, M.H., Ma- kuch, R.W., Carney, D.N., Johnston-Early, A., Minna, J.D., Glatstein. E.: Randomized trial of chemotherapy with or without adjuvant chest irradiation in limited stage small cell lung cancer. In Adjuvant Therapy of Cancer IV, Jones, SE., Salmon, SE. (Eds.). Orlando, Grune & Strat- ton. 1984, pp. 147-155.
8.
9.
10.
11.
12.
13.
14.
15.
16.
Johnson, B.E., Becker, B., Goff, W.B.. Petronas, N., Kreh- biel, M.A., Makuch, R.W., McKenna, G., Glatstein, E., Ihde, D.C.: Neurologic, neuropsychologic. and computed cranial tomography scan abnormalities in 2- to IO-year survivors of small cell lung cancer. J. C/in. Oncol. 3: 1659- 1667, 1985. Kaplan, E.L., Meier, P.: Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 53: 457-48 I. 1958. Komaki, R., Cox, J.D., Whitson, E.: Risk ofbrain metasta- sis from small cell carcinoma of the lung related to length of survival and prophylactic irradiation. Cancer Treat. Rep. 65: 811-814, 1981. Levitt, M., Meikle, A., Murray, N., Weinerman, B.: Oat cell carcinoma ofthe lung: CNS metastases in spite of pro- phylactic brain irradiation. Cancer Treat. Rep. 62: 131- 133, 1978. Lucas, CF.. Robinson, B., Hoskin, P.J., Yarnold, J.R., Smith, I.E., Ford, H.T.: Morbidity of cranial relapse in small cell lung cancer and the impact of radiation therapy. Cancer Treat. Rep. 70: 565-570, 1986. Newman, S.J., Hansen, H.H.: Frequency, diagnosis and treatment of brain metastases in 247 patients with bron- chogenic carcinoma. Cancer 33: 492-496, 1974. Nugent, J.L., Bunn, P.A., Matthews, M.J., Ihde, D.C., Co- hen, M.H., Gazdar, A.F., Minna, J.D.: CNS metastases in small cell bronchogenic carcinoma. Cancer 44: 1885- 1893, 1979. Rosen, S.T., Makuch, R.W., Lichter, A.S., Ihde. D.C., Matthews, M.J., Minna, J.D., Glatstein, E., Bunn, P.A.: Role of prophylactic cranial irradiation in prevention of central nervous system metastases in small cell lung can- cer. Amer. J. Med. 74: 615-623, 1983. Van Hazel, G.A., Scott, M., Eagan, R.T.: The effect of CNS metastases on the survival of patients with small cell carci- noma of the lung. Cancer 51: 933-937, 1983.