
Results of interferon-alpha therapy in patients with chronic myelogenous leukemia 60 years of age...
4
Results of Interferon-Alpha Therapy in Patients With Chronic Myelogenous Leukemia 60 Years of Age and Older Jorge Cortes, MD, Hagop Kantarjian, MD, Susan O’Brien, MD, L.E. Robertson, MD, Sherry Pierce, RN, Moshe Talpaz, MD, Houston, Texas PURPOSE: To determine the response rate to interferon-alpha (IFN-CX) in patients with chronic myelogenous leukemia (CML) aged 60 years and older. PATIENTS AND METHODS: Patients with CML aged 60 years and older included in all protocols with IFN-(11 therapy for early chronic phase CML at the M.D. Anderson Cancer Center were analyzed. They were treated with human leukocyte or recombinant human IFN-a 5x 106 U/m* daily alone or in combination with hydroxyurea or IFN gamma. The clinical characteristics of the patients were analyzed and their hematologic and cytogenetic responses to IFN-a and survival from the initiation of therapy were determined. Results were compared with those of younger patients treated in the same protocols. Treatment-related toxicity was also analyzed. RESULTS: Thirty-five of 274 (13%) patients included in trials of IFN-a-based regimens for CML were 60 years and older. Older patients had a higher percentage of bone marrow blasts (P = 0.04) and basophils (P = 0.09) than younger patients. Sixty-nine percent achieved a complete hematologic remission with IFNw therapy, and 51% had a cytogenetic response, which was major in 26% and complete (Philadelphia chromosome-positive cells = 0%) in 20%. Their median survival was 64 months, and the estimated 5-year survival rate was 62%. These results were not different from those in younger patients. Twenty-two patients (63%) had at least grade 2 toxicity requiring dose adjustment. The most frequent side effects were neurotoxicity in 31% and chronic fatigue in 29%. CONCLUSIONS: Patients with CML 60 years of age and older respond well to IFN-a therapy, but experience more toxicity. This therapy should be considered for these patients if they are otherwise in good condition, with careful attention to IFNw toxicity and its management. From the Department of Hematology (JC, HK, SO, LER, SP) and Section of Biologic Studres (MT), University of Texas, M.D. Anderson Cancer Center, Houston, Texas. Requests for reprrnts should be addressed to Hagop Kantarjian, MD, Department of Hematology, M.D. Anderson Cancer Center, 1515 Holcombe Boulevard Box 61, Houston, Texas 77030. Manuscript submitted March 2, 1995 and accepted in rewed form December 13, 1995. C hronic myelogenous leukemia (CML) is a clonal myeloproliferative disorder characterized by the presence of a translocation t(9;2f!)(q34;qll) known as the Philadelphia chromosome (Ph).‘J It has a biphasic or triphasic course with a chronic phase that lasts a median of 5 to 7 years in recent tri- als. It eventually progresses to a blastic phase, which is almost inevitably fatal.’ This may be preceded by an accelerated phase. Although treatment with con- ventional chemotherapy such as busulfan and hy- droxyurea can control the hematologic manifesta- tions of the disease, Ph-positive clonal leukemic cells still predominate, and the final outcome is mostly un- affected.” To date, only two approaches have proven effective in producing long-lasting suppression of the Ph-positive cells, resulting in prolonged survival: al- logeneic bone marrow transplantation (BMT)“-7 and interferon alpha (IFN-a).8vQ Approximately loo/oto 20% of all patients with CML are 60 years of age and older. l,l” Most series using BMT limit this treatment option to patients younger than 55 to 60 years of age. 6,Ti Therefore, one potentially useful alternative for these patients at present is IFN-cx ther- apy. In the general population, the rate of complete hematologic remissions is 70% to SO%, and major cy- togenetic remissions are achieved in 20% to 35%.‘a There is little information on the response rate and tolerance to IFN-a in patients aged 60 years and older. The purpose of this analysis was to investigate whether patients aged 60 years and older respond to IFN-a with a similar rate as do younger patients, and to analyze the side effects of IFN-cr therapy in this age group. PATIENTS AND METHODS From 1982 to 1990, 274 consecutive patients with CML in the early chronic phase (ie, <l year from di- agnosis) were treated at M.D. Anderson Cancer Center with IFN-a as their primary therapy. Thirty-five of these patients (13%) were 60 years of age or older at the time of the initiation of therapy and constitute the basis for this report. Informed consent was obtained from all patients according to institutional guidelines. Treatment Protocols Patients were enrolled in different protocols with IFN-a. Eight of the 35 patients were treated with hu- man leukocyte IFN-a; 14 patients received recombi- nant human IFN-a alone (n = 11) or with recombinant 452 April 1996 The American Journal of Medicind Volume 100
-
Upload
jorge-cortes -
Category
Documents
-
view
213 -
download
1
Transcript of Results of interferon-alpha therapy in patients with chronic myelogenous leukemia 60 years of age...

Results of Interferon-Alpha Therapy in Patients With Chronic Myelogenous Leukemia 60 Years of Age and Older Jorge Cortes, MD, Hagop Kantarjian, MD, Susan O’Brien, MD, L.E. Robertson, MD, Sherry Pierce, RN, Moshe Talpaz, MD, Houston, Texas
PURPOSE: To determine the response rate to interferon-alpha (IFN-CX) in patients with chronic myelogenous leukemia (CML) aged 60 years and older.
PATIENTS AND METHODS: Patients with CML aged 60 years and older included in all protocols with IFN-(11 therapy for early chronic phase CML at the M.D. Anderson Cancer Center were analyzed. They were treated with human leukocyte or recombinant human IFN-a 5x 106 U/m* daily alone or in combination with hydroxyurea or IFN gamma. The clinical characteristics of the patients were analyzed and their hematologic and cytogenetic responses to IFN-a and survival from the initiation of therapy were determined. Results were compared with those of younger patients treated in the same protocols. Treatment-related toxicity was also analyzed.
RESULTS: Thirty-five of 274 (13%) patients included in trials of IFN-a-based regimens for CML were 60 years and older. Older patients had a higher percentage of bone marrow blasts (P = 0.04) and basophils (P = 0.09) than younger patients. Sixty-nine percent achieved a complete hematologic remission with IFNw therapy, and 51% had a cytogenetic response, which was major in 26% and complete (Philadelphia chromosome-positive cells = 0%) in 20%. Their median survival was 64 months, and the estimated 5-year survival rate was 62%. These results were not different from those in younger patients. Twenty-two patients (63%) had at least grade 2 toxicity requiring dose adjustment. The most frequent side effects were neurotoxicity in 31% and chronic fatigue in 29%.
CONCLUSIONS: Patients with CML 60 years of age and older respond well to IFN-a therapy, but experience more toxicity. This therapy should be considered for these patients if they are otherwise in good condition, with careful attention to IFNw toxicity and its management.
From the Department of Hematology (JC, HK, SO, LER, SP) and Section of Biologic Studres (MT), University of Texas, M.D. Anderson Cancer Center, Houston, Texas.
Requests for reprrnts should be addressed to Hagop Kantarjian, MD, Department of Hematology, M.D. Anderson Cancer Center, 1515 Holcombe Boulevard Box 61, Houston, Texas 77030.
Manuscript submitted March 2, 1995 and accepted in rewed form December 13, 1995.
C hronic myelogenous leukemia (CML) is a clonal myeloproliferative disorder characterized by
the presence of a translocation t(9;2f!)(q34;qll) known as the Philadelphia chromosome (Ph).‘J It has a biphasic or triphasic course with a chronic phase that lasts a median of 5 to 7 years in recent tri- als. It eventually progresses to a blastic phase, which is almost inevitably fatal.’ This may be preceded by an accelerated phase. Although treatment with con- ventional chemotherapy such as busulfan and hy- droxyurea can control the hematologic manifesta- tions of the disease, Ph-positive clonal leukemic cells still predominate, and the final outcome is mostly un- affected.” To date, only two approaches have proven effective in producing long-lasting suppression of the Ph-positive cells, resulting in prolonged survival: al- logeneic bone marrow transplantation (BMT)“-7 and interferon alpha (IFN-a).8vQ
Approximately loo/o to 20% of all patients with CML are 60 years of age and older. l,l” Most series using BMT limit this treatment option to patients younger than 55 to 60 years of age. 6,Ti Therefore, one potentially useful alternative for these patients at present is IFN-cx ther- apy. In the general population, the rate of complete hematologic remissions is 70% to SO%, and major cy- togenetic remissions are achieved in 20% to 35%.‘a There is little information on the response rate and tolerance to IFN-a in patients aged 60 years and older.
The purpose of this analysis was to investigate whether patients aged 60 years and older respond to IFN-a with a similar rate as do younger patients, and to analyze the side effects of IFN-cr therapy in this age group.
PATIENTS AND METHODS From 1982 to 1990, 274 consecutive patients with
CML in the early chronic phase (ie, <l year from di- agnosis) were treated at M.D. Anderson Cancer Center with IFN-a as their primary therapy. Thirty-five of these patients (13%) were 60 years of age or older at the time of the initiation of therapy and constitute the basis for this report. Informed consent was obtained from all patients according to institutional guidelines.
Treatment Protocols Patients were enrolled in different protocols with
IFN-a. Eight of the 35 patients were treated with hu- man leukocyte IFN-a; 14 patients received recombi- nant human IFN-a alone (n = 11) or with recombinant
452 April 1996 The American Journal of Medicind Volume 100
interferon gamma (IFN-y) (n = 3); and 13 patients received recombinant IFN-a and hydroxyurea The patients’ char- acteristics and response rates in these studies have consistently been similar, and are therefore analyzed as a single group.
The IFN-a was given at a dosage of 5X lo6 U/m’ per day. The dosage was decreased by 25% if patients de- veloped persistent grade 2 toxicity. For grade 3 to 4 toxicities, IFN-a was interrupted until resolution of the adverse effects, and resumed at 50% of the initial dosage. If white blood cell (WBC) counts were lower than 2X 1OVL or platelet counts lower
TABLE I Clinical Characteristics of Patients 60 Years of Age and Older
Characteristic Age 260 Years Age ~60 Years P Value
Soleen size 210 ems 29 22 0.42 White blood ceils ~100~ Peripheral blood
Blasts ~3% Basophils ~7%
Bone marrow Blasts ~5% Basophils ~3%
Platelets 2700x 10q/L Hemoglobin <12g/dL Synthesis model stage
1 2 3
:109/L 44
26 26 0.88 13 13 0.8
17 6 0.04 49 33 0.09 29 20 0.33 41 47 0.62
28 67 36 22 36 11
59 0.14
<O.OOl
Data reported as percentage of patients with each characteristic.
than 60X10g/L, the dosage was re- duced by 25%. For patients treated with IFN-y, the dosage was 0.025 mg/m” per day. Hydroxyurea was given at a dosage of 0.5 to 2 g/d and adjusted to keep the WBC count below 5X10g/L and platelet count above 60X log/L.
Response Criteria Responses were defined as previously described.i’
Briefly, a complete hematologic response was defined as the normalization of the peripheral blood counts and differential, including a WBC count of < 10 X log/L, platelet <450X log/L, no immature peripheral blasts, promyelocytes or myelocytes; and disappearance of all signs and symptoms of the disease. Cytogenetic responses were defined as complete when Ph-posi- tive cells were undetectable by cytogenetic analysis using a Giemsa-banding technique’“; partial if Ph-pos- itive cells constituted between 1% and 34% of cells; and minor if Ph-positive cells represented between 35% and 90%. Patients with less than 35% Ph-positive metaphases (ie, both complete and partial cytoge- netic responses) were considered to have a major cy- togenetic response.
Statistical Analysis The disease characteristics and response to ther-
apy were compared with those in the younger popu- lation. Categorical characteristics were compared us ing a &i-square test. Survival curves were constructed by the method of Kaplan and Meier,13 and compared using a log-rank test. l4 Survival was calculated in all patients from the inmation of therapy with 1FN-o.
RESULTS A total of 35 patients 60 years of age and older were
treated with IFN-a. Their median age was 65 years (range 60 to 76). Their disease characteristics are shown in Table I. When compared with the younger
population treated in a similar way in the same pe- riod of time, patients aged 60 years and ollder had a higher incidence of bone marrow blast percentage 25% (17% versus 6%, P = 0.04), and a trend for a higher incidence of bone marrow basophils 23% (4!9% versus 33%, P = 0.09). Other characteristics of known prog- nostic significance were similar in both age groups.
Patients were also classified according to the pre- viously described synthesis prognostic staging sys- tem.‘” This system identifies four stages of the dis- ease according to the number of identified adverse prognostic features in each patient. Since age 260 years is considered an adverse feature, all patients had a score of 21, but the presence of only 1 poor- prognosis characteristic is still considered1 stage 1, whereas 2 characteristics define stage 2, and 23 fea- tures define stage 3; stage 4 is the accelerated phase. The study population included 9 patients in stage 1, 14 in stage 2, and 12 in stage 3. As per the inclusion criteria, no patients were in stage 4. This i.s in con- trast with the younger patients, of whom 67% were in stage 1,22% in stage 2, and 11% in stage 3 (1’ <O.OOl).
The response to IFN-or is shown in Table II. Twenty-four of the 35 patients (69%) achieved a com- plete hematologic remission. This is comparable to the 81% complete hematologic response rate (194 of 239 patients) in younger patients (P = 0.13). Eighteen pa- tients (51%) had a cytogenetic response. Major cyto- genetic responses were seen in 9 patients (:!6%), 7 of whom (20%) achieved complete cytogenetic remis- sion. These response rates were not different to the response rates in younger patients: any cytogenetic re- sponse in 59% (P = 0.5); major in 39% (P = 0.18); and complete in 27% (P = 0.51). Only 1 of the 7 elderly pa- tients who achieved a complete cytogenetic remission has lost it, for a durable complete cytogenetic remis- sion rate of 86%, which is similar to the 92% rate in younger patients.
April 1996 The American Journal of Medicine@ Volume 100 453
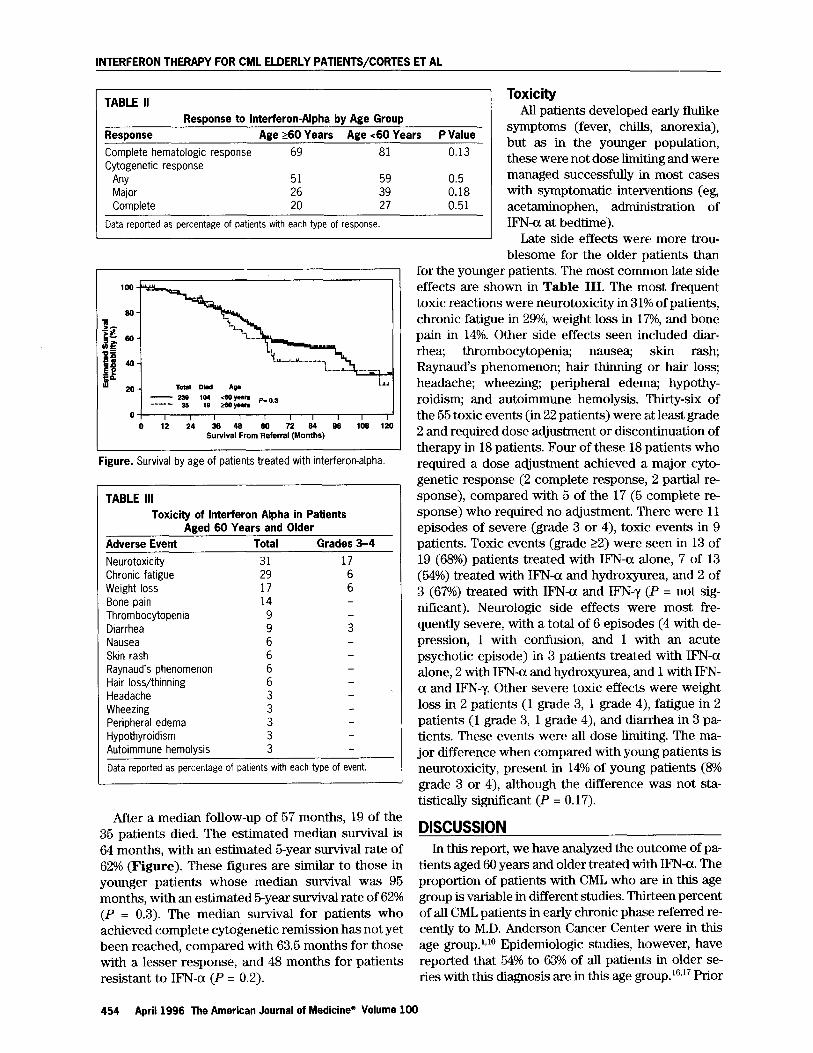
TABLE II Response to Interferon-Alpha by Age Group
Response Age 260 Years Age ~60 Years P Value Complete hematologic response 69 81 0.13 Cytogenetic response
Any 51 59 0.5 Major 26 39 0.18 Complete 20 27 0.51
Data reported as percentage of patients with each type of response.
I
20 - Total Dkd AIP
- 23s 1; -gJ P=S.S ..--‘-- 3s
0 I I I I I I I I I I 0 12 24 38 48 SO 72 04 OS 102 120
Survival From Referral (MonthS)
Figure. Survival by age of patients treated with interferon-alpha.
TABLE III Toxicity of Interferon Alpha in Patients
Aged 60 Years and Older Adverse Event Total Grades 3-4
Neurotoxicity 31 17 Chronic fatigue 29 6 Weight loss 17 6 Bone pain 14 Thrombocytopenia 9 Diarrhea 9 3 Nausea 6 Skin rash 6 Raynaud’s phenomenon 6 -
Hair loss/thinning 6 Headache 3 Wheezing 3 Peripheral edema 3 Hypothyroidism 3 Autoimmune hemolysis 3
Data reported as percentage of patients with each type of event.
After a median follow-up of 57 months, 19 of the 35 patients died. The estimated median survival is 64 months, with an estimated 5-year survival rate of 62% (Figure). These figures are similar to those in younger patients whose median survival was 95 months, with an estimated 5-year survival rate of 62% (P = 0.3). The median survival for patients who achieved complete cytogenetic remission has not yet been reached, compared with 63.5 months for those with a lesser response, and 48 months for patients resistant to IFN-a (P = 0.2).
Toxicity All patients developed early flulike
symptoms (fever, chills, anorexia), but as in the younger population, these were not dose limiting and were managed successfully in most cases with symptomatic interventions (eg, acetaminophen, administration of IFN-cx at bedtime).
Late side effects were more trou- blesome for the older patients than
for the younger patients. The most common late side effects are shown in Table III. The most frequent toxic reactions were neurotoxicity in 31% of patients, chronic fatigue in 29%, weight loss in 17%, and bone pain in 14%. Other side effects seen included diar- rhea; thrombocytopenia; nausea; skin rash; Raynaud’s phenomenon; hair thinning Ior hair loss; headache; wheezing; peripheral edem.a; hypothy- roidism; and autoimmune hemolysis. Thirty-six of the 55 toxic events (in 22 patients) were at least grade 2 and required dose adjustment or discontinuation of therapy in 18 patients. Four of these 18 patients who required a dose adjustment achieved a major cyto- genetic response (2 complete response, 2 partial re- sponse), compared with 5 of the 17 (5 complete re- sponse) who required no adjustment. There were 11 episodes of severe (grade 3 or 4), toxic events in 9 patients. Toxic events (grade 22) were seen in 13 of 19 (68%) patients treated with IFN-a alone, 7 of 13 (54%) treated with IFN-a and hydroxyurea, and 2 of 3 (67%) treated with IFN-a and IFN-y (P = not sig- nificant). Neurologic side effects were most fre- quently severe, with a total of 6 episodes (4 with de- pression, 1 with confusion, and 1 with an acute psychotic episode) in 3 patients treated with IFN-a alone, 2 with IFN-a and hydroxyurea, and 1 with IFN- a and IFN-?I. Other severe toxic effects were weight loss in 2 patients (1 grade 3, 1 grade 4), fatigue in 2 patients (1 grade 3, 1 grade 4), and diarrhea in 3 pa- tients. These events were all dose limiting. The ma- jor difference when compared with young patients is neurotoxicity, present in 14% of young patients (8% grade 3 or 4), although the difference was not sta- tistically significant (P = 0.17).
DISCUSSION In this report, we have analyzed the outcome of pa-
tients aged 60 years and older treated with 1FN-a. The proportion of patients with CML who are in this age group is variable in different studies. Thirteen percent of all CML patients in early chronic phase referred re- cently to M.D. Anderson Cancer Center were in this age group. l,l” Epidemiologic studies, however, have reported that 54% to 63% of all patients in older se- ries with this diagnosis are in this age group. 16,17 Prior
454 April 1996 The American Journal of Medicine@ Volume 100

INTERFERON THERAPY FOR CML ELDERLY PATiENTS/CORTES ET AL
to 1983, the incidence of older age in our studies was ~&XI.’ The lower incidence in recent studies reflects in part a referral bias whereby elderly patients are not considered fit for treatment options other than con- ventional chemotherapy, and are therefore not re- ferred. Other factors accounting for the differences in the incidence of older age in various series are the inclusion of patients in different stages of the disease, and the inclusion of patients with Ph-negative CML and chronic myelomonocytic leukemia in some se- ries. Patients with Ph-negative, breakpoint cluster re- gion-negative disease are more likely to be older.lO,‘s
Regardless of the current referral practice, older patients are generally not candidates for allogeneic bone marrow transplant. In our studies, their out- come with IFN-a therapy was favorable in this age group. They had similar rates of complete hemato- logic response, major cytogenetic response, and com- plete cytogenetic response as younger patients, and their survival was also similar (Figure). As is the case in younger patients, complete cytogenetic remissions were durable among older patients.
Elderly patients tolerate IFN-a therapy less well. lvlg Twenty-six percent of the patients in this report ex- perienced severe, dose-limiting toxicity, compared with loo/o to 20% in the overall population.’ Despite the need for dose adjustment, 2 of these patients achieved a complete cytogenetic remission, and 3 oth- ers a complete hematologic response. In our experi- ence, response to IF’N-a in CML is dose dependent. A recent report has suggested that lower doses may be effective.20 Although every attempt should be made to deliver optimal doses to all patients, elderly pa- tients may tolerate only lower doses of IF%-a and will require dose adjustments. Whether lower doses will be as effective in this particular age group remains to be studied.
We conclude that CML patients aged 60 years and older respond to IF’N-a as well as younger patients do. Although they have a higher incidence of toxic events, these patients should be offered this thera- peutic alternative and monitored closely for side ef- fects during the course of therapy.
REFERENCES 1. Kantarjian H, Dersseroth A, Kurzrock R, et al. Chronrc myelogenous . - leukemia: a concise update. Blood. 1993;82:691-703.
2. Kurzrock R, Gutterman JU, Talpaz M. The molecular genehcs of Philadelphia-
chromosome positive leukemias. NEJM. 1988;319:990-998. 3. Hehlmann R, Heimpel H, Hasford J, et al. Randomized ‘comparison of
busuffan and hydroxyurea in chronrc myelogenous leukemia: lprolongation of survrval by hydroxyurea. Blood. 1993;83:398-407.
4. Thomas ED, Clii RA, Fefer A, et al. Marrow transplantation for the treatment
of chronic myelogenous leukemra. Ann intern Med. 1986;104:155.
5. Goldman JM, Apperley JF, Jones L, et al. Bone marrow transplantation for
patients with chronic myeloid leukemia. NEJM. 1986;314:202. 6. Biggs JC, Szer J, Crilley P, et al. Treatment of chronic myeloid leukemia with
altogenerc bone marrow transplantation after preparation with BuCy2. Blood.
1992;80:1352-1357. 7. Clift RA, Buckner CD, Thomas ED, et al. Marrow transplantation for chronic
myeloid leukemia: a randomtzed study comparing cyclophosphamrde and total
body inadiation with busutian and cyclophosphamide. Blood. 1994;84:2036-2043.
8. Talpaz M, Kantarjian H, Kurzrock R, et al. Interferon-alpha produces
sustained cytogenetic responses in chronic myelogenous leukemia. Ann Intern
Med. 1991;114:532-538, 9. Kantarjian HM, Smith TL, O’Brien S, et ai. Prolonged survival following
achievement of a cytogenetic response with alpha interferon therapy in chronic
myelogenous leukemia. Ann Intern Med. 1995;122:254-261, 10. Cortes J, Talpaz M, Beran M, et al. Philadelphia-chromosome negative
chronic myelogenous leukemia with rearrangement of the breakpoint cluster
region: long-term follow-up results. Cancer. 1995;75:464-470.
11. Talpaz M, Kantarjian HM, McCredie K, et al. Hematologic remission and
cytogenetic improvement Induced by recombinant human interkeron alpha, in
chronrc myelogenous leukemia. NEJM. 1986;314:1065-1069. 12. Trujillo JM, Cork A, Ahern MJ, et al. Hematologic and cytofogrc characterization
of 8/21 translocation acute granulocytic leukemia. Blood. 1979;53:695-706. 13. Kaplan EL, Meier P. Nonparametric estimation from incomplete
observations. J Am Stat Assoc. 1958;53:457481. 14.Cox DR. Regression models and life tables. J Royal Stat Sot.
1972;34:187-220. 15. Kantarjian HM, Keating MJ, Smith TL, et al. Proposal for a simple synthesis prog
nostic stagrng system in chronic myelogenous leukemia. Am JMed. 1990;88:1-8. 16. Brincker H. Population-based age- and sex-specific incidence rates in the 4
marn types of leukemia. Scan J Haematol. 1982;29:241-249. 17.Baranovsky A, Myers MH. Cancer incidence and survival in patients 65
years of age and older. CA Cancer J Clin. 1986;36:26-41. 18. Kantarjian HM, Shtalrid M, Kurzrock R, et al. Signtiicance and correlatrons
of molecular analysis results in patients wrth Philadelphia chromosomenegative
chronic myelogenous leukemia and chronic myelomonocytic leukemia. Am J
Med. 1988;85:639-644. 19. Quesada JR, Talpaz M, RIOS A, et al. Clinical toxicity of the interferons in
cancer patients: a review. J Clm Oncol. 1986;4:234-243. 20,Schofield JR, Robinson WA, Murphy JR, Rovira DK. Low doses of interferon-
a are as effechve as higher doses in inducing remissrons and prolonging
survival in chronic myeloid leukemra. Ann intern Med. 1994;121:736-744.
April 1996 The American Journal of Medicine* Volume 100 455


















