Results from the ICD-10 v2010 bridge coding study...
37
Office for National Statistics Statistical Bulletin 1 Statistical Bulletin Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths Date: 1 February 2011 Coverage: England and Wales Theme: Health The software used by Office for National Statistics (ONS) for cause of death coding has been updated this year from the International Classification of Diseases, Tenth Revision (ICD–10) v2001.2 to v2010. This bulletin presents the main findings from a bridge coding study of 2009 stillbirth and neonatal death registrations (in which deaths were independently coded using v2001.2 and v2010), to help users understand the impact of this change on perinatal mortality statistics for England and Wales. The impact of ICD–10 v2010 on other deaths has been investigated in a separate study. The main changes in ICD–10 v2010 are amendments to the rules used to assign underlying cause of death. However, stillbirths and neonatal deaths are certified using a perinatal death certificate where underlying cause is not assigned in the usual way. Therefore these main changes do not affect stillbirths and neonatal deaths. • There were no new codes or changes to cause of death codes in the ‘Pregnancy, Childbirth and Postnatal Care’ chapter. • The introduction of a new code (P91.6) to further specify hypoxia does not alter the broader group of deaths due to asphyxia at, before or during labour. This was the main amendment for ‘Certain Conditions Originating in the Perinatal Period’. • One minor change concerned a rare disorder for the ‘Congenital Malformations, Deformations and Chromosomal Abnormalities’ chapter. Eisenmenger’s defect remains as Q21.8 but Eisenmenger’s syndrome or complex move to the ‘Diseases of the circulatory system’ chapter. • At ONS, unexplained deaths in infancy were defined by combining Sudden Infant Death Syndrome (R95) with unascertained deaths (R99). In ICD–10 v2010, R99 still includes unspecified causes of mortality such as undetermined natural causes but a new code R97 groups deaths where the cause remained unknown. UK Data Archive Study Number 8043 - Births Registrations in England and Wales: Secure Access
Transcript of Results from the ICD-10 v2010 bridge coding study...

Office for National Statistics Statistical Bulletin 1
Statistical Bulletin
Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths Date: 1 February 2011 Coverage: England and Wales Theme: Health
The software used by Office for National Statistics (ONS) for cause of death coding has been updated this year from the International Classification of Diseases, Tenth Revision (ICD–10) v2001.2 to v2010. This bulletin presents the main findings from a bridge coding study of 2009 stillbirth and neonatal death registrations (in which deaths were independently coded using v2001.2 and v2010), to help users understand the impact of this change on perinatal mortality statistics for England and Wales. The impact of ICD–10 v2010 on other deaths has been investigated in a separate study.
The main changes in ICD–10 v2010 are amendments to the rules used to assign underlying cause of death. However, stillbirths and neonatal deaths are certified using a perinatal death certificate where underlying cause is not assigned in the usual way. Therefore these main changes do not affect stillbirths and neonatal deaths. • There were no new codes or changes to cause of death codes in the ‘Pregnancy, Childbirth and
Postnatal Care’ chapter. • The introduction of a new code (P91.6) to further specify hypoxia does not alter the broader
group of deaths due to asphyxia at, before or during labour. This was the main amendment for ‘Certain Conditions Originating in the Perinatal Period’.
• One minor change concerned a rare disorder for the ‘Congenital Malformations, Deformations
and Chromosomal Abnormalities’ chapter. Eisenmenger’s defect remains as Q21.8 but Eisenmenger’s syndrome or complex move to the ‘Diseases of the circulatory system’ chapter.
• At ONS, unexplained deaths in infancy were defined by combining Sudden Infant Death
Syndrome (R95) with unascertained deaths (R99). In ICD–10 v2010, R99 still includes unspecified causes of mortality such as undetermined natural causes but a new code R97 groups deaths where the cause remained unknown.
UK Data Archive Study Number 8043 - Births Registrations in England and Wales: Secure Access

Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths
Office for National Statistics Statistical Bulletin 2
Introduction In January 2011, the Office for National Statistics (ONS) introduced a new version of the 10th revision of the International Classification of Diseases (ICD–10) used to code cause of death. ICD–10 was introduced in England and Wales in January 2001. Since then amendments have been authorised by the World Health Organisation (WHO) to correct errors in the software supporting the automatic coding or to accommodate new codes in response to new conditions, such as the H1N1 virus (swine flu). Some of these corrections have been implemented by ONS manually. Throughout this period the international community using ICD–10 has determined changes to the classification to reflect new understandings about how causes of death are attributed. Most of the decisions impact on the rules which determine a single underlying cause from the list of conditions mentioned on the death certificate. This underlying cause is either the disease which initiated the train of events leading directly to death or the circumstances of the accident or violence which produced the fatal injury. These rules are applied to all death certificates in England and Wales for deaths occurring from 28 days after birth and older.
Stillbirths and neonatal deaths A stillbirth is where a baby is born after 24 or more weeks completed gestation and does not, at any time, breathe or shows signs of life. The 24 weeks relate to the gestation period before the fetus is delivered irrespective of the gestational age when it is thought to have died. Any death before 24 weeks gestation (a fetal death) is not certificated and ONS does not report on these deaths. Neonatal deaths are those which occur under 28 days following a live birth. If the baby showed any sign of life, this is considered a live born child irrespective of the number of weeks duration of a pregnancy.
In 1986 England and Wales introduced a special certificate for stillbirths and neonatal deaths following the recommendations of WHO at the international conference for the 9th Revision of the International Classification of Diseases1. These certificates are designed to collect information about the mother and the fetus or baby in order to determine the earliest cause in the chain of events that led to the death of the fetus or baby. While this certificate permits more flexibility for those completing the certificates it is not possible to derive an underlying cause directly from the information recorded. This means that the main amendments implemented in ICD–10 v2010 do not impact on the cause coding of stillbirths and neonatal deaths.
There are two ways of considering cause codes for stillbirths and neonatal deaths. All codes relating to the cause of death text (‘mentions’) can be examined. The certificates have two rows relating to conditions in the fetus or baby, two pertaining to conditions in the mother and a fifth row for general conditions which may relate to both or either. Each row may have several codes allocated to it.
A second approach to enable a better understanding of the causes relating to stillbirths and neonatal deaths is to group the mentions. ONS devised a hierarchical classification system2 to identify a single underlying mechanism based on the Wigglesworth classification3. The cause

Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths
Office for National Statistics Statistical Bulletin 3
groups are organised around the likely timing of the condition or damage leading to the death in relation to birth: before, during or, for neonates, after. New and amended codes present in ICD–10 v2010 will be added to the algorithm creating the ONS cause groups for stillbirths and neonatal deaths.
The ICD–10 manual groups diseases into chapters. The three chapters which are most relevant for stillbirths and neonatal deaths are Chapter XV Pregnancy, Childbirth and the Puerperium (codes O00–O99); XVI Certain Conditions Originating in the Perinatal Period (Codes P00–P96); and XVII Congenital Malformations, Deformations and Chromosomal Abnormalities (Codes Q00–Q99). Each chapter is further divided into blocks, for example the ‘birth trauma’ grouping is one of 10 blocks in Chapter XVI.
Bridge coding study To understand and quantify the impact of the introduction of ICD–10 v2010 on mortality statistics, ONS carried out a bridge coding study in which deaths were independently coded using the ICD–10 introduced in 2001 (ICD–10 v2001.2) and the new ICD–10 version 2010 (ICD–10 v2010). Stillbirths and neonatal deaths are not processed through the main Automated Cause Coding System (PC-ACCS) to determine underlying cause but are instead run through a modified version of the ONS software. This TRACER dictionary system allocates ICD–10 codes to all mentions. The v2001.2 coding was performed on TRACER in the main production environment and records were then extracted and run through the updated TRACER dictionary (v2010) in the test environment.
There were 3,688 stillbirths registered in England and Wales in 2009. Of these, 3,632 were fully coded using both ICD–10 versions (98.5 per cent). The remaining 56 stillbirths went to inquest and were coded manually using ICD–10 v2001.2 and were not coded again for ICD–10 v2010.There were 2,251 neonatal deaths registered in England and Wales in 2009 and all were fully coded on both versions. Deaths from 2009 were chosen because this was the most recent published data year available.
Results The number of mentions varied between 1 and 7 for stillbirths and 1 and 10 for neonatal deaths. As expected, the vast majority of codes were unchanged at the chapter and block level. Known code changes relevant for stillbirths and neonates are highlighted below.
XV Pregnancy, Childbirth and the Puerperium (Codes O00–O99) No new codes or code changes in ICD–10 v2010 concerned this chapter.
XVI Certain Conditions Originating in the Perinatal Period (Codes P00–P96) In the P91 group ‘Other disturbances of cerebral status of newborn’, a new code has been introduced: P91.6 ‘Hypoxic ischaemic encephalopathy of newborn’. Previously, this disorder was coded in P21.9 ‘Birth asphyxia, unspecified’. Other mentions of anoxia, asphyxia and hypoxia not otherwise specified still code to P21.9. This change will not affect the ONS Classification where group P200–P219 and group P910–P919 were both included in the ‘Asphyxia, anoxia or trauma’ cause group.

Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths
Office for National Statistics Statistical Bulletin 4
XVII Congenital Malformations, Deformations and Chromosomal Abnormalities (Codes Q00–Q99) One amendment concerns a rare congenital heart defect. Eisenmenger’s defect is still coded to Q21.8 but Eisenmenger’s syndrome or complex is coded to I27.8 ‘Other pulmonary heart diseases’. In 2009 there were no stillbirths or neonatal deaths coded to this rare congenital condition. Other minor amendments in this chapter did not have an impact on the stillbirths or neonatal deaths.
XVIII Symptoms, Signs and Abnormal Clinical and Laboratory Findings, not elsewhere classified: code block ‘Ill-defined and unknown causes of mortality (R95–R99) There are no changes to code R95 ‘Sudden Infant Death Syndrome’. Deaths so coded have been included with v2001.2 code R99 ‘Other ill-defined and unspecified causes of mortality’ to produce reports on ‘Unexplained deaths in infancy’. In ICD–10 v2010, this code is further divided. The undetermined and unspecified causes of death still go to code R99 but deaths of unknown cause go to new code R97. To further clarify this distinction, R99 includes deaths where the cause cannot be determined due to the circumstances (for example, only a skeleton was found) and deaths of natural causes though unspecified. R97 includes deaths where the aetiology remained undetermined despite medical investigations. This distinction will be further explored when the deaths occurring in 2011 and coded to ICD–10 v2010 are reported for the ‘Unexplained deaths in infancy’ report.
Future work ONS introduced the new version of the ICD–10 software for all deaths that are registered from January 2011 onwards. Infant and perinatal mortality statistics by ONS Classification of cause of death for the 2011 data year coded using ICD–10 v 2010 are expected to be published in autumn 2012. While this bulletin has highlighted the main changes relevant for perinatal mortality, any impact of these changes on the ONS cause groups will be explained when these statistics are published.

Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths
Office for National Statistics Statistical Bulletin 5
Background Notes 1. A Bridge coding analysis of the impact on all deaths at 28 days and over is also available on the
ONS website at: www.ons.gov.uk/ons/search/index.html?newquery=icd-10+bridge+coding 2. All figures in this bulletin are based on 2009 death registrations data for England and Wales. 3. Examples of the stillbirth certificate (Annex A) and the neonatal death certificate (Annex B) can
be found in the ONS publication Mortality statistics: Childhood, infant and perinatal, available on the ONS website at: www.ons.gov.uk/ons/rel/vsob1/child-mortality-statistics--childhood--infant-and-perinatal/2009/index.html
4. A brief description of the ONS cause groups can be found in ‘Notes and definitions’ and the list of ICD–10 codes assigned to each group can be found in Annex J for stillbirths and Annex K for neonatal deaths in the ONS publication Mortality statistics: Childhood, infant and perinatal, available on the ONS website at: www.ons.gov.uk/ons/rel/vsob1/child-mortality-statistics--childhood--infant-and-perinatal/2009/index.html
5. Details of the policy governing the release of new data are available from the Media Relations Office.
6. National Statistics are produced to high professional standards set out in the Code of Practice for Official Statistics. They undergo regular quality assurance reviews to ensure that they meet customer needs. They are produced free from any political interference. © Crown copyright 2011.
References 1 World Health Organisation (1977) Manual of the international statistical classification of diseases, injuries, and causes of death, Volume 1. World Health Organization: Geneva. 2 Dattani, N. and Rowan, S. (2002) ‘Causes of neonatal deaths and stillbirths: a new hierarchical classification in ICD–10’, Health Statistics Quarterly 15 pp 16–22, available on the Office for National Statistics website at: www.ons.gov.uk/ons/rel/hsq/health-statistics-quarterly/no--15--autumn-2002/index.html 3 Wigglesworth, J.S. (1980) ‘Monitoring perinatal mortality. A pathophysiological approach’, Lancet 2 pp 684–86
…………………………………………………………………………………………………………
Issued by: Office for National Statistics, Government Buildings, Cardiff Road, Newport NP10 8XG
Media contact: Tel: Media Relations Office 0845 6041858 Emergency on-call 07867 906553 Email: [email protected]
Statistical contact: Tel: Julie Messer 01633 456021

Results from the ICD-10 v2010 bridge coding study: stillbirths and neonatal deaths
Office for National Statistics Statistical Bulletin 6
Email: [email protected]
Website: www.ons.gov.uk

Statisticalbulletin:
ImpactoftheImplementationofIRISSoftwareforICD-10CauseofDeathCodingonMortalityStatistics,EnglandandWalesThedifferencesproducedbycategorisingdeathsusingMMDSandIRISsoftware,andtheeffectonstatisticsthatusecauseofdeathdataofusingIRISsoftware.
Contact:ClaudiaWells
Releasedate:8August2014
Nextrelease:Tobeannounced

Tableofcontents1. Mainfindings
2. Background
3. Reasonforthechange
4. MainchangesintroducedbyONSusingIRISsoftwarev2013
5. EvaluatingtheimpactofIRISonmortalitystatistics
6. Results
7. Downloadablereferencetables
8. Backgroundnotes

MainfindingsDualcodingof38,718deathsregisteredin2012inEnglandandWalesshowedstatisticallys ignificantpercentageincreasesinthedeathsallocatedtoanunderlyingcauseinsevenICD-10chapters,ands ignificantdecreasesforfivechapterswhencodedinICD-10v2013(IRIS).However95%ofdeathsremainedinthesamechapter.
Achangeinthecodingofchestinfectionscontributedtoareductionof2.5%indeathsallocatedanunderlyingcauseofrespiratorydiseaseandanincreaseof7.0%inthoseallocatedtothementalandbehaviouraldisorderschapter,whichincludesdementia.
Deathsgivenanunderlyingcauseofdementiawerealsoincreasedbyarulechangetocountaspirationpneumoniaasbeingaconsequenceofoneofanumberofotherconditions.Thetotalpercentagechangeindeathsattributedtoanunderlyingcauseofdementiawas7.1%.
Deathsallocatedcertaininfectiousandparasiticdiseasesasanunderlyingcauseincreasedby4.9%followingthetransferofdeathsinvolvingsepsis/septicaemiafromotherchapters.
Arulechangetocountdiabetesastheunderlyingcauseofcertaintypesofrenaldiseaseledtoanincreaseof5.7percentinthechapteronendocrine,nutritionalandmetabolicdiseases.Deathswithanunderlyingcauseofdiabetesroseby6.8%.
1.

BackgroundTheOfficeforNationalStatistics(ONS)codecauseofdeathusingtheWorldHealthOrganization's(WHO)InternationalClassificationofDiseases,TenthRevision(ICD-10).Wherepossible,deathsareautomaticallycodedusingspecialistsoftware,withtheremainingdeathsbeingmanuallycodedbyhighlytrainedcoders.ICD-10wasintroducedinEnglandandWalesinJanuary2001.SincethenvariousamendmentshavebeenauthorisedbyWHO.Amendmentsmay(forexample)correcterrorsinthesoftwaresupportingautomaticcoding,accommodatenewcodesinresponsetonewconditions,suchastheH1N1virus(swineflu),orincorporateadvancesinmedicalknowledgeoftherelationshipbetweenconditions.
UntilDecember2010,ONSusedtheMortalityMedicalDataSystem(MMDS)ICD-10version2001.2softwareprovidedbytheUnitedStatesNationalCenterforHealthStatistics(NCHS)tocodecauseofdeath.InJanuary2011,thiswasupdatedtoversion2010,whichincorporatedmostoftheWHOamendmentsauthorisedupto2009.
On1January2014,ONSchangedthesoftwareusedtocodecauseofdeathtoapackagecalledIRIS(version2013).ThedevelopmentofIRISwassupportedbyEurostat,thestatisticalofficeoftheEuropeanUnion,andisnowmanagedbytheIRISInstitutehostedbytheGermanInstituteofMedicalDocumentationandInformationinCologne.IRISsoftwareversion2013incorporatesallofficialupdatestoICD-10approvedbyWHO,whichweretimetabledforimplementationbefore2014.
2.
ReasonforthechangeTheIRISsoftwarehasbeendevelopedtoprovideacommonautomatedcauseofdeathcodingsystemtocodecauseofdeathinformationprovidedondeathcertificatesinanylanguage,usingICDmortalitycodingrulesandinstructions.TheuseoftheIRISsoftwarewillimprovethecomparabilityofmortalitystatisticsacrossEuropeandinternationally.CurrentlyIRISusescomponentsoftheNCHSMMDStocodethecausesofdeathmentionedonthedeathcertificate,andtoallocatetheunderlyingcauseofdeath.ThesecomponentswillbereplacedwithversionsdevelopedbytheIRISInstituteinaforthcomingIRISversion.
3.

MainchangesintroducedbyONSusingIRISsoftwarev2013
IRISincludesmajorupdatestotheICD-10approvedbyWHO.Therehavebeenadditionsto,anddeletionsfrom,thetabularlistofICDcodes(volume1);amendmentstotheselectionandmodificationrulescontainedintheinstructionmanual(volume2);andchangestothealphabeticalindex(volume3).
Theseupdatesincludes ignificantchangestotheuseofcodeswithintheneoplasmschapter(ICD-10codesC00-D48)whichincludesdeathsfromcancers(ICD-10codesC00-C97).
Asmallnumberofchangestothecodingofotherspecificconditionshavebeenmadetobringpreviouscodingpracticeintolinewithinternationalcodingrules.
Forstillbirthsandneonataldeaths,anymaternalconditionmentionedonthedeathcertificatewillbecodedtothePChapter(certainconditionsoriginatingintheperinatalperiod)ratherthanelsewhereintheICDclass ification.PreviouslythesedeathsmayhavebeencodedtotheOchapter(pregnancy,childbirthandthepuerperium).
4.

EvaluatingtheimpactofIRISonmortalitystatisticsONScarriedoutadualcodingstudyinwhichasampleofdeathsregisteredthroughout2012,alreadycodedusingtheICD-10v2010softwareandrules(NCHS),wererecodedusingICD-10v2013rules(IRIS).
SampleToavoidseasonalinfluencesoncausesofdeathaffectingtheanalysis,recordswereselectedfromeachquarterof2012.Weekscontaining,orimmediatelyfollowingabankholiday,wereexcludedduetotheatypicalnumberofdeathregistrationsinthoseweeks.Neonataldeaths(under28days)wereexcluded,andtheimpactofthecodingchangeonthesedeathswillbereportedseparately.
Intotal38,718deathsregisteredinfourweeks(oneweekineachofJanuary,April,JulyandOctober2012)weredualcoded,comprising7.8%ofallnon-neonataldeathsregisteredin2012.
LimitationsThesamplesizeof38,718deathsdoesnotgiveenoughstatisticalpowertoanalysetheimpactofchangingfromICD-10v2010(NCHS)toICD-10v2013(IRIS)forlesscommoncategoriesofcauseofdeath,suchasdiseasesoftheskinandsubcutaneoustissueorveryspecificcausesofdeath,suchasmalignantneoplasmofthepalate,asthereareveryfewdeathsfromthesecausesinthesample.ThesmallsamplesizeisalsoaprobleminthosecaseswherethechangesbetweentheICD-10versionsarerelativelysmall.
Asthesampleofrecordswasdualcodedinatestenvironment,therewereasmallnumberofdifferencesinthecodingpracticesusedcomparedwiththelivecodingenvironment.Forexample,inthelivecodingenvironment,aspecialon-screenbrowserisusedtoassistmanualcoding,butthisbrowserwasnotavailableforthedualcoding.Itisanticipatedthattheseprocessingdifferenceswillhaveaminimalimpactoncodingforthemajorityofdeaths.Thebiggestimpactofthesedifferencesinthecodingprocesswillbeondeathsthatarecertifiedbyacoronerfollowinganinquest(forexample,deathsfromexternalcausessuchasdrugpoisoning),asthesedeathsarealwaysmanuallycoded.However,theimpactofslightmethodologicaldifferencesislikelytobesmall,evenwiththesemanuallycodeddeaths.
5.
Results6.

Theresultsreportedherearebasedontheunderlyingcauseofdeath.ThisisdefinedbytheWHOas:
thediseaseorinjurywhichinitiatedthetrainofmorbideventsleadingdirectlytodeath
thecircumstancesoftheaccidentorviolencewhichproducedthefatalinjury
Moreinformationabouttheselectionofunderlyingcauseofdeathfromamongtheconditionsmentionedonadeathcertificatecanbefoundinthebackgroundnotes.
Table1(59KbExcelsheet)(http://www.ons.gov.uk/ons/rel/subnational-health3/impact-of-the-implementation-of-iris-software-for-icd-10-cause-of-death-coding-on-mortality-statistics/england-and-wales/rft-table-1.xls)showsacross-tabulationofdeathsfromthedualcodingstudygroupedbytheICD-10chapteroftheunderlyingcauseofdeath,presentingresultsfrombothICD-10versions(ICD-10v2010,NCHSandICD-10v2013,IRIS).Thetableshowsthatmorethan95%ofdeathsinthissampleremainedinthesamechapter.However,thereweremovementsinandoutofsomechaptersreflectingthechangesintheselectionoftheunderlyingcauseofdeathfromthecombinationofconditionsrecordedonthedeathcertificate.Theimpactofthesemovementsonspecificchaptersisexaminedintheindividualchaptersectionsbelow.
Comparabilityratios(withconfidenceintervals)havebeencalculatedusingstandardmethods.ThesearetheratioofthenumberofdeathscodedtoaparticularunderlyingcauseinICD-10v2010(NCHS),tothenumbercodedtothesamecauseinICD-10v2013(IRIS).Theseratiosreflecttheneteffectofthechange.Iftheratiois1,thenumberofdeathscodedtothatcauseisthesameinbothversions.Ifthecomparabilityratiois0.5,halfasmanydeathshavebeencodedtothatcauseusingICD-10v2013(NCHS),comparedwithICD-10v2010(IRIS).Confidenceintervalsindicatethereliabilityofthecomparabilityratio.Whereacomparabilityratioisgiven,butitsconfidenceintervalincludes1,thismeansthatthedifferencebetweenthenumberofdeathsallocatedtothatunderlyingcauseusingICD-10v2010(NCHS)andICD-10v2013(IRIS)wasnotstatisticallysignificant.
Thedatasetofsampledrecords,includingcodesforeveryconditionmentionedonthedeathcertificateandtheunderlyingcauseofdeathcodedusingbothICD-10v2010(NCHS)andICD-10v2013(IRIS)isavailableintable2(18.86MbExcelsheet)(http://www.ons.gov.uk/ons/rel/subnational-health3/impact-of-the-implementation-of-iris-software-for-icd-10-cause-of-death-coding-on-mortality-statistics/england-and-wales/rft-table-2.xls).
ICertaininfectiousandparasiticdiseases(ICD-10codesA00–B99)

Overallthenumberofdeathsassignedtotheinfectionschapterincreasedby4.9%(astatisticallysignificantchange).Thebiggestincreaseisindeathsfromsepsis/septicaemia(ICD-10codeA41)andbacterialinfectionsofunspecifiedsite(A49).Thesedeathswerepreviouslycodedtoavarietyofchapters,mostcommonlyrespiratorydiseases(suchaschestinfectionsorchronicobstructivepulmonarydisease).
Therewereonlyasmallnumberofwithinchaptercodingchanges,wheretheunderlyingcauseofdeathwasassignedtotheinfectiousdiseasechapterinbothICD-10v2010(NCHS)andICD-10v2013(IRIS),butthespecificcodediffered.
IINeoplasms(ICD-10codesC00–D48)Thenumberofdeathsassignedtoneoplasmshasincreasedveryslightlyby0.3%.Whilstinabsoluteterms,thisisnotabigincrease,becausealargenumberofpeoplediefromneoplasms,thisincreaseisstatisticallysignificant.
TherearealsoanumberofspecificchangestoICD-10codingpracticeswhichaffectthecodingofdeathswithintheneoplasmschapter.Specifically,thecodeformalignantneoplasms(cancers)ofindependent(primary)multiplesites(C97)isnolongerinuse.Instead,ICD-10v2013(IRIS)codeseachcancermentionedandthenassignstheunderlyingcausetothefirstmentionedcancer.ThereforedeathsthatwerepreviouslyassignedanunderlyingcauseofC97arenowdistributedthroughoutthemalignantneoplasmcodes.
InICD-10v2010(NCHS),anycancerthatwasdescribedasmetastaticwouldbeamendedfromasecondarycancercodetotheappropriateprimarycode,ifitwastheonlycancermentionedonthedeathcertificate.InICD10v2013(IRIS),thesecodeswillonlybeamendedtotheprimarycancercodeifthecancersiteisnotrecognisedasacommonsiteformetastases.Cancersthatarerecognisedasonesthatcommonlymetastasisewillremainassecondarycodesandbeassumedtobeduetoanunknowncarcinoma.Asaresult,inICD-10v2013(IRIS),thenumberofdeathswithanunderlyingcausecodeofunknowncarcinoma(C80)hasincreased.
IIIDiseasesofthebloodandblood-formingorgansandcertaindisordersinvolvingtheimmunemechanism(ICD-10codesD50–D89)Thenumberofdeathsassignedtothischapterdecreasedby1.1%,whichwasnotastatisticallysignificantchange.However,thesampleofdualcodeddataonlycontainedasmallnumberofdeathswithanunderlyingcauseassignedtothischapter,sothesefindingsshouldbetreatedwithcaution.

IVEndocrine,nutritionalandmetabolicdiseases(ICD-10codesE00–E90)Therehasbeenastatisticallysignificantincreaseof5.7%inthenumberofdeathsassignedto‘endocrine,nutritionalandmetabolicdiseases’inICD-10v2013(IRIS).Thisincreaseismainlycausedbydeathsmovingfromdiseasesofthegenitourinarysystem(N00–N99)andcirculatorysystem(I00–I99)inICD-10v2010(NCHS)toendocrine,nutritionalandmetabolicdiseases(E00–E90)inICD-10v2013(IRIS).Morespecifically,deathswheretheunderlyingcausewaspreviouslycodedasrenalfailure(N17–N19)orhypertensiverenaldisease(I12)inICD-10v2010(NCHS)arenowcodedasdiabetes(E10–E14)ifthelatterwasmentionedonthedeathcertificate.ThisisduetoachangetoICDcodingrulesaffectingtheselectionoftheunderlyingcauseofdeath,whererenalfailureisnowconsideredasanobviousconsequenceofdiabetes,soifbotharementionedonthedeathcertificate,diabeteswillnowbeselectedastheunderlyingcauseofdeath.Thischangehasresultedina6.8%riseinthenumberofdeathswithanunderlyingcauseofdiabetesusingICD-10v2013(IRIS).
Therewereveryfewwithin-chapterchangesforendocrine,nutritionalandmetabolicdiseases.
VMentalandbehaviouraldisorders(ICD-10codesF00–F99)Thenumberofdeathsallocatedto‘mentalandbehaviouraldisorders’hasincreasedby7.0%(astatisticallysignificantchange).Thisincreaseislargelyduetodeathswhichwerepreviouslyassignedanunderlyingcauseofrespiratorydisease,nowbeingassignedtothementalandbehaviouraldisorderschapter(mainlytheF01andF03dementiacodes).
Themainreasonforthisincreaseisthechangetothecodingofchestinfections,whichisdescribedinthesectionon‘Diseasesoftherespiratorysystem’.Specifically,deathswhichmentionbothachestinfection(ICD-v2010codeJ98andv2013codeJ22)anddementia(F01orF03)arenowallocatedanunderlyingcauseofdementia,whereasinICD-10v2010(NCHS),thechestinfectionwouldhavebeenassignedastheunderlyingcause.
Thesecondreasonforthisincreaseindementiadeathsisduetoacodingchangethataffectsdeathswherebothaspirationpneumonia(ICD-10codeJ69)anddementia(F01orF03)arementionedonthedeathcertificate.PreviouslyinICD-10v2010(NCHS),theunderlyingcausewasassignedtoJ69,butinICD-10v2013(IRIS),dementiaisassignedastheunderlyingcause.Thisisbecauseaspirationpneumonia(J69)isconsideredan‘obviousconsequence’ofconditionsthataffectswallowing,andinICD-10v2013(IRIS),dementiawasaddedtothelistofconditionsthataffectswallowing.

ThepercentageofdeathswithICD-10codesF01orF03mentionedonthedeathcertificatewasthesame,whetherICD-10v2010(NCHS)orICD-10v2013(IRIS)wasusedtocodethedeaths.ThishighlightsthefactthatitisonlytheallocationofunderlyingcausefordementiathathaschangedinICD-10v2013(IRIS).Overall,thischangehascauseda7.1%increaseinthenumberofdeathswheredementiawasallocatedastheunderlyingcause.
Thischangefollowsonfromthelargeincreaseindeathsfromdementiareportedin2011deathregistrationsdata,whentheICD-10v2010(NCHS)wasfirstintroducedinEnglandandWales.MoreinformationonthispreviouschangecanbefoundontheONSwebsite(http://www.ons.gov.uk/ons/rel/subnational-health3/results-of-the-icd-10-v2010-bridge-coding-study--england-and-wales--2009/2009/index.html).
FormoreinformationontheWHOrulesusedtodecidewhichconditionmentionedonadeathcertificateshouldberecordedastheunderlyingcauseofdeath,seebackgroundnotes1–4.
Therewereveryfewwithin-chapterchangesformentalandbehaviouraldisorders.
VIDiseasesofthenervoussystem(ICD-10codesG00–G99)Therehavebeenanumberofcodingchangesthathaveaffectedwhetheradeathisassignedanunderlyingcauseinthediseasesofthenervoussystemchapter.However,thesechangeshavetendedtocanceleachotherout.Thereforetheneteffectisaverysmallincrease(0.4%)inthenumberofdeathsassignedtothischapterwhichisnotstatisticallysignificant.
Asinthecaseofdementia,deathsthatmentionedeitheraspirationpneumonia(J69)orachestinfection(J98),aswellasadiseaseofthenervoussystem(mostcommonlyG30Alzheimer’sdisease,G20Parkinson’sdisease,orG31otherdegenerativediseasesofnervoussystem,notelsewhereclassified)wereallocatedanunderlyingcauseofJ69orJ98inICD-10v2010(NCHS).However,inICD-10v2013(IRIS),theunderlyingcauseisallocatedtothediseaseofthenervoussystem.Thereasonsforthisarediscussedinthementalandbehaviouraldisorderssectionabove.
Thereversetrendwasseenfordeathsthatmentionedbothpneumoniaandadiseaseofthenervoussystem,inthesecasespneumoniaisselectedastheunderlyingcause,becauseofchangeswithrespecttowhichdiseasesarenowconsideredtobeaconsequenceofanothercondition.
VIIDiseasesoftheeyeandadnexa(ICD-10codesH00–H59)

ThenumberofdeathsclassifiedtothesechaptersintheannualmortalitystatisticsisextremelysmallandONSexpecttoseenosignificantchangeinthereportedstatistics.
VIIIDiseasesoftheearandmastoidprocess(ICD-10codesH60–H95)ThenumberofdeathsclassifiedtothesechaptersintheannualmortalitystatisticsisextremelysmallandONSexpecttoseenosignificantchangeinthereportedstatistics.
IXDiseasesofthecirculatorysystem(ICD-10codesI00–I99)Diseasesofthecirculatorysystemshoweda0.7%decreasebetweenICD-10v2010(NCHS)andICD-10v2013(IRIS).Althoughinabsolutetermsthisisarelativelysmalldrop,duetothelargenumberofpeoplewhodiefromcirculatorydiseases,itisastatisticallysignificantdecrease.Thissmalldecreaseiscausedbyanupdatetotheselectionrulesthatareappliedwhenthecirculatorydiseasearementionasasignificantconditioncontributingtothedeathbutnotpartofthedirectduetosequenceleadingtodeath.Inthesecasesthecirculatorydiseasewillonlybeselectedastheunderlyingcauseifdescribedassevere,graveoradvanced.
XDiseasesoftherespiratorysystem(ICD-10codesJ00–J99)InICD-10v2013(IRIS)achangehasbeenmadetothecodingofdeathsmentioningachestinfection.PreviouslychestinfectionswerecodedtoICD-10codeJ98(otherrespiratorydisorders),butanamendmenttotheICD-10alphabeticalindexinv2013(IRIS)meansthatchestinfectionsarenowcodedtoJ22(unspecifiedacutelowerrespiratoryinfections).ExistingICD-10rulesforassigningtheunderlyingcauseofdeathmeanthatJ22canbepartofanacceptablecausalsequencewithmanydifferentconditions.ForexampleifJ22andF03(dementia)werebothmentionedonthedeathcertificate,becauseJ22canbecausedbyF03,dementia(F03)wouldbeassignedastheunderlyingcause(assumingnootherconditionswerementioned).Incontrast,ifbothJ98andF03werementionedonthedeathcertificate,J98wouldbeassignedastheunderlyingcause,becauseJ98isnotarecognisedconsequenceofdementia.Infact,J98isonlyrecognisedasaconsequenceofasmallnumberofconditions,soislesslikelytobeselectedastheunderlyingcausethanJ22.

Itisrelativelycommonforchestinfectionstobementionedonadeathcertificate,sothischangewillhaveanimpactonmortalitystatistics,basedonunderlyingcauseofdeath.Thedualcodeddatashowsastatisticallysignificantdecreaseofaround2.5%ofdeathswithanunderlyingcauseassignedtothischapter,betweenICD-10v2010(NCHS)andICD-10v2013(IRIS).Thisdecreaseislargelyduetodeathswhichwerepreviouslyassignedtotherespiratorydiseaseschapternowbeingassignedtomentalandbehaviouraldisorders(mostlydementia),diseasesofthenervoussystem(mostlyAlzheimer’sdisease)andtoneoplasms.
XIDiseasesofthedigestivesystem(ICD-10codesK00–K93)Therewasastatisticallysignificantdecreaseof2.2%ofdeathswithanunderlyingcauseassignedtothischapter,betweenICD-10v2010(NCHS)andICD-10v2013(IRIS).Themainreasonforthischangeisthewaypost-operativeconditionsarecodedwhenmentionedonthedeathcertificate.Somedeathsthatwerepreviouslyassignedtoadigestivediseaseunderlyingcausearenowassignedtoeitherarespiratoryorcirculatorydiseasecauseofdeath.
XIIDiseasesoftheskinandsubcutaneoustissue(ICD-10codesL00–L99)Therewasa2.8%increaseinthenumberofdeathsallocatedtothischapterusingICD-10v2013(IRIS).However,therearerelativelyfewdeathsfromdiseasesoftheskinandsubcutaneoustissue,sothisincreasewasnotstatisticallysignificant.
XIIIDiseasesofthemusculoskeletalsystemandconnectivetissue(ICD-10codesM00–M99)Therewasa13.1%decreaseinthenumberofdeathsassignedtothischapterusingICD-10v2013(IRIS),whichwasstatisticallysignificant.
Aswithdiseasesofthedigestivesystem,themainreasonforthischangeisthewaypost-operativeconditionsarecoded,sonowsomedeathsthatwerepreviouslyassignedanunderlyingcauseofdeathcodewithinthediseasesofthemusculoskeletalsystemandconnectivetissuechapterarenowassignedtocodesintherespiratorydiseases,circulatorydiseasesorexternalcauseschapters.
XIVDiseasesofthegenitourinarysystem(ICD-10codesN00–N99)

Therehasbeenastatisticallysignificant7.9%decreaseinthenumberofdeathscodedtodiseasesofthegenitourinarysystem,usingICD-10v2013(IRIS).Themajorityofthedecreaseisexplainedbydeathsthatwerepreviouslyassignedanunderlyingcauseofdeathcodeinthediseasesofthegenitourinarysystemchapter,nowbeingassignedacirculatorydiseaseorendocrine,nutritionalandmetabolicdiseasesastheunderlyingcauseofdeath.ThebiggestchangeisfordeathsthatwerepreviouslyassignedtoN03(chronicnephriticsyndrome),whicharenowassignedtoeitherI12(hypertensiverenaldisease),I13(hypertensiveheartandrenaldisease).
Afurtherchangerelatestodeathswheretheunderlyingcausewaspreviouslyassignedtorenalfailure(N17–N19)orhypertensiverenaldiseasecode(I12)inICD-10v2010(NCHS),whicharenowassignedtoadiabetes(E10–E14)code.
XVPregnancy,childbirthandthepuerperium(ICD-10codesO00–O99)ThenumberofdeathsclassifiedtothischapterintheannualmortalitystatisticsissmallandONSexpecttoseenosignificantchange.Therewere7deathsassignedtothischapterinthesampleandthecodingremainedthesamebetweenICD-10v2010(NCHS)andICD-10v2013(IRIS).
XVICertainconditionsoriginatingintheperinatalperiod(ICD-10codesP00–P96)ChapterXVIhasnotbeenexaminedinthisreport,astherewerelessthan20deathsassignedtothischapterinthesample.Thesedeathsoccurredinthepostneonatalperiod(over28days),asubstantialproportionofdeathsassignedtothischapterviatheroutinecauseofdeathcodingprocessesoccurintheneonatalperiod(under28days).
In1986inlinewithWHOrecommendations,aneonataldeathcertificatewasintroducedinEnglandandWaleswhichalloweddiseasesorconditionsinthefetusorinfant,maternaldiseasesorconditionsaffectingthefetusorinfantandotherrelevantcausestoallberecorded.Sinceequalweightingisgiventoconditionsinthefetus/infantandinthemother,itisnotpossibletoidentifyasingleunderlyingcauseofdeathforneonataldeaths.

AnimportantchangehasbeenmadebyONStohowconditionsmentionedontheneonataldeathcertificatearecoded,wherethedeathwascausedbyamaternalcondition.Previously,theseneonataldeathswouldhavebeenassignedamaternaldiseasecode(forexample,aconditionrelatingtopregnancy,childbirthandthepuerperium,ICD-10codesO00–O99).However,inICD-10v2013(IRIS)thematernalconditionthatcontributedtotheneonataldeathisassignedacodeintherangeP00–P04(fetusandnewbornaffectedbymaternalfactorsandbycomplicationsofpregnancy,labouranddelivery).Soifthebabydiedasaresultofmaternalpre-eclampsia,theneonataldeathwouldpreviouslyhavebeenassignedtheO14code,butwillnowbeassignedtheP00.0code.ThisisinlinewithEuropeanICDcodingpractices.Amoredetailedexplanationofthesechangesandanalysisoftheirimpactonneonataldeathsandstillbirths,includingafullcodemappingdocument,willbepublishedlaterin2014.
XVIICongenitalmalformations,deformationsandchromosomalabnormalities(ICD-10codesQ00–Q99)Thenumberofdeathscodedtothischapterincreasedsignificantlyby11.7%usingICD-10v2013(IRIS).Themainreasonforthisincreaseisdeathswhichwerepreviouslycodedasmentalandbehaviouraldisorders,whicharenowcodedascongenitalmalformations,deformationsandchromosomalabnormalities.SpecificallydeathsthatmentionDownsyndrome(Q90.9)anddementia(F03)arenowassignedanunderlyingcauseofDownsyndrome.Whilstthisincreaseisstatisticallysignificant,substantialproportionsofdeathsfromthiscauseoccurintheneonatalperiod,andthesedeathshavenotbeenanalysedinthisreport.
XVIIISymptoms,signsandabnormalclinicalandlaboratoryfindings,notelsewhereclassified(ICD-10codesR00–R99)Therehasbeenasmall(0.9%),butstatisticallysignificantincreaseinthenumberofdeathsassignedtothischapterusingICD-10v2013(IRIS).
XXExternalcausesofmortality(ICD-10codesU50.9,V01–Y89)

Therehasbeenastatisticallysignificantincreaseof3.1%inthenumberofdeathsfromexternalcausesusingICD-10v2013(IRIS).Thelargestincreasehascomefromdeathspreviouslyassignedtoacodeinthediseaseofthemusculoskeletalsystemandconnectivetissuechapter(ICD-10codesM00–M99)inICD-10v2010(NCHS),whicharenowbeingassignedtoexternalcausecodesinICD-10v2013(IRIS).ThemajorityofthisincreaseisduetodeathspreviouslycodedtoM25(Otherjointdisorders,notelsewhereclassified),whicharenowassignedtotheY83.1code(Surgicaloperationwithimplantofartificialinternaldevice).
TherearealsoarelativelylargenumberofdeathsthatwerepreviouslyassignedtoacirculatorydiseasecodeinICD-10v2010(NCHS),whicharenowassignedtoanexternalcausecodeinICD-10v2013(IRIS).Someofthesechangesarefromdeathsthatmentionacirculatorydisease(forexampleischaemicheartdisease),whichhasbeenoperatedon(forexample,heartbypasssurgery.InICD-10v2010(NCHS),thecirculatorydiseasewasselectedastheunderlyingcause,butinICD-10v2013(IRIS),theoperationisselectedastheunderlyingcause(Y83orY84–complicationofsurgicalormedicalprocedure).
DownloadablereferencetablesDatafromthedualcodingstudyareavailabletodownloadfromtheONSwebsite.
Table1(59KbExcelsheet)(http://www.ons.gov.uk/ons/rel/subnational-health3/impact-of-the-implementation-of-iris-software-for-icd-10-cause-of-death-coding-on-mortality-statistics/england-and-wales/rft-table-1.xls)presentsthesampledrecordsbyICD-10chapteroftheunderlyingcauseofdeath,showingresultsfrombothICD-10versions(ICD-10v2010,NCHSandICD-10v2013,IRIS).
Table2(18.86MbExcelsheet)(http://www.ons.gov.uk/ons/rel/subnational-health3/impact-of-the-implementation-of-iris-software-for-icd-10-cause-of-death-coding-on-mortality-statistics/england-and-wales/rft-table-2.xls)presentsthedatasetofdualcodeddata,includingtheselectedunderlyingcauseofdeatheverymentionedconditiononthedeathcertificatecodedusingbothICD-10v2010(NCHS)andICD-10v2013(IRIS),byageandsex.
7.
Backgroundnotes8.

1. ThedeathcertificateusedinEnglandandWalesaccordswiththatrecommendedbyWHO.Itissetoutintwoparts.PartIgivestheconditionorsequenceofconditionsleadingdirectlytodeath,whilePartIIgivesthedetailsofanyassociatedconditionswhichcontributedtothedeath,butarenotpartofthecausalsequence.AnexampleofthedeathcertificateusedinEnglandandWalesisavailableinAnnexAofthemortalitymetadata(2.7MbPdf)(http://www.ons.gov.uk/ons/guide-method/user-guidance/health-and-life-events/mortality-metadata.pdf)ontheONSwebsite.
2. TheGeneralPrincipleforselectionoftheunderlyingcauseofdeathstatesthatwhenmorethanoneconditionisenteredonthedeathcertificate,theconditionenteredonthelowestusedlineofPartIshouldbeselected,butonlyifitcouldhavegivenrisetoalltheconditionsenteredaboveit.Ifthisisnotthecasethenthefollowingselectionrulesareapplied:
Rule1.Ifthereis areportedsequenceterminatingintheconditionenteredfirstonthedeathcertificate,selecttheoriginatingcauseofthis sequence.
Rule2.Ifthereis noreportedsequenceterminatingintheconditionfirstenteredonthedeathcertificate,selectthefirst-mentionedcondition
Rule3.IftheconditionselectedbytheGeneralPrinciple,Rule1orRule2isobviouslyadirectconsequenceofanotherreportedcondition(whetherinPartIorPartIIofthedeathcertificate),selectthis primarycondition
3. Modificationtablesallowtheidentificationofvalidcausalsequencesofconditionsandgivemodificationrulestoimprovetheusefulnessandprecisionofmortalitydata.Forexample,thetableswillidentifyadirectcausalsequencebetweentwoconditions,however,thereareparticularconditions,combinationsorcircumstanceswhenmodificationrulesarethenappliedtoselectthecorrectunderlyingcauseofdeath.Sowithsomedeathcertificates,twoormorecausesmaybegiventhat,whenlinkedtogether,pointtoanothercause(notexplicitlymentionedonthecertificate)astheunderlyingcause.
4. InformationontherulesandguidelinesadoptedbyWHOfortheselectionofunderlyingcauseofdeathareavailableinVolume2(http://apps.who.int/classifications/icd/en/index.html)oftheICD-10manualwhichcanbedownloadedfromtheWHOwebsite
5. SpecialextractsandtabulationsofdeathsdataforEnglandandWalesareavailabletoorder(subjecttolegalframeworks,disclosurecontrol,resourcesandagreementsofcosts,whereappropriate).Suchenquiriesshouldbemadeto:

ContactdetailsforthisstatisticalbulletinClaudiaWellsmortality@ons.gsi.gov.ukTelephone:+44(0)1633455867
MortalityAnalysisTeamOfficeforNationalStatisticsGovernmentBuildingsCardiffRoadNewportNP108XGTel:+44(0)1633455867E-mail:[email protected](http://www.ons.gov.uk/ons/about-ons/business-transparency/freedom-of-information/ons-charging-policy/index.html)isavailableontheONSwebsite.Wewouldwelcomefeedbackonthecontent,formatandrelevanceofthisrelease.Pleasesendfeedbacktothepostaloremailaddressabove.
6. FollowONSonTwitter(http://www.ons.gov.uk/ons/external-links/social-media/ons-twitter.html)andFacebook(http://www.ons.gov.uk/ons/external-links/social-media/index.html).
7. Detailsofthepolicygoverningthereleaseofnewdataareavailablebyvisitingwww.statisticsauthority.gov.uk/assessment/code-of-practice/index.html(http://www.statisticsauthority.gov.uk/assessment/code-of-practice/index.html)orfromtheMediaRelationsOfficeemail:[email protected]

16 October 2014
Office for National Statistics | 1
Childbearing by Registration Statusin England and Wales, Using BirthRegistration Data for 2012 and 2013Author Name(s): Oliver Dormon, ONS
Abstract
This article examines the characteristics of birth registrations occurring in England and Walesbetween 28th May 2012 and 31st October 2013. This period corresponds to the availability of newinformation on previous children and previous marriages for all women registering births, wherepreviously this had only been available for married women. This article also presents comparisonsbetween births registered by same sex female couples with other registrations.
Introduction
The principal variables used for this investigation relate to whether a woman has been previouslyor ever married, and how many children she has previously had which allows us to identify firsttime mothers and mothers who have already had at least one child. These variables are theones improved by changes to the Population Statistics Act that came into force on 28th May 2012.
Investigation of the quality of these new data that expand the coverage of aspects of the registrationdata is ongoing at ONS. Some unexpected results have been identified in the proportion of womenreporting a previous birth, which is thought to affect all ages, and all registration groups. Furtherinformation on this can be found in a companion paper published today (The paper can be found onour methodology page). Given the unexpected size of the difference between the new data and olddata on previous children, this paper represents our current findings and the results of exploratoryanalysis, and should not be used for purposes that require precise figures. However this paper doesprovide the first detailed breakdown of age of mother at first birth by registration types and also thefirst insight into registrations made by same sex couples under Human Fertilisation and EmbryologyAct 2008 (HFEA).
There were just over 1 million live births (1.02 million) occurring between 28th May 2012 and 31stOctober 2013. Therefore these data provide the scope for examination of some relatively raregroups.
Table 1 gives overall figures and defines some of the terms used in this paper for clarity. Becausethis paper is concerned with births rather than the life course of women, it is important to understand

16 October 2014
Office for National Statistics | 2
what can and can’t be inferred from the data. The analysis looks at point in time data, for birthsregistered in a specific time period, and the status of the women registering those births at thattime. Throughout this paper it is important to remember that the registration groups apply onlyto the status of the woman at the time of the birth, and will be fluid over a woman’s lifetime. Forexample it should be assumed that where women are described as “cohabiting”, this is synonymouswith “cohabiting at the time of the baby’s birth”. For the sake of simplicity, short labels are used todescribe the different groups, but the information in table 1 should be used to aid understanding ofeach group.
Table 1 : Description and distribution of registration types
Label foranalysis
Marital births Cohabiting births Non-cohabitingbirths
Lone births
Explanation ofgroup
Births to womenwho are married
or in a civilpartnership at
the time of birthregistration.
Throughout thispaper “married”is used to mean“married or in a
civil partnership”except where
specifically statedotherwise.
Births registeredby a couple who
are currentlyliving at the sameaddress, but whoare not currently
married or civilpartnered.
Births registeredby a couple who
give differentaddresses, so donot live together. No information
is available onwhat the actual
partnershipstatus of thesecouples is, but
both parents areregistered.
Births to womenwho register
the birth as asole registration.
No informationon the father is
recorded, and weassume these are
lone parents atregistration.
Number of birthsin group (28 May2012 - 31 October2013)
538,104 (53%) 319,193 (31%) 107,845 (11%) 58,291 (6%)
Table source: Office for National Statistics
Download table
XLS format(26 Kb)
How Have Types of Birth Registration Changed Over Time?
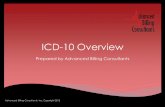
Figure 1 gives context by showing the changing pattern of births by registration type in Englandand Wales over time. In 1986 (the earliest year for which comparable data are available on birthregistrations) nearly 80% of births were to married women, but by 2013 this had declined to justover 50%. Here the 2013 figure relates only to births occurring in calendar year 2013, and is givento allow comparison with the 1986 and 2003 figures.

16 October 2014
Office for National Statistics | 3
Figure 1 – Birth registrations by type, 1986, 2003 and 2013, England and Wales
Source: Office for National Statistics
Notes:1. Click on chart image to enlarge
Download chart
XLS format(18 Kb)
What Proportion of Births are to Previously Married or Remarried Women?
Overall only 6.1% of births were registered by previously married or remarried women. With thenew data available to ONS these figures can be broken down to give a more complete picture ofbirth registrations. Figure 2 shows the births broken down into eight categories. It is immediately
clear that births to first time married1 women made up approximately half of all births in this period,reflecting the traditional majority situation for childbearing. While this group still made up the majorityof births, its share has declined substantially over time. It is also clear from these figures that themarried group is dominated by women who have not been married before, with births to thesewomen accounting for more than 20 times as many births as to remarried women.

16 October 2014
Office for National Statistics | 4
Figure 2 : Total births by registration group and whether mother previously married, May2012 – October 2013 (labels show % of total)
Source: Office for National Statistics
Notes:1. Click on chart image to enlarge
Download chart
XLS format(26 Kb)
This pattern was repeated for other birth registration groups; women who have been previouslymarried (widows and divorcees) are also the minority among those not currently married. Womenwho are lone parents when registering a birth are the group most likely to have been previouslymarried, with 8.3% of lone mothers registering a birth having been previously married.
Births registered by previously married women tend to take place at older ages. They are moreconcentrated in the 35-44 age group, with 51.8% of births to previously married women takingplace at this age, compared to only 22.8% for women who have not been previously married.
Notes
1. “Married” and “previously married” are used to encompass “married or in a civil partnership”and “previously married or in a civil partnership” respectively. This is done for the sake ofconciseness and readability of the paper. Where civil partnerships are considered separately,this will be clearly noted.
Comparing Registration Status for First Births with Subsequent Births
Overall approximately 34.6% of births between 28th May 2012 and 31st October 2013 were firstbirths. Table 2 shows that nearly half of all first births occurred within marriage, and slightly over athird were to women who were cohabiting. Roughly one in nine first births were registered by womenwho were not cohabiting, but who provide information on the father, and about one in sixteen wereregistered by lone mothers.
Proportionally more second and higher order births were registered within marriage than first births,which suggests that some women have their first birth outside marriage but then marry before

16 October 2014
Office for National Statistics | 5
a second or higher order birth. In contrast, second and higher order births were less likely to beregistered to cohabiting couples, so it is likely that most of the difference will be due to womencohabiting at their first birth and being married by their second or higher order birth.
Table 2 : Proportion of first / subsequent births in each registration group (May 2012 -October 2013)
Proportion of births in each registration group
First Births Second and higher orderbirths
Marital Births 47.3% 55.8%
Cohabiting Births 35.2% 28.8%
Non-cohabiting Births 11.3% 10.1%
Lone Births 6.3% 5.3%
Total number of births 385,304 726,870
Table source: Office for National Statistics
Download table
XLS format(25.5 Kb)
How Does Proportion of First Births Vary by Registration Group?
One of the key differences between registration groups is whether women have previous children,or the birth they are currently registering is their first. Figure 3 shows that this varies substantiallyby registration type. Nearly half of registrations to women who are cohabiting and to lone mothers(for women who have never been married) are first births. This compares to 1 in 5 for previouslymarried lone mothers and less than 1 in 7 for previously married women who were partnered but notcohabiting.

16 October 2014
Office for National Statistics | 6
Figure 3 : % of births that are first births, May 2012 – October 2013
Source: Office for National Statistics
Notes:1. Click on chart image to enlarge
Download chart
XLS format(25.5 Kb)
It is worth noting that there is an age component to these figures. Women’s relationship status willchange over time, and it is expected that older women will be more likely to have previous children,or to have been previously married. Table 3 shows the percentage of births that are first births foreach of the registration groups, by age.

16 October 2014
Office for National Statistics | 7
Table 3 : Proportion of births that are first births by registration group, May 2012 – October2013
Marital Births Cohabiting Births Non-cohabitingBirths
Lone BirthsProportionof birthsthat arefirstbirths
Mothernotpreviouslymarried
Motherpreviouslymarried
Mothernevermarried
Motherevermarried
Mothernevermarried
Motherevermarried
Mothernevermarried
Motherevermarried
Under 20 68% 39% 71% 66% 76% 73% 76% 68%
20-24 47% 40% 50% 35% 48% 32% 49% 33%
25-29 41% 30% 41% 27% 28% 17% 32% 22%
30-34 34% 26% 38% 25% 23% 13% 26% 19%
35-39 23% 20% 36% 22% 22% 10% 26% 16%
40-44 21% 17% 34% 19% 25% 10% 33% 17%
45+ 35% 23% 42% 26% 30% 15% 42% 28%
Table source: Office for National Statistics
Table notes:1. Caution must be taken when interpreting figures for previously married women under age 20 as the number of
births in these groups is very small.
Download table
XLS format(26.5 Kb)
As an example of how to interpret table 3, for women who were aged 35-39, non-cohabiting and hadbeen ever married, only 10% of births were first births, meaning that 90% of the women registering abirth in this group already had at least one other child.
As would be expected the proportion of births that are first births declines with age for virtually allgroups, from age 20-24 to age 40-44. The proportion of births that are first births actually increasesfor all groups for women aged 45 and over, but this age group represents relatively few births(approximately 2,800 in total). The reason for this spike at the end of the series is unclear from thedata available, but it is reasonable to assume that Assisted Reproductive Technology (ART) use inolder women will play a part in increasing first births at this age.
Table 3 shows that differences in previous children between registration groups hold even whenage is taken into account. It is also evident that for all registration types, women who havebeen previously married are more likely to have had previous children than those who have notbeen previously married, as fertility rates are higher within marriage than outside marriage.

16 October 2014
Office for National Statistics | 8
How Does Mean Age of Mother at Birth Vary by Registration Group?
This section looks at the mean age of childbearing for each registration group, in particular
examining any differences. Table 4 shows the mean age (unstandardised1) of mothers at the timeof the birth. This is also split into mean age for first births, second and subsequent births (where awoman states she has two or more previous children).
Table 4 : Mean age of mother by birth order and registration group, May 2012 - October 2013
Mean age of mother (in years) at...
First Birth Second Birth SubsequentBirths
All Births
Marital Births 30.7 32.0 33.1 31.9
Cohabiting Births 27.3 28.6 30.6 28.5
Non-cohabitingBirths
23.5 26.1 30.1 26.1
Lone Births 24.3 26.5 30.6 26.8
All Births 28.3 30.2 32.0 29.9
Table source: Office for National Statistics
Download table
XLS format(25.5 Kb)
As would be expected the mean age of first birth was lower than for all births. The mean age forsecond births was similar to the mean age for all births, and the mean age of subsequent births wasthe highest. The highest mean age of first births was for births registered within marriage, where themother was on average 30.7. This can be compared to the mean age of first births registered bynon-cohabiting women at 23.5, more than seven years younger.
The mean age of births registered by lone women and non-cohabiting women was similar forall numbers of previous children shown here, suggesting that these groups have a similar agepattern. In contrast births registered to cohabiting women tended to be to older women, with meanages between the relatively high mean ages of mother for marital births, and relatively lower meanages of mother for lone and non-cohabiting births. The mean age of subsequent births for non-cohabiting women is the same as for cohabiting women, despite the very different mean ages of firstand second births for these groups.
As previously noted because women can move between registration groups we cannot calculate(and the data do not imply) an “average time between births” for any specific group. The womenregistering a second birth in any given group could have had their first birth in another group, as was

16 October 2014
Office for National Statistics | 9
suggested by the information in table 2. This means the average ages must be interpreted with care,but still give a good overall picture of the births being registered.
Notes
1. To produce age standardised comparisons would require data on population sizes byregistration status. These are not available, and could not be reliably created given the fluidnature of registration groups. This means that the mean ages are unstandardised, and so will beaffected by the age distribution of women within each group.
How are Births Distributed Between Ages and Registration Groups?
Figure 4 shows the number of first and subsequent births to each registration group by age. Thishelps to put the information in Table 4 into context. All groups had more first births than subsequentbirths under age 20, but for older age groups, there were more subsequent births (with the exceptionof cohabiting women who had slightly more first births than subsequent in the 20-24 age group).
Looking at the married group, the largest in the data, we can see that first and subsequent birthsfollow the same age pattern, a roughly normal distribution peaking at age 30-34 , but there weremore than twice as many subsequent births as first for women aged 20-44. This can be comparedto the pattern for cohabiting women, where the distributions do not match, as first births tend to beat younger ages than subsequent births. As noted earlier this is likely to be because some womenwill register their first birth outside marriage, and then register a subsequent birth within marriage,emphasising that the registration groups are fluid.
Births to the youngest women (those aged under 25) are most common among lone mothers andnon-cohabiting mothers, with roughly half of the births to these groups being registered by womenaged under 25. Around one third of births to cohabiting women took place at ages under 25, andrelatively few, only one in every 14, marital births were registered by a woman aged under 25.
Births registered by lone mothers and non cohabiting women were more concentrated in theyounger ages, whereas marital births were more concentrated between ages 25 and 39. The largestproportion of births to women aged over 40 was for marital births, with approximately 5% of maritalbirths occurring over this age.

16 October 2014
Office for National Statistics | 10
Figure 4 : First and subsequent births to each registration group by age, May 2012 - October2013
Source: Office for National Statistics
Notes:1. Please note the scale of the Y-axis varies between registration groups.2. Click on chart image to enlarge
Download chart
XLS format(26 Kb)
What do we Know About Same Sex Female Parents?
Births to same sex parents are a relatively new occurrence with regards to birth registrationsin England and Wales. The Human Fertilisation and Embryology Act 2008 (HFEA) containedprovisions enabling two females in a same sex couple to register a birth from 1 September 2009
onwards1. These births make up a very small proportion of the total births registered in this period,so although we can do some overview analysis, caution must be taken when drawing conclusionsfrom these figures.

16 October 2014
Office for National Statistics | 11
Approximately 0.13% of births (around 1,250 births) registered in the period were registered underthis Act during the period May 2012 to October 2013. These births were more likely to be within alegal union (70% registered within civil partnership) compared to other births (53% in marriage). Themajority of the remainder were registered by a cohabiting couple (25%) with approximately 3% eachof HFEA births being registered by lone mothers or non-cohabiting mothers. It is likely that this isa result of the more conscious process and intentions that same sex couples go through to have ababy (all registrations under HFEA will by definition have been planned).
Table 5 shows some key statistics that are compared between HFEA and all other registrations.
Table 5 : HFEA and other registrations compared , May 2012 – October 2013
Measure HFEA Registrations All other Registrations
Proportion of women married orin a civil partnership
70% 53%
Average age of mother at births 33.8 years 29.9 years
Proportion of first / subsequentbirths
67% first births, 33%subsequent births
38% first births, 62%subsequent births
Percentage of womenpreviously married or civil
partnered
8.4% 6.1%
Table source: Office for National Statistics
Download table
XLS format(25.5 Kb)
Table 5 shows that births registered under HFEA are more likely to be to women who have beenpreviously married or civil partnered, than births to opposite sex couples. The reasons for this areunclear, though it may be related to the older age profile of women registering a birth under theHFEA.
Births registered under HFEA parents are also much more likely to be first births, and the averageage of mother is older when compared to other births. This is likely to be a factor of access to fertility
treatment (NICE3 guidelines establish a lower age limit to NHS funded fertility treatment). Individualchoices may also play a part, but that is outside the limits of our analysis.
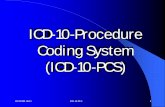
Figure 5 shows the grouped age distribution of the age of mother for HFEA registrations comparedwith all other registrations. As with partnership status it is likely that the more planned nature ofbirths to same sex couples has an impact here, as there are more births to older women. TheHFEA distribution shows much smaller proportions of births to women aged under 30 but largerproportions to women aged over 30. As previously mentioned, the number of births to same sex

16 October 2014
Office for National Statistics | 12
couples is much smaller than to opposite sex couples so the figures are likely to be more prone tovariation.
Figure 5 : Distribution of births by age of mother; HFEA and all other registrations compared,May 2012 – October 2013
Source: Office for National Statistics
Notes:1. Click on chart image to enlarge
Download chart
XLS format(18 Kb)

16 October 2014
Office for National Statistics | 13
Notes
1. The process for two men to register as the parents of a baby is different and is not processedthrough birth registrations, and so it is not possible to present any information on male same sexparents here.
2. Here 'same sex' is used to denote births registered under HFEA regulations, and opposite sex isall other births.
3. The National Institute of Clinical Excellence (NICE) regulates many aspects of NHS funding andtreatment options.
Summary Points
• There were a total of 1.02 million births registered between 28th May 2012, and 31st October2013, of which 53% were within marriage and 31% were to cohabiting women.
• The majority of births were to women who had not been previously married, with only 6.1%of all births to previously married or remarried women. Lone mothers registering a birth wereproportionally most likely to have been previously married (8.3% of lone births were to previouslymarried women).
• About half of all first births took place within marriage (47.3%), and this increased for second andsubsequent births (55.8%).
• Births to never married cohabiting women were the most likely to be first births (44% were firstbirths), and those to previously married non cohabiting women were the least likely (14% werefirst births).
• The mean age of mother at first birth was highest for births registered within marriage (30.7years) and lowest for births registered by non-cohabiting women (23.5 years).
• Approximately half of all births registered by lone mothers and non-cohabiting mothers were towomen aged under 25.
• Births registered to same sex female parents under HFEA regulations showed an older averageage of mother (33.8), and were more likely to be in a legal union (70%) than other births.
Conclusions
This paper has looked at the characteristics of births registered between late May 2012 and the endof October 2013, based on their registration group. It is clear that there are substantial differencesbetween births in each registration group, with regard to the age of mother and also the likelihood ofa birth being the mother’s first or subsequent birth. Figure 3 showed that the difference in proportionof births that are first can be substantial when different registration groups are compared.
It is also clear that births to first time married women, and women who are cohabiting but have neverbeen married, make up the majority of births, and that births registered in these groups tend to havean older age of mother than births registered by lone mothers or non-cohabiting mothers.

16 October 2014
Office for National Statistics | 14
Some insight is also gained into the patterns for women registering births in same sex couples,where 95% were registered to civil partnered or cohabiting women, a much higher proportion inmore established couples than for opposite sex couples.
As more data become available valuable insight could be gained by examining the registrationgroups in more detail. Currently the proportion of first births that take place within marriage is slightlybelow the proportion of all births that take place in marriage and the proportion of first births thatare registered by cohabiting couples is slightly above the proportion of all births registered bycohabiting couples. This could be caused by women having their first birth outside marriage, andthen subsequent births within marriage. This would also explain why births outside marriage tendto have a lower age of mother. If this trend continues we could see further differences between theregistration groups, and divergence, even if the overall level of births within marriage remainedconstant.
Substantial differences exist between registration groups for births in 2012 and 2013, and furtherresearch is needed as more data becomes available to help understand what we can learn from thenew Population Statistics Act data.
Background notes
1. Details of the policy governing the release of new data are available by visitingwww.statisticsauthority.gov.uk/assessment/code-of-practice/index.html or from the MediaRelations Office email: [email protected]
These National Statistics are produced to high professional standards and released according tothe arrangements approved by the UK Statistics Authority.
Copyright
© Crown copyright 2014
You may use or re-use this information (not including logos) free of charge in any formator medium, under the terms of the Open Government Licence. To view this licence, visitwww.nationalarchives.gov.uk/doc/open-government-licence/ or write to the Information Policy Team,The National Archives, Kew, London TW9 4DU, or email: [email protected].
This document is also available on our website at www.ons.gov.uk.