Results Elective Duodenal Ulcer Surgery...
6
Results of Elective Duodenal Ulcer Surgery in Women: Comparison of Truncal Vagotomy and Antrectomy, Gastric Selective Vagotomy and Pyloroplasty, Proximal Gastric Vagotomy J. LYNWOOD HERRINGTON, JR., M.D., JOHN L. SAWYERS, M.D. This study provides a retrospective comparative analysis of re- sults in 90 women patients who underwent three different elec- tive operations for intractable duodenal ulcer disease. Group I (30 patients) underwent truncal vagotomy/antrectomy (TV+A); Group II (30 patients) gastric selective vagotomy/pyloro- plasty (GSV+P); and Group III proximal gastric vagotomy (PGV). There were no operative deaths among the 90 pa- tients. No patient after TV+A has developed a recurrent ulcer. Two recurrent ulcers developed after GSV+P, and one gastric ulcer occurred after PGV. Dumping, diarrhea, and reflux gas- tritis were lower after PGV than with TV+A and GSV+P. Fol- low-up studies have been from six months to ten years. The clinical results among the three groups of women patients com- pare favorably with results obtained in a recent prospective randomized study using the identical operative procedures in three groups of men patients operated upon for intractability. There was no statistically significant difference between women and men after similar operative procedures, but the post- gastrectomy sequelae were less after PGV in both women and men patients. HROUGHOUT THE EXTENSIVE LITERATURE on the I surgical treatment of duodenal ulcer, scant data exists comparing long-term results between men and women patients. Even rarer are reports dealing solely with results limited to women. Nevertheless the im- pression exists that long-term clinical results in women compare unfavorably with men, particularly when the indication for operation is intractability. This study was designed to provide a retrospective comparative analysis of results among three groups of adult women who underwent different operations for chronic duodenal ulcer. In addition, clinical results are compared to results from a prospective randomized study of adult men with chronic duodenal ulcer who underwent the same duodenal ulcer operations. The Presented at the Annual Meeting of the Southern Surgical Association, Hot Springs, Virginia, December 5-7, 1977. Reprint requests: John L. Sawyers, M.D., St. Thomas Hospital, P.O. Box 380, Nashville, Tennessee 37202. Submitted for publication: December 8, 1977. From the Department of Surgery, Vanderbilt University, and the Surgical Service of St. Thomas and Metropolitan Nashville General Hospitals, Nashville, Tennessee principal indication for operation in each patient was intractability, and no patient with active bleeding, acute perforation, or obstruction was introduced into this study. Clinical Material The 90 women in this study were divided into three groups of 30 patients each. Group I (average age 49 years) underwent truncal vagotomy +antrectomy (TV +A); Group II, gastric selective vagotomy+pyloroplasty (GSV+P) (average age 40 years); and Group III (aver- age age 45 years) proximal gastric vagotomy (PGV) (Fig. 1). Follow-up studies on the patients extends from six months to ten years with the majority of patients being followed more than four years (Table 1). Operating Techniques The technique of truncal vagotomy+antrectomy has been previously described by us.9.10'14 A 2-3 cm seg- ment is excised from both the anterior and posterior vagal nerve trunk. Approximately 40% of the distal stomach is removed taking care that the distal resection extends beyond the pylorus. Gastrointestinal contin- uity is reestablished by the Schoemaker modification of the Billroth I gastroduodenostomy. Gastric selective vagotomy divides all vagal fibers to the stomach, but leaves the hepatic and celiac rami intact.8 In addition, the dissection is carried cephalad 5 cm above the esophagogastric junction as is done with proximal gastric vagotomy. A Finney pyloroplasty was 0003-4932-78-0500-0576-0085 © J. B. Lippincott Company 576
Transcript of Results Elective Duodenal Ulcer Surgery...

Results of Elective Duodenal Ulcer Surgery in Women:
Comparison of Truncal Vagotomy and Antrectomy, Gastric SelectiveVagotomy and Pyloroplasty, Proximal Gastric Vagotomy
J. LYNWOOD HERRINGTON, JR., M.D., JOHN L. SAWYERS, M.D.
This study provides a retrospective comparative analysis of re-sults in 90 women patients who underwent three different elec-tive operations for intractable duodenal ulcer disease. Group I(30 patients) underwent truncal vagotomy/antrectomy (TV+A);Group II (30 patients) gastric selective vagotomy/pyloro-plasty (GSV+P); and Group III proximal gastric vagotomy(PGV). There were no operative deaths among the 90 pa-tients. No patient after TV+A has developed a recurrent ulcer.Two recurrent ulcers developed after GSV+P, and one gastriculcer occurred after PGV. Dumping, diarrhea, and reflux gas-tritis were lower after PGV than with TV+A and GSV+P. Fol-low-up studies have been from six months to ten years. Theclinical results among the three groups of women patients com-pare favorably with results obtained in a recent prospectiverandomized study using the identical operative procedures inthree groups of men patients operated upon for intractability.There was no statistically significant difference between womenand men after similar operative procedures, but the post-gastrectomy sequelae were less after PGV in both women andmen patients.
HROUGHOUT THE EXTENSIVE LITERATURE on the
I surgical treatment of duodenal ulcer, scant dataexists comparing long-term results between men andwomen patients. Even rarer are reports dealing solelywith results limited to women. Nevertheless the im-pression exists that long-term clinical results in womencompare unfavorably with men, particularly when theindication for operation is intractability.
This study was designed to provide a retrospectivecomparative analysis of results among three groups ofadult women who underwent different operations forchronic duodenal ulcer. In addition, clinical results arecompared to results from a prospective randomizedstudy of adult men with chronic duodenal ulcer whounderwent the same duodenal ulcer operations. The
Presented at the Annual Meeting of the Southern SurgicalAssociation, Hot Springs, Virginia, December 5-7, 1977.
Reprint requests: John L. Sawyers, M.D., St. Thomas Hospital,P.O. Box 380, Nashville, Tennessee 37202.
Submitted for publication: December 8, 1977.
From the Department of Surgery, Vanderbilt University,and the Surgical Service of St. Thomas and Metropolitan
Nashville General Hospitals, Nashville, Tennessee
principal indication for operation in each patient wasintractability, and no patient with active bleeding, acuteperforation, or obstruction was introduced into thisstudy.
Clinical Material
The 90 women in this study were divided into threegroups of 30 patients each. Group I (average age 49years) underwent truncal vagotomy +antrectomy (TV+A);Group II, gastric selective vagotomy+pyloroplasty(GSV+P) (average age 40 years); and Group III (aver-age age 45 years) proximal gastric vagotomy (PGV)(Fig. 1).
Follow-up studies on the patients extends from sixmonths to ten years with the majority of patients beingfollowed more than four years (Table 1).
Operating Techniques
The technique of truncal vagotomy+antrectomy hasbeen previously described by us.9.10'14 A 2-3 cm seg-ment is excised from both the anterior and posteriorvagal nerve trunk. Approximately 40% of the distalstomach is removed taking care that the distal resectionextends beyond the pylorus. Gastrointestinal contin-uity is reestablished by the Schoemaker modificationof the Billroth I gastroduodenostomy.
Gastric selective vagotomy divides all vagal fibersto the stomach, but leaves the hepatic and celiac ramiintact.8 In addition, the dissection is carried cephalad5 cm above the esophagogastric junction as is done withproximal gastric vagotomy. A Finney pyloroplasty was
0003-4932-78-0500-0576-0085 © J. B. Lippincott Company
576

RESULTS OF ULCER SURGERY 577
FIG. 1. Retrospective Study-90 female patients.
TRUNCAL VAGOTOMY -
ANTRECTOMY
30 patients
GASTRIC SELECTIVEVAGOTOMY-PYLOROPLASTY
30 patients
PROXIMAL GASTRICVAGOTOMY
30 patients
used as the complementary drainage procedure in allpatients.The technique ofproximal gastric vagotomy has been
identical to that described by Goligher and Johnston.6"2The entire lesser gastric curve is freed of all neuro-
vascular attachments beginning cephalad to the antralparietal border as defined by the insertion of the an-
terior nerve of Latarjet onto the lesser curvature(Crow's foot) and extending 5-6 cm cephalad to thegastroesophageal junction. The anterior and posteriornerves of Latarjet supplying the gastric antrum andthe hepatic and celiac branches are left intact. Thecriminal nerve of Grassi, from the posterior vagal trunkto the gastric fundus,7 is divided, and the distal esopha-gus carefully circumscribed to divide any vagal fibrilsrunning down the esophageal wall. As a final step, thelesser gastric curve is imbricated by approximating theanterior and posterior walls.
Hospital Complications
There was no operative or hospital mortality amongthe 90 patients. One patient in the PGV group diedsix months following operation of unrelated causes andis included in the follow-up data. There have been no
additional deaths during the long-range study.In the TV+A group, two patients had significant
wound infections, and one patient developed a pulmo-nary embolus but survived. No other patient amongthe three groups has had a suspected or proven pul-monary embolus or significant respiratory or cardiaccomplication during hospitalization. Among the GSV+Ppatients one wound infection occurred. In the PGVgroup, one patient underwent iatrogenic splenectomyand developed a left subphrenic abscess requiring
drainage. Two additional patients developed minorwound infections (Table 2). Ten of the 30 PGV pa-
tients (33.3%) upon careful questioning experiencedepigastric fullness and early satiety. In five of thesepatients, symptoms disappeared completely in two tothree weeks, but in the remaining five, mild symptomsextended into the long-range follow-up in four, andone patient required reoperation for poor gastricemptying.
Results
The one patient in the PGV group who died sixmonths postoperatively after a sudden episode of non-occlusive mesentric vascular disease had obtained anexcellent clinical result up to the time of her fatal ill-ness. All other patients have been followed closely byrepeated examinations, including clinical evaluation,gastrointestinal roentgen studies, endoscopy, and gas-tric secretory analysis when indicated.
TABLE 1. Length of Follow-up
TV + A GSV + P PGVNo. Pts. No. Pts. No. Pts.
9-10 yr 18-9 yr 17-8 yr 26-7 yr 65-6 yr 44-5 yr 14 5 63-4 yr 6 5 72-3 yr 5 6 71-2 yr 5 0 46moto lyr 0 0 6
30 30 30
VOl. 187.o NO. 5

Ann. Surg. * May 1978HERRINGTON AND SAWYERS
TABLE 2. Mortality-Morbidity
TV + A GSV + P PGV
Operative mortality 0 0 0Wound infection 2 1 2Pulmonary embolus 1 0 0Subphrenic abscess 0 0 1
Results have been recorded using the Visick classi-fication with Visick I (excellent result) representingthe patient who is free of all gastrointestinal complaintsand is in an excellent nutritional state. Visick II (goodresult) represents a patient with mild fullness, milddiarrhea, or occasional dumping. The patient is free ofulcer disease and in excellent nutritional state. TheVisick III (fair result) represents a patient with ap-preciable dumping symptoms, significant reflux gastri-tis, and/or moderate diarrhea. A Visick IV (poor result)indicates the patient with recurrent ulcer, severe nu-tritional deficits or severe postgastrectomy problems.
Results, tabulated in Table 3, have been analyzed byour biostatistical department. The Visick I grading inthe PGV group (77%) represents a statistically signifi-cant difference (p < 0.5) over the Visick I grading inthe TV+A and GSV+P groups. No other significantdifference exists in the overall clinical results. Al-though satisfactory results (Visick I and II) were ob-tained in 97% of the PGV group, there was no sig-nificant difference between these and those in theTV+A or GSV+P groups as regards excellent and goodresults (Visick I and II).
Long-range Sequelae
Long-range complications are recorded in Table 4.The incidence of dumping was less after PGV whencompared to both TV+A and GSV+P. With the lattertwo operations, the dumping syndrome occurred withalmost equal frequency. No patient, however, experi-enced dumping to a severe or incapacitating degree.Diarrhea was less in patients who had PGV and GSV+Pand higher after TV+A. Because of the small numberof patients having diarrhea, the statistical evaluationshowed only a borderline difference between PGV and
TABLE 3. Overall Clinical Appraisal
TV+A GSV + P PGV
Visick I (16) 53%1 83% (15) 50% 90% (23) 77%* 197%Visick II (9) 30% (12) 40%1 (6) 20%Visick III (2) 7% (1) 3% (0) 0%Visick IV (3) 10% (2) 7% (1) 3%
30 Pts. 30 Pts. 30 Pts.
* p < .05.
TABLE 4. Long-range Sequelae
TV + A GSV + P PGV
Dumping (6) 20% (7) 23% (1) 3%Diarrhea (5) 17% (2) 7% (1) 3%Epigastric fullness (3) 10% (2) 7% (5) 17%Reflux gastritis (5) 17% (3) 10% (0) 0%Weight loss (3) 20% (2) 7% (0) 0%
TV+A as regards the incidence of diarrhea (p = .07).Seventeen per cent of patients experienced mild tomoderate diarrhea after TV+A, but no patient de-veloped severe diarrhea.
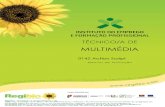
Persistent epigastric fullness has been more commonin patients who had PGV than TV+A or GSV+P. Fourof the five patients in the PGV group continue to ex-perience mild fullness over a one to three year follow-up. One patient experienced severe epigastric fullnessand delayed gastric emptying which necessitated antralresection six months following the initial operation(Figs. 2 and 3). She is now doing well almost fouryears postresection, but is classified as a poor result(Visick IV).There is a significant difference in the incidence of
reflux gastritis with TV+A and GSV+P when com-pared to PGV. Of the five patients in the TV+A groupwith reflux, symptoms were of such severity in threethat Roux-en-Y diversion became necessary. Thesethree patients represent poor results (Visick IV). Thetwo remaining patients are currently being managedmedically and are classified as fair results (Visick III).The three patients in the GSV+P group have mild refluxsymptoms and are being managed by conservativemeans.
Weight loss has not been a major problem after anyofthe three operative procedures. No patient after PGVhas lost weight, and actually five of the 30 patients havegained weight. No excessive weight loss has occurredafter TV+A or GSV+P.
Recurrent Ulcer
Frequent and thorough evaluations during thefollow-up study have shown that no patient afterTV+Ahas developed a proven or suspected recurrent duo-denal ulcer. Likewise, no gastric ulcer has occurred inthe group (Table 5).Among the GSV+P patients, one recurrent duodenal
ulcer and one gastric ulcer have developed. The re-current duodenal ulcer became manifest by the onsetof epigastric pain five years postoperative in a 27-year-old patient. The ulcer was demonstrated by both x-raystudy and endoscopy. Treatment consisted of antral re-section.The gastric ulcer occurred in a 31-year-old patient
578

RESULTS OF ULCER SURGERY 579seven years postoperative. It was manifest by the on-
set of epigastric pain, and the ulcer was located on theposterior wall of the distal antrum. The duodenal ulcer
had remained healed. There was no evidence of gastric
stasis and the patient had received no ulcerogenic medi-
cation. The Hollander test which had been negativefollowing GSV+P had reverted to positive. At reopera-tion an intact nerve fiber was found on the posterioresophageal wall coursing down to the gastric fundus.
The nerve was divided and the gastric selective vago-
tomy was converted to truncal vagotomy. The gastric
antrum was then removed. The patient has done well
since this procedure which was carried out over three
years ago. The nerve coursing along the posterioresophageal wall probably represented the criminalnerve of Grassi which is the most cephalad of the lX
gastric nerve fibers originating from the posterior nerveof Latarjet. Both of these patients are listed as poorresults (Visick IV).
No recurrent duodenal ulcer has developed in the
PGV group. The patient with epigastric fullness and
As*
FIG. 3. Upper gastrointestinal contrast study in the same patientfollowing antral resection with a Billroth I reconstruction.
gastric stasis previously alluded to was also found on
endoscopy to have a 3 mm superficial antral ulce'r, but
the duodenal ulcer had remained healed (Table 5). She
has been recorded a poor result (Visick IV).
Gastric Secretory Data
Postoperative gastric analysis was done in the TV+A
and the PGV groups only if circumstances arose which
warranted such studies. In the GSV+P group, 63% of
patients were subjected to the Hollander test. Seven-
teen patients had negative response and two patients
~~~~~~~~~~~demonstrated an early positive response, but neither
has developed a recurrent ulcer. Two of the 17 patients
with a negative test during the early postoperative pe-
TABLE 5. Recurrent Ulcer
FIG. 2. Upper gastrointestinal barium study showing gastric retentionfollowing PGV.
TV + A GSV + P PGV
Duodenal ulcer 0 1 0Gastric ulcer 0 1 1
Vol. 187 . No. 5

HERRINGTON AND SAWYERS
TABLE 6. Comparative Results -Women vs. Men
TV + A
Women Men
Visick I 16 (53%) 83% Visick I 28 (56%) 94%Visick II 9 (30%) 8 Visick II 19 (38%)Visick III 2 (7%) Visick III 0 (0%)Visick IV 3 (10%) Visick IV 3 (6%)
30 Pts 50 Pts
riod later reverted to positive. One ofthese cases repre-
sents the patient who developed the gastric ulceration.
Comparative Results (Women vs. Men)
In a recently published prospective randomizedstudy comparing TV+A, GSV+P, and PGV in adultmen with duodenal ulcer intractability,13 we found thatexcellent and good results (Visick I and Visick II) wereobtained in 94% of patients with TV+A, 84% withGSV+P, and 96% with PGV.
In a comparison of clinical results with TV+A inwomen from this present study and in men from theprospective randomized study, we find that the excel-lent results (Visick I) in both groups are approximatelyequal, 53% and 56%. Although 94% of men obtainedoverall satisfactory results (Visick I and Visick II) as
opposed to 83% for women, this is not statisticallysignificant.
In comparison of women and men patients who un-
derwent GSV+P, there was not a significant difference(p = .05) in Visick I grading, being 73% for men and50% for women. The overall satisfactory results (VisickI and II) also show no significant difference (Table 7).The Visick I and II grading, satisfactory results, after
PGV were almost equal among men and women pa-
tients (Table 8). Also, in both sexes PGV was associ-ated with less dumping, diarrhea, and reflux gastritisthan TV+A and GSV+P (Table 9).
Discussion
Results of duodenal ulcer surgery in adult women
have received little consideration in the literature.
TABLE 7. Comparative Results -Women vs. Men
GSV + P
Women Men
Visick I 15 (50%) 190% Visick I 27 (73%) 183%Visick II 12 (40%) | Visick II 4 (11%)Visick III 1 (3%) Visick III 5 (13%)Visick IV 2 (7%) Visick IV 1 (3%)
30 Pts 37 Pts
Some surgeons contend that the overall clinical resultsin women are inferior to men, but conclusions havelargely been based on assumptions rather than com-
parative studies. Minimal or borderline indications fordefinitive ulcer operation may account for some of theunsatisfactory results. This has been our impressionfrom evaluation of some of the women referred forconsideration of remedial surgery for postgastrectomysequelae. In Amdrup's current Mid Way reports3'5 on
748 patients who had either GSV+P or GSV+A andPGV with or without drainage, he found no differencein the overall results between women and men patients.
In the present study women who had either TV+Aor GSV+P obtained acceptable clinical results. Theincidence of dumping after either operation did notdiffer appreciably from that in men. It is of interestthat no women presented with either severe diarrheaor severe dumping. The most frequent unsatisfactoryresult in women with TV + A and GSV + P was refluxgastritis which is currently being recognized withgreater frequency in both women and men.
Although sufficient time has not elapsed to evaluatelong-term results of PGV, the 30 women in this studyhave done well during their six months to five year
follow-up. Except for the complication of persistentepigastric fullness, the incidence of long-term sequelaehas been remarkably low. Postprandial fullness is a
frequent complication in both women and men afterPGV. After each of the three types of vagotomy, intra-gastric pressure and transmural gastric tone are ele-vated, thus preventing the stomach from undergoingreceptive relaxation and accommodation to distention.Fortunately, this problem is transient and disappears-usually in a few weeks. Another reason for epigastricfullness after PGV may be related to the distal extentof the gastric denervation along the lesser gastriccurve. If the antrum is denervated distal to the Crow'sfoot, gastric stasis and gastric ulceration may developin a certain percentage of patients. For this reason,
Amdrup'4 prefers a less extensive distal dissection thandoes Johnston12 and leaves intact a 1-2 cm innervatedsegment of lesser curve cephalad to the Crow's foot.The long-range effectiveness of PGV without drain-
TABLE 8. Comparative Results-Women vs. Men
PGV
Women Men
Visick I 23 (77%) 97% Visick I 71 (83%) 196Visick II 6 (20%) J Visick II 11 (13%)Visick III 0 (0%) Visick III 1 (1%)Visick IV 1 (3%) Visick IV 3 (3%)
30 Pts 86 Pts
580 Ann. Surg. o May 1978

Vol. 187 . No. 5 RESULTS OF ULCER SURGERY 581
TABLE 9. Long-term Sequelae- Women vs. Men
Women Men
TVA + A GSV + P PGV TVA + A GSV + P PGV30 Pts 30 Pts 30 Pts 50 Pts 37 Pts 86 Pts
Dumping 20% 23% 3% 22% 23% 1%Diarrhea 17% 7% 3% 18% 3% 1%Reflux gastritis 17% 10% 3 4% 5% 1%Epigastric fullness 10% 7% 17% 0 8% 7%
age in preventing recurrent ulceration is unknown sincethe operation was first done only seven years ago. InJensen's experience most ulcer recurrences (bothwomen and men) appeared within 30 months, but hehas recently observed a few recurrent ulcers developafter five to six years. In Jensen's five to eight yearstudy, the recurrence rate is 9%.11 Amdrup2 predictsthat the recurrent ulcer rate of PGV will approximatethat of GSV+P.
This study indicates that definitive ulcer operationsin women with intractable duodenal ulcer yield overallsatisfactory results. There appears to be little differencein the comparative results ofTV + A and GSV + P be-tween men and women. PGV in both men and women isaccompanied by fewer postgastrectomy sequelae thanoccur after either TV + A or GSV + P.
References1. Amdrup, E., Clemmesen, T. and Andreassen, J.: Selective Gas-
tric Vagotomy. Technique and Primary Results. Am. J. Dig.Dis., 12:351, 1967.
2. Amdrup, E.: Personal communication, 1977.3. Amdrup, E., Andersen, D. and H0strup, H.: A Mid Way Report
on Primary Results in 748 Patients and Incidence of SequelsFollowing PCV and Selective Gastric Vagotomy. World J.Surg., in press.
4. Amdrup, E., Andersen, D. and Jensen, H.: Parietal Cell (highlyselective or proximal gastric) Vagotomy for Peptic Ulcer Dis-ease. World J. Surg., 1:19, 1977.
5. Andersen, D., Hostrup, H. and Amdrup, E.: A Mid Way Reporton Reduction in Acid Secretion and Ulcer Recurrence RateFollowing PCV and Selective Gastric Vagotomy. World J.Surg., in press.
6. Goligher, J. C.: A Technique for Highly Selective (parietal cellor proximal gastric) Vagotomy for Duodenal Ulcer. Br. J.Surg., 61:337, 1974.
7. Grassi, G. and Orecchia, C.: A Comparison of Intra-operativeTests of Completeness of Vagal Section. Surgery, 75:155,1974.
8. Griffith, C. A.: Selective Gastric Vagotomy. Surg. Clin. NorthAm., 46:367, 1966.
9. Herrington, J. L., Jr.: Vagotomy-Antrectomy: Surg. Clin. NorthAm., 56: 1335, 1976.
10. Herrington, J. L., Jr.: Vagotomy-Antrectomy for DuodenalUlcer-Surgical Procedures. Warner-Chilcot Laboratories 3:7, 1966.
11. Jensen, H. E.: One Hundred Patients, 5-8 Years After PCV.World J. Surg., in press.
12. Johnston, D. and Wilkinson, A. R.: Highly Selective Vagotomywithout a Drainage Procedure in the Treatment of DuodenalUlcer, Br. J. Surg., 57:289, 1970.
13. Sawyers, J. L., Herrington, J. L., Jr. and Burney, D. P.: Proxi-mal Gastric Vagotomy Randomized with Vagotomy-Antrec-tomy and Selective Gastric Vagotomy-Pyloroplasty. Ann.Surg., 186:510, 1977.
14. Sawyers, J. L. and Herrington, J. L.: Vagotomy-antrectomy.In Harkins, H. N., Nyhus, L. M. and Wastell, C., Surgeryof the Stomach and Duodenum. 3rd edition, Boston, Little,Brown and Company, in press.
DIscUSSION
DR. JONATHAN A. VAN HEERDEN (Rochester, Minnesota): Wehave felt for a long time that there is-and I might stress, fortunately-a distinct difference between men and women, as far as the resultsof peptic ulcer are concerned. It has been our clinical impressionthat women are more prone to postgastric surgery syndromes thanmen, and for this reason we have been somewhat reticent in per-forming resective procedures in women. This paper would suggest,and perhaps prove, that our belief has for many years been in error.Along the same lines, we have felt that it is crucial to identify in
both men and women the so-called "nervous puker" preoperatively;i.e., the patient who is dumping before you operate on their stomach,for they will tolerate gastric surgery poorly indeed.
Fortunately for this group of people, and for perhaps all peoplewith duodenal, and perhaps gastric ulcer disease, proximal gastricvagotomy has come on the scene. This operation is currently ourprocedure ofchoice for the surgical treatment ofduodenal ulceration,with very few exceptions. We have performed this procedure now
in just over 220 patients over the past five years, without any sig-nificant operative morbidity and no operative mortality.Thus far, there have been three proved and three suspected re-
current ulcers, for a recurrence rate of approximately 3%. As Dr.Herrington stressed, though, the last word is not in, and I don't thinkthat one can really talk about this operation before a much longertime has gone by.The reduction in gastric acid secretion (slide) in our experience
has been most gratifying. Here, for example, is a patient whosefasting pH was 1.5; basal acid output, 17.8; MAO, 36. Ten dayslater pH is 6.5, BAO is 0.38, and the MAO, 17.4.
(Slide) We wondered if we were doing the operation correctly,evaluated a series of patients, and found that our average decreasein BAO was 82%, in contrast to Dr. Goligher's group, in which itwas 92%; so we thought we were doing not too badly. The averagedecrease in MAO was 58%, in contrast to Dr. Goligher's 51%.
I would like to ask the authors the following four questions. First,in the antrectomy group in this paper, 17% of women and only 6% ofthe men fell into the Visik 3 and 4 categories. Do the authors there-