
Restorative Dentistry...• No bevels on occlusal margins • Bevel F & L of proximal box •...
97
Restorative Dentistry 2016 Review
Transcript of Restorative Dentistry...• No bevels on occlusal margins • Bevel F & L of proximal box •...

Restorative Dentistry
2016 Review

DisclaimerThe views expressed in thispresentation are those of the authorsand do not necessarily reflect theofficial policy or position ofThe Department of Defense, theUnited States Government or theAGD

Critical pH ◦ Enamel = 5.5
◦ Dentin = 6.5
Below this pH:◦ Hydroxyapatite is driven into solution
◦ Net result is demineralization
Critical organism: S mutans

Visual
Tactile
Radiographic
Transillumination

Caries disclosing agents
Elective tooth separation
Digital radiography
Qualitative Laser Fluorescence◦ DIAGNOdent
◦ Caries management by risk assessment (CAMBRA) is an evidence-based approach to preventing or treating dental caries at the earliest stages. Caries protective factors are biologic or therapeutic measures that can be used to prevent or arrest the pathologic challenges posed by the caries risk factors.

Light source may be visible light or laser diode
Viable for pit and fissures/occlusal caries only
Example: Diagnodent® (Kavo)

Recognizes pathological changes at early stage◦ Initial lesions, demineralization, etc.
Laser diode provides pulsed light onto tooth (655nm)
Healthy tooth structure: no fluorescence
Carious tooth structure: fluorescence extent of caries

Establishing Caries Risk
Low Medium High
No new carious lesions 1 new carious lesion > 1 new lesion
in 3 years in 3 years in 3 years
Adequately restored Exposed roots Hx of root caries
surfaces
Good oral hygiene Fair oral hygiene Poor oral hygiene
Regular dental visits Irregular visits Irregular visits
Incipient lesions Incipient lesions
with poor salivary flow
Ortho treatment Strep mutans >100,000
CFUs

Duraflor® varnish application each visit
OHI to include use of fluoridated toothpaste/rinse
Dietary Counseling
Xylitol gum
Digital or conventional
radiographic monitoring
Monitor closely with other
diagnostic techniques

Symptoms◦ Pain on chewing, pressure
pathognomonic- pain on release
◦ Sensitivity to cold, heat, sweets
Diagnosis◦ Masticatory test - Tooth Slooth
◦ Stain
◦ Transillumination
◦ Periodontal probing

Evaluation◦ Locate the fracture
◦ Evaluate the pulp/periodontium
Immediate treatment◦ Ortho band, reduce/round off cusp,
remove cusp, sedative restoration, bonded restoration?
Definitive Treatment◦ Complex amalgam, partial/full
coverage cast restoration

Catch-all phrase for abrasion, erosion or abfraction
Erosion-chemical; smooth and rounded
Abrasion-mechanical (cupped or notched)
Abfraction (and NCCL in general) is multifactorial
Attrition: natural wear of teeth vs teeth

Research by Garguilo, et al (1961)◦ Connective tissue attachment = 1.07 mm
◦ Epithelial attachment = 0.97 mm
◦ Sulcus = 0.7 mm
Maynard and Wilson (1979) ◦ If impinged on:
Marginal tissue recession
Apical migration of attachment
Sulcus
Epithelial
Attachment
CT Attachment

DENTINAL TUBULES
Caused by the movement of fluid in the dental tubules displaces odontoblastic cell bodies (Branstrom)

Forms before eruption
Forms most of teeth
Regularly arranged dentinal tubules◦ 1 micron wide at DEJ
◦ 5 microns wide at pulp
◦ 35,000/mm2 at DEJ
◦ 75,000/mm2 at pulp

Forms after eruption
Forms from very mild stimulus◦ Normal occlusion
Uneven deposition◦ Floor
◦ Roof of chamber

AKA Reparative Dentin
Forms in response to an insult
Odontoblasts killed and replaced by mesenchymal cells
Disorganized tubules
Decreases dentin permeability◦ Increases protection
1.5-3.5/day



Cavity Sealers 2-5m◦ Varnishes◦ DBAs
Cavity Liners < 0.5mm◦ Resins in thin layers◦ RMGI, GI, ◦ CaOH
Cavity Bases >0.5mm◦ RMGI◦ ZnPO4◦ ZOE
Summitt Oper Dent 1994

Use minimum thickness necessary◦ 0.5 - 0.75 mm under amalgam
Minimize extent of liner/base◦ Do not base to “ideal” outline
Function ◦ Reduce bulk of “shrinking” materials
◦ Block out undercuts
Choose high MOE material under amalgam

From extension for preventionto …
prevention of extension or ...
constriction with conviction
Bottom line: Restoration size no larger than necessary for caries removal and to provide adequate retention and resistance

Conservative preparation (prevention of extension)◦ Minimal loss of sound tooth structure
◦ Maintain tooth strength
Restoration strength increased◦ Smaller condenser size (amalgam)
◦ Occlusal contacts not on margins

Narrow occlusal outline ( or none)
Rounded internal line angles
Bevelled axio-pulpal line angle
Sharp axio-gingival
"S" or reverse curve
Proximal B-L walls converge occlusally

Conventional
Glass Ionomers Resin-Modified
Glass Ionomers
RMGI
Polyacid - Modified
Composite Resins
Resin Based
CompositeCOMPOMERS
Fluoride ReleaseCTE
TranslucencyTensile Strength
Fracture Toughness

Composition◦ Resin (matrix phase) - UDMA/Bis-GMA/TEGDMA
◦ Dispersed phase (fillers)
Inorganic- Quartz, Silica, Zirconium Silicate, etc
Organic- ground microfill
◦ Cured by free radical polymerization
◦ Coupling phase – silane adheres particles to matrix
◦ Resin adhesive chemically links (polymerizes) to resin matrix

5
2.5
1.0
.5
.04 .
Small Particle
Minifill
Point 4 Microfill
Mic
ron
s

Filler◦ Glass/quartz, 1-10 (80+%)
◦ Colloidal silica, .04 (10 - 20%)
50 - 88% filled by wt
40 - 70% filled by vol
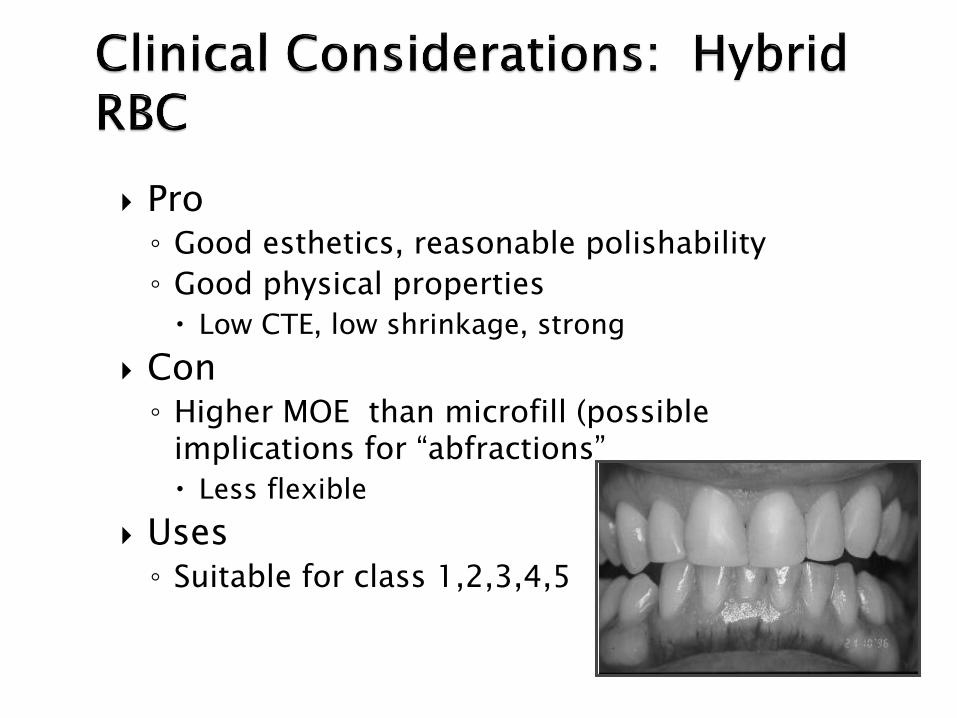
Pro ◦ Good esthetics, reasonable polishability
◦ Good physical properties
Low CTE, low shrinkage, strong
Con◦ Higher MOE than microfill (possible
implications for “abfractions”
Less flexible
Uses◦ Suitable for class 1,2,3,4,5

Very smooth finish, excellent esthetics
Poor lab behavior, good clinical behavior
Higher coefficient of thermal expansion than hybrids
May show greater water sorption over time
MOE may actually improve performance in Class V’s (abfraction?)

Average particle size is 0.4 m
An attempt to have the “best of both worlds”
Layered, anatomical build-up advocated for maximum esthetics
Examples:
Point-4 (Kerr)
Esthet-X (Caulk)
Synergy (Coltene/Whaledent)
Apollo (DMD)
Vitalescence (Ultradent)
Renew (Bisco)

The concept: ◦ Higher resin content
◦ Less viscosity
◦ Better adaptation to cavity walls
◦ Shock absorption through gasket effect

Pro◦ Flow easily◦ Elastic modulus permits flex and flow which may
absorb stresses (Think class V)
Con◦ More resin, less filler and all the downsides◦ Questionable ability to withstand high stress and
wear◦ Flowability = runny, difficult to control
Bottom Line: Minimal data to support use in Class II boxes; Better margins, less leakage have not been demonstrated

Penetrates microcracks, irregularities
Seals tooth-restoration interface
Enhances longevity of restoration (Leinfelder)
Technique◦ Cure, etch accessible margins, dry
◦ Low viscosity bonding agent, cure
Fortify, Optiguard, Permaseal, Protect-it

Esthetics
It’s not amalgam ◦ environmental issues
◦ ”toxicity”
Non-conductive
Conservative preparation

Polymerization shrinkage
Marginal leakage
Secondary caries
Post-op sensitivity
Technique sensitivity
Wear resistance

All resin based composites shrink upon curing
Polymerization shrinkage places stress on enamel and dentin bonds
Resin shrinks towards the center of the mass of material, “pulling” on the walls as it shrinks
The configuration of the cavity preparation is important to consider

Competition between: polymerization contraction forces
strength of bonds to tooth
C = Total Bonded Area
Total Unbonded Area
higher C-Factor = more stress
A class 1 preparation has the highest C factor
C-FACTOR
C=2
C=1
C=1
C=2
C=5

Interproximal contacts difficult
Physical properties poorer than amalgam
Water sorption
Depth of cure?
Lack of foolproof DBA
Technique sensitive!

When esthetics critical Conservative prep
feasible◦ occlusal outline narrow◦ gingival margin in
enamel◦ centric stops on tooth
structure
No evidence of excessive occlusal wear

High caries risk
Extensive preparations
Heavy occlusal function
Lack of enamel
Subgingival extension
Isolation inadequate

Conservative, adhesive preparation◦ Rounded internal line angles
◦ Occlusal width 1/3 intercuspal distance
◦ Avoid centric stop
Proximal box◦ Retention grooves may be beneficial (Summitt, et al. Quint Int 1994; 25:251-257)
◦ Gingival margin in enamel if possible

• Pre-wedge• helps achieve contact
• protects RD and gingiva
• Conservative adhesive prep• rounded internal line angles
• occlusal width 1/3 ICD
• avoid centric stop
• Proximal box• retention grooves?

• No bevels on occlusal margins
• Bevel F & L of proximal box
• significantly reduces marginal leakage
• improves access to enamel rod ends
• improves access for finishing
• Bevel on gingival margin
• only if wide band of enamel present

Bevel
Round internal line angles
Do not extend/bevelFissureotomy
Limit preparation to only what you need for access to caries and undermined enamel

Don’t bevel occlusal
Consider bevel of F and L margins of boxes◦ improves access to enamel rod ends
◦ improves access for finishing
Bevel gingival wall only if abundant enamel

Metal bands acceptable◦ Should be thin (0.0010”) and pliable
◦ Burnish against contact
◦ Use with conventional tofflemire
Clear bands OK but:◦ Thicker, non-burnishable
◦ Strong memory
◦ High cost

Wooden wedges preferable◦ Slight compression holds gingival margin tightly
◦ Secure
◦ Inexpensive
Clear wedges (e.g. Premier Cure-Thru®)◦ No resiliency
◦ Quite expensive
◦ Enhancement of cure unproven
(Ciamponi, et al. Quint Int 1994; 25:599-601)

Difficult to establish contact◦ Composite is not condensable
◦ Some matrix systems aggravate situation
Proximal contours often not ideal
Finishing procedures can open contact
Wear can complicate matters◦ Results in flat surface

Pre-wedge, proper matrix
Careful interproximal finishing
Pre-polymerized pellet
Ceramic insert
Condensable/Packable Composites
Belvedere Composite Contact Former
Curing tip (Denbur)
Segmental Matrices with Bitine ring

Lack of enamel
Moisture control difficult
Bonding system manipulation challenging
Poor access◦ Curing “chancy”
◦ Finishing difficult
Longevity of bond to cementum suspect

Particularly indicated when no enamel at margin
RMGI fill apical to contact
Resin based composite coronal to contact
Decreased microleakage◦ Allows stress relaxation
◦ Decreases bulk of composite
◦ Predictable dentin bond
Burgess, et. al. Compend Cont Ed Dent 1996; 17: 731-748

Advantages◦ Chemical bond to dentin
◦ Chemical bond to resin
◦ Anticariogenic effects
◦ Volume reduction of resin
◦ Elastic bonding layer
Closed Sandwich
Open Sandwich

What are you placing in the box?
a. Packable composite
b. Flowable composite
c. Resin-Modified Glass
Ionomer
d. Compomer The only way to reduce the overall shrinkage is to use less composite
material…hence…the sandwich technique

Most Common Lights = Quartz Tungsten Halogen!
Light intensity = mW/cm2
Conventional curing = 400-500 mW/cm2.
◦ Note increase from standard 300mW /cm2 of 5 years ago
Why the interest?◦ Time savings
◦ High-tech bragging rites
◦ Wavelength—468nm

Think about meaning of numbers!◦ Light tip diameter should approximate diode
Barghi, et. al. J Dent Res 1995; (abstr 152)
Leonard, et. al. Oper Dent 1999; 1:31-37
◦ Large tip : diode overstates the output
◦ Demetron guidelines
> 300 is OK- 400-500 has become the standard
200 - 300 requires longer curing time (but OK)
< 200 a problem

New Curing Techniques◦ High intensity and Multi-mode curing
High intensity
Lasers
Plasma arc (PAC) lights
◦ Newer lights will offer multi-mode (variable intensity) curing
Designed to allow stress relief before final set

Don’t cure to the advertised depth (< 3mm)
Wavelengths too focused ◦ Photoinitiators in different materials may not be
sensitive in narrow range
Generate high internal polymerization forces
May form shorter polymer chains (thus poorer physical properties)
Expensive

Continuous vs Discontinuous
“Soft Start” (pulse delayed)◦ Short burst, delay, final cure
◦ Extends visco-elastic stage of resin curing
◦ Often used as generic term
◦ Specifically refers to discontinuous method
◦ No solid science to prove efficacy

Light Emitting Diode
No bulbs or filaments
Doesn’t heat up (as much)
More energy efficient
Longer life
First generation- much lower irradiance in milliwatts◦ <200 mW/cm2
◦ Poor performance
Versalux
Elipar Freelight

Second generation◦ 600 mW/cm2
◦ Very promising
Problem: some have narrow spectrum◦ Some materials won’t cure◦ Improving!◦ Some heat is still generated◦ More efficient than QTH◦ Spectrum may be more narrow
than QTH◦ LEDs undergo less degradation
than QTH LE Demetron
Ultraume

Enhances completeness of cure May actually increase stress in tooth◦ Versluis, et. al. J Dent Res 1996; 75: 871-
877
Potential for incorporation of voids Takes time Microleakage not significantly better,
regardless of filling technique◦ Hilton. Quintessence Int 1997; 28: 135-
144

Wibowo et al (1999) ◦ Studied seven techniques w/ incremental
placement of Class II composites
◦ NONE produced gingival margin free of marginal leakage
◦ Best outcome w/ RMGI in box (closed sandwich)
◦ Flowable comp & condensable had poor performance

50% sealant retention (single application) 10-15 years
Effective caries resistance even when majority sealant lost;
resin remains in deeper fissure

Most conservative of all
Most failures are from improper isolation/moisture contamination
If you seal over active caries the caries will most likely become bacteriologically inactive and the disease process stops.

Selected fossa well isolated from another fossa containing restoration
Incipient caries in pit & fissure confined to enamel
Occlusal caries on contralateral tooth

Carious lesions, diagnosed & undiagnosed at the base of the fissure are arrested by sealants (Mertz-Fairhurst, 1986; Handelman 1991)
Decision to use sealants on known carious lesions “is responsibility of the dentist”ADA Report on Sealants, JADA April 1997

Pit and fissure sealants in combination with small amalgam restorations
Non-coalesced pits and fissures around restoration sealed
Significantly improved marginal integrity

Carbide & Diamond Burs 1/16" Shank- Tiny dental burs for ...
... Friction Grip 1/16" Shank Carbide Burs- Price $3.60 each.
www.shorinternational.com/BurSuperCarbide.htm

Restore carious lesions with minimum of tooth removal
Prevent caries from attacking other pits and fissures

Advantages◦ Sustained fluoride
release/rechargeable
◦ Biocompatibility
◦ Adhesion to tooth structure
Ionic bonds to tooth mineral
◦ Coefficient of thermal expansion

Disadvantages◦ Short working time
◦ Long setting time
◦ Technique sensitive
◦ Brittleness
◦ Esthetics

Advantages◦ Combines benefits of glass ionomers and
composite resin
◦ Increased working time
◦ Improved physical properties
◦ Improved esthetics
◦ Immediate finishing
◦ Record of clinical success

Powder◦ Ion-leachable aluminafluorosilicate glass
Liquid◦ Water
◦ HEMA/Bis-GMA
◦ Polyacid (may contain photocurable side chains)
methacrylate groups grafted onto PAA molecule
◦ Photoinitiator
Net resin content is approximately 5%

Smear layer removal allows access to dentin surface
Softens surface to facilitate ion exchange
Energizes surface for better wetting
Rule of 200◦ Concentration x time = 200
25% PAA x 8 sec

Exposure to exogenous fluorides results in a transient rise in F- release (“recharge” phenomenon)◦ Wistrom, et al. J Dent Res 1995; 74: abstr 767◦ Hatibovic-Kofman. J Dent Res 1994; 73: abstr 260◦ Alvarez & Burgess. J Dent Res 1994; 73: abstr 259
Avoid acidic F formulations - may degrade surface◦ Burgess, 1996 ◦ Fluoride release greatest for GI, then RMGI,
compomer, least is with composite

Resin-based composites that contain GI components◦ Radiopaque alumino fluoro-silicate glass
◦ Acidic polymerizable monomers
◦ Light-curing polymers
Insufficient GI components for significant acid-base reaction◦ Won’t cure w/o light
Examples◦ Dyract AP, Compoglass F, Hytac,
F 2000

Subject to greater loading than anterior teeth
Endodontically treated posterior tooth should receive cuspal coverage
Posts indicated only when not enough remaining tooth structure or pulp chamber height to retain core

Carbamide peroxide◦ Initially 10% to 15%
◦ 10% C.P. 3.6% H2O2 + 6.4% Urea
◦ Higher concentrations now being marketed
Matrix ◦ Carbopol (B.F. Goodrich)
10% Carbamide peroxide with carbopol◦ Only concentration with ADA acceptance
◦ Longest track record

Action by oxygen free radical (oxidation reaction)◦ Organic molecules are broken down
to smaller, less-colored molecules
◦ Diffusion/penetration of tooth structure established
Alteration of the enamel◦ Changes light reflectance to cause an
apparent lightening

Aging-related discoloration
Mild to moderate tetracycline stains (variable success)
Fluorosis
Generalized mild to moderate staining
Pre/Post restorative (veneers, microabrasion)

Anterior teeth subjected to lateral forces
Routine use of post/core and crown not indicated
Post/core indicated if :◦ Insufficient remaining coronal dentin
◦ Tooth to be abutment for FPD or RPD

Severe staining of most types
Sensitive teeth (recession)
Smokers (relative)
Extensive restorative history
Unrealistic patient expectations
Known sensitivity to bleaching agent
Pregnant or nursing women

Tooth sensitivity
Soft tissue effects
Alteration of tooth structure?
Effect on restorative materials
Safety - Oxygen free radicals?

Bleaching frequently causes minor tooth discomfort
Sensitivity is transient Related to agent strength / exposure time Tooth sensitivity can be controlled by:◦ Reduction of exposure time/concentration◦ Fluoride treatment◦ Use of desensitizing agents◦ Desensitizing agents being added
by manufacturer

Most SEM studies of enamel surfaces show little or no change in morphology
Studies show no significant effects on physical properties of enamel
Salivary remineralization might reverse any physical changes that occur
Slight surface pitting with 50% H2O2 office bleach

Minimal to no effect on composite or porcelain
Change in color of composites insignificant
Increased release of mercury from amalgam,◦ 2 reports
Methacrylate temporary resins discolor orangish
Bis-acryl and polycarbonate not affected

Little to no gingival irritation with well fitting trays and use of rubber dam when indicated (In-office systems)
May irritate tissue at higher concentrations
Indices and gingival biopsies report no lasting effect
Some patients gingival health improves due to increased oral hygiene and oxygen tension

Depends on the type/degree of stain◦ Haywood advocates 4-6 months for severe TCN
cases
Should see lightening within 3-4 days Pt’s compliance before and after
treatment is key Effective 75 - 90% of selected cases◦ Depends on study
Longevity is reasonable, but variable◦ May require re-treatment periodically

35-50% Hydrogen Peroxide◦ Shofu HiLite
◦ Opalescence Xtra (Ultradent)
◦ Superoxol
35-40% Carbamide Peroxides◦ Accelerate (Den Mat)
Hydrogen Peroxide/Carbamide Peroxide Combos◦ White Speed (Discus Dental)

Long track record (a.k.a. “walking bleach”)
Must remove all composite from access
External cervical resorption concerns!◦ Adequate seal over RCT
◦ Consider saline/perborate vs superoxol/perborate
◦ Correlated with use of
Heat
High concentration bleaching agents

Chemo-mechanical removal of superficial enamel discoloration◦ 1986: Croll
18% HCL/Pumice mixture
Wooden applicator used for abrasion
◦ 1990: Croll
11% HCL/Abrasive paste
10:1 gear reduction handpiece/special mandrels
PREMA System

Indications
◦ Enamel fluorosis
Brown lesions, white, yellow
◦ Superficial enamel hypoplasia/hypocalcification
◦ Lesions less than 200 µ in depth
Most brown defects respond well
25-50% of white lesions are too deep
Contraindications
◦ Deep enamel lesions
◦ Tetracycline staining
◦ Dentinogenesisimperfecta
◦ Any discoloration of dentinal origin

Onlays
Desire 2.0 mm reduction over functional cusps
At least 1.5 mm over non-functional cusps
Desire bulk of ceramic at the margin
Rounded internal angles
Smooth walls2 mm
>2 mm

Tooth Reduction
Based on ceramic strength, not software designDimensions:
At least 2.0 mm in the central fossaAt least 2.0 mm in a F-L dimensionAt least 1.5 mm axially (box)
>2.0 mm
>1.5 mm

Preparation Guidelines
Smooth, sharp well-defined margins
Smooth divergent tapered walls (6o- 8
o)
Smoothly rounded internal angles
Exit angles and margins approaching 90o
Adequate tooth reduction
TaperedParallel Undercut


















