Restoration of divergent implants with a 2-piece screw-retained fixed… · 2016-05-04 · CLINICAL...
4
CLINICAL REPORT Restoration of divergent implants with a 2-piece screw-retained fixed, complete dental implant prostheses Stavros Pelekanos, DDS, Dr med dent, a Georgia Pozidi, DDS, b and Stefanos Kourtis, DDS, Dr med dent c Rehabilitating a completely edentulous maxilla with an implant-retained prosthesis is challenging. The resorptive pattern of the alveolar crest leads to hard and soft tissue defects that cannot always be addressed with augmentation procedures. 1-3 Deficiencies in the horizontal plane and a prosthetically unfavorable implant position may compromise esthetics, phonetics, and function. 1,4 Lip support is usually achieved with pink ceramic or acrylic resin. 2 An edentulous maxilla can be restored with an implant overdenture or a fixed implant prosthesis. 2,5 Maxillary implant overdentures are associated with more technical complications and biological problems than a fixed implant-supported prosthesis. A higher incidence of post- insertion maintenance (clip or attachment replacement/ reactivation) and mucosal inflammation has been re- ported. 1,4,6-8 Fixed implant-supported maxillary prosthe- ses give greater patient satisfaction and a lower incidence of prosthetic complication. 1,4 An implant-supported fixed prosthesis with metal superstructure and acrylic resin gingiva has been extensively used in the treatment of the edentulous mandible. 2,9 Although long-term survival rates are well documented, technical complications are pros- thetic screw loosening and/or fractures, abutment frac- tures, and fracture or wear of acrylic resin teeth. 2,9-11 Fabrication is more demanding in the maxilla. Large interabutment spaces can disrupt speech and oral hygiene under flange extensions and around abutments is diffi- cult. 2,10,11 Ease of oral hygiene and retrievability of the prosthesis during the maintenance phase are essential for long-term success. This report describes the clinical and laboratory stages in fabricating a 2-piece fixed screw- retained prosthesis on multiple divergent implants in a resorbed maxilla. CLINICAL REPORT A 40-year-old woman with high esthetic expectations wished to “have her teeth restored.” Clinical and radio- graphic evaluation showed a severely resorbed maxilla with 6 osseointegrated implants (Bego Semados S im- plants; Bego GmbH & Co) with no signs of pathology (Fig. 1). The patient had a fixed metal-reinforced tooth implant- and tissue-supported (“tripod”) interim pros- thesis in the maxilla. The maxillary left canine and implant corresponding to the right lateral incisor were used as abutments while 2 flanges extending on to the tuberosities provided additional support. 12 All im- plants were suboptimally placed, emerging bucally from the alveolar crest on divergent axes (Figs. 2, 3). Despite a poor prognosis, the left maxillary canine was used to support the interim restoration. Asymmetry in the levels of the periimplant mucosal margins and extensive bone resorption of the maxilla Supported by Greek State Scholarships Foundation grant 98138/B7/19-7-2013. The sponsors had no involvement in the collection, analysis and interpretation of data, or the writing of the report. a Assistant Professor, Department of Prosthodontics, Dental School, University of Athens, Athens, Greece. b Postgraduate student, Department of Prosthodontics, Dental School, University of Athens, Athens, Greece. c Associate Professor, Department of Prosthodontics, Dental School, University of Athens, Athens, Greece. ABSTRACT Restoring a severely resorbed maxilla is challenging because of poor bone quality and the resorptive pattern that follows tooth loss. When bone augmentation is not possible, implants are placed in suboptimal positions, making the prosthetic rehabilitation more complex. This report presents the steps used to rehabilitate a severely resorbed maxilla with divergent implants, using an implant-supported 2-piece screw-retained prosthesis. (J Prosthet Dent 2016;115:389-392) THE JOURNAL OF PROSTHETIC DENTISTRY 389
Transcript of Restoration of divergent implants with a 2-piece screw-retained fixed… · 2016-05-04 · CLINICAL...

CLINICAL REPORT
Supported byinterpretationaAssistant PrbPostgraduatcAssociate Pr
THE JOURNA
Restoration of divergent implants with a 2-piecescrew-retained fixed, complete dental implant prostheses
Stavros Pelekanos, DDS, Dr med dent,a Georgia Pozidi, DDS,b and Stefanos Kourtis, DDS, Dr med dentc
ABSTRACTRestoring a severely resorbed maxilla is challenging because of poor bone quality and theresorptive pattern that follows tooth loss. When bone augmentation is not possible, implants areplaced in suboptimal positions, making the prosthetic rehabilitation more complex. This reportpresents the steps used to rehabilitate a severely resorbed maxilla with divergent implants, using animplant-supported 2-piece screw-retained prosthesis. (J Prosthet Dent 2016;115:389-392)
Rehabilitating a completelyedentulous maxilla with animplant-retained prosthesis ischallenging. The resorptivepattern of the alveolar crestleads to hard and soft tissuedefects that cannot always be
addressed with augmentation procedures.1-3 Deficienciesin the horizontal plane and a prosthetically unfavorableimplant position may compromise esthetics, phonetics,and function.1,4 Lip support is usually achieved with pinkceramic or acrylic resin.2An edentulous maxilla can be restored with an implantoverdenture or a fixed implant prosthesis.2,5 Maxillaryimplant overdentures are associated with more technicalcomplications and biological problems than a fixedimplant-supported prosthesis. A higher incidence of post-insertion maintenance (clip or attachment replacement/reactivation) and mucosal inflammation has been re-ported.1,4,6-8 Fixed implant-supported maxillary prosthe-ses give greater patient satisfaction and a lower incidenceof prosthetic complication.1,4 An implant-supported fixedprosthesis with metal superstructure and acrylic resingingiva has been extensively used in the treatment of theedentulousmandible.2,9 Although long-term survival ratesare well documented, technical complications are pros-thetic screw loosening and/or fractures, abutment frac-tures, and fracture or wear of acrylic resin teeth.2,9-11
Fabrication is more demanding in the maxilla. Largeinterabutment spaces can disrupt speech and oral hygieneunder flange extensions and around abutments is diffi-cult.2,10,11 Ease of oral hygiene and retrievability of the
Greek State Scholarships Foundation grant 98138/B7/19-7-2013. The spof data, or the writing of the report.
ofessor, Department of Prosthodontics, Dental School, University of Athense student, Department of Prosthodontics, Dental School, University of Atheofessor, Department of Prosthodontics, Dental School, University of Athen
L OF PROSTHETIC DENTISTRY
prosthesis during the maintenance phase are essential forlong-term success. This report describes the clinical andlaboratory stages in fabricating a 2-piece fixed screw-retained prosthesis on multiple divergent implants in aresorbed maxilla.
CLINICAL REPORT
A 40-year-old woman with high esthetic expectationswished to “have her teeth restored.” Clinical and radio-graphic evaluation showed a severely resorbed maxillawith 6 osseointegrated implants (Bego Semados S im-plants; Bego GmbH & Co) with no signs of pathology(Fig. 1). The patient had a fixed metal-reinforced toothimplant- and tissue-supported (“tripod”) interim pros-thesis in the maxilla. The maxillary left canine andimplant corresponding to the right lateral incisor wereused as abutments while 2 flanges extending on tothe tuberosities provided additional support.12 All im-plants were suboptimally placed, emerging bucally fromthe alveolar crest on divergent axes (Figs. 2, 3). Despite apoor prognosis, the left maxillary canine was used tosupport the interim restoration.
Asymmetry in the levels of the periimplant mucosalmargins and extensive bone resorption of the maxilla
onsors had no involvement in the collection, analysis and
, Athens, Greece.ns, Athens, Greece.s, Athens, Greece.
389

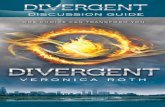
Figure 1. Panoramic radiograph obtained prior to prosthetic treatment. Figure 2. Initial clinical situation. Implant corresponding to right lateralincisor with labial inclination.
Figure 3. Definitive cast mounted on semiadjustable articulator incentric relation. Waxing sleeves indicate implant divergent axes andbuccal inclination.
Figure 4. Artificial tooth arrangement. Teeth aligned and gingivaexposed harmoniously according to esthetic principles.
390 Volume 115 Issue 4
in combination with the amount of mucosa seen onsmiling required the use of artificial gingiva (Fig. 2). Adiagnostic artificial tooth arrangement was set up (SRVivodent; Ivoclar Vivadent AG). A clinical evaluationverified the correct position and alignment of the teeth,centric relation, vertical dimension, mandibular move-ments, and pink and white esthetics (Fig. 4).
The prosthesis needed to compensate for the de-ficiencies in both the hard and soft tissues. The prosthesiswas screw-retained because of the patient’s esthetic de-mands. At the time of treatment, prefabricated, angledabutments for screw type prostheses (Sub-tech Multiplusabutments; Bego GmbH & Co) were not available. Tocompensate for the implants’ divergent axes, a 2-pieceprosthesis was fabricated.13,14 It consisted of a cast metalCo-Cr substructure (Dentaurum GmbH & Co) attached tothe implants with abutment screws. The substructure wasdesigned to retain individual metal ceramic crowns toreplace the maxillary teeth. All individual crowns werecemented, with the exception of the left and right firstmolars, right canine, right lateral incisor, and left first
THE JOURNAL OF PROSTHETIC DENTISTRY
premolar. In order to ensure retrievability, these 5 crownswere retained with friction splints (Friction Splint FS1;Bredent GmbH & Co) (Figs. 5-7). The neck of the implantcorresponding to the right lateral incisor was higher thanthat of the other implants, so this individual crown wascemented (Figs. 2, 5). This design allowed adequate lipsupport without increasing structural bulk.
An acrylic resin replica of the diagnostic waxing wasfabricated on the definitive cast, which was then cut backwith standard chamfer preparations (Fig. 5). The waxing,casting, and ceramic layering (IPS d.SIGN; Ivoclar Viva-dent AG) of the crowns followed a standard protocol(Figs. 6, 7).
A clinical evaluation of the prosthesis verified passivefit and accessibility for oral hygiene (Fig. 8). The naturalgingival contour and lip support of the definitive treat-ment (Figs. 9, 10) fulfilled the patient’s esthetic criteria.Figure 11 shows the anterior guidance during all eccentricmovements (video, available online). After insertion ofthe definitive prosthesis, the patient was scheduled for a4-monthly recall.
Pelekanos et al

Figure 5. Acrylic resin replica with 4 friction splints in place. Figure 6. Laboratory evaluation of framework passive fit.
Figure 7. Definitive restoration prior to insertion. Figure 8. Definitive restoration allowed use of interdental brushes.
Figure 9. Panoramic radiograph after treatment.
April 2016 391
DISCUSSION
The patient’s high esthetic demands necessitated a fixedprosthesis despite the need for extensive lip supportdue to bone resorption. Apart from the promising successrates of fixed prostheses, the present screw-retentiondesign offers the advantage of precluding the useof cement and therefore minimizes the risk of peri-implantitis due to residual cement.15-17 In addition,while technically demanding, fabricating the prosthesisin 2 pieces meant that the primary structure, whichhad an increased volume of metal, was not exposed toany further thermal procedures after casting and thepolymer materials could be modified.10,18 Individualteeth could be characterized independently of thematerial replicating the soft tissues.
A possible drawback is that the pink resin gingiva thatcompensated for the resorption covers the labial part ofthe residual ridge, therefore necessitating meticulous oralhygiene. The use of friction splints ensures easy access tothe fixation screws. Thus, during follow-up the pros-thodontist could easily remove the prosthesis. Ease ofrepair was also ensured. In case of complications, the
Pelekanos et al
individual crowns could be removed without disturbingthe other components.13 Another possibility would bethe use of angled abutments for screw-retained pros-theses used to redirect screw access in situations withprosthetically unfavorable implant angulations.19 At thetime of treatment, however, these were not yet available.
THE JOURNAL OF PROSTHETIC DENTISTRY

Figure 11. Anterior guidance during eccentric movements.
Figure 10. Esthetic result.
392 Volume 115 Issue 4
The fabrication of the primary structure usingcomputer-aided design and computer-aided manufac-turing (CAD/CAM) techniques might improve the fit.10,13
Those techniques may be limited by a variety of factors,including the implant company, the type of CAD/CAMsystem, the implant-abutment connection, and theimplant angulation. At the time of treatment however, theavailable systems could not accommodate the angulationof the implants.
Rehabilitating the resorbed maxilla with 2-piecereconstructions has been reported.13,14 It is a technicallydemanding approach associated with higher costand complicated laboratory procedures.20 It does, how-ever, offer a clinical solution where an implant-supportedfixed prosthesis is indicated for a patient with a resorbedmaxilla and high esthetic demands.
SUMMARY
A 2-piece, screw-retained implant-supported prosthesiswas fabricated to restore 6 divergent implants on a resorbedmaxilla. A primary castmetal frameworkmimicking the softtissues was fitted to the implants with screw retention. The
THE JOURNAL OF PROSTHETIC DENTISTRY
secondary prosthesis consisted of independent metalceramic crownsfitted to the implant-supported framework.The prosthesis satisfied the patient’s esthetic demands. Theuse of pink acrylic resin corrected the asymmetrical gingivalmargin and provided adequate lip support withoutimpeding speech or oral hygiene. Retrievability and ease ofrepair were also addressed.
REFERENCES
1. Att W, Bernhart J, Strub JR. Fixed rehabilitation of the edentulous maxilla:Possibilities and clinical outcome. J Oral Maxillofac Surg 2009;67:60-73.
2. Sadowski S. The implant-supported prosthesis for the edentulous arch:Design considerations. J Prosthet Dent 1997;78:28-33.
3. Zitzmann NU, Marinello CP. Treatment plan for restoring the edentulousmaxilla with implant supported restorations: removable overdenture versusfixed partial denture design. J Prosthet Dent 1999;82:188-96.
4. Sadowski S. Treatment considerations for maxillary implant overdentures: Asystematic review. J Prosthet Dent 2007;97:340-8.
5. Henry P. A review of guidelines for implant rehabilitation of the edentulousmaxilla. J Prosthet Dent 2002;87:281-8.
6. Andriotelli M, Att W, Strub JR. Prosthodontic complications with implantoverdentures: A systematic literature review. Int J Prosthodont 2010;23:195-203.
7. Zitzmann NU, Marinello CP. Treatment outcomes of fixed or removableimplant-supported prostheses in the edentulous maxilla. Part II: clinicalfindings. J Prosthet Dent 2000;83:434-42.
8. Kiener P, Oetterli M, Mericske E, Mericske-Stern R. Effectiveness of maxillaryoverdentures supported by implants: maintenance and prosthetic complica-tions. Int J Prosthodont 2001;14:133-40.
9. Jemt T, Johansson J. Implant treatment in the edentulous maxillae: a 15-yearfollow-up study on 76 consecutive patients provided with fixed prostheses.Clin Implant Dent Relat Res 2006;8:61-9.
10. Drago C, Howell K. Concepts for designing and fabrication metal implantframeworks for hybrid implant prostheses. J Prosthodont 2012;21:413-24.
11. Jemt T. Fixed implant-supported prostheses in the edentulous maxilla. A five-year follow-up report. Clin Oral Implants Res 1994;5:142-7.
12. Chronopoulos V, Kourtis S, Katsikeris N, Nagy W. Tooth- and tissue-supported provisional restorations for the treatment of patients withextended edentulous spans. J Esthet Restor Dent 2009;21:7-17.
13. Chronaios D, Spyropoulou P, Razoog M, Sieraalta M. Material options forrestoring intentionally misaligned implants on maxillary edentulous arch: Aclinical report. J Prosthet Dent 2013;109:145-8.
14. Tsoutis K, Katsikeris N, Chronopoulos V, Kourtis S. Rehabilitation of theedentulous maxilla with autogenous bone grafts from the iliac crest andimplant-supported combined fixed restorations. A challenging task. EDIJournal 2011;7:66-72.
15. Sailer I, Mulhemann S, Zwalen M, Hammerle CH, Schneider D. Cementedand screw-retained implant reconstructions: a systematic review of the sur-vival and complication rates. Clin Oral Implants Res 2012;23:163-201.
16. Agar J, Cameron S, Hughbankc J, Parker H. Cement removal from restora-tions luted to titanium abutments with simulated subgingival margins.J Prosthet Dent 1997;78:43-7.
17. Wilson T. The positive relationship between excess cement and peri-implantdisease: a prospective clinical endoscopic study. J Periodontol 2009;80:1388-92.
18. Coachman C, Salama M, Graber D, Calamita M, Salama H, Cabral G.Prosthetic gingival reconstruction in fixed partial restorations. Part 3: Labo-ratory procedures and maintenance. Int J Periodontics Restorative Dent2010;30:19-29.
19. Berroeta E, Zabalequi I, Donovan T, Chee W. Dynamic abutment: A methodfor redirecting screw access for implant-supported restorations: Technicaldetails and a clinical report. J Prosthet Dent 2015;113:516-9.
20. Zitzmann NU, Marinello CP. Treatment outcomes of fixed or removableimplant-supported prostheses in the edentulous maxilla. Part I: patients’assessments. J Prosthet Dent 2000;83:424.
Corresponding author:Dr Stavros Pelekanos163B El. Venizelou (Thiseos) AvKallithea AthensGREECEEmail: [email protected]
AcknowledgmentsThe authors thank the laboratory practice of Mr M. Papastamos for fabricating thedefinitive restoration.
Copyright © 2016 by the Editorial Council for The Journal of Prosthetic Dentistry.
Pelekanos et al