Restenosis After Drug-Eluting Stent ...eluting stent implantation in the left anterior descending...
2
IMAGES IN INTERVENTION Restenosis After Drug-Eluting Stent Implantation in a Patient With Polycythemia Vera Optical Coherence Tomography and Pathological Findings Akiko Fujino, MD,* Hiroyuki Hao, MD,* Noriko Kajimoto, MD,* Rika Kawakami, MD,* Takahiro Imanaka, MD,y Kenichi Fujii, MD,y Takashi Abe, MD,z Masaharu Ishihara, MD,y Seiichi Hirota, MD* A n 83-year-old woman was referred to our hospital due to diverticular bleeding of the colon. She had a history of everolimus- eluting stent implantation in the left anterior descending artery (31 months before) and the right coronary artery (20 and 31 months before) because of stable angina. She was prescribed aspirin 100 mg/day and clopidogrel 75 mg/day, followed by sin- gle antiplatelet therapy by aspirin during the last 8 months. Aspirin was discontinued for the endo- scopic therapy at her admission. Complete blood count showed hemoglobin of 17.5 g/dl and hemato- crit of 55.2%, from which polycythemia vera (PV) was suspected. Three days after admission, she died of sudden cardiac arrest. Autopsy revealed the cause of her death to be pulmonary thromboembo- lism. PV was confirmed by bone marrow examina- tion. Ex vivo optical coherence tomography (St. Jude Medical, St. Paul, Minnesota) and pathol- ogy of coronary arteries were examined. Optical coherence tomography illustrated neointima with high-intensity signal and irregular luminal sur- face (Figure 1A). A signal-rich, slit-like structure (Figure 1B) with microchannels (Figure 1C) suggested thrombus formation. Corresponding histology re- vealed neointima composed of granulation tissue (Figures 1D and 1G). Organized fibrin thrombi (Figures 1E and 1H) and capillaries (Figures 1F and 1I) were also identified. Increased hematocrit levels and vascular inflam- mation are the intrinsic risks of thrombosis in the PV patient (1–3). The current case presented in-stent restenosis with extensive inflammation, which might be associated with PV. The strategy for coro- nary intervention in PV patients should be deliberate due to their high thrombogenic risk. REPRINT REQUESTS AND CORRESPONDENCE: Dr. Hiroyuki Hao, Department of Surgical Pathology, Hyogo College of Medicine, 1-1, Mukogawa-cho, Nishinomiya, Hyogo 663-8501, Japan. E-mail: [email protected]. From the *Department of Surgical Pathology, Hyogo College of Medicine, Nishinomiya, Hyogo, Japan; yDivision of Coronary Heart Disease, Department of Internal Medicine, Hyogo College of Medicine, Nishinomiya, Hyogo, Japan; and the zDepartment of Gastroenterology, Takarazuka Municipal Hospital, Takarazuka, Hyogo, Japan. The authors have reported that they have no relationships relevant to the contents of this paper to disclose. JACC: CARDIOVASCULAR INTERVENTIONS VOL. 8, NO. 7, 2015 ª 2015 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2015.01.030
Transcript of Restenosis After Drug-Eluting Stent ...eluting stent implantation in the left anterior descending...

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S VO L . 8 , N O . 7 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 5 . 0 1 . 0 3 0
IMAGES IN INTERVENTION
Restenosis After Drug-Eluting StentImplantation in a Patient WithPolycythemia VeraOptical Coherence Tomography and Pathological Findings
Akiko Fujino, MD,* Hiroyuki Hao, MD,* Noriko Kajimoto, MD,* Rika Kawakami, MD,* Takahiro Imanaka, MD,yKenichi Fujii, MD,y Takashi Abe, MD,z Masaharu Ishihara, MD,y Seiichi Hirota, MD*
A n 83-year-old woman was referred to ourhospital due to diverticular bleeding ofthe colon. She had a history of everolimus-
eluting stent implantation in the left anteriordescending artery (31 months before) and the rightcoronary artery (20 and 31 months before) becauseof stable angina. She was prescribed aspirin 100mg/day and clopidogrel 75 mg/day, followed by sin-gle antiplatelet therapy by aspirin during the last 8months. Aspirin was discontinued for the endo-scopic therapy at her admission. Complete bloodcount showed hemoglobin of 17.5 g/dl and hemato-crit of 55.2%, from which polycythemia vera (PV)was suspected. Three days after admission, shedied of sudden cardiac arrest. Autopsy revealed thecause of her death to be pulmonary thromboembo-lism. PV was confirmed by bone marrow examina-tion. Ex vivo optical coherence tomography (St.Jude Medical, St. Paul, Minnesota) and pathol-ogy of coronary arteries were examined. Opticalcoherence tomography illustrated neointima with
From the *Department of Surgical Pathology, Hyogo College of Medicine, Nis
Disease, Department of Internal Medicine, Hyogo College of Medicine, Ni
Gastroenterology, Takarazuka Municipal Hospital, Takarazuka, Hyogo, Jap
relationships relevant to the contents of this paper to disclose.
high-intensity signal and irregular luminal sur-face (Figure 1A). A signal-rich, slit-like structure(Figure 1B) with microchannels (Figure 1C) suggestedthrombus formation. Corresponding histology re-vealed neointima composed of granulation tissue(Figures 1D and 1G). Organized fibrin thrombi(Figures 1E and 1H) and capillaries (Figures 1Fand 1I) were also identified.
Increased hematocrit levels and vascular inflam-mation are the intrinsic risks of thrombosis in the PVpatient (1–3). The current case presented in-stentrestenosis with extensive inflammation, whichmight be associated with PV. The strategy for coro-nary intervention in PV patients should be deliberatedue to their high thrombogenic risk.
REPRINT REQUESTS AND CORRESPONDENCE:
Dr. Hiroyuki Hao, Department of Surgical Pathology,Hyogo College of Medicine, 1-1, Mukogawa-cho,Nishinomiya, Hyogo 663-8501, Japan. E-mail:[email protected].
hinomiya, Hyogo, Japan; yDivision of Coronary Heart
shinomiya, Hyogo, Japan; and the zDepartment of
an. The authors have reported that they have no

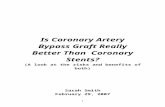
FIGURE 1 Ex Vivo Optical Coherence Tomography and Histopathology of In-Stent Restenosis in the Patient With Polycythemia Vera
Optical coherence tomography (OCT) indicated in-stent restenosis with high-intensity signal and irregular luminal surface (A). A signal-rich,
slit-like structure with luminal narrowing (B) and heterogeneous neointima with microchannels (C) were also identified. Corresponding his-
topathology showed neointima composed of granulation tissue (D and G). Bridging organized fibrin thrombi (E and H), and multiple capillary
formation in the neointima (F and I) were also identified. (A to C) Arrows indicate stent struts. (D to F) Masson’s trichrome: scale bar ¼ 1 mm.
(G to I) Masson’s trichrome, high-magnification view of the boxed areas in panels D to F, respectively.
Fujino et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 7 , 2 0 1 5
In-Stent Restenosis in Polycythemia Vera J U N E 2 0 1 5 : e 1 1 1 – 2
e112
RE F E RENCE S
1. Elliott MA, Tefferi A. Thrombosis and haemor-rhage in polycythaemia vera and essential throm-bocythaemia. Br J Haematol 2005;128:275–90.
2. Barbui T, Carobbio A, Finazzi G, et al. Inflam-mation and thrombosis in essential thrombocy-themia and polycythemia vera: different role of
C-reactive protein and pentraxin 3. Haematologica2011;96:315–8.
3. Michiels JJ. Platelet-mediated microvascularinflammation and thrombosis in thrombocy-themia vera: a distinct aspirin-responsive arterialthrombophilia, which transforms into a bleeding
diathesis at increasing platelet counts. Pathol Biol(Paris) 2003;51:167–75.
KEY WORDS drug-eluting stent, in-stentrestenosis, optical coherence tomography,pathology, polycythemia vera