RESPONSIBLE OPIATE PRESCRIBING - MCW … · Demonstrate appropriate use of prescription data...
50
RESPONSIBLE OPIATE PRESCRIBING CRESTA JONES MD
Transcript of RESPONSIBLE OPIATE PRESCRIBING - MCW … · Demonstrate appropriate use of prescription data...

RESPONSIBLE OPIATE PRESCRIBINGCRESTA JONES MD

DISCLOSURES
No conflicts to report

OBJECTIVES
Understand the scope and extent of the opiate abuse crisis in the United States
Demonstrate appropriate opiate prescribing for both acute and chronic pain
Demonstrate appropriate use of prescription data monitoring programs (PDMPs), including as they apply to Wisconsin state law

THE OPIOID EPIDEMIC : US stats
Opioid overuse/abuse is an epidemicOpioids – leading cause of injury death Continuing to increase
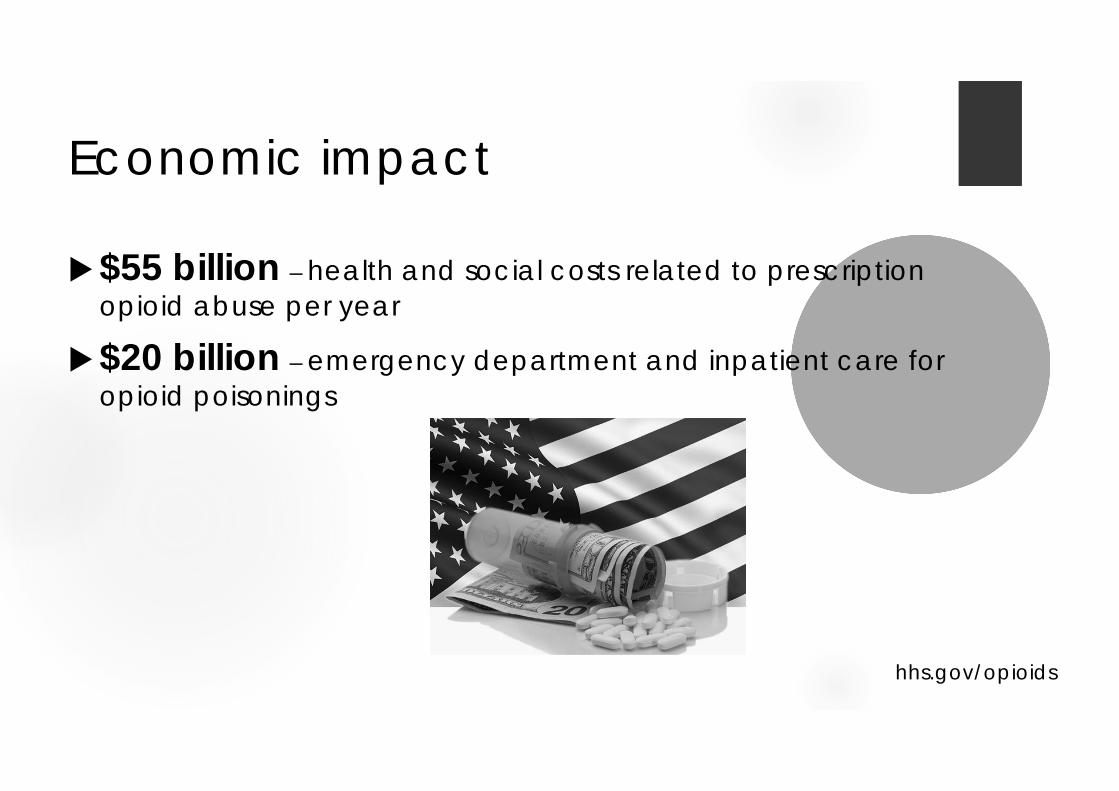
Economic impact
$55 billion – health and social costs related to prescription opioid abuse per year
$20 billion – emergency department and inpatient care for opioid poisonings
hhs.gov/opioids

Just another day in the US….....
650,000 opioid prescriptions dispensed3900 people initiate nonmedical use
prescription opioids580 people initiate heroin use
hhs.gov/opioids

cdc.gov

cdc.gov

cdc.gov

THE OPIOID EPIDEMIC : WI
163,000 opiate use disorder Leading cause of injury deaths in Wisconsin
Motor vehicle accidents, suicide, firearms Prescription opioids – more overdose deaths
than heroin + cocaine
dhs.wisconsin.gov/publications/p01129.pdf

dhs.wisconsin.gov
Who uses opiates?
JAMA Psychiatry 2014

They started with a prescription….

…..and they are women.

HOW DID THIS HAPPEN?
Increased prescriptions

HOW DID THIS HAPPEN?
Increased prescriptions
1991: 76 million RX

HOW DID THIS HAPPEN?
Increased prescriptions
1991: 76 million RX 2014:

HOW DID THIS HAPPEN?
Increased prescriptions
1991: 76 million RX 2014, 240 million RX =
Every US adult - 5 mg hydrocodone every 6 hours for 45 days
hhs.gov/opioids

Opiate use disorder – United States
5% of the world population…..
…...80% of the world’s opiates!
www.samhsa.gov, March 2015

HOW DID THIS HAPPEN?
Increased social acceptability for use

HOW DID THIS HAPPEN?
Increased acceptability for use History – acute and cancer pain only 1996 – extended release for non – cancer pain
Oxycontin - ER “non addictive” Based on 1 year addiction rates 1%Postoperative IV narcotics


HOW DID THIS HAPPEN?
Aggressive marketing by pharmaceutical companies

SINCE 1999, OPIOID PRESCIPTIONS HAVE QUADRUPLED….
BUT REPORTED PAIN REMAINS UNCHANGED!
McNett, M – Wisconsin Medical Society

OPIATE PRESCRIBING GUIDELINES
www.wisconsinmedicalsociety.org
www.cdc.gov
www.dsps.wi.gov
www.painphysicianjournal.com

OPIATE PRESCRIBING GUIDELINES
www.dsps.wi.gov

OPIATE PRESCRIBING GUIDELINES Address acute and chronic pain Chronic – longer than 3 months, past expected
tissue healing Not for active cancer treatment, end-of-life,
palliative care Not designed for pediatric pain
www.dsps.wi.gov

1. EVALUATING PAIN
Pain is subjective Patient reported measures We must accept the patient’s report of pain….
Commensurate with causative factors? Factors adequately evaluated?Already addressed with non-opioid therapy?

2. TREATMENT OF ACUTE PAIN
Consider non-opioid first Opioid – START LOW AND GO SLOW!
Most less than 3 days (MAX: 5 days) CDC = 7 days
Consider med you can refill (APAP/codeine)Consider 2 small Rx, specific refill dates

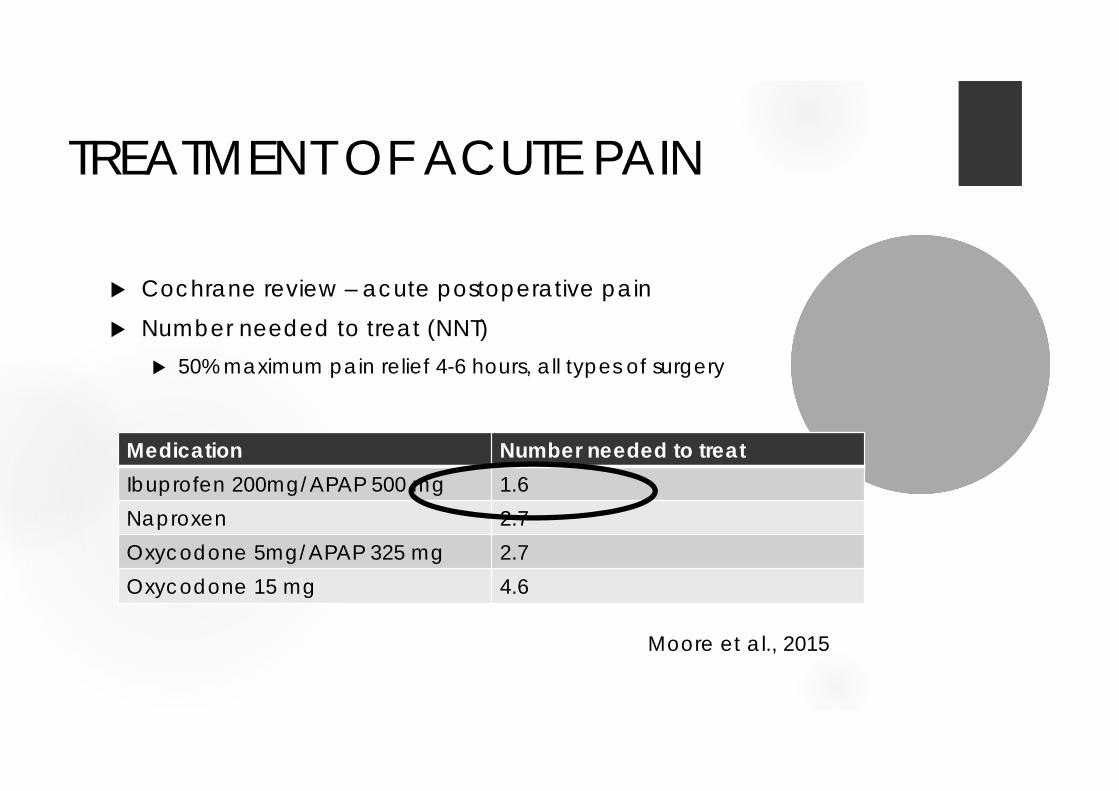
TREATMENT OF ACUTE PAIN
Cochrane review – acute postoperative pain Number needed to treat (NNT)
50% maximum pain relief 4-6 hours, all types of surgery
Medication Number needed to treatIbuprofen 200mg/APAP 500 mg 1.6Naproxen 2.7Oxycodone 5mg/APAP 325 mg 2.7Oxycodone 15 mg 4.6
Moore et al., 2015
TREATMENT OF ACUTE PAIN
Cochrane review – acute postoperative pain Number needed to treat (NNT)
50% maximum pain relief 4-6 hours, all types of surgery
Medication Number needed to treatIbuprofen 200mg/APAP 500 mg 1.6Naproxen 2.7Oxycodone 5mg/APAP 325 mg 2.7Oxycodone 15 mg 4.6
Moore et al., 2015

Hill MV, et al, 2017 642 outpatient surgical procedures Partial mastectomies, laparoscopic cholecystectomy,
laparoscopic/open inguinal hernia repair Opiate naive patients
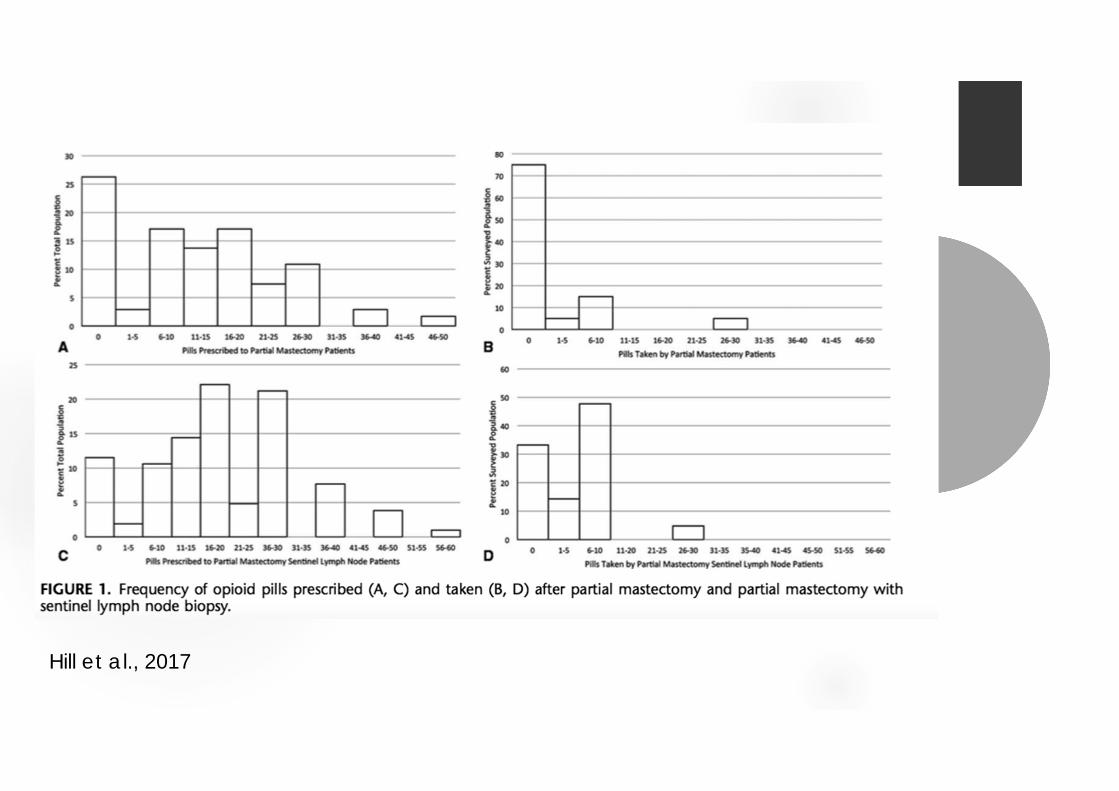
Hill et al., 2017

Hill et al., 2017

Hill et al., 2017

Hill et al., 2017

71% of opioid pills prescribed were NOT taken!!
Hill et al., 2017

What to do with all those extra meds?
Fire safe storage DEA National Drug Take-Back Days – April 29,
2017 Sealable plastic bag with water + dirt, cat
litter, coffee grounds Away from children Out of home for open house, social events
etc.
fda.gov

3. IDENTIFY AND TREAT THE CAUSE OF PAIN
Address the underlying condition as the primary objective
Avoid opiates if unwilling to obtain definitive treatment for condition causing pain
Avoid if medical condition present is not reasonably expected to cause pain severe enough for opioids Non-anatomic pain, residual pain at old surgical sites
Refer patient if needed

4. OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : ACUTE PAIN
Evidence for opioids is weak Try first
Acetaminophen/NSAIDs Lidocaine gel, biofreeze PT/OT Manipulation, massage Cognitive behavioral therapy
If severe enough for opioids, ALWAYS use in combination with other treatments
OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : ACUTE EXTENDED PAIN
Look for complications of acute pain: Surgical complication Nonunion of fracture Constipation as side effect of treatment
Complication ruled out, transition to non-opioid treatment

OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : ACUTE EXTENDED PAIN
Weaning opioids for acute extended pain (more than one week)
Decrease 10-25% per week Non-narcotics for acute pain treatment Start treatment for chronic pain – refer if indicated

OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : CHRONIC PAIN
Past expected healing >3 months Studies– few benefits, substantial increase mortality
72% INCREASE IN CARDIOVASCULAR MORTALITY No quality evidence to support use > 6 months Already initiated
Close monitoring, PDMP Refer for additional treatment Contract – no early fills, no other fills, urine drug screen

Patient obligations : opiate prescribing
I will not increase my dose or use without permission. I will not obtain opioids from other prescribers, or allow them to
adjust my dose. I will use the medication exactly as directed. I will never share, sell or allow others access to my medication. I will not receive early refills. I will not abuse other drugs or alcohol during my treatment. I will bring my pills and medication bottles to each appointment.
Patient obligations: opiate prescribing
I will call the office at least 2 business days before I need a refill. If I miss my appointment, I may not get a refill. I will not call for opioids during evenings, holidays or weekends. I will only use one pharmacy for my opioid prescriptions. I will give a urine drug screen anytime I am asked. I will notify the office as soon as possible of any new medical
condition. I will not drive or use heavy machinery while taking opioids. I will follow up as requested. I agree to allow my provider to contact all my other caregivers as
needed.

wisconsinmedicalsociety.org, Opiate CME programming

OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : UNWILLING PATIENT
Patient unwilling to accept other treatments Questionable justification for non – use “nothing else works” Intolerance to all other treatments

5. UTILIZE A SINGLE PROVIDER
Dedicated provider – primary care, pain specialist Check PDMP before start Ask about existing pain contracts Plan - acute pain outside office hours
Call immediately next office day Have ED contact primary prescriber
No early refills Fire safe

6. EXACERBATIONS OF CHRONIC PAIN
Avoid chronic pain treatment in the emergency dept.
Contact chronic pain doctor Avoid IV/IM opiates – preferred agent
hydromorphone Refer back to primary provider