Respiratory therapy in Covid-19 I can see clearly now…
49
Respiratory therapy in Covid-19 I can see clearly now… Leo Heunks, pulmonologist - intensivist Dept. Intensive Care, Amsterdam UMC
Transcript of Respiratory therapy in Covid-19 I can see clearly now…

Respiratory therapy in Covid-19
I can see clearly now…
Leo Heunks, pulmonologist - intensivist
Dept. Intensive Care, Amsterdam UMC

Disclosures
• Liberate Medical: Research grant paid to institution
• Getinge, Liberate Medical: Speakers fee
• Zonmw: research grants
• ERS: research grant for WEAN SAFE network

Question 1
Awake prone positioning improves gas exchange and risk of ETI in CoVID-19
A. Gas exchange Yes; ETI No
B. Gas exchange Yes; ETI Yes
C. Gas exchange No; ETI Yes
D. Gas exchange No; ETI No

Question 2
CoVID-19 ARDS is different from classical ARDS (mechanics, gas exchange).
A. Yes
B. No

Question 3
In early CoVID-19 ARDS PEEP should be set lower than in classical ARDS
A. Yes
B. No

Topics Covid-ARDS (CARDS)
• Pathophysiology CARDS
• Role for HFNT ?
• Role for awake proning ?
• Novel insights invasive ventilation

Am J Respir Crit Care Med, March, 2020, ePub
N=16
“Give minimal PEEP”

NVIC Webinar 7 apr 2020

COVID pulmonary phenotypes
Low elastance
Low lung weight
Low V/Q
Low recruitability
“L-type”
High elastance
High lung weight
High R-L shunt
High recruitability
“H-type”
spontaneous evolution P-SILI
Loss hypoxic pulm. vasoc.
Gattinoni, Int Care Med, online Apr 14, 2020

• Prospective observational study, Italy
• Covid-ARDS, N=301
• Measurements in first 24h, VCV, paralysed

N=301 N=2643

Compliance and lung weight
Crs ±similar when corrected for BMI, sex and ARDS cause
41 ml/cmH2O
32 ml/cmH2O

Only 5.5% of Covid-ARDS have Crs > 95th percentile of classic ARDS

Respiratory physiology
N=30/group
ARDS
P/F ±125mmHg
<24 h ETI
0
5
10
15
20
25
Pplat,cmH2O
2021
Haudebourg, Am J Respir Crit Care Med, 2020
0
5
10
15
20
25
DP,cmH2O
910
0
5
10
15
20
25
PEEP,cmH2O
810
Covid Non-Covid
NS NS NS

Respiratory physiology (P,eso)
N=30/group
ARDS
P/F ±125mmHg
<24 h ETI
0
3
6
9
12
15
P,L EI,cmH2O
1414
Haudebourg, Am J Respir Crit Care Med, 2020
0
20
40
60
80
100
C,lung ml/cmH2O
5759
0
3
6
9
12
15
P,L EE,cmH2O
02
Covid Non-Covid
NS NS

Interim conclusion physiology CARDS
1. Respiratory mechanics / gas exchange ± classical ARDS
2. Subgroup with disproportionate hypoxemia due to shunt
3. Extensive endothelial damage: pulmonary thrombosis

High Flow Nasal Therapy
Frat, NEJM, 2015

• N=34,
• O2 > 5 L/min;
• Pa,o2 / Fi,o2 124 mmHg before HFNT
• Mean duration HFNT 6 days
%
0
20
40
60
80
100
1515
70
Weaned
Continued
Dead
Guy, Eur Respir J, 2020

• PPE:
• FFP2, waterproof gowns, gloves, overshoes, eye and head protection
• Patient surgical mask when HCW entering room
• Of 44 HCW, 1 infected most likely social contact
Guy, Eur Respir J, 2020

• N=28, Sp,o2 <92% with NRM
• Resp rate 26 (12-40) / min
• Pa,o2 57 mmHg
• Pa,co2 32 mmHg
%0
20
40
60
80
100
32
68
SuccessFailed

• Health care workers exposure
• N=73,
• mean exposure 48h; weekly swaps (or symptoms)
• Gown, gloves, hair cover, face shields, FFP 2/3
• All negative in study period (10 days) and +14 days

HFNT in Covid
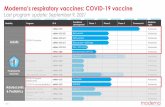
• Retrospective analysis, Paris hospitals
• N=379: 39% HFNT
• Baseline characteristics =
Demoule, Am J Respir Crit Care, 2020%
0
20
40
60
80
100
ETI 28 d Mortality 28 d
30
75
21
56
HFNTNRM<.0001
NS

HFNT in Covid
• Adjusted on propensity score
• N=137 per group
Demoule, Am J Respir Crit Care, 2020%
0
20
40
60
80
100
ETI 28 d Mortality 28 d
22
72
21
55
HFNTNRM<.0001
NS

Interim conclusion HFNT in CoVID
1. May reduce rate of intubation (remember Florali trial)
2. No data to support increased risk for HCW (…)
3. My opinion: Apply in patients “failing” NRM

Awake prone

Awake prone
Gattinoni Semin Resp CCM, 2019

• Single center, feasibility study, N = 56
• Require O2 a/o CPAP
• Non-ICU patients
• Aim for 3 h in prone (if less considered non-feasible)
• Pri. Outcome: △P/F before prone and 1 h after resupination (“recruitment”)

Awake prone
79% of patients with helmet
Feasible 84% of patients

Results
mm
Hg
0
100
200
300
400
P/F
193
286
181
SP1PP 10 minSP2<.0001
NS
• No difference
• Resp rate
• Paco2
• Accessory resp muscles
• Comfort score
• …

N=23 N=23 • No differences except time to prone
• No differences in outcome
• i.e. intubation 30% in both groups
Responders vs non-responders

Awake prone: case series
Sartini, JAMA 2020N=15, all NIV

Conclusion awake proning
1. Generally feasible and safe; Improvement in oxygenation
2. No (relevant) effect on oxygenation with resupination
3. My interpretation: “wait for further trials”

Patient self-inflicted lung injury
Brochard, Am J Respir Crit Care Med, 2017

Quantification of drive: P0.1
Telias, ICM, 2018
Healthy subjects:
P0.1 0.5 1.5 cmH2O
P0.1 intubated patients:
P0.1 < 1.5 cmH2O: over-assist
P0.1 > 3.5 cmH2O: under-assist

Esnault, Am J Respir Crit Care Med, in press
• Retrospective study (2 centers), Covid-ARDS, N=28
• PSV mode, measurement of P0.1 (mean of 3)
• Relapse of ventilatory failure in next 24h
• e.g. decrease P/F >20%; increase in Paco2 >10mmHg
• Protocolized weaning

Results
• Mean P0.1 4.4 ± 3.0 cmH2O; 32% followed by respiratory deterioration
Esnault, Am J Respir Crit Care Med, in press
6.93.0Best prognostic performance:
P0.1 >4.0 cmH2O:
Sens: 89% Spec: 74% PPV: 62% NPV: 93%

Early intubation?

Interim conclusion respiratory drive
1. Substantial (?) No of Covid patients high respiratory drive
2. High drive associated with respiratory deterioration (preliminary)
3. Monitor drive / effort (P0.1)

PEEP setting in Covid…

• Expert centers
• N=83, mean age 49 yrs
• Lung protective ventilation during ECMO
• Pa,o2 / Fi,o2 60 mmHg [54 - 68] @ PEEP 14 cmH2O (“sicker than EOLIA”)

36%
• Median length ECMO
• 20 days
• Median LOS ICU
• 36 days !


I can see clearly now: CARDS “=“ ARDS
1. Pathophysiology: not so different from classical ARDS
2. Lung protective ventilation: not so different from classical ARDS
3. Lung protective ventilation: understand respiratory physiology (ARDS & CARDS)
@drLeoHeunks

RESPIRATOIRE THERAPIE BIJ COVID-19
Leo Heunks
Op de volgende slides heeft de spreker een aantal vragen beantwoord die
door de deelnemers zijn gesteld en die tijdens de sessie niet zijn behandeld.

Wat zou jouw voorkeur zijn bij PEEP instellen bij COVID ARDS: gebruik PEEP tabellen, EIT of middels transpulmonaal drukken of anderszins en heeft de mate van shunting of obesitas hier nog een rol in?
Voor de klinische praktijk is het gebruik van de PEEP tabellen een redelijke keus. Ondanks de diverse studies die gedaan zijn waarbij deze tabellen zijn vergeleken met een andere techniek van PEEP titratie, laten die geen voordeel zien ten opzichte van de tabellen. Zoals besproken in de presentatie is het van belang de ademmechanica van de patiënt in overweging te nemen. Bij patiënten met een hoge compliantie zou ik de “lage PEEP / hoge Fio2 tabel gebruiken” en bij een lagere compliantie de “hoge PEEP / lage Fio2 tabel”. Als je helemaal een pragmatisch antwoord wenst: Mild ARDS gebruik PEEP van ongeveer 9 cmH2O en in matig-ernstig ARDS ± 15cmH2O. Dit is ook wat American Thoracic Society adviseert (Fan et al, AJRCCM 2017; PMID: 28459336).
PEEP titratie op basis van oesofagusballon gebruiken wij alleen bij complexe patiënten, bijvoorbeeld morbide obesitas, interstitiële longaandoeningen of zeer ernstige oxygenatiestoornissen (“pre-ECMO”). Uiteraard oesofagusballon alleen gebruiken bij voldoende expertise.
Ik zie elektrische impedantie tomografie vooralsnog vooral voor research, maar het aantal publicaties en expertise neemt snel toe en ik verwacht dat in de nabije toekomst er wel een rol is in patiëntenzorg.

Hoe is P-SILI bedside beste te meten (P0.1 of Pmus of anderzins) en wat zijn goede P-SILI eindpunten?
Het is belangrijk te realiseren dat P-SILI een relatief nieuw concept is en er geen klinische trials zijn die dit concept bewijzen. Ik denk wel dat er voldoende fysiologische studies en kleine klinische studies zijn die laten zien dat hoge ademarbeid longschade kan induceren / verergeren. Het lijkt daarom heel redelijk om ademarbeid / effort van patiënt te monitoren. Hiervoor is P0.1 het eenvoudigst. Referentie waarden zijn tussen 1.0 en ±4cmH2O (Telias et al, AJRCCM, 2020, PMID: 32097569; Jonkman, de Vries, Heunks, Crit Care , 2020, PMID: 32204710). Deze laatste referentie geeft ook toelichting hoe je beademing aanpast bij te hoge / lage P0.1.

Hoe om te gaan met P0.1, teugvolumes en beademingsdrukken bij switch PC/VC->PS. Ter voorbeeld: hoge TV bij lage drukken en hoge P0.1: wat te doen? Het antwoord hangt in grote mate af van de ernst van de longschade op dat moment (P/F ratio). Indien patiënt evident aan het verbeteren is (verbetering van de P/F ratio), zou ik wat liberaler zijn in TV, en tot 7 a 8 ml/Kg PBW accepteren en ook wat hogere P0.1 dan hierboven genoemd. Echter als P/F ratio slechter wordt, dan eerst proberen door middel van verhogen inspiratoire support de P0.1 te laten dalen. Als dat niet lukt dan lage dosis sedatie, bij voorkeur met propofol (zie ook: Jonkman, de Vries, Heunks, Crit Care , 2020, PMID: 32204710).

(Awake) proning wordt meestal met rugligging vergeleken. Is het niet zinvoller om awake patiënten met lagere P/F ratio’s preferentieel op hun zij te laten liggen en dat ook als controlegroep te nemen voor studies?
De gedachte achter buikligging is dat de basis van de “driehoek-vormig long” (zie presentatie) boven komt te liggen en dus V/Q ratio’s verbeteren en vooral de ademmechanica verbetert. Het is belangrijk om te benadrukken dat bij geïntubeerde patiënten het primaire doel van buikligging NIET is om de oxygenatie te verbeteren, maar om long-protectiever te kunnen beademen. Post hoc analyse van de PROSEA trial (Guerin, NEJM 2015) heeft aangetoond dat overlevingsvoordeel onafhankelijk is van de verbetering in oxygenatie (Albert et al, AJRCCM, 2014, PMID: 24528322).
Vanuit fysiologisch perspectief zie ik mogelijk een rol voor zijligging bij (voornamelijk) unilaterale longafwijkingen. Bij positioneren van de gezonde long onder, kunnen V/Q verhoudingen verbeteren. Er zijn echter nog geen geode trials en daarom zou ik het i.p. niet adviseren.

Zijn er al gegevens over de rol van longvaatweerstand en rechter ventrikel (cor pulmonale?) bij COVID-ARDS, oa. in vergelijk met klassieke ARDS? En is hier een verschil in prevalentie longembolieën van belang?
Het beeld zoals we het nu kennen bij COVID19-ARDS is vooral longvaattrombose ten gevolge van endotheel schade en niet zozeer longembolie. Uit onze eigen uitgebreide analyse lijkt er geen verschil in ademmechanica en zelfs gaswisseling tussen patiënten zonder en met longtrombose.