Resisting Temptation: Can Abuse- Deterrent Formulations...
13
© 2016 by the American Pharmacists Association. All rights reserved. 1 Resisting Temptation: Can Abuse- Deterrent Formulations Curb Opioid Abuse? Jeffrey Fudin, PharmD, DAAPM, FCCP, FASHP Clinical Pharmacy Specialist & PGY2 Pain Residency Director; Stratton VA Medical Center Adjunct Affiliations; Albany College of Pharmacy & Health Sciences, Western New England University, UCONN School of Pharmacy Shellie Keast, PharmD, PhD Assistant Professor University of Oklahoma College of Pharmacy Pharmacy Management Consultants 2 Disclosures • Dr. Keast declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria. • Dr. Fudin declares the following The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. • Kaléo (Speakers Bureau, Advisory Board) • KemPharm (Consultant) • Millennium Health, LLC (Speakers Bureau) • Remitigate, LLC (Founder, Owner) • Scilex Pharmaceuticals (Consultant) • Zogenix (Consultant) • Faculty (PainWeek; PainWeekEnds) 3 • Target Audience: Pharmacists • ACPE#: 0202-0000-16-072-L01-P • Activity Type: Knowledge-based 4 Learning Objectives 1. Explain how altering opioid formulations for abuse affects their kinetics and increases overdose risks 2. Compare and contrast tamper-deterrent opioid formulations and other pharmacological approaches to deter abuse 3. Describe validated risk assessment tool applicability for employing universal precautions and how this could apply to tamper-deterrent preference 4. Describe national and state efforts to curb abuse and misuse 5. Describe issues surrounding the selection of tamper- resistant products for individual patients 5 Which of the following factors does not influence the likability of opioids for abuse? A. Media attention B. High first-pass metabolism C. Tampering susceptibility D. Peer preferences 6 Embeda and Suboxone are examples of which type of approach to abuse-deterrent formulations (ADFs)? A. Physical barrier B. Viscosity management C. Sequestered antagonist D. Aversion agent
Transcript of Resisting Temptation: Can Abuse- Deterrent Formulations...

© 2016 by the American Pharmacists Association. All rights reserved.
1
Resisting Temptation: Can Abuse-Deterrent Formulations Curb Opioid
Abuse?
Jeffrey Fudin, PharmD, DAAPM, FCCP, FASHPClinical Pharmacy Specialist & PGY2 Pain Residency Director;
Stratton VA Medical Center
Adjunct Affiliations; Albany College of Pharmacy & Health Sciences, Western New England University, UCONN School of Pharmacy
Shellie Keast, PharmD, PhDAssistant Professor
University of Oklahoma College of PharmacyPharmacy Management Consultants
2
Disclosures• Dr. Keast declares no conflicts of interest, real or apparent, and no financial
interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
• Dr. Fudin declares the following
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
• Kaléo (Speakers Bureau, Advisory Board)
• KemPharm (Consultant)• Millennium Health, LLC (Speakers
Bureau)
• Remitigate, LLC (Founder, Owner)• Scilex Pharmaceuticals (Consultant)• Zogenix (Consultant)• Faculty (PainWeek; PainWeekEnds)
3
• Target Audience: Pharmacists
• ACPE#: 0202-0000-16-072-L01-P
• Activity Type: Knowledge-based
4
Learning Objectives
1. Explain how altering opioid formulations for abuse affects their kinetics and increases overdose risks
2. Compare and contrast tamper-deterrent opioid formulations and other pharmacological approaches to deter abuse
3. Describe validated risk assessment tool applicability for employing universal precautions and how this could apply to tamper-deterrent preference
4. Describe national and state efforts to curb abuse and misuse
5. Describe issues surrounding the selection of tamper-resistant products for individual patients
5
Which of the following factors does not influence the likability of opioids for abuse?
A. Media attention
B. High first-pass metabolism
C. Tampering susceptibility
D. Peer preferences
6
Embeda and Suboxone are examples of which type of approach to abuse-deterrent formulations (ADFs)?
A. Physical barrier
B. Viscosity management
C. Sequestered antagonist
D. Aversion agent
© 2016 by the American Pharmacists Association. All rights reserved.
7
What 2 pharmacokinetic properties are exploited to increase abuse potential?
A. Half-life and elimination factor
B. Maximum plasma concentration and time to peak concentration
C. Receptor binding affinity and excretion factor
D. Enzyme degradation and pro-drug metabolism
8
Which of the following national organizations have developed plans to curb misuse of prescription opioids?
A. Center for Disease Control and Prevention
B. Center for Medicare and Medicaid Services
C. Office of the President
D. All of the above
9
Which of the following characteristics is NOT associated with high nonmedical opioid use or use disorders?
A. Sedative use disorder
B. Disabled for work
C. Private insurance
D. Depression
10
IntroductionCurrent State of Prescription Drug Abuse
EpidemicDr. Shellie Keast
11
The Prescription Drug Abuse Epidemic
Source: National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services. 12
Nonmedical Use of Pain Relievers (NMPR)• 4.3 million used prescription pain relievers for nonmedical
purposes (1.6% of population)1
• Use has decreased from 2002, but plateaued beginning in 20131
• Marijuana, prescription pain relievers, and cocaine remain the main issues of concern1,2
© 2016 by the American Pharmacists Association. All rights reserved.
13
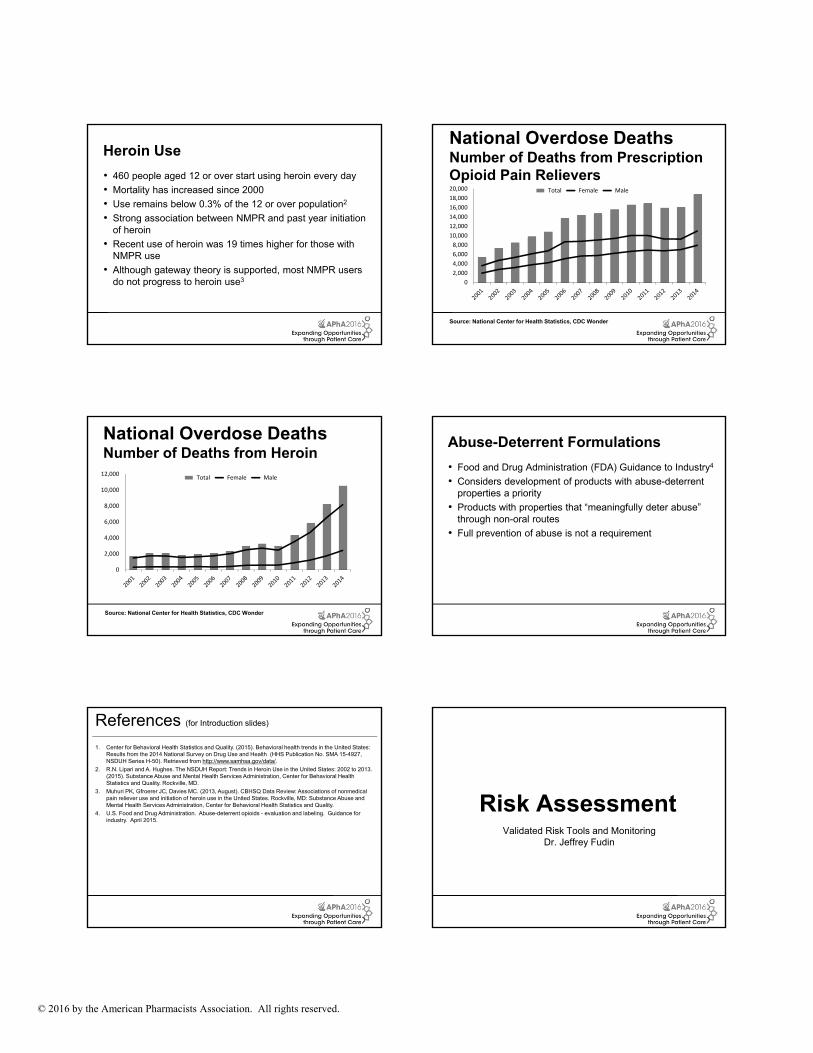
Heroin Use
• 460 people aged 12 or over start using heroin every day
• Mortality has increased since 2000
• Use remains below 0.3% of the 12 or over population2
• Strong association between NMPR and past year initiation of heroin
• Recent use of heroin was 19 times higher for those with NMPR use
• Although gateway theory is supported, most NMPR users do not progress to heroin use3
14
National Overdose DeathsNumber of Deaths from Prescription Opioid Pain Relievers
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000 Total Female Male
Source: National Center for Health Statistics, CDC Wonder
15
National Overdose DeathsNumber of Deaths from Heroin
0
2,000
4,000
6,000
8,000
10,000
12,000 Total Female Male
Source: National Center for Health Statistics, CDC Wonder
16
Abuse-Deterrent Formulations
• Food and Drug Administration (FDA) Guidance to Industry4
• Considers development of products with abuse-deterrent properties a priority
• Products with properties that “meaningfully deter abuse” through non-oral routes
• Full prevention of abuse is not a requirement
17
References (for Introduction slides)
1. Center for Behavioral Health Statistics and Quality. (2015). Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health (HHS Publication No. SMA 15-4927, NSDUH Series H-50). Retrieved from http://www.samhsa.gov/data/.
2. R.N. Lipari and A. Hughes. The NSDUH Report: Trends in Heroin Use in the United States: 2002 to 2013. (2015). Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Rockville, MD.
3. Muhuri PK, Gfroerer JC, Davies MC. (2013, August). CBHSQ Data Review: Associations of nonmedical pain reliever use and initiation of heroin use in the United States. Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality.
4. U.S. Food and Drug Administration. Abuse-deterrent opioids - evaluation and labeling. Guidance for industry. April 2015.
18
Risk AssessmentValidated Risk Tools and Monitoring
Dr. Jeffrey Fudin
© 2016 by the American Pharmacists Association. All rights reserved.
19
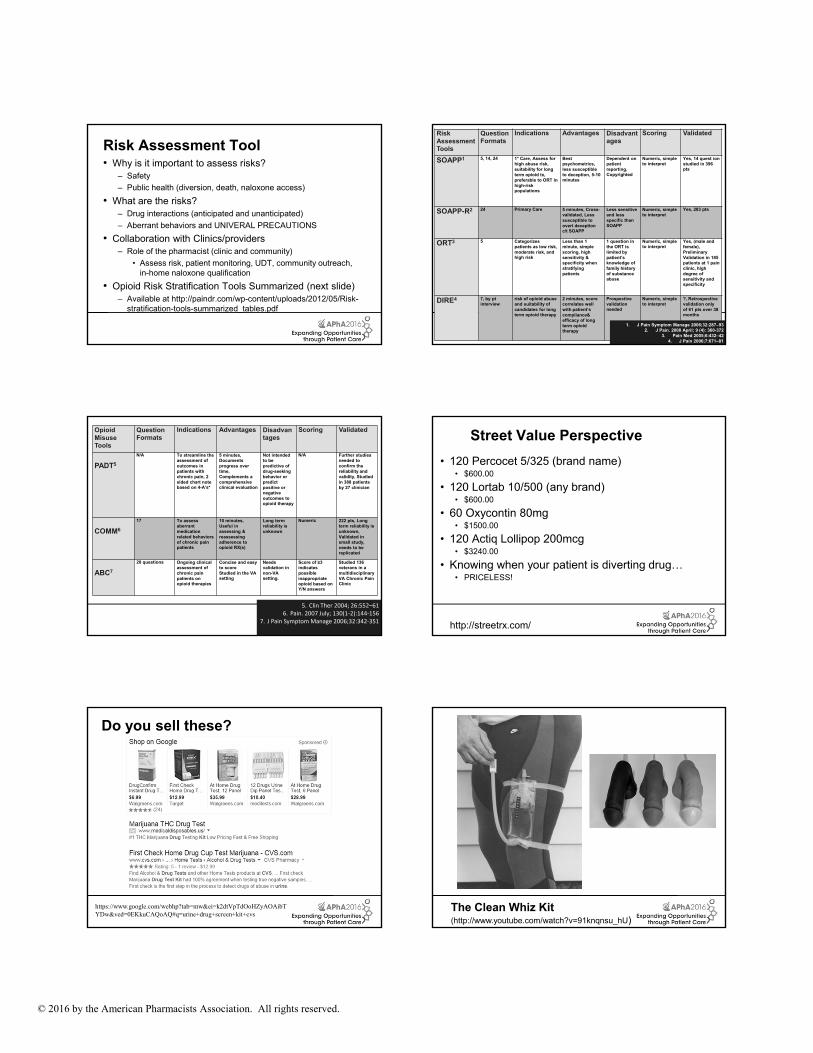
Risk Assessment Tool• Why is it important to assess risks?
– Safety
– Public health (diversion, death, naloxone access)
• What are the risks?– Drug interactions (anticipated and unanticipated)
– Aberrant behaviors and UNIVERAL PRECAUTIONS
• Collaboration with Clinics/providers– Role of the pharmacist (clinic and community)
• Assess risk, patient monitoring, UDT, community outreach,in-home naloxone qualification
• Opioid Risk Stratification Tools Summarized (next slide)– Available at http://paindr.com/wp-content/uploads/2012/05/Risk-
stratification-tools-summarized_tables.pdf
20
Risk Assessment Tools
Question Formats
Indications Advantages Disadvantages
Scoring Validated
SOAPP1 5, 14, 24 1° Care, Assess for high abuse risk, suitability for long term opioid tx, preferable to ORT in high-risk populations
Best psychometrics, less susceptible to deception, 5-10 minutes
Dependent on patient reporting, Copyrighted
Numeric, simple to interpret
Yes, 14 quest ion studied in 396 pts
SOAPP-R2 24 Primary Care 5 minutes, Cross-validated, Less susceptible to overt deception c/t SOAPP
Less sensitive and less specific than SOAPP
Numeric, simple to interpret
Yes, 283 pts
ORT3 5 Categorizes patients as low risk, moderate risk, and high risk
Less than 1 minute, simple scoring, high sensitivity & specificity when stratifying patients
1 question in the ORT is limited by patient’s knowledge of family history of substance abuse
Numeric, simple to interpret
Yes, (male and female), Preliminary Validation in 185 patients at 1 pain clinic, high degree of sensitivity and specificity
DIRE4 7, by pt interview
risk of opioid abuse and suitability of candidates for long term opioid therapy
2 minutes, score correlates well with patient’s compliance& efficacy of long term opioid therapy
Prospective validation needed
Numeric, simple to interpret
?, Retrospective validation only of 61 pts over 38 months
1. J Pain Symptom Manage 2006;32:287–93 2. J Pain. 2008 April; 9 (4): 360-372
3. Pain Med 2005;6:432–424. J Pain 2006;7:671–81
21
Opioid Misuse Tools
Question Formats
Indications Advantages Disadvantages
Scoring Validated
PADT5
N/A To streamline the assessment of outcomes in patients with chronic pain, 2 sided chart note based on 4-A’s*
5 minutes, Documents progress over time, Complements a comprehensive clinical evaluation
Not intended to be predictive of drug-seeking behavior or predict positive or negative outcomes to opioid therapy
N/A Further studies needed to confirm the reliability and validity, Studied in 388 patients by 27 clinician
COMM6
17 To assess aberrant medication related behaviors of chronic pain patients
10 minutes, Useful in assessing & reassessing adherence to opioid RX(s)
Long term reliability is unknown
Numeric 222 pts, Long term reliability is unknown, Validated in small study, needs to be replicated
ABC7
20 questions Ongoing clinical assessment of chronic pain patients on opioid therapies
Concise and easy to scoreStudied in the VA setting
Needs validation in non-VA setting.
Score of ≥3 indicates possible inappropriate opioid based on Y/N answers
Studied 136 veterans in a multidisciplinary VA Chronic Pain Clinic
5. Clin Ther 2004; 26:552–616. Pain. 2007 July; 130(1‐2):144‐156
7. J Pain Symptom Manage 2006;32:342‐351 22
Street Value Perspective
• 120 Percocet 5/325 (brand name) • $600.00
• 120 Lortab 10/500 (any brand)• $600.00
• 60 Oxycontin 80mg• $1500.00
• 120 Actiq Lollipop 200mcg• $3240.00
• Knowing when your patient is diverting drug…• PRICELESS!
http://streetrx.com/
23
Do you sell these?
https://www.google.com/webhp?tab=mw&ei=k2dtVpTdOoHZyAOAibTYDw&ved=0EKkuCAQoAQ#q=urine+drug+screen+kit+cvs 24
The Clean Whiz Kit (http://www.youtube.com/watch?v=91knqnsu_hU)

© 2016 by the American Pharmacists Association. All rights reserved.
25
Urine Drug Testing (UDT) Rationale
• Guidelines recommend UDT as standard of care when
prescribing chronic opioid therapy, especially for CNCP1‐5
• Helps to ensure compliance and mitigate risk1‐5
• Detects presence of illicit substances
• Detects absence of prescribed medication
• Helps to justify continual prescriptions
• Supports clinician decision to discontinue controlled substance
medication
26
Urine Drug Testing (UDT) Rationale
• Supports justification for closer monitoring
(more frequent visits / lab monitoring)
• Supports behavior modification and referral to
psychologist
Potential Pitfalls6-8
• Patient reliability to report compliance, use and misuse is
dubious and often poor
• Behavior alone is unreliable for identifying patients at risk
non-compliance, abuse, misuse, and diversion
27
References (for UDT slides)
1. Chou R, Fanciullo G, Fine P et al. Clinical Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer Pain. American Pain Society & American Academy of Pain Medicine Opioids Guideline Panel. Pain. 2009; 10(2):113-130.
2. Gourlay DL, Heit HA, Caplan YH. Urine Drug Testing in Clinical Practice: the Art and Science of Patient Care. 2010. Stamford, CT: PharmaCom Group, Inc.
3. Federation of State Medical Boards of the United States. Model Policy for the Use of Controlled Substances for the Treatment of Pain. J Pain & Palliative Care Pharmacotherapy. 2005; 19(2):73-78.
4. Manchikanti L, Abdi S, Atluri S et al. American Society of Interventional Pain Physicians (ASIPP) Guidelines for Responsible Opioid Prescribing in Chronic Non-Cancer Pain: Part 2-Guidance. Pain Physician. 2012; 15:S67-S116.
5. VA/DoD. Clinical Practice Guideline For Management of Opioid Therapy For Chronic Pain. 2010. [Online] Published May 2010. Accessed March 26, 2014. Available at http://www.va.gov/painmanagement/docs/cpg_opioidtherapy_fulltext.pdf
6. Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS. Validity of self-reported drug use in chronic pain patients. Clin J Pain 1999;15:184-191.2.
7. Berndt S, Maier C, Schultz HW. Polymedication and medication compliance in patients with chronic nonmalignant pain. Pain 1993;52:331-339j.
8. Katz NP, Sherburne S, Beach M, et al. Behavioral monitoring and urine toxicology testing in patients receiving long-term opioid therapy. Anesth Analg 2003;97:1097-1102.
28
Immune Assay (IA)
• In office or send out• Inexpensive• Results are quick (minutes)• Helps for initial detection• False negatives/positives• False patient accusations• Easier for pts to manipulate
low sensitivity, esp w/ synthetics• Presence/absence of RX class
only• No option for synthetics,
designer drugs, and unique natural products
Chromatography
• Usually send-out• More expensive• 24 hours to 1 week (per lab)• Final result• Definitive testing• Justifies RX decisions• 99.999 percent reliability
high sensitivity• Presence/absence of RX
metabolites• Custom option for synthetics,
designer drugs, and unique natural products
Types of Urine Drug Testing
29
Opioid Chemistry and Cross-sensitivity
Paindr.com; RESOURCES TAB; Opioid Chemistry30
Phenyl-Propylamines
Paindr.com; RESOURCES TAB; Opioid Chemistry
© 2016 by the American Pharmacists Association. All rights reserved.
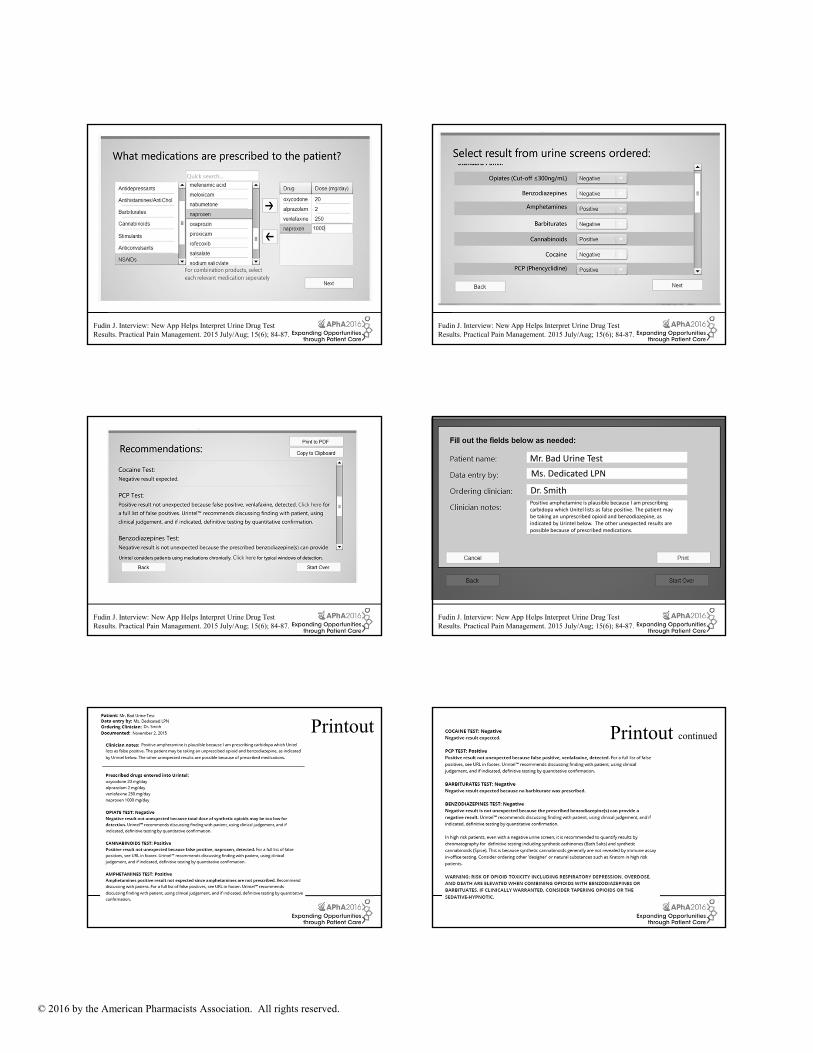
31Fudin J. Interview: New App Helps Interpret Urine Drug Test Results. Practical Pain Management. 2015 July/Aug; 15(6); 84-87. 32
Fudin J. Interview: New App Helps Interpret Urine Drug Test Results. Practical Pain Management. 2015 July/Aug; 15(6); 84-87.
33Fudin J. Interview: New App Helps Interpret Urine Drug Test Results. Practical Pain Management. 2015 July/Aug; 15(6); 84-87. 34
Mr. Bad Urine Test
Ms. Dedicated LPN
Dr. SmithPositive amphetamine is plausible because I am prescribing carbidopa which Unitel lists as false positive. The patient may be taking an unprescribed opioid and benzodiazepine, as indicated by Urintel below. The other unexpected results are possible because of prescribed medications.
Fudin J. Interview: New App Helps Interpret Urine Drug Test Results. Practical Pain Management. 2015 July/Aug; 15(6); 84-87.
35
Printout
36
Printout continued
© 2016 by the American Pharmacists Association. All rights reserved.
37
Efforts to Curb Misuse
Recent National and State EffortsDr. Shellie Keast
38
Recent National Efforts to Curb Misuse• 2010 – First abuse-deterrent opioid introduced (oxycodone
extended-release)
• 2011 – Obama Administration detailed a response to the drug abuse crisis1
• 2012 – CMS issues strategies to reduce diversion in Medicaid2
• 2013 – FDA required changes to long-acting and extended release opioid pain medications and released draft guidance on abuse-deterrent opioids3
39
Recent National Efforts to Curb Misuse, Cont.• 2015 – Issues final guidance to industry regarding abuse-
deterrent opioids4
• 2015 – Obama Administration announced new steps to increase access to drug treatment5
• 2015 – CDC launches Prescription Drug Overdose: Prevention for states6
40
State Efforts
• States have also initiated efforts to curb abuse
• Kentucky enacted a strict mandate for PDMP (2012)
• Massachusetts developed a comprehensive strategy to end opioid abuse (2014)
• Arizona issued opioid prescribing guidelines (2014)
• Wisconsin begins “Dose of Reality” media campaign (2015)
• The list goes on…..
41
Oklahoma’s History
• Medicaid policies to curb abuse and misuse7:– 2003 to 2015: 13 unique policies implemented
– Various levels of success
• Governor's task on prescription opioid abuse (2012)
• Senate study on opioids with abuse-deterrent properties (2015)
• General agreement that solution requires collaborative effort between state agencies and communities
42
Research on Effect of Abuse-Deterrent Opioids• Largely centered around oxycodone extended-release8-17
• Changes in use of oxycodone extended-release after release of new formulation18
– Decrease from 46% to 26% in past-month use in first year
– 33% of abuser of original formulation continued to abuse new
– 33% of abusers of original changed drugs
– 5% indicated new influenced decision to stop abusing drugs
• Most who continued abusing either changed to oral route or defeated the abuse-deterrent mechanism
• 70% who switched drugs turned to heroin
© 2016 by the American Pharmacists Association. All rights reserved.
43
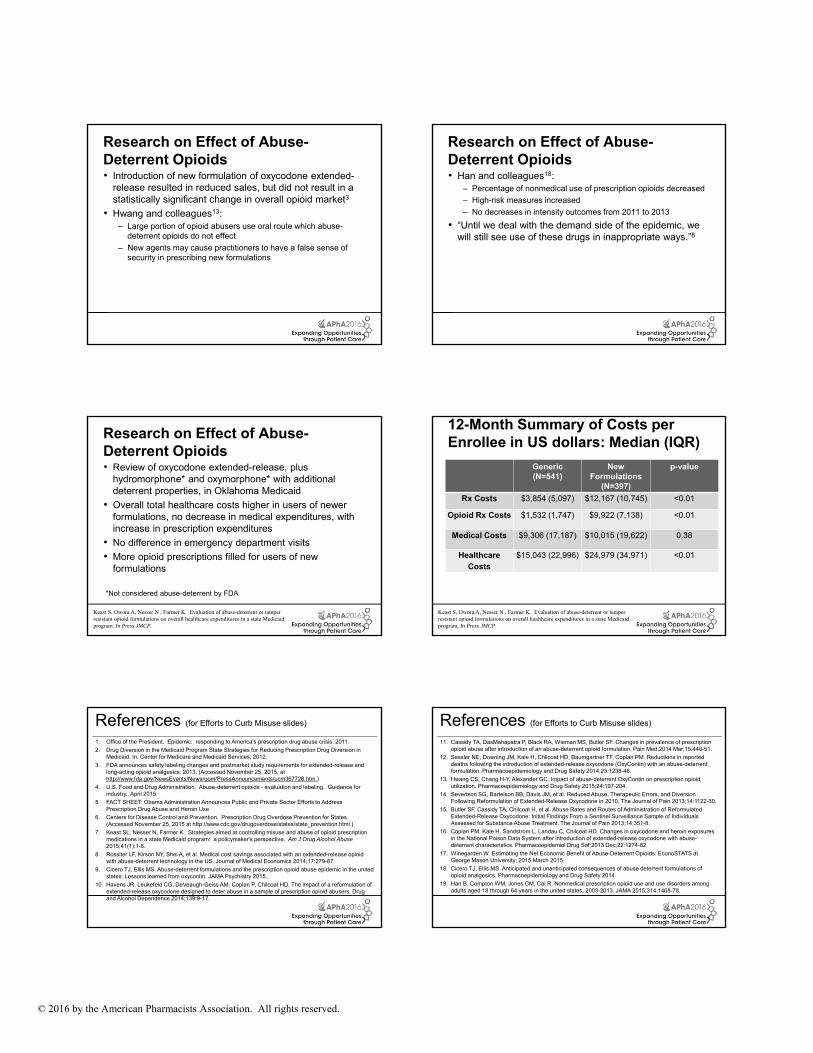
Research on Effect of Abuse-Deterrent Opioids• Introduction of new formulation of oxycodone extended-
release resulted in reduced sales, but did not result in a statistically significant change in overall opioid market3
• Hwang and colleagues13:– Large portion of opioid abusers use oral route which abuse-
deterrent opioids do not effect
– New agents may cause practitioners to have a false sense of security in prescribing new formulations
44
Research on Effect of Abuse-Deterrent Opioids• Han and colleagues18:
– Percentage of nonmedical use of prescription opioids decreased
– High-risk measures increased
– No decreases in intensity outcomes from 2011 to 2013
• “Until we deal with the demand side of the epidemic, we will still see use of these drugs in inappropriate ways.”8
45
Research on Effect of Abuse-Deterrent Opioids• Review of oxycodone extended-release, plus
hydromorphone* and oxymorphone* with additional deterrent properties, in Oklahoma Medicaid
• Overall total healthcare costs higher in users of newer formulations, no decrease in medical expenditures, with increase in prescription expenditures
• No difference in emergency department visits
• More opioid prescriptions filled for users of new formulations
*Not considered abuse-deterrent by FDA
Keast S, Owora A, Nesser N , Farmer K. Evaluation of abuse-deterrent or tamper resistant opioid formulations on overall healthcare expenditures in a state Medicaid program. In Press JMCP. 46
12-Month Summary of Costs per Enrollee in US dollars: Median (IQR)
Generic (N=541)
New Formulations
(N=397)
p-value
Rx Costs $3,854 (5,097) $12,167 (10,745) <0.01
Opioid Rx Costs $1,532 (1,747) $9,922 (7,138) <0.01
Medical Costs $9,306 (17,187) $10,015 (19,622) 0.38
Healthcare Costs
$15,043 (22,996) $24,979 (34,971) <0.01
Keast S, Owora A, Nesser N , Farmer K. Evaluation of abuse-deterrent or tamper resistant opioid formulations on overall healthcare expenditures in a state Medicaid program. In Press JMCP.
47
References (for Efforts to Curb Misuse slides)
1. Office of the President. Epidemic: responding to America's prescription drug abuse crisis. 2011.
2. Drug Diversion in the Medicaid Program State Strategies for Reducing Prescription Drug Diversion in Medicaid. In: Center for Medicare and Medicaid Services; 2012.
3. FDA announces safety labeling changes and postmarket study requirements for extended-release and long-acting opioid analgesics. 2013. (Accessed November 25, 2015, at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm367726.htm.)
4. U.S. Food and Drug Administration. Abuse-deterrent opioids - evaluation and labeling. Guidance for industry. April 2015.
5. FACT SHEET: Obama Administration Announces Public and Private Sector Efforts to Address Prescription Drug Abuse and Heroin Use
6. Centers for Disease Control and Prevention. Prescription Drug Overdose Prevention for States. (Accessed November 25, 2015 at http://www.cdc.gov/drugoverdose/states/state_prevention.html.)
7. Keast SL, Nesser N, Farmer K. Strategies aimed at controlling misuse and abuse of opioid prescription medications in a state Medicaid program: a policymaker's perspective. Am J Drug Alcohol Abuse2015;41(1):1-6.
8. Rossiter LF, Kirson NY, Shei A, et al. Medical cost savings associated with an extended-release opioid with abuse-deterrent technology in the US. Journal of Medical Economics 2014;17:279-87.
9. Cicero TJ, Ellis MS. Abuse-deterrent formulations and the prescription opioid abuse epidemic in the united states: Lessons learned from oxycontin. JAMA Psychiatry 2015.
10. Havens JR, Leukefeld CG, DeVeaugh-Geiss AM, Coplan P, Chilcoat HD. The impact of a reformulation of extended-release oxycodone designed to deter abuse in a sample of prescription opioid abusers. Drug and Alcohol Dependence 2014;139:9-17.
48
References (for Efforts to Curb Misuse slides)
11. Cassidy TA, DasMahapatra P, Black RA, Wieman MS, Butler SF. Changes in prevalence of prescription opioid abuse after introduction of an abuse-deterrent opioid formulation. Pain Med;2014 Mar;15:440-51.
12. Sessler NE, Downing JM, Kale H, Chilcoat HD, Baumgartner TF, Coplan PM. Reductions in reported deaths following the introduction of extended-release oxycodone (OxyContin) with an abuse-deterrent formulation. Pharmacoepidemiology and Drug Safety 2014;23:1238-46.
13. Hwang CS, Chang H-Y, Alexander GC. Impact of abuse-deterrent OxyContin on prescription opioid utilization. Pharmacoepidemiology and Drug Safety 2015;24:197-204.
14. Severtson SG, Bartelson BB, Davis JM, et al. Reduced Abuse, Therapeutic Errors, and Diversion Following Reformulation of Extended-Release Oxycodone in 2010. The Journal of Pain 2013;14:1122-30.
15. Butler SF, Cassidy TA, Chilcoat H, et al. Abuse Rates and Routes of Administration of Reformulated Extended-Release Oxycodone: Initial Findings From a Sentinel Surveillance Sample of Individuals Assessed for Substance Abuse Treatment. The Journal of Pain 2013;14:351-8.
16. Coplan PM, Kale H, Sandstrom L, Landau C, Chilcoat HD. Changes in oxycodone and heroin exposures in the National Poison Data System after introduction of extended-release oxycodone with abuse-deterrent characteristics. Pharmacoepidemiol Drug Saf;2013 Dec;22:1274-82.
17. Winegarden W. Estimating the Net Economic Benefit of Abuse-Deterrent Opioids: EconoSTATS at George Mason University; 2015 March 2015.
18. Cicero TJ, Ellis MS. Anticipated and unanticipated consequences of abuse deterrent formulations of opioid analgesics. Pharmacoepidemiology and Drug Safety 2014.
19. Han B, Compton WM, Jones CM, Cai R. Nonmedical prescription opioid use and use disorders among adults aged 18 through 64 years in the united states, 2003-2013. JAMA 2015;314:1468-78.
© 2016 by the American Pharmacists Association. All rights reserved.
49
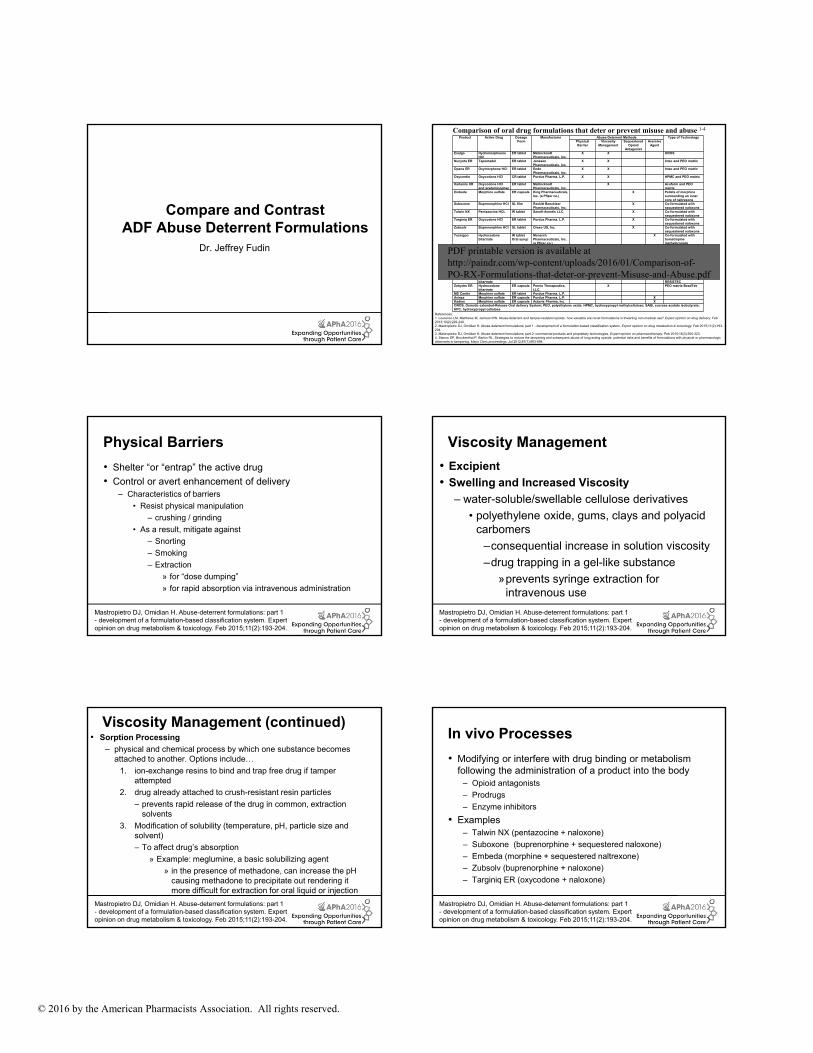
Compare and Contrast ADF Abuse Deterrent Formulations
Dr. Jeffrey Fudin
Product Active Drug Dosage Form
Manufacturer Abuse-Deterrent Methods Type of TechnologyPhysical Barrier
Viscosity Management
Sequestered Opioid
Antagonist
Aversive Agent
Exalgo Hydromorphoone HCl
ER tablet Mallinckrodt Pharmaceuticals, Inc.
X X OROS
Nucynta ER Tapentadol ER tablet Janssen Pharmaceuticals, Inc.
X X Intac and PEO matrix
Opana ER Oxymorphone HCl ER tablet Endo Pharmaceuticals, Inc.
X X Intac and PEO matrix
Oxycontin Oxycodone HCl CR tablet Purdue Pharma, L.P. X X HPMC and PEO matrix
Xartemis XR Oxycodone HCl and acetaminophen
ER tablet Mallinckrodt Pharmaceuticals, Inc.
X Acuform and PEO matrix
Embeda Morphine sulfate ER capsule King Pharmaceuticals, Inc. (a Pfizer co.)
X Pellets of morphine surrounding an inner core of naltrexone
Suboxone Buprenorphine HCl SL film Reckitt Benckiser Pharmaceuticals, Inc.
X Co-formulated with sequestered naloxone
Talwin NX Pentazocine HCL IR tablet Sanofi-Aventis LLC. X Co-formulated with sequestered naloxone
Targiniq ER Oxycodone HCl ER tablet Purdue Pharma, L.P. X Co-formulated with sequestered naloxone
Zubsolv Buprenorphine HCl SL tablet Orexo US, Inc. X Co-formulated with sequestered naloxone
Tussigon Hydrocodone bitartrate
IR tabletOral syrup
Monarch Pharmaceuticals, Inc. (a Pfizer co.)
X Co-formulated with homatropine methylbromide
Oxecta Oxycodone HCl IR tablet King Pharmaceuticals, Inc. (a Pfizer co.)
X X Aversion and PEO matrix
Remoxy Oxycodone HCl ER capsule Pain Therapeutics (a Durect Corporation co.)
X ORADUR and SAIB matrix
Xtampza Oxycodone HCl ER capsule Collegium Pharmaceutical, Inc.
? ? DeteRx
Hysingla ER Hydrocodone bitartrate
ER tablet Purdue Pharma, L.P. X X PEO matrix and HPC RESISTEC
Zohydro ER Hydrocodone bitartrate
ER capsule Pernix Therapeutics, LLC.
X PEO matrix BeadTek
MS Contin Morphine sulfate ER tablet Purdue Pharma, L.P.Avinza Morphine sulfate ER capsule Purdue Pharma, L.P. XKadian Morphine sulfate ER capsule Actavis Pharma, Inc. XOROS, Osmotic extended-Release Oral delivery System; PEO, polyethylene oxide; HPMC, hydroxypropyl methylcellulose; SAIB, sucrose acetate isobutyrate; HPC, hydroxypropyl cellulose
Comparison of oral drug formulations that deter or prevent misuse and abuse 1-4
References:1. Lourenco LM, Matthews M, Jamison RN. Abuse-deterrent and tamper-resistant opioids: how valuable are novel formulations in thwarting non-medical use? Expert opinion on drug delivery. Feb 2013;10(2):229-240.2. Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204.3. Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 2: commercial products and proprietary technologies. Expert opinion on pharmacotherapy. Feb 2015;16(3):305-323.4. Stanos SP, Bruckenthal P, Barkin RL. Strategies to reduce the tampering and subsequent abuse of long-acting opioids: potential risks and benefits of formulations with physical or pharmacologic deterrents to tampering. Mayo Clinic proceedings. Jul 2012;87(7):683-694.
PDF printable version is available athttp://paindr.com/wp-content/uploads/2016/01/Comparison-of-PO-RX-Formulations-that-deter-or-prevent-Misuse-and-Abuse.pdf
51
Physical Barriers
• Shelter “or “entrap” the active drug
• Control or avert enhancement of delivery– Characteristics of barriers
• Resist physical manipulation
– crushing / grinding
• As a result, mitigate against
– Snorting
– Smoking
– Extraction
» for “dose dumping”
» for rapid absorption via intravenous administration
Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204. 52
Viscosity Management
• Excipient
• Swelling and Increased Viscosity
– water-soluble/swellable cellulose derivatives
• polyethylene oxide, gums, clays and polyacid carbomers
–consequential increase in solution viscosity
–drug trapping in a gel-like substance
»prevents syringe extraction for intravenous use
Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204.
53
Viscosity Management (continued)• Sorption Processing
– physical and chemical process by which one substance becomes attached to another. Options include…
1. ion-exchange resins to bind and trap free drug if tamper attempted
2. drug already attached to crush-resistant resin particles
– prevents rapid release of the drug in common, extraction solvents
3. Modification of solubility (temperature, pH, particle size and solvent)
– To affect drug’s absorption
» Example: meglumine, a basic solubilizing agent
» in the presence of methadone, can increase the pH causing methadone to precipitate out rendering it more difficult for extraction for oral liquid or injection
Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204. 54
In vivo Processes
• Modifying or interfere with drug binding or metabolism following the administration of a product into the body
– Opioid antagonists
– Prodrugs
– Enzyme inhibitors
• Examples– Talwin NX (pentazocine + naloxone)
– Suboxone (buprenorphine + sequestered naloxone)
– Embeda (morphine + sequestered naltrexone)
– Zubsolv (buprenorphine + naloxone)
– Targiniq ER (oxycodone + naloxone)
Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204.
© 2016 by the American Pharmacists Association. All rights reserved.
55
Other In vivo OptionsInactive prodrug mitigates against…
– Parenteral
– Nasal
– Smoking
• Pharmacokinetic advantages…
– Extends time to peak
• Possibly lessen the euphoric effects
Enzyme inhibitors
– Inhibit or slow the transformation to drug to active metabolite
Sequestered metabolic blocking agents
– Released upon administration of a tampered product
• deter abuse by crushing or chewing for snorting or parenteral administration
• Advantage over antagonist formulations, blunted immediate withdrawal
Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204. 56
Modifying Drug Favorability• Oxecta has 2 unique abuse deterrent properties
– Sodium lauryl sulfate - snorting becomes unpleasant
– Excipient results in gel formation with attempt to dissolve
• Previous to Oxecta – Acurox
• Oxycodone + niacin
• Other Aversive Options– constituents that trigger unpleasant and very noxious SEs
• laxatives (ex. bisacodyl, casanthanol, senna), nauseants (zinc salts, ipecac, cephaeline), bittering agents (ex. menthol, eucalyptus oil, denatonium benzoate, denatonium saccharide), and mucous membrane irritants (resiniferatoxin, olvanil, sodium lauryl sulfate)
Mastropietro DJ, Omidian H. Abuse-deterrent formulations: part 1 - development of a formulation-based classification system. Expert opinion on drug metabolism & toxicology. Feb 2015;11(2):193-204.
57
Patient SelectionDr. Shellie Keast
58
Right Drug for the Right Patient
• Choosing the proper patient for an abuse-deterrent product may not be straightforward
• Choice may be based more on who is most likely to abuse opioids
• Characteristics associated with high nonmedical use or use disorders (Han 2015):
– Sedative use disorders
– Other substance disorders (nicotine, etc)
– Disabled for work
– Medicaid as primary insurance
– Depression, mental health diagnoses
59
Right Drug for the Right Patient
• Incorporate risk assessment tools before prescribing
• Perform frequent Urine Drug Testing
• Utilization of PDMP monitoring systems by all providers
• Have a plan to discontinue opioids prior to initiation
• Pain management patient contracts– http://www.aafp.org/fpm/2001/1100/fpm20011100p47-rt1.pdf
– Provide structure, support, and monitoring1
• Know the demographics and abuse rates in your practice area
• Remember that abuse-deterrent opioids can still be abused by oral route of administration
1. Hariharan J, Lamb GC, Neuner JM. Long-Term Opioid Contract Use for Chronic Pain Management in Primary Care Practice. A Five Year Experience. Journal of General Internal Medicine 2007;22:485-90. 60
Manipulating the ADFAnd Altered Pharmacokinetics
Dr. Jeffrey Fudin
© 2016 by the American Pharmacists Association. All rights reserved.
61
One step forward, two steps back
62
Where to buy them…
https://www.youtube.com/watch?v=XemdKyIrWUo
63https://drugs-forum.com/forum/showthread.php?t=255151
64
Overcoming Abuse Deterrent Tablets
https://www.youtube.com/watch?v=2pnfuz2_y0Y
65
Pharmacist & Community ServiceCan we help?
https://www.youtube.com/results?search_query=evzio+fudin66
Trying to help other addicts…
https://www.youtube.com/watch?v=KE8NFd4TUVc
© 2016 by the American Pharmacists Association. All rights reserved.
67
Key Points• Nonmedical use of pain relievers continues to be an
important medical and societal problem.
• Abuse-deterrent formulations are being developed to “meaningfully deter abuse” through non-oral routes.
• Patients with increase substance abuse risk include male gender, family and/or personal hx substance abuse, smoker, alcoholism, PTSD, schizophrenia
• National and state entities are actively involved in efforts to curb misuse
• Current research into abuse-deterrent formulations indicate some decrease in non-oral misuse, but heroin use may be increasing
• ADF’s do not prevent abuse; they mitigate risks
68
Key Points
• Selecting the right patient for these formulations is challenging – planning and monitoring are the key
• ADF’s are not created equal
– Some deter abuse by injecting oral formulations
– Some deter abuse by snorting
– Some deter dose-dumping when ingested with alcohol
– All can be taken in large quantities and cause death
• Newer formulation on the way may overcome this
69
Which of the following factors does not influence the likability of opioids for abuse?
A. Media attention
B. High first-pass metabolism
C. Tampering susceptibility
D. Peer preferences
• ANSWER: B. Factors that influence opioid abuse attractiveness include media attention, peer preferences, low cost, availability, tampering susceptibility, and a high attractiveness quotient (high Cmax, low Tmax).
70
Embeda and Suboxone are examples of which type of approach to abuse-deterrent formulations (ADFs)?
A. Physical barrier
B. Viscosity management
C. Sequestered antagonist
D. Aversion agent
ANSWER: C. Embeda and Suboxone contain sequestered naltrexone and naloxone, respectively.
71
What 2 pharmacokinetic properties are exploited to increase abuse potential?
A. Half-life and elimination factor
B. Maximum plasma concentration and time to peak concentration
C. Receptor binding affinity and excretion factor
D. Enzyme degradation and pro-drug metabolism
ANSWER: B. An increased maximum plasma concentration (Cmax) and decreased time to maximum concentration (Tmax) increase abuse potential.
72
Which of the following national organizations have developed plans to curb misuse of prescription opioids?
A. Center for Disease Control and Prevention
B. Center for Medicare and Medicaid Services
C. Office of the President
D. All of the above
ANSWER: D. All of the listed organizations have developed plans to curb misuse. States have also developed localized plans to curb misuse.

© 2016 by the American Pharmacists Association. All rights reserved.
73
Which of the following characteristics is NOT associated with high nonmedical opioid use or use disorders?
A. Sedative use disorder
B. Disabled for work
C. Private insurance
D. Depression
ANSWER: C. Medicaid as primary insurance is a characteristic associated with high nonmedical opioid use or use disorder.


















