Resistencias a los ARVs - fai.org.co · PDF fileMargot NA et al. Anti Res 2016 Margot NA et...
47
José Luis Blanco Servicio de Enfermedades Infecciosas Hospital Clinic. Barcelona Resistencias a los ARVs Medellin, 1 de Julio del 2017
Transcript of Resistencias a los ARVs - fai.org.co · PDF fileMargot NA et al. Anti Res 2016 Margot NA et...

José Luis BlancoServicio de Enfermedades Infecciosas
Hospital Clinic. Barcelona
Resistencias a los ARVs
Medellin, 1 de Julio del 2017

Presenter Disclosure Information
– Research Support: ViiV, BMS, MSD, Jansen
– Speaker’s Bureau: Abbvie, Bristol-Myers Squibb, Merck,Jansen, ViiV Healthcare, Stendhal
– Advisory Panel: Gilead, Stendhal, Gador,Jansens, ViiV

Agenda
• Introducción: conceptos básicos
• Test de resistencias: nuevas herramientas
• Resistencias en el paciente naïve
• Resistencias a los ANITI/ANNITI/PI: qué debemos saber
• INIs: datos de resistencias
• Conclusiones

0 2-6 w
Virological Failure (VF)
VL<50 cop/mL
VF
“Blip”
VL<200 cop/mL
• Check again patient’s adherence
• Rule out DDI
• Infections/vaccinations

Resistance: more than “Genetic barrier”

VL
Limit of Detection
VF
ART: A+B+C+D
week/sdays yearsmonths
mutation to B
mutation to A
mutation to C
time
drug A: very low robustness(GB)
drug B: low robustnessdrug C: moderate robustness
drug D: high robustness
mutation to D
i.e.: EFV, NEV
i.e.: d4t, PI/r
i.e. : IP non boostedi.e.: 3TC
INIs
RAL,EGV/COBI
DGV (?)*
*from in vitro data
“Robustedness”: in vivo concept

High Level of Resistance
“Genetic Barrier-GB”: concept
Drug A: low GB
Drug B: moderate GB
Drug C: high GB
3TC
i.e.: EFV, NEV, RPV, 3TC
i.e. : IP/r
i.e.: ETR
INIs
RAL,EGV/COBI
DGV (?)*
each step = 1 mutation ABC*d4T*, TDF*
1 mutationDrug CDrug A Drug B
2-3 mutations >3 mutations
* : depends on the pathway of scape
ETR DRV/r
M184V G190A
Y181C
I84V
L33F
V32I
I47V
I54L
TDF
K65R
TDF
K70R
K219Q
T215F
M41L
T210W


Agenda
• Introducción: conceptos básicos
• Test de resistencias: nuevas herramientas
• Resistencias en el paciente naïve
• Resistencias a los ANITI/ANNITI/PI: qué debemos saber
• INIs: datos de resistencias
• Conclusiones

Standard Sanger Sequencing Detects the Most Common Circulating HIV-1 Variants

Standard
Cloning
Allele-specific PCR Parallel Allele-Specific
Sequencing (PASS)
Single
Genome
sequencing
Ultra deep sequencing
(454 life sciences/Roche)
Concept Analysis of
single CFUs
with indiviual
clones
Differential
amplification of
mutants vs WT in
real-time PCR
Single-base allele
sequencing of polonies
fixed to an acrylamide
surface
Massive
sequencing of
single genome
molecules
Massively parallel
microfluidic solid-surface
sequencing of single
molecules (105 reads)
Sensitivity > 10% 0.003 - 0.4% 0.1% 2% 0.5 – 1%
# mutations multiple 1 1 per round (up to 22
rounds)
Multiple within 300 bp
Linked
mutations
Yes No Yes Yes Yes
Labor
Intensity
Cost
Best Experience,
PPV
S, PPV, NPV,
Affordable
S, linkage of muts Linkage Linkage, Accuracy, S, NPV,
Labor intensity, Rapidity
of results
Worst S, NPV Only 1 mutant,
Sp, effect of
polymorphisms,
Cost, Labor intensity Cost, time and
labor
consuming
Short sequence,
background noise, Sp
TOOLS TO STUDY MINORITY VARIANTS
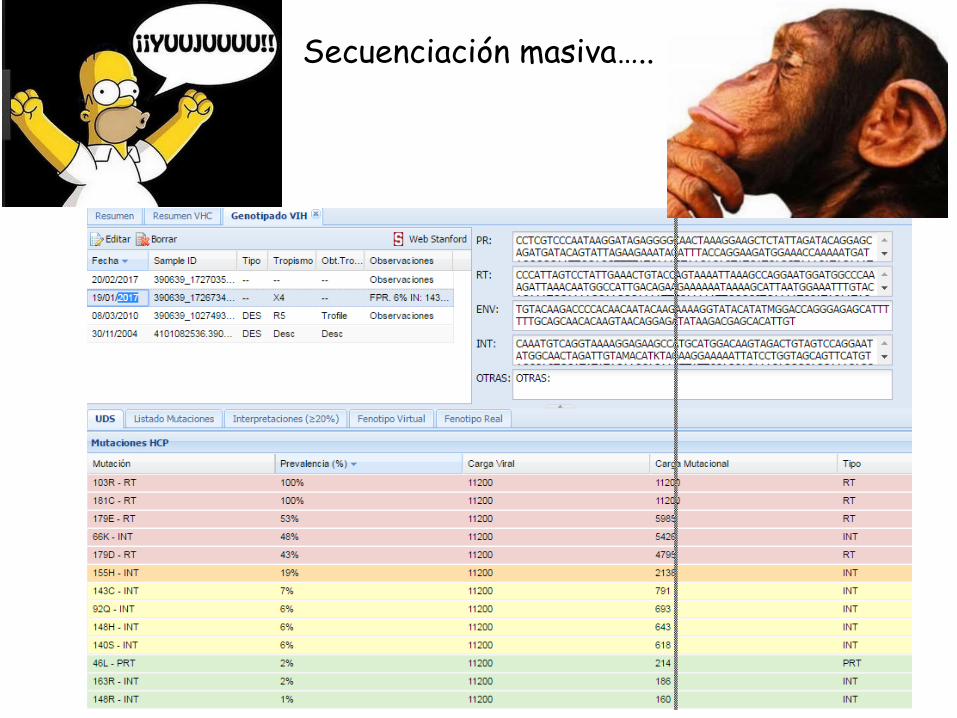
Secuenciación masiva…..

FV???

Secuenciación masiva…..

Agenda
• Introducción: conceptos básicos
• Test de resistencias: nuevas herramientas
• Resistencias en el paciente naïve
• Resistencias a los ANITI/ANNITI/PI: qué debemos saber
• INIs: datos de resistencias
• Conclusiones

Avila-Ríos et al., unpublished
Publications on HIV TDR in the Andean Region, 2000-2015
Colombia
Peru
Venezuela
Low level HIVDRModerate level HIVDRHigh level HIVDR
Special populationsPregnant women
TDRprevalence(%)
AuthorsYearof
publicationCountryandarea
Samplingyears
StudyPopulation NAnydrug
classNRTI NNRTI PI
DiazGranadoset
al.
2010 Colombia(Bogotá/
Cundinamarca,Valle
delCauca,Antioquia,
Atlantico/Bolivar,Santander,Caldas/
Risaralda)
2006-2008Mixed 103 5.8 2.9 4.9 1.0
MSM 326 3.4 2.1 0.6 1.8Lamaetal. 2006 Peru(Lima,Sullana,
Piura,Arequipa,
Iuitos,Pucallpa)
2002-2003
RecentlyinfectedMSM(DetunedEIA)
33 3.0 3.0 3.0 3.0
Guaniraetal. 2009 Perú(Lima,Arequipa,
Ica,Sullana)and
Ecuador(Guayaquil)
2006 MSM 117 4.3 0.6 2.6 0.6
Soriaetal. 2011 Peru(Lima) 2007-2009 Mixed 96 1.0 0 1.0 0
Delgadoetal. 2001 Venezuela 1999 Mixed 31 3.2 3.2 0 0
Bouchardetal. 2007 Venezuela(Caracas,
CentralVenezuela)
2003 Mixed 20 5.0 5.0 0 0
Rangeletal. 2009 Venezuela(Caracas) 2004-2007 Mixed 63 11.0 9.5 3.2 1.6
Castilloetal. 2009 Venezuela(Caracas) 2008 Mixed 62 6.5 3.2 1.6 1.6

No KEY InSTIs mutations

DEPARTAMENTO DE INVESTIGACIÓN EN ENFERMEDADES INFECCIOSAS
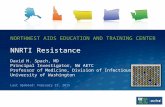
INI TDR survey in Mexico
17.3%
52.1 %26.5 %
No data 4.1 %
Major INI TDR mutations
INI TDR1.0%
Accessory INI TDR mutations
Atypical polymorphisms in IN positions associated with DR
Agenda
• Introducción: conceptos básicos
• Test de resistencias: nuevas herramientas
• Resistencias en el paciente naïve
• Resistencias a los ANITI/ANNITI/PI: qué debemos saber
• INIs: datos de resistencias
• Conclusiones

RESISTENCIAS a los ANITI
Mutaciones seleccionadasInicialmente por el fármaco
Mutaciones existentesque condicionan resistencia
cruzada al fármaco
AZT: 215YddI: 74V3TC: 184Vd4T: 75VFTC: 184VTDF: 65RABA: 74V/65R
En monoterapia En combinación
Depende:
-NRTI acompañante
-Niveles PK??
-Otros F
acompañantes
- TAMs
- 41L,210W, 215Y (via 1)
- 67N,70R,215F,219Q (via 2)
- 184V
- Otras : 65R,74V, 44D,118I
- Patrones multi-R: 151Q,69SSS

21 - GILEAD CONFIDENTIAL AND PROPRIETARY DRAFT. FOR INTERNAL USE ONLY. NOT FOR DISTRIBUTION OR PROMOTION.21 - GILEAD CONFIDENTIAL AND PROPRIETARY DRAFT. FOR INTERNAL USE ONLY. NOT FOR DISTRIBUTION OR PROMOTION.
LYMPHOCYTE
TFV
OAT
1 & 3
OAT
1 & 3
RENAL
TUBULAR
CELL
TFV
RENAL
TUBULAR
CELL
PLASMA
TFV
ESTER
AMIDATE
DIANION
TDF(tenofovir
disoproxil
fumarate)
300 mg
TAF(tenofovir
alafenamide)
25 mg
TFV(tenofovir)
PRO
DRUGLONGER PLASMA HALF-LIFE † - GREATER PLASMA
STABILITY
SHORT PLASMA
HALF-LIFE†
TFV HIV
GI TRACT
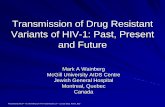
TAF – A Novel Prodrug of Tenofovir
Prodrug Pharmacology‡
OAT, organic anion transporter; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate; TFV, tenofovir.
TAF results in 80-90% lower TFV plasma levels compared to TDF
1. Sax P, et al. Lancet 2014 2. Ruane P, et al. J Acquir Immune Defic Syndr 2013; 63:449-5. 3. Data on file

0
20
40
60
80
100
120
TDF(300 mg)
TAF(25 mg)
Pla
sma
TFV
(%
of
TDF
valu
e)
~90% less TFV in
plasma
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
TDF(300 mg)
TAF(25 mg)
HIV
RN
A r
ed
uct
ion
; Day
11
(Lo
g10
c/m
L)
~ 0.5 Log more in VL
reduction
Ruane P et al. JAIDS 2013;63:449–455
P=0.024
Phase Ib, randomised, dose ranging study, evaluating antiviral activity, safety and pharmacokinetics/pharmacodynamics of 10 day monotherapy with TAF (N=38)
In comparison to TDF, antiviral activity was increased with TAF and TFV exposure was decreased at an approximately 90% lower dose
Study GS-US-120-0104
Virological and PK comparison of TAF and TDF

Ruane P, et al. JAIDS 2013;63:449-455.
Study GS-US-120-0104M
ed
ian
ch
an
ge
fro
m B
as
eli
ne
H
IV-1
RN
A (
log
10
c/m
L)
0.5
0.0
-0.5
-1.0
-1.5
-2.07 14 21
Placebo (N =7)
TDF 300mg (N =6)
TAF 8mg (N =9)
TAF 25mg (N =8)
TAF 40mg (N =8)
Day
Dosing period

Resistance
• 2 participants on E/C/F/TAF and 4 on E/C/F/TDF had newly detected
genotypic resistance between Weeks 96 and 144
• In participants with genotypic resistance, there was no significant difference
in median baseline VL between E/C/F/TAF and E/C/F/TDF (HIV-RNA
252,200 vs 115,500 copies/mL; p=0.27)
2
4
INSTI, integrase strand transfer inhibitor; VF, virologic failure.
Participants, % (n)
VF With
Resistance
INSTI + NRTI
Resistance
NRTI
Resistance Only
INSTI
Resistance Only
E/C/F/TAF 1.4 (12) 8 4 0
E/C/F/TDF 1.4 (12) 7 4 1
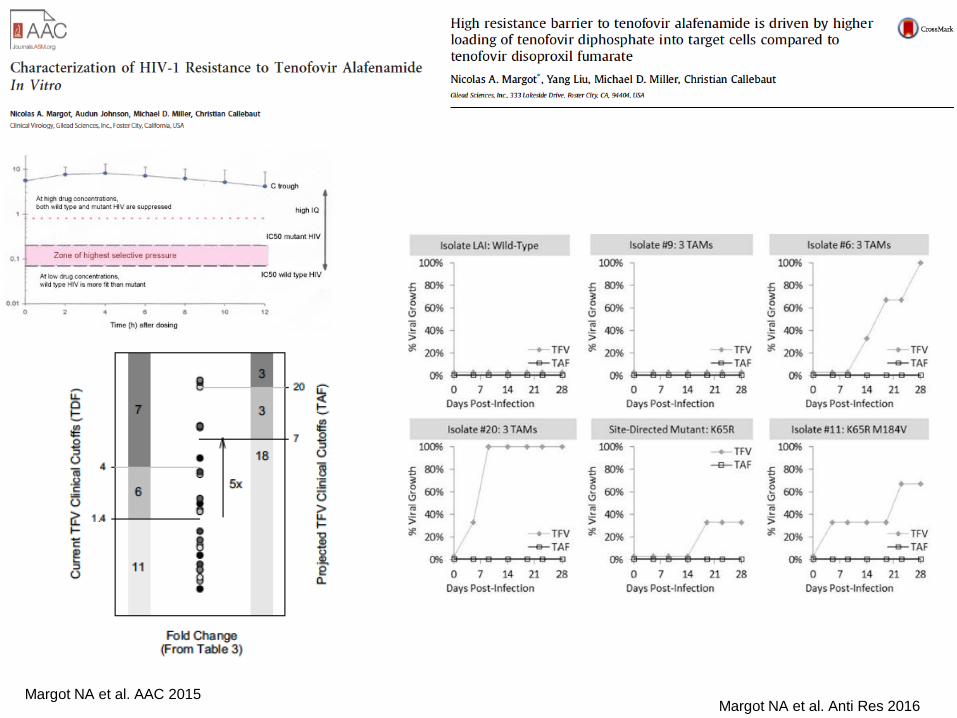
Margot NA et al. Anti Res 2016Margot NA et al. AAC 2015
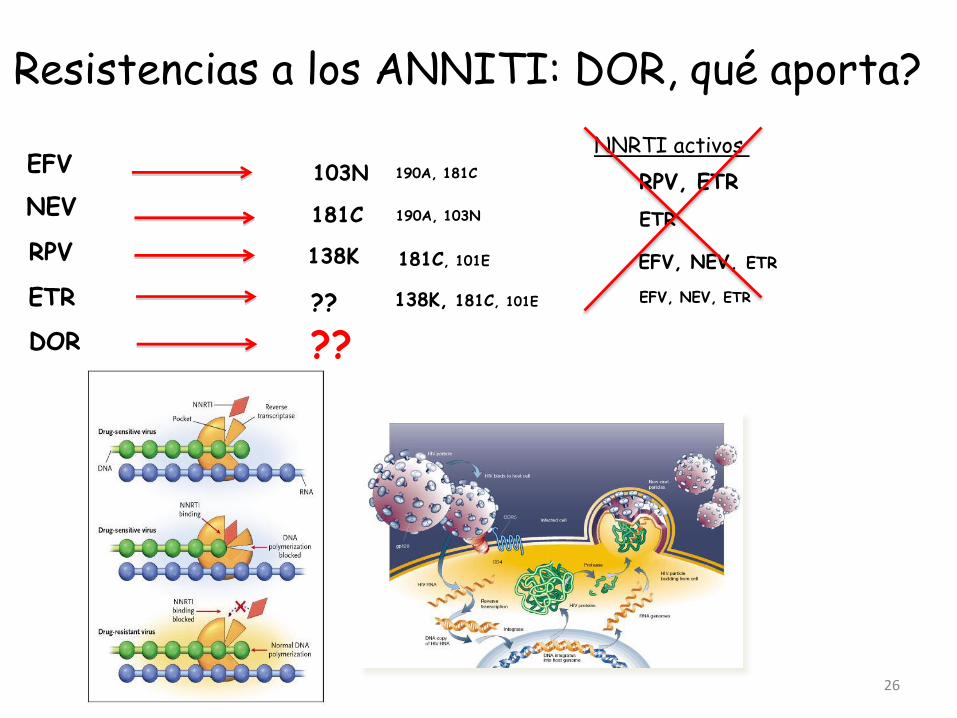
NEV
EFV
RPV
ETR
103N
181C
138K
138K, 181C, 101E??
RPV, ETR
ETR
EFV, NEV, ETR
190A, 181C
190A, 103N
181C, 101E
EFV, NEV, ETR
26
Resistencias a los ANNITI: DOR, qué aporta?
DOR ??
NNRTI activos


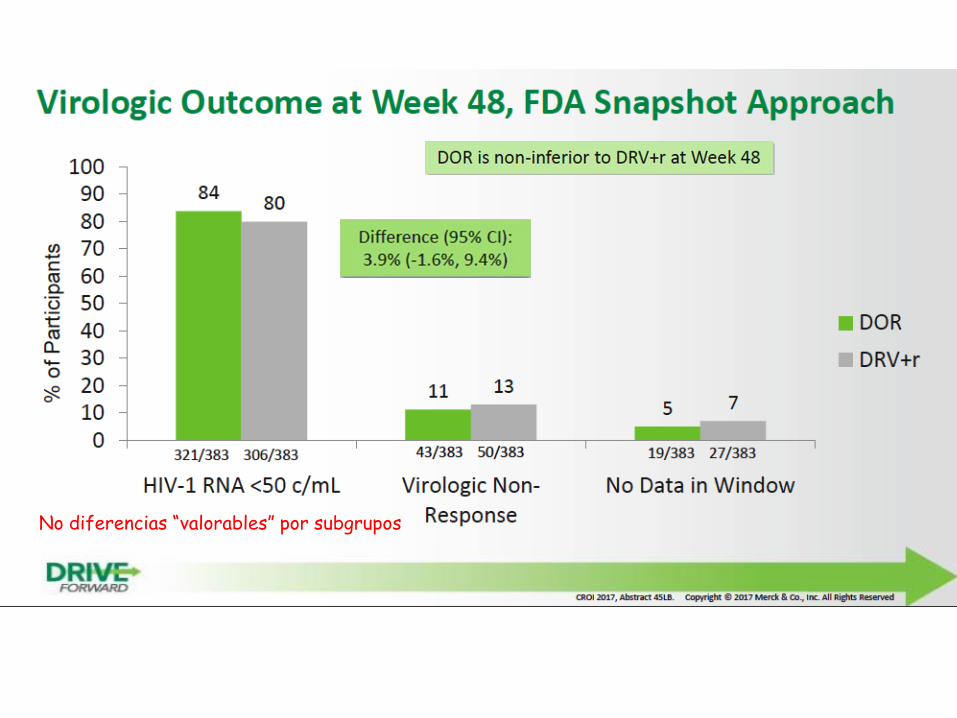
No diferencias “valorables” por subgrupos

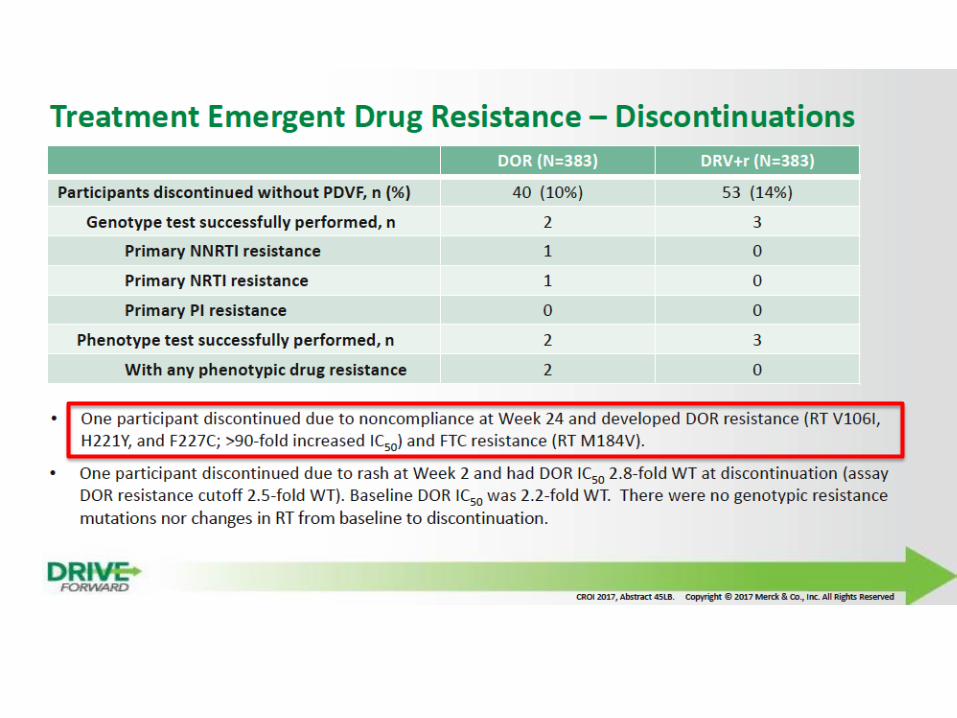
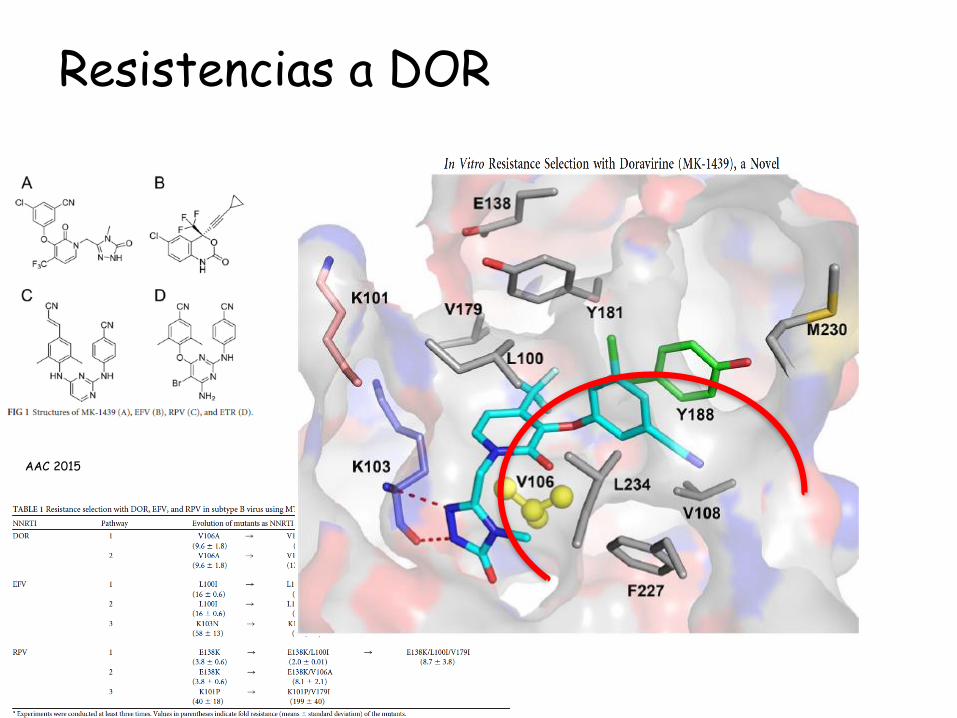
Resistencias a DOR
AAC 2015
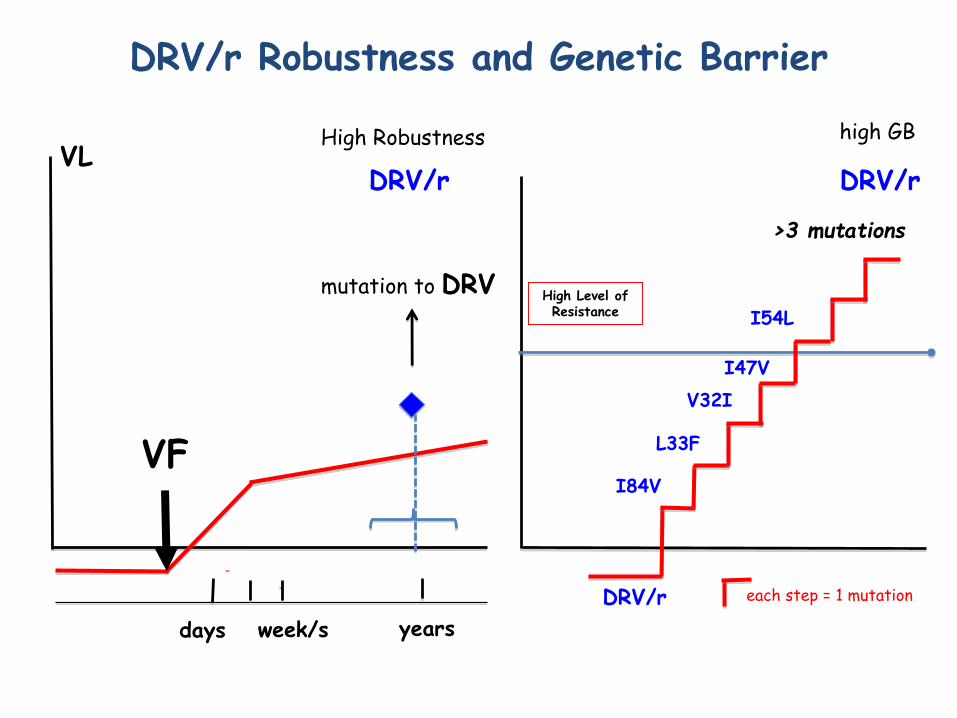
High Level of Resistance
DRV/r Robustness and Genetic Barrier
high GB
each step = 1 mutation
DRV/r
>3 mutations
DRV/r
I84V
L33F
V32I
I47V
I54L
VL
VF
week/sdays years
mutation to DRV
High Robustness
DRV/r

DRV: ratio Cmin/IC50 y t1/2d.
Van Lunzen J. Lancet Infect Dis 2012; 12: 111–18.
DRV/r: t1/2 disociativa: 240 hDRV/r: Cmin/ IC50: 35
Dierynck I, et al. Journal of virol. 2007;81(24):13845-13851

Cahn P, et al. AIDS 2011

Posología de Darunavir/ritonavir
Paciente naïve osin DRV-RAMs
Paciente con DRV-RAMs
800/100 qd 600/100 bid

FC>4 3-4 2-3 <2
50V 54M
76V
84V
32I
33F
47V
74P
11I
54L 89V
De Meyer S. Abst 54. EU DRW. Budapest 2008

Agenda
• Introducción: conceptos básicos
• Test de resistencias: nuevas herramientas
• Resistencias en el paciente naïve
• Resistencias a los ANITI/ANNITI/PI: qué debemos saber
• INIs: datos de resistencias
• Conclusiones

EGV
RAL
DTG
155H (+92Q+74M)
148R/H/K
66I/A/K + 92Q
[2DR/3DR]
148R/H/K
?? 263K /148R/H/K
INSTI Pathways of resistance
Blanco JL, personal comunication
143R/H/C (+92Q+97A)
140A/S (+138A/K)
148R/H/K
148R/H/K 140A/S (+138A/K)
[1DR] All the same than RAL,EGVmainly 148X and others 118R

SECUENCIAR OR NOT SECUENCIAR

De Souza, et al. JAC 2015; Fourati S, et al JAC 2015
32/92= 35%
Is it “correct” sequencing INSTIs?

Resistance to DTG
In vivo :(naïves)
No data yet….
SPRING-21 96 sem SINGLE2 96 sem FLAMINGO3 48 sem
n (%) DTG 50 mg (n=411)
DTG 50 mg +ABC/3TC (n=414)
DTG 50 mg(n=234)
Pacientes con FVDP 20 (5) 18 (4) 2 (<1)
Mutaciones de resistencia a ITIAN 0 0 0
Mutaciones de resistencia a INI 0 0¶ 0a
??

Why these“Robustness”and GB?
PK and Inhibitory Quotient(IQ):
Plasma levels at 24 h post-dose
IC-DTG90
0 5
Time post-dose (hours)
10.0
1.0
DT
G p
lasm
a co
ncent
rati
ons
(µg/
mL)
0.1
10 15 20 25
50 mg QD
PA-IC90 0.064 µg/mL*
19 folds
= 19
DTG disassociation from IN-DNA

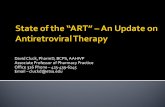
Comprehensive Assessment of Resistance Mutations Selected by Dolutegravir (DTG) in Subjects Failing DTG-Monotherapy after Switching from other Therapies (Redomo
Study)
Blanco JL1, Oldenbuettel C2, Thomas R3, Mallolas J1, Wolf E2,
Brenner BG4,Spinner CD2, Wainberg MA4, Martinez E1
1 Hospital Clinic, Barcelona, Spain. 2 MVZ Karlsplatz, HIV Research and Clinical Care Centre, Munich, Germany. 3 Clinique Actuel, Montreal,
Quebec, Canada. 4 McGill AIDS Centre Montreal, Quebec, Canada

Susceptible ReducedSusceptibility
Resistance
<2.5-fold ≥2.5-10-fold >10-fold
Susceptibility to INSTIs
Q148H/R + G140A/S (n=12)
WT
BIC
DTG
EVG
RAL
143Q148H
G140S
143Q148H
G140S
143Q148R
G140A
143Q148H
G140S
143
143Q148H
G140SQ148H
G140S
Q148H
G140S
143Q148H
G140S
Q148H
G140S
Q148H
G140SQ148R
G140S
Q148R
G140S
14th European Workshop on HIV & Hepatitis. Abstract O-01Poster 497. CROI 2017
Conclusiones• La Barrera a las Resistencias (BR) es una combinación de
“Robusted” y “Barrera genética”
• Los estudios de secuenciación masiva detectan resistencias en poblaciones minoritarias que tenemos que aprender a interpretar.
• Los niveles de TFV intracelular que se alcanzan con TAF incrementan su IQ y conceptualmente su barrera a las resistencias
• Doravirine es un ANNITI con un perfil de resistencias “diferente”
• Darunavir es el IP con mayor BR
• Dolutegravir (DTG) es el INsTI comercializado con mayor BR

Gracias!