Resident Intimidation
30
Resident Intimidation Seemal R. Desai, MD Vice-Chair, AMA-RFS Governing Council Honolulu, Hawaii Interim Meeting
description
Resident Intimidation. Seemal R. Desai, MD Vice-Chair, AMA-RFS Governing Council Honolulu, Hawaii Interim Meeting. Introduction. Overview of Intimidation AMA-RFS recognition of the issue History of graduate medical education Recent changes in GME Is intimidation an issue? - PowerPoint PPT Presentation
Transcript of Resident Intimidation

Resident IntimidationResident Intimidation
Seemal R. Desai, MDVice-Chair, AMA-RFS Governing CouncilHonolulu, HawaiiInterim Meeting

Introduction
• Overview of Intimidation
• AMA-RFS recognition of the issue
• History of graduate medical education
• Recent changes in GME
• Is intimidation an issue?
• Consequences of intimidation
• Proposed solutions

Intimidation
• Definition -- attempt to frighten by acting in a dominating manor with the goal of making people do what the intimidator wants.
• Behavioral trait – present in everyone
• Behavioral theorists suggest it is seen in children as a consequence of being intimidated by others

AMA-RFS
• Section within the AMA
• Approx. 25,000 resident and fellow members
• 76 State and specialty societies
• Annual and Interim Assemblies

AMA-RFS
• Member Connect Survey – • 688 Residents and Fellows responded
• Identified four issues of importance• Medical Liability
• Educational Loan Debt
• Uninsured
• Intimidation
• Over 75% of residents think it is important that the AMA address the issue of intimidation

Member Connect Survey
• Prevalence• Resident members asked if they have
experienced:• Non-physical harm threatened
• Pressure to report work hours inaccurately
• Sexual Harassment
• Physical Harm Threatened
• 25% have had non-physical harm threatened
• 22% have been pressured to report inaccurate duty hours

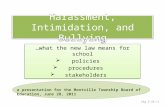
Perpetrators
Who Perpetrated the Intimidation?
42%
53%
34%
20%
72%64%
14%
36%
14%21%
30%
44%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Nonphysical harmthreatened
Pressure to ReportWork HoursIncorrectly
Sexual Harrassment Physical HarmThreatened
Senior Resident/Fellow Attending Other

Member Connect Survey
• Reporting – • 68% of residents believe they would know
how to report intimidation
• 50% responded they would not be comfortable reporting intimidation to their residency program

Reporting
How Comfortable Would You Be in Reporting Intimidation in Your Residency Program?
Very Comfortable29%
Somewhat Comfortable
21%
Somewhat Uncomfortable
27%
Very Uncomfortable
23%

History of Graduate Medical Education
• 1914 – CMEH approved list of hospitals for internship
• 1923 – CMEH approved list for GME
• 1928 – Essentials of Approved Residencies and Fellowships – set standards
• 1953 – RRC was developed
• 1981 – LCGME became the ACGME
• Now 26 RRC’s, TYRC, IRC

Trend in Graduate Medical Education
1914
2006
Standardization of Medical Education
1910
1920
1930
1940
1950
1960
1970
1980
1990
2000

Trend in Graduate Medical Education
1914
2006
Standardization of Medical Education
1910
1920
1930
1940
1950
1960
1970
1980
1990
2000
Learners Teachers
Learners Teachers
Learners Teachers

Trend in Graduate Medical Education
1914
2006
Standardization of Medical Education
1910
1920
1930
1940
1950
1960
1970
1980
1990
2000
Learners Teachers
Learners Teachers
Learners Teachers
Educational Values

Trend in Graduate Medical Education
1914
2006
Standardization of Medical Education
1910
1920
1930
1940
1950
1960
1970
1980
1990
2000
Learners Teachers
Learners Teachers
Learners Teachers
Generation Gap ConflictGeneration Gap Conflict
Educational Values

Sir William Osler
• Father of Medical Education
• Established the sleep-in residency program
• Residencies were open-ended and had a long tenure
• Residents led restricted and almost monastic lifestyle
• System spans the generations
• May now be obsolete

Generations
• Traditionalists
• Baby Boomers
• Generation X
• Generation Y

Generations
• Traditional or Silent Generation 1925-1945• Term was title of Nov 5, 1951 cover of Time
• Raised during the post-war depression
• Faith in institutions, government, business, family, or church
• William Manchester commented: • Withdrawn, cautious, unimaginative, indifferent
• Respect authority
• Subscribe to a top-down model of authority
• Included: Johnny Carson, Sandra Day O’Connor, Clint Eastwood, Neil Armstrong

Generations
• Baby Boomer 1946-1964• Born during economic prosperity post WWII
• First generation that had advanced degrees
• Vietnam War
• Idealistic leaders that succeed by leading in the worst of times
• Political leaders today
• It is estimated that the Boom Generation will hold a plurality in Congress until 2015, the White House until 2021, and will have a majority in the Supreme Court from 2010 to 2030.

Generations
• Generation X 1961-1981• Term popularized by Coupland’s 1991 novel
“Generation X…” described the loss of the icons of the baby boomer generation
• Jane Deverson – coined term in a text where she described this gen. “sleeps together before marriage, don’t believe in God, dislike the Queen, and don’t respect parents”
• Skeptical, raised during recession and downsizing
• More concerned with work-life balance than boomers
• Self driven, learners, skilled individuals

Generations
• Generation Y – 1977-2003• Technology driven
• Tolerant of multiculturalism
• Customizing of everything
• Typically received positive affirmation from parents
• Expect the same affirmation by teachers
• Insist on a work-life balance

Why is there a problem now?
• More Intimidation or Less Tolerance?
• Sentinel Events• ACGME Core Competencies
• 2003 Residency Work Hour Reforms
• Diversification of the workplace
• Is medicine the only industry affected?• Military
• Corporate workplace

Institute for Safe Medication Practices
• Survey published in March, 2004• 2095 staff from different hospitals
• >80% felt mild intimidation
• 48% suffered strong verbal abuse
• 43% experienced threatening body language
• 4% physically abused

Consequences of Intimidation
Patient Care
• Dishonesty• Reporting
• Patient data
• Fear to act
• Congested communication
• Compromises in patient care
• Individual
• Relationship injuries
• Depression
• Fatigue
• Resignation or Transfer
• Perpetuation of cycle

Solutions
• Education
• Identification
• Enforcement

Education
• Education Goals• Diversity Training
• Behavioral Training
• Generation Gap Training
• Forum• Medical School
• Workshops/Seminars
• On-line curriculum

Identification
• Natural History of Reporting• Fear of consequences
• Doubt of anonymity
• Whistleblower
• Monitoring mechanisms• Exit interviews
• Ombudsman program
• Hotline for reporting intimidation

Enforcement
• Benign Enforcement• Resident-Faculty Compact
• Faculty-Resident Compact
• Ombudsman Program
• Punitive Enforcement• Requires identification of a systems problem
• Labor intensive

Summary
• 75% of AMA-RFS members rank intimidation as a top issues for residents
• Generation Gaps create conflict that lends itself to intimidation
• The consequences of intimidation are destructive to education and patient care
• Solutions to intimidation involve a multidirectional approach including: education, identification, and enforcement

Contact Information
Seemal Desai, MDVice-Chair, AMA-RFS Governing Council
The University of Alabama Birmingham