Researchreport 1989 8 Analysis Revised Student Descriptive Questionnaire

doi: 10.2522/ptj.20110310Originally published online June 14, 2012
2012; 92:1278-1291.PHYS THER. B. Cain
JulieHolleran, Miriam R. Rafferty, Kelly S. Rodriguez and T. George Hornby, Catherine R. Kinnaird, Carey L.InjuryStepping in People With Incomplete Spinal CordDuring Exoskeletal-, Elliptical-, or Therapist-Assisted Kinematic, Muscular, and Metabolic Responses
http://ptjournal.apta.org/content/92/10/1278found online at: The online version of this article, along with updated information and services, can be
Online-Only Material 10310.DC1.html
http://ptjournal.apta.org/content/suppl/2012/09/24/ptj.201
Collections
Therapeutic Exercise Spinal Cord Injuries
Kinesiology/Biomechanics Gait Disorders
Gait and Locomotion Training Adaptive/Assistive Devices
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

Kinematic, Muscular, and MetabolicResponses During Exoskeletal-,Elliptical-, or Therapist-AssistedStepping in People With IncompleteSpinal Cord InjuryT. George Hornby, Catherine R. Kinnaird, Carey L. Holleran, Miriam R. Rafferty,Kelly S. Rodriguez, Julie B. Cain
Background. Robotic-assisted locomotor training has demonstrated some effi-cacy in individuals with neurological injury and is slowly gaining clinical acceptance.Both exoskeletal devices, which control individual joint movements, and ellipticaldevices, which control endpoint trajectories, have been utilized with specific patientpopulations and are available commercially. No studies have directly comparedtraining efficacy or patient performance during stepping between devices.
Objective. The purpose of this study was to evaluate kinematic, electromyo-graphic (EMG), and metabolic responses during elliptical- and exoskeletal-assistedstepping in individuals with incomplete spinal cord injury (SCI) compared withtherapist-assisted stepping.
Design. A prospective, cross-sectional, repeated-measures design was used.
Methods. Participants with incomplete SCI (n�11) performed 3 separate boutsof exoskeletal-, elliptical-, or therapist-assisted stepping. Unilateral hip and kneesagittal-plane kinematics, lower-limb EMG recordings, and oxygen consumption werecompared across stepping conditions and with control participants (n�10) duringtreadmill stepping.
Results. Exoskeletal stepping kinematics closely approximated normal gait pat-terns, whereas significantly greater hip and knee flexion postures were observedduring elliptical-assisted stepping. Measures of kinematic variability indicated consis-tent patterns in control participants and during exoskeletal-assisted stepping,whereas therapist- and elliptical-assisted stepping kinematics were more variable.Despite specific differences, EMG patterns generally were similar across steppingconditions in the participants with SCI. In contrast, oxygen consumption was con-sistently greater during therapist-assisted stepping.
Limitations. Limitations included a small sample size, lack of ability to evaluatekinetics during stepping, unilateral EMG recordings, and sagittal-plane kinematics.
Conclusions. Despite specific differences in kinematics and EMG activity, meta-bolic activity was similar during stepping in each robotic device. Understandingpotential differences and similarities in stepping performance with robotic assistancemay be important in delivery of repeated locomotor training using robotic or ther-apist assistance and for consumers of robotic devices.
T.G. Hornby, PT, PhD, Depart-ment of Physical Therapy andDepartment of Kinesiology andNutrition, University of Illinois atChicago, Chicago, Illinois; SensoryMotor Performance Program,Rehabilitation Institute of Chi-cago, Chicago, Illinois; andDepartment of Physical Medicineand Rehabilitation, NorthwesternUniversity Feinberg School ofMedicine, Chicago, Illinois. Mail-ing address: Department of Phys-ical Therapy and Department ofKinesiology and Nutrition, Univer-sity of Illinois at Chicago, 1919 WTaylor St, 4th Floor, M/C 898, Chi-cago, IL 60612 (USA). Address allcorrespondence to Dr Hornby at:[email protected].
C.R. Kinnaird, MS, Sensory MotorPerformance Program, Rehabilita-tion Institute of Chicago.
C.L. Holleran, PT, NCS, SensoryMotor Performance Program,Rehabilitation Institute ofChicago.
M.R. Rafferty, PT, NCS, SensoryMotor Performance Program,Rehabilitation Institute ofChicago.
K.S. Rodriguez, PT, NCS, SensoryMotor Performance Program,Rehabilitation Institute ofChicago.
J.B. Cain, MS, Department ofPhysical Therapy and Departmentof Kinesiology and Nutrition, Uni-versity of Illinois at Chicago, andSensory Motor Performance Pro-gram, Rehabilitation Institute ofChicago.
[Hornby TG, Kinnaird CR, HolleranCL, et al. Kinematic, muscular,and metabolic responses duringexoskeletal-, elliptical-, or therapist-assisted stepping in people withincomplete spinal cord injury.Phys Ther. 2012;92:1278–1291.]
© 2012 American Physical TherapyAssociation
Published Ahead of Print:June 14, 2012
Accepted: June 5, 2012Submitted: September 18, 2011
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
1278 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

Current evidence supports theuse of repetitive, task-specificpractice in patients with neu-
rological injury to improve locomo-tor function. Gait training, or loco-motor training (LT),1,2 provided topatients with neurological injury canimprove walking independence, gaitspeed, timed distance walking, gaitefficiency, maximal aerobic capacity,and daily stepping activity.1–5 Aprimary limitation of providing LToverground is the labor-intensivedemands of safely supporting indi-viduals with substantial lower-extremity weakness and simultane-ously assisting stepping. Use ofmotorized treadmills with counter-weight harness systems may increasethe safety and convenience of LTwhile providing more precise con-trol of body-weight support (BWS)6
and stepping velocity.7 Unfortu-nately, the physical effort requiredby therapists to assist stepping inpatients with minimal volitionalcontrol may limit the amount of LT.8
Despite this required effort, provid-ing kinematic assistance duringtreadmill stepping in patients withreduced volitional control followingstroke or spinal cord injury (SCI) canelicit muscle activity patterns associ-ated with upright walking and mayfacilitate locomotor recovery.9–11
Various motorized, programmable(robotic) devices have been devel-oped to facilitate LT and can be clas-sified into 2 distinct types. Exoskele-tal devices12–14 are secured to thepatient’s limbs or trunk and provideconstant or variable assistance atunilateral or bilateral hip and kneejoints to approximate normal gaitkinematics during treadmill step-ping. Conversely, robotic ellipticaldevices8,15,16 utilize endpoint (foot)control strategies to guide steppingmovements. Selected studies havedemonstrated positive outcomesusing either type of robotic device,although both possess shortcomingsthat may limit their efficacy. For
example, exoskeletal devices canclosely approximate “normal” kine-matics, which may be considered apositive aspect of various rehabilita-tion strategies.14,17,18 However, stabi-lization and physical guidance of thetrunk, pelvis, and lower limbsthrough prescribed movement tra-jectories can minimize movementvariability,19 which is thought to bea critical feature underlying motorlearning.18 Providing such assistancealso may reduce the muscular andmetabolic demands associated withstepping.20 During repeated LT,increased muscle activity appropri-ate for the biomechanical subtasksof walking (eg, limb swing or pro-pulsion) and increased metabolicactivity during LT are thought tobe critical features that facilitateimprovements in walking recovery.Alternatively, these constraints mayaugment specific muscle activity dur-ing portions of the gait cycle whensuch activity would be unwanted.Specifically, selected devices utilizeelastic straps at the forefoot to aiddorsiflexion during limb swing,which may increase plantar pressureand plantar-flexor stretch and con-tribute to increased extensor electro-myograpic (EMG) activity duringswing.20 These combined limitationsin patient performance duringexoskeletal-assisted stepping werepostulated to contribute to thereduced efficacy of repeated LTusing this device compared withtherapist-assisted LT.21
In contrast, elliptical devices repre-sent a control strategy that also couldfacilitate walking improvements,although this strategy may possesssimilar limitations. Consistent withexoskeletal devices, elliptical assis-tance also may reduce volitionalactivity, and continuous plantar pres-sure on the footplates may providestimuli associated with limb loadingduring swing. However, single end-point control of limb movementsrepresents a simpler design, which
could allow more variability of jointkinematics during stepping practiceby minimizing stabilization of thepelvis and lower limbs. Alternatively,the lack of kinematic constraints maylead to abnormal gait kinematics,which has been thought by otherinvestigators to impair restorationof normal walking patterns.8,17,18
Recent data suggest that hip andknee angular excursions of individu-als without neurological injury dur-ing elliptical stepping are slightlyflexed compared with overgroundwalking,22 although this has notbeen established in patients withneurological injury.
Despite the limitations of both loco-motor control strategies, thereduced therapist effort afforded byeither device may increase deliveryof LT in individuals with substantialweakness but emerging recovery ofstrength early following neurologicalinjury. Such training provided soonafter injury may facilitate greatergains in walking function.23 Ques-tions remain as to what control strat-egies optimize locomotor recovery.Previous investigations have focusedon evaluation of patient perfor-mance (ie, gait kinematics, muscle
Available WithThis Article atptjournal.apta.org
• eTable 1: Kinematic Excursionsand Measures of Variability inParticipants Without Neurologicalor Orthopedic Injury and inParticipants With Incomplete SCI
• eTable 2: Muscle ActivityPatterns in Participants WithoutNeurological or Orthopedic Injuryand in Participants WithIncomplete SCI
• eTable 3: Spearman CorrelationCoefficients for SteppingPerformance Variables and LowerExtremity Motor Score forIndividuals With Incomplete SCI
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1279 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

activity patterns, and metabolic costof stepping) with either device com-pared with overground or treadmillstepping.20,22 However, no studieshave compared differences betweendevices in individuals with neurolog-ical impairments (see Regnaux et al24
for a single-subject comparison).3
The primary goals of this study wereto evaluate kinematic, EMG, and met-abolic responses of individuals withincomplete SCI (iSCI) duringtherapist-, exoskeletal-, and elliptical-assisted stepping. Consistent withprevious data,19–21 substantial differ-ences in performance variablesfavoring one stepping condition overanother may provide insight into thepotential efficacy of training para-digms and provide an argument forpreferentially utilizing one methodof assistance. In contrast, if perfor-mance variables are not differentacross stepping conditions, otherfactors such as the number of thera-pists required to provide steppingtraining or the cost of the device mayfacilitate selective utilization of thesedevices in the clinical setting.
In the current study, we hypothe-sized that therapist-assisted steppingwould result in greater metaboliccosts and more appropriate muscleactivation patterns than eitherrobotic LT device, with few differ-ences between devices. We furtheranticipated greater hip and kneeflexion and greater kinematic vari-ability with elliptical-assisted step-ping, although kinematic trajectoriesevaluated during exoskeletal-assistedstepping would mimic those of indi-viduals without neurological injury.Despite these kinematic differences,we anticipated that the metabolicand muscular behaviors would besimilar for each stepping device, butinferior to therapist-assisted steppingas needed. Evaluation of steppingperformance with different roboticdevices may generate hypotheses
about their potential efficacy duringrepeated LT.25
MethodParticipantsPotential research participants withiSCI were recruited from the outpa-tient clinics of the RehabilitationInstitute of Chicago. Individualswere classified by the American Spi-nal Injury Association (ASIA) Impair-ment Scale (AIS)26 as C or D, indicat-ing motor incomplete lesions.Additional inclusion criteria were:participant age between 18 and75 years, history of iSCI �6 months,neurological lesion level higher thanT10, and lower-extremity passive
range of motion (ROM) consistentwith upright human locomotion.Exclusion criteria were: concurrentillness that might limit exercise orwalking performance, includingunhealed decubiti, substantial car-diopulmonary or metabolic disease,history of osteoporosis, active heter-otopic ossification, or other periph-eral or central neurological injury,and inability to tolerate upright posi-tions for 30 minutes. Ten partici-pants without neurological or ortho-pedic injury (5 men and 5 women,age range�25–41 years) also wererecruited to evaluate normative EMGresponses and kinematics duringunassisted treadmill stepping. Each
The Bottom Line
What do we already know about this topic?
Robotic devices have the potential to alleviate the physical labor oftherapists during the gait training of patients with severe motor deficitsfollowing neurological injury. Many robotic devices have been developedand tested; some devices, such as exoskeletal devices, control individualjoint motion, whereas other devices, such as elliptical devices, controlonly the end-point (ie, foot) trajectories. These devices can vary in theircontrol strategies, complexity, and costs; however, no studies havedirectly compared these different types of devices.
What new information does this study offer?
This study provides a physiological rationale for understanding the potentialdifferences between exoskeletal and elliptical devices. It found few differ-ences between the devices in terms of joint kinematics, muscle activitypatterns, and metabolic cost of walking. The physiological basis for use of onedevice versus another, therefore, may not be warranted. Although furtherrandomized trials are forthcoming, the use of the costly and complex exo-skeletal devices might not be necessary, because the end-point control strat-egies of elliptical devices may provide equivalent outcomes.
If you’re a patient or a caregiver, what might thesefindings mean for you?
Although patients with severe motor deficits following neurological injurycould benefit from using either an exoskeletal device or an ellipticaldevice for locomotor training, the lower costs and the simplicity ofelliptical devices mean that these devices may be more common inrehabilitation facilities.
Comparison of Robotic-Assisted Stepping
1280 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

participant provided writteninformed consent prior to the study.
Clinical examination included assess-ment of lower-extremity strengthand walking ability using reliable andvalid outcome measures in thispatient population. Strength wasdetermined using the ASIA LowerExtremity Motor Score (LEMS).27 TheWalking Index for Spinal Cord InjuryII (WISCI II)28 was used to evaluatethe use of braces, assistive devices,and therapist assistance during over-ground walking. If participants withiSCI could ambulate without assis-tance, preferred overground gaitspeed was determined using theGaitMat II (EQ Inc, Chalfont,Pennsylvania).29
Experimental DesignA repeated-measures experimentaldesign was used to assess the biome-chanical and physiological responsesto therapist-assisted treadmill step-ping, robotic exoskeletal stepping,and robotic elliptical stepping inparticipants with iSCI. Comparisonsbetween kinematics and EMG activ-ity of participants without injury dur-ing treadmill stepping and data col-lected in participants with iSCIduring each stepping condition alsowere made.
InstrumentationThe equipment and details of theexperimental setup for therapist-,exoskeletal- and elliptical-assistedstepping have been describedpreviously8,20 (Fig. 1). During all test-ing, participants were secured over amotorized treadmill with a harness-counterweight support system (Wood-way GmbH, Weil am Rhein, Ger-many). Participants were allowed touse the bilateral handrails to maintainpostural stability, although they wereasked to minimize upper-extremityweight bearing.
During therapist-assisted stepping,manual assistance was provided by
up to 2 therapists (1 at each leg) asneeded to advance the limbs duringswing or to provide knee extensionin stance.21 Trunk and pelvic stabili-zation was provided as needed bynylon straps attached to the harnessdirectly above the waist and anteri-orly to the treadmill handrails. Thestraps were removed if patientscould maintain pelvic stability inde-pendently during treadmill stepping.Participants with iSCI were allowedto wear their customary ankle-footorthosis as necessary.
During exoskeletal stepping, partici-pants were positioned in an exoskel-etal robotic orthosis (Lokomat,Hocoma AG, Zurich, Switzerland) asdescribed previously.20 The harnesswas secured to the orthosis at thepelvis and trunk, with lateral andposterior pads limiting pelvic move-ment in all planes. Bilateral hip andknee joints were aligned with theorthotic joint axes, and the devicewas secured to participants withthigh, shank, and waist straps. Fortesting purposes, the knee joint wasaligned slightly anterior to the
robotic knee axis to minimize kneehyperextension. Elastic strapsattached to the orthosis and the par-ticipant’s forefoot were used to assistdorsiflexion during swing. If partici-pants demonstrated sufficient voli-tional dorsiflexion, no elastic strapswere used. Sagittal-plane gait kine-matics similar to upright humanlocomotion were automated by lin-ear actuators at bilateral hip andknee joints programmed to guidesymmetrical stepping patterns timedto the treadmill speed.
Elliptical-assisted stepping was per-formed using the Pedago (Lokohelp,Zlin, Czech Republic), an automated,elliptical training device that issecured to the treadmill frame andoperates in conjunction with thetreadmill.8 A servomotor drives theelliptical device in a fixed trajectory(0.5-m step length), and an encodermatches the speed of the ellipticaldevice movement to the treadmillspeed. Participants’ feet weresecured in long, rigid boots extend-ing below the knee, which wereattached to the levers extending lat-
Figure 1.Experimental setup for kinematic, electromyographic, and metabolic data collectionduring therapist-assisted stepping (A), exoskeletal-assisted stepping (B), and elliptical-assisted stepping (C).
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1281 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

erally from the device. Motion of theankle was constrained, although theboots could rotate about the leversin the sagittal plane. Pelvic and trunksupport was provided as necessaryvia nylon straps attached to the har-ness and treadmill handrails (4 par-ticipants total), similar to therapist-assisted stepping.
Hip and knee kinematics and surfaceEMG recordings were collected onthe left limb in all participants. Jointkinematics were estimated usingelectrogoniometers (Delsys Inc, Bos-ton, Massachusetts) secured acrossthe hip and knee joints and cali-brated (�3 joint angles throughoutthe available ROM) prior to eachtesting condition to account formovement between protocols. Foot-switches (Noraxon USA Inc, Scotts-dale, Arizona) were placed on theforefoot and toes and the hindfoot(minimum of 4 footswitches) to esti-mate the timing of unilateral stanceand swing gait phases. Electromyo-graphic recordings were obtainedfrom the tibialis anterior (TA), soleus(SOL), medial gastrocnemius (MG),vastus lateralis (VL), rectus femoris(RF), and medial hamstring (MH)muscles using adhesive Ag-AgCl elec-trodes (ConMed Corp, Utica, NewYork) and a commercial EMG system(Noraxon USA Inc). The EMG signalswere amplified (10�) and band-passfiltered at 10 to 500 Hz.
Oxygen consumption (V̇O2; mL/kg/min) was determined using a portablemetabolic system (CosMed USA Inc,Chicago, Illinois) calibrated prior totesting using room air and a referencegas mixture (16% oxygen and 5% car-bon dioxide). Metabolic data were col-lected on a breath-by-breath basis andstored for subsequent analysis.
ProcedureAll participants with SCI were famil-iarized to stepping in each device for2 to 4 minutes prior to testing. Rest-ing V̇O2 measurements were col-
lected while sitting for 2 minutesprior to each testing condition. Par-ticipants then were instrumented ineach device with 40% BWS, and 6minutes of continuous stepping wasperformed. Treadmill speed was setat 1.5 kmph (0.42 m/s). This speed isbelow published recommendationsfor LT,1 but was chosen to accom-modate the degree of motor impair-ments and the physical assistancerequired to facilitate continuousstepping for 6 minutes. Furtherexoskeletal- and elliptical-assistedstepping was performed in the pas-sive mode of operation to minimizedifferences across testing condi-tions. Auditory cues using a metro-nome were used to ensure similarcadences (44 steps/min), whichwere fixed in the elliptical device atthis speed. During exoskeletal-assisted stepping, hip and knee kine-matics were adjusted to standard set-tings, with the hip kinematicsreadjusted to ensure cadences simi-lar to those of elliptical-assisted step-ping. Stepping kinematics and EMGdata also were collected on 10 par-ticipants without injury during tread-mill stepping at the same speed andcadence assessed in participantswith iSCI.
Throughout testing, participants withiSCI were provided initial instructionsto generate the maximal effortrequired to perform continuous step-ping. Verbal encouragement was pro-vided throughout testing to maximizeparticipant effort, although no addi-tional feedback was provided. Noadditional therapist assistance wasprovided during elliptical- orexoskeletal-assisted stepping. Aftereach 6-minute bout of walking, partic-ipants rested for �20 minutes.
Data AnalysisKinematic, EMG, and footswitchdata were sampled at 1,000 Hz dur-ing the final 30 seconds of the last 3minutes of each testing bout using acustom-designed MatLab (The Math-
Works Inc, Natick, Massachusetts)program. Footswitch data were uti-lized to estimate stance and swingphases during exoskeletal- andtherapist-assisted stepping on thetreadmill surface. During ellipticaltesting, plantar pressure during theapparent swing phase of the gaitcycle was sufficient to intermittentlyactivate footswitches and could notbe used to detect gait transitions.Instead, gait transitions were esti-mated using hip kinematics. Specifi-cally, during treadmill walking inparticipants without neurologicalinjury, gait transitions are associatedwith a rapid change in hip excursionfrom peak flexion toward extension(swing-stance) and peak extensiontoward flexion (stance-swing).Accordingly, early stance (initial con-tact) was estimated as the transitionfrom peak hip flexion toward exten-sion, and swing initiation was deter-mined as the transition from peakhip extension to flexion.
Primary kinematic measures includedpeak swing-phase hip and knee flex-ion, peak stance-phase hip and kneeextension, and total joint ROM dur-ing stepping. We evaluated intralimbconsistency of the hip-knee kinemat-ics using the average coefficient ofcorrelation (ACC).30,31 The ACC usesa vector coding technique to esti-mate the consistency of sagittal-plane hip-knee angles throughoutthe normalized gait cycle usingangle-angle plots. For each 1% of thegait cycle, the change in hip-kneeangles on the phase plane was rep-resented by a vector, whose lengthand direction were determined usingthe following equations:
(1) li � �xi2 � yi
2
(2) cos�i �xi
li
(3) sin�i �yi
li
Comparison of Robotic-Assisted Stepping
1282 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

where xi and yi are the change in thehip and knee angle from frame i toi�1 and li is the length of that vec-tor. The mean cos� and sin� for agiven frame (percentage of the gaitcycle) over multiple gait cycles thenwere determined. The correlationcoefficient (ai) for each frame wasevaluated by the following equation:
(4) ai � �cos��2
i� sin��
2
i
where cos�� i and sin�� i are the meancos� and sin� for each i frame. Val-ues of ai were used as the measure ofdispersion across gait cycles of thehip and knee angles at each percent-age of the gait cycle. All ai valueswere represented as a single variableby calculating the mean correlationcoefficient (ACC) for all i frames.Perfectly consistent hip-knee trajec-tories across all gait cycles generatean ACC value of 1.0 (no units), andno consistency provides a value of0.0.
Electromyographic signals were fil-tered using a fourth-order recursiveButterworth filter (band-pass30–450 Hz, band-stop 58–62 Hz)and full-wave rectified. Linear enve-lopes of the filtered, rectified EMGsignal were created using a 20-Hzlow-pass filter (fourth-order recur-sive Butterworth). Electromyo-graphic activity was normalized topercentage of the gait cycle. Differ-ences in EMG amplitudes and timingduring stepping conditions weredetermined using a variation of theSpastic Locomotor Disorder Index(SLDI),32 which evaluated timing ofEMG responses relative to normativedata, determined from 10 partici-pants without neurological injury.Normative data were first evaluatedto determine periods of consistentEMG during the gait cycle (“on” peri-ods) versus periods without muscleactivity (“off” periods), with each“on” period provided as a percent-age of the gait cycle: TA: 0%–15%,
65%–100%; MG: 5%–55%; SOL:5%–55%; RF: 0%–25%, 50%–75%,95%–100%; VL: 0%–25%, 50%–75%,95%–100%; MH: 0%–25%, 65%–100%. “On” periods were consistentwith published data,33 with theexception of VL activity during 50%to 75% of the gait cycle (see“Results” section). Using these data,the SLDI was calculated as the ratioof rectified EMG area during the “off”periods for each muscle to the areaduring the “on” periods, wherelower SLDI values indicate normaltiming. Because electrodes were notremoved throughout testing of par-ticipants with iSCI, EMG data during“on” and “off” periods also werecompared among stepping condi-tions. Comparison between partici-pants without injury during treadmillwalking and those with iSCI duringall conditions were limited to SLDIvalues.
Measurements of V̇O2 were averagedacross 1-minute intervals duringeach stepping condition, withsteady-state V̇O2 calculated frommean data over minutes 4 to 6. Base-line metabolic values from quiet sit-ting were subtracted from walkingV̇O2 measurements.
Primary statistical analysis focusedon differences in kinematic, EMG,and metabolic parameters in partici-pants with SCI during each steppingcondition using one-way repeated-measures analyses of variance, withpost hoc Tukey-Kramer tests usedif differences were significant(��.05). In addition, separateunpaired comparisons (t tests) ofkinematics and EMG activity (SDLIonly) were made between partici-pants with iSCI during the differentstepping conditions and participantswithout injury during treadmillstepping.
Secondary analyses focused on asso-ciations between stepping perfor-mance of participants with iSCI in
each robotic device and their clinicalcharacteristics, including LEMS andWISCI scores and duration postin-jury. As LEMS and WISCI scores weresignificantly correlated (Spearmanrho�.91) and associations withLEMS were greater, only correlationswith LEMS are detailed. Further-more, because of the difficulty incomparing absolute metabolic andEMG activity across participants,metabolic and EMG responses (“on”area) during stepping with eithertype of robotic device were normal-ized to (divided by) data collectedduring therapist-assisted stepping. Incontrast, absolute knee and hipangular excursions were utilized andcompared across robotic-assistedstepping conditions. Parametric andnonparametric (Spearman) correla-tion analyses were performed asappropriate. Statistical calculationswere performed using SPSS version15 (SPSS Inc, Chicago, Illinois).
Role of the Funding SourceThe study was funded by the NationalInstitute of Disability and Rehabilita-tion Research (H133N060014). Theelliptical device was provided by themanufacturers for evaluation free ofcharge. Neither source played a rolein study design, data collection andanalysis, or interpretation.
ResultsEleven individuals with iSCI partici-pated in the present study. In 1 par-ticipant, the hip electrogoniometerwas detached during exoskeletalstepping and, in another participant,EMG activity was not collected dur-ing treadmill stepping. Hip kinemat-ics and EMG activity data, therefore,were analyzed from 10 participantswith iSCI, with knee kinematics andV̇O2 data available from all 11 partic-ipants with iSCI. Ten of these partic-ipants had previous experience withtherapist-assisted stepping, 9 hadprevious experience with exoskele-tal stepping, and 4 had previousexperience with elliptical stepping.
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1283 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

Kinematics and EMG activity of theparticipants with iSCI were com-pared against those of 10 partici-pants without injury during treadmillwalking. Clinical characteristics ofthe participants with iSCI are pro-vided in the Table, indicatingreduced overground walking speedswith use of assistive devices or brac-ing or no independent walking abil-ity. Data on use of an ankle-footorthosis and number of therapistsrequired during therapist-assistedstepping also are provided.
Kinematic ParametersGait kinematics collected duringtherapist-, exoskeletal-, and elliptical-assisted stepping in participants withiSCI revealed significant differencesacross testing conditions and com-pared with participants withoutinjury during treadmill stepping.Data from a single participant withiSCI are provided in Figure 2A, alongwith averaged kinematic data for par-ticipants without injury. All kine-matic data are provided in eTable 1(available at ptjournal.apta.org).
Comparison of hip excursionsrevealed more flexed postures in par-
ticipants with iSCI in all steppingconditions compared with partici-pants without injury, with 6.5 to 16degrees (mean range) greater swing-phase flexion and 7.1 to 22 degreesless stance-phase extension. Signifi-cant differences from participantswithout injury were observed in par-ticipants with iSCI only during ellip-tical stepping for peak hip flexionand extension (both P�.03;eTab. 1). Comparisons among partic-ipants with incomplete SCI indicatedthat all hip kinematic variables werestatistically different (Fig. 2C). Posthoc assessments revealed greaterswing-phase hip flexion duringelliptical-assisted versus therapist-assisted versus exoskeletal-assistedstepping and less stance-phaseextension during elliptical-assistedversus exoskeletal-assisted stepping.Hip ROM during stepping also wasgreater during elliptical- andtherapist-assisted stepping versusexoskeletal-assisted stepping.
Knee kinematic data also revealedmore flexed postures in participantswith iSCI during all stepping condi-tions compared with participantswithout injury, with 14 to 21 degrees
increased swing-phase knee flexionand 8.1 to 14 degrees decreasedstance-phase knee extension. Signif-icant differences in knee flexionwere observed between participantswith iSCI and those without injuryacross all stepping conditions,whereas peak knee extension in par-ticipants with iSCI was differentfrom that of participants withoutinjury only during exoskeletal-assisted stepping. Comparisonsamong different stepping conditionsrevealed nonsignificant (�10°) dif-ferences for peak knee flexion andextension (Fig. 2D), although totalknee ROM was greater duringelliptical- versus exoskeletal-assistedstepping.
Evaluation of intralimb kinematicvariability using the ACC alsorevealed differences across steppingconditions and between participantgroups. Single-subject hip-kneeangle-angle plots and grouped dataduring the 3 testing conditions areprovided in Figures 2E and 2F. Aver-age data indicate that the largest ACCvalues occurred during exoskeletal-assisted stepping (eTab. 1) and wereconsistent with ACC values of partic-
Table.Participants’ Clinical Characteristics and Demographics: Age, Level of Injury (LOI), American Spinal Injury Association ImpairmentScale (AIS) Classification, Duration of Injury (DOI), Lower Extremity Motor Score (LEMS), Walking Speed, Walking Index forSpinal Cord Injury-II (WISCI II) Score, Ankle-Foot Orthosis (AFO) Use During Stepping With Therapist Assistance, and Number ofPhysical Therapists Required to Assist During Therapist-Assisted Stepping
ParticipantNo.
Age(y) LOI
AISClassification
DOI(mo) LEMS
WalkingSpeed(m/s)
WISCIII
Score
AFO UseDuring
Stepping
No. of PhysicalTherapistsRequired
1 18 C4–C6 C 20 8 0 Yes 2
2 30 C7 D 44 24 0.24 9 No 1
3 27 C5–C8 C 20 4 0 Yes 2
4 50 C2–C3 D 28 45 0.52 13 No 0
5 31 T3 C 51 18 0.08 9 Yes 1
6 41 T1 C 220 16 6 Yes 2
7 61 T7 C 367 21 0.10 9 Yes 1
8 43 C5 C 84 9 0 Yes 2
9 19 T6–T7 C 25 21 0.16 9 Yes 1
10 47 C5–C6 D 276 42 0.74 19 No 0
11 62 C4 D 80 36 0.50 19 No 0
Comparison of Robotic-Assisted Stepping
1284 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from
ipants without neurological injury.In contrast, ACC values duringtherapist- and elliptical-assisted step-ping were similar to each other butlower than in exoskeletal-assistedstepping. Significant differenceswere observed only betweenexoskeletal- and therapist-assistedstepping.
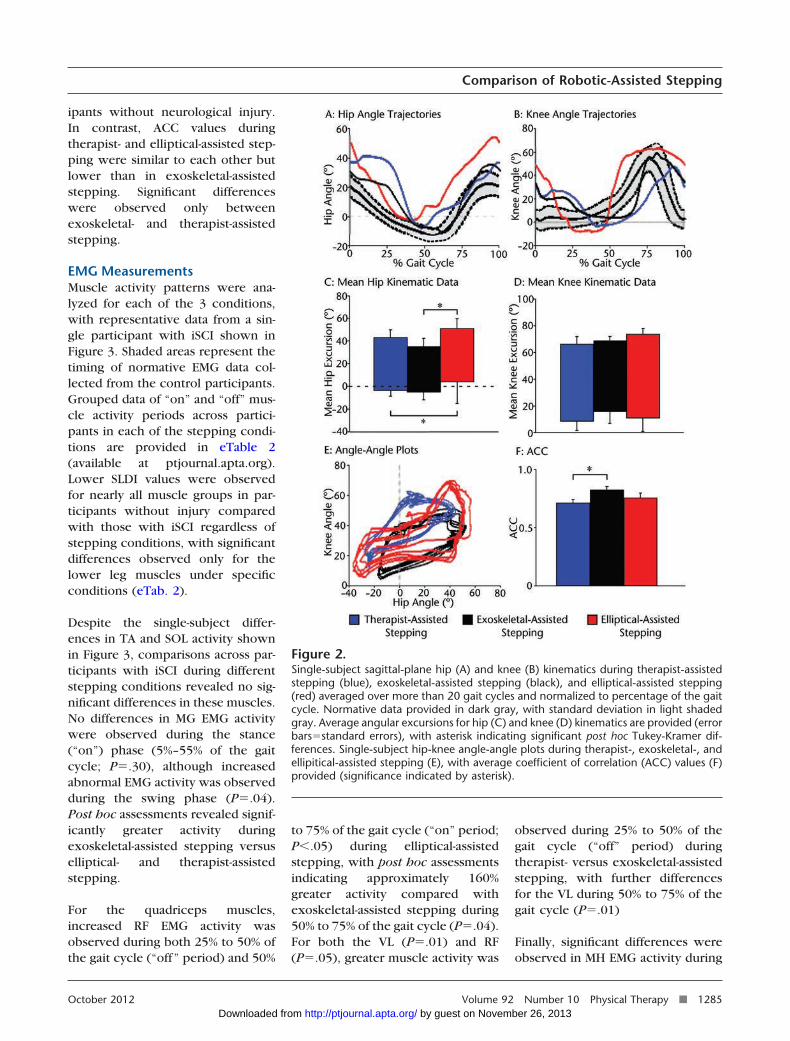
EMG MeasurementsMuscle activity patterns were ana-lyzed for each of the 3 conditions,with representative data from a sin-gle participant with iSCI shown inFigure 3. Shaded areas represent thetiming of normative EMG data col-lected from the control participants.Grouped data of “on” and “off” mus-cle activity periods across partici-pants in each of the stepping condi-tions are provided in eTable 2(available at ptjournal.apta.org).Lower SLDI values were observedfor nearly all muscle groups in par-ticipants without injury comparedwith those with iSCI regardless ofstepping conditions, with significantdifferences observed only for thelower leg muscles under specificconditions (eTab. 2).
Despite the single-subject differ-ences in TA and SOL activity shownin Figure 3, comparisons across par-ticipants with iSCI during differentstepping conditions revealed no sig-nificant differences in these muscles.No differences in MG EMG activitywere observed during the stance(“on”) phase (5%–55% of the gaitcycle; P�.30), although increasedabnormal EMG activity was observedduring the swing phase (P�.04).Post hoc assessments revealed signif-icantly greater activity duringexoskeletal-assisted stepping versuselliptical- and therapist-assistedstepping.
For the quadriceps muscles,increased RF EMG activity wasobserved during both 25% to 50% ofthe gait cycle (“off” period) and 50%
to 75% of the gait cycle (“on” period;P�.05) during elliptical-assistedstepping, with post hoc assessmentsindicating approximately 160%greater activity compared withexoskeletal-assisted stepping during50% to 75% of the gait cycle (P�.04).For both the VL (P�.01) and RF(P�.05), greater muscle activity was
observed during 25% to 50% of thegait cycle (“off” period) duringtherapist- versus exoskeletal-assistedstepping, with further differencesfor the VL during 50% to 75% of thegait cycle (P�.01)
Finally, significant differences wereobserved in MH EMG activity during
Figure 2.Single-subject sagittal-plane hip (A) and knee (B) kinematics during therapist-assistedstepping (blue), exoskeletal-assisted stepping (black), and elliptical-assisted stepping(red) averaged over more than 20 gait cycles and normalized to percentage of the gaitcycle. Normative data provided in dark gray, with standard deviation in light shadedgray. Average angular excursions for hip (C) and knee (D) kinematics are provided (errorbars�standard errors), with asterisk indicating significant post hoc Tukey-Kramer dif-ferences. Single-subject hip-knee angle-angle plots during therapist-, exoskeletal-, andellipitical-assisted stepping (E), with average coefficient of correlation (ACC) values (F)provided (significance indicated by asterisk).
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1285 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

the “on” phase (65%–100% of thegait cycle; P�.01), with post hocanalyses revealing 3-fold greateractivity during exoskeletal- versuselliptical-assisted stepping.
Metabolic ParametersAnalysis of metabolic responses inindividuals with SCI revealed markeddifferences across stepping condi-tions (Fig. 4). Average peak V̇O2
during therapist-assisted steppingwas 19.7% (SD�9.4%) and 19.8%(SD�10.2%) greater than peakV̇O2 observed during elliptical-and exoskeletal-assisted stepping,respectively (P�.01), with no differ-ences between these stepping con-ditions and robotic-assisted stepping.
Association Between SteppingPerformance and ClinicalCharacteristicsPotential associations between clini-cal characteristics (LEMS, durationpost-SCI) and stepping performance(gait kinematics, EMG activity, V̇O2)were determined during robotic-assisted stepping (as normalized totherapist-assisted stepping condi-tion). There were no significant cor-relations between duration post-SCIand any stepping performance vari-able. In contrast, significant correla-tions between LEMS and steppingperformance variables wereobserved, with specific relationshipsprovided in Figure 5 (all coefficientsare shown in eTab. 3, available atptjournal.apta.org). For gait kinemat-ics, LEMS were not well correlatedwith hip kinematics (eg, peak hipflexion versus LEMS; Fig. 5A), withlarger but negative correlation coef-ficients demonstrated for knee kine-matics (eg, peak knee extensionversus LEMS, Fig. 5B). Significant cor-relations, however, were observedonly between LEMS and peak kneeflexion during exoskeletal-assistedstepping.
Positive correlations also wereobserved between LEMS and
Figure 3.Rectified, filtered, single-subject electromyographic (EMG) activity for the (A) tibialisanterior (TA), (B) medial gastrocnemius (MG), (C) soleus (SOL), (D) rectus femoris (RF),(E) vastus lateralis (VL), and (F) medial hamstring (MH) muscles recorded duringtherapist-assisted stepping (blue), exoskeletal-assisted stepping (black), and elliptical-assisted stepping (red). Data were averaged over more than 20 gait cycles and nor-malized to percentage of the gait cycle. Shaded areas indicate periods of normativeEMG activity evaluated in 10 participants without neurological injury.
Figure 4.Grouped averages of oxygen consumption (V̇O2) during each 6-minute bout oftherapist-assisted stepping (blue), exoskeletal-assisted stepping (black), and elliptical-assisted stepping (red). Data were averaged over each minute. Asterisk indicatedsignificant post hoc Tukey-Kramer differences.
Comparison of Robotic-Assisted Stepping
1286 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

selected measures of EMG and met-abolic activity, and relationshipswere significant only during elliptical-assisted stepping conditions. Figure5C demonstrates the moderate cor-relation between LEMS and RF activ-ity (“on” area) during ellipticalstepping, with minimal correlationduring exoskeletal-assisted stepping.Similar findings were observed forthe VL and MG (eTab. 3). Similarly,V̇O2 was significantly related to LEMSfor elliptical-assisted stepping butnot exoskeletal-assisted stepping(Fig. 5D).
DiscussionDirect comparison of the efficacy ofrobotic- and therapist-assisted LTmay provide clinicians with quanti-tative data to help determine whichtraining paradigms may be mostappropriate for their patient popula-tion. In the absence of such data,evaluation of physiological and bio-mechanical variables during step-ping with different devices may pro-vide insight into how patients wouldrespond to such interventions. Previ-ous studies evaluating differences inmetabolic costs and EMG patternsduring therapist- and exoskeletal-assisted stepping provided potentialinsight into how patients with neu-rological injury responded torepeated LT using these paradigms(for example, see Israel et al20).
Differences in KinematicParametersEvaluation of kinematic behaviors inparticipants with iSCI revealed gen-erally increased hip and knee flexioncompared with those of participantswithout injury, although greater hipflexion postures were observed withelliptical-assisted stepping. Thesefindings were anticipated in light of arecent investigation detailing kine-matic behaviors in individuals with-out neurological injury during ellip-tical stepping.22 Using 4 commercialdevices, hip and knee flexion wereincreased approximately 15 and 10
degrees, respectively, during mid-swing compared with overgroundwalking, with smaller differences(�10°) during stance. Although thedegree of hip and knee flexionobserved in participants with iSCI inthe present investigation was greaterthan that observed previously in indi-viduals without neurological injury,greater knee flexion postures may berelated to the reduced volitionalstrength of this patient population(Fig. 5B), regardless of the deviceused.
Differences in kinematic consistency(ACC) across assisted stepping con-ditions also were observed and antic-ipated based on previous data. Inparticular, ACC values observed inparticipants with iSCI duringexoskeletal-assisted stepping, wherekinematics were precisely con-
trolled,34 were high and closelyresembled those of participantswithout neurological injury duringunassisted stepping. Althoughtherapist-assisted stepping may beable to more closely approximatenormal kinematics than demon-strated in this study, selected partic-ipants with iSCI could step withoutsubstantial assistance, and no correc-tions were made by the assistingtherapists to normalize stepping pat-terns. Providing such assistance asneeded to other participants likelyvaried on a step-by-step basis, whichalso could account for the lowerACC values. Elliptical-assisted step-ping also demonstrated substantialvariability in intralimb coordinationsimilar to therapist-assisted condi-tions, where control of endpointkinematics can allow individuals toexplore different hip and knee
Figure 5.Associations between Lower Extremity Motor Score (LEMS) and (A) peak hip flexion(P�.48 for exoskeletal-assisted stepping, P�.65 for elliptical-assisted stepping), (B) peakknee extension (P�.14 for exoskeletal-assisted stepping, P�.11 for elliptical-assistedstepping), (C) rectus femoris muscle (RF) electroyographic (EMG) activity during “on”period (P�.42 for exoskeletal-assisted stepping, P�.01 for elliptical-assisted stepping),and (D) oxygen consumption (V̇O2) (P�.13 for exoskeletal-assisted stepping, P�.02for elliptical-assisted stepping). Black�therapist-assisted stepping minus exoskeletal-assisted stepping, red�therapist-assisted stepping minus elliptical-assisted stepping.
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1287 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

kinematic configurations. The com-bined results suggest substantialvariations between robotic-assistedstepping paradigms dependent onthe control strategy used, with simi-larities between kinematics of theparticipants with iSCI duringexoskeletal-assisted stepping andcontrol participants, and betweentherapist- and elliptical-assisted step-ping conditions.
The practice of kinematically correctmovement patterns during trainingtraditionally has been viewed as adesired strategy of rehabilitationinterventions,8,17,18 which can beprovided by exoskeletal devices.However, previous studies that haveevaluated gait-related changes fol-lowing exoskeletal-assisted LT, par-ticularly those that provided precisecontrol of joint kinematics, indicatedvery few alterations in spatiotempo-ral kinematics21 or joint kinemat-ics,19,35 particularly compared withunconstrained practice or therapist-assistance as needed. Rather, train-ing strategies characterized bygreater variability of movement pat-terns while still approximating nor-mal stepping patterns as performedwith therapist-assisted LT resultedin larger improvements in spatiotem-poral and kinematic consistency(ACC values) and performance19 fol-lowing completion of training.Although there is little knowledgeof what the optimal variability ofstepping would be to facilitate step-ping recovery in patient popula-tions, elliptical-assisted steppingappeared to approximate gait kine-matics and consistency similar tothose observed with therapist-assisted stepping. Despite these sim-ilarities, a concern regarding provid-ing elliptical-assisted stepping maybe the demonstration of increasedhip flexion and reduced extension,which theoretically could be rein-forced during repeated LT with ellip-tical assistance. However, previousLT studies using elliptical devices
have not reported whether suchbehaviors were observed followingtraining.16,36
Differences in EMG ActivitySelective alterations in EMG ampli-tude and timing were observedacross stepping conditions.Increased swing-phase MG activityduring exoskeletal-assisted steppingwas demonstrated (also see Israelet al20), which may be due toincreased plantar pressure andplantar-flexion stretch provided withelastic straps to assist dorsiflex-ion.37,38 However, swing-phase MGactivity was not significantly greaterduring elliptical-assisted steppingdespite presumed continuous plan-tar pressure. The extent of plantarpressure and plantar-flexor stretchpresent during exoskeletal-assistedstepping was not clear in the presentstudy, although future assessment offorces and pressures and of anklekinematics could help elucidate theircontribution to altered MG activity.Conversely, increased MG activitybut not SOL activity may representincreased volitional effort duringswing phase knee flexion, as MHactivity also was increased in theswing phase during exoskeletal-assisted stepping.39 However, kneeflexors typically act eccentricallyduring swing to minimize kneeextension prior to initial contact, andthe increased MH and MG activitymay represent increasing musclestretch with passive knee extension.
For upper leg (thigh) muscles, therealso were selective differences inmuscle activity patterns betweengroups. Quadriceps muscle activitywas significantly different acrossstepping conditions in participantswith SCI in previous studies,20,39
with increased activity in mid-stanceand stance-swing transitions (25%–75% of the gait cycle) duringtherapist- or elliptical-assisted step-ping compared with exoskeletal-assisted stepping. Increased quadri-
ceps muscle EMG activity during25% to 50% of the gait cycle is notnormally observed in participantswithout neurological injury duringunassisted stepping and would gen-erally be considered aberrant muscleactivity. However, increased quadri-ceps muscle activity during elliptical-and therapist-assisted stepping mayhave been necessary to maintainupright (extended) limb postureswithout exoskeletal bracing aboutthe knee. The positive correlationbetween quadriceps muscle EMGactivity and LEMS during ellipticalstepping may indicate increased voli-tional effort to maintain greaterextension for those with sufficientstrength. Regardless, increased quad-riceps muscle activity during stancewas observed in therapist- andelliptical-assisted stepping condi-tions, and increased MG and MHactivity was observed in exoskeletal-assisted stepping during swing.
Differences in MetabolicParametersAlthough V̇O2 is considered a mea-sure of demands on the cardiovascu-lar system to deliver oxygen to work-ing muscles during aerobic tasks,4
evaluation of V̇O2 also provides anestimate of the rate of continuousmuscular activity during these tasks.Previous studies performed on indi-viduals without neurological injurydemonstrated the potential contribu-tions of various biomechanical sub-tasks of upright locomotion to theoverall cost of walking (ie, uprightstance,40 propulsion,41 limb swing,42
lateral stability43) by providing assis-tance for these tasks and simultane-ously investigating the changes inV̇O2 and EMG activity. As evaluationof EMG activity from all muscles sub-serving upright walking is difficult ifnot impossible, evaluation of V̇O2 inthese studies provided a more globalestimate of how biomechanical assis-tance may alter the muscular require-ments of a locomotor task.
Comparison of Robotic-Assisted Stepping
1288 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

In the present study, we believe theobservation of differences in V̇O2
responses of approximately 20% dur-ing therapist- versus either robotic-assisted stepping condition likelyreflected reduced muscle activity.Such differences may have been due,in part, to differences in quadricepsmuscle activity between tasks,although other factors might havecontributed. One explanation maybe the lack of feedback providedduring robotic-assisted stepping, asprevious data indicated nearly equiv-alent V̇O2 between therapist- andexoskeletal-assisted stepping withprovision of external feedback oflower-limb forces.20 Reduced V̇O2
also could be accounted for by thebiomechanical constraints providedduring robotic-assisted stepping,41–43
including the assistance provided bythese devices. Although the precisereasons for the observed differencesare not clear, increased metabolic(ie, aerobic) demands during LThave been considered an importantcomponent of selective LT para-digms.4,44,45 Reducing the metabolicdemands during LT may subse-quently reduce the gains in locomo-tor performance, which was postu-lated to contribute to greaterwalking-related gains followingtherapist- versus exoskeletal-assistedLT in individuals poststroke.21
Given the combined differences andsimilarities in patient performanceduring elliptical- and exoskeletal-assisted stepping, an argument forpreferentially providing assistancewith one type of control strategyor robotic device over the othermay not be warranted. Duringexoskeletal-assisted stepping, hipand knee kinematic trajectories andestimates of consistency (ACC)were very similar to data obtained inparticipants without neurologicalinjury. However, a previous studyhas shown that exoskeletal-assistedLT may not be optimal for induc-ing changes in locomotor perfor-
mance, particularly compared withtherapist-assisted stepping.21 Fur-thermore, the magnitude and timingof EMG activity in selected muscleswere altered substantially duringexoskeletal-assisted stepping ascompared to both therapist- andelliptical-assisted stepping. Forelliptical-assisted stepping, EMGactivity and kinematic consistencywere very similar to those for thetherapist-assisted stepping condi-tion, although the kinematic (hip)trajectories during elliptical-assistedstepping were significantly differentfrom normal gait kinematics. To mit-igate these limitations, specific per-turbations could be provided to bet-ter optimize stepping patterns witheither device. For example, controlalgorithms for providing variablekinematic trajectories duringexoskeletal-assisted stepping couldbe provided. In addition, providingmore BWS and securing the pelvisand trunk more anteriorly duringelliptical-assisted training mayincrease hip extension toward morenormal ranges. Such subtle changesmay improve patient performance ineach device, although the long-termeffects with LT are not clear.
Despite these differences in kinemat-ics and muscular activity, metaboliccosts were similar between robotic-assisted stepping conditions, andboth were significantly less than inthe therapist-assisted stepping condi-tion. However, both devices mini-mize the physical effort on the partof therapists, which may improvedelivery to those with substantialweakness. Providing initial assis-tance with either device may facili-tate early practice of LT, and transi-tioning to therapist-assisted steppingmay be warranted with improve-ments in volitional strength andreduced effort required on the partof the treating therapists. This ratio-nale for providing initial guidanceand gradually reducing assistance aswarranted is consistent with the
guidance hypothesis46 (also Schmidtand Lee47) and may facilitate relearn-ing of independent stepping follow-ing neurological injury.
LimitationsLimitations in the present studyincluded a small sample size, lack ofability to evaluate kinetics or anklekinematics during assisted stepping,and unilateral recordings of EMGactivity and kinematics. In addition,we did not quantify the extent ofupper-extremity support across eachcondition, and handrails were notinstrumented to estimate upper-extremity forces. If participants didrequire some handrail support,attempts were made to ensure con-sistent upper-extremity use acrossstepping conditions. Furthermore,instructions to work as hard as pos-sible have been used in previousassessments of robotic-assisted step-ping performance,20 although indica-tors of exertion or effort were notprovided as feedback to participantsor investigators.
ConclusionThe present article details differ-ences in kinematics, metabolic costs,and muscle activity patterns inparticipants with iSCI duringexoskeletal-, elliptical-, and therapist-assisted stepping. Although the pres-ent discussion and previous find-ings19–21 suggest that therapist-assisted stepping may elicit betterpatient performance and improvedstepping-related outcomes com-pared with exoskeletal-assisted step-ping, specific limitations of eachrobotic device limit the ability toprovide recommendations for eitherdevice over the other. Rather, bothdevices could be considered a “step-ping stone” to eventually transitionto therapist-assisted stepping.
The combined findings, therefore,may provide a preliminary strategyfor progressing LT and may facilitateselection of devices for use in the
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1289 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

clinical setting and their furtherdevelopment. For example, currentcost estimates for available exoskel-etal robotic orthoses start at morethan $200,000, whereas the price ofthe elliptical devices can be muchless (ie, less than $100,000). Differ-ences in cost may be related to thecomplexity of controlling multiplejoint trajectories during steppingversus simpler control of single end-point kinematics. Importantly, provi-sion of additional feedback, assis-tance as needed, and flexibility tovary kinematic trajectories and tread-mill speeds are possible with someof the current LT devices, and thesefeatures may augment patient partic-ipation.48–50 However, such featuresrequire additional costs, and theirefficacy during LT is uncertain.Future studies might focus on iden-tifying which control strategies canbest facilitate stepping performancein patients at varying degrees ofrecovery following neurologicalinjury.
Dr Hornby, Ms Kinnaird, and Ms Rodriguezprovided concept/idea/research design. DrHornby, Ms Kinnaird, and Ms Cain providedwriting. Dr Hornby, Ms Kinnaird, Ms Holle-ran, Ms Rafferty, and Ms Rodriguez provideddata collection and analysis. Dr Hornby, MsKinnaird, and Ms Rafferty provided projectmanagement. Dr Hornby provided fund pro-curement, facilities/equipment, and institu-tional liaisons. Ms Rodriguez provided studyparticipants. Ms Kinnaird provided clericalsupport. Ms Kinnaird, Ms Holleran, and MsRodriguez provided consultation (includingreview of manuscript before submission).
This study was approved by the InstitutionalReview Board of Northwestern University.
The study was funded by the National Insti-tute of Disability and Rehabilitation Research(H133N060014).
DOI: 10.2522/ptj.20110310
References1 Behrman A, Harkema S. Locomotor training
after human spinal cord injury: a series ofcase studies. Phys Ther. 2000;80:688–700.
2 Behrman A, Lawless-Dixon AR, Davis SB,et al. Locomotor training progression andoutcomes after incomplete spinal cordinjury. Phys Ther. 2005;85:1356–1371.
3 Hesse S, Bertelt C, Jahnke MT, et al. Tread-mill training with partial body weight sup-port compared with physiotherapy innonambulatory hemiparetic patients.Stroke. 1995;26:976–981.
4 Macko RF, Ivey FM, Forrester LW, et al.Treadmill exercise rehabilitation improvesambulatory function and cardiovascularfitness in patients with chronic stroke: arandomized, controlled trial. Stroke. 2005;36:2206–2211.
5 Moore JL, Roth EJ, Killian C, Hornby TG.Locomotor training improves daily step-ping activity and gait efficiency in individ-uals poststroke who have reached a “pla-teau” in recovery. Stroke. 2010;41:129–135.
6 Visintin M, Barbeau H, Korner-Bitensky N,Mayo NE. A new approach to retrain gaitin stroke patients through body weightsupport and treadmill stimulation. Stroke.1998;29:1122–1128.
7 Sullivan K, Knowlton BJ, Dobkin BH. Steptraining with body weight support: effectof treadmill speed and practice paradigmson poststroke locomotor recovery. ArchPhys Med Rehabil. 2002;83:683–691.
8 Tyson SF, Connell LA, Busse ME, Lennon S.What is Bobath? A survey of UK strokephysiotherapists’ perceptions of the con-tent of the Bobath concept to treat pos-tural control and mobility problems afterstroke. Disabil Rehabil. 2009;31:448–457.
9 Beres-Jones JA, Harkema SJ. The humanspinal cord interprets velocity-dependentafferent input during stepping. Brain.2004;127:2232–2246.
10 Harkema S, Hurley SL, Patel UK, et al.Human lumbosacral spinal cord interpretsloading during stepping. J Neurophysiol.1997;77:797–811.
11 Maegele M, Muller S, Wernig A, et al.Recruitment of spinal motor pools duringvoluntary movements versus steppingafter human spinal cord injury. J Neu-rotrauma. 2002;19:1217–1229.
12 Colombo G, Joerg M, Schreier R, Dietz V.Treadmill training of paraplegic patientsusing a robotic orthosis. J Rehabil ResDev. 2000;37:693–700.
13 Colombo G, Wirz M, Dietz V. Driven gaitorthosis for improvement of locomotortraining in paraplegic patients. SpinalCord. 2001;39:252–255.
14 Lennon S, Ashburn A, Baxter D. Gait out-come following outpatient physiotherapybased on the Bobath concept in peoplepost stroke. Disabil Rehabil. 2006;28:873–881.
15 Hesse S, Sarkodie-Gyan T, Uhlenbrock D.Development of an advanced mechanisedgait trainer, controlling movement of thecentre of mass, for restoring gait in non-ambulant subjects. Biomed Tech (Berl).1999;44:194–201.
16 Hesse S, Uhlenbrock D, Werner C, Barde-leben A. A mechanized gait trainer forrestoring gait in nonambulatory subjects.Arch Phys Med Rehabil. 2000;81:1158–1161.
17 Bobath B. Adult Hemiplegia: Evaluationand Treatment. 3rd ed. Oxford, UnitedKingdom: Butterworth-Heinemann; 1990.
18 Lennon S, Baxter D, Ashburn A. Physio-therapy based on the Bobath concept instroke rehabilitation: a survey within theUK. Disabil Rehabil. 2001;23:254–262.
19 Lewek MD, Cruz TH, Moore JL, et al.Allowing intralimb kinematic variabilityduring locomotor training poststrokeimproves kinematic consistency: a sub-group analysis from a randomized clinicaltrial. Phys Ther. 2009;89:829–839.
20 Israel JF, Campbell DD, Kahn JH, HornbyTG. Metabolic costs and muscle activitypatterns during robotic- and therapist-assisted treadmill walking in individualswith incomplete spinal cord injury. PhysTher. 2006;86:1466–1478.
21 Hornby TG, Campbell DD, Kahn JH, et al.Enhanced gait-related improvements aftertherapist- versus robotic-assisted locomo-tor training in subjects with chronicstroke: a randomized controlled study.Stroke. 2008;39:1786–1792.
22 Burnfield JM, Shu Y, Buster T, Taylor A.Similarity of joint kinematics and muscledemands between elliptical training andwalking: implications for practice. PhysTher. 2010;90:289–305.
23 Horn SD, DeJong G, Smout RJ, et al. Strokerehabilitation patients, practice, and out-comes: is earlier and more aggressive ther-apy better? Arch Phys Med Rehabil. 2005;86:S101–S114.
24 Regnaux JP, Saremi K, Marehbian J, et al.An accelerometry-based comparison of 2robotic assistive devices for treadmill train-ing of gait. Neurorehabil Neural Repair.2008;22:348–354.
25 Israel JF, Hornby TG. Physiologicalresponses of individuals with incompletespinal cord injury during robotic-assistedtreadmill walking. Presented at: CombinedSections Meeting of the American PhysicalTherapy Association; February 2–6, 2006;San Diego, California.
26 Consortium for Spinal Cord Injury Medi-cine. Outcomes Following Traumatic Spi-nal Cord Injury: Clinical Practice Guide-lines for Health-Care Professionals.Washington, DC: Paralyzed Veterans ofAmerica; 1999.
27 El Masry WS, Tsubo M, Katoh S, et al. Val-idation of the American Spinal Injury Asso-ciation (ASIA) motor score and the NationalAcute Spinal Cord Injury Study (NASCIS)motor score. Spine. 1996;21:614–619.
28 Dittuno PL, Dittuno JF Jr. Walking Indexfor Spinal Cord Injury (WISCI II): scalerevision. Spinal Cord. 2001;39:654–656.
29 Pomeroy VM, Chambers SH, Giakas G,Bland M. Reliability of measurement oftempo-spatial parameters of gait afterstroke using GaitMat II. Clin Rehabil.2004;18:222–227.
30 Daly JJ, Roenigk KL, Butler KM, et al.Response of sagittal plane gait kinematicsto weight-supported treadmill training andfunctional neuromuscular stimulation fol-lowing stroke. J Rehabil Res Dev. 2004;41:807–820.
31 Field-Fote E. Spinal cord stimulation facil-itates functional walking in a chronic,incomplete spinal cord injured subject.Spinal Cord. 2002;40:428.
Comparison of Robotic-Assisted Stepping
1290 f Physical Therapy Volume 92 Number 10 October 2012 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

32 Fung J, Barbeau H. A dynamic EMG profileindex to quantify muscular activation dis-order in spastic paretic gait. Electroencepha-logr Clin Neurophysiol. 1989;73:233–244.
33 Perry J. Gait Analysis: Normal and Path-ological Function. Thorofare, NJ: SlackInc; 1992.
34 Hidler J, Wisman W, Neckel N. Kinematictrajectories while walking within theLokomat robotic gait-orthosis. Clin Bio-mech (Bristol, Avon). 2008;23:1251–1259.
35 Hornby TG, Campbell DD, Zemon DH,Kahn JH. Clinical and quantitative evalua-tion of robotic-assisted treadmill walkingto retrain ambulation following spinalcord injury. Top Spinal Cord Inj Rehabil.2005;11:1–17.
36 Pohl M, Werner C, Holzgraefe M, et al.Repetitive locomotor training and physio-therapy improve walking and basic activi-ties of daily living after stroke: a single-blind, randomized multicentre trial(DEutsche GAngtrainerStudie, DEGAS).Clin Rehabil. 2007;21:17–27.
37 Conway BA, Hultborn H, Kiehn O. Propri-oceptive input resets central locomotorrhythm in the spinal cat. Exp Brain Res.1987;68:643–656.
38 Pearson K, Collins DF. Reversal of theinfluence of group Ib afferents from plan-taris on activity in medial gastrocnemiusmuscle during locomotor activity. J Neu-rophysiol. 1993;70:1009–1017.
39 Hidler JM, Wall AE. Alterations in muscleactivation patterns during robotic-assistedwalking. Clin Biomech (Bristol, Avon).2005;20:184–193.
40 Grabowski A, Farley CT, Kram R. Indepen-dent metabolic costs of supporting bodyweight and accelerating body mass duringwalking. J Appl Physiol. 2005;98:579–583.
41 Gottschall J, Kram R. Energy cost and mus-cular activity required for propulsion dur-ing walking. J Appl Physiol. 2003;94:1766–1772.
42 Gottschall J, Kram R. Energy cost and mus-cular activity required for leg swing duringwalking. J Appl Physiol. 2005;99:23–20.
43 Donelan JM, Shipman DW, Kram R, KuoAD. Mechanical and metabolic require-ments for active lateral stabilization inhuman walking. J Biomech. 2004;37:827–835.
44 Macko RF, DeSouza CA, Tretter LD, et al.Treadmill aerobic exercise trainingreduces the energy expenditure and car-diovascular demands of hemiparetic gaitin chronic stroke patients. A preliminaryreport. Stroke. 1997;28:326–330.
45 Macko RF, Smith GV, Dobrovolny CL, et al.Treadmill training improves fitness reservein chronic stroke patients. Arch Phys MedRehabil. 2001;82:879–884.
46 Winstein CJ, Pohl PS, Lewthwaite R.Effects of physical guidance and knowl-edge of results on motor learning: supportfor the guidance hypothesis. Res Q ExercSport. 1994;65:316–323.
47 Schmidt R, Lee T. Motor Control andLearning: A Behavioral Emphasis. 3rded. Champaign, IL: Human Kinetics Inc;1999.
48 Brutsch K, Koenig A, Zimmerli L, et al.Virtual reality for enhancement of robot-assisted gait training in children with cen-tral gait disorders. J Rehabil Med. 2011;43:493–499.
49 Koenig A, Omlin X, Bergmann J, et al. Con-trolling patient participation during robot-assisted gait training. J Neuroeng Rehabil.2011;8:14.
50 Koritnik T, Koenig A, Bajd T, Riener R,Munih M. Comparison of visual and hapticfeedback during training of lower extrem-ities. Gait Posture. 2010;32:540–546.
Comparison of Robotic-Assisted Stepping
October 2012 Volume 92 Number 10 Physical Therapy f 1291 by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from

doi: 10.2522/ptj.20110310Originally published online June 14, 2012
2012; 92:1278-1291.PHYS THER. B. Cain
JulieHolleran, Miriam R. Rafferty, Kelly S. Rodriguez and T. George Hornby, Catherine R. Kinnaird, Carey L.InjuryStepping in People With Incomplete Spinal CordDuring Exoskeletal-, Elliptical-, or Therapist-Assisted Kinematic, Muscular, and Metabolic Responses
References
http://ptjournal.apta.org/content/92/10/1278#BIBLfor free at: This article cites 45 articles, 20 of which you can access
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on November 26, 2013http://ptjournal.apta.org/Downloaded from