RESEARCH UPDATE IN PHENYLKETONURIA Dr. Maureen Cleary Great Ormond Street Hospital NHS Trust.
55
RESEARCH UPDATE IN PHENYLKETONURIA Dr. Maureen Cleary Great Ormond Street Hospital NHS Trust
-
Upload
savanah-harler -
Category
Documents
-
view
222 -
download
0
Transcript of RESEARCH UPDATE IN PHENYLKETONURIA Dr. Maureen Cleary Great Ormond Street Hospital NHS Trust.

RESEARCH UPDATE IN PHENYLKETONURIA
Dr. Maureen Cleary
Great Ormond Street Hospital NHS Trust
Blood-brain barrier studies in PKU
• Blood-brain barrier studies in PKU
• Large Neutral amino acids
• Essential fatty acids supplementation
• Biopterin treatment
• Ammonia lyase
• Gene therapy

Blood-brain barrier studies

Phenylketonuria
• Monitor metabolic control by blood phe
• Preferable to measure phe at site of action (brain) rather than point of delivery (blood)

1H-Magnetic Resonance Spectroscopy
• Nucleus is magnetic– Magnetic field causes all the magnetic nuclei to align
themselves to the major axis of the field
• A second magnetic field is applied– Nuclei tilted to a specific angle
• When field removed they re-align themselves to the major axis of the magnetic field
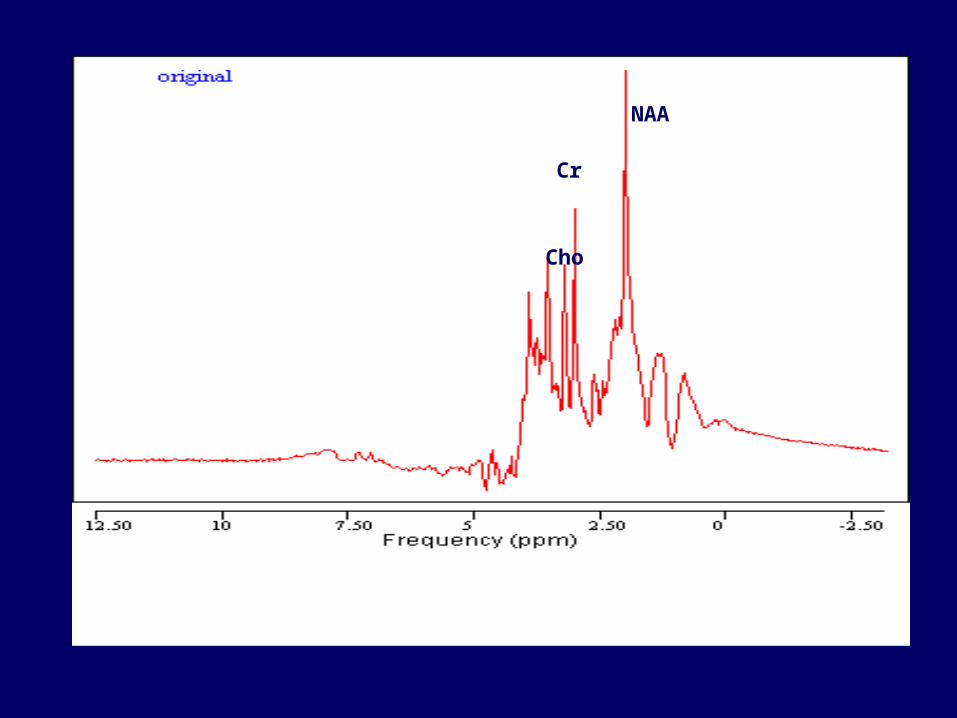
Magnetic Resonance Spectroscopy
• capable of identifying different molecules
• Same nuclei eg protons experience different local magnetic fields
• Give rise to different MR spectra
• Area under peak proportional to concentration

NAA
Cr
Cho

1H-Magnetic Resonance Spectroscopy in PKU
• Non-invasive assessment of changes in brain metabolism
• Initial reports measure N-Acetyl-Aspartate, NA Choline, inositol, creatinine
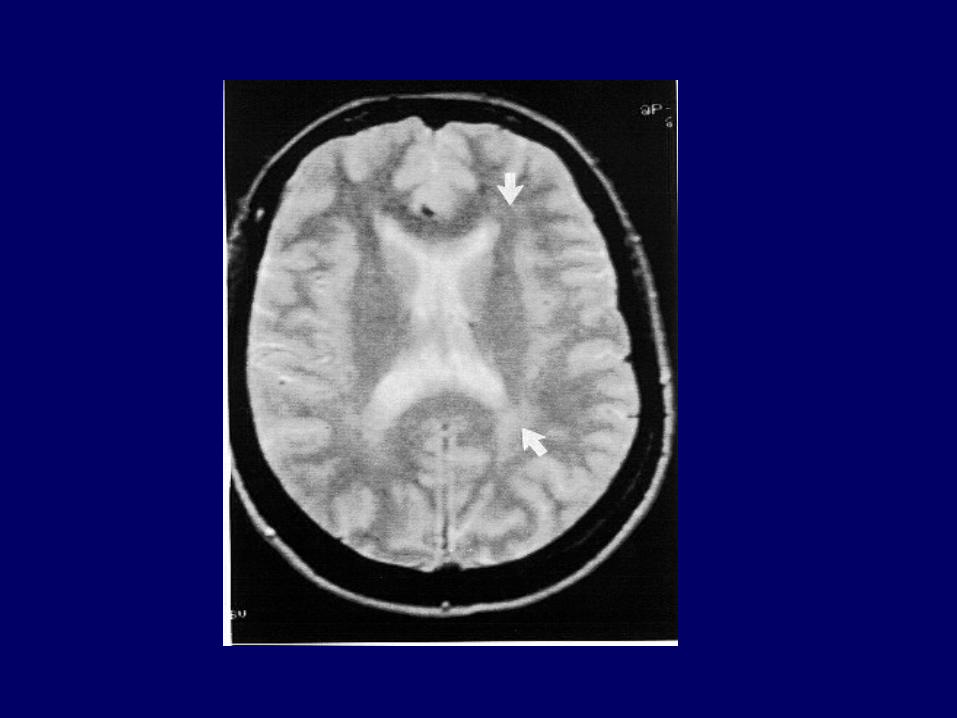

1H-Magnetic Resonance Spectroscopy in PKU
• Normal NAA, choline, creatinine
• Suggests no demyelination

PKU and Magnetic Resonance Spectroscopy (MRS)
• Rabbit made hyperphe
• MRS detected ‘phe’ peak
• Intensity correlated with brain phe on postmortem
• Correlated poorly with plasma phe

MRS and brain phe
• 1995
– Detection and quantitation methodology of brain metabolites in patients with PKU
NAA
Cr
Cho
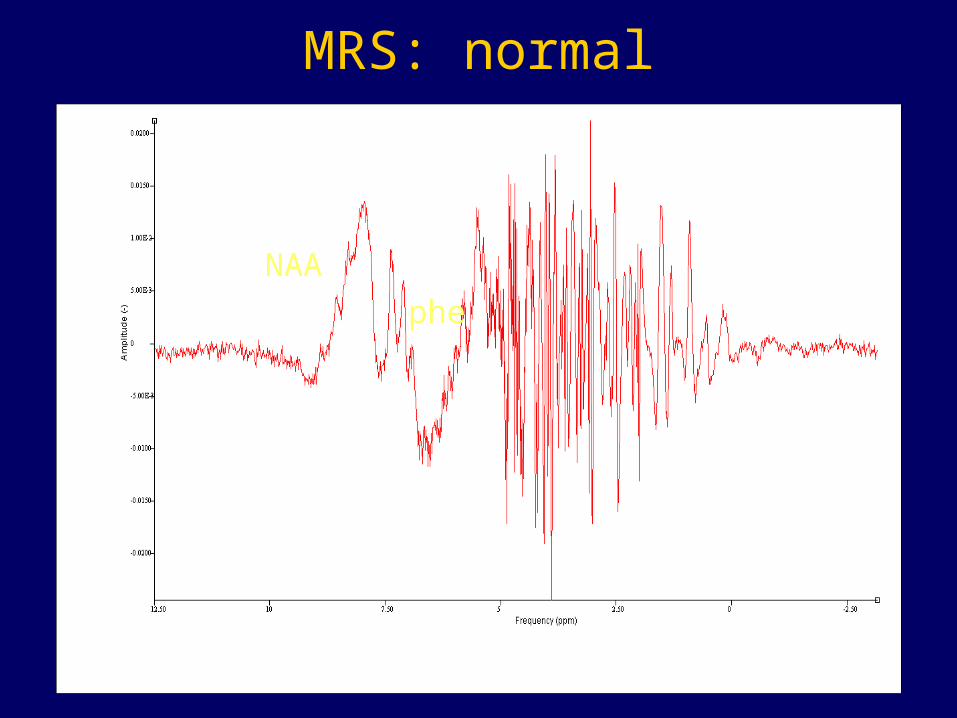
MRS: normal
phe
NAA

MRS: PKU
NAAphe

Measurement of phe
• Present in relatively small quantities– Cf NAA, choline
– Need to use ‘difference spectroscopy’
– i.e. subtract spectra from non PKU controls

MRS of brain phe studies in PKU
• 17 PKU (mean age 25.8 yrs)
• 10 healthy controls (25.3)
• Early treated
• 6 off diet, 3 protein restricted, 8 on aa supp
• (stopped 2 weeks pre-scan)
• ‘steady state’» (Rupp et al., 2001)

MRS results
• Control brain phe mean 0.05, sd 0.025
• Blood versus brain linear relationship
• Blood to brain phe: 4:1
• Measurement error 0.03mol/kg ww

Blood- brain relationship
Pietz et al.,(1999)

Magnetic Resonance Spectroscopy
Weglage et al., 1998• two siblings aged 17 and 30 yrs early treated• R408W/R408W• IQ’s 90 and 77• oral load phe
• max brain phe 12-23 hrs post phe load• sib I blood 2448: brain 642 (IQ 90)• sib II blood 2316: brain 804 (IQ 77)

Magnetic Resonance Spectroscopy
Weglage et al., 1998• 4 untreated adults• two IQ unobtainable ages 34 and 28 yrs• blood 1320,1211/ brain 650,670
• two IQ 100 and 105 ages 33 and 31 yrs• blood 1200, 1210/ brain <200, <200
• Suggests– Intervariability of brain phe
– Explains different outcomes
• Only really explains unusual patients
MRS blood:brain
• Pietz et al., (1999)– linear blood: brain 4:1
• Moller et al.,(2000)– saturated at higher phe levels
• Moats et al. (2000)– ?? exponential

Blood-brain relationships
Pietz et al.,(1999) Moller et al.,(2000)
Moats et al., (2000)
Large Neutral amino acids

LNAA and PKU
• Large neutral amino acids compete for entry to brain with phenylalanine

Large neutral amino acids and PKU
• Administer large quantities of LNAA and reduce phe entry to the brain
Large Neutral AminoAcids and PKU
• What is the evidence that it should work?
– Earlier studies (animals or functional testing)
– Later studies (humans) using Magnetic Resonance Spectroscopy

LNAA and PKU
• Cerebral protein synthesis reduced in hyperphe state in rats
• Improves upon supplementing with LNAA– Binek-Singer & Johnson, 1982
LNAA and PKU: effect of supplements on brain amino acids in animals
• Rats phe hydroxylase inhibited– Phe load– Phe load + LNAA
– LNAA group had lower brain phe and similar blood phe
• Andersen & Avins, 1976

LNAA and cerebral function in PKU
• Valine, isoleucine and leucine supplements– Reduced brain and CSF phe in rats
• Six patients with pku improved neuropsych performance whilst taking VIL– Berry et al., 1985

LNAA, PKU and MRS
• Later studies using MRS in humans
• One study
• Pietz et al., (1999)– Six adults – Loading with oral phe 100mg/kg– Loading with oral phe plus LNAA– EEG testing

LNAA, PKU and MRS: Pietz et al. (1999)
• Rise in brain phe occurred after loading
• This rise blocked when LNAA taken with phe load
• EEG spectra abnormalities not seen when LNAA ingested

LNAA study• Brain phe after oral phe load
– mean preload 252– mean post load 6 hrs 344– mean post load 12 hrs 377
• Brain phe after oral phe + LNAA– mean preload 226– mean post load 6 hrs 235– mean post load 12 hrs 210

Further considerations
• Is MRS sufficiently robust tool for intervention studies?
• What are the relationships between BB phe entry and actual brain tissue phe levels?
LNAA, MRS and MOUSE
• PAHENU-2 mouse model – 0.5g/kg or 1.0 g/kg PreKUnil– Reduction in blood phe and brain phe
– Spectroscopy on homogenized mouse brain– BCAT activity increased on LNAA
• (only two mice in each group)
• Matalon et al, (2003)

Conclusions
• MRS can define a peak which is markedly elevated in individuals with PKU compared to normal spectra
• MRS can show reduction in this peak when interventions occur such as LNAA application
• MRS can show some unusual individuals who have low brain phe and are ‘protected’

Conclusions
• Blood:brain barrier relationship not clear
• Extent of inter-individual variability not clear
• Safety of long term LNAA not proven
• To use the technique in dynamic studies need clarity of these changes through the day

Essential fatty acids in PKU

Essential fatty acids in PKU• Diet low in animal protein
– low intake alpha-linolenic acid– low docoshexanoic acid– importance in brain cell membrane
• Infant aminoacid formulae can be supplemented with PUFA’s
• Should children’s formulae also be supplemented?

Essential fatty acids in PKU
• AA product supplemented with fatty acids
• Children had higher levels of DHA than unsupplemented group
• Considered more palatable than unsupplemented formula
PKU and biopterin
PKU
• Phenylalanine Tyrosine
Biopterin metabolism

Biopterin responsive PKU
• Should we be treating some patients with biopterin?

Role of biopterin in PKU
• Biopterin co-factor for phe hydroxylase
• Inborn errors of biopterin detected by PKU screening programme
• On biopterin those patient usually no longer need phe restriction

Biopterin in PKU
• Recent observation that biopterin may benefit phe hydroxylase deficient patients

Biopterin in PKU
• Hyperphe rather than classical PKU• Mutations with residual activity• Frequently (but not exclusively) missense
mutations within the coding region for the catalytic domain


Biopterin and PKU
• Suggest loading test in all patients
• However newborn failed loading test patients have subsequently been found to be responsive

Biopterin and pku
• Cost of diet v. cost of biopterin
• Who would benefit?
• Does it benefit those with severe PKU?
• Is it safe in pregnancy?
• Trial later this year 2004

Alternative therapies
• Ammonia lyase therapy
• Recombinant phenylalanine ammonia lyase
• converts phe to trans-cinnamic acid in the gut
• reduces plasma phe by approx 50% in PKU mouse

New therapies
• Ammonia lyase treatment– may be useful– needs further studies to test safety– may still need some diet– may be many years before available

PKU and Gene therapy

Alternative therapies
• GENE THERAPY– Adv/RSV-hPAH infused into portal vein of
PAHenu2 mice– phe levels normalised with sufficient dose– comparable to 10-20% enzyme activity– successful only in short term– could not be duplicated due to immune
response to vector

Conclusions
• Research is fairly active in PKU
• Biopterin trial will find some individuals with milder PKU who may benefit form Biopterin treatment
• Enzyme treatment is underway