Research on lifestyles and health: Searching for meaning
11
~ ) Pergamon 0277-9536(94)00410-2 Soc. Sci. Med. Vol.41, No. 6, pp. 845--855,1995 ElsevierScience Ltd. Printedin Great Britain RESEARCH ON LIFESTYLES AND HEALTH: SEARCHING FOR MEANING KATHRYN DEAN, 1"2 CONCHA COLOMER 2 and SANTIAGO PI~REZ-HOYOS2 IResearch and Training, Population Health Studies, DK-2100 Copenhagen, Denmark and 2Val6ncia Institute of Public Health, Val6ncia, Spain A~tract--This paper is based on an alternative approach to standard quantitative analyses in research on behavior and health. Theory and methods focused on the elaboration of complex situational and behavioral influences on health are used in secondary analyses of data from a population health survey in Spain. Findings showing fundamental differences in the relationships among the behavioral and health variables within various age, gender and social groups illustrate the importance of studying interacting influencesin relevant subgroups of the population. Quite meaningful findingscan be hidden in behavioral research limited to identifying global statistical correlations in cross-sectional and longitudinal data. The impact that statistical methods can have on the findingsfrom analyses that are not guided by theory and logic based on substantive questions derived from the research literature is discussed. The results point to the need to study patterns of behavior in their contexts of occurrencein research on lifestyles and health. In recent years a multitude of investigations have examined behavioral habits of individuals in relation to different health outcomes. This paper discusses this body of research and presents results from a popu- lation health study that illustrate the need to rethink standard approaches to analyzing data. We argue that new approaches to research on health related behavior are needed for building knowledge in the field. It has become customary in research on behavioral habits to focus on specific behaviors that have been statistically associated with morbidity or mortality in population health data. A limited number of behaviors are studied in what is loosely labelled lifestyle research. Tobacco or alcohol consumption, physical exercise and/or dietary practices are studied almost exclusively in this research tradition. These behaviors are examined statistically against a wide array of self-reported measures of morbidity or register data on disease specific or total mortality. Huge bodies of research literature have grown up around these four behaviors. Statistical correlations found are often inconsistent or even directly contra- dictory. Investigations relating the same behavior statistically to the same outcome may find a signifi- cant statistical effect in one study and no effect in another, or even effects in opposite directions for the same factor [1]. The data on diet and CVD illustrate the problems. Because of correlations found between blood choles- terol and CVD, diets high in saturated fat have been especially targeted in behavioral research and pro- grams. It is now known that the global statistical correlations hide serious contradictions like the high coronary disease rates of Asian immigrants to Britain in spite of lower blood cholesterol, blood pressure and tobacco consumption than the non-immigrant British population [2]. There is evidence that among women high blood cholesterol is not statistically associated with mor- tality, not even cardiovascular disease mortality [3]. Other findings contradicting the saturated fat/high cholesterol hypothesis include, the relatively low rates of CVD in some countries (e.g. France) despite relatively high content of saturated fat in the diet and the findings in some cohort and case control studies that fruit, vegetable or cereal consumption is negatively related to CVD with no link found for saturated fatty acid [4]. After years of population interventions and health education seeking to lower blood cholesterol levels in general populations without consideration of the contradictions in the evidence, a U-shaped association between level of blood cholesterol and subsequent mortality is now receiving greater atten- tion [5]. On the one hand, high blood cholesterol is related to higher risk of death from coronary heart disease (for men), but at the same time there is a higher risk of death from noncoronary heart disease causes with lower levels of blood cholesterol. This means that not only have extensive population financial resources been used for misleading health education and services, but that for many people, especially women, the advice may have been danger- ous, increasing their risk for other health problems. The U-shaped curve illustrates methodological prob- lems and limitations in both the paradigm of risk factor etiology underlying this type of research, and in the approaches to statistical analysis that have dominated this research tradition [6]. 845
-
Upload
kathryn-dean -
Category
Documents
-
view
212 -
download
0
Transcript of Research on lifestyles and health: Searching for meaning

~ ) Pergamon 0277-9536(94)00410-2 Soc. Sci. Med. Vol. 41, No. 6, pp. 845--855, 1995
Elsevier Science Ltd. Printed in Great Britain
RESEARCH ON LIFESTYLES AND HEALTH: SEARCHING FOR MEANING
KATHRYN DEAN, 1"2 CONCHA COLOMER 2 and SANTIAGO PI~REZ-HOYOS 2 IResearch and Training, Population Health Studies, DK-2100 Copenhagen, Denmark and
2Val6ncia Institute of Public Health, Val6ncia, Spain
A~tract--This paper is based on an alternative approach to standard quantitative analyses in research on behavior and health. Theory and methods focused on the elaboration of complex situational and behavioral influences on health are used in secondary analyses of data from a population health survey in Spain.
Findings showing fundamental differences in the relationships among the behavioral and health variables within various age, gender and social groups illustrate the importance of studying interacting influences in relevant subgroups of the population. Quite meaningful findings can be hidden in behavioral research limited to identifying global statistical correlations in cross-sectional and longitudinal data.
The impact that statistical methods can have on the findings from analyses that are not guided by theory and logic based on substantive questions derived from the research literature is discussed. The results point to the need to study patterns of behavior in their contexts of occurrence in research on lifestyles and health.
In recent years a multitude of investigations have examined behavioral habits of individuals in relation to different health outcomes. This paper discusses this body of research and presents results from a popu- lation health study that illustrate the need to rethink standard approaches to analyzing data. We argue that new approaches to research on health related behavior are needed for building knowledge in the field.
It has become customary in research on behavioral habits to focus on specific behaviors that have been statistically associated with morbidity or mortality in population health data. A limited number of behaviors are studied in what is loosely labelled lifestyle research. Tobacco or alcohol consumption, physical exercise and/or dietary practices are studied almost exclusively in this research tradition. These behaviors are examined statistically against a wide array of self-reported measures of morbidity or register data on disease specific or total mortality.
Huge bodies of research literature have grown up around these four behaviors. Statistical correlations found are often inconsistent or even directly contra- dictory. Investigations relating the same behavior statistically to the same outcome may find a signifi- cant statistical effect in one study and no effect in another, or even effects in opposite directions for the same factor [1].
The data on diet and CVD illustrate the problems. Because of correlations found between blood choles- terol and CVD, diets high in saturated fat have been especially targeted in behavioral research and pro- grams. It is now known that the global statistical correlations hide serious contradictions like the high coronary disease rates of Asian immigrants to Britain
in spite of lower blood cholesterol, blood pressure and tobacco consumption than the non-immigrant British population [2].
There is evidence that among women high blood cholesterol is not statistically associated with mor- tality, not even cardiovascular disease mortality [3]. Other findings contradicting the saturated fat/high cholesterol hypothesis include, the relatively low rates of CVD in some countries (e.g. France) despite relatively high content of saturated fat in the diet and the findings in some cohort and case control studies that fruit, vegetable or cereal consumption is negatively related to CVD with no link found for saturated fatty acid [4].
After years of population interventions and health education seeking to lower blood cholesterol levels in general populations without consideration of the contradictions in the evidence, a U-shaped association between level of blood cholesterol and subsequent mortality is now receiving greater atten- tion [5]. On the one hand, high blood cholesterol is related to higher risk of death from coronary heart disease (for men), but at the same time there is a higher risk of death from noncoronary heart disease causes with lower levels of blood cholesterol. This means that not only have extensive population financial resources been used for misleading health education and services, but that for many people, especially women, the advice may have been danger- ous, increasing their risk for other health problems. The U-shaped curve illustrates methodological prob- lems and limitations in both the paradigm of risk factor etiology underlying this type of research, and in the approaches to statistical analysis that have dominated this research tradition [6].
845

846 Kathryn Dean et al.
Similar problems pervade the population health statistics on cancer, the second major cause of mor- tality after cardiovascular disease in industrialized societies [7]. Sixty-five percent of all cancers occur in persons over 65 years of age and cancer incidence and mortality are increasing. A decline in lung cancer among men in the United States has been attributed to male reductions in smoking, but evidence incon- sistent with this hypothesis is the lack of similar declines in cancers of the esophagus and larynx, other fatal smoking related cancers. An issue in scientific debates about lung cancer research is the possibility that changes in occupational or environmental exposures to carcinogens may account for reductions in lung cancer. Generally, the cancer patterns of industrialized countries cannot be explained by either health related behaviors or aging.
The underlying problem creating the confusion in population research on health related behavior is the multicausal nature of disease which is not reflected in the dominate approaches to research on population health issues. Both theoretical and methodological problems need to be addressed in research on health related behaviors.
LIFESTYLE: DISCRETE BEHAVIORS OR WAYS OF LIVING?
Lifestyle has become an umbrella term for examin- ing a limited number of behaviors in data collected from population samples. Not only is the range of behavior studied very narrow, behaviors generally are examined separately, or at best, parallel to each other. This approach to the subject of health related behavior is incompatible with the meaning of the concept of lifestyle and with learning about how the behavior of individuals affects health and longevity.
Lifestyle is a sociocultural phenomenon arising from interactions between patterns of behavior and life situations [8]. Behavioral practices are shaped by values and beliefs learned in cultural settings, and by opportunities and constraints defined by specific social and economic situations. Furthermore, behaviors are not simple determinants of health. They interact with biological, psychological and social influences to shape both health and longevity. Reductionistic conceptualizations of lifestyle are not compatible with the real interacting biological, psychological and cultural systems that determine health over the life course [9].
New approaches to lifestyle research can integrate epidemiological and social science knowledge and skills in order to study patterns of behavior in the contexts in which they occur. It is a major thesis of the Val6ncia Lifestyle Project that lifestyle research needs to focus on the complexity inherent in ways of living. Our initial efforts in this direction involve using a different methodological approach to the analysis of existing population health data in order to obtain a meaningful foundation for our subsequent
work. For the purpose of studying interactions among social and behavioral influences, it is efficient to start by using new approaches to the analysis of existing data. Much untapped knowledge is locked up in data bases that have been analyzed in quite limited proforma ways [10].
THE ELCHE HEALTH SURVEY
The research project providing the data analyzed in this paper resembles many contemporary population health surveys. However, our approach to the analy- sis of the data differs from most standard approaches to research on individual health practices. Our goal is to shift the theoretical and analytic focus from predicting the statistical effects of specific behaviors in health data to understanding the interrelationships among behavioral and other influences that affect health. The first stage of the project involves elaborat- ing the complex relationships among the behavior, social situation and health variables in available data in order to obtain useful information for the next stage of the project. Even though we were limited to data not directly designed for these purposes, it was deemed possible to identify networks of relationships among behavioral and situational variables that suggest contextual issues for further study.
This preliminary work is a secondary analysis of data collected in the health survey conducted in the Elche, Spain Healthy Cities project. A cross sectional interview design was used to collect health data from a stratified random sample of the 126,156 people over 15 years of age who live in Elehe. A 600 person sample, stratified according to residential districts, was obtained from a register generated by the municipal authorities. Of the sample of 600 people over 15 years of age, interviews were obtained from 513 persons for a response rate of 86%. Table 1 shows the age, sex and education distribution of the sample obtained and the respondents included in the analysis presented below. The entire sample could not be included in the analysis due to missing values. While adjustments sometimes are made to include respondents with missing values, such procedures distort the findings in unknown ways. Our goal is not to make population estimates, but to understand relationships among variables. The sample is gener- ally representative of the age distribution of the population, but contains larger proportions of females and persons with more education.
A structured interview protocol, developed in the Public Health Department of the University of Alicante, was used to collect data in five subject areas: self perceived health; morbidity, behavioral habits; health service use and socioeconomic status. From this data, 11 variables relevant for the purposes of our study were selected. We focused on the more studied behaviors in our initial work, except that consumption of dietary fat was not included. In a lifestyle perspective, dietary behavior means the con-

Research on lifestyles and health
Table 1. Age, education and sex distributions of the sample in relationship to Elche population Population Total sample Analysed sample
Age 14-24 30601 24.3% 138 26.9% 72 17.2% 25-39 38324 30.4% 152 29.6% 146 34.8% 4(~54 26836 21.3% 110 21.4% 101 24.1% >55 30406 24.0% 112 21.8% 100 23.9%
Education No formal 64025 50.8% 173 33.8% 156 37.2% Primary 48799 38.7% 239 46.4% 195 46.5% Secondary 9600 7.6% 71 13.8% 44 10.5% University 3732 2.9% 29 5.8% 24 5.7%
Gender Male 61876 49.0% 205 40.0% 166 39.6% Female 64291 51.0% 308 60.0% 253 60.4%
847
tent and amount of food intake relative to the total life situation. The relevance for health of a single component of the diet depends on the total diet as well as other factors, genetic and environmental.
The smoking, alcohol and exercise variables in this initial analysis are limited to the general practice of these behavioral habits. Detailed information based on the epidemiological experience reported in the literature for collecting data on these practices was collected on the nature and frequency of the behavioral habits. However, as discussed above, our concern is not in finding 'independent' correlations between specific variable pairs and certainly not any supposed dose response relationships between specific behaviors and health variables. We question the soundness of analyses that imply causal connec- tions of this sort because other influences moderate and change the relationships found between an agent/behavior and an effect. In cross-sectional population survey data, such relationships are meaningless. This project is concerned with patterns of behavior and the contexts in which they occur. The major validity issues at this stage are conceptual validity in lifestyle research and the impact of the statistical analysis on the validity and meaningfulness of the findings.
The sample size places limits on the number of categories that can be included in meaningful analyses of the multidimensional tables included in the analysis. Focusing on patterns and interactions among the different types of variables is best achieved by limiting the categories and analyzing the data in a statistical model that can examine all of the vari- ables in a unified framework. For all of these reasons, the smoking, alcohol and exercise variables included in the analysis focus on the general practice of these behavioral habits. Subsequent work in the project, based on the findings of our secondary analyses, will integrate information about content and range of the behavioral practices. An overview of the variables is found in Table 2: the variable categories, the number of respondents in each category and the percentage distributions. The tendency to use medication is examined in this study for two reasons. Large bodies of empirical research suggest that women and men
use medicines in fundamentally different ways, and that these gender differences also apply to alcohol consumption. We therefore are interested in studying relationships between the tendency to use medi- cations and alcohol consumption in a lifestyle frame- work that examines gender differences in the context of the life situation. Secondly, the use of prescription medication in relation to nonprescription drug use is theoretically an indicator of the seriousness of health problems, and thus useful to study with the general, but imprecise, measures of health in this existing data set.
Perceived health status and the presence of chronic health problems are examined as indicators of global health. Perceived health has predicted morbidity and mortality in various studies [11], yet little is under- stood about the meaning of these relationships and available evidence points to the need to understand more about how this variable relates to factors that influence health and to other measures of health [12]. Any health impact accruing from the behavioral and situational variables may be expected to be manifested by the presence of chronic health prob- lems.
Based in the theoretical perspective that lifestyles are patterns of living shaped in social and situational settings, we expect interactions among the behavior variables to differ for subgroups of the population. Both because gender is one of the most fundamental determinants of life situational differences and because sex differences in morbidity and mortality are among the more universal inequalities in population health statistics, all analyses will be conducted separately for men and women in order to increase the validity and meaningfulness of the findings. If we only entered gender in the multivariate analysis of the total data set possible gender determined differ- ences in patterns of relationships could not emerge. Another fundamental influence on lifestyle is social status which is negatively associated with morbidity and mortality in all countries. The nature of social status inequalities in health is not understood [13]. We examine this issue by differentiating the edu- cation, income and employment status components of social status.

848 Kathryn Dean et al.
Table 2. Categories and frequency distribution of the 12 variables selected for the analysis
Variables Frequency Percentage
Gender Male 166 39.6 Female 253 60.4
Age 14~24 72 17.2 25-39 146 34.8 40-54 101 24.1 Over 55 100 23.9
Employment status Full time 138 32.9 Part-time 58 13.8 Unemployed 58 13.8 Housewife 114 27.2 Retired 51 12.2
Family monthly income Under 50000 pts 88 21.0 50000-100000 pts 156 37.2 100000-150000 pts 102 24.3 Over 150000 pts 73 17.4
Education level No formal education 156 37.2 Primary school 195 46.5 Secondary school 44 10.5 Attended university 24 5.7
Smoking Current smoker 172 41.1 Ex-smoker 50 11.9 Never smoked 197 47.0
Ah'ohol Habitual drinker 163 38.9 Occasional drinker 169 40.3 Non-drinker 87 20.8
Regular exercise No 279 66.6 Yes 140 33.4
Prescription medication use No 276 65.9 Yes 143 34.1
Non-prescription medication use No 385 91.9 Yes 34 8.1
Perceived health status Good 216 51.6 Fair 171 40.8 Bad 32 7.6
Chronic illness No 165 39.4 Yes 254 60.6
used multivariate regression models that build on assumptions of normally distributed variables and analysis of the covariance matrix, the graphical models are concerned with partial correlations and partial covariance structures. Models based on simple parametric structures do not allow the elaboration of conditional and moderating influences [15].
Graphical chain models provide a method for assigning a theoretically based structure to the analy- sis [16]. In this study, the social situational variables are placed on the highest level, followed by the behavioral habits, with the two types of medication use and the two health variables examined as out- come measures. Between blocks, tests of relationships are allowed only from higher to lower recursive blocks (represented by arrows suggesting a direc- tional relationship), while the relationships among variables are tested within each recursive block (no arrows are allowed). The statistical tests used in the graphical analysis are gamma correlation coefficients for ordinal level variables and chi square tests for the nominal variables. Exact P values are calculated for both types of tests.
This methodological approach helps to reduce the well known problems of model choice in multivariate procedures, minimizing when conducted correctly, well justified concerns about 'data drudging' in empirical studies. It is, of course, theory and knowledge of the substantive domain that must guide the researcher using graphical chain models. Always a matter of judgement and expertise, the specification of the recursive structure will depend on the research question and the theoretical framework guiding the analysis. For most variables directional influence is time bound and special caution must be used in analysis and interpretation of findings from cross-sectional data. The important advantages of the methodological approach are derived from the ability to concentrate on meaningful connections among variables that constitute causation in the real world and from moving beyond the limitations of para- metric models and the seriously confounding effects of multicolinearity.
METHODS THAT ELABORATE COMPLEXITY
The goal of shifting the emphasis from predicting statistical effects of specific factors to studying pat- terns of interrelationships among the structural, behavioral and health variables required analytic methods that elaborate direct and indirect relation- ships among the different types of variables. Graphi- cal interaction models were chosen for this purpose [14]. A subclass of log linear models, the graphical models build on the property of conditional indepen- dence to produce an independence graph. The graph, a direct mathematical representation produced in the statistical analysis, presents the pattern of multi- variate associations and dependencies in the multi- dimensional problem. In contrast to some widely
THE FINDINGS
A correlation matrix showing relationships between variable pairs is presented in Table 3. As would be expected, strong negative correlations were found between perceived health status and both chronic health problems and use of prescription medications. Older people more often report chronic conditions, use of prescription medications and poor health. Chronic conditions and prescription medications were more often reported by women, while men more often reported better health. Regular exercise, alcohol consumption and smoking were more common among younger people, the higher educated and the employed. Men more often

z
~ ~ ~ -
o o o o o o o o - - I I
~ - ~ o o o o o o o o - -
I
I I
o o o o o o - -
I I
o o o ~ - - I I
I [ I
I
om
<
~~.~ ~ ~z
Research on lifestyles and health 849
E
II t L ..d
~ov II V~. ~e
reported regular exercise as well as considerably greater consumption of both alcohol and tobacco.
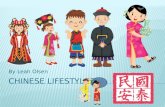
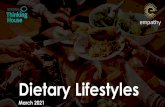
Figures 1 and 2 present the results of the multi- variate graphical analyses of the variables for women and men respectively. The findings confirm our expectation of gender specific interactions among the variables. Alcohol and tobacco consumption are related for men, but not for women. On the other hand, physical activity is related to alcohol consump- tion for women, but not for men. The only social situational variable related to the male behavior is the direct influence of education on both physical activity and alcohol consumption, and its indirect influence on smoking. Among women physical activity differs according to income.
Consistent with the findings from many investigations, females used more prescription medi- cations than males, 40.3% compared to 24.7%. The sex difference did not appear, however, in the use of non-prescription medicines. A slightly larger proportion of men, 9.6% compared to 7.1% of the women reported that they had used non-prescription medication during the prior two weeks. Figures 1 and 2 show that the two types of medicines were inversely related for women, while there was no independent statistical relationship between the two variables for men. None of the behavioral habits were related to using medicines among men, but alcohol consump- tion was related to using prescription medicines among women.
While these findings suggested possibly relevant gender specific aspects of lifestyles more work was required before any interpretations could be drawn. The number and magnitude of the relationships between age and most of the other variables pointed to fundamental age differences in the patterns of relationships, indicating that the interactions among variables needed to be studied within a narrower age range. New analysis were conducted to examine the relationships among the variables for young men and women (under 40 years of age) in relation those over 40 years of age.
Figures 3 and 4 reveal striking differences in the statistical connections among the variables for younger relative to older women. No statistically significant relationships between either the social situational or the behavioral variables and the health measures were found for women under 40 years of age. For women over 40, however, strong statistical connections between the levels of influence emerge. Education is positively related to perceived health status. Education is also positively related to alcohol consumption, which in turn is positively related to perceived health status and negatively related to use of prescription medications. Income and employment status are not directly related to either the medication or the health variables. Income is, however, positively related to exercise, which in turn is positively related to perceived health status. Employment status is related to smoking, which surprisingly is negatively
S,$M 4116~G

850 Kathryn Dean et al.
IN~-0ME v 0 F & / I \~ '~ " '<u3s I ISMOKE
~¢::~/ I N~X-7. ~ ~ ] y ~ 7-0.47, P0 I ~'/ ~ ] ~ ° I ~ , j ~ ~, PR~ESC_dRIP HEALTH
/ ._L.. Z l ~--s~l" I ~ ~ I~ _- -J~¢ '_~ / /E-MeLOY ~ I EDU~ATI~3N I EXERCISE . /1 I ~'~ ~ . e ~<.~ ' -o
/ I
y = gamma correlations for ordinal structure ~2 = significant relationships without ordinal structure P = exact P values Fig. 1. Direct and indirect relationships between social situation, behavior and health variables in the
sample of women from the Elche health cities study.
correlated with chronic illness. As with the younger women, smoking is not related to either of the other two behavioral variables or to the use of medication. Even though based on exact P val- ues, the relationships for smoking may have little meaning due to the high proport ion (93%) of these older women who reported that they have never smoked.
Some similarities in medication behavior among younger compared to older women were found, but also unexpected differences. The use of prescription drugs is negatively correlated with taking non-
prescription drugs and with perceived health status among both the older and the younger women. Surprisingly, the use of prescription drugs is posi- tively related to being chronically ill only among the younger women. The use of non-prescription drugs is negatively related to perceived health status among the younger, but not the older women.
In Fig. 5 the findings for younger men show that parallel to the findings for younger women, the social and behavioral variables are generally not indepen- dently related to the medication and health variables. An exception is the strong relationship between
INCOME
~-~%o SMOjKE
G,
~ ,23 EXERCISE
k ALC~OHOL
HEALTH
PRESCRIP
q 0 ~ . 5 4 , P 0.043.._( II,l, )
y = gamma correlations for ordinal structure )~2 = significant relationships without ordinal structure P = exact P values
Fig. 2. Direct and indirect relationships between social situation, behavior and health variables in the sample of men from the Elche healthy cities study.

Research on lifestyles and health 851
I N C O M E
E D U C A ~ T I O N
E M P L O Y
SMOKE
EXERCISE
ALCOHOL
7 -0 .57 , P 0
P R E S C R I P H E A L T H
NONp,~IRES C -
"~ = gamma correlat ions for ordinal structure
~2 = s ignif icant relat ionships without ordinal structure
P = exact P values
Fig. 3. Direct and indirect relationships between social situation behavior and health variables among women under 40 years of age in the Elche healthy cities study.
education and perceived health status. Alcohol consumption is negatively related to exercise and positively related to use of prescription drugs among the younger men.
Figure 6 shows that the influence of the situational and behavioral variables emerges among the older men. However, the pattern of relationships is quite different than the findings for the older women. Occupational status becomes a central variable, related directly to alcohol consumption, use of pre- scription medicines and perceived health status, and indirectly through perceived health status and the
use of prescription drugs to being chronically ill. Smoking and drinking are strongly positively related and, again surprisingly, smoking is negatively related to having a chronic illness. There is no relationship between the use of prescription and nonprescription drugs among men. A large positive correlation between use of prescription medicine and chronic illness was found among the older men.
In contrast to the older women, the majority of the men over 40 were current smokers. The large negative correlation between smoking and having a chronic illness among these men is partially due to the wide
IN 'C '~E .
E M P L O Y
S OO E / ~ ~ ' 6 2 , p t~ .
~" . . . . G T ; n 0 2 5 -
E X E R C I S E ~ " ~ / ~ . /
'Oo ,~ I ~,'~ U , • ~3 - - , , ~ / o ~ .~"
A L C O H O L
P R E S C R I P
¥ = gamma correlat ions for ordinal structure
X 2 = signif icant relat ionships without ordinal structure
P = exact P values
Fig. 4. D i rec t a n d indi rec t r e l a t ionsh ips be tween socia l s i tua t ion , b e h a v i o r a n d hea l th va r i ab les a m o n g w o m e n over 40 years o f age in the Elche hea l t hy cities s tudy.

852 Kathryn Dean e t al.
I N C O M E
EMPLOY
SM. OKE
? 0.43, P 0 . 0 2
E X E R C I S E ~,
e7
A L C O H O L
/
NON~.,PRESC
H E A L T H ___..........l~-.-- ~
O
? = gamma correlations for ordinal structure Z 2 = significant relationships without ordinal structure
P = exact P values
Fig. 5. Direct and indirect relationships between social situation, behavior and health variables among men under 40 years of age in the Elche healthy cities study.
range of conditions included in the chronic conditions variable. A variable including only tumor, heart condition, bronchitis, and mouth or gum problems, conditions that have been statistically associated with smoking, is not negatively related to the health variable. Proportionately more ex-smokers reported chronic conditions, indicating a tendency in the ex- pected direction even though the result is not statisti- cally significant.
Comparison of the global correlations between variables seen in Table 3 and the relationships found in the graphic analyses confirm the importance
of studying patterns of relationships in relevant sub- groups of the population. Strong and highly signifi- cant relationships disappear completely in the results of the multivariate analysis as, for example the relationship between perceived health status and smoking. Many of the bivariate relationships hold only for specific subgroups, as for example the strong negative relationship between perceived health status and chronic conditions, which is not found in any of the multivariate graphical analyses except for men over 40 years of age, where the gamma correlation becomes much stronger, -0 .85, P = 0.000 in com-
I N C O M E
~ I E D U C A T I O N
EMPLOY~ ?0.33, P O . 0 i
S~s6,
A L C O H O L
J
I
J
PRESCRIP
• "~q~ H E A L T H
N ON,,,~PRESC
"/= gamma correlations for ordinal structure ;(2 = significant relationships without ordinal structure
P = exact P values
Fig. 6. Direct and indirect relationships between social situation, behavior and health variables among men over 40 years of age in the Elche healthy cities study•

Research on lifestyles and health 853
parison to the -0 .51 , P = 0 . 0 0 0 in the bivariate relationship for the total sample. In some instances the direction of the relationship changes, as the bivariate positive relation between regular exercise and alcohol consumption, which becomes a strong negative relationship among males under 40 years of age. These examples reveal that hidden relationships which are important for understanding the health impact of lifestyles may never be found without appropriate and careful analysis.
DISCUSSION
The statistical analysis conducted in this investigation uncovered relationships and important subgroup differences in patterns of relationships among variables that would not have been found with most standard approaches to data analysis. Had the data been analyzed with standard regression pro- cedures numerous statistical associations would have been found, but misleading relationships arising from analyzing the combined data rather than studying relevant subgroups would not have been identified. Relationships would have been found that 'held' after gender and age are 'controlled', but the mean- ingful content behind the statistical effects of age and gender would be lacking. At the same time, important relationships would have remained hidden.
It is known that attitudes and behavior are culturally determined variables and that many are gender specific. Likewise, it is known that social situational variables and their impact on health change over the life course. Even though the effects of behavior on health are both interactive and cumu- lative, standard analytic approaches generally ignore the complex interactions inherent in causal processes. Studying discrete behaviors by statistically 'con- trolling' for other causal factors implies simple cause and effect relationships that are not tenable. In spite of the limitations of this existing data set, the results of our analysis suggest processes of influence with implications for health promotion and for designing new research.
The findings point to the fundamental importance of employment status for men in contemporary Spain, and as would be expected suggest that health impact of work and unemployment are cumulative. Among older men statistically independent relation- ships between the work status variable and perceived health status, use of medications, and through the medication variable, to chronic health problems were found. The statistical relationships between education and income and the health variables were indirect, operating through the employment status variable. The findings show that unemployed and pensioned men feel more ill and proportionately more often have chronic conditions and that those with less education and lower incomes are overrepresented among the unemployed and ill. The indirect relation- ship between employment status and chronic con-
ditions operates through the partial relationship between taking prescription medications and chronic conditions providing a validity check for the chronic illness variable.
The strong positive relationship that emerges between smoking and alcohol among older men in contrast to younger men suggests interactive and addictive effects of using these two substances over time. It is perhaps the interactive effects of using the substances and the addictive aspects of their use that need intensive study both in relation to causal influ- ences and health outcomes. This is also suggested by the unexpected findings on the smoking and health variables. The lack of a significant relationship between the smoking and health variable, of course, does not mean that smoking is not dangerous for health. The effects are cumulative and many older smokers may be dead. What the findings illustrate is the need to study multiple influences, and especially for older men, work and employment status, if health and lifestyles are to be understood. Not at all surpris- ing given the extensive documentation of social class differences in health and longevity, the findings point to the neglected dimensions of time and context in superficial relationships between specific behaviors and specific diseases.
For women, the implications of the findings are quite different. The employment status variable has no influence on the health variables, suggesting work experience and role responsibilities are fundamentally different for older women compared to men. One may anticipate cohort effects to influence these relationships in the future.
No relationships were found between smoking and alcohol consumption among women. Also in contrast to men, exercise was related to perceived health status among women. Gender differences in behavioral practices and in relationships between behavior and health are areas of research with great potential for expanding knowledge about lifestyle and health. Gender differences in using chemical substances, especially multiple substances, probably are a contributing factor to gender differences in morbidity and mortality.
The important finding emerges that among older women the negative relationship between prescrip- tion medication use and perceived health status grows stronger, while in contrast to men, a relationship between prescription medicines and chronic con- ditions was not found. At the same time, only 31% of the men in comparison to 53% of the women reported taking prescription medications during the study period. Thus it is not health problems alone that are shaping the far greater medicine use among w o m e n .
Perhaps the most important results of this study have to do with the illustrations of the limits of statistical analysis, the impact of averages and the statistical artifacts that can mislead the researcher. An example of these problems is the relationship

854 Kathryn Dean et al.
between education and smoking in the total female sample, which is not found among either the younger or older women when examined separately. Similarly, among men the relationships between education and both exercise and alcohol in the total sample, are absent when the sample is divided into age groups. At the same time, quite meaningful relationships appear when the subgroups of the sample are studied that do not hold in the total sample or in other subgroups. The findings show clearly that without theory and awareness of the existing knowledge to guide the analysis in a research area, statistical re- lationships have little meaning and can be seriously misleading.
The concept of lifestyle inherently means ways or styles of living that are not the same for all people. Ways or patterns of living involve widely different combinations of specific behavioral practices that may characterize subgroups of the population. Preoccupation with specific behavioral practices interferes with the process of obtaining knowledge about the health enhancing or health damaging effects of different patterns o f daily life. It also ignores the cultural and situational determinants of lifestyles and the importance of realistic options for living in ways that may be more health enhancing.
In order to build a body of knowledge about lifestyles and health, research which charts the pat- terning and interactions among behaviors that may damage or protect health, and which identifies the direct and indirect relationships between behavioral and other relevant variables is needed. Statistical predictions of negative health outcomes based on some variable (behavioral or any other) can only be a starting point in the search for understanding complex causal processes affecting health [17]. Mortality and morbidity predictions arising from a behavioral practice hide the fundamentally different effects that behavior has for members of different subgroups of the population and at different periods over the life course. Thus serious contradictions and uncertainties pervade the research literature on specific health related behaviors.
A major source of the problem is excessive focus on the concept of risk and the methods used to measure it [6]. Rose, analyzing methodological issues in epidemiological research, pointed out that measuring relative risk in 'exposed' individuals and 'non-exposed' individuals is neither a measure of etiological outcome nor of public health importance. The concept of relative risk, he noted, has unfortu- nately almost excluded other approaches to quantify- ing causal importance [18]. The power of statistical procedures to distort and hide as well as to predict and elucidate is revealed when one elaborates com- plex relationships in data collected from population samples.
In conclusion, findings from this secondary analysis of available data from the Elche Healthy Cities project point to the need to study behaviors
that may affect health in relation to other behaviors, placing behavioral practices in a contextual perspec- tive. While it is impossible to draw any conclusions about aging or cohort effects from this secondary analysis of existing data, the results suggest research issues which should guide our work in the next stages of the project. The results also illustrate the limits of behavioral studies focused on analyzing global corre- lations in cross-sectional or longitudinal data [6, 15]. The impact that statistical methods can have on the 'findings' in research on population health is illustrated. Statistical procedures are tools, and like all tools, must be suited to the job at hand and used correctly to achieve valid and meaningful results. No single study or methodological approach can stand alone. Exploratory work of this type can facilitate the relevance and rigor of research on lifestyles and health.
REFERENCES
I. Webster L. and Weiss N. Alcoholic beverage consump- tion and the risk of endometrial cancer. Int. J. Epi- demiol. 18, 786, 1989. McCormick J. and Skrabanek P. Coronary heart disease is not preventable by population interventions. The Lancet 8615, 839, 1988.
2. McKeigue P. and Marmot M. Mortality from CHD in Asian communities. Br. Med. Jl 297, 903, 1988.
3. Jacobs D., Blackburn H., Higgins M., Reed D., lso H., McMillan G., Neaton J., Nelson J., Potter J., Rifkind B., Rossouw J., Shekelle R. and Yusuf S. Report of the conference on low blood cholesterol: mortality associ- ations. Circulation 86, 1046, 1992.
4. James W., Duthie G. and Wahle K. The Mediterranean diet: protective or simply non-toxic? Eur. J. clin. Nutr. 43, 31, 1989.
5. Hulley S., Walsh J. and Newman T. Health policy on blood cholesterol: time to change directions. Circulation 86, 1026, 1992.
6. Dean K. Intregrating theory and methods in population health research. In Population Health Research: Linking Theory and Methods (Edited by Dean K.). Sage Publi- cations, London, 1993.
7. Davis D. and Hoel D. Figuring out cancer. Int. J. Hlth Serv. 22, 447, 1992.
8. Coreil J., Levin G. and Jaco G. Life style--an emerging concept in the sociomedical sciences. Cult. Med. Psy- chiat. 9, 423, 1985. Kickbusch I. Lifestyles and health. Soc. Sci. Med. 22, 117, 1986. Blaxter M. Health and Lifestyles. Tavistock/Routledge, London, 1992.
9. Dean K. Self-care components of lifestyles: the import- ance of gender, attitudes and the social situation. Soc. Sci. Med. 29, 137, 1989.
10. Glymour R., Scheines R., Spirtes P. and Kelly K. Discovering Causal Structure: Artificial Intelligence, Philosophy o f Science, and Statistical Modelling. Aca- demic Press, New York, 1992; Dean, 1993, see Ref. [6].
I 1. Kaplan G. and Camacho T. Perceived health and mortality: a nine-year follow-up of the human popu- lation laboratory cohort. Am. J. Epidemiol. 117, 292, 1983. Cockerham W., Sharp K. and Wilcox J. Aging and perceived health status. J. Geront. 38, 349, 1983.
12. Jylh~i M., Leskinen E., Alanen E., Leslinen A. and Heikkinen E. Self-rated health and associated factors among men of different ages. J. Geront. 41, 710, 1986.
13. Marmot M., Kogevinas M. and Elston M. Socio- economic Status and Disease. In Health Promotion Research: Towards a New Social Epidemiology (Edited

Research on lifestyles and health 855
by Badura B. and Kickbusch I.). World Health Organization Regional Publications Series No. 37, Copenhagen 1992. Blaxter M. Health services as a defence against the consequences of poverty in industrialized societies. Soc. Sci. Med. 17, 1139, 1983.
14. Whittaker, J. Graphical interaction models: a new approach for statistical modelling. In Population Health Research: Linking Theory and Methods (Edited by Dean K.). Sage Publications, London, 1993. Whittaker J. Graphical Models in Applied MultiL, ariate Statistics. Wiley, New York, 1990.
15. Dean K., Kreiner S. and McQueen D. Researching population health: new directions. In Population Health Research: Linking Theory and Methods (Edited by Dean K.). Sage Publications, London 1993.
16. Wermuth N. Associations structures with few variables: characteristics and examples. In. Population Health, Research: Linking Theory and Methods (Edited by Dean K.). Sage Publications, London, 1993.
17. Dean K. Social support and health: pathways of influence. J. Hlth Prom. 1, 133, 1986.
18. Rose G. Sick individuals and sick populations. Int. J. Epidemiol. 14, 32, 1985.