Research Article The Use of a Validated Claustrophobia ...€¦ · The Use of a Validated...
5
Journal of Sleep Medicine & Disorders Cite this article: Aljasmi M, Cheng P, Agarwal K, Uppalapati S, Moss K, et al. (2016) The Use of a Validated Claustrophobia Questionnaire in Predicting Future Compliance to Continuous Positive Airway Pressure (Cpap) in Obstructive Sleep Apnea (Osa). J Sleep Med Disord 3(2): 1044. Central *Corresponding author Mohammed AlJasmi, Department of Sleep Medicine, Henry Ford Hospital, 2799 West Grand Blvd, Detroit, MI, 48202, USA, Fax: 313-916-5150; Email: Submitted: 28 February 2016 Accepted: 23 March 2016 Published: 25 March 2016 ISSN: 2379-0822 Copyright © 2016 Aljasmi et al. OPEN ACCESS Keywords • Obstructive sleep apnea (OSA) • Continuous positive airway pressure (CPAP) • Claustrophobia • Adherence • Compliance Research Article The Use of a Validated Claustrophobia Questionnaire in Predicting Future Compliance to Continuous Positive Airway Pressure (Cpap) in Obstructive Sleep Apnea (Osa) Mohammed Aljasmi*, Philip Cheng, Kunal Agarwal, Sri Uppalapati, Kenneth Moss, Vivek Venugopal, Luisa Bazan and Christopher Drake Department of Sleep Medicine, Henry Ford Hospital, USA Abstract Study objectives: Adherence to CPAP therapy is a well-documented problem in treatment of OSA. Many patients report that CPAP masks feel claustrophobic, which serves as a psychological barrier from regular use. We hypothesized that individuals reporting high anxiety related to claustrophobia may be at higher risk for low adherence. Methods: We performed a prospective chart review of 45 patients who were newly diagnosed with OSA. Patients were provided with a claustrophobia questionnaire that measures fear of suffocation and fear of restriction. Adherence data was collected at first follow-up visit after starting CPAP therapy. Compliance data includes average usage within 30 days and the frequency of usage for at least 4 hours during the night on 70% of nights. The relationship between CPAP use and claustrophobia was test via a multiple linear regression with the dependent variable as the percentage of days with 4 or more hours of CPAP use within the last one-month. Results: Results revealed that claustrophobia was robustly related to adherence. Specifically, higher anxiety related to suffocation and restriction was related lower frequency of nightly CPAP use over 4 hours A disproportionately higher rate of failed adherence in the high-claustrophobia group (3.3%) compared to the low- claustrophobia group (71.4%), χ 2 (1) = 7.7, p < .01. Both age (β = -.06, se = .03) and claustrophobia (β = -.13, se = .03) predicted decrease CPAP use Conclusions: Screening for claustrophobia may allow for early identification of patients at risk for low adherence. Once identified, these patients can be triaged for additional support via effective interventions such as CPAP desensitization. INTRODUCTION Obstructive sleep apnea (OSA) is a disorder that is characterized by obstructive apneas and hypopneas due to repetitive collapse of the upper airway during sleep. It is independently associated with an increased risk of mortality, in addition to associations with diabetes, hypertension, stroke, coronary artery disease, and heart failure [1-5]. Continuous positive airway pressure (CPAP) is an effective therapy for OSA, but adherence has been demonstrated to be suboptimal [6]. It is estimated that 29 to 83 percent of patients are non- adherent to CPAP, when non-adherence is defined as a mean of ≤ 4 hours of use per night [7,8]. It has been demonstrated that patients generally make the decision to adhere to CPAP therapy within the first week of therapy [7,9,10]. Even one night without CPAP may mitigate the benefits of CPAP therapy, which include fewer apneas and hypopneas, reduced daytime sleepiness, and
Transcript of Research Article The Use of a Validated Claustrophobia ...€¦ · The Use of a Validated...
Journal of Sleep Medicine & Disorders
Cite this article: Aljasmi M, Cheng P, Agarwal K, Uppalapati S, Moss K, et al. (2016) The Use of a Validated Claustrophobia Questionnaire in Predicting Future Compliance to Continuous Positive Airway Pressure (Cpap) in Obstructive Sleep Apnea (Osa). J Sleep Med Disord 3(2): 1044.
Central
*Corresponding authorMohammed AlJasmi, Department of Sleep Medicine, Henry Ford Hospital, 2799 West Grand Blvd, Detroit, MI, 48202, USA, Fax: 313-916-5150; Email:
Submitted: 28 February 2016
Accepted: 23 March 2016
Published: 25 March 2016
ISSN: 2379-0822
Copyright© 2016 Aljasmi et al.
OPEN ACCESS
Keywords•Obstructive sleep apnea (OSA)•Continuous positive airway pressure (CPAP)•Claustrophobia•Adherence•Compliance
Research Article
The Use of a Validated Claustrophobia Questionnaire in Predicting Future Compliance to Continuous Positive Airway Pressure (Cpap) in Obstructive Sleep Apnea (Osa)Mohammed Aljasmi*, Philip Cheng, Kunal Agarwal, Sri Uppalapati, Kenneth Moss, Vivek Venugopal, Luisa Bazan and Christopher DrakeDepartment of Sleep Medicine, Henry Ford Hospital, USA
Abstract
Study objectives: Adherence to CPAP therapy is a well-documented problem in treatment of OSA. Many patients report that CPAP masks feel claustrophobic, which serves as a psychological barrier from regular use. We hypothesized that individuals reporting high anxiety related to claustrophobia may be at higher risk for low adherence.
Methods: We performed a prospective chart review of 45 patients who were newly diagnosed with OSA. Patients were provided with a claustrophobia questionnaire that measures fear of suffocation and fear of restriction. Adherence data was collected at first follow-up visit after starting CPAP therapy. Compliance data includes average usage within 30 days and the frequency of usage for at least 4 hours during the night on 70% of nights. The relationship between CPAP use and claustrophobia was test via a multiple linear regression with the dependent variable as the percentage of days with 4 or more hours of CPAP use within the last one-month.
Results: Results revealed that claustrophobia was robustly related to adherence. Specifically, higher anxiety related to suffocation and restriction was related lower frequency of nightly CPAP use over 4 hours A disproportionately higher rate of failed adherence in the high-claustrophobia group (3.3%) compared to the low-claustrophobia group (71.4%), χ2(1) = 7.7, p < .01. Both age (β = -.06, se = .03) and claustrophobia (β = -.13, se = .03) predicted decrease CPAP use
Conclusions: Screening for claustrophobia may allow for early identification of patients at risk for low adherence. Once identified, these patients can be triaged for additional support via effective interventions such as CPAP desensitization.
INTRODUCTIONObstructive sleep apnea (OSA) is a disorder that is
characterized by obstructive apneas and hypopneas due to repetitive collapse of the upper airway during sleep. It is independently associated with an increased risk of mortality, in addition to associations with diabetes, hypertension, stroke, coronary artery disease, and heart failure [1-5]. Continuous positive airway pressure (CPAP) is an effective therapy for OSA,
but adherence has been demonstrated to be suboptimal [6].
It is estimated that 29 to 83 percent of patients are non-adherent to CPAP, when non-adherence is defined as a mean of ≤ 4 hours of use per night [7,8]. It has been demonstrated that patients generally make the decision to adhere to CPAP therapy within the first week of therapy [7,9,10]. Even one night without CPAP may mitigate the benefits of CPAP therapy, which include fewer apneas and hypopneas, reduced daytime sleepiness, and

Aljasmi et al. (2016)Email:
J Sleep Med Disord 3(2): 1044 (2016) 2/5
Central
improvements in sleep architecture, daily activity, quality of life, hypertension, and neurobehavioral performance [11-14]. Prior research has also identified that adherence in the first 30 days of CPAP use is strongly predictive of future use [8] Such factors that have been shown to predict future CPAP compliance include: CPAP adherence during the first week, increased self reported daytime sleepiness as defined by Epworth Sleepiness Scale (ESS) scores greater than 10 after CPAP use less than or equal to three months, disease severity as identified by increased apnea/hypopnea index scores (AHI) [15], and certain psychological traits, such as lack of claustrophobic tendencies [16]. Furthermore, Drake et al. revealed that the best predictor of CPAP compliance was change in sleep efficiency from diagnostic to titration night, indicating that patients whose sleep improved most on the titration night had the highest levels of compliance [17]. Additionally, individuals whose sleep improved during the CPAP titration demonstrated two hours of increased nightly compliance, even after correcting for disease severity at initial polysomnography [17].
One treatment-specific barrier that is commonly encountered in the clinical setting and anecdotally discussed in the literature is claustrophobia. Claustrophobia is an anxiety disorder of specific phobia type in which individuals experience fear or avoid situations which involve enclosed places [18,19]. Claustrophobia includes components of fear of restriction and fear of suffocation [20].
Early studies of CPAP non-adherence identified claustrophobia as a self-reported barrier to CPAP treatment adherence [21]. Less consistent users of CPAP were also identified as more frequently self-reporting claustrophobia as a treatment barrier [22], with 63% of the participants reporting claustrophobic tendencies after one night of CPAP exposure [23]. In reviewing prior literature, claustrophobia serves as an influential factor on CPAP adherence and as a significant clinical issue [24,25].
Our aim is to identify patients with claustrophobia and determine its impact on CPAP adherence. While also trying to replicate previous findings and clarify claustrophobia itself as a crucial predictor of CPAP adherence, we further hypothesized that individuals reporting high anxiety related to claustrophobia may be at higher risk for low adherence.
METHODSParticipants were recruited from Henry Ford Hospital
Sleep Medicine clinical sleep centers during the 6-month study period. We prospectively followed 43 patients who were newly diagnosed with OSA. Inclusion criteria were: (1) adults (≥18 years of age) with newly diagnosed OSA (Apnea-hypopnea index, AHI ≥5 events/hours) by polysomnogram (PSG) or home sleep study (HST), (2) referred to CPAP titration PSG, (3) CPAP prescription accepted after in-laboratory CPAP titration PSG, (4) able to read and understand English. Exclusion criteria were: 1) supplemental oxygen required during titration PSG; 2) any medical contraindication to using CPAP for treatment of OSA; 3) refusal of CPAP for home treatment at the time of CPAP treatment recommendation. Patients were also excluded from the study if they had a history of acute or chronic pain, were taking any analgesics, had a history of tobacco use, alcohol or drug abuse
and central nervous system acting medications at the time of the screening.
Polysomnography (PSG)
Standard methods for nocturnal PSG assessment were used, the recordings obtained from each participant included standard frontal (F4-M1), central (C4-M1) and occipital (O2-M1), electroencephalograms (EEGs). Single lead II electrocardiography, chin and bilateral anterior tibialis surface electromyogram, and right and left electrooculography, respiratory effort by thoracic and abdominal piezoelectric belts, oxygen saturation by pulse oximetry, and nasal air flow were performed according to established guidelines. All data were collected and monitored using a computerized PSG system and attended by registered polysomnographic technologists. AHI was defined as the total number of apneas and hypopneas per hour of sleep. The severity of OSA was graded as mild (AHI 5–15 events/hour), moderate (AHI >15–30 events/hour), and severe (AHI >30 events/hour).
CPAP use
An internal processor housed within standard CPAP devices measured CPAP use. CPAP use was defined as the mean nightly duration of treatment use at effective pressure; usage was calculated as the mean hours of use at one month of treatment. Additionally, usage for at least 4 hours during the night on 70% of nights was also determined.
Claustrophobia questionnaire
Claustrophobia severity was assessed with the Claustrophobia Questionnaire (CLQ). Rachman and Taylor, 1993, confirmed a two-dimensional structure of this questionnaire.19 Participants were asked how much fear they would experience in each of 36 claustrophobic situations. A principal component analysis confirmed that two factors, interpreted as fear of restriction and fear of suffocation, were underlying self- reported claustrophobic constructs. A subsequent study further developed the CLQ and reduced it to 26 items, 14 items for the suffocation scale and 12 items for the restriction scale [7]. Scores 35 or greater on the CLQ was deemed as clinically significant claustrophobia, determined based on normed mean and standard deviation provided in the validation study.
In addition to the claustrophobia questionnaire, participants also reported feelings of claustrophobia associated with CPAP use. Participants were prompted by the statement “Please rate how claustrophobic you felt while using CPAP”, and responded with a 1 to 10 rating (1 = Not at all, 10 = extremely).
Procedure
Institutional Review Board approval was obtained from Henry Ford Hospital in Detroit, Michigan. During their consultation visit, patients were provided with the 26-item claustrophobia questionnaire that measures fear of suffocation and fear of restriction. Patients proceeded through the standard clinical evaluation and were diagnosed with obstructive sleep apnea either through a portable sleep study or an in lab diagnostic study. Patients willing to go through treatment were titrated through an in lab titration study to find the optimal CPAP pressure to reduce the AHI to less than five. All subjects were provided standardized
Aljasmi et al. (2016)Email:
J Sleep Med Disord 3(2): 1044 (2016) 3/5
Central
education on OSA, PSG, HST, CPAP titration, and CPAP treatment by educational video and a printed pamphlet about OSA. The respective clinical sleep provider initiated CPAP treatment and a home medical equipment supplier designated by participants insurance provider provided CPAP device instructions. Participants returned to the sleep center after one month of CPAP treatment for a study termination research visit. CPAP use for the outcome interval of 30 days was obtained at this visit by data extraction from the CPAP device secure digital memory card.
Statistical Analysis
The sample was first characterized by demographics, AHI severity, claustrophobia, and CPAP adherence. The relationship between CPAP use and claustrophobia was test via a multiple linear regression with the dependent variable as the percentage of days with 4 or more hours of CPAP use within the last 3 months. Age and sex were entered as covariates in the initial model. A chi-square test was also conducted to compare the frequency of meeting adherence criteria between low and high claustrophobia groups.
RESULTSA total of 45 participants were included in this sample. As
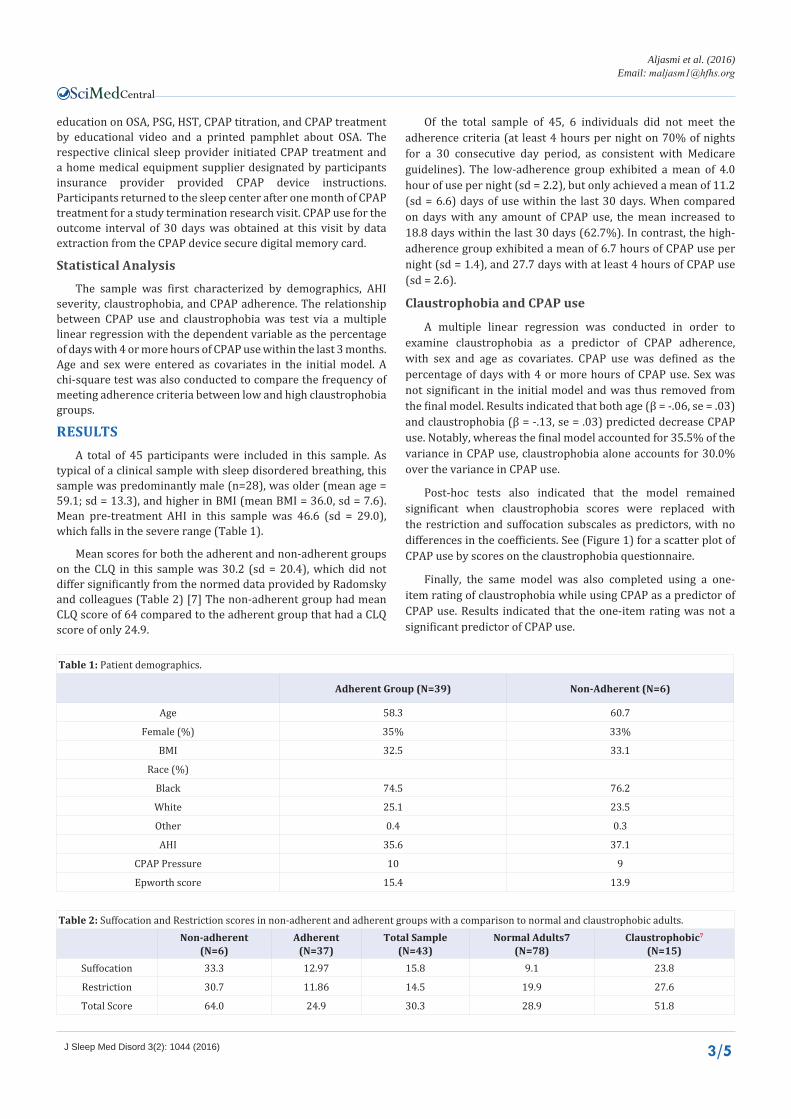
typical of a clinical sample with sleep disordered breathing, this sample was predominantly male (n=28), was older (mean age = 59.1; sd = 13.3), and higher in BMI (mean BMI = 36.0, sd = 7.6). Mean pre-treatment AHI in this sample was 46.6 (sd = 29.0), which falls in the severe range (Table 1).
Mean scores for both the adherent and non-adherent groups on the CLQ in this sample was 30.2 (sd = 20.4), which did not differ significantly from the normed data provided by Radomsky and colleagues (Table 2) [7] The non-adherent group had mean CLQ score of 64 compared to the adherent group that had a CLQ score of only 24.9.
Of the total sample of 45, 6 individuals did not meet the adherence criteria (at least 4 hours per night on 70% of nights for a 30 consecutive day period, as consistent with Medicare guidelines). The low-adherence group exhibited a mean of 4.0 hour of use per night (sd = 2.2), but only achieved a mean of 11.2 (sd = 6.6) days of use within the last 30 days. When compared on days with any amount of CPAP use, the mean increased to 18.8 days within the last 30 days (62.7%). In contrast, the high-adherence group exhibited a mean of 6.7 hours of CPAP use per night (sd = 1.4), and 27.7 days with at least 4 hours of CPAP use (sd = 2.6).
Claustrophobia and CPAP use
A multiple linear regression was conducted in order to examine claustrophobia as a predictor of CPAP adherence, with sex and age as covariates. CPAP use was defined as the percentage of days with 4 or more hours of CPAP use. Sex was not significant in the initial model and was thus removed from the final model. Results indicated that both age (β = -.06, se = .03) and claustrophobia (β = -.13, se = .03) predicted decrease CPAP use. Notably, whereas the final model accounted for 35.5% of the variance in CPAP use, claustrophobia alone accounts for 30.0% over the variance in CPAP use.
Post-hoc tests also indicated that the model remained significant when claustrophobia scores were replaced with the restriction and suffocation subscales as predictors, with no differences in the coefficients. See (Figure 1) for a scatter plot of CPAP use by scores on the claustrophobia questionnaire.
Finally, the same model was also completed using a one-item rating of claustrophobia while using CPAP as a predictor of CPAP use. Results indicated that the one-item rating was not a significant predictor of CPAP use.
Table 1: Patient demographics.
Adherent Group (N=39) Non-Adherent (N=6)
Age 58.3 60.7
Female (%) 35% 33%
BMI 32.5 33.1
Race (%)
Black 74.5 76.2
White 25.1 23.5
Other 0.4 0.3
AHI 35.6 37.1
CPAP Pressure 10 9
Epworth score 15.4 13.9
Table 2: Suffocation and Restriction scores in non-adherent and adherent groups with a comparison to normal and claustrophobic adults.Non-adherent
(N=6)Adherent
(N=37)Total Sample
(N=43)Normal Adults7
(N=78)Claustrophobic7
(N=15)Suffocation 33.3 12.97 15.8 9.1 23.8
Restriction 30.7 11.86 14.5 19.9 27.6
Total Score 64.0 24.9 30.3 28.9 51.8

Aljasmi et al. (2016)Email:
J Sleep Med Disord 3(2): 1044 (2016) 4/5
Central
Claustrophobia and CPAP adherence
In order to examine claustrophobia and CPAP adherence, a chi-squared test was also conducted. Individuals were considered adherent if they reported use of CPAP for 4 or more hours for at least 70% of the last 30 days. Individuals were also categorized as low or high claustrophobia based on a threshold of 35 on the Claustrophobia questionnaire. Results revealed a disproportionately higher rate of failed adherence in the high-claustrophobia group (3.3%) compared to the low-claustrophobia group (71.4%), χ2 (1) = 7.7, p < .01.
DISCUSSIONThis study indicates that patients reporting higher
claustrophobia are less likely to use CPAP for at least 4 hours a night. Notably, 30% the variance in a critical CPAP usage metric, one that determines insurance coverage of the CPAP machine, was accounted by responses on the claustrophobia questionnaire completed at intake. No differences were detected between the restriction and suffocation subscales, suggesting that each subscale is equally predictive of CPAP adherence. Finally, responses on the claustrophobia questionnaire outperformed a one-item rating of feelings of claustrophobia specific to CPAP use, suggesting that it may be important to assess for claustrophobia independent of CPAP use.
The results have important clinical implications for patients diagnosed with OSA. Most notably, screening for claustrophobia may allow for early identification of patients at risk for low adherence. Once identified, these patients can be triaged for additional support via effective interventions, such as desensitization, hypnotic use, or other therapy.
Desensitization involves several therapeutic sessions where the patient becomes gradually sensitized to the CPAP mask and machine pressures until the optimal pressure and is obtained. This brief intervention has some preliminary support as an approach to reducing or eliminating claustrophobia in CPAP-
treated OSA [26,27]. However, future research is needed to test such a strategy in an adequately powered randomized controlled trial to assess if it improves CPAP compliance.
Prior research focusing on hypnotic therapy to aid with CPAP compliance has revealed conflicting results. Bradshaw et al. reported that zolpidem after titration, but commencing with the first 14 days of CPAP did not improve compliance compared to placebo or standardized therapy [28]. Another study demonstrated that a single dose of zaleplon at the start of a split-night CPAP titration does not result in superior CPAP adherence or improvement in symptoms at 1-month compared to placebo [29]. In contrast, Lettieri et al. found that eszopiclone for the first 14 nights of CPAP was associated with greater long-term compliance than placebo [30]. In addition, in a retrospective study, they found an association between hypnotic (mostly zolpidem, and to lesser extent eszopiclone) use during CPAP titration and improved compliance at 4-6 weeks [31].
This study is unique in that it examines the domains of suffocation and restriction to delineate the prevalence of these core components of claustrophobia in adults with CPAP-treated OSA, using a validated claustrophobia questionnaire. In the long term, the proposed selected questionnaire should aid in selecting claustrophobic patients so that interventions, such as desensitization, may be enacted. This will permit patients to become more rapidly compliant with their CPAP machines, eliminate unnecessary repeat sleep studies, and save time and unneeded cost.
CONCLUSIONPatients reporting increased feelings of suffocation and
restriction as related to claustrophobia demonstrate decreased CPAP compliance. Screening for claustrophobia assists with early identification of patients at risk for low adherence. These classified patients can then be referred to effective behavioral therapies, such as CPAP desensitization.
ACKNOWLEDGEMENTCurrent Knowledge/Study Rationale: Many patients
report that CPAP masks feel claustrophobic, which serves as a psychological barrier from regular use. We hypothesized that individuals reporting high anxiety related to claustrophobia may be at higher risk for low adherence.
REFERENCES1. West SD, Nicoll DJ, Stradling JR. Prevalence of obstructive sleep apnoea
in men with type 2 diabetes. Thorax. 2006; 61: 945-950.
2. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000; 342: 1378-1384.
3. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005; 353: 2034-2041.
4. Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001; 163: 19-25.
5. Kushida CA, Littner MR, Hirshkowitz M, Morgenthaler TI, Alessi CA,
Figure 1 Scatter plot of CPAP use by total score on the Claustrophobia questionnaire.
Aljasmi et al. (2016)Email:
J Sleep Med Disord 3(2): 1044 (2016) 5/5
Central
Aljasmi M, Cheng P, Agarwal K, Uppalapati S, Moss K, et al. (2016) The Use of a Validated Claustrophobia Questionnaire in Predicting Future Compliance to Continuous Positive Airway Pressure (Cpap) in Obstructive Sleep Apnea (Osa). J Sleep Med Disord 3(2): 1044.
Cite this article
Bailey D, et al. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Sleep. 2006; 29: 375-380.
6. Weaver TE, Kribbs NB, Pack AI, Kline LR, Chugh DK, Maislin G, et al. Night-to-night variability in CPAP use over the first three months of treatment. Sleep. 1997; 20: 278-283.
7. Radomsky AS, Rachman S, Thordarson DS, McIsaac HK, Teachman BA. The Claustrophobia Questionnaire. J Anxiety Disord. 2001; 15: 287-297.
8. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008; 5: 173-178.
9. Aloia MS, Arnedt JT, Stanchina M, Millman RP. How early in treatment is PAP adherence established? Revisiting night-to-night variability. Behav Sleep Med. 2007; 5: 229-240.
10. Rosenthal L, Gerhardstein R, Lumley A, Guido P, Day R, Syron ML, et al. CPAP therapy in patients with mild OSA: implementation and treatment outcome. Sleep Med. 2000; 1: 215-220.
11. Kribbs NB, Pack AI, Kline LR, Getsy JE, Schuett JS, Henry JN, et al. Effects of one night without nasal CPAP treatment on sleep and sleepiness in patients with obstructive sleep apnea. Am Rev Respir Dis. 1993; 147: 1162-1168.
12. Grunstein RR, Stewart DA, Lloyd H, Akinci M, Cheng N, Sullivan CE. Acute withdrawal of nasal CPAP in obstructive sleep apnea does not cause a rise in stress hormones. Sleep. 1996; 19: 774-782.
13. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006.
14. Young LR, Taxin ZH, Norman RG, Walsleben JA, Rapoport DM, Ayappa I. Response to CPAP withdrawal in patients with mild versus severe obstructive sleep apnea/hypopnea syndrome. Sleep. 2013; 36: 405-412.
15. McArdle N, Devereux G, Heidarnejad H, Engleman HM, Mackay TW, Douglas NJ. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1999; 159: 1108-1114.
16. Chasens ER, Pack AI, Maislin G, Dinges DF, Weaver TE. Claustrophobia and adherence to CPAP treatment. West J Nurs Res. 2005; 27: 307-321.
17. Drake CL, Day R, Hudgel D, Stefadu Y, Parks M, Syron M, et al. Sleep during titration predicts continuous positive airway pressure
compliance. Sleep. 2003; 26: 308-311.
18. Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association. 2000.
19. Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association. 2013.
20. Rachman S, Taylor S. Analyses of claustrophobia. J Anxiety Disord. 1993; 7: 281-291.
21. Katsantonis GP, Schweitzer PK, Branham GH, Chambers G, Walsh JK. Management of obstructive sleep apnea: comparison of various treatment modalities. Laryngoscope. 1988; 98: 304-309.
22. Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, et al. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis. 1993; 147: 887-895.
23. Edmonds JC, Yang H, King TS, Sawyer DA, Rizzo A, Sawyer AM. Claustrophobic tendencies and continuous positive airway pressure therapy non-adherence in adults with obstructive sleep apnea. Heart Lung. 2015; 44: 100-106.
24. Shapiro GK, Shapiro CM. Factors that influence CPAP adherence: an overview. Sleep Breath. 2010; 14: 323-335.
25. Weaver TE. Adherence to positive airway pressure therapy. Curr Opin Pulm Med. 2006; 12: 409-413.
26. Edinger JD, Radtke RA. Use of in vivo desensitization to treat a patient’s claustrophobic response to nasal CPAP. Sleep. 1993; 16: 678-680.
27. Means MK, Edinger JD. Graded exposure therapy for addressing claustrophobic reactions to continuous positive airway pressure: a case series report. Behav Sleep Med. 2007; 5: 105-116.
28. Bradshaw DA, Ruff GA, Murphy DP. An oral hypnotic medication does not improve continuous positive airway pressure compliance in men with obstructive sleep apnea. Chest. 2006; 130: 1369-1376.
29. Park JG, Olson EJ, Morgenthaler TI. Impact of zaleplon on continuous positive airway pressure therapy compliance. J Clin Sleep Med. 2013; 9: 439-444.
30. Lettieri CJ, Shah AA, Holley AB, Kelly WF, Chang AS, Roop SA, et al. Effects of a short course of eszopiclone on continuous positive airway pressure adherence: a randomized trial. Ann Intern Med. 2009; 151: 696-702.
31. Collen J, Lettieri C, Kelly W, Roop S. Clinical and polysomnographic predictors of short-term continuous positive airway pressure compliance. Chest. 2009; 135: 704-709.


















