Research Article The Characterization of Biological Rhythms...
8
Research Article The Characterization of Biological Rhythms in Mild Cognitive Impairment Elisabet Ortiz-Tudela, 1 Antonio Martinez-Nicolas, 1 Carmen Díaz-Mardomingo, 2 Sara García-Herranz, 2 Inmaculada Pereda-Pérez, 3 Azucena Valencia, 3 Herminia Peraita, 2 César Venero, 3 Juan Antonio Madrid, 1 and Maria Angeles Rol 1 1 Chronobiology Laboratory, Department of Physiology, Faculty of Biology, University of Murcia, Campus de Espinardo, Espinardo, 30100 Murcia, Spain 2 Department of Basic Psychology, Universidad Nacional de Educaci´ on a Distancia (UNED), 28040 Madrid, Spain 3 Department of Psychobiology, Universidad Nacional de Educaci´ on a Distancia (UNED), 28040 Madrid, Spain Correspondence should be addressed to Juan Antonio Madrid; [email protected] Received 8 May 2014; Revised 8 July 2014; Accepted 8 July 2014; Published 17 July 2014 Academic Editor: omas Van Groen Copyright © 2014 Elisabet Ortiz-Tudela et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Introduction. Patients with dementia, especially Alzheimer’s disease, present several circadian impairments related to an accelerated perturbation of their biological clock that is caused by the illness itself and not merely age-related. us, the objective of this work was to elucidate whether these circadian system alterations were already present in patients with mild cognitive impairment (MCI), as compared to healthy age-matched subjects. Methods. 40 subjects (21 patients diagnosed with MCI, 74.1 ± 1.5 y.o., and 19 healthy subjects, 71.7 ± 1.4 y.o.) were subjected to ambulatory monitoring, recording wrist skin temperature, motor activity, body position, and the integrated variable TAP (including temperature, activity, and position) for one week. Nonparametrical analyses were then applied. Results. MCI patients exhibited a significant phase advance with respect to the healthy group for the following phase markers: temperature M5 (mean ± SEM: 04:20 ± 00:21 versus 02:52 ± 00:21) and L10 (14:35 ± 00:27 versus 13:24 ± 00:16) and TAP L5 (04:18 ± 00:14 versus 02:55 ± 00:30) and M10 (14:30 ± 00:18 versus 13:28 ± 00:23). Conclusions. ese results suggest that significant advances in the biological clock begin to occur in MCI patients, evidenced by an accelerated aging of the circadian clock, as compared to a healthy population of the same age. 1. Introduction Normal aging is accompanied by a progressive impairment of circadian rhythms [1]. ese changes include higher frag- mentation, lower amplitude, and a phase advance of the rest- activity and temperature rhythms [2–4] parallel to impair- ment of the sleep-wake architecture [2, 5]. e modifications observed with aging have also been related to a progressive impairment in cognitive performance [5]. Furthermore, an exacerbation of these changes in the circadian system is also found with Alzheimer’s disease (AD) [6]. Mild cognitive impairment (MCI) is a heterogeneous condition in which subjects belonging to the amnestic sub- group present a high risk of developing dementia [7], with conversion rates to AD close to 12% per year [8]. Compared to the relatively large number of articles devoted to the study of circadian alterations in AD, only scarce and sometimes contradictory data are available on the possible impairment of the circadian system in MCI. In this sense, a phase delay of the rest-activity rhythm has been recognized as a risk factor for developing MCI [9, 10]. On the contrary, a phase advance in the dim light melatonin onset, the gold standard for circadian phase assessment, has been reported in MCI patients [11]. e use of a single circadian marker for circadian assessment in such patients with low circadian robustness could explain such discrepancies. Furthermore, internal desynchrony among the different rhythms could also account for these inconsistencies. As a result, reliable evaluation through multichannel ambulatory monitoring of the status of the circadian system is beginning to receive Hindawi Publishing Corporation BioMed Research International Volume 2014, Article ID 524971, 7 pages http://dx.doi.org/10.1155/2014/524971
-
Upload
nguyenquynh -
Category
Documents
-
view
227 -
download
0
Transcript of Research Article The Characterization of Biological Rhythms...

Research ArticleThe Characterization of Biological Rhythms inMild Cognitive Impairment
Elisabet Ortiz-Tudela,1 Antonio Martinez-Nicolas,1 Carmen Díaz-Mardomingo,2
Sara García-Herranz,2 Inmaculada Pereda-Pérez,3 Azucena Valencia,3 Herminia Peraita,2
César Venero,3 Juan Antonio Madrid,1 and Maria Angeles Rol1
1 Chronobiology Laboratory, Department of Physiology, Faculty of Biology, University of Murcia, Campus de Espinardo,Espinardo, 30100 Murcia, Spain
2Department of Basic Psychology, Universidad Nacional de Educacion a Distancia (UNED), 28040 Madrid, Spain3 Department of Psychobiology, Universidad Nacional de Educacion a Distancia (UNED), 28040 Madrid, Spain
Correspondence should be addressed to Juan Antonio Madrid; [email protected]
Received 8 May 2014; Revised 8 July 2014; Accepted 8 July 2014; Published 17 July 2014
Academic Editor: Thomas Van Groen
Copyright © 2014 Elisabet Ortiz-Tudela et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Introduction. Patients with dementia, especially Alzheimer’s disease, present several circadian impairments related to an acceleratedperturbation of their biological clock that is caused by the illness itself and not merely age-related. Thus, the objective of this workwas to elucidate whether these circadian system alterations were already present in patients withmild cognitive impairment (MCI),as compared to healthy age-matched subjects.Methods. 40 subjects (21 patients diagnosed with MCI, 74.1 ± 1.5 y.o., and 19 healthysubjects, 71.7 ± 1.4 y.o.) were subjected to ambulatory monitoring, recording wrist skin temperature, motor activity, body position,and the integrated variable TAP (including temperature, activity, and position) for one week. Nonparametrical analyses were thenapplied. Results. MCI patients exhibited a significant phase advance with respect to the healthy group for the following phasemarkers: temperature M5 (mean ± SEM: 04:20 ± 00:21 versus 02:52 ± 00:21) and L10 (14:35 ± 00:27 versus 13:24 ± 00:16) andTAP L5 (04:18 ± 00:14 versus 02:55 ± 00:30) and M10 (14:30 ± 00:18 versus 13:28 ± 00:23). Conclusions. These results suggest thatsignificant advances in the biological clock begin to occur inMCI patients, evidenced by an accelerated aging of the circadian clock,as compared to a healthy population of the same age.
1. Introduction
Normal aging is accompanied by a progressive impairmentof circadian rhythms [1]. These changes include higher frag-mentation, lower amplitude, and a phase advance of the rest-activity and temperature rhythms [2–4] parallel to impair-ment of the sleep-wake architecture [2, 5]. The modificationsobserved with aging have also been related to a progressiveimpairment in cognitive performance [5]. Furthermore, anexacerbation of these changes in the circadian system is alsofound with Alzheimer’s disease (AD) [6].
Mild cognitive impairment (MCI) is a heterogeneouscondition in which subjects belonging to the amnestic sub-group present a high risk of developing dementia [7], withconversion rates to AD close to 12% per year [8]. Compared
to the relatively large number of articles devoted to the studyof circadian alterations in AD, only scarce and sometimescontradictory data are available on the possible impairmentof the circadian system in MCI. In this sense, a phasedelay of the rest-activity rhythm has been recognized as arisk factor for developing MCI [9, 10]. On the contrary, aphase advance in the dim light melatonin onset, the goldstandard for circadian phase assessment, has been reportedin MCI patients [11]. The use of a single circadian markerfor circadian assessment in such patients with low circadianrobustness could explain such discrepancies. Furthermore,internal desynchrony among the different rhythms couldalso account for these inconsistencies. As a result, reliableevaluation through multichannel ambulatory monitoring ofthe status of the circadian system is beginning to receive
Hindawi Publishing CorporationBioMed Research InternationalVolume 2014, Article ID 524971, 7 pageshttp://dx.doi.org/10.1155/2014/524971

2 BioMed Research International
attention [12, 13]. A better understanding of the changes inthis system would aid in the implementation of preventiontherapies, such as controlled bright light therapy and/ormelatonin administration, which have already proven theirrelevance in these pathologies [14].
To this end, in this study we propose the integration of3 circadian rhythms, wrist temperature, motor activity, andbody position, into the composite variable TAP [12] in orderto describe circadian system alterations associated withMCI.
2. Methods
2.1. Study Group. Our study is part of a larger ongoing studyin which 247 participants are being followed for several yearsin order to determine the prevalence and stability of the dif-ferent MCI subtypes [15, 16]. The participants were recruitedin the Autonomous Community of Madrid (ACM, Spain).The larger sample of participants was originally a mixedsample of individuals presenting mild cognitive impair-ment and unimpaired subjects.
The inclusion criteria resulted in a sample of subjectsaged between 65 and 90 y.o. who volunteered to participate inthe study and agreed to follow-up visits and different assess-ments. Conversely, medical conditions such as neurode-generative disease, severe cognitive impairment, disablingchronic diseases, psychiatric disorders, marked neurologicalabnormalities (aphasia, agraphia, and/or apraxia), severesensory deficits, depression, diabetes, and cerebrovascularaccidents were considered to be exclusion criteria. Both theinclusion and exclusion criteria have been previously definedby Venero et al. (2013) [15].
From the initial group of 247 subjects participating inthe previous study [15], we selected a subsample to matchcognitive condition (based on psychometric criteria, accord-ing to the standard guidelines [17]), gender, and age betweenthe mild cognitive impairment and control groups and whoagreed to rhythm monitoring during a one-week period.Our subsample consisted of 40 subjects, 21 of whom werediagnosed as suffering fromMCI (6 nonamnestic, 2 amnestic,and 13 multidomain) (74.1 ± 1.5 y.o.) and an age-matchedhealthy population of 19 subjects (71.7 ± 1.4 y.o., 𝑃 > 0.05)for age comparisons between healthy and MCI subjects. Themultidomain subgroup exhibited no differences in age withrespect to the healthy group (71.7 ± 1.4 y.o. versus 73.9 ± 1.1for healthy and MD subjects, respectively; 𝑃 = 0.22). Withrespect to gender, the control group consisted of a sampleof 14 women and 5 men, while the MCI group included 15women and 6 men.
During this time, all subjects were submitted to cognitiveassessment (including the episodic memory Verbal LearningTest from Complutense University, TAVEC; the Spanishversion of the Mini-Mental State Examination (MMSE); theYesavage Scale to assess the participant’s emotional state;the Blessed Dementia Scale as a personal autonomy scale;several language tests for phonetic and semantic fluency; TrailMaking Test-A measuring attention span; Trail Making Test-B and alternating graphs and loops for executive function;and the Rey-Osterrieth complex figure test for constructivepraxis, among others), as detailed in Venero et al. (2013) [15].
These subjects also wore temperature, activity, body position,and luxometer sensors.
The study was approved by the Ethics and ResearchCommittee at the UNED (Spanish National University ofDistance Education) and the University of Murcia (SPAIN),and all participants provided written consent to perform theneuropsychological test battery and wear the sensors for oneweek. The study also abided by the Helsinki Declaration of1975 (revised in 2013).
2.2. Rhythm Assessment
2.2.1. Temperature Rhythm. Wrist temperature rhythm wasassessed continuously for 7 days using a temperature sen-sor (Thermochron iButton DS1921H, Dallas, Maxim) pro-grammed to sample once every 10 minutes; said monitoringdevice was attached as previously described [12, 18].
2.2.2. Body Position and Rest-Activity Rhythm. Thebody pos-ition and rest-activity rhythms were assessed over the courseof the same 7 days using an actimeter (Hobo Pendant G Ac-celeration Data Logger) placed on the nondominant arm.
The sensor was programmed to record data every 30 sec-onds, and the variables were obtained as described by Ortiz-Tudela et al. (2010) [12].
2.2.3. TAP Computation. Wrist temperature, motor activity,and body position were combined according to the algo-rithms described by Ortiz-Tudela et al. (2010) [12] in order toobtain the integrated TAP variable. TAP values ranged from0 to 1. Values near 1 indicate a low wrist temperature, a highlevel of activity, and a vertical arm position, suggesting a highlevel of activation, whereas values near 0 correspond to a highwrist temperature, a low level of activity, and a horizontal armposition, which is compatible with quiet sleep.
2.2.4. Environmental Light-Exposure Recording. All subjectswere required to wear a HOBO Pendant Temperature/LightData Logger UA-002-64 (Onset Computer, Bourne, Mas-sachusetts, USA) on a lanyard close to their eyes to recordlight exposure.
Participants were instructed to wear the luxometer overtheir clothing and to leave it on the bedside table as they slept,according to previously described methodology [19].
2.2.5. Temporal Series Analysis. In order to characterize thecircadian pattern for TAP and each individual variable, weperformed the following nonparametric analysis (as previ-ously described by van Someren et al. (1999) [20]).
Interdaily Stability (IS). This quantifies rhythm stability overdifferent days. It varies between 0 for Gaussian noise and 1 fora perfect stability, where the rhythm repeats itself exactly, dayafter day.Intradaily Variability (IV). This parameter shows the frag-mentation of the rhythm. Its values oscillate between 0 (whenthe wave is perfectly sinusoidal) and 2 (Gaussian noise).
PhaseMarkers.The timing of the ten or five consecutive hourswith the lowest values (L10 and L5, resp.) and the timing

BioMed Research International 3
of the ten or five consecutive hours with the highest values(M10 andM5, resp.) were calculated. M5 for temperature andL5 for activity, position, TAP, and light exposure representedthe phase markers occurring during the night, while L10 fortemperature and M10 for activity, position, TAP, and lightexposure were the phase markers during the day.
Relative Amplitude (RA).This refers to the difference betweenthemean values of the ten consecutive hours with the highestvalues and the mean values of the five consecutive hours withthe lowest values (VM10 and VL5, resp.) divided by VM10 +VL5; to facilitate comparisons among variables, the differencebetween the VL10 and VM5 divided by VL10 + VM5 was alsoused. This parameter was multiplied by ten for temperature.
Circadian Function Index (CFI). CFI incorporates threeparameters (IV, IS, and RA) and can be calculated for anyvariable. IV values were inverted and normalized between 0and 1, with 0 being a noise signal and 1 a perfect sinusoid.Finally, CFI was calculated as the average of these three para-meters. Consequently, CFI oscillates between 0 (absence ofcircadian rhythmicity) and 1 (a robust circadian rhythm)[12].
Wrist Temperature Increase Onset (WTiO). This parameterhas recently been described by Bonmati-Carrion et al. (2014)[21] and has been shown to be very closely correlated withthe Dim Light Melatonin Onset (DLMO). According to itsdefinition, we calculated L2 and M5 for wrist temperatureand their corresponding VL2 and VM5 (i.e., the center ofthe period of the 2 and 5 consecutive hours of lowest (L2)and highest (M5) values of wrist temperature).Therefore, theWTiO corresponds to the time when 35% of the differencebetween L2 and M5 is achieved after L2.
2.3. Statistical Analyses. Firstly, descriptive statistics werecalculated for every parameter chosen. Comparisons betweenthe distribution of the recorded variables according to time(when averaging data on an hourly basis) and group (MCIor healthy) were performed by a repeated-measures ANOVA(significance level set at 𝑃 < 0.05) and post hoc comparisonsusing Bonferroni’s test.
A Student’s 𝑡-test was applied when comparisons fordemographic characteristics (age and cognitive state), non-parametrical parameters, and WTiO between two groupswere performed. Thus, the values for each parameter werecompared between healthy and MCI subjects and betweenhealthy and multidomain subjects. The interest in evaluatingthe differences between the healthy andMD subgroups lies inthe fact that themultidomain subgroup exhibits amore severecognitive impairment and a brain activity similar to that seenin Alzheimer’s disease patients (Lopez et al., 2014) [22].
The statistical analyses were performed using the PASWStatistics 18 software (IBM, USA).
3. Results
3.1. Overall Rhythm View. Both MCI patients and healthysubjects showed altered circadian patterns of wrist
temperature, motor activity, body position, and TAP thatwere characteristic of aged persons [1, 3, 4, 12, 19, 21, 23, 24].However, subjects with MCI showed a clear phase advancefor some markers of the circadian system.
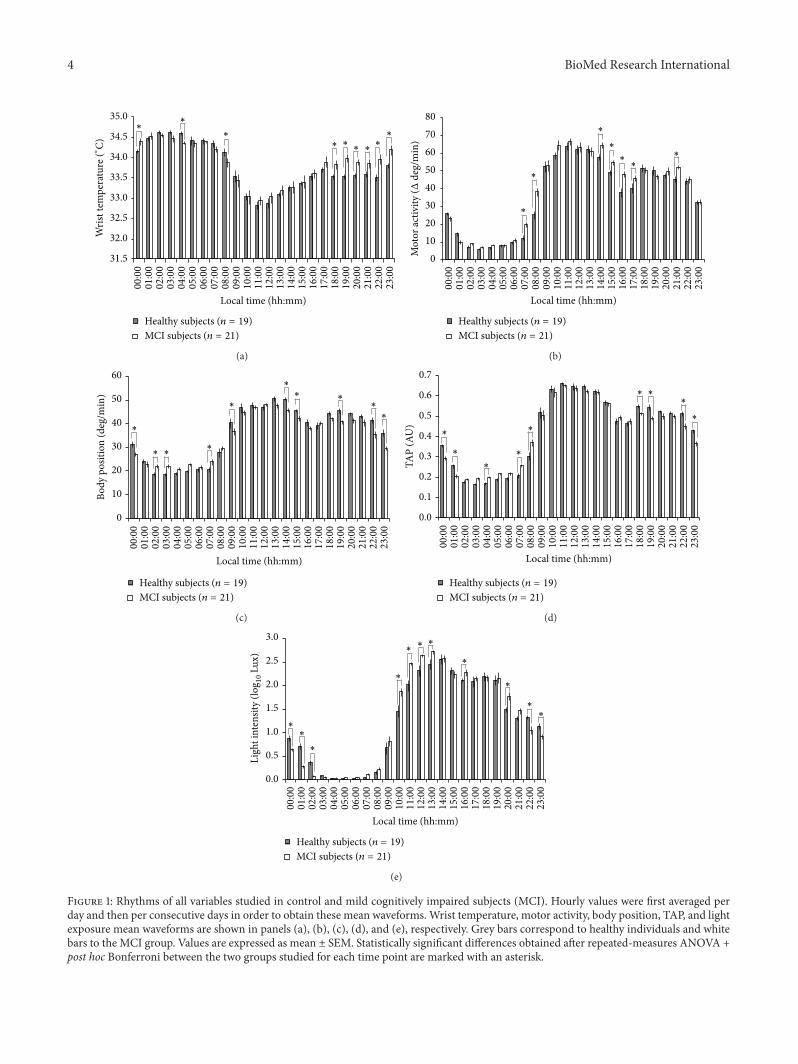
With respect to the wrist temperature rhythm (Figure1(a)), thewakemaintenance zone disappeared in both groups.This time interval of minimal sleep probability coincideswith minimal values of daily distal temperatures in healthyadults, usually between 20:00 and 22:00 h [12, 18]. This isin contrast to our findings, where the minimal values wereshifted to just after the moment of awakening. However,this alteration was more pronounced in MCI subjects, whopresented statistically significant higher temperature values(𝑃 < 0.05) than healthy controls between 20:00 h and 22:00 hbut also at 17:00 h, 18:00 h, 23:00 h, and 00:00 h.
The motor activity rhythm (Figure 1(b)) exhibited sig-nificantly higher values (𝑃 < 0.05) for MCI subjects at07:00 h and 08:00 h (suggesting an earlier activation of thesesubjects), around the postprandial hours (14:00 to 17:00), andat 21:00 h with respect to healthy subjects.
Both body position (Figure 1(c)) and the integrated vari-able TAP (Figure 1(d)) exhibited a general trend towardsnocturnal activation in MCI subjects. Statistically significant(𝑃 < 0.05) higher values were found in the MCI group forTAP at 04:00 h and 07:00 h and for body position at 02:00 h,03:00 h, and 07:00 h. However, a reduced activation wasdetected during the daytime in MCI, with lower statisticallysignificant values for comparisons between MCI and healthysubjects for TAP at 18:00 h, 19:00 h, 22:00 h, and 23:00 h andfor body position at 14:00 h, 15:00 h, 19:00 h, 22:00 h, and23:00 h, 𝑃 < 0.05.
MCI subjects were exposed to high levels of light (Figure1(e)) earlier than healthy subjects, as their light intensitylevels were significantly higher from 10:00 h to 13:00 h, and at16:00 h and 20:00 h. On the contrary, healthy subjects showedsignificantly higher light exposure from 22:00 h to 02:00 h.
3.2. Nonparametrical Characterization of Rhythms. Whencomparing nonparametrical indexes between healthy andMCI groups, significant differences were found with respectto timing (Table 1). Thus, a consistent phase advance in MCIsubjects was evident forwrist temperatureM5 and L10, aswellas for TAP L5 and M10.
Furthermore, when focusing on the most severelyaffected MCI subjects in our sample as determined bylower scores on the Mini-Mental State Examination and thepsychometric evaluation [15], that is, the multidomain (MD)subgroup (𝑛 = 13), a phase advance was once again con-firmed for wrist temperature rhythm M5 (𝑃 = 0.009) andL10 (𝑃 = 0.042) and for TAP L5 (𝑃 = 0.012), as com-pared to healthy subjects (Table 1). Although this phaseadvance was consistently observed for the remaining vari-ables, statistical significance was not achieved. When exam-ining the multidomain group (𝑛 = 13) with respect to theremaining mild cognitive impaired subjects (𝑛 = 8), that is,MCI subjects not included in the MD subgroup, we founda significant phase advance in the MD subgroup for M10(15:29±00:46 versus 13:31±00:21, 𝑃 = 0.02), a phase markerfor the rest-activity rhythm.
4 BioMed Research International
31.5
32.0
32.5
33.0
33.5
34.0
34.5
35.0
00:0
001
:00
02:0
003
:00
04:0
005
:00
06:0
007
:00
08:0
009
:00
10:0
011
:00
12:0
013
:00
14:0
015
:00
16:0
017
:00
18:0
019
:00
20:0
021
:00
22:0
023
:00
Local time (hh:mm)
Healthy subjects (n = 19)MCI subjects (n = 21)
Wris
t tem
pera
ture
(∘C)
∗∗
∗
∗ ∗∗ ∗
∗
∗
(a)
01020304050607080
00:0
001
:00
02:0
003
:00
04:0
005
:00
06:0
007
:00
08:0
009
:00
10:0
011
:00
12:0
013
:00
14:0
015
:00
16:0
017
:00
18:0
019
:00
20:0
021
:00
22:0
023
:00
Local time (hh:mm)
Healthy subjects (n = 19)MCI subjects (n = 21)
∗
∗
∗
∗
∗∗
∗
Mot
or ac
tivity
(Δde
g/m
in)
(b)
0
10
20
30
40
50
60
00:0
001
:00
02:0
003
:00
04:0
005
:00
06:0
007
:00
08:0
009
:00
10:0
011
:00
12:0
013
:00
14:0
015
:00
16:0
017
:00
18:0
019
:00
20:0
021
:00
22:0
023
:00
Body
pos
ition
(deg
/min
)
Local time (hh:mm)
∗
∗ ∗∗
∗
∗
∗ ∗∗
∗
Healthy subjects (n = 19)MCI subjects (n = 21)
(c)
TAP
(AU
)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
00:0
001
:00
02:0
003
:00
04:0
005
:00
06:0
007
:00
08:0
009
:00
10:0
011
:00
12:0
013
:00
14:0
015
:00
16:0
017
:00
18:0
019
:00
20:0
021
:00
22:0
023
:00
Local time (hh:mm)
∗
∗
∗
∗
∗
∗ ∗∗
∗
Healthy subjects (n = 19)MCI subjects (n = 21)
(d)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
00:0
001
:00
02:0
003
:00
04:0
005
:00
06:0
007
:00
08:0
009
:00
10:0
011
:00
12:0
013
:00
14:0
015
:00
16:0
017
:00
18:0
019
:00
20:0
021
:00
22:0
023
:00
Local time (hh:mm)
∗∗
∗
∗
∗∗ ∗
∗
∗
∗
∗
Healthy subjects (n = 19)MCI subjects (n = 21)
Ligh
t int
ensit
y (lo
g 10
Lux)
(e)
Figure 1: Rhythms of all variables studied in control and mild cognitively impaired subjects (MCI). Hourly values were first averaged perday and then per consecutive days in order to obtain these mean waveforms. Wrist temperature, motor activity, body position, TAP, and lightexposure mean waveforms are shown in panels (a), (b), (c), (d), and (e), respectively. Grey bars correspond to healthy individuals and whitebars to the MCI group. Values are expressed as mean ± SEM. Statistically significant differences obtained after repeated-measures ANOVA +post hoc Bonferroni between the two groups studied for each time point are marked with an asterisk.

BioMed Research International 5
Table 1: Nonparametrical characterization of the study group.
Healthy MCI MD MCI except MDWrist temperature
IS 0.49 ± 0.04 0.43 ± 0.04 0.41 ± 0.05 0.46 ± 0.07IV 0.20 ± 0.02 0.20 ± 0.02 0.19 ± 0.03 0.22 ± 0.03RA 0.25 ± 0.02 0.23 ± 0.02 0.22 ± 0.02 0.25 ± 0.05M5 04:20 ± 00:211a 02:52 ± 00:212 02:53 ± 00:22b 06:26 ± 02:31L10 14:35 ± 00:271a 13:24 ± 00:162 13:18 ± 00:20b 14:32 ± 00:50CFI 0.55 ± 0.02 0.52 ± 0.02 0.51 ± 0.02 0.53 ± 0.04
Motor activityIS 0.45 ± 0.02 0.46 ± 0.02 0.49 ± 0.02 0.41 ± 0.05IV 0.77 ± 0.03 0.73 ± 0.03 0.73 ± 0.03 0.73 ± 0.05RA 0.78 ± 0.02 0.80 ± 0.02 0.80 ± 0.03 0.81 ± 0.04L5 03:48 ± 00:11 03:23 ± 00:13 03:10 ± 00:17 03:55 ± 00:25M10 14:34 ± 00:17 14:08 ± 00:21 13:31 ± 00:21∗ 15:29 ± 00:46∗
CFI 0.62 ± 0.02 0.63 ± 0.01 0.64 ± 0.02 0.62 ± 0.02Body position
IS 0.50 ± 0.04 0.47 ± 0.05 0.49 ± 0.06 0.44 ± 0.07IV 0.31 ± 0.02 0.33 ± 0.03 0.32 ± 0.03 0.34 ± 0.05RA 0.47 ± 0.04 0.43 ± 0.04 0.45 ± 0.05 0.41 ± 0.06L5 04:34 ± 00:29 02:53± 00:47 03:01 ± 00:57 03:46 ± 01:21M10 14:30 ± 00:45 12:57 ± 00:57 12:50 ± 01:17 12:01 ± 01:37CFI 0.61 ± 0.03 0.58 ± 0.03 0.59 ± 0.04 0.56 ± 0.04
TAPIS 0.61 ± 0.03 0.57 ± 0.04 0.60 ± 0.04 0.53 ± 0.10IV 0.26 ± 0.02 0.28 ± 0.02 0.28 ± 0.02 0.27 ± 0.04RA 0.55 ± 0.03 0.49 ± 0.04 0.51 ± 0.04 0.48 ± 0.08L5 04:18 ± 00:141a 02:55 ± 00:302 03:15 ± 00:19b 03:36 ± 00:27M10 14:30 ± 00:181a 13:28 ± 00:232 13:30 ± 00:23 13:57 ± 00:54CFI 0.68 ± 0.02 0.64 ± 0.03 0.65 ± 0.03 0.62 ± 0.06
Light exposureIS 0.64 ± 0.03 0.68 ± 0.02 0.67 ± 0.02 0.70 ± 0.03IV 0.26 ± 0.02 0.25 ± 0.01 0.27 ± 0.01 0.23 ± 0.02RA 0.98 ± 0.01 0.97 ± 0.01 0.98 ± 0.01 0.96 ± 0.02L5 04:17 ± 00:09 03:56 ± 00:13 03:43 ± 00:08 04:17 ± 00:20M10 14:29 ± 00:15 14:18 ± 00:05 14:11 ± 00:05 14:29 ± 00:07CFI 0.83 ± 0.01 0.84 ± 0.01 0.84 ± 0.01 0.85 ± 0.02These indexes were calculated throughout the study for the healthy group (𝑛 = 19), the cognitively impaired group (MCI, 𝑛 = 21), the multidomain subgroup(MD, 𝑛 = 13), and MCI patients excluding the multidomain subgroup (MCI except MD, 𝑛 = 8).Student’s 𝑡-tests were used to compare the healthy andMCI groups (different numbers, “1” and “2”, indicate statistically significant differences), the healthy andMD subgroups (different letters, “a” and “b”, indicate statistically significant differences), and the MD subgroup and the rest of the MCI patients (an asteriskmarks statistically significant differences). In addition, significant differences are highlighted in bold.All values are expressed as mean ± SEM.IS stands for interdaily stability; IV for intradaily variability; RA for relative amplitude; M5 and M10 for the center of the consecutive period of 5 and 10 hoursof maximum values, respectively; L10 and L5 indicate the consecutive 10- and 5-hour periods of minimum values, respectively; and CFI corresponds to thecircadian function index.
TheWTiO parameter was determined to occur at 22:48±00:34 h and 21:49 ± 00:23 h for healthy and mild cognitivelyimpaired patients, respectively. Despite the tendency to bephase-advanced in MCI subjects as well, this difference wasnot significant (𝑃 = 0.156).
4. Discussion
Our study, complementing that previously published byVenero et al. (2013) [15], highlights differences that beginto occur in the circadian timing system of MCI subjects.

6 BioMed Research International
We found that the MCI group presented a phase advancein temperature, activity, position, TAP, and light exposurerhythms with respect to a healthy age-matched population.
Inconsistent changes in circadian timing have alreadybeen reported for the rest-activity rhythm in MCI. In thissense, Cochrane et al. (2012) [25] observed a phase delayin this rhythm in MCI subjects. Furthermore, other studieshave identified this phase delay of the rest-activity rhythmas a predictor for developing MCI [9, 10]. However, arecent study combining polysomnography, actigraphy, andmelatonin analysis showed a clear phase advance in sleep anddim lightmelatonin onset in patients withMCI [11], similar tothat observed by us using rhythmic multivariable recordings.Moreover, in our study, this phase advance was also signifi-cant in the subgroup of patients with MD, characterized bymultiple domain impairment, in contrast to single amnesticMCI and nonamnesticMCI.This circadian alteration is simi-lar to that observed during normal aging, since elderly peopleconsistently show a phase advance in their circadian rhythms[2]. This discrepancy between our study and the results ofCochrane (2012) [25], Schlosser Covell et al. (2012) [10], andTranah (2011) [9] could be possibly attributed to how phasesare calculated. These authors calculate the acrophase of therest-activity rhythm using the cosinor method. Thus, a sinewave fit to a time series [26] is compulsory, while a nonpara-metrical rhythm characterization does not assume any wave-form a priori [20].The rest-activity rhythm resembles more asquared wave than a sine wave, and given the nocturnal agita-tion called “sundowning” that appears in AD [6, 8], the cosi-normay delay themoment of maximum activity (acrophase).
5. Conclusions
Altogether, and taking into account the exploratory natureof the study, it seems that MCI subjects begin to experiencesome of the early circadian rhythms disturbances associatedwith premature aging and AD, which are especially patentin those subjects categorized in the multidomain group.Furthermore, the TAP variable may be a relevant tool forthese studies, in which a multiple-rhythm assessment couldcontribute to a better understanding of the pathology studied.This is especially true considering that TAP provides a moreglobal insight into circadian system status, overcoming arti-facts that influence isolated variables. These results empha-size the potential benefits of chronoenhancement therapiesalready proposed [8], which could help resynchronize thebiological clock and thus prevent some of the symptomssuffered by these patients.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
Acknowledgments
The authors wish to thank M. Martınez for kindly reviewingthe paper, the Instituto de Salud Carlos III, the Ministryof Science and Innovation, and the Ministry of Economy
and Competitiveness for their financial support of this studythrough the Red de Investigacion Cooperativa en Envejeci-miento y Fragilidad (The Ageing and Frailty CooperativeResearchNetwork), RETICEF (RD06/0013/0019, RD06/0013/1027, RD12/0043/0011, SEJ 2007/63325, BFU 2010-21945-CO1,and IPT-2011-0833-900000), the latter two including FEDERcofunding granted to JuanAntonioMadrid. Furthermore, theauthors wish to thank the Ministry of Education and Sciencefor the research fellowship awarded to Elisabet Ortiz-Tudela(AP2008-2850), and the UNED for the research fellowshipawarded to Inmaculada Pereda-Perez.
References
[1] B. L. Myers and P. Badia, “Changes in circadian rhythms andsleep quality with aging: mechanisms and interventions,” Neu-roscience and Biobehavioral Reviews, vol. 19, no. 4, pp. 553–571,1995.
[2] D.Dijk, J. F.Duffy, andC.A.Czeisler, “Contribution of circadianphysiology and sleep homeostasis to age-related changes inhuman sleep,” Chronobiology International, vol. 17, no. 3, pp.285–311, 2000.
[3] D. Weinert and J. Waterhouse, “The circadian rhythm of coretemperature: effects of physical activity and aging,” Physiologyand Behavior, vol. 90, no. 2-3, pp. 246–256, 2007.
[4] J. M. Oosterman, E. J. W. van Someren, R. L. C. Vogels, B. vanHarten, andE. J. A. Scherder, “Fragmentation of the rest-activityrhythm correlates with age-related cognitive deficits,” Journal ofSleep Research, vol. 18, no. 1, pp. 129–135, 2009.
[5] E. F. Pace-Schott and R. M. C. Spencer, “Age-related changes inthe cognitive function of sleep,” Progress in Brain Research, vol.191, pp. 75–89, 2011.
[6] D. A. Weldemichael and G. T. Grossberg, “Circadian rhythmdisturbances in patients with Alzheimer’s disease: a review,”International Journal of Alzheimer’s Disease, vol. 2010, ArticleID 716453, 9 pages, 2010.
[7] B. Dubois, H. H. Feldman, C. Jacova et al., “Research criteriafor the diagnosis of Alzheime's disease: revising the NINCDS-ADRDA criteria,” The Lancet Neurology, vol. 6, no. 8, pp. 734–746, 2007.
[8] D. P. Cardinali, A. M. Furio, and L. I. Brusco, “Clinical aspectsof melatonin intervention in Alzheimer’s disease progression,”Current Neuropharmacology, vol. 8, no. 3, pp. 218–227, 2010.
[9] G. J. Tranah, T. Blackwell, K. L. Stone et al., “Circadian activityrhythms and risk of incident dementia and mild cognitiveimpairment in older women,” Annals of Neurology, vol. 70, no.5, pp. 722–732, 2011.
[10] G. E. Schlosser Covell, P. S. Dhawan, J. K. Lee Iannotti et al.,“Disrupted daytime activity and altered sleep-wake patternsmay predict transition to mild cognitive impairment or demen-tia: a critically appraised topic,” Neurologist, vol. 18, no. 6, pp.426–429, 2012.
[11] S. L. Naismith, I. B. Hickie, Z. Terpening et al., “Circadian mis-alignment and sleep disruption in mild cognitive impairment,”Journal of Alzheimer’s Disease, vol. 38, no. 4, pp. 857–866, 2014.
[12] E. Ortiz-Tudela, A. Martinez-Nicolas, M. Campos, M. A. Rol,and J. A.Madrid, “Anew integrated variable based on thermom-etry, actimetry and body position (TAP) to evaluate circadiansystem status in humans,” PLoS Computational Biology, vol. 6,no. 11, Article ID e1000996, 2010.
BioMed Research International 7
[13] V. Kolodyazhniy, J. Spati, S. Frey et al., “An improvedmethod forestimating human circadian phase derived from multichannelambulatorymonitoring and artificial neural networks,”Chrono-biology International, vol. 29, no. 8, pp. 1078–1097, 2012.
[14] R. F. Riemersma-van der Lek, D. F. Swaab, J. Twisk, E. M. Hol,W. J. G. Hoogendijk, and E. J. W. van Someren, “Effect of brightlight and melatonin on cognitive and noncognitive functionin elderly residents of group care facilities: a randomized con-trolled trial,” The Journal of the American Medical Association,vol. 299, no. 22, pp. 2642–2655, 2008.
[15] C. Venero, C. Dıaz-Mardomingo, I. Pereda-Perez et al., “In-creased morning salivary cortisol levels in older adults withnonamnestic and multidomain mild cognitive impairment,”Psychoneuroendocrinology, vol. 38, no. 4, pp. 488–498, 2013.
[16] H. Peraita, S. Garcıa-Herranz, and C. Dıaz-Mardomingo, “Evo-lution of specific cognitive subprofiles of mild cognitive impair-ment in a three-year longitudinal study,” Current Aging Science,vol. 4, no. 2, pp. 171–182, 2011.
[17] R. C. Petersen, “Mild cognitive impairment as a diagnosticentity,” Journal of Internal Medicine, vol. 256, no. 3, pp. 183–194,2004.
[18] J. A. Sarabia, M. A. Rol, P. Mendiola, and J. A. Madrid, “Circa-dian rhythm of wrist temperature in normal-living subjects Acandidate of new index of the circadian system,” Physiology &Behavior, vol. 95, no. 4, pp. 570–580, 2008.
[19] A. Martinez-Nicolas, E. Ortiz-Tudela, J. A. Madrid, and M. A.Rol, “Crosstalk between environmental light and internal timein humans,” Chronobiology International, vol. 28, no. 7, pp. 617–629, 2011.
[20] E. J. W. van Someren, D. F. Swaab, C. C. Colenda, W. Cohen,W. V. McCall, and P. B. Rosenquist, “Bright light therapy:improved sensitivity to its effects on rest- activity rhythms inAlzheimer patients by application of nonparametric methods,”Chronobiology International, vol. 16, no. 4, pp. 505–518, 1999.
[21] M. A. Bonmati-Carrion, B. Middleton, V. Revell, D. J. Skene, M.A. Rol, and J. A. Madrid, “Circadian phase asessment by ambu-latory monitoring in humans: correlation with dim light mela-tonin onset,” Chronobiology International, vol. 31, no. 1, pp. 37–51, 2013.
[22] M. E. Lopez, P. Cuesta, P. Garces et al., “MEG spectral analysisin subtypes of mild cognitive impairment,”Age, vol. 36, no. 3, p.9624, 2014.
[23] A. Martinez-Nicolas, E. Ortiz-Tudela, M. A. Rol, and J. A.Madrid, “Uncovering different masking factors on wrist skintemperature rhythm in free-living subjects,” PLoS ONE, vol. 8,no. 4, Article ID e61142, 2013.
[24] A. Blazquez, A. Martinez-Nicolas, F. J. Salazar, M. A. Rol, and J.A. Madrid, “Wrist skin temperature, motor activity, and bodyposition as determinants of the circadian pattern of bloodpressure,” Chronobiology International, vol. 29, no. 6, pp. 747–756, 2012.
[25] A. Cochrane, I. H. Robertson, and A. N. Coogan, “Associationbetween circadian rhythms, sleep and cognitive impairment inhealthy older adults: an actigraphic study,” Journal of NeuralTransmission, vol. 119, no. 10, pp. 1233–1239, 2012.
[26] D. S. Minors and J. M. Waterhouse, “Mathematical and statis-tical analysis of circadian rhythms,” Psychoneuroendocrinology,vol. 13, no. 6, pp. 443–464, 1988.

Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporation http://www.hindawi.com
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttp://www.hindawi.com
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
International Journal of
Microbiology