Research Article Persistent Primitive Olfactory Artery in ...primitive olfactory artery (PO A)...
8
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 903460, 7 pages http://dx.doi.org/10.1155/2013/903460 Research Article Persistent Primitive Olfactory Artery in Serbian Population Ljiljana VasoviT, 1 Milena TrandafiloviT, 2 Slobodan VlajkoviT, 1 Ivan JovanoviT, 1 and SlaZana UgrenoviT 1 1 Department of Anatomy, Faculty of Medicine, University of Niˇ s, Boulevard Dr. Zoran Ðinđi´ c 81, 18000 Niˇ s, Serbia 2 Center for Biomedical Researches, Faculty of Medicine, University of Niˇ s, Boulevard Dr. Zoran Ðinđi´ c 81, 18000 Niˇ s, Serbia Correspondence should be addressed to Ljiljana Vasovi´ c; [email protected] Received 11 April 2013; Accepted 17 June 2013 Academic Editor: Hongjuan Liu Copyright © 2013 Ljiljana Vasovi´ c et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. e continuation of the cranial branch of the primitive internal carotid artery is called the primitive olfactory artery (POℓA). It takes this name according to the fact that it is mainly concerned with supplying the developing nasal region. We reported two new cases of the persistent POℓA (PPOℓA) in Serbian population aſter retrospective analysis of digital images of 200 fetal and 269 adult cases. is PPOℓA originated from the precommunicating part (A1) of the right anterior cerebral artery, coursed along the olfactory tract, and turned on the medial cerebral hemisphere in both male adults. Some vascular variations (fenestration of the A1 and the median artery of the corpus callosum) were associated with this persistent vessel. According to the fact that we did not find aneurysm in our previous and two recent cases, we are of the opinion that PPOℓA is usually asymptomatic in Serbian population. 1. Introduction During embryonic development of the vascular system, the primitive olfactory artery (POℓA) represents a continuation of the cranial branch of the primitive internal carotid artery (ICA) [1]. It may be presumed that a fenestration of the anterior cerebral artery (ACA) is the remnant of the embry- onal plexiform anastomosis between the ACA and the POℓA [2, 3]. Some authors noted that POℓA normally regresses to the remnant—the recurrent artery of Heubner (RAH) [4, 5]. Other authors supported this claim by the evidence of an aplasia of the RAH [6–8] and/or the anterior communicating artery [6, 9]. A persistence of the POℓA (PPOℓA) is very rare accord- ing to the fact that its incidence was noted in 0.14% [10] to 0.29% [11] of cases. Morphologically, the PPOℓA usually courses anterome- dially along the ipsilateral olfactory tract, and aſter a turn, it supplies the ACA territory [4]. Pathoanatomically, a relatively frequent location of an aneurysm on the hairpin bend of the PPOℓA emphasizes the importance of hemodynamic stress in this persistent primitive vessel [7, 12, 13]. Reports of single cases or retrospective studies about special and/or general features of the PPOℓA came usually from Japan [5–10, 12–17] and Korea [11, 18, 19], although there were case reports from UK [20], Taiwan [21], and Serbia [22]. Previous incidental finding of the PPOℓA in one adult cadaver [22], and the description of fenestration of the precommunicating part (A1) of the ACA [3] and/or RAH in fetuses [23], inspired us to a more detailed investigation of the POℓA persistence in Serbian population. 2. Materials and Methods We did a retrospective analysis of digital images of brain vessels of 200 fetal and 269 adult cadavers, dissected at the Department of Anatomy and Institute of Forensic Medicine in Niˇ s, respectively. 2.1. Fetal Cadavers. Fetuses of both genders, from 9 to 32 weeks of gestation, were a part of the collection of our Department of Anatomy, and they were used in the prepara- tion of doctoral thesis [24]. All fetuses were obtained legally from the Clinic of Gynecology and Obstetrics in Niˇ s. e Council for Postgraduate Study of the Faculty of Medicine in Niˇ s gave permission to investigate the fetal material. e arteries of fetuses were injected with Micropaque or latex
Transcript of Research Article Persistent Primitive Olfactory Artery in ...primitive olfactory artery (PO A)...

Hindawi Publishing CorporationBioMed Research InternationalVolume 2013, Article ID 903460, 7 pageshttp://dx.doi.org/10.1155/2013/903460
Research ArticlePersistent Primitive Olfactory Artery in Serbian Population
Ljiljana VasoviT,1 Milena TrandafiloviT,2 Slobodan VlajkoviT,1
Ivan JovanoviT,1 and SlaZana UgrenoviT1
1 Department of Anatomy, Faculty of Medicine, University of Nis, Boulevard Dr. Zoran Ðinđic 81, 18000 Nis, Serbia2 Center for Biomedical Researches, Faculty of Medicine, University of Nis, Boulevard Dr. Zoran Ðinđic 81, 18000 Nis, Serbia
Correspondence should be addressed to Ljiljana Vasovic; [email protected]
Received 11 April 2013; Accepted 17 June 2013
Academic Editor: Hongjuan Liu
Copyright © 2013 Ljiljana Vasovic et al.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The continuation of the cranial branch of the primitive internal carotid artery is called the primitive olfactory artery (POℓA). Ittakes this name according to the fact that it is mainly concerned with supplying the developing nasal region. We reported twonew cases of the persistent POℓA (PPOℓA) in Serbian population after retrospective analysis of digital images of 200 fetal and 269adult cases. This PPOℓA originated from the precommunicating part (A1) of the right anterior cerebral artery, coursed along theolfactory tract, and turned on the medial cerebral hemisphere in both male adults. Some vascular variations (fenestration of the A1and the median artery of the corpus callosum) were associated with this persistent vessel. According to the fact that we did not findaneurysm in our previous and two recent cases, we are of the opinion that PPOℓA is usually asymptomatic in Serbian population.
1. Introduction
During embryonic development of the vascular system, theprimitive olfactory artery (POℓA) represents a continuationof the cranial branch of the primitive internal carotid artery(ICA) [1]. It may be presumed that a fenestration of theanterior cerebral artery (ACA) is the remnant of the embry-onal plexiform anastomosis between the ACA and the POℓA[2, 3]. Some authors noted that POℓA normally regresses tothe remnant—the recurrent artery of Heubner (RAH) [4, 5].Other authors supported this claim by the evidence of anaplasia of the RAH [6–8] and/or the anterior communicatingartery [6, 9].
A persistence of the POℓA (PPOℓA) is very rare accord-ing to the fact that its incidence was noted in 0.14% [10] to0.29% [11] of cases.
Morphologically, the PPOℓA usually courses anterome-dially along the ipsilateral olfactory tract, and after a turn, itsupplies theACA territory [4]. Pathoanatomically, a relativelyfrequent location of an aneurysm on the hairpin bend of thePPOℓA emphasizes the importance of hemodynamic stressin this persistent primitive vessel [7, 12, 13].
Reports of single cases or retrospective studies aboutspecial and/or general features of the PPOℓA came usually
from Japan [5–10, 12–17] and Korea [11, 18, 19], although therewere case reports fromUK [20], Taiwan [21], and Serbia [22].
Previous incidental finding of the PPOℓA in one adultcadaver [22], and the description of fenestration of theprecommunicating part (A1) of the ACA [3] and/or RAH infetuses [23], inspired us to amore detailed investigation of thePOℓA persistence in Serbian population.
2. Materials and Methods
We did a retrospective analysis of digital images of brainvessels of 200 fetal and 269 adult cadavers, dissected at theDepartment of Anatomy and Institute of Forensic Medicinein Nis, respectively.
2.1. Fetal Cadavers. Fetuses of both genders, from 9 to 32weeks of gestation, were a part of the collection of ourDepartment of Anatomy, and they were used in the prepara-tion of doctoral thesis [24]. All fetuses were obtained legallyfrom the Clinic of Gynecology and Obstetrics in Nis. TheCouncil for Postgraduate Study of the Faculty of Medicinein Nis gave permission to investigate the fetal material. Thearteries of fetuses were injected with Micropaque or latex

2 BioMed Research International
through the left cardiac ventricle or through the commoncarotid artery. All fetuses were fixed in 10% formalin for2 weeks. Fetal brains were removed and kept in individualcalvarias. The measurements were performed by means ofan ocular micrometer mounted on an operating microscope(Olympus).
2.2. Adult Cadavers. The dissected brains originated fromcadavers of both genders, different ages (from the neonate to95 years), and different causes of death in the period between2006 and 2013. Investigation of these cases was in accordancewith the rules of the internal Ethics Committee (no. 01-9068-4) of our Faculty of Medicine. Morphological features ofbrain arteries (caliber, possible vessel’s abnormalities) wereobserved by using a magnifying glass and recorded on afilm. Measurement of the external diameter of arteries wasperformed by ImageJ (http://rsb.info.nih.gov/ij/index.html).
3. Results and Discussion
3.1. Results. We discovered two new cases of the PPOℓA inadults. The first case of the PPOℓA was found in a malecadaver, aged 58 and autopsied due to cardiac arrest; anothercasewas found in amale, aged 61, whodied due to polytraumaat the Orthopedic Clinic.
(1) Case I. The PPOℓA had a common origin with theRAH from the A1 of the right ACA at the level ofthe proximal part of the fenestration (Figure 1(a)). Itsbeginning was about 7mm away from ICA bifurca-tion.The caliber of the right A1 was 2.03mm, whereasthe caliber of the PPOℓA was 1.41mm. The latterfollowed the olfactory tract in the first part of itscourse, and after that, it turned and passed on themedial telencephalic surface. However, we did notphotograph its termination. In addition, the medianartery of the corpus callosum was also presented(Figure 1(b)).
(2) Case II. The PPOℓA was a branch of the right A1(Figure 2(a)).The beginning of the PPOℓAwas about6mm away from ICA bifurcation. The caliber ofthe right A1 was 2.50mm, whereas caliber of thePPOℓAwas 1.40mm.The latter followed the olfactorytract in the first part of its course, and after that,it passed similar to the callosomarginal artery; abihemispheric branch was also evidenced at the levelof its termination (Figure 2(b)). Ipsilaterally, the RAHoriginated from the PPOℓA; it was duplicated at thebeginning. Atherosclerotic plaques were significantlypresent at the cerebral arteries, especially along mainbrain arteries.
(3) Comparison of PPOℓAs in the Literature. Generaland special data about PPOℓAs in our and otherpopulations are presented in Table 1.
3.2. Discussion. Firstly, we noted some data and disagree-ments in the literature about the POℓAorigin [1, 6, 25], POℓArudiments [1] or a lack of embryologic explanation of A1
variable side branches [15, 26], as well as an origin [20] ortermination [8, 15] of the PPOℓA.
Moffat [1] described that POℓAhas a similar developmentin the rat’s and human embryos up to an 18mm stage. Duringthe development of vascular system in a 3.7mm embryo, thecontinuation of the dorsal aorta forms the primitive ICA [1],except for its first segment which was formed by the primitivethird aortic arch [6]. At the level of the forebrain the ICAgives the primitivemaxillary artery, and then ICAdivides intothe cranial and caudal branches. In embryos of 4 to 5.7mm(28–30 days), the cranial branch constitutes the primitiveolfactory artery (POℓA), which branches off the anteriorchoroidal and middle cerebral arteries [6]. According todata from the paper by Horie et al. [13], the definitiveACA extends superiorly between the cerebral hemispheres,associated with regression of the POℓA untill the 7th weekof gestation. According to the picture of human embryo inthe paper by Katayama et al. [14], the POℓA retains its originfrom the A1 to the 9mm embryonic stage. Komiyama [25]and Okahara et al. [6] stressed that the POℓA terminatesin the nasal fossa, and “secondary artery” constitutes themedial olfactory artery, which supplies the olfactory bulb.This medial olfactory artery becomes the ACA proper in an11.5 to 18mmembryo, while the terminal portion of the POℓAusually regresses. Kim et al. [27] noted the existence of theplexiformanastomosis between theACAand thePOℓA in theillustration of a 14mm embryo. Lateral olfactory branches ofthe POℓA include the RAH, anterior choroidal, lateral striate,and middle cerebral arteries. Moffat [1] noted that the POℓAin a 24mmhuman embryo forms an inconstant striate branchof the ACA.
Okahara et al. [6] noted that the PPOℓA arises only fromthe A1 part, as in cases described by Moffat [20] and Horieet al. [13], as well as in recent cases. In addition, we couldcompare the origin of PPOℓA from the A1 part in thesecases with the POℓA origin in an 18mm human embryowhose picture was displayed in the paper by Katayama etal. [14]. Tsutsumi et al. [8] described that PPOℓA originatedfrom A1-A2 junction. However, many authors described itsinternal carotid origin [7, 9, 14, 16, 19, 21]. In our previouscase the PPOℓA and posterior communicating artery hada common origin from the middle cerebral artery (MCA)[22]. It can be said that the case, described by Lin et al.[21], in which PPOℓA continued from an accessory MCA,resembles our case. Interesting anomaly was found in five ratembryos studied. In these specimens the cranial branch ofthe ICA terminated as the MCA, whereas the POℓA was acontinuation of the primitive maxillary artery [1].
Several types of the PPOℓA are described in the literature.In the first type described by Nozaki et al. [7] the PPOℓArose from the ICA, ran along the olfactory tract, and made ahairpin bend to supply the territory of the ACA postcommu-nicating part (A2). In the second type, described by the sameauthors, the PPOℓA rose from the ACA and passed throughthe cribriform plate of the ethmoid bone to supply the nasalcavity, similar to the ethmoidal arteries.The case described byEnomoto et al. [15], on computer tomography angiography(CTA), and the case described by Moffat [20] on autopsywere classified as the second type. Komiyama [25] noted that

BioMed Research International 3
Right Left
1
23
4
56
78
12910
11
∗
(a)
LeftRight
4
4
5∗
(b)
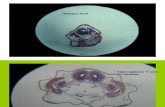
Figure 1: Persistent primitive olfactory artery (PPOℓA) as a side branch of the precommunicating part (A1) of the right anterior cerebralartery (ACA). It originates at the level of proximal end of the A1 fenestration (a) and courses to the medial surface of the frontal lobe (b).Cerebral part (C4) of the right internal carotid artery (1); left C4 (2); right A1 (3); A1 fenestration (∗); right PPOℓA (4); right recurrent arteryof Heubner (RAH) (5)); anterior communicating artery (ACoA) (6)); left A1 (7); left RAH (8); right postcommunicating part (A2) of the ACA(9); median artery of the corpus callosum (10); left A2 (11); left medial frontoorbital artery (12).
Right Left
12
3
45
6
7
89 11
(a)
LeftRight
3
5
4
4
(b)
Figure 2: Persistent primitive olfactory artery (PPOℓA) as a side branch of the precommunicating part (A1) of the right anterior cerebralartery (ACA). It originates from the anterior wall of the A1 (a) and courses to the medial surface of the frontal lobe, where the PPOℓA gaveoff a bihemispheric branch (b). Cerebral part (C4) of the right internal carotid artery (1); left C4 (2); right A1 (3); right PPOℓA (4); rightrecurrent artery of Heubner (RAH) (5)); anterior communicating artery (ACoA) (6); left A1 (7); left RAH (8); right postcommunicating part(A2) of the ACA (9); left A2 (11).
this second type of the PPOℓA is homologous to the internalethmoidal artery in the dog. In the third (transitory) typedescribed by Horie et al. [13], the PPOℓA divided into twobranches; one artery was similar to Nozaki’s type 1, whereasthe second one had features of Nozaki’s type 2. In our “third”type, the PPOℓA of the MCA origin had a common trunk
with posterior communicating artery (PCoA) and coursedforward to the ipsilateral olfactory tract [22]. The case of thePPOℓA termination (PPOℓA—cortical frontal vein shunt)described by Tsutsumi et al. [8] was classified as type 4.
Medial frontoorbital and frontopolar arteries are differentfrom the PPOℓA according to the beginning (A2 part) and

4 BioMed Research International
Table1:Com
paris
onof
generaland
speciald
ataa
bout
thep
ersis
tent
prim
itive
olfactoryartery
(PPOℓA)p
resented
inou
rand
otherinvestig
ations.
Cou
ntry
[autho
rs]
Age∗
Gender(no
.)Initial
symptom
sDiagn
osis
PPOℓA
Incidental
finding
Relatio
nof
number
cases
Vascular
source
Side
Nozaki’s
andnew
types∗∗
Associated
varia
tions
(no.)Aneurysmatic
artery
(no.)
Other
cerebral
patholog
ySinglecases
Korea[
18]
24F
Vertigo
3DCT
A+
ICA
RI
Serbia[22]
35M
Myoc.
infarctio
nAu
topsy
+ICA
pR
III
Orig
in/end
ofther
ight
PCoA
Japan[14
]42
M3D
CTA
+ICA
LI
ACoA
Japan∗∗∗
[15]
44M
Headache
CTA
+(II)
Anasto
m.w
ithleftant.ethm
.a.
Left
fronto-orbital
artery
(PPOℓA)
Intracerebral
hem./S
AH
Japan[7]
54F
Ano
smia
Cereb.
angio.
+ICA
L/R
IAC
oAapl.
RAHsa
pl.
Japan[14
]55
FCereb.
angio.
+ICA
LII
ICA
Japan∗∗∗
[16]
59F
+ICA
LI
ACA
Japan∗∗∗
[17]
59F
Hyposmia
+ICA
RPP
OℓA
Japan[8]
59M
Generalseizure
CTA
+A1-A
2R
(IV)
PPOℓA-
cort.front.
vein
shun
tRA
Hapl.
Intracerebral
hem.
Taiwan∗∗∗
[21]
62F
Cereb.
angio.
+ICA
R(I)
Moyam
oyap
h.Fetal
PCA
MCA
acc.
MCA
occl.
Korea[
19]
68F
Headache
CTA
+ICA
R(I)
PPOℓA
bulbou
sdilatatio
n
Japan[9]
69M
Lossof
consciou
sness
3DCT
A+
ICA
R(I)
ACoA
apl.
PPOℓA/le
ftA1-A
2/ICA
UK[20]
71M
Gastric
carcinom
aAu
topsy
+A1
L(II)
Dou
bleA
CoA
Japan[13]
78M
Headache
Axial
Dyn
aCT/DSA
+A1
RTransitory
type
(I/II
)
PPOℓA-
ethm
oidal
anastomosis
RightA
1SA
H

BioMed Research International 5
Table1:Con
tinued.
Cou
ntry
[autho
rs]
Age∗
Gender(no
.)Initial
symptom
sDiagn
osis
PPOℓA
Incidental
finding
Relatio
nof
number
cases
Vascular
source
Side
Nozaki’s
andnew
types∗∗
Associated
varia
tions
(no.)Aneurysmatic
artery
(no.)
Other
cerebral
patholog
yRetro
spectivestudies
Japan[5]
M(1)
Clinica
lor
forensic
investigatio
ns
MRA
1/900
ICA
RJapan[6]
CTA/M
RA1/3
700
ICA
LJapan∗∗∗
[12]
5/?
ICA
PPOℓA(1)
Korea[
11]
24 −82
M(17)
F(12)
MRA
/CTA
29/9841
L(19
)R(7)
LR(3)
ACAhypo
p.(3)
M1fen
(1)
PPOℓA(2)
ICA(1)
Threec
ereb.
arteriæ
(1)
Japan[10]
36 −81
M(6)
F(8)
MRA
14/3491
L(7)
R(6)
LR(1)
VAfen.
(1)
MCA
acc.(1)
MAC
C(1)
MCA
(1)
PPOℓA(1)
Serbia(recentstudy)
0−95
M(2)
Autopsy
2/469
A1
R(2)
IA1fen
(1)
MAC
C(1)
∗
Sing
lecasesa
realignedaccordingto
thea
ge.
∗∗
Nozaki’s[7]a
ndnewtypesa
remarkedby
Romaniannu
mbers.
∗∗∗
Datafrom
thep
aper
byKa
tayamae
tal.[14
].Female(F);m
ale(M);left(L);rig
ht(R);myocardial(myoc.);three-dim
ensio
nalcom
putertom
ograph
yang
iography
(3DCT
A);cerebralangiograph
y(cereb.angio.);digitalsub
tractio
nangiograph
y(DSA
);magnetic
resonancea
ngiography
(MRA
);internalcarotid
artery
(ICA);persistentcranialbranch
oftheinternalcarotidartery
(ICAp );ju
nctio
nofthep
recommun
icatinga
ndpo
stcom
mun
icatingp
arts(A
1-A2)
ofthea
nterior
cerebral
artery
(ACA
);po
sterio
rcommun
icatingartery
(PCoA
);aplasia
oftheanterio
rcommun
icatingartery
(ACoA
apl.);recurrent
artery
ofHeubn
er(RAH);accessorymiddlecerebral
artery
(MCA
acc.);
poste
riorc
erebralartery(PCA
);fenestr
ationof
thes
phenoidpartof
theM
CA(M
1fen);vertebralartery(VA);medianartery
ofthec
orpu
scallosum
(MAC
C);hem
orrhage(
hem.);
occlu
sion(occl.);sub
arachn
oid
hemorrhage(SA
H).

6 BioMed Research International
their course. Exceptions were possible as in cases describedby Enomoto et al. [15] and Krishnamoorthy et al. [26].
We described some cases of the POℓA partial persistencein human fetuses [23]. Recently, we described these two casesof the PPOℓA, found only among adult cadavers. Previous[22] and recent cases indicate that the incidence of the PPOℓAis 0.64% in Serbian population. These incidences were 0.14%in the Japanese population [10] and 0.29% in the Koreanpopulation [11]. For the purpose of calculating of number ofpublished cases, we included some paper abstracts [12, 14–17]in the list of references. Based on the case numbers in ourTable 1 and Moffat’s allegation about two cases of the PPOℓAdescribed in 1951 and 1961 by other authors [1], we counted67 cases to this time. Based also on the cases in the sametable, we could note that PPOℓA was more frequent in malesand on the left side, although the POℓA persisted on the rightside in males of Serbian population, as we noted in our work.The existence of bilateral PPOℓA was noted five times in theliterature [7, 10, 11]. The youngest person was 18 years old [5]and the oldest 82 years [11].
In summary, we did not find any aneurysmon the PPOℓAin our cases, opposite to some authors who found it on thePPOℓA hairpin bend [9, 12, 15, 17], and/or on other cerebralarteries [9–11, 13, 14, 16]. Association of the PPOℓA and othervascular variations were also noted [7, 11, 20, 22], as in ouradult cases.
4. Conclusions
The primitive olfactory artery is a rare persistent primitivevessel (0.64%) in Serbian population. It was incidental findingin presented cases. We did not find any complete vasculartrunk in fetuses, but we did in adults of male gender, on theright side.
Acknowledgments
The authors wish to thank Mrs Zorica Antic, Professor ofEnglish in Faculty ofMedicine of Nis, for assistance in editingthe text. Contract Grant sponsor is Ministry of Education,Science and Technological Development of Republic of Ser-bia (nos. 41018 and 175092).
References
[1] D. B. Moffat, “The embryology of the arteries of the brain.Arris and Gale lecture delivered at the Royal College of sur-geons of England,” pp. 368–382, 1962, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2414182/pdf/annrcse00385-0020.pdf.
[2] T. Minakawa, M. Kawamata, M. Hayano, and K. Kawakami,“Aneurysms associated with fenestrated anterior cerebral arter-ies. Report of four cases and review of the literature,” SurgicalNeurology, vol. 24, no. 3, pp. 284–288, 1985.
[3] J. S. Koh, S. H. Lee, J. S. Bang, and G. K. Kim, “Three-dimensional angiographic demonstration of plexiform fenes-trations of the proximal anterior cerebral artery associated witha ruptured aneurysm,” Journal of Korean Neurosurgical Society,vol. 44, no. 5, pp. 338–340, 2008.
[4] S. J. Dimmick and K. C. Faulder, “Normal variants of thecerebral circulation at multidetector CT angiography,” Radio-graphics, vol. 29, no. 4, pp. 1027–1043, 2009.
[5] A.Uchino, A. Sawada, Y. Takase, and S. Kudo, “MR angiographyof anomalous branches of the internal carotid artery,”AmericanJournal of Roentgenology, vol. 181, no. 5, pp. 1409–1414, 2003.
[6] M. Okahara, H. Kiyosue, H. Mori, S. Tanoue, M. Sainou, andH. Nagatomi, “Anatomic variations of the cerebral arteries andtheir embryology: a pictorial review,” European Radiology, vol.12, no. 10, pp. 2548–2561, 2002.
[7] K. Nozaki,W. Taki, O. Kawakami, and N. Hashimoto, “Cerebralaneurysm associated with persistent primitive olfactory arteryaneurysm,” Acta Neurochirurgica, vol. 140, no. 4, pp. 397–402,1998.
[8] S. Tsutsumi, Y. Shimizu, Y. Nonaka et al., “Arteriovenous fistulaarising from the persistent primitive olfactory artery with dualsupply from the bilateral anterior ethmoidal arteries—casereport,” Neurologia Medico-Chirurgica, vol. 49, no. 9, pp. 407–409, 2009.
[9] T. Yamamoto, K. Suzuki, T. Yamazaki, W. Tsuruta, T. Tsu-rubuchi, and A. Matsumura, “Persistent primitive olfactoryartery aneurysm—case report,” Neurologia Medico-Chirurgica,vol. 49, no. 7, pp. 303–305, 2009.
[10] A. Uchino, N. Saito, E. Kozawa, W. Mizukoshi, and K. Inoue,“Persistent primitive olfactory artery:MR angiographic diagno-sis,” Surgical and Radiologic Anatomy, vol. 33, no. 3, pp. 197–201,2011.
[11] B. R. Kwon, S. H. Yeo, H. W. Chang et al., “Magnetic resonanceangiography and CT angiography of persistent primitive olfac-tory artery: incidence and association rate with aneurysm inKorea,” Journal of the Korean Society of Radiology, vol. 66, no.6, pp. 493–499, 2012.
[12] T. Kaneko, K. Suetake, T. Shinya, and M. Takeda, “Persistentprimitive olfactory artery: report of 5 cases,” NeurologicalSurgery, vol. 27, no. 10, pp. 933–939, 1999.
[13] N. Horie, M. Morikawa, S. Fukuda, K. Hayashi, K. Suyama, andI. Nagata, “New variant of persistent primitive olfactory arteryassociated with a ruptured aneurysm,” Journal of Neurosurgery,vol. 117, no. 1, pp. 26–28, 2012.
[14] M. Katayama, Y. Shimamoto, and S. Suga, “Primitive olfac-tory artery—characteristics and cerebral aneurysms asso-ciated with primitive olfactory artery,” Niche Neuro-Angi-ology Conference, (Jpn/Eng), 2012, http://nnac.umin.jp/nnac/Download 2012 files/Katayama.pdf.
[15] H. Enomoto, H. Goto, and M. Murase, “A ruptured cerebralaneurysm of the frontoorbital artery and the coexisting anas-tomosis with the anterior ethmoidal artery. A case report,”Neurological Surgery, vol. 14, no. 2, pp. 203–206, 1986.
[16] T. Tsuji, M. Abe, and K. Tabuchi, “Aneurysm of a persistentprimitive olfactory artery: case report,” Journal of Neurosurgery,vol. 83, no. 1, pp. 138–140, 1995.
[17] A. Yamaura, M. Takase, and H. Makino, “An aneurysm of theproximal anterior cerebral artery at the olfactory bulb,” SurgicalNeurology, vol. 12, no. 5, pp. 425–427, 1979.
[18] M. S. Kim and G. J. Lee, “Diagnosis of persistent primitiveolfactory artery using computed tomography angiography,”Journal of Korean Neurosurgical Society, vol. 49, no. 5, pp. 290–291, 2011.
[19] S. H. Yeo, B. H. Rho, E. Kim, C. H. Sohn, and H. W. Chang,“Diagnosis of persistent primitive olfactory artery using CTangiography: a case report,” Journal of the Korean Society ofRadiology, vol. 61, no. 3, pp. 139–141, 2009.

BioMed Research International 7
[20] D. B. Moffat, “A case of peristence of the primitive olfactoryartery,”Anatomischer Anzeiger, vol. 121, no. 5, pp. 477–479, 1967.
[21] W.-C. Lin, S.-W. Hsu, Y.-L. Kuo, J. A. Feekes, and H.-C. Wang,“Combination of olfactory course anterior cerebral artery andaccessory middle cerebral artery (MCA) with occluded insitu MCA and related moyamoya phenomenon,” Brain andDevelopment, vol. 31, no. 4, pp. 318–321, 2009.
[22] L. Vasovic, I. Jovanovic, S. Ugrenovic, and M. Trandafilovic,“Remnants of embryonic arteries on the brain base: a casereport,”World Journal of Neuroscience, vol. 2, no. 2, pp. 133–137,2012.
[23] L. Vasovic, S. Ugrenovic, and I. Jovanovic, “Human fetal medialstriate artery or artery of Heubner,” Journal of NeurosurgeryPediatrics, vol. 3, no. 4, pp. 296–301, 2009.
[24] L. Vasovic, Morphological characteristics of the cerebral arterialcircle with different origin of the vertebral arteries [M.S. thesis],Faculty of Medicine, Nis, Serbia, 1990.
[25] M. Komiyama, “Persistent primitive olfactory artery,” Surgicaland Radiologic Anatomy, vol. 34, no. 1, pp. 97–98, 2012.
[26] T. Krishnamoorthy, A. K. Gupta, R. N. Bhattacharya, B. J.Rajesh, and S. Purkayastha, “Anomalous origin of the callo-somarginal artery from the A1 segment with an associatedsaccular aneurysm,” American Journal of Neuroradiology, vol.27, no. 10, pp. 2075–2077, 2006.
[27] T. H. Kim, H. K. Lee, J. J. Rhee, S. J. Lee, C. H. Lee, and M. S.Kim, “The incidence and clinical significance of fenestrationsin the horizontal segment of the anterior cerebral arterydetected by conventional angiography and magnetic resonanceangiography,” Journal of Korean Neurosurgery Society, vol. 40,no. 1, pp. 74–78, 2006.

Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporation http://www.hindawi.com
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttp://www.hindawi.com
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
International Journal of
Microbiology