Research Article Current Epidemiological Assessment of...
6
Research Article Current Epidemiological Assessment of Bancroftian Filariasis in Tanga Region, Northeastern Tanzania Happyness J. Mshana, 1,2 Vito Baraka, 1,3 Gerald Misinzo, 2 and Williams H. Makunde 1 1 National Institute for Medical Research, Tanga Research Centre, P.O. Box 5004, Tanga, Tanzania 2 Sokoine University of Agriculture, Morogoro, Tanzania 3 Global Health Institute, University of Antwerp, Antwerp, Belgium Correspondence should be addressed to Happyness J. Mshana; [email protected] Received 20 July 2016; Revised 3 October 2016; Accepted 8 November 2016 Academic Editor: Jean-Paul J. Gonzalez Copyright © 2016 Happyness J. Mshana et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Tanzania started a countrywide lymphatic filariasis elimination programme in 2000 adopting the mass drug administration (MDA) strategy. e drug used for the programme was the combination of ivermectin and albendazole. However, there is limited information on the current epidemiological trend of the infections, where MDA implementation is ongoing. e present study aimed at assessing the current status of Bancroſtian filariasis infection rate and morbidity where MDA has been distributed and administered for over eight rounds. Methodology. e study was a cross-sectional descriptive study involving 272 individuals (>18 years) from endemic communities in Tanga region where MDA has been implemented. Clinical, sociodemographic, and circulating filarial antigen (CFA) test was undertaken using immune chromatographic card test according to the manufacturer’s instructions. Results. A total of 472 individuals were screened: 307/472 (65.1%) were males while 165/472 (34.9%) were females. e overall prevalence of CFA was 5.51%, that of hydrocoele was 73.2%, and that of lymphoedema was 16.0%. e prevalence of hydrocoele combined with lymphoedema was 5.5%. Conclusion. Our findings demonstrate a considerable reduction in filarial infection. However, there is clear evidence of ongoing transmission despite the 8 rounds of MDA. It is unlikely that the annual MDA would interrupt filarial transmission; therefore, additional strategies are needed to accelerate lymphatic filariasis control and elimination. 1. Introduction Lymphatic filariasis (LF) is the second leading cause of long-term disability globally due to lymphoedema, elephan- tiasis, and hydrocele [1]. e long-term disability is trig- gered through overt hydrocoele, lymphoedema, elephanti- asis, repeated orchitis, and adenolymphangitis [2]. ese acute and chronic pathologies impose a significant imped- iment to socioeconomic development and an extremely poor quality of life [3]. LF affects more than 120 million individuals globally [4]. It is estimated that around 20% of the world population in more than 83 countries are at risk of acquiring infection which is 1.1 billion people [5]. In the endemic communities, 7% of the adult population suffer from lymphoedema whereas 30–50% develop hydrocele [6]. In sub-Saharan Africa (SSA), the predominant parasite is filarial nematode Wuchereria bancroſti (W. bancroſti) which is estimated to affect 500 million people [7]. Epidemiological mapping in Tanzania has shown that the risk is particularly high in the coastal zone along the Indian Ocean although cases are also reported in other mainland regions [8]. In response to the World Health Organization (WHO) Global Programme to Eliminate Lymphatic Filariasis (GPELF) that aimed at filariasis elimination, Tanzania established the National Lymphatic Filariasis Elimination Programme (NLFEP) in 2000 where targeted communities were given a combination of ivermectin and albendazole (ALB+IV) annually [8]. e ivermectin dosage is administered according to body weight (150–200 g/kg) while 400 mg of albendazole is given to individuals aged ≥5 years in all endemic districts. In some settings, it has shown a reduction of infections rate to low levels as 1%. Hindawi Publishing Corporation Journal of Tropical Medicine Volume 2016, Article ID 7408187, 5 pages http://dx.doi.org/10.1155/2016/7408187
Transcript of Research Article Current Epidemiological Assessment of...

Research ArticleCurrent Epidemiological Assessment of Bancroftian Filariasis inTanga Region Northeastern Tanzania
Happyness J Mshana12 Vito Baraka13 Gerald Misinzo2 and Williams H Makunde1
1National Institute for Medical Research Tanga Research Centre PO Box 5004 Tanga Tanzania2Sokoine University of Agriculture Morogoro Tanzania3Global Health Institute University of Antwerp Antwerp Belgium
Correspondence should be addressed to Happyness J Mshana jeremiahappinessyahoocom
Received 20 July 2016 Revised 3 October 2016 Accepted 8 November 2016
Academic Editor Jean-Paul J Gonzalez
Copyright copy 2016 Happyness J Mshana et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Background Tanzania started a countrywide lymphatic filariasis elimination programme in 2000 adopting the mass drugadministration (MDA) strategy The drug used for the programme was the combination of ivermectin and albendazole Howeverthere is limited information on the current epidemiological trend of the infections where MDA implementation is ongoingThe present study aimed at assessing the current status of Bancroftian filariasis infection rate and morbidity where MDAhas been distributed and administered for over eight rounds Methodology The study was a cross-sectional descriptive studyinvolving 272 individuals (gt18 years) from endemic communities in Tanga region where MDA has been implemented Clinicalsociodemographic and circulating filarial antigen (CFA) testwas undertaken using immune chromatographic card test according tothemanufacturerrsquos instructionsResults A total of 472 individuals were screened 307472 (651) weremales while 165472 (349)were females The overall prevalence of CFA was 551 that of hydrocoele was 732 and that of lymphoedema was 160 Theprevalence of hydrocoele combined with lymphoedema was 55 Conclusion Our findings demonstrate a considerable reductionin filarial infection However there is clear evidence of ongoing transmission despite the 8 rounds of MDA It is unlikely thatthe annual MDA would interrupt filarial transmission therefore additional strategies are needed to accelerate lymphatic filariasiscontrol and elimination
1 Introduction
Lymphatic filariasis (LF) is the second leading cause oflong-term disability globally due to lymphoedema elephan-tiasis and hydrocele [1] The long-term disability is trig-gered through overt hydrocoele lymphoedema elephanti-asis repeated orchitis and adenolymphangitis [2] Theseacute and chronic pathologies impose a significant imped-iment to socioeconomic development and an extremelypoor quality of life [3] LF affects more than 120 millionindividuals globally [4] It is estimated that around 20 ofthe world population in more than 83 countries are at riskof acquiring infection which is 11 billion people [5] In theendemic communities 7 of the adult population sufferfrom lymphoedema whereas 30ndash50 develop hydrocele [6]In sub-Saharan Africa (SSA) the predominant parasite is
filarial nematode Wuchereria bancrofti (W bancrofti) whichis estimated to affect 500 million people [7] Epidemiologicalmapping in Tanzania has shown that the risk is particularlyhigh in the coastal zone along the Indian Ocean althoughcases are also reported in other mainland regions [8]
In response to the World Health Organization(WHO) Global Programme to Eliminate LymphaticFilariasis (GPELF) that aimed at filariasis eliminationTanzania established the National Lymphatic FilariasisElimination Programme (NLFEP) in 2000 where targetedcommunities were given a combination of ivermectin andalbendazole (ALB+IV) annually [8] The ivermectin dosageis administered according to body weight (150ndash200 120583gkg)while 400mg of albendazole is given to individuals agedge5 years in all endemic districts In some settings it hasshown a reduction of infections rate to low levels as 1
Hindawi Publishing CorporationJournal of Tropical MedicineVolume 2016 Article ID 7408187 5 pageshttpdxdoiorg10115520167408187
2 Journal of Tropical Medicine
Conversely the endemic areas along the coast of the IndianOcean have shown a high prevalence of infection up to 633despite the ongoing MDA for over eight years [8] It wasanticipated that using the MDA strategy as recommendedin WHO guidelines on MDA coverage (gt65) through avariety of approaches will lead to interrupting transmission[3] whereby microfilariae (mf) levels will reach below 1
However evidence in Tanga region has shown thatdespite 8 rounds of MDA and supplementation with otherinterventions such as the provision of insecticide-treatednets (ITNs) still both infection and clinical disease ratesremain high especially along the coastline [8]The prevalencein Tanga region before the MDA survey in 2004 of thecommunity mf was 245 that of CFAwas 633 and that ofspecific antibodies to recombinant filarial antigen was 789In comparison after 8 rounds of MDA the CFA and mfprevalence in combined study communities was reduced by755 and 896 respectively compared to baseline levelswhile the CFA prevalence in school children was reducedby 909 compared to baseline [8] The present study wasdesigned to ascertain the LF infections rates and morbiditiesafter the MDA rounds in Tanga region
2 Methods
21 Study Area and Population The study was conductedin Tanga region in Northeastern Tanzania along the IndianCoast (05∘041015840S 39∘061015840E) The region is characterised mainlyby two rain seasons annually the long rains from March toJune and the less intensive short rains from November toDecember The majority of the inhabitants practice subsis-tence farming fishing and livestock keeping The climate inTanga region is warm and wet In most cases there is no bigvariation of temperature at the coast due to the influence ofthe Indian Ocean Also the region is characterised by highhumidity which often goes up to 100maximum and rangesfrom 65 to 70 minimumThere are health facilities in mostvillages in the regions and the majority of the populationhave access to a health facility within a distance of 6 kmMost of the houses are made of mud walls with their roofsthatched with dried coconut leaves This makes it easier forthe vector to penetrate Bancroftian filariasis control startedin 2004 usingMDAcampaigns and advocacywith ivermectinand albendazole in all districts [8] The estimated populationsize of the area was 2045205 inhabitants according to 2012national census survey [9]
22 Study Design The study was a cross-sectional descrip-tive study conducted between April and May 2015 The studyparticipants were selected using convenience sampling anonprobability sampling technique where individuals wereselected based on their convenient accessibility and proxim-ity
23 Ethical Considerations Ethical clearance for the studywas granted by theMedical Research Coordinating Commit-tee of the National Institute forMedical Research in Tanzania(NIMR-MRCC) The investigators explained the purpose of
Table 1 Sociodemographic characteristics of the study population
Characteristics Frequency (119873) Proportion ()Age group in years18ndash31 36 13232ndash45 66 24546ndash59 58 21360ndash73 90 33174ndash87 22 81Sex ratio (female male) 33 239OccupationPeasant farmers 102 375Fishermen 170 625119873 number of individuals
the study and all study participants consented orally and inwriting
24 Clinical Examination A clinician experienced in LFexamined those patients and recorded the swelling of thelower limbs and scrotum in stages according to Meyrowitschet al [10] Thereafter a semistructured questionnaire wasused to collect the demographic information and other clin-ical disease conditions Individuals with lymphoedema andhydrocoele stages lower than III were treated with antibiotic(doxycycline or tetracycline) for 7 days and topical broad-spectrum antifungal cream as recommended by the studyphysician
25 Parasitological Examination Patients were then askedto donate 100 120583L for circulating filarial antigen examinationusing immune chromatographic test cards The BinaxNOWFilariasis immune chromatographic card test (Alere IncScarborough ME) was used to detect circulating filarial anti-gen as described in the WHO guidelines [11] Briefly 100120583Lof finger-prick blood was collected from each individualand then transferred to an immune chromatographic cardtest using a calibrated capillary tube The test was read 10minutes after closing the card as per the manufacturerrsquosinstructions The antigen contains the epitope present incirculating W bancrofti antigen that was detected by theBinaxNOWFilariasis testThe identification number and testresult of each individual tested were recorded in the casereport form
3 Results
A total of 472 individuals were examined during the com-munity survey among whom 651 (307) were males while349 (165) were females Of those 272 were recruited forthe study of whom 8786 were males and 1214 werefemales 119901 le 00001 The rest did not fulfil the inclusioncriteria as presented in the flow diagram (Figure 1)The studypopulation that was more frequently observed with highproportionwas the 32ndash45-year age groupwith a rate of 242followed by the 60ndash73-year age groupwith a rate of 331 andthe majority of them were fishermen (625) (Table 1)
Journal of Tropical Medicine 3
Total individuals screenedn = 472
Male n = 68 Male n = 307 Female n = 165 Female n = 132
Male n = 239(8786)
Female n = 33(1214)
Total individuals recruitedn = 272
Elig
ibili
tyIn
clude
dId
entifi
catio
nSc
reen
ing
Figure 1 Study profile of the individuals recruited in the cross-sectional survey in Tanga region
018ndash31 32ndash45 46ndash59 60ndash73 74ndash87
Age group
MaleFemale
05
1
15
2
25
3
35
4
45
Prop
ortio
ns (
)
Figure 2 Age distribution of lymphoedema pathology according tostages in the examined individuals
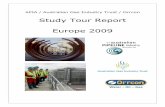
Females were observed to have a higher proportion oflymphoedema than males in the age group of 32ndash45 years(Figure 2) Figures 3 and 4 summarise the infection ratesin the study group whereby 551 of the 272 individualswere CFA-positive and the majority of those were males(33) Few of the confirmed CFA patients were females(221) The proportions of scrotal hydrocele in males above18 years old were high (732) as compared to lymphoedema(158) Conversely the proportion of individuals with bothlymphoedema and hydrocele was 551
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
HCHCampLE
0
5
10
15
20
25
30
Prop
ortio
ns (
)
Figure 3 Age distribution of scrotal hydrocoele pathology accord-ing to stages in those examined individuals HC hydrocoeleHCampLE hydrocoele and lymphoedema
4 Discussion
In our study hydrocoele has been shown to be the main pub-lic health problem causing debilitation in males and similarlylymphoedema in females as observed elsewhere [12] It hasalso been shown in our study that these conditions affectthe 32ndash45-year age group Recent studies focusing on themolecularmechanism regulating blood and lymphatic vesselsgrowth have shown that vascular endothelial growth factorscontrol angiogenesis and lymphangiogenesis in humans [13]which is a process of developing lymphangiectasia as a clinical
4 Journal of Tropical Medicine
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
CDAAInfection
0
5
10
15
20
25
30
Prop
ortio
ns (
)
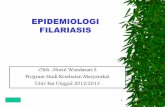
Figure 4 Acute and chronic clinical disease stratified into agegroups CD chronic pathology (lymphedema hydrocele and lym-phedema combined with hydrocele) AA acute attacks (filarialfever) infection circulating filarial antigen (CFA)
disease Similarly expression of VEGF-A and VEGF-C hasbeen shown to be upregulated by proinflammatory cytokinesaffecting the lymphatic vessels in males [13] However cur-rently there is limited data on the heterogeneity of the diseaseSince the pathogenesis and development of lymphoedemaremain largely unknown there is a need for future studies toexplore the role of genetics in relation to clinical phenotypesto better understand the disease aetiology and optimise thecontrol strategies The results of this study suggest thatduring the era of lymphatic filariasis control of infectionsthe disease has shown a clear reduction of acute infectionandmorbidity rates compared to the baseline study especiallyin the older age group This could have been triggered bythe host human-immune and parasite interaction leadingto the clearance of acute infection [12] On the other handthe presence of adult worms and their secretions and thedeath of such adult worms may lead to dilatation of scrotallymphatic vessel causing dysfunction and accumulation ofprotein-rich fluid in the tissue causing lymphangiectasia [13]However there is still ongoing LF transmission in some ofthe studied communities in the region and it is unlikely thatthe annual single dose can interrupt the transmission andtherefore other strategies such as biannual administrationof MDA can be applied to interrupt the transmission asobserved in other studies In Figure 4 young age groups(18ndash31 years) have increasing acute and chronic infectionsA similar observation has been shown in Fiji [14] Theseare the productive segment in the communities indicatinga shifting trend of the clinical disease into the lower agegroups because low-level transmission continues in thosecommunities This could be possibly due to some existinghotspots in the communities whereby mosquito vectors pickinfection from humans and maintain the local transmission
[15] It is also likely that the postponement of the MDAdistribution within the timely scheduled period could havehalted reaching the desired coverage of at least 65 accordingto theWHO hence leading to LF resurgence [14] It is vital toexpand the frequency of drug administration to a maximumof three doses per year expand the age range of the targetpopulation and improve health education to the communitywith the aim of increasing coverage within the targetedareas Similarly we should conduct an anthropological studyto find out why transmission continues although MDA isin place tracking factors associated with that such as theincentive to drug distributors health system roles in thedistrict timely availability of drugs financial resources andadvocacy and training of distributors The need for adequatefinancial and logistics resources is paramount to successfullyachieve the targeted coverage and reach the end goal of theprogramme Adequate resources and infrastructural supportshould be available to ensure timely availability and supply oftheMDAdrugs to reach the implementation units in endemiccommunities Moreover more evidence is needed to assesswhether parasite genetic variability has implications in theeffectiveness of diagnostic test epidemiology and control ofthe disease [16] as well as cross-reactivity of the ICT cardto non-W bancrofti filariae that could reinforce doubts onthe validity of the current map of LF as observed in otherstudies [17] Formulation of guidelines for LF coendemicareas assessment is therefore very important It is worthalso addressing issues related to the vector for successfulcontrol of LF MDA in combination with other interventionssuch as insecticide-treated nets will improve reduction ofinfection and interrupt transmission of the infection in thecommunities However insecticide resistance could lead toa substantial increase and persistence of filarial infectionincidence [18]
5 Conclusion
Our findings have shown a considerable reduction in filar-ial infection However there is clear evidence of ongoingtransmission despite the 8 rounds of MDA using ivermectinand albendazole It is unlikely that annual mass drug admin-istration would interrupt filarial transmission thereforeoptimised strategies are needed to accelerate control andelimination of targets
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to the villagers in Tanga regionfor their dedicated cooperation and to the technical stafffromNIMR-Tanga (FidelisMumburi Xavaeli Ngowi CharlesGuzo and Tembo) for their assistance in the field and thelaboratory This study received financial support from Uni-versity Hospital Bonn Institute for Medical MicrobiologyImmunology and Parasitology (Grant Code PF 6732-1)
Journal of Tropical Medicine 5
References
[1] S Wynd W D Melrose D N Durrheim J Carron and MGyapong ldquoUnderstanding the community impact of lymphaticfilariasis a review of the sociocultural literaturerdquo Bulletin of theWorld Health Organization vol 85 no 6 pp 493ndash498 2007
[2] S Babu and T B Nutman ldquoImmunopathogenesis of lymphaticfilarial diseaserdquo Seminars in Immunopathology vol 34 no 6 pp847ndash861 2012
[3] WHO ldquoGlobal programme to eliminate lymphatic filariasisrdquoin A Handbook of Practical Entomology for National LymphaticFilariasis Elimination Programmes p 1 WHO 2013
[4] K Ichimori ldquoMDAmdashlymphatic filariasisrdquo Tropical Medicineand Health vol 42 no 2 supplement pp 21ndash24 2014
[5] E A Ottesen ldquoEditorial the global programme to eliminatelymphatic filariasisrdquoTropicalMedicine and InternationalHealthvol 5 no 9 pp 591ndash594 2000
[6] L Batsa Anti-wolbachia treatment of lymphatic filariasis andgenetic analysis of the pathology of lymphedema as a clinicalmanifestation of the disease [PhD dissertations] 2012
[7] P J Hotez and A Kamath ldquoNeglected tropical diseases in sub-Saharan Africa review of their prevalence distribution anddisease burdenrdquo PLoS Neglected Tropical Diseases vol 3 no 8article e412 2009
[8] P E Simonsen Y A Derua S M Magesa et al ldquoLymphaticfilariasis control in Tanga Region Tanzania status after eightrounds of mass drug administrationrdquo Parasites amp Vectors vol 7no 1 article 507 2014
[9] National Bureau of Statistics (NBS) andOffice of Chief Govern-ment Statistician Zanzibar (OCGS) 2012 Population and Hous-ing Census Population Distribution by Administrative Units KeyFindings The United Republic of Tanzania 2013
[10] D W Meyrowitsch P E Simonsen and W H MakundeldquoBancroftian filariasis analysis of infection and disease in fiveendemic communities of north-eastern Tanzaniardquo Annals ofTropical Medicine and Parasitology vol 89 no 6 pp 653ndash6631995
[11] L Original Preparing and Implementing a National Plan toEliminate Lymphatic Filariasis World Health 2000
[12] D G Addiss and M A Brady ldquoMorbidity management in theglobal programme to eliminate lymphatic filariasis a review ofthe scientific literaturerdquo Filaria Journal vol 6 article 2 2007
[13] K M Pfarr A Y Debrah S Specht and A Hoerauf ldquoFilariasisand lymphoedemardquo Parasite Immunology vol 31 no 11 pp664ndash672 2009
[14] M E Mwakitalu M N Malecela E M Pedersen F WMosha and P E Simonsen ldquoUrban lymphatic filariasis in themetropolis of Dar es Salaam Tanzaniardquo Parasites and Vectorsvol 6 article 286 p 13 2013
[15] R T Rwegoshora E M Pedersen D A Mukoko et alldquoBancroftian filariasis patterns of vector abundance and trans-mission in twoEast African communities with different levels ofendemicityrdquo Annals of Tropical Medicine and Parasitology vol99 no 3 pp 253ndash265 2005
[16] S Nuchprayoon A Junpee and Y Poovorawan ldquoRan-dom amplified polymorphic DNA (RAPD) for differentiationbetween Thai and Myanmar strains of Wuchereria bancroftirdquoFilaria Journal vol 6 no 6 article 6 2007
[17] S Wanji N Amvongo-Adjia A J Njouendou et al ldquoFurtherevidence of the cross-reactivity of the Binax NOW FilariasisICT cards to non- Wuchereria bancrofti filariae experimental
studies with Loa loa and Onchocerca ochengirdquo Parasites ampVectors vol 9 article 267 pp 1ndash10 2016
[18] N Protopopoff J Matowo R Malima et al ldquoHigh level ofresistance in the mosquito Anopheles gambiae to pyrethroidinsecticides and reduced susceptibility to bendiocarb in north-western Tanzaniardquo Malaria Journal vol 12 article 149 pp 1ndash82013
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Journal of Tropical Medicine
Conversely the endemic areas along the coast of the IndianOcean have shown a high prevalence of infection up to 633despite the ongoing MDA for over eight years [8] It wasanticipated that using the MDA strategy as recommendedin WHO guidelines on MDA coverage (gt65) through avariety of approaches will lead to interrupting transmission[3] whereby microfilariae (mf) levels will reach below 1
However evidence in Tanga region has shown thatdespite 8 rounds of MDA and supplementation with otherinterventions such as the provision of insecticide-treatednets (ITNs) still both infection and clinical disease ratesremain high especially along the coastline [8]The prevalencein Tanga region before the MDA survey in 2004 of thecommunity mf was 245 that of CFAwas 633 and that ofspecific antibodies to recombinant filarial antigen was 789In comparison after 8 rounds of MDA the CFA and mfprevalence in combined study communities was reduced by755 and 896 respectively compared to baseline levelswhile the CFA prevalence in school children was reducedby 909 compared to baseline [8] The present study wasdesigned to ascertain the LF infections rates and morbiditiesafter the MDA rounds in Tanga region
2 Methods
21 Study Area and Population The study was conductedin Tanga region in Northeastern Tanzania along the IndianCoast (05∘041015840S 39∘061015840E) The region is characterised mainlyby two rain seasons annually the long rains from March toJune and the less intensive short rains from November toDecember The majority of the inhabitants practice subsis-tence farming fishing and livestock keeping The climate inTanga region is warm and wet In most cases there is no bigvariation of temperature at the coast due to the influence ofthe Indian Ocean Also the region is characterised by highhumidity which often goes up to 100maximum and rangesfrom 65 to 70 minimumThere are health facilities in mostvillages in the regions and the majority of the populationhave access to a health facility within a distance of 6 kmMost of the houses are made of mud walls with their roofsthatched with dried coconut leaves This makes it easier forthe vector to penetrate Bancroftian filariasis control startedin 2004 usingMDAcampaigns and advocacywith ivermectinand albendazole in all districts [8] The estimated populationsize of the area was 2045205 inhabitants according to 2012national census survey [9]
22 Study Design The study was a cross-sectional descrip-tive study conducted between April and May 2015 The studyparticipants were selected using convenience sampling anonprobability sampling technique where individuals wereselected based on their convenient accessibility and proxim-ity
23 Ethical Considerations Ethical clearance for the studywas granted by theMedical Research Coordinating Commit-tee of the National Institute forMedical Research in Tanzania(NIMR-MRCC) The investigators explained the purpose of
Table 1 Sociodemographic characteristics of the study population
Characteristics Frequency (119873) Proportion ()Age group in years18ndash31 36 13232ndash45 66 24546ndash59 58 21360ndash73 90 33174ndash87 22 81Sex ratio (female male) 33 239OccupationPeasant farmers 102 375Fishermen 170 625119873 number of individuals
the study and all study participants consented orally and inwriting
24 Clinical Examination A clinician experienced in LFexamined those patients and recorded the swelling of thelower limbs and scrotum in stages according to Meyrowitschet al [10] Thereafter a semistructured questionnaire wasused to collect the demographic information and other clin-ical disease conditions Individuals with lymphoedema andhydrocoele stages lower than III were treated with antibiotic(doxycycline or tetracycline) for 7 days and topical broad-spectrum antifungal cream as recommended by the studyphysician
25 Parasitological Examination Patients were then askedto donate 100 120583L for circulating filarial antigen examinationusing immune chromatographic test cards The BinaxNOWFilariasis immune chromatographic card test (Alere IncScarborough ME) was used to detect circulating filarial anti-gen as described in the WHO guidelines [11] Briefly 100120583Lof finger-prick blood was collected from each individualand then transferred to an immune chromatographic cardtest using a calibrated capillary tube The test was read 10minutes after closing the card as per the manufacturerrsquosinstructions The antigen contains the epitope present incirculating W bancrofti antigen that was detected by theBinaxNOWFilariasis testThe identification number and testresult of each individual tested were recorded in the casereport form
3 Results
A total of 472 individuals were examined during the com-munity survey among whom 651 (307) were males while349 (165) were females Of those 272 were recruited forthe study of whom 8786 were males and 1214 werefemales 119901 le 00001 The rest did not fulfil the inclusioncriteria as presented in the flow diagram (Figure 1)The studypopulation that was more frequently observed with highproportionwas the 32ndash45-year age groupwith a rate of 242followed by the 60ndash73-year age groupwith a rate of 331 andthe majority of them were fishermen (625) (Table 1)
Journal of Tropical Medicine 3
Total individuals screenedn = 472
Male n = 68 Male n = 307 Female n = 165 Female n = 132
Male n = 239(8786)
Female n = 33(1214)
Total individuals recruitedn = 272
Elig
ibili
tyIn
clude
dId
entifi
catio
nSc
reen
ing
Figure 1 Study profile of the individuals recruited in the cross-sectional survey in Tanga region
018ndash31 32ndash45 46ndash59 60ndash73 74ndash87
Age group
MaleFemale
05
1
15
2
25
3
35
4
45
Prop
ortio
ns (
)
Figure 2 Age distribution of lymphoedema pathology according tostages in the examined individuals
Females were observed to have a higher proportion oflymphoedema than males in the age group of 32ndash45 years(Figure 2) Figures 3 and 4 summarise the infection ratesin the study group whereby 551 of the 272 individualswere CFA-positive and the majority of those were males(33) Few of the confirmed CFA patients were females(221) The proportions of scrotal hydrocele in males above18 years old were high (732) as compared to lymphoedema(158) Conversely the proportion of individuals with bothlymphoedema and hydrocele was 551
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
HCHCampLE
0
5
10
15
20
25
30
Prop
ortio
ns (
)
Figure 3 Age distribution of scrotal hydrocoele pathology accord-ing to stages in those examined individuals HC hydrocoeleHCampLE hydrocoele and lymphoedema
4 Discussion
In our study hydrocoele has been shown to be the main pub-lic health problem causing debilitation in males and similarlylymphoedema in females as observed elsewhere [12] It hasalso been shown in our study that these conditions affectthe 32ndash45-year age group Recent studies focusing on themolecularmechanism regulating blood and lymphatic vesselsgrowth have shown that vascular endothelial growth factorscontrol angiogenesis and lymphangiogenesis in humans [13]which is a process of developing lymphangiectasia as a clinical
4 Journal of Tropical Medicine
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
CDAAInfection
0
5
10
15
20
25
30
Prop
ortio
ns (
)
Figure 4 Acute and chronic clinical disease stratified into agegroups CD chronic pathology (lymphedema hydrocele and lym-phedema combined with hydrocele) AA acute attacks (filarialfever) infection circulating filarial antigen (CFA)
disease Similarly expression of VEGF-A and VEGF-C hasbeen shown to be upregulated by proinflammatory cytokinesaffecting the lymphatic vessels in males [13] However cur-rently there is limited data on the heterogeneity of the diseaseSince the pathogenesis and development of lymphoedemaremain largely unknown there is a need for future studies toexplore the role of genetics in relation to clinical phenotypesto better understand the disease aetiology and optimise thecontrol strategies The results of this study suggest thatduring the era of lymphatic filariasis control of infectionsthe disease has shown a clear reduction of acute infectionandmorbidity rates compared to the baseline study especiallyin the older age group This could have been triggered bythe host human-immune and parasite interaction leadingto the clearance of acute infection [12] On the other handthe presence of adult worms and their secretions and thedeath of such adult worms may lead to dilatation of scrotallymphatic vessel causing dysfunction and accumulation ofprotein-rich fluid in the tissue causing lymphangiectasia [13]However there is still ongoing LF transmission in some ofthe studied communities in the region and it is unlikely thatthe annual single dose can interrupt the transmission andtherefore other strategies such as biannual administrationof MDA can be applied to interrupt the transmission asobserved in other studies In Figure 4 young age groups(18ndash31 years) have increasing acute and chronic infectionsA similar observation has been shown in Fiji [14] Theseare the productive segment in the communities indicatinga shifting trend of the clinical disease into the lower agegroups because low-level transmission continues in thosecommunities This could be possibly due to some existinghotspots in the communities whereby mosquito vectors pickinfection from humans and maintain the local transmission
[15] It is also likely that the postponement of the MDAdistribution within the timely scheduled period could havehalted reaching the desired coverage of at least 65 accordingto theWHO hence leading to LF resurgence [14] It is vital toexpand the frequency of drug administration to a maximumof three doses per year expand the age range of the targetpopulation and improve health education to the communitywith the aim of increasing coverage within the targetedareas Similarly we should conduct an anthropological studyto find out why transmission continues although MDA isin place tracking factors associated with that such as theincentive to drug distributors health system roles in thedistrict timely availability of drugs financial resources andadvocacy and training of distributors The need for adequatefinancial and logistics resources is paramount to successfullyachieve the targeted coverage and reach the end goal of theprogramme Adequate resources and infrastructural supportshould be available to ensure timely availability and supply oftheMDAdrugs to reach the implementation units in endemiccommunities Moreover more evidence is needed to assesswhether parasite genetic variability has implications in theeffectiveness of diagnostic test epidemiology and control ofthe disease [16] as well as cross-reactivity of the ICT cardto non-W bancrofti filariae that could reinforce doubts onthe validity of the current map of LF as observed in otherstudies [17] Formulation of guidelines for LF coendemicareas assessment is therefore very important It is worthalso addressing issues related to the vector for successfulcontrol of LF MDA in combination with other interventionssuch as insecticide-treated nets will improve reduction ofinfection and interrupt transmission of the infection in thecommunities However insecticide resistance could lead toa substantial increase and persistence of filarial infectionincidence [18]
5 Conclusion
Our findings have shown a considerable reduction in filar-ial infection However there is clear evidence of ongoingtransmission despite the 8 rounds of MDA using ivermectinand albendazole It is unlikely that annual mass drug admin-istration would interrupt filarial transmission thereforeoptimised strategies are needed to accelerate control andelimination of targets
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to the villagers in Tanga regionfor their dedicated cooperation and to the technical stafffromNIMR-Tanga (FidelisMumburi Xavaeli Ngowi CharlesGuzo and Tembo) for their assistance in the field and thelaboratory This study received financial support from Uni-versity Hospital Bonn Institute for Medical MicrobiologyImmunology and Parasitology (Grant Code PF 6732-1)
Journal of Tropical Medicine 5
References
[1] S Wynd W D Melrose D N Durrheim J Carron and MGyapong ldquoUnderstanding the community impact of lymphaticfilariasis a review of the sociocultural literaturerdquo Bulletin of theWorld Health Organization vol 85 no 6 pp 493ndash498 2007
[2] S Babu and T B Nutman ldquoImmunopathogenesis of lymphaticfilarial diseaserdquo Seminars in Immunopathology vol 34 no 6 pp847ndash861 2012
[3] WHO ldquoGlobal programme to eliminate lymphatic filariasisrdquoin A Handbook of Practical Entomology for National LymphaticFilariasis Elimination Programmes p 1 WHO 2013
[4] K Ichimori ldquoMDAmdashlymphatic filariasisrdquo Tropical Medicineand Health vol 42 no 2 supplement pp 21ndash24 2014
[5] E A Ottesen ldquoEditorial the global programme to eliminatelymphatic filariasisrdquoTropicalMedicine and InternationalHealthvol 5 no 9 pp 591ndash594 2000
[6] L Batsa Anti-wolbachia treatment of lymphatic filariasis andgenetic analysis of the pathology of lymphedema as a clinicalmanifestation of the disease [PhD dissertations] 2012
[7] P J Hotez and A Kamath ldquoNeglected tropical diseases in sub-Saharan Africa review of their prevalence distribution anddisease burdenrdquo PLoS Neglected Tropical Diseases vol 3 no 8article e412 2009
[8] P E Simonsen Y A Derua S M Magesa et al ldquoLymphaticfilariasis control in Tanga Region Tanzania status after eightrounds of mass drug administrationrdquo Parasites amp Vectors vol 7no 1 article 507 2014
[9] National Bureau of Statistics (NBS) andOffice of Chief Govern-ment Statistician Zanzibar (OCGS) 2012 Population and Hous-ing Census Population Distribution by Administrative Units KeyFindings The United Republic of Tanzania 2013
[10] D W Meyrowitsch P E Simonsen and W H MakundeldquoBancroftian filariasis analysis of infection and disease in fiveendemic communities of north-eastern Tanzaniardquo Annals ofTropical Medicine and Parasitology vol 89 no 6 pp 653ndash6631995
[11] L Original Preparing and Implementing a National Plan toEliminate Lymphatic Filariasis World Health 2000
[12] D G Addiss and M A Brady ldquoMorbidity management in theglobal programme to eliminate lymphatic filariasis a review ofthe scientific literaturerdquo Filaria Journal vol 6 article 2 2007
[13] K M Pfarr A Y Debrah S Specht and A Hoerauf ldquoFilariasisand lymphoedemardquo Parasite Immunology vol 31 no 11 pp664ndash672 2009
[14] M E Mwakitalu M N Malecela E M Pedersen F WMosha and P E Simonsen ldquoUrban lymphatic filariasis in themetropolis of Dar es Salaam Tanzaniardquo Parasites and Vectorsvol 6 article 286 p 13 2013
[15] R T Rwegoshora E M Pedersen D A Mukoko et alldquoBancroftian filariasis patterns of vector abundance and trans-mission in twoEast African communities with different levels ofendemicityrdquo Annals of Tropical Medicine and Parasitology vol99 no 3 pp 253ndash265 2005
[16] S Nuchprayoon A Junpee and Y Poovorawan ldquoRan-dom amplified polymorphic DNA (RAPD) for differentiationbetween Thai and Myanmar strains of Wuchereria bancroftirdquoFilaria Journal vol 6 no 6 article 6 2007
[17] S Wanji N Amvongo-Adjia A J Njouendou et al ldquoFurtherevidence of the cross-reactivity of the Binax NOW FilariasisICT cards to non- Wuchereria bancrofti filariae experimental
studies with Loa loa and Onchocerca ochengirdquo Parasites ampVectors vol 9 article 267 pp 1ndash10 2016
[18] N Protopopoff J Matowo R Malima et al ldquoHigh level ofresistance in the mosquito Anopheles gambiae to pyrethroidinsecticides and reduced susceptibility to bendiocarb in north-western Tanzaniardquo Malaria Journal vol 12 article 149 pp 1ndash82013
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Journal of Tropical Medicine 3
Total individuals screenedn = 472
Male n = 68 Male n = 307 Female n = 165 Female n = 132
Male n = 239(8786)
Female n = 33(1214)
Total individuals recruitedn = 272
Elig
ibili
tyIn
clude
dId
entifi
catio
nSc
reen
ing
Figure 1 Study profile of the individuals recruited in the cross-sectional survey in Tanga region
018ndash31 32ndash45 46ndash59 60ndash73 74ndash87
Age group
MaleFemale
05
1
15
2
25
3
35
4
45
Prop
ortio
ns (
)
Figure 2 Age distribution of lymphoedema pathology according tostages in the examined individuals
Females were observed to have a higher proportion oflymphoedema than males in the age group of 32ndash45 years(Figure 2) Figures 3 and 4 summarise the infection ratesin the study group whereby 551 of the 272 individualswere CFA-positive and the majority of those were males(33) Few of the confirmed CFA patients were females(221) The proportions of scrotal hydrocele in males above18 years old were high (732) as compared to lymphoedema(158) Conversely the proportion of individuals with bothlymphoedema and hydrocele was 551
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
HCHCampLE
0
5
10
15
20
25
30
Prop
ortio
ns (
)
Figure 3 Age distribution of scrotal hydrocoele pathology accord-ing to stages in those examined individuals HC hydrocoeleHCampLE hydrocoele and lymphoedema
4 Discussion
In our study hydrocoele has been shown to be the main pub-lic health problem causing debilitation in males and similarlylymphoedema in females as observed elsewhere [12] It hasalso been shown in our study that these conditions affectthe 32ndash45-year age group Recent studies focusing on themolecularmechanism regulating blood and lymphatic vesselsgrowth have shown that vascular endothelial growth factorscontrol angiogenesis and lymphangiogenesis in humans [13]which is a process of developing lymphangiectasia as a clinical
4 Journal of Tropical Medicine
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
CDAAInfection
0
5
10
15
20
25
30
Prop
ortio
ns (
)
Figure 4 Acute and chronic clinical disease stratified into agegroups CD chronic pathology (lymphedema hydrocele and lym-phedema combined with hydrocele) AA acute attacks (filarialfever) infection circulating filarial antigen (CFA)
disease Similarly expression of VEGF-A and VEGF-C hasbeen shown to be upregulated by proinflammatory cytokinesaffecting the lymphatic vessels in males [13] However cur-rently there is limited data on the heterogeneity of the diseaseSince the pathogenesis and development of lymphoedemaremain largely unknown there is a need for future studies toexplore the role of genetics in relation to clinical phenotypesto better understand the disease aetiology and optimise thecontrol strategies The results of this study suggest thatduring the era of lymphatic filariasis control of infectionsthe disease has shown a clear reduction of acute infectionandmorbidity rates compared to the baseline study especiallyin the older age group This could have been triggered bythe host human-immune and parasite interaction leadingto the clearance of acute infection [12] On the other handthe presence of adult worms and their secretions and thedeath of such adult worms may lead to dilatation of scrotallymphatic vessel causing dysfunction and accumulation ofprotein-rich fluid in the tissue causing lymphangiectasia [13]However there is still ongoing LF transmission in some ofthe studied communities in the region and it is unlikely thatthe annual single dose can interrupt the transmission andtherefore other strategies such as biannual administrationof MDA can be applied to interrupt the transmission asobserved in other studies In Figure 4 young age groups(18ndash31 years) have increasing acute and chronic infectionsA similar observation has been shown in Fiji [14] Theseare the productive segment in the communities indicatinga shifting trend of the clinical disease into the lower agegroups because low-level transmission continues in thosecommunities This could be possibly due to some existinghotspots in the communities whereby mosquito vectors pickinfection from humans and maintain the local transmission
[15] It is also likely that the postponement of the MDAdistribution within the timely scheduled period could havehalted reaching the desired coverage of at least 65 accordingto theWHO hence leading to LF resurgence [14] It is vital toexpand the frequency of drug administration to a maximumof three doses per year expand the age range of the targetpopulation and improve health education to the communitywith the aim of increasing coverage within the targetedareas Similarly we should conduct an anthropological studyto find out why transmission continues although MDA isin place tracking factors associated with that such as theincentive to drug distributors health system roles in thedistrict timely availability of drugs financial resources andadvocacy and training of distributors The need for adequatefinancial and logistics resources is paramount to successfullyachieve the targeted coverage and reach the end goal of theprogramme Adequate resources and infrastructural supportshould be available to ensure timely availability and supply oftheMDAdrugs to reach the implementation units in endemiccommunities Moreover more evidence is needed to assesswhether parasite genetic variability has implications in theeffectiveness of diagnostic test epidemiology and control ofthe disease [16] as well as cross-reactivity of the ICT cardto non-W bancrofti filariae that could reinforce doubts onthe validity of the current map of LF as observed in otherstudies [17] Formulation of guidelines for LF coendemicareas assessment is therefore very important It is worthalso addressing issues related to the vector for successfulcontrol of LF MDA in combination with other interventionssuch as insecticide-treated nets will improve reduction ofinfection and interrupt transmission of the infection in thecommunities However insecticide resistance could lead toa substantial increase and persistence of filarial infectionincidence [18]
5 Conclusion
Our findings have shown a considerable reduction in filar-ial infection However there is clear evidence of ongoingtransmission despite the 8 rounds of MDA using ivermectinand albendazole It is unlikely that annual mass drug admin-istration would interrupt filarial transmission thereforeoptimised strategies are needed to accelerate control andelimination of targets
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to the villagers in Tanga regionfor their dedicated cooperation and to the technical stafffromNIMR-Tanga (FidelisMumburi Xavaeli Ngowi CharlesGuzo and Tembo) for their assistance in the field and thelaboratory This study received financial support from Uni-versity Hospital Bonn Institute for Medical MicrobiologyImmunology and Parasitology (Grant Code PF 6732-1)
Journal of Tropical Medicine 5
References
[1] S Wynd W D Melrose D N Durrheim J Carron and MGyapong ldquoUnderstanding the community impact of lymphaticfilariasis a review of the sociocultural literaturerdquo Bulletin of theWorld Health Organization vol 85 no 6 pp 493ndash498 2007
[2] S Babu and T B Nutman ldquoImmunopathogenesis of lymphaticfilarial diseaserdquo Seminars in Immunopathology vol 34 no 6 pp847ndash861 2012
[3] WHO ldquoGlobal programme to eliminate lymphatic filariasisrdquoin A Handbook of Practical Entomology for National LymphaticFilariasis Elimination Programmes p 1 WHO 2013
[4] K Ichimori ldquoMDAmdashlymphatic filariasisrdquo Tropical Medicineand Health vol 42 no 2 supplement pp 21ndash24 2014
[5] E A Ottesen ldquoEditorial the global programme to eliminatelymphatic filariasisrdquoTropicalMedicine and InternationalHealthvol 5 no 9 pp 591ndash594 2000
[6] L Batsa Anti-wolbachia treatment of lymphatic filariasis andgenetic analysis of the pathology of lymphedema as a clinicalmanifestation of the disease [PhD dissertations] 2012
[7] P J Hotez and A Kamath ldquoNeglected tropical diseases in sub-Saharan Africa review of their prevalence distribution anddisease burdenrdquo PLoS Neglected Tropical Diseases vol 3 no 8article e412 2009
[8] P E Simonsen Y A Derua S M Magesa et al ldquoLymphaticfilariasis control in Tanga Region Tanzania status after eightrounds of mass drug administrationrdquo Parasites amp Vectors vol 7no 1 article 507 2014
[9] National Bureau of Statistics (NBS) andOffice of Chief Govern-ment Statistician Zanzibar (OCGS) 2012 Population and Hous-ing Census Population Distribution by Administrative Units KeyFindings The United Republic of Tanzania 2013
[10] D W Meyrowitsch P E Simonsen and W H MakundeldquoBancroftian filariasis analysis of infection and disease in fiveendemic communities of north-eastern Tanzaniardquo Annals ofTropical Medicine and Parasitology vol 89 no 6 pp 653ndash6631995
[11] L Original Preparing and Implementing a National Plan toEliminate Lymphatic Filariasis World Health 2000
[12] D G Addiss and M A Brady ldquoMorbidity management in theglobal programme to eliminate lymphatic filariasis a review ofthe scientific literaturerdquo Filaria Journal vol 6 article 2 2007
[13] K M Pfarr A Y Debrah S Specht and A Hoerauf ldquoFilariasisand lymphoedemardquo Parasite Immunology vol 31 no 11 pp664ndash672 2009
[14] M E Mwakitalu M N Malecela E M Pedersen F WMosha and P E Simonsen ldquoUrban lymphatic filariasis in themetropolis of Dar es Salaam Tanzaniardquo Parasites and Vectorsvol 6 article 286 p 13 2013
[15] R T Rwegoshora E M Pedersen D A Mukoko et alldquoBancroftian filariasis patterns of vector abundance and trans-mission in twoEast African communities with different levels ofendemicityrdquo Annals of Tropical Medicine and Parasitology vol99 no 3 pp 253ndash265 2005
[16] S Nuchprayoon A Junpee and Y Poovorawan ldquoRan-dom amplified polymorphic DNA (RAPD) for differentiationbetween Thai and Myanmar strains of Wuchereria bancroftirdquoFilaria Journal vol 6 no 6 article 6 2007
[17] S Wanji N Amvongo-Adjia A J Njouendou et al ldquoFurtherevidence of the cross-reactivity of the Binax NOW FilariasisICT cards to non- Wuchereria bancrofti filariae experimental
studies with Loa loa and Onchocerca ochengirdquo Parasites ampVectors vol 9 article 267 pp 1ndash10 2016
[18] N Protopopoff J Matowo R Malima et al ldquoHigh level ofresistance in the mosquito Anopheles gambiae to pyrethroidinsecticides and reduced susceptibility to bendiocarb in north-western Tanzaniardquo Malaria Journal vol 12 article 149 pp 1ndash82013
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Journal of Tropical Medicine
18ndash31 32ndash45 46ndash59 60ndash73 74ndash87Age group
CDAAInfection
0
5
10
15
20
25
30
Prop
ortio
ns (
)
Figure 4 Acute and chronic clinical disease stratified into agegroups CD chronic pathology (lymphedema hydrocele and lym-phedema combined with hydrocele) AA acute attacks (filarialfever) infection circulating filarial antigen (CFA)
disease Similarly expression of VEGF-A and VEGF-C hasbeen shown to be upregulated by proinflammatory cytokinesaffecting the lymphatic vessels in males [13] However cur-rently there is limited data on the heterogeneity of the diseaseSince the pathogenesis and development of lymphoedemaremain largely unknown there is a need for future studies toexplore the role of genetics in relation to clinical phenotypesto better understand the disease aetiology and optimise thecontrol strategies The results of this study suggest thatduring the era of lymphatic filariasis control of infectionsthe disease has shown a clear reduction of acute infectionandmorbidity rates compared to the baseline study especiallyin the older age group This could have been triggered bythe host human-immune and parasite interaction leadingto the clearance of acute infection [12] On the other handthe presence of adult worms and their secretions and thedeath of such adult worms may lead to dilatation of scrotallymphatic vessel causing dysfunction and accumulation ofprotein-rich fluid in the tissue causing lymphangiectasia [13]However there is still ongoing LF transmission in some ofthe studied communities in the region and it is unlikely thatthe annual single dose can interrupt the transmission andtherefore other strategies such as biannual administrationof MDA can be applied to interrupt the transmission asobserved in other studies In Figure 4 young age groups(18ndash31 years) have increasing acute and chronic infectionsA similar observation has been shown in Fiji [14] Theseare the productive segment in the communities indicatinga shifting trend of the clinical disease into the lower agegroups because low-level transmission continues in thosecommunities This could be possibly due to some existinghotspots in the communities whereby mosquito vectors pickinfection from humans and maintain the local transmission
[15] It is also likely that the postponement of the MDAdistribution within the timely scheduled period could havehalted reaching the desired coverage of at least 65 accordingto theWHO hence leading to LF resurgence [14] It is vital toexpand the frequency of drug administration to a maximumof three doses per year expand the age range of the targetpopulation and improve health education to the communitywith the aim of increasing coverage within the targetedareas Similarly we should conduct an anthropological studyto find out why transmission continues although MDA isin place tracking factors associated with that such as theincentive to drug distributors health system roles in thedistrict timely availability of drugs financial resources andadvocacy and training of distributors The need for adequatefinancial and logistics resources is paramount to successfullyachieve the targeted coverage and reach the end goal of theprogramme Adequate resources and infrastructural supportshould be available to ensure timely availability and supply oftheMDAdrugs to reach the implementation units in endemiccommunities Moreover more evidence is needed to assesswhether parasite genetic variability has implications in theeffectiveness of diagnostic test epidemiology and control ofthe disease [16] as well as cross-reactivity of the ICT cardto non-W bancrofti filariae that could reinforce doubts onthe validity of the current map of LF as observed in otherstudies [17] Formulation of guidelines for LF coendemicareas assessment is therefore very important It is worthalso addressing issues related to the vector for successfulcontrol of LF MDA in combination with other interventionssuch as insecticide-treated nets will improve reduction ofinfection and interrupt transmission of the infection in thecommunities However insecticide resistance could lead toa substantial increase and persistence of filarial infectionincidence [18]
5 Conclusion
Our findings have shown a considerable reduction in filar-ial infection However there is clear evidence of ongoingtransmission despite the 8 rounds of MDA using ivermectinand albendazole It is unlikely that annual mass drug admin-istration would interrupt filarial transmission thereforeoptimised strategies are needed to accelerate control andelimination of targets
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to the villagers in Tanga regionfor their dedicated cooperation and to the technical stafffromNIMR-Tanga (FidelisMumburi Xavaeli Ngowi CharlesGuzo and Tembo) for their assistance in the field and thelaboratory This study received financial support from Uni-versity Hospital Bonn Institute for Medical MicrobiologyImmunology and Parasitology (Grant Code PF 6732-1)
Journal of Tropical Medicine 5
References
[1] S Wynd W D Melrose D N Durrheim J Carron and MGyapong ldquoUnderstanding the community impact of lymphaticfilariasis a review of the sociocultural literaturerdquo Bulletin of theWorld Health Organization vol 85 no 6 pp 493ndash498 2007
[2] S Babu and T B Nutman ldquoImmunopathogenesis of lymphaticfilarial diseaserdquo Seminars in Immunopathology vol 34 no 6 pp847ndash861 2012
[3] WHO ldquoGlobal programme to eliminate lymphatic filariasisrdquoin A Handbook of Practical Entomology for National LymphaticFilariasis Elimination Programmes p 1 WHO 2013
[4] K Ichimori ldquoMDAmdashlymphatic filariasisrdquo Tropical Medicineand Health vol 42 no 2 supplement pp 21ndash24 2014
[5] E A Ottesen ldquoEditorial the global programme to eliminatelymphatic filariasisrdquoTropicalMedicine and InternationalHealthvol 5 no 9 pp 591ndash594 2000
[6] L Batsa Anti-wolbachia treatment of lymphatic filariasis andgenetic analysis of the pathology of lymphedema as a clinicalmanifestation of the disease [PhD dissertations] 2012
[7] P J Hotez and A Kamath ldquoNeglected tropical diseases in sub-Saharan Africa review of their prevalence distribution anddisease burdenrdquo PLoS Neglected Tropical Diseases vol 3 no 8article e412 2009
[8] P E Simonsen Y A Derua S M Magesa et al ldquoLymphaticfilariasis control in Tanga Region Tanzania status after eightrounds of mass drug administrationrdquo Parasites amp Vectors vol 7no 1 article 507 2014
[9] National Bureau of Statistics (NBS) andOffice of Chief Govern-ment Statistician Zanzibar (OCGS) 2012 Population and Hous-ing Census Population Distribution by Administrative Units KeyFindings The United Republic of Tanzania 2013
[10] D W Meyrowitsch P E Simonsen and W H MakundeldquoBancroftian filariasis analysis of infection and disease in fiveendemic communities of north-eastern Tanzaniardquo Annals ofTropical Medicine and Parasitology vol 89 no 6 pp 653ndash6631995
[11] L Original Preparing and Implementing a National Plan toEliminate Lymphatic Filariasis World Health 2000
[12] D G Addiss and M A Brady ldquoMorbidity management in theglobal programme to eliminate lymphatic filariasis a review ofthe scientific literaturerdquo Filaria Journal vol 6 article 2 2007
[13] K M Pfarr A Y Debrah S Specht and A Hoerauf ldquoFilariasisand lymphoedemardquo Parasite Immunology vol 31 no 11 pp664ndash672 2009
[14] M E Mwakitalu M N Malecela E M Pedersen F WMosha and P E Simonsen ldquoUrban lymphatic filariasis in themetropolis of Dar es Salaam Tanzaniardquo Parasites and Vectorsvol 6 article 286 p 13 2013
[15] R T Rwegoshora E M Pedersen D A Mukoko et alldquoBancroftian filariasis patterns of vector abundance and trans-mission in twoEast African communities with different levels ofendemicityrdquo Annals of Tropical Medicine and Parasitology vol99 no 3 pp 253ndash265 2005
[16] S Nuchprayoon A Junpee and Y Poovorawan ldquoRan-dom amplified polymorphic DNA (RAPD) for differentiationbetween Thai and Myanmar strains of Wuchereria bancroftirdquoFilaria Journal vol 6 no 6 article 6 2007
[17] S Wanji N Amvongo-Adjia A J Njouendou et al ldquoFurtherevidence of the cross-reactivity of the Binax NOW FilariasisICT cards to non- Wuchereria bancrofti filariae experimental
studies with Loa loa and Onchocerca ochengirdquo Parasites ampVectors vol 9 article 267 pp 1ndash10 2016
[18] N Protopopoff J Matowo R Malima et al ldquoHigh level ofresistance in the mosquito Anopheles gambiae to pyrethroidinsecticides and reduced susceptibility to bendiocarb in north-western Tanzaniardquo Malaria Journal vol 12 article 149 pp 1ndash82013
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Journal of Tropical Medicine 5
References
[1] S Wynd W D Melrose D N Durrheim J Carron and MGyapong ldquoUnderstanding the community impact of lymphaticfilariasis a review of the sociocultural literaturerdquo Bulletin of theWorld Health Organization vol 85 no 6 pp 493ndash498 2007
[2] S Babu and T B Nutman ldquoImmunopathogenesis of lymphaticfilarial diseaserdquo Seminars in Immunopathology vol 34 no 6 pp847ndash861 2012
[3] WHO ldquoGlobal programme to eliminate lymphatic filariasisrdquoin A Handbook of Practical Entomology for National LymphaticFilariasis Elimination Programmes p 1 WHO 2013
[4] K Ichimori ldquoMDAmdashlymphatic filariasisrdquo Tropical Medicineand Health vol 42 no 2 supplement pp 21ndash24 2014
[5] E A Ottesen ldquoEditorial the global programme to eliminatelymphatic filariasisrdquoTropicalMedicine and InternationalHealthvol 5 no 9 pp 591ndash594 2000
[6] L Batsa Anti-wolbachia treatment of lymphatic filariasis andgenetic analysis of the pathology of lymphedema as a clinicalmanifestation of the disease [PhD dissertations] 2012
[7] P J Hotez and A Kamath ldquoNeglected tropical diseases in sub-Saharan Africa review of their prevalence distribution anddisease burdenrdquo PLoS Neglected Tropical Diseases vol 3 no 8article e412 2009
[8] P E Simonsen Y A Derua S M Magesa et al ldquoLymphaticfilariasis control in Tanga Region Tanzania status after eightrounds of mass drug administrationrdquo Parasites amp Vectors vol 7no 1 article 507 2014
[9] National Bureau of Statistics (NBS) andOffice of Chief Govern-ment Statistician Zanzibar (OCGS) 2012 Population and Hous-ing Census Population Distribution by Administrative Units KeyFindings The United Republic of Tanzania 2013
[10] D W Meyrowitsch P E Simonsen and W H MakundeldquoBancroftian filariasis analysis of infection and disease in fiveendemic communities of north-eastern Tanzaniardquo Annals ofTropical Medicine and Parasitology vol 89 no 6 pp 653ndash6631995
[11] L Original Preparing and Implementing a National Plan toEliminate Lymphatic Filariasis World Health 2000
[12] D G Addiss and M A Brady ldquoMorbidity management in theglobal programme to eliminate lymphatic filariasis a review ofthe scientific literaturerdquo Filaria Journal vol 6 article 2 2007
[13] K M Pfarr A Y Debrah S Specht and A Hoerauf ldquoFilariasisand lymphoedemardquo Parasite Immunology vol 31 no 11 pp664ndash672 2009
[14] M E Mwakitalu M N Malecela E M Pedersen F WMosha and P E Simonsen ldquoUrban lymphatic filariasis in themetropolis of Dar es Salaam Tanzaniardquo Parasites and Vectorsvol 6 article 286 p 13 2013
[15] R T Rwegoshora E M Pedersen D A Mukoko et alldquoBancroftian filariasis patterns of vector abundance and trans-mission in twoEast African communities with different levels ofendemicityrdquo Annals of Tropical Medicine and Parasitology vol99 no 3 pp 253ndash265 2005
[16] S Nuchprayoon A Junpee and Y Poovorawan ldquoRan-dom amplified polymorphic DNA (RAPD) for differentiationbetween Thai and Myanmar strains of Wuchereria bancroftirdquoFilaria Journal vol 6 no 6 article 6 2007
[17] S Wanji N Amvongo-Adjia A J Njouendou et al ldquoFurtherevidence of the cross-reactivity of the Binax NOW FilariasisICT cards to non- Wuchereria bancrofti filariae experimental
studies with Loa loa and Onchocerca ochengirdquo Parasites ampVectors vol 9 article 267 pp 1ndash10 2016
[18] N Protopopoff J Matowo R Malima et al ldquoHigh level ofresistance in the mosquito Anopheles gambiae to pyrethroidinsecticides and reduced susceptibility to bendiocarb in north-western Tanzaniardquo Malaria Journal vol 12 article 149 pp 1ndash82013
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom