RESEARCH AND DEVELOPMENT GRANTS 2012/13 · Simulation Fellow Luke Regan ... patient based on ward...
28
CLINICAL SKILLS MANAGED EDUCATIONAL NETWORK RESEARCH AND DEVELOPMENT GRANTS 2012/13 RESEARCH REPORT Title Medical Students Driven to Distraction. Improving patient safety teaching through the use of a simulated ward round experience: a prospective control study Author Ian Thomas Highland Medical Education Centre, University of Aberdeen, Centre for Health Sciences, Old Perth Road, Inverness. Contributors Ian Thomas Clinical Teaching Fellow Laura Nicol Simulation Fellow Luke Regan Clinical Teaching Fellow Drieka Maliepaard Clinical Skills Facilitator Lindsay Clark Clinical Skills Facilitator Kenneth Walker Consultant surgeon John Duncan Consultant surgeon The author would like to thank the Clinical Skills Managed Educational Network for its generous support – without which this study would not have been completed.
Transcript of RESEARCH AND DEVELOPMENT GRANTS 2012/13 · Simulation Fellow Luke Regan ... patient based on ward...
CLINICAL SKILLS MANAGED EDUCATIONAL NETWORK
RESEARCH AND DEVELOPMENT GRANTS 2012/13
RESEARCH REPORT
Title
Medical Students Driven to Distraction.
Improving patient safety teaching through the use of
a simulated ward round experience: a prospective control study
Author
Ian Thomas
Highland Medical Education Centre, University of Aberdeen,
Centre for Health Sciences, Old Perth Road, Inverness.
Contributors Ian Thomas
Clinical Teaching Fellow
Laura Nicol
Simulation Fellow
Luke Regan
Clinical Teaching Fellow
Drieka Maliepaard
Clinical Skills Facilitator
Lindsay Clark
Clinical Skills Facilitator
Kenneth Walker
Consultant surgeon
John Duncan
Consultant surgeon
The author would like to thank the Clinical Skills Managed Educational Network for its
generous support – without which this study would not have been completed.

1
MEDICAL STUDENTS DRIVEN TO DISTRACTION
IMPROVING PATIENT SAFETY TEACHING THROUGH THE USE OF
A SIMULATED WARD ROUND EXPERIENCE: A PROSPECTIVE CONTROL STUDY
ABSTRACT
INTRODUCTION
Medical error is common, with poor situational awareness an important aetiological dynamic.
This is a key consideration for junior doctors, for whom distraction and interruption are
endemic in clinical work.
RESEARCH QUESTIONS
The objectives of this study are:
• To explore in a simulated ward experience, if final year medical undergraduates are
able to manage realistic ward-based distractions in order to mitigate medical error.
If this is not the case, then:
• Can a simulated ward experience with feedback be used to improve distractor
management to reduce medical-error making behaviour?
METHODS
A simulated ward round experience for undergraduates was designed with a focus on
distraction and medical error. Conducted as a prospective control trial, 14 students were
enrolled to an intervention group. Students undertook a baseline ward round and received
feedback focused on distractor management and medical error. Four weeks later, students

2
participated in a post-intervention ward round. An independent group of 14 students were
recruited to a control group – who underwent the same experience, but with no targeted
feedback between simulations. Error rates and distractor management was assessed during
simulations.
RESULTS
There was significant positive correlation between medical error-making and the
mismanagement of distractions. At baseline total medical error rates were high – with 72 and
76 documented mistakes in the intervention and control groups respectively.
All forms of simulation training reduced medical error post-intervention: with medical error-
making falling by 76% in the intervention group (p-value <0.0001) and 42% in the control
group (p-value <0.0001).
DISCUSSION & CONCLUSION
Medical students are not equipped to manage ward-based distractions in order to mitigate
medical error. These skills can be taught through simulation. This is the first study of its
kind to demonstrate an undergraduate teaching intervention with improvement in patient
safety behaviour. Curricular integration of the simulated ward round experience is
recommended.

3
INTRODUCTION
Despite best intentions, many patients worldwide suffer avoidable iatrogenic harm. In the
United States 98,000 deaths per year are directly attributable to medical error. 1 Worldwide,
this equates to 6 daily aircraft crashes without survivors. 2 Medical error has persisted
throughout the decades, 3, 4, 5 despite significant technological advances – and arguably non-
technical skills 6 are now the rate-limiting step. A breakdown in these skills is responsible for
56-82% of healthcare-related errors. 7&8 Healthcare professionals must be grounded in non-
technical skills and in particular situational awareness – as dealing with interruption and
multi-tasking are an integral part of the job. 9, 10, 11, 12 Clinician-stress has been shown to
heighten clinical error 13, 14, 15 and indeed distraction plays a central role. 16, 17 It is junior
trainees who report the highest levels of stress in clinical practice. 18 Unfortunately, stress
conversion into medical error is also highest amongst trainee cohorts, 19, 20 a group that feels
ill-prepared by medical school curriculums for managing heavy workloads and prioritising. 21
Medical educators should seek innovative learning experiences to teach non-technical and
patient safety skills to undergraduates. This is in line with the World Health Organisation’s 22
Patient Safety Curriculum and advice from the General Medical Council 23 endorsing the use
of simulated training environments. Simulation has contributed to our understanding of the
detrimental clinical impact of interruption on adherence to protocols, 24 performance in
emergency scenarios, 25, 26 clinical reasoning 27 and accurate calculating of drug doses. 28 As
new graduates will initially work within a ward setting – the environment most prone to
clinical error 29 it is logical to consider a simulated ward experience as a potential teaching
modality.
Nikendi 30 argues that:

4
‘‘Ward round training which eases the transition from observing ward rounds to conducting
them on one’s own is urgently required.’’
There has since been a trend to greater utilisation of simulated ward experiences 31, 32 with
newer generations 33, 34 concentrating on the impact of ward-based distraction. However,
these have merely documented participant acceptability and quantified baseline medical error
rates.
Although the body of evidence is growing, it stops short of demonstrable behavioural change.
Research which shows that simulated ward rounds can achieve this is required.
The objectives of this study are:
• To explore in a simulated ward experience, if final year medical undergraduates are
able to manage realistic ward-based distractions in order to mitigate medical error.
If this is not the case, then:
• Can a simulated ward experience with feedback be used to improve distractor
management to reduce medical-error making behaviour?

5
PEDAGOGICAL DEVELOPMENT OF THE SIMULATED WARD EXPERIENCE
A simulated ward round experience was created at the University of Aberdeen for final year
medical students with a focus on distraction and medical error.
Medical students played the part of a Foundation doctor leading a 30-minute ward round,
consisting of three patients, as shown in Figure 1.
Figure 1 – Role allocation during simulation
Patient with pneumonia:
played by a volunteer
patient.
Foundation doctor: played
by a final year medical
student. Leads the ward
round, makes diagnoses and
appropriate management
plans.
Staff nurse: played by a clinical skills
facilitator. Gives an appropriate
handover of patients to the doctor
and assists with execution of
management plans.
Patient notes
Video-recording equipment

6
Three patient scenarios were designed:
• An elderly lady with pneumonia
• A post-operative male patient with chest pain
• An elderly diabetic male with confusion
At each bed space the doctor was expected to complete a number of clinical duties, with
associated potential medical errors as shown in Figure 2.
As shown in Figures 3 and 4, a set of six realistic, time-critical distractions were deployed.
During simulation the student’s performance was assessed with medical errors and distractor
management recorded on a standardised checklist.

7
Figure 2 – Expected task completion and associated errors during the ward round
Expected task completion
Potential associated medical errors
At start of the simulation
Correctly prioritizes patients (chest pain,
followed by pneumonia then cognitive
impairment)
Does not correctly prioritize patients
Bed 1 – Clinical Problem: Pneumonia
Correctly diagnoses pneumonia
Fails to reach or gives incorrect diagnosis.
Staff nurse has to prompt with diagnosis
Utilizes blood results to calculate patient’s
CURB-65 score
Does not recognize that blood results in notes
do not correspond to correct patient
Correctly calculates CURB-65 score as a
marker of disease severity
Incorrectly calculates CURB-65 score and
nurse must provide appropriate score
Prescribes appropriate antibiotic therapy for
patient based on ward protocol
Fails to recognize patient is allergic to first-
line therapy
Correctly checks antibiotic vial with nurse
ahead of medication administration
Authorizes administration of date-expired
medication vial
Bed 2 – Clinical Problem: Post-operative chest pain
Correctly diagnoses non-ST elevation
myocardial infarction (NSTEMI)
Fails to reach or gives incorrect diagnosis.
Staff nurse has to prompt with diagnosis
Prescribes appropriate therapy for NSTEMI
based on ward protocol
Fails to appreciate patient is post-operative
and anti-coagulation is contraindicated
Nurse asks doctor to prescribe Paracetemol
for patient on regular Co-codamol.
Fails to recognize patient receiving Co-
codamol and Paracetemol contraindicated
Bed 3 – Clinical Problem: Diabetic with cognitive impairment
Amends Insulin dose as per recommendation
in notes from diabetic specialist nurse
Misreads handwritten entry in notes as 25
units: and not 2.5 units: resulting in overdose.
Deals with upset relative who comes into the
ward wanting to speak to the doctor
Does not check relative’s identity and
discloses information on incorrect patient

8
Figure 3 – Ward round facilitation with distraction deployment
Facilitators and assessors sat behind the one-way mirror overlooking the simulated
ward. Time-critical distractions were orchestrated from the observation suite with
communication established through the use of ear pieces and microphones.
One-way mirror Ear piece
Microphone
Timed-distractions
checklist
IT equipment to
facilitate
simulation
Doctor answering his page during simulation
Domestic hoovering at patient bedside as
doctor prescribes
Ward radio switched on at start of simulation
exercise

9
Figure 4 – List of standardised time-critical distractions
Distraction Time-critical deployment Potential associated medical
error
Ward radio switched on
(at 70 decibels)
At the start of the ward
round
Doctor incorrectly prioritizes
order of patients to be seen
Domestic hoovers at the
patient bed space
When the doctor is
reviewing the antibiotic
protocol for chest infection
Doctor prescribes protocol-
driven antibiotic to which
patient is allergic
Doctor’s pager set off
When doctor is reviewing
the chest pain protocol
Doctor prescribes protocol-
driven anti-coagulation and
fails to appreciate patient is
immediately post-operative
Nurse asks doctor to
prescribe Paracetemol for
separate unrelated patient
As doctor is prescribing
protocol-driven chest pain
medication on drug kardex
Prescribes anticoagulation +/-
makes any other related
prescription error
Telephone call into the ward
As doctor is reviewing the
diabetic specialist nurses’
written request in the
medical notes to increase
dose of Insulin to 2.5 units
Misreads handwriting and
prescribes an overdose of 25
units of insulin instead of
desired 2.5 units
Dealing with upset relative
who enters ward and wishes
to speak with the doctor
As student is prescribing
change of Insulin dose on
drug kardex
Fails to check identity of
relative and discloses
confidential information
pertaining to a different
patient

10
METHODS
A prospective control study was conducted, as shown in Figure 5. 14 students were recruited
to an intervention group by simple randomisation and undertook a baseline ward round.
Post-simulation students received immediate individualized feedback, targeted around
distractor management and its relationship to medical error using SET-GO criteria. 35
Following a lag time of 4 weeks students completed a post-intervention ward round of
comparable rigour, achieved by modification of the baseline ward round’s surface
characteristics. Separately, 14 students were similarly recruited to a control group who
undertook the same experience, but did not receive targeted feedback on distraction and error.
Medical error rates and distractor management was assessed at all simulations.

11
Figure 5 – Study design flow diagram
September
2013
Eligibility: 26 final year medical
students at University of Aberdeen
Eligibility: 25 final year medical
students at University of Aberdeen Volunteers: 20 students Volunteers: 22 students
Recruitment: 14 students Recruitment: 14 students
Baseline
Ward round
Baseline
Ward round
Targeted
feedback No targeted
feedback
Post-intervention
ward round
Post-intervention
ward round
Dropout rate:
Intervention group N=0
Control group N=0
Data analysis: 14 students Data analysis: 14 students
Exclusion rate:
Intervention group N=0
Control group N=0
October
2013
November
2013
December
2013
12
RESULTS
Study demographics
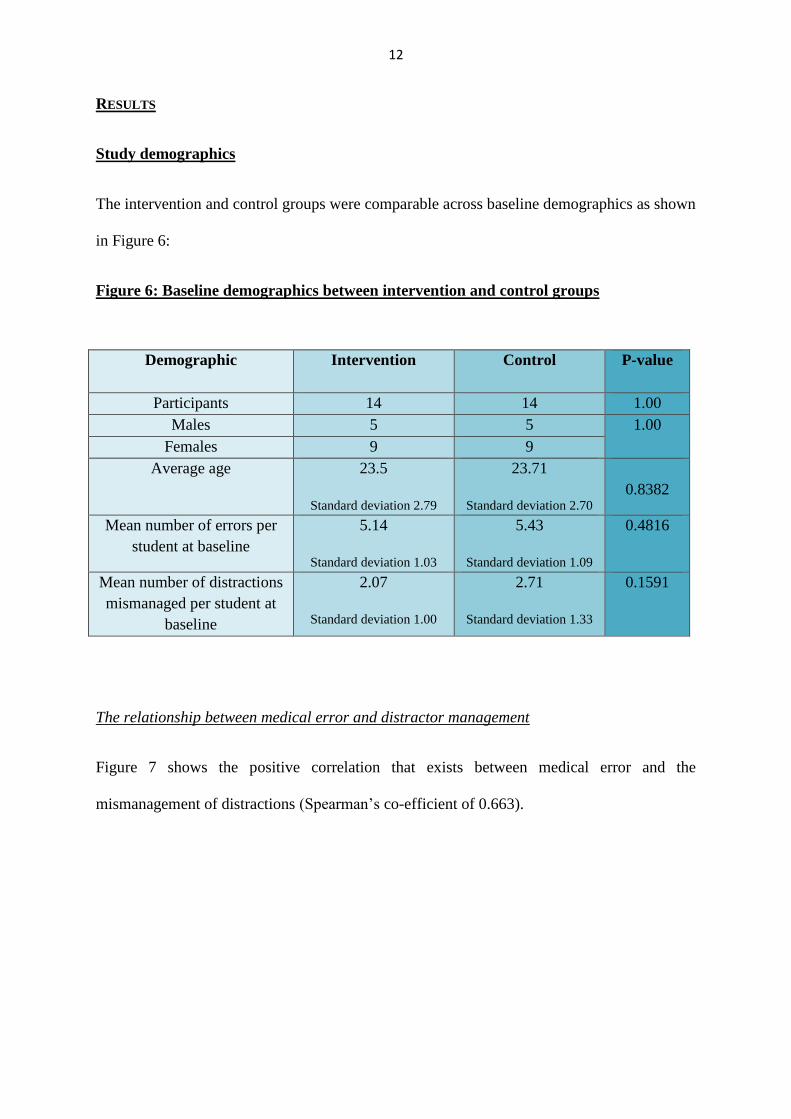
The intervention and control groups were comparable across baseline demographics as shown
in Figure 6:
Figure 6: Baseline demographics between intervention and control groups
Demographic
Intervention Control P-value
Participants 14 14 1.00
Males 5 5 1.00
Females 9 9
Average age 23.5
Standard deviation 2.79
23.71
Standard deviation 2.70
0.8382
Mean number of errors per
student at baseline
5.14
Standard deviation 1.03
5.43
Standard deviation 1.09
0.4816
Mean number of distractions
mismanaged per student at
baseline
2.07
Standard deviation 1.00
2.71
Standard deviation 1.33
0.1591
The relationship between medical error and distractor management
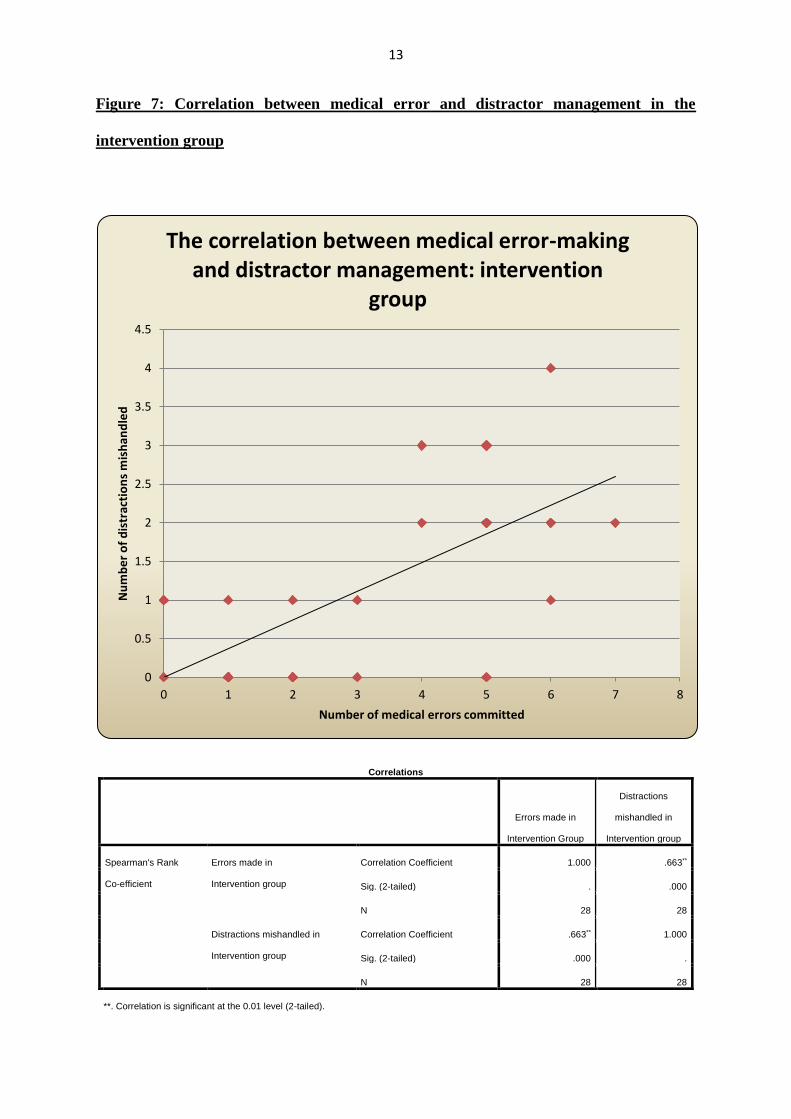
Figure 7 shows the positive correlation that exists between medical error and the
mismanagement of distractions (Spearman’s co-efficient of 0.663).
13
Figure 7: Correlation between medical error and distractor management in the
intervention group
Correlations
Errors made in
Intervention Group
Distractions
mishandled in
Intervention group
Spearman's Rank
Co-efficient
Errors made in
Intervention group
Correlation Coefficient 1.000 .663**
Sig. (2-tailed) . .000
N 28 28
Distractions mishandled in
Intervention group
Correlation Coefficient .663** 1.000
Sig. (2-tailed) .000 .
N 28 28
**. Correlation is significant at the 0.01 level (2-tailed).
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 1 2 3 4 5 6 7 8
Nu
mb
er
of
dis
trac
tio
ns
mis
han
dle
d
Number of medical errors committed
The correlation between medical error-making and distractor management: intervention
group
14
Baseline medical errors and distractor management
In the intervention group a total of 72 medical errors were committed at baseline,
representing a mean of 5.14 errors per student. In the control group baseline medical errors
were similar – with 76 medical errors witnessed (mean 5.43 medical errors per student).
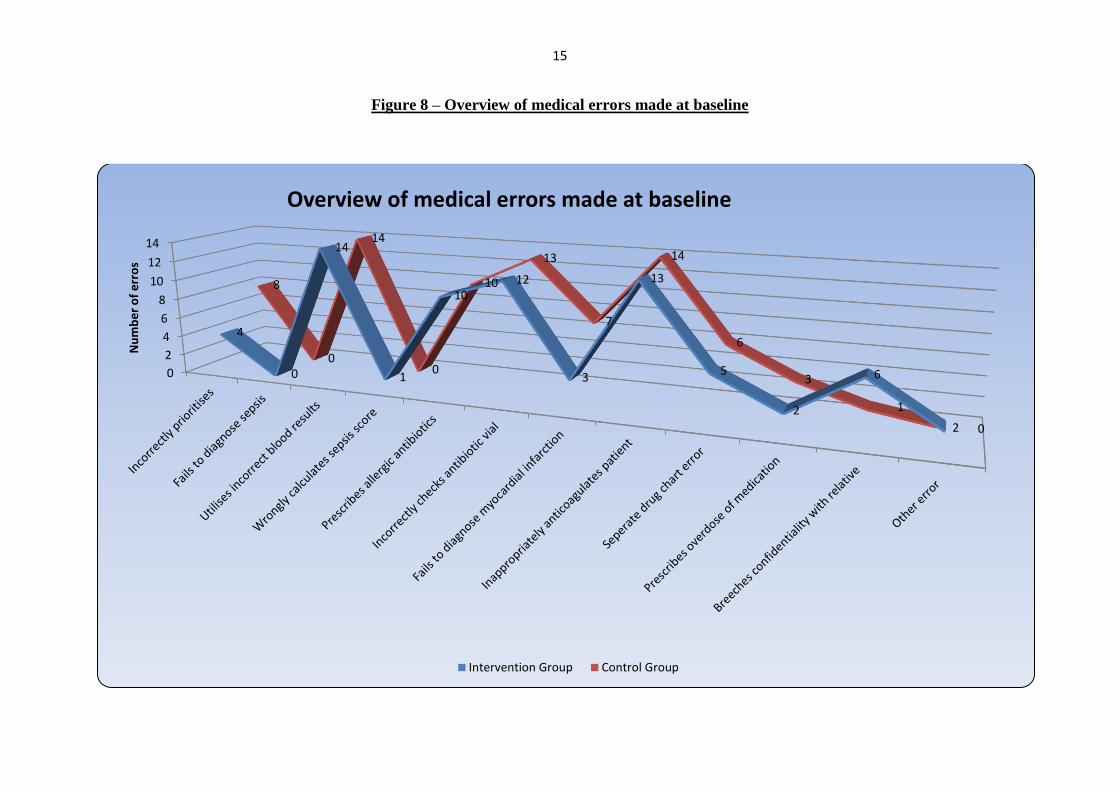
The pattern of error between intervention and control groups mirrored one another closely as
shown in Figure 8.
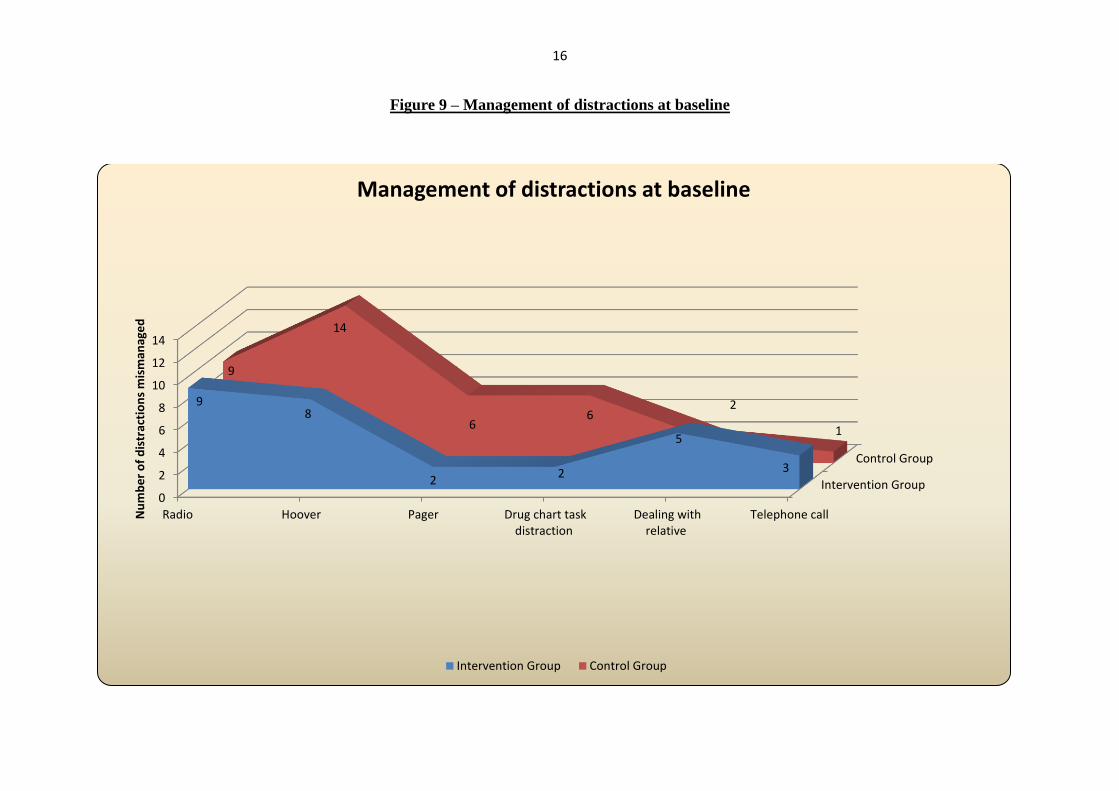
At baseline distractions were poorly managed in both groups. In the intervention group a
total of 29 distractions were mishandled compared to 38 in the control group. The pattern of
distractor management between groups at baseline is shown in Figure 9.
15
Figure 8 – Overview of medical errors made at baseline
0
2
4
6
8
10
12
14
4
0
14
1
1012
3
13
5
2
6
2
8
0
14
0
10
13
7
14
6
3
1
0
Nu
mb
er
of
err
os
Overview of medical errors made at baseline
Intervention Group Control Group
16
Figure 9 – Management of distractions at baseline
Intervention Group
Control Group
0
2
4
6
8
10
12
14
Radio Hoover Pager Drug chart taskdistraction
Dealing withrelative
Telephone call
98
22
5
3
9
14
66
2
1
Nu
mb
er
of
dis
trac
tio
ns
mis
man
age
d
Management of distractions at baseline
Intervention Group Control Group

17
Change in patient safety behaviours between simulations
At post-intervention medical error making fell in both groups – showing that any form of
simulation benefits patient safety behaviours. The reduction in error-rates between baseline
and post-intervention simulations is shown in Figure 10. In the intervention arm medical
errors post-intervention fell by 76.39% (p-value <0.0001), compared to 42.11% (p-value
<0.0001) in the control arm. Although medical error rates fell in both groups, intervention
conferred an additional 34.28% improvement over control (p-value 0.0016).
Figure 11 gives an overview of the errors that that persisted at the post-intervention
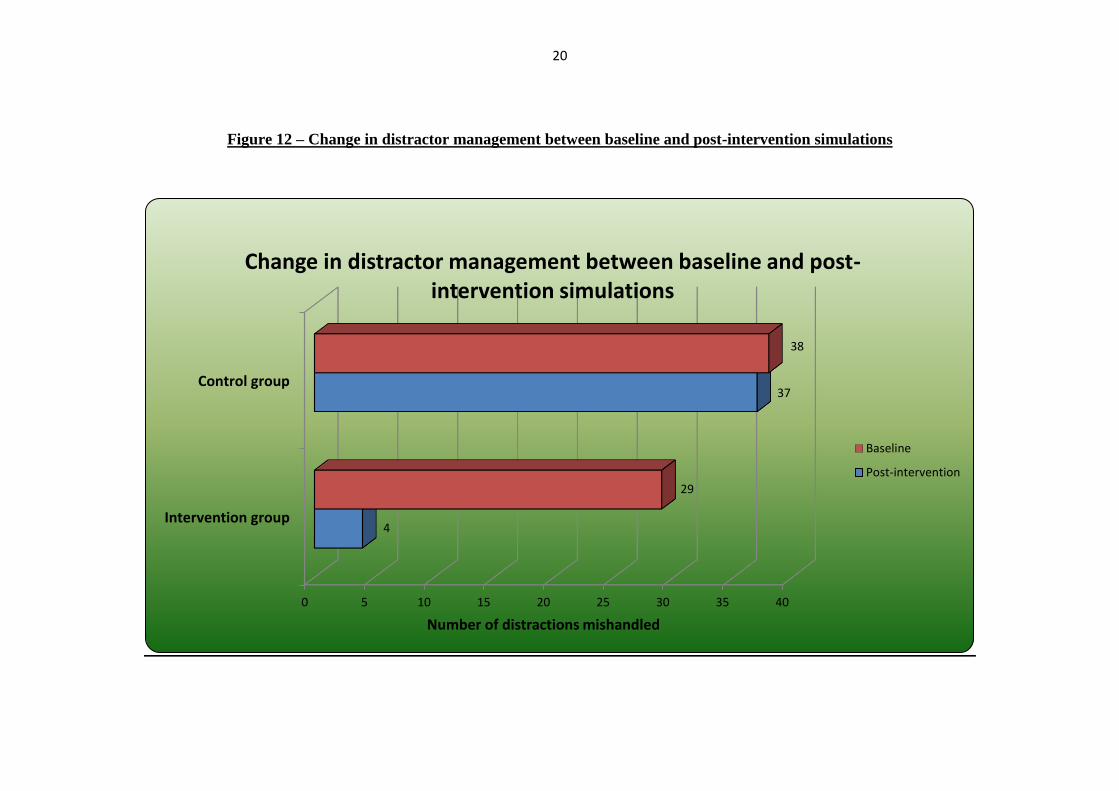
simulation. Figure 12 outlines the change in distractor management between simulations. In
the intervention group distractor management improved by 86.21% (p-value <0.0001):
whereas in the control group there was a 2.63% improvement (p-value 0.7929).

18
Figure 10 – Change in error making rates between baseline and post-intervention simulations
0
10
20
30
40
50
60
70
80
Total errors in Interventiongroup
Total errors in Controlgroup
Life threatening errors inIntervention group
Life threatening errors inControl group
7276
2527
17
44
6
18
Nu
mb
er o
f er
rors
co
mm
itte
d
Reduction in medical error rates between baseline and post-intervention simulations
Baseline Post-intervention

19
Figure 11 – Overview of medical errors made at post-intervention
0
2
4
6
8
10
12
14
0 0
5
21 2
0
4
0
3
00
4
0
14
1
6
10
8
24
13
Nu
mb
er
of
err
os
Overview of medical errors made at post-intervention simulation
Intervention Group Control Group
20
Figure 12 – Change in distractor management between baseline and post-intervention simulations
0 5 10 15 20 25 30 35 40
Intervention group
Control group
4
37
29
38
Number of distractions mishandled
Change in distractor management between baseline and post-intervention simulations
Baseline
Post-intervention
21
Students completed an online electronic questionnaire on their experience of the simulated
ward round. 27 out of 28 students completed the evaluation (response rate = 96.43%). The
simulations were deemed to be valuable and of high-fidelity. All students felt that mandatory
integration of this experience into the final year curriculum to be important.
22
DISCUSSION
Final year medical students are not equipped with the skills to manage ward-based
distraction, in order to mitigate common medical error. This research is one of the first
studies of its kind to demonstrate that simulated ward training can improve undergraduate
patient safety behaviours.
The study suggests that didactic patient safety teaching is of limited benefit to
undergraduates. All students at the start of the academic year (and prior to study
commencement) received didactic teaching on a range of patient safety domains: including
non-technical skills and dealing with stress at work. Despite such instruction, students
committed large numbers of medical errors at baseline simulation.
Study limitations
• The study was conducted a small single-centre trial with 14 participants in each arm.
Despite the small sample size, study power was over 80% owing to the magnitude of
error-reduction rates.
• Despite randomisation the author accepts the potential for selection bias. Participants
took part on a voluntary basis – and arguably an engaged volunteer cohort, may be most
amenable to the effects of simulation and feedback.
• This study was not designed as a randomised control trial. This could have been achieved
by recruiting all participants at the same time in the academic calendar. However, all
students share on-site accommodation. As such, there was concern about cross-
contamination.
• Feedback delivered to the intervention group focussed on both distractor management and
medical error. Future studies should include additional intervention arms. For example,
feedback on distractor management alone.
23
RECOMMENDATION
Consideration to curricular integration of simulated ward experience is recommended. The
cost of running a single day of simulation, as described, per student is £61 (which includes
consumables and faculty cost). However, modalities to minimise cost and reduce faculty
burden to potentiate feasibility exist. For research purposes the simulated ward round
experience was faculty-intensive. Pragmatically, this experience could be resourced by three
volunteer patients, one staff nurse and a single clinical teaching fellow. To increase student
throughput, having a two-patient ward round would minimise simulation duration to 20
minutes, and increase daily capacity to 17 students. Revised costings for the faculty-light
simulation are £27.52 per student.
The following three areas of future research are suggested:
• Evidencing a curriculum-feasible version of the simulation, suitable for institutional roll-
out.
• Development and assessment of this teaching modality as a vehicle for inter-professional
education.
• To assess the predictive validity of a simulated ward round in assessing future
performance. For example, do simulated ward round behaviours transfer into clinical
practice?
24
CONCLUSION
The development of the experience comes at a pivotal time in medical education: in wake of
the recent Francis 36 report – an era that will see patient safety teaching in undergraduate
curriculums come under much sharper focus. Incorporation of simulation-based education
into undergraduate institutions is challenging. However curricular integration as outlined by
best practice in simulation 37 is essential if the benefits of simulation are to be realised. Given
student acceptability and positive patient safety behavioural change, curricular integration is a
challenge that medical educators must now meet - as pragmatic solutions to potentiate
feasibility exist.
Word count = 1500 words
(Excluding abstract and references)

25
REFERENCES
Citation Reference
1 KOHN, L. et al., 2000.
To err is Human – Building a safer health system.
1st Edition. National Academy Press. Washington, D.C.
2 NULL, G. et al., 2003.
Death by medicine
http://www.webdc.com/pdfs/deathbymedicine.pdf (Accessed 05.10.13)
3 SCHIMMEL, E., 1964.
The hazards of hospitalization. Annals of Internal Medicine, 60: pp. 100-110
4 STEEL, K. et al., 1981.
Iatrogenic illness on a general medical service at a university hospital. New
England Journal of Medicine, 304: pp. 638-642
5 BEDELL, S. et al., 1991.
Incidence and characteristics of preventable iatrogenic cardiac arrest. Journal
of the American Medical Association, 265(21), pp. 2815-2820
6 FLIN, R. et al., 2008.
Safety at the Sharp End: A guide to non-technical skills. Aldershot: Ashgate
Publishing.
7 SCHAREIN, P. and TRENDELENBURG, M., 2013.
Critical incidents in a tertiary care clinic for internal medicine. Biomed Central
Research Notes, 16(6), pp. 276
8 COOPER, J. et al., 1978.
Preventable anaesthesia mishaps: a study of human factors. Anaesthesiology,
49(6), pp. 399-406
9 SPENCER, R. et al., 2004.
Variation in communication loads on clinical staff in the emergency
department. Annals of Emergency Medicine, 44(3), pp. 268-273
10 TIPPING, M. et al., 2010.
Where did the day go? A time-motion study of hospitalists. Journal of Hospital
Medicine, 5(6), pp. 323-328
11 WEIGL, M. et al., 2013.
Relationship of multitasking, physicians’ strain and performance: an
observation study in ward physicians. Journal of Patient Safety, 9(1), pp. 18-23
12 WEIGL, M. et al., 2011.
Hospital doctors’ workflow interruptions and activities: an observation study.
British Medical Journal of Quality and Safety, 20(6), pp. 491-497
13 HOUSTON, D. et al., 1997.
Psychological distress and error making among junior house officers. British
Journal of Health Psychology, 2(2), pp. 141–151.
14 FIRTH-COZENS, J. et al., 1997.
Doctors’ perceptions of the links between stress and lowered clinical care.
Social Science and Medicine, 44(7), pp. 1017-1022
15 FEDDOCK, C. et al., 2007.
Do pressure and fatigue influence resident job performance? Medical Teacher,
29(5), pp.495-497
26
16 WESTBROOK, J. et al., 2010.
Association of interruptions with an increased risk and severity of medication
administration errors.
Archives of Internal Medicine, 170(8), pp. 683-690
17 MOORTHY, K. et al., 2003.
The effect of stress-inducing conditions on the performance of a laparoscopic
task. Surgical Endoscopy, 17(9), pp. 1481-1484
18 STUCKY, E. et al., 2009.
Intern to attending: assessing stress among physicians. Academic Medicine,
84(2): 251-257
19 ARORA, S. et al., 2010.
The impact of stress on surgical performance: a systematic review of the
literature. Surgery, 147(3), pp. 318-330
20 PERSOON, M. et al., 2011
The effect of distraction in the operating room during endourological
procedures. Surgical Endoscopy, 25(2), pp. 437-443
21 ILLING, J. et al., 2008.
How prepared are medical graduates to begin practice? A comparison of three
diverse UK medical schools.
The General Medical Council.
http://www.gmcuk.org/FINAL_How_prepared_are_medical_
graduates_to_begin_practice_September_08.pdf_29697834.pdf
(Accessed 15.09.13)
22 WORLD HEALTH ORGANISATION, 2009
WHO Patient Safety Curriculum Guide. World Health Organisation.
http://www.who.int/patientsafety/education/curriculum/en/
(Accessed 15.09.13)
23 GENERAL MEDICAL COUNCIL, 2009.
Tomorrow’s Doctors. GMC.
http://www.gmcuk.org/TomorrowsDoctors_2009.pdf_39260971.pdf (Accessed 18.10.13)
24 LIU, D. et al., 2009.
Interruptions and blood transfusion checks: lessons from the simulated
operating room.
Anesthesia and Analgesia, 108(1), pp. 219-222
25 MERRY, A. et al., 2008.
A simulation design for research evaluating safety innovations in anaesthesia.
Anaesthesia, 63(12), pp. 1349-1357
26 HARVEY, A. et al, 2012.
Impact of stress on resident performance in simulated trauma scenarios. Journal
of Trauma and Acute Care Surgery, 72(2), pp. 497-503
27 POTTIER, P. et al., 2013.
Effect of stress on clinical reasoning during simulated ambulatory consultations.
Medical Teacher, 35(6), pp. 472-480
28 LEBLANC, V. et al., 2005.
Paramedic performance in calculating drug doses following stressful scenarios
in a human patient simulator. Pre-hospital Emergency Care, 9(4), pp. 439-444
29 NEALE, G. et al., 2001.
Exploring the causes of adverse events in NHS hospital practice. Journal of the

27
Royal Society of Medicine, 94(7), pp. 322–330
30 NIKENDI, C. et al., 2008.
Ward rounds: how prepared are future doctors? Medical Teacher, 30(1), pp.
88-91
31 MCGLYNN, M. et al., 2012.
How we equip undergraduates with prioritisation skills using simulated
teaching scenarios. Medical Teacher, 34(7), pp. 526-529
32 MCGREGOR, C. et al., 2012.
Preparing medical students for clinical decision making: a pilot study exploring
how students make decisions and the perceived impact of a clinical decision
making teaching intervention. Medical Teacher, 34(7), pp 508-517
33 SMITH, S. et al., 2012.
A study of innovative patient safety education. Clinical Teacher, 9(1), pp. 37-
40
34 PUCHER, P. et al., 2013.
Validation of the Simulated Ward Environment for Assessment of Ward-Based
Surgical Care.
Annals of Surgery, March 6th 2013. (E-pub ahead of print)
35 SILVERMAN, J. et al., 1997.
The Calgary-Cambridge approach to communication skills teaching: The SET-
GO method of descriptive feedback.
Education for General Practice, 8: pp. 16-23
36 FRANCIS, R., 2013.
The Francis Enquiry. The Health Foundation.
http://www.health.org.uk/areas-of-work/francis-inquiry
(Accessed 12.12.13)27
37 ISSENBERG, S. et al., 2005.
Features and uses of high-fidelity medical simulations that lead to effective
learning: a BEME systematic review. Medical Teacher, 27(1), pp. 10-28.