Reproductive & DevelopmentalReproductive & Developmental Toxicology Studies 2015_Day … · ·...
78
Toxicology for Industrial and Regulatory Scientists Reproductive & Developmental Reproductive & Developmental Toxicology Studies Kok Wah Hew, Ph.D., DABT Takeda Pharmaceutical Company Deerfield, IL 60015 kok ah he @takeda com kok-wah.hew@takeda.com April 29 2015 April 29, 2015
Transcript of Reproductive & DevelopmentalReproductive & Developmental Toxicology Studies 2015_Day … · ·...

Toxicology for Industrial and Regulatory Scientists
Reproductive & DevelopmentalReproductive & Developmental Toxicology Studies
Kok Wah Hew, Ph.D., DABT, ,Takeda Pharmaceutical Company
Deerfield, IL 60015kok ah he @takeda [email protected]
April 29 2015April 29, 2015

Reproductive Toxicity Testing for Pharmaceuticals
Goals
Testing for Pharmaceuticals
Overview of reprotox study design & evaluation endpoints Allow better communication with reprotox study director Understand and interpret reprotox data Allow better communication of reprotox data to Project
Team Clinicians Regulators etcTeam, Clinicians, Regulators, etc.
Importance of nonclinical reprotox studies Difficult/unethical to perform these studies in humans
(lack of human data to assess risk to reproduction) Data will be used for risk assessment in product label Data will be used for risk assessment in product label
2

Reproductive Toxicity Testing for PharmaceuticalsTesting for Pharmaceuticals
OutlineOutline Biology/hormonal regulation of mammalian
male and female reproductive systemsmale and female reproductive systems
Mammalian reproductive cycle and development
Fertility and early embryonic development study
Embryo-fetal development studies
Pre- and postnatal development study
Juvenile animal study Juvenile animal study
3

Male Reproductive Systemp y
Rodent (Frontal View) Human (Frontal View)
4

Male Reproductive System: Testisp y
S ti f i if t b lSection of seminiferous tubule
Spermatozoa (n)
Spermatid (n)
Secondary spermatocyte (n)
Primary spermatocyte (2n)
Leydig cell
Sertoli cell
Spermatogonium (2n)Tight junction*
Sertoli cell* Forms the blood-testis barrier
5

Cycle of Seminiferous EpitheliumVI VII VIII IX X XI
Seminiferoustubule
y p
Rats ≈ 60 days
ba
b
yMen ≈ 74 days
Transit of sperm from testis to cauda epididymis
Rats ≈ 4 days
Cycle Figure from Russell et al., Histological and Histopathological Evaluation of the Testis
a
yMen ≈ 2 days
Histopathological Evaluation of the Testis, Cache River Press, Clearwater, FL, 1990, with permission.
6

Rat Testis: Cross-SectionRat Testis: Cross Section
7Roman numeral in lumen indicates stage of spermatogenesis

Hormonal Control of Testicular Functions
Hypothalamus GnRH
Inhibin Testosterone Testosterone
Pituitary
T t t
LHFSH
Leydig cellsSeminiferous
tubule
Testosterone
ABPDHT
Stimulation/secretion
Negative
Male sexual development,protein synthesis, Negative
feedback
ABP: androgen-binding protein
p y ,cell growth, etc.
DHT: dihydro-testosterone 8

Male Reproductive Systemp y Hypothalamus: receives input from the CNS and rest of the
body; secretes GnRH to stimulate the pituitarybody; secretes GnRH to stimulate the pituitary.
Pituitary: responds to GnRH by releasing LH and FSH.
Testis: responds to LH/FSH produces sperm secretes Testis: responds to LH/FSH, produces sperm, secretes Testosterone from Leydig cells
Androgen-binding protein and inhibin by Sertoli cellsd og b d g p o a d b by o
Epididymis*: a single tube that modifies sperm to confer motility and fertilizing ability.
Accessory Sex Organs (Prostate & Seminal Vesicles)*: contribute fluid that carry sperm, provide beneficial environment for sperm motility and transport.environment for sperm motility and transport.
9
* Functions regulated by testosterone and dihydro-testosterone
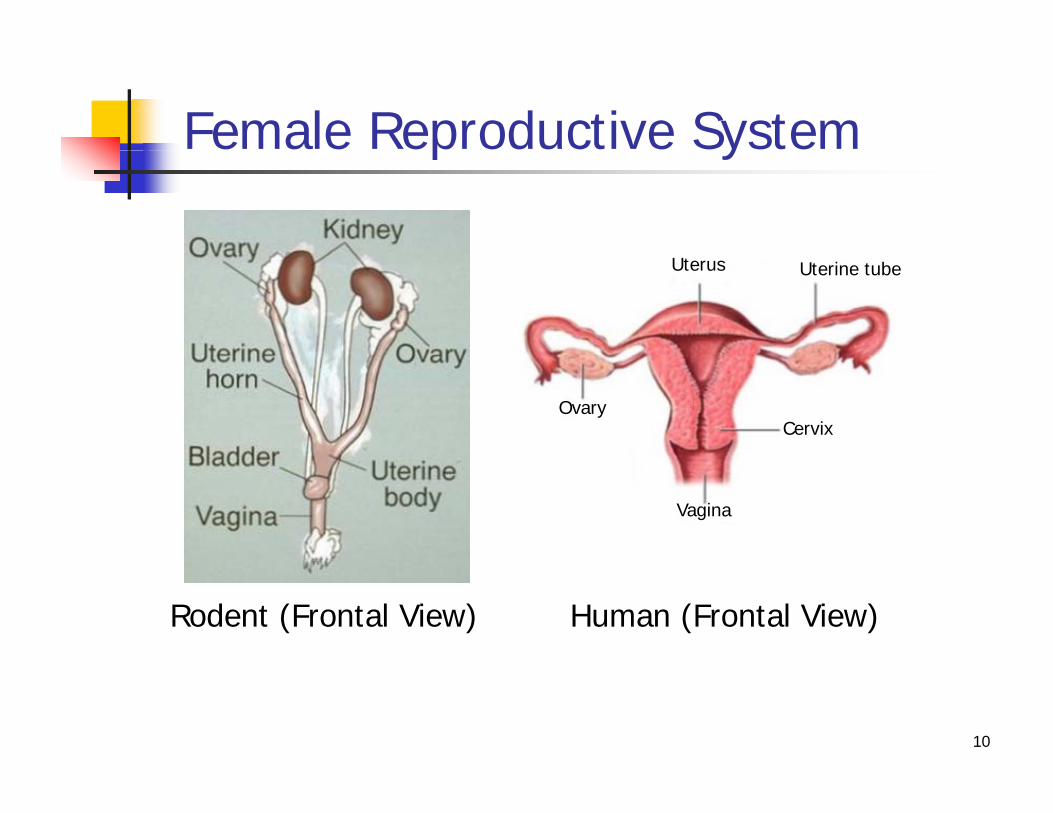
Female Reproductive Systemp y
Uterus Uterine tube
OvaryCervix
Vagina
Rodent (Frontal View) Human (Frontal View)
10

Ovulation, Fertilization, & Implantation, , p
Oocyte
Granulosa cells (stimulated by FSH,Granulosa cells (stimulated by FSH, produce & secrete estradiol)
Theca cells (stimulated by LH, participate in estradiol synthesis)
Ovarian follicle
11
participate in estradiol synthesis)

Female Reproductive System: Hormonal Control
Hypothalamus
Hormonal ControlGnRH
-/+
Uterus Uterine tube PituitaryLH
-/+
Granulosa cells
Theca cells
Ovary
yFSHLH
-/+
Vagina
OvaryCervix -/+
Oocyte
Corpus luteum Oocyte
Ovulation
Ovarian follicleStimulation/
secretion
Progesterone EstradiolOvulation
12*In rats, mice, hamster
Negative/positivefeedback-/+

Female Reproductive Systemp y
Hypothalamus: receives input from the CNS and rest of the body; secretes GnRH to stimulate the pituitary.
Pituitary: responds to GnRH by releasing LH and FSH.
Ovary: responds to LH/FSH, releasing oocytes, secretes
Estradiol from follicular cellsEstradiol from follicular cells
Progesterone and inhibin from corpus luteum
Oviduct Uterus Cervix Vagina*: Oocyte “handling” Oviduct, Uterus, Cervix, Vagina*: Oocyte handling , facilitate and enable egg and sperm transport, and maintain pregnancy.
13
* Functions of these organs regulated by estradiol and progesterone

Hormonal Changes During Human Menstrual Cycle and PregnancyMenstrual Cycle and Pregnancy
0 5 10 15 20 25 Days28/0 5 10 15 20 25
GonadotropinsLH
FSH
Ovary/FolliclesFollicular LutealPregnancy
yFollicular Luteal
ProgesteronehCG Ovarian Steroids
g
EstradiolhCG
14
P. Foster with permission hCG: human chorionic gonadotropin

Temporal Comparison of Menstrual vs. Estrous CyclesMenstrual vs. Estrous Cycles
Ovulation
Follicle
Menses
Corpus Luteum
man
Menses
Day 1 14 28
Hum
Day 1
Diestrus(48 hr)
Proestrus(18 hr)
Estrus(28 hr)
Metestrus(6 hr)t (48 hr) (18 hr) (28 hr) (6 hr)
Day 1 2 3 4
Rat
15

Reproductive Cycle & Reproductive Toxicity Studies
MatingGamete♂
p odu o y ud
Dosing period
Delivery
in uteroDevelopment
F1Maturation
F0
♂
Mating
Development
Growth/DevelopmentF1Gamete
Maturation♀ Delivery
Sexual Maturation F1
GestationSegmented approach to evaluate reproductive toxicity for pharmaceuticals
F2Seg. I
Seg. II
Fertility & early embryonic development study
Embryo-fetal development study
Seg. III Pre- & postnatal development study
16

Fertility & Early Embryonic y y yDevelopment Study
17

Fertility & Early Embryonic Development StudyDevelopment Study
Purposep To assess effects of compound on fertility and early embryonic
development when exposure occurred during gamete development, fertilization & before implantationp
Timing of study during drug development [ICH M3(R2)] Required before Phase III for subjects with reproductive capabilities Required before Phase III for subjects with reproductive capabilities Not needed for inclusion of subjects with reproductive potential in
Phase I/II if adequate microscopic exams were performed in reproductive organs in repeat-dose study of at least 2 weeks inreproductive organs in repeat-dose study of at least 2 weeks in duration
Not needed for drugs intended to treat patients with advanced cancer [ICH S9] Use general tox data to assess effects on reproductive[ICH S9]. Use general tox data to assess effects on reproductive organs
18

Fertility & Early Embryonic Development Study (Segment I)Development Study (Segment I)
MatingT t t P i dIn life
n=20/sex/group
Gamete
MaturationF1
Treatment Period
♂In-life
Termination Male: 2-10 weeks before cohabitation, during cohab. & 2-3 weeks post-mating
F l 2 k b f h bit ti
Gamete
in utero
DevelopmentF0
Female: 2 weeks before cohabitation, during cohab. & until GD 6/7 (monitor estrous cycle until successful mating)
Gamete
Maturation♀
Evaluate effects on• F0 gamete maturation• F0 mating behavior & fertilityF0 mating behavior & fertility• F1 implantation & pre-implantation embryos GD: Gestation Day
19

Reproductive Endpoints for MalesReproductive Endpoints for Males
Fertility and fecundity (ability to produce litters, b f i l t b /litt )number of implants or embryos/litter)
Mating behavior, time to mate, etc.
Organ weights (testis and accessory organs)
Sperm indicesd d d ( d ) Sperm count in testis and epididymis (sperm production)
Sperm motility (sperm function) Sperm morphology (sperm quality)p p gy ( p q y)
Histopathology (typically performed in repeat-dose study) Effects on spermatogenesis (most sensitive endpoint in male)
20

Reproductive Endpoints for Females
Successful fertilization, implantation, and gestation
Reproductive Endpoints for Females
, p , g
Estrous cyclicity (sensitive marker of hormonal changes)
Number of implants embryo/fetus numbers pregnant Number of implants, embryo/fetus, numbers pregnant per group
Organ weights and histologyg g gy
21

Fertility & Early Embryonic Development Study: Evaluation Endpoints
Estrous cyclicity
Study: Evaluation Endpoints
Precoital interval
Mating and fertility indicesg y
Cesarean section parameters
Organ weights Organ weights
Sperm parameters
Histopathology Histopathology
22
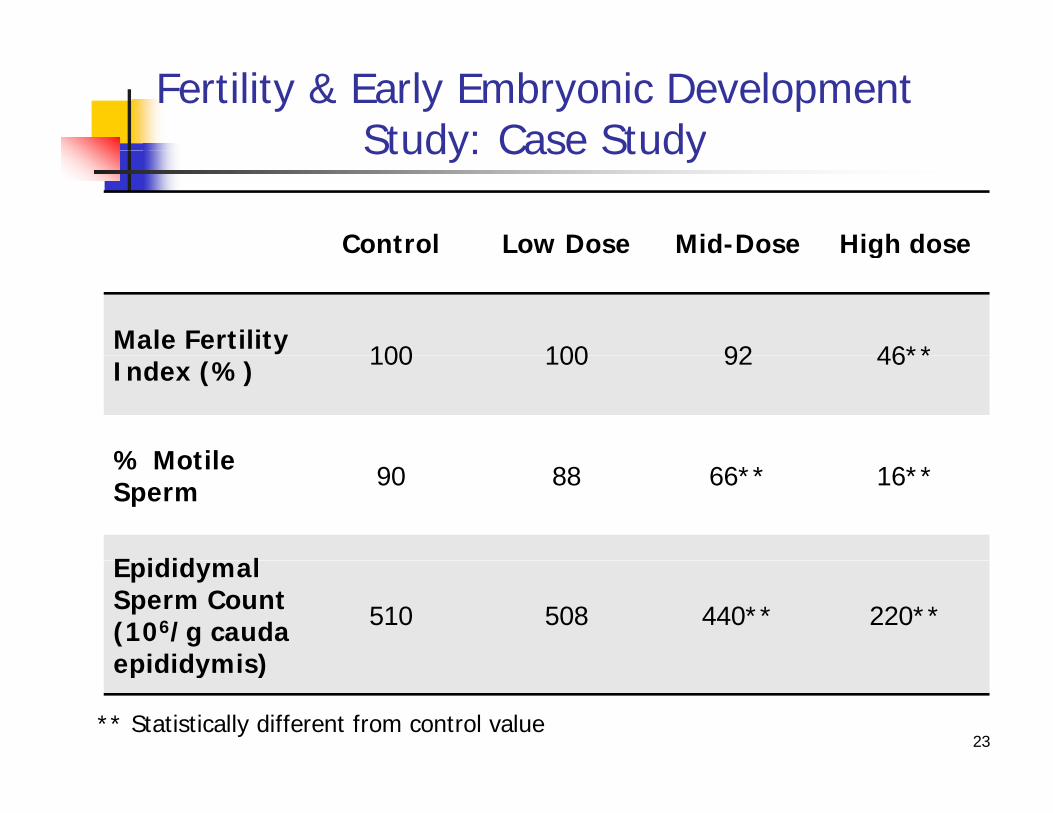
Fertility & Early Embryonic Development Study: Case StudyStudy: Case Study
Control Low Dose Mid-Dose High doseControl Low Dose Mid Dose High dose
Male Fertility 100 100 92 46**Index (%) 100 100 92 46**
% Motile% Motile Sperm 90 88 66** 16**
E idid lEpididymal Sperm Count (106/g cauda epididymis)
510 508 440** 220**
23** Statistically different from control value
epididymis)

Fertility & Early Embryonic Development Study: Case Study
Interpretation
Study: Case Study
p Male fertility affected at the high dose
Sperm parameters affected at the mid- and high doseSperm parameters affected at the mid and high dose Rodent has large sperm reserve and can tolerate some
effects on sperm without effect on fertility
Same is not true for humans
For potential risk on sperm parameters in men, needs to evaluate exposure margin between mid-dose andevaluate exposure margin between mid dose and therapeutic dose
24

Embryo-Fetal yDevelopment Study
25

Embryo-Fetal Development Studyy p y
PurposeT ff t f d b f t l d l t h To assess effects of compound on embryo-fetal development when exposure occurred in utero
Timing of study during drug development [ICH M3(R2)]Timing of study during drug development [ICH M3(R2)] Required before exposure to women of childbearing potential (WOCBP) Not needed for inclusion of WOCBP if
Short term trials (e g 2 weeks) with intensive control of pregnancy risk Short term trials (e.g., 2 weeks) with intensive control of pregnancy risk Trials must include WOCBP, but with sufficient precautions to prevent pregnancy
WOCBP (up to n=150, with adequate birth control) may be included in Phase I/II (up to 3 months) if data from preliminary embryo-fetalPhase I/II (up to 3 months) if data from preliminary embryo fetal development studies (2 species) are available
For anticancer drug [ICH S9] Not needed if genotoxic or has class effect on developmental tox If required, complete by marketing application (NDA/MAA)
26

Overview of Human DevelopmentFertilization I l t tiFertilization Implantation
Period of Organogenesis Modified from Moore 198827

Window of Sensitivity is Greatest during OrganogenesisOrganogenesis
vity Fertilization
I l t ti
High
Sens
itiv
Growth & differentiation of organs
Implantation
Organogenesisree
of S
BirthOrganogenesis
0 5 9 10 11 12 13 14 21-22
Deg
Low
Rat Gestation (Days)0 5 9 10 11 12 13 14 21 22
Period of Treatment Period for
Modified from Wilson (1973)
Period of Organogenesis
Treatment Period for Segment II Study=
28

Stages of in utero DevelopmentFertilization
ImplantationBirth
Embryonic Period Fetal Period
(Establishment of body (Growth/differentiation of
Segment II Treatment Period
(Establishment of body form, Organogenesis)
( /organ systems)* Days from fertilization
Implantation* Organogenesis Ends* Birth*
Mouse 5 15 19-20
Rat 5-6 16 21-22
Rabbit 6-7 19 30-32
Monkey 9** 44-45 166
Human 6-7 50-56 266** Dosing typically starts on GD 20 due to the need to confirm pregnancy by ultrasound on GD 18-20 29

Embryo-Fetal Development Study(Segment II or Teratology*)(Segment II or Teratology )
F0 MatingIn life
F1♂
Treatment Period
In-lifeTermination
in utero
Development* Study of Terata (Monster)
or birth defects
♀
Evaluate effects on• Viability of F1 embryos & fetuses• Growth of F1 embryos & fetusesGrowth of F1 embryos & fetuses• Structural development of F1 embryos & fetuses
30

Embryo-Fetal Developmental Study DesignEmbryo Fetal Developmental Study Design
Objective: Assess test article toxicity on maternal gestation an embryonic and fetaldevelopmentdevelopment
– Conventionally one rodent species and a non-rodent species (rabbit)– Exposure post-implantation to end of organogenesis– Endpoints: evaluate maternal toxicity, embryo/fetal death, fetal external, soft tissue and p y, y / , ,
skeletal alterations
FemaleCesareanSection +Fetal ExamsGD 0n=20/group
* *
Rat GD 6Rabbit GD 6/7
Rat GD 20-21Rabbit GD 29-30
Fetal ExamsGD 0n 20/group
Rat GD 16Rabbit GD 20
GD 0=Gestation Day 0, day when mating is confirmed
* Blood samples are typically obtained from satellite animals for toxicokinetics
Treatment Period
Range-finding study is usually performed to select doses for the definitive study:typically 4-5 dose groups + controls, n=5-6/group, limited fetal exam (external)
31

Preliminary Embryo-Fetal Developmental Study Designy y p y g
Objective: Assess drug toxicity on maternal gestation & embryonic andfetal development in order to allow inclusion of women offetal development, in order to allow inclusion of women ofchildbearing potential (up to 150, using adequate birth controlmethods) for trials of up to 3 months [ICH M3(R2)]
– One rodent species and a non-rodent species (rabbit)One rodent species and a non rodent species (rabbit)– Exposure from post-implantation to end of organogenesis– Endpoints: evaluate maternal toxicity, embryo/fetal death, fetal external
and soft tissue alterationsand soft tissue alterations
Femalen=6-8/group
CesareanSection +Fetal ExamsGD 0
Rat GD 6Rabbit GD 6/7
Rat GD 20-21Rabbit GD 29-30
Fetal ExamsGD 0
Rat GD 16Rabbit GD 20
GD 0=Gestation Day 0, day when mating is confirmed
32
Treatment Period

Endpoints in Embryo-Fetal Development StudiesEndpoints in Embryo Fetal Development Studies
Maternal endpoints Clinical signs, abortion (rabbit only) Food consumption, body weights, body weight gains
Fetal endpoints Fetal endpoints Number, sex ratio, viability, weight
External examination (all live fetuses)
Rats Half get examined for internal soft tissue structure, using conventional and
commonly-accepted dissection methodscommonly accepted dissection methods
Other half get examined for hard tissue structure (Alizarin Red staining for calcified tissue, sometimes Alcian Blue staining for cartilage)
Rabbits all animals get e amined fo soft tiss e st t es
33
Rabbits: all animals get examined for soft tissue structuresfollowed by hard tissue stains and examination
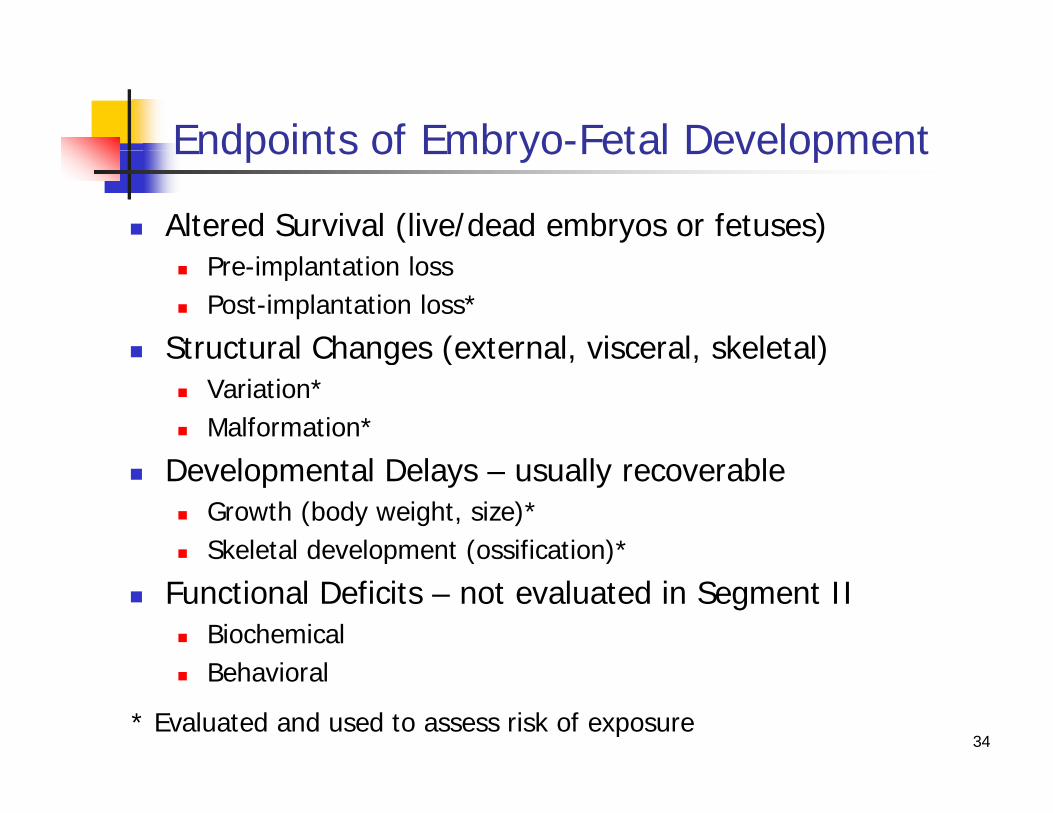
Endpoints of Embryo-Fetal DevelopmentEndpoints of Embryo Fetal Development
Altered Survival (live/dead embryos or fetuses) Pre-implantation loss Post-implantation loss*
Structural Changes (external, visceral, skeletal) Structural Changes (external, visceral, skeletal) Variation* Malformation*
D l l D l ll bl Developmental Delays – usually recoverable Growth (body weight, size)* Skeletal development (ossification)*p ( )
Functional Deficits – not evaluated in Segment II Biochemical
B h i l Behavioral
34* Evaluated and used to assess risk of exposure

Malformations and VariationsMalformations and Variations
Malformation is a permanent structural change that maystructural change that may adversely affect survival, development or function
Spina bifidaHydrocephaly Spina bifida
Variation is a divergence gbeyond the usual range of structural constitution that may not adversely
7th Cervical rib
that may not adversely affect survival or health
Incomplete centrum ossification
35

Data Interpretationp
Litter is the statistical unit
Maternal toxicity can affect fetal development (e.g., low fetal weight, supernumerary ribs)
S h bl ft bi th Some changes are recoverable after birth (e.g., wavy ribs, delayed ossification)
Read changes against concurrent controls and against the Read changes against concurrent controls and against the historical control database in the lab
To tell if something is noise or really treatment-induced Look for patterns Dose-relationship Greater number of dams affected
36
Greater number of dams affected (rather than many pups from 1 dam)

Litter Mean Calculation Litter No. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Total MeanNo.
No. affected fetuses
0 0 0 0 0 0 0 0 0 4 0 1 0 0 1 6
No fetuses/litter
7 10 8 10 7 8 8 7 9 14 4 8 4 9 8 121 5%
% affected fetuses/litter
0 0 0 0 0 0 0 0 0 28.6 0 12.5 0 0 12.5
Total no affected fetuses 6
53.6% 3.6%
Total no. affected fetuses=6Total no. fetuses evaluated=121% affected fetuses/litter=(6/121) x 100 5%*
Correct value53.6%15 3.6%
37
* Incorrect value because did not consider individual litter as an experimentalunit, i.e., each litter contains different no. of fetuses.

Integrated Approach in Data InterpretationIntegrated Approach in Data Interpretation
Spontaneous vs. treatment-related pmalformations/variations
Dose-response relationshipDose response relationship
Presence/absence of maternal toxicity
C i d Cross-species concordance
Similarities/differences in pharmacokinetics (test species vs. humans)
Exposure ratio (test species/humans)
38

Embryo-Fetal Development StudyCase Study
Control Low Dose Mid-Dose High dose
Case Study
Maternal Body Weight Normal Normal 4% less than 18% less than Body Weight Gain
Normal Normal control value control value**
Mean Fetal Weight (g) 3.5 3.8 3.4 2.9**
% Fetus With Delayed Ossification
0 0 1 5**Ossification
39** Statistically different from control value

Embryo-Fetal Development StudyCase Study
Interpretation
Case Study
Interpretation Maternal toxicity at the high dose
Fetal effects observed at the high dose Low fetal weight and delayed ossification are signs
f th t d tiof growth retardation
Fetal effects likely due to maternal toxicity (l i ht i ) t th hi h d(low weight gain) at the high dose
40

Pre- & Postnatal Development Study
41

Pre- and Postnatal Development Studyp y
Purposep To assess effects of compound on pre- and postnatal
development when exposure occurred in utero and during postnatal development (via mother’s milk)
Timing of study during drug development [ICH M3(R2)]Timing of study during drug development [ICH M3(R2)] Required for marketing approval submission (NDA/MAA)
Not needed for drugs intended to treat patients with g padvanced cancer [ICH S9]
42

Pre- & Postnatal Development Study (Segment III)(Segment III)
Treatment PeriodDeliveryF1
♂
in utero
DevelopmentM ti
F0
F1
In-life
GD 6 – LD 20 (n=20/group)
Growth/Development
Sexual Maturation
MatingF1
F1
♀Termination
Ⓐ
Evaluate effects on
Sexual Maturation F1
Gestation
Ⓐ
Ⓑ• Maternal gestation, parturition, nursing behavior & lactation • F1 viability and growth• F1 functional development & reproductive capability
F2
GD=Gestation Day, day of mating confirmation is GD 0LD=Lactation Day, day of delivery is LD 0
Ⓐ F1 GD 13Ⓑ F1 LD 4
43

Endpoints of Pre-/Postnatal Development StudyEndpoints of Pre /Postnatal Development Study
Maternal (F0) parameters( ) p
Clinical signs, food consumption, body weights, body weight gains
Gestation length
Parturition, nesting & nursing behavior
Litter size
Lactation (presence/absence of milk in the stomach of offspring)
44

Endpoints of Pre-/Postnatal Development Study
F1 Parameters
Endpoints of Pre /Postnatal Development Study
Viability (usually culled to 4/sex/litter on Lactation Day 4) Growth (body weight) Physical development Physical development
Pinna detachment Incisor eruption Eyelid opening Eyelid opening Vaginal opening Preputial separation
Reflexological & Sensory Development Reflexological & Sensory Development Righting reflex Negative geotaxis Pupillary reflex
45
Pupillary reflex Preyer reflex

Endpoints of Pre-/Postnatal Development Study
F1 Parameters (cont.)
Endpoints of Pre /Postnatal Development Study
Motor activity functions Open field test
Fi “8” Figure “8” maze
Learning and memory tests Passive avoidance Passive avoidance Water maze
Reproductive performance F1 Fertility F1 Gestation F2 viability
46
F2 viability

Data InterpretationData Interpretation
Litter is the statistical unit (where appropriate) Maternal toxicity can affect growth and development of offspring Endpoints ranked by sensitivity
Viable litter size Viable litter size Neonatal growth (body weight is the most sensitive indicator) & survival Gestation length
Landma ks of se al mat it Landmarks of sexual maturity Functional maturation, learning & memory capability
Evaluate all study data as a whole, not individual endpoints in i l tiisolation
To tell if something is noise or really treatment-related Dose-relationship
47
p Greater number of dams affected
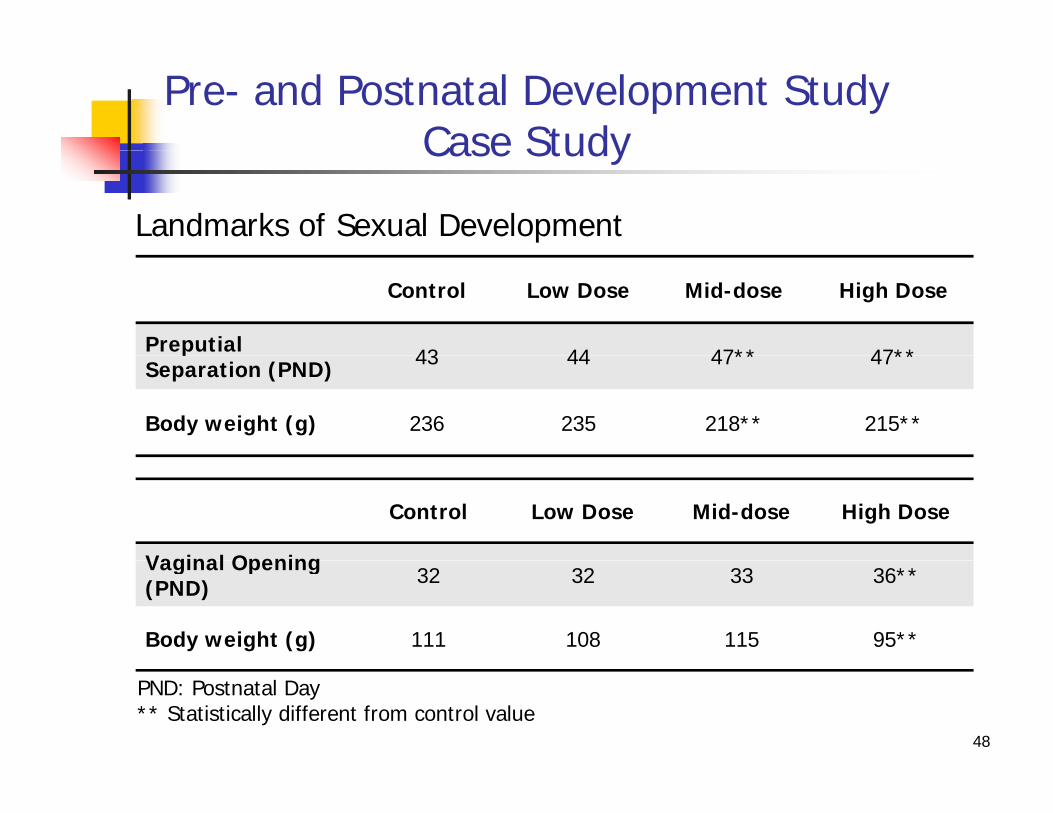
Pre- and Postnatal Development StudyCase StudyCase Study
Landmarks of Sexual Development
Control Low Dose Mid-dose High Dose
Preputial 43 44 47** 47**pSeparation (PND) 43 44 47** 47**
Body weight (g) 236 235 218** 215**
Control Low Dose Mid-dose High Dose
Vaginal OpeningVaginal Opening (PND) 32 32 33 36**
Body weight (g) 111 108 115 95**
48
PND: Postnatal Day** Statistically different from control value

Pre- and Postnatal Development StudyCase Study
Interpretation
Case Study
Interpretation Sexual maturation was delayed in males and females
Body weights in the affected groups were Body weights in the affected groups were correspondingly lower than controls
Delay in sexual maturation was due to growth Delay in sexual maturation was due to growth retardation
49

Range-finding StudyRange finding Study
Fertility & early embryonic development study Range-finding study often not necessary
Typically use data from repeat-dose studies to select doses
Embryo-fetal development studies Rat: best to do a range-finding study
Rabbit: range-finding study a must
Pre- & postnatal development study Range-finding study often not necessary
Typically use data from embryo-fetal development study to select dosesselect doses
50

Dose Selection
High dose
Dose Selection
Should produce maternal or parental toxicity
In the absence of maternal toxicity, limit dose or i f ibl d b dmaximum feasible dose may be used
Sufficient exposure should be demonstrated
In the absence of parental toxicity or sufficient exposure In the absence of parental toxicity or sufficient exposure, alternative vehicle, route, dosing regimen, or species should be considered
Low dose
Should be the No-Observed-Adverse-Effect Level (NOAEL) Exposure at multiples of clinical efficacious dose, if possible
51

Toxicokinetics in Reproductive Toxicity Studies
Generally not determined in
Reproductive Toxicity Studies
y Fertility and early embryonic development study
Pre- and postnatal development study
Embryo-fetal development studies Not a requirement but generally performed in dam/doe to
determine maternal exposure
Useful for new drug, to provide exposure margin over human exposure (assessment of human risk in drug label)exposure (assessment of human risk in drug label)
Generally not determined in fetus due to
Technical difficulties in obtaining sufficient fetal blood samples
No comparative information in humans
52

Assessment of Risk in Reproduction & Pregnancy
US Label (until June 29, 2015): 8.1 (Pregnancy), 8.3 (Nursing Mothers), 13 1 (Carcinogenesis Mutagenesis Impairment of Fertility)13.1 (Carcinogenesis, Mutagenesis, Impairment of Fertility)
Pregnancy CategoriesA: Not teratogenic in humansA: Not teratogenic in humansB: Not teratogenic in animal & no controlled human dataC: Teratogenic in animals & no controlled human dataD: Teratogenic in humans but benefit to mother may outweigh risk
to fetusX: Teratogenic in humans risk of use during pregnancy outweighsX: Teratogenic in humans, risk of use during pregnancy outweighs
any possible benefit
EU: Guideline on Risk Assessment of Medicinal Products on Human
53
EU: Guideline on Risk Assessment of Medicinal Products on Human Reproduction and Lactation: From Data to Labelling (2009)

Pregnancy & Lactation Labeling Rule (PLLR)*
8.1 Pregnancy Pregnancy exposure registryg y p g y Risk summary (required information) Clinical considerations Data
8.2 Lactation Risk summary (required information)
Cli i l id ti Clinical considerations Data
8.3 Females and males of reproductive potential Pregnancy testing Contraception Infertility
54
y* Final Rule: Content and Format of Labeling for Human Prescription Drug and Biological Products; Requirements for Pregnancy and Lactation Labeling (effective June 30, 2015)

Reproductive/Developmental p / pToxicity Studies for Chemicals
55

Reproductive/Developmental Toxicity Studies for Chemicals*
Prenatal developmental toxicity studyE f t ti d (GD) 6/7 th h d f (GD 20 i
Toxicity Studies for Chemicals
Exposure from gestation day (GD) 6/7 through end of pregnancy (GD 20 in rats and GD 28/29 in rabbits)
C-section on the day before delivery, perform fetal exams similar to Segment II studies for drugsSegment II studies for drugs
Reproduction and fertility effect study (2-generation reproduction study) Exposure 10 weeks (males/females) before cohabitation, during
cohabitation pregnancy and lactationcohabitation, pregnancy and lactation Exposure continues for selected F1 offspring that are mated and allowed to
deliver and maintain their (F2) pups to weaningAssess effects on reproductive development for 2 generations Assess effects on reproductive development for 2 generations
Developmental neurotoxicity study Exposure from GD 6 to postnatal day 10 or 21 Evaluate developing nervous system
56* See guidelines listed in Slide No. 75.

Juvenile Animal Studyy
57

Juvenile Animal Studyy
Purposep To assess effects of compound on postnatal growth
and development when (direct) exposure occurred from neonatal to pre-adult period
Timing of study during drug development [ICH M3(R2)]Timing of study during drug development [ICH M3(R2)] Prior to long-term pediatric study Generally not needed to support short-term pharmaco-y pp p
kinetic studies in pediatric population (e.g., 1 to 3 doses)
58

Different Age Groups in Pediatric Population & Juvenile AnimalsPopulation & Juvenile Animals
Human Rat Dog Cynomolgus Monkeyg Monkey
Neonate Birth – 1 month Birth – PND 7 Birth – 3 weeks Birth – 4 months
Infant 1 – 24 months PND 7 – 21 3 – 6 weeks 4 – 6 months
Child 2 – 12 years PND 21 – 35 6 – 20 weeks 6 – 36 months
Adolescent 12 – 16 years PND 35 – 60 5 – 8 months 3 – 5 years
PND=Postnatal Day
Pediatric population has different subgroups each showing a
Adolescent 12 – 16 years PND 35 – 60 5 – 8 months 3 – 5 years
59
Pediatric population has different subgroups, each showing a different stage/rate of growth and organ/system maturation

Physiology/Pharmacokinetics in Neonate/Infant Compared to AdultNeonate/Infant Compared to Adult
Neonate/Infant
GI Motility/pH Lower GI motility ( GI absorption), higher pH ( absorption of basic molecule, absorption of acidic molecule)
P t i Bi di T i ll l f dProtein Binding Typically lower, more free compound
Total Water Content Higher, affects volume of distribution
Metabolism Enzymes not fully developed, affecting pharmacokinetics
Biliary Excretion Lower, may half-life
60
Glomerular Filtration Lower, may half-life

Organ/System Maturation Period in Human
Urinary System
g / yGI: Gastrointestinal
Dosing period in juvenile animal study ill be dete mined b ta get o gans
Pulmonary/GI Systems
ywill be determined by target organs that are undergoing development
during clinical exposure
Cardiovascular/Immune Systems
Central Nervous/Reproductive Systems
Biotransformation Enzymes
Skeletal System
Central Nervous/Reproductive Systems
61Birth 2 years 12 years 16 years
y

Non-Clinical Studies Performed to Support Pediatric Use
Animals should beAnimals should be treated throughout the stages of development that are comparable to pthe timing of exposure in the intended pediatric population
62

Adult vs. Juvenile Animal Study
Evaluate drug’s effect on developmental stage
y
and effect of developmental stage on drug
Repeat-Dose Studies J il A i l St diRepeat Dose Studies in Adult Animals Juvenile Animal Studies
A 1 t D Y d l Varies, depending onAge at 1st Dose Young adult Varies, depending on pediatric regimen
Typically standard e g Varies depending onDosing Period Typically standard, e.g.,4-, 13-week
Varies, depending on pediatric regimen
Study
63
Study Endpoints Typically standard Study-specific

Factors InfluencingJuvenile Animal Study Design
Pediatric indication
Juvenile Animal Study Design
Pediatric population Age range
D ti f Duration of exposure
Toxicity of drug in adult human/animal
Wh th t t id tifi d i d lt d Whether target organs identified in adults undergo significant postnatal development
Differences in pharmacology pharmacokinetics and Differences in pharmacology, pharmacokinetics, and toxicity profiles between adult and pediatric population
64

Juvenile Animal Study Design (1)
Step-wise Approach in Designing Juvenile Animal Study
y g ( )
1. Determine dosing regimen in pediatric population Dosing begins from age X Dosing extends from age X to YDosing extends from age X to Y
2. Identify appropriate Species Target organs (observed in adult humans and animals) Developing organs/systems in humans at age X to Y, and corresponding
developing intervals for these and target organs in test species
3. Determine age at 1st dose and dosing period based on #1 and #2
4. Study should include evaluation of effects onO / t i #2 Organs/systems in #2
Growth, functional & structural development, as appropriate65

Juvenile Animal Study Design (2)
Step-wise Approach in Designing Juvenile Animal Study
y g ( )
5. Dose route Intended route of clinical exposure, as appropriate Use labs whose technicians are competent in dosing young pupsUse labs whose technicians are competent in dosing young pups
6. Essential to perform pilot/range-finding study
7. Study should includey Toxicokinetic evaluation Recovery assessment
B th t d d i i ll li t d i lBecause the study design is usually complicated, uses many animals, takes a long time to complete and expensive, important to design the study appropriately
Where possible, get concurrence on study design from regulatory agencies
66

SummarySummary
Important to understand biology/timing of development
Embryo/fetus depends on dams for growth & development
Important to distinguish between direct fetal toxicity & fetal changes due to maternal toxicity
Litter is the unit for evaluation/comparison
U i t t d h t l t d ti t i it Use integrated approach to evaluate reproductive toxicity
Fetal/pup weight is the most sensitive indicator for growth & development& development
For juvenile animal studies Need to know the age range and duration of exposure, target organs, g g p , g g ,
timing of organ/system development in animals vs. humans
67

ICI 204,636: Segment I Studies in Alpk:ApfSK (Wistar-derived) Rats
Male Fertility StudyTreatment Period
GD: Gestation Day11 weeksMating*
♂C-section on GD 21 to
perform uterine/fetal exam
F1 in uteroDevelopment
F0
♀ e e op e♀
* Control and high-dose males mated twice, (1) after 11 weeks of dosing [for up to 3 weeks], (2) 2 weeks after the end of dosing (at the end of 1st mating period)Lo nd mid do e m le ifi ed t Week 17 18 high do e m le ifi ed t
68
Low and mid-dose males sacrificed at Week 17-18, high-dose males sacrificed at the end of 2nd pairing

ICI 204,636: Segment I Studies in Alpk:ApfSK (Wistar-derived) Rats
Treatment PeriodFemale Fertility StudyGD: Gestation DayLD: Lactation Day
Mating
y y
C-section on GD 21 to perform uterine/fetal exam
F1 i t
F0
♂ Dosing completed
LD 22-24 F1 males sacrificed at th d f tiF1 in utero
Development♀2 weeks
the end of mating
F1 growth/development
F1 females sacrificed
69
on GD 21 or LD 22-24

ICI 204,636: Embryo-Fetal Development Studies
F0 Mating
Treatment Period
Alpk ApfSK rats GD 6 15F0 Mating
F1
♂In-life
Termination
Alpk:ApfSK rats: GD 6-15
Dutch Belted rabbits: GD 6-18
GD: Gestation Day
in utero
Development
F1 GD: Gestation Day
♀
70
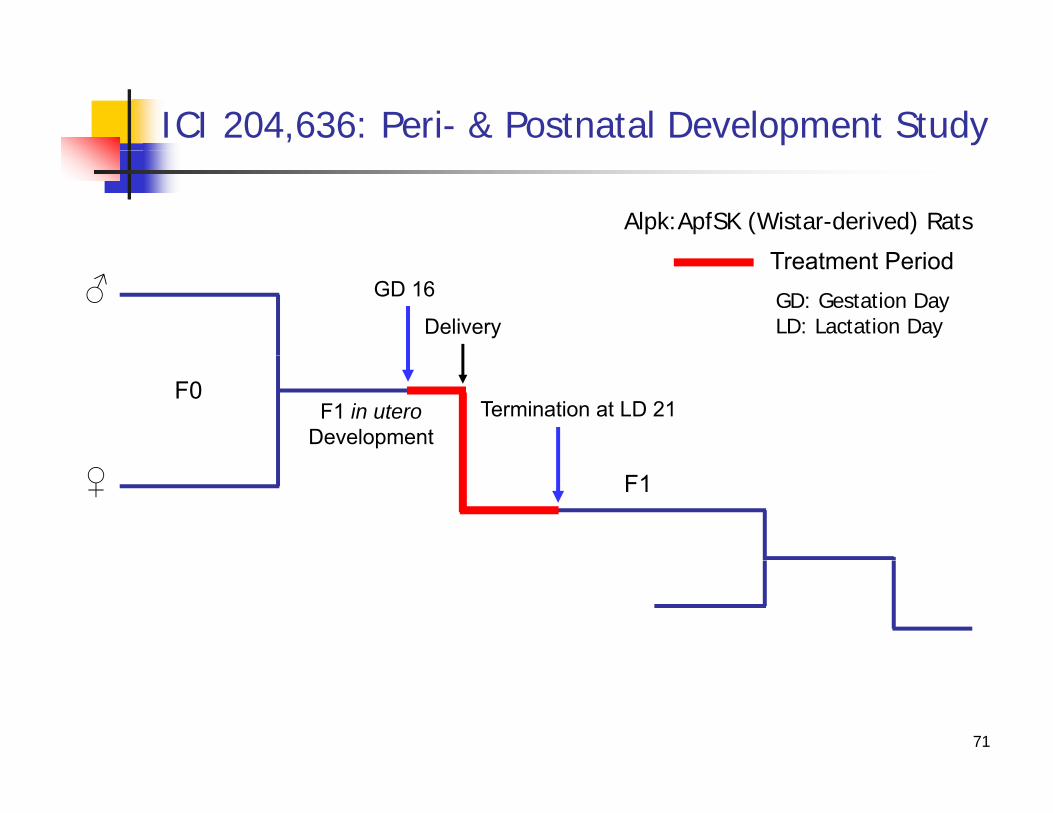
ICI 204,636: Peri- & Postnatal Development Study
T t t P i d
Alpk:ApfSK (Wistar-derived) Rats
Treatment Period
Delivery♂ GD: Gestation Day
LD: Lactation Day
GD 16
F1 in uteroDevelopment
F0Termination at LD 21
F1♀
71

AbbreviationsAbbreviations
ABP Androgen-binding protein CNS Central nervous system DHT Dihydro-testosterone FSH Follicle-stimulating hormoneg GD Gestation day GnRH Gonadotropin-releasing hormone LD Lactation day LD Lactation day LH Luteinizing hormone MAA Marketing Authorisation Application
NDA New Drug Application NDA New Drug Application NHP Nonhuman primate PND Postnatal day WOCBP Women of childbearing potential
72

References (1)
1. ICH M3(R2) Nonclinical Safety Studies for the Conduct of Human Clinical Trials and Marketing Authorization for Pharmaceuticals (June 2009).
2. ICH S5(R2): Detection of Toxicity to Reproduction for Medicinal Products & Toxicity to Male Fertility (Nov. 2005).
3. ICH S6(R1): Addendum to ICH S6: Preclinical Safety Evaluation of Biotechnology-derived Pharmaceuticals (Draft Guidance, Oct. 2009).
4. ICH S9:Nonclinical Evaluation for Anticancer Pharmaceuticals (March 2010).5. FDA Guidance for Industry: Nonclinical Safety Evaluation of Pediatric Drug Products (Feb. 2006).6. CHMP Guideline on Risk Assessment of Medicinal Products on Human Reproduction and Lactation:
From Data to Labelling (Jan. 2009).7. CHMP Guideline on the Need for Non-Clinical Testing in Juvenile Animals on Pharmaceuticals for
Paediatric Indications (Aug. 2008).8. PMDA Guideline on the Non-clinical Safety Study in Juvenile Animals for Pediatric Drugs (Oct.
2012).9. Lerman SA, Hew KW, Stewart J, Stump DG, Wise LD. 2009. The nonclinical fertility study design
for pharmaceuticals. Birth Defects Research Part B: Developmental and Reproductive Toxicology86(6):429-436.
10. Wise LD, Buschmann J, Feuston MH, Fisher JE, Hew KW, Hoberman AM, Lerman SA, Ooshima Y, St DG 2009 E b f t l d l t l t i it t d d i f h ti l Bi th
73
Stump DG. 2009. Embryo-fetal developmental toxicity study design for pharmaceuticals. Birth Defects Research Part B: Developmental and Reproductive Toxicology 86(6):418-428.

References (2)
11. Bailey GP, Wise LD, Buschmann J, Hurtt M, Fisher JE. 2009. Pre- and postnatal developmental toxicity study design for pharmaceuticals. Birth Defects Research Part B: Developmental and Reproductive Toxicology 86(6):437-445.
12. Chellman GJ, Bussiere JL, Makori N, Martin PL, Ooshima Y, Weinbauer GF. 2009. Developmental and reproductive toxicology studies in nonhuman primates. Birth Defects Research Part B: Developmental and Reproductive Toxicology 86(6):446-462.
13 C GD B il GP B h J F t MH Fi h JE H KW H b AM O hi13. Cappon GD, Bailey GP, Buschmann J, Feuston MH, Fisher JE, Hew KW, Hoberman AM, Ooshima Y, Stump DG, Hurtt ME. 2009. Juvenile animal toxicity study designs to support pediatric drug development. Birth Defects Research Part B: Developmental and Reproductive Toxicology86(6):463-469.
14. Martin PL. 2008. Reproductive toxicity testing for biopharmaceuticals. In: J.A. Cavagnaro (Ed.), p y g p g ( ),Preclinical Safety Evaluation of Biopharmaceuticals. John Wiley & Sons, Inc., Hoboken, NJ, pp. 357-377.
15. Morford LL, Bowman CJ, Blanset DL, Bøgh IB, Chellman GJ, Halpern WG, Weinbauer GF, Coogan TP. 2011. Preclinical safety evaluations supporting pediatric drug development with biopharmaceuticals: strategy challenges current practices Birth Defects Research Part B:biopharmaceuticals: strategy, challenges, current practices. Birth Defects Research Part B: Developmental and Reproductive Toxicology 92:359-380.
16. Developmental and Reproductive Toxicology, 3nd Edition (R.D. Hood, Ed.) Informa Healthcare, London, 2012.
17. Teratogenicity Testing: Methods and Protocols (P.C. Barrow, Ed.) Humana Press, New York,
74
17. Teratogenicity Testing: Methods and Protocols (P.C. Barrow, Ed.) Humana Press, New York, 2013.
18. Link to ICH Safety Guidelines: http://www.ich.org/products/guidelines/safety/article/safety-guidelines.html

Reproductive Toxicity Testing Guidelines for Chemicals
United States Environmental Protection Agency (US EPA) Health Effects Test Guidelines OPPTS 870.3700, Prenatal Developmental Toxicity Study, August 1998. [OECD Guideline
Guidelines for Chemicals
, p y y, g [414, January 2001]
US EPA Health Effects Test Guidelines OPPTS 870.3800, Reproduction and Fertility Effects, August 1998. [Two-Generation Reproduction Toxicity Study OECD Guideline 416, January 2001]2001]
US EPA Health Effects Test Guidelines OPPTS 870.6300, Developmental Neurotoxicity Study, August 1998. [OECD Guideline 426, October 2007]
Organisation for Economic Cooperation and Development (OECD) Guideline for Testing of Chemicals: 415, One-Generation Reproduction Toxicity Study, May 1983.
OECD Guideline for the Testing of Chemicals, 443, Extended One-Generation Reproductive Toxicity Study July 2012Toxicity Study, July 2012.
OECD Guideline for Testing of Chemicals: 421, Reproduction/Developmental Toxicity Screening Test, July 1995. [EPA OPPTS 870.3550, July 2000]
O C G id li f i f Ch i l 22 C bi d d i i S d OECD Guideline for Testing of Chemicals: 422, Combined Repeated Dose Toxicity Study with the Reproduction/Developmental Toxicity Screening Test, March 1996. [EPA OPPTS 870.3650, July 2000]
75

Glossary of Reproductive Indices/Terms (1)Glossary of Reproductive Indices/Terms (1)
Precoital Intervals (Days) = Number of days to mate successfully
Male Mating Index (%) = Number of ♂ with evidence of mating
Total number of ♂ used for matingX100
Male Fertility Index (%) = Number of ♂ siring at least 1 litter
Total number of ♂ with evidence of matingX100
Female Mating Index (%) = Number of ♀ with evidence of mating
Total number of ♀ used for matingX100
Female Fertility Index (%) = Number of ♀ with confirmed pregnancy
Total number of ♀ with evidence of matingX100
76
Gestation Index (%) = Number of ♀ with live pup
Number of ♀ with evidence of pregnancyX100

Glossary of Reproductive Indices/Terms (2)Glossary of Reproductive Indices/Terms (2)
Pre-implantation Loss (%) =Number of corpora lutea – Number of implants
X100Pre implantation Loss (%) = Total number of corpora lutea
X100
P i l i L (%)Number of implants – Number of viable embryos
X100
Number of pups born alive
Post-implantation Loss (%) = p y
Total number of implantsX100
Live Birth Index (%) = Number of pups born alive
Total number of pups bornX100
Number of live pups (at a given time point)Survival Index (%) =
Number of live pups (at a given time point)
Total number of pups bornX100
Number of pups with evidence of milk in stomach
77
Lactation Index (%) = Number of pups with evidence of milk in stomach
Total number of pups bornX100

Please click on the link below to enter your comments on the talkenter your comments on the talk
https://www.surveymonkey.com/s/VNHVGKT
78








![Developmental Toxicology, Third Edition[1]](https://static.fdocuments.in/doc/165x107/547f7ec2b379594e2b8b5882/developmental-toxicology-third-edition1.jpg)