Report of an inspection of a Designated Centre for Older ... mature garden with walkways, garden...
32
Page 1 of 32 Report of an inspection of a Designated Centre for Older People Issued by the Chief Inspector Name of designated centre: Strathmore Lodge Nursing Home Name of provider: Hasta Healthcare Limited Address of centre: Friary Walk, Callan, Kilkenny Type of inspection: Unannounced Date of inspection: 12 September 2019 Centre ID: OSV-0004449 Fieldwork ID: MON-0027664
Transcript of Report of an inspection of a Designated Centre for Older ... mature garden with walkways, garden...

Page 1 of 32
Report of an inspection of a Designated Centre for Older People Issued by the Chief Inspector Name of designated centre:
Strathmore Lodge Nursing Home
Name of provider: Hasta Healthcare Limited
Address of centre: Friary Walk, Callan, Kilkenny
Type of inspection: Unannounced
Date of inspection:
12 September 2019
Centre ID: OSV-0004449
Fieldwork ID: MON-0027664

Page 2 of 32
About the designated centre
The following information has been submitted by the registered provider and describes the service they provide. Strathmore Lodge Nursing Home is located within the urban setting of Callan, Co. Kilkenny. It is registered for 60 residents. It is a two-storey facility with lifts and stairs access on either side of the centre to enable easy access. All bedroom accommodation comprises single rooms with en-suite facilities of assisted shower, toilet and handwash sink. There are day rooms, dining rooms and activity rooms on both floors as well as seating areas throughout. Residents have access to a secure mature garden with walkways, garden furniture and raised flower beds. Strathmore Lodge Nursing Home provides 24-hour nursing care to both male and female residents. It can accommodate older people with a range of diagnoses and younger people whose assessed needs can be met by the centre. Long-term care, convalescence care, respite and palliative care is provided and low to maximum dependency residents can be cared for in Strathmore Lodge. The following information outlines some additional data on this centre.
Number of residents on the
date of inspection:
53

Page 3 of 32
How we inspect
This inspection was carried out to assess compliance with the Health Act 2007 (as amended), the Health Act 2007 (Care and Welfare of Residents in Designated Centres for Older People) Regulations 2013 (as amended), and the Health Act 2007 (Registration of Designated Centres for Older People) Regulations 2015 (as amended). To prepare for this inspection the inspector of social services (hereafter referred to as inspectors) reviewed all information about this centre. This included any previous inspection findings, registration information, information submitted by the provider or person in charge and other unsolicited information since the last inspection.
As part of our inspection, where possible, we:
speak with residents and the people who visit them to find out their
experience of the service,
talk with staff and management to find out how they plan, deliver and monitor
the care and support services that are provided to people who live in the
centre,
observe practice and daily life to see if it reflects what people tell us,
review documents to see if appropriate records are kept and that they reflect
practice and what people tell us.
In order to summarise our inspection findings and to describe how well a service is
doing, we group and report on the regulations under two dimensions of:
1. Capacity and capability of the service:
This section describes the leadership and management of the centre and how
effective it is in ensuring that a good quality and safe service is being provided. It
outlines how people who work in the centre are recruited and trained and whether
there are appropriate systems and processes in place to underpin the safe delivery
and oversight of the service.
2. Quality and safety of the service:
This section describes the care and support people receive and if it was of a good
quality and ensured people were safe. It includes information about the care and
supports available for people and the environment in which they live.
A full list of all regulations and the dimension they are reported under can be seen in
Appendix 1.

Page 4 of 32
This inspection was carried out during the following times:
Date Times of
Inspection
Inspector Role
12 September 2019 12:00hrs to 21:00hrs
Leanne Crowe Lead
12 September 2019 12:00hrs to 21:00hrs
Mary O'Donnell Support
Page 5 of 32
What residents told us and what inspectors observed
Residents told inspectors they were happy and very well cared for in the centre. Some residents who could not express their own opinions were represented by family members.
The staff were highly complimented by residents and family members. They liked the fact that staff were local and described staff as approachable, caring and responsive to residents' needs. Many of the residents and relatives who met inspectors commented on how busy staff were but they always try to get to you. Residents and relatives were very pleased with the improvements made to the secure garden. They had been involved in selecting the colours and painting the garden furniture. They were also involved in decorating the centre's chicken coop which was home to four hens. These hens had been hatched in an incubator in the centre. One resident told inspectors that it was very important to have hens as many of the residents were from farming backgrounds.
Social aspects of life in the centre were complimented, with residents enjoying a variety of activities. Music, arts and crafts and outside activities were particularly popular. Residents had access to raised beds for planting and they were working on tomato plants when inspectors arrived. The garden was now designed to meet residents’ needs with lawns, flower containers, a bird feeding station and a gazebo to enable residents to spend time outdoor whatever the weather. Relatives were less complimentary about the interior and described the premises as clinical rather than homely. Residents and relatives commented that they sometimes got unpleasant odours from laundry skips, which were stored in the corridor. Relatives were pleased to see that a television was installed in the lounge on the ground floor on the day of inspection. They hoped that this would encourage residents to stay up later and socialise together in the evenings instead of going to their rooms to watch television or retiring to bed early. Some visitors wondered if there was a lack of staff to supervise residents in the lounge in the evening, stating that residents who hadn’t gone to bed were seated at the nurses’ station on both floors each evening. A relative commented that ‘it is like everything shuts down here after 6:30 in the evening and there is nothing homely about that”.
Residents were satisfied with the menu options. They knew the chef and they confirmed that their personal food preferences were respected. One resident said he was provided with fish for supper often because the chef knows he loves fish. Some residents were pleased that buffet breakfast had been introduced and said they wouldn’t miss it. They said they can get up and go to bed when they like and one resident who requires assistance of two said she was afraid to stay up until night staff came on duty because they may leave her until last.
Residents were satisfied with the laundry service and that their laundry was marked and returned safely to them. Residents and relatives were satisfied that single ensuite rooms were provided but some relatives were not satisfied with the standard

Page 6 of 32
of cleanliness in the bed rooms. When asked if issues of concern had been raised with management, residents said they would tell one of the staff and things were usually sorted. While some relatives said that any complaints were dealt with quickly, others said they were reluctant to complain.
Capacity and capability
This was an unannounced inspection triggered following the receipt of information which raised concerns about staffing, staff training and development, infection control, medication management, and management of the designated centre. None of the concerns raised were substantiated. Inspectors also followed up on solicited information, such as notifications, submitted by the registered provider and person in charge since a previous inspection in May 2018, as well as the actions in place to address issues identified on that inspection. The findings of this inspection were that the registered provider had not ensured that there were appropriate systems and processes in place to underpin the safe delivery and oversight of the service.
Since February 2019, there has been three changes to the person in charge, with the most recent appointment in July 2019. This person was on planned leave at the time of this unannounced inspection. Inspectors found that while there was a clearly defined management structure in place between the person in charge and registered provider, there were insufficient resources to provide a quality service and sufficient oversight of the service was not being maintained. For example, there had been significant staff turnover since the beginning of 2019. While management had made efforts to recruit staff for any vacancies, some gaps remained at the time of the inspection. Inspectors found that regular meetings were taking place between key members of the management team and records of these were available for review. Regular reports in relation to key performance indicators were discussed at these meetings. However, from audit reports and fire safety matters identified during inspection, the inspectors were not assured that appropriate management systems were in place to ensure that the service provided on an ongoing basis was safe and effectively monitored by the provider. For example, there was no documented process for identifying and mitigating risks including fire safety risks in the centre. Observed risks had not being identified, documented or mitigated by the provider:
The fire safety risks associated with the decision not to fit automatic door closers had not been reviewed.
Some audits completed within the centre were found to be of poor quality, and others that conveyed poor findings had not been actioned as required.
While the registered provider had proactively contracted a private fire safety consultant to carry out an inspection of the centre, the corresponding report had not been distributed to relevant staff in order to develop an action plan.

Page 7 of 32
Regulation 15: Staffing
Inspectors were not assured that there were sufficient staff to meet the needs of residents, particularly on night duty. Household staff hours required review. While there had been a high level of staff turnover between January and September, efforts had been made to recruit the staff required to fill these vacancies. At the time of the inspection, three vacancies were yet to be filled. In the interim, the centre's own staff were being used to replace planned and unplanned leave, which effectively eliminated the reliance on agency staff.
Inspectors observed staff attending to residents' needs in person-centred manner throughout the inspection. However, inspectors also noted some delays in answering call bells or responding to requests from residents, as well as sometimes failing to supervise residents gathered in communal areas. This indicated that improvement was needed in relation to staffing levels or the allocation of staff.
Staff files contained the information required by the regulations, but there was no evidence that references were verified by management. All staff had An Garda Síochana vetting in place prior to commencing their respective posts.
Judgment: Substantially compliant
Regulation 16: Training and staff development
Significant improvement was required to ensure staff were adequately trained, this had also been identified in the previous inspection. For example, records indicated that some staff did not have up to date training in areas such as fire safety, moving and handling practices and the prevention, detection and response to abuse. The quality of training provided to household was inadequate for them to competently perform their duties. In addition three housekeeping staff did not have training in infection control. Staff had availed of other training relevant to their role, such as dementia care, medication management and restrictive practice. The training programme for health care assistants would benefit from the inclusion of training to support staff to assist residents with swallowing problems to eat and drink. Inspectors observed unsafe practices when a resident was assisted to drink.
There was evidence that staff were supervised by the nursing management team.
Annual appraisals took place with all staff. These included a self-evaluation followed by a review with a senior member of staff.
Judgment: Not compliant

Page 8 of 32
Regulation 23: Governance and management
There was a clearly defined management structure in place in the centre. The management structure had undergone significant changes in the current registration cycle. There was a change of company directors in February 2018. Recently the nominated provider representative had changed and the centre had three changes of person in charge in 2019. Staff turnover was also noted to be high during this period. On the day of inspection a clinical nurse manager was deputising for the person in charge, who was on leave. A former person in charge and a clinical director came on site to support the inspection.
Management meetings occurred in the centre and it was clear that key performance indicators were reviewed at these meetings. However, minutes of these meetings did not demonstrate a consistent approach to reviewing the service.
The management systems to monitor the quality and safety of the service were ineffective. The new person in charge was in the process of revising the auditing programme since their appointment to the role in July 2019. However, there was evidence that the annual schedule of audits had not been implemented. Some of the scheduled audits including infection control audits were not carried out and the audits which had been completed were of poor quality. For example, the call bell audits only covered time periods before 13:00 hrs and no other time frames were audited. The manual handling audits consisted of an observation of one resident being transferred. There was little evidence that the information collated from audits was analysed to inform continuous quality improvements in the service.
Improvements had been made since the previous inspection in May 2018. For example, staff files showed that all staff were Garda Vetted prior to taking up employment. Additionally, the external garden area had been upgraded to a high standard. However, other non-compliances observed in the centre on the last inspection had not been adequately addressed. And some of the improvements that had been made had not been sustained.
The centre required further resources in relation to the following areas:
Staffing Further enhancement of the internal premises to create a more homely
environment for residents
Infection control Fire safety issues.
This will be outlined further under Regulations 15, 17, 27 and 28.
Judgment: Not compliant

Page 9 of 32
Regulation 24: Contract for the provision of services
A sample of contracts were reviewed. These had been signed by the resident and/or their next of kin. The contract also outlined the fees to be charged to residents, although clarification was required regarding the fees charged for newspapers.
Judgment: Compliant
Regulation 3: Statement of purpose
The statement of purpose had been revised to reflect the changes to management including the name of the new provider and person in charge. The provider was required to review the whole time equivalent staffing section to ensure it reflected current staffing levels on the rosters. Some sections required further information such as:
The deputising arrangements in the absence of the person in charge
The list of allied health services which were available to residents More detailed descriptions of the en suites facilities.
Judgment: Substantially compliant
Regulation 31: Notification of incidents
Inspectors reviewed the accident and incident book and found that all incidents were reported as required.
Judgment: Compliant
Regulation 34: Complaints procedure
The complaints procedure was displayed prominently in the centre. There was a nominated person who dealt with complaints. The complaints records viewed by inspectors included information about the nature of the complaint, investigation of the complaint and action plans to address the complaint. The level of satisfaction of the complainant was also documented.
Judgment: Compliant

Page 10 of 32
Quality and safety
Overall, the inspection findings showed that the residential centre was providing good quality care and support. However, systems to monitor risk and the safety of residents required significant improvement.
The premises had a good building layout with single occupancy ensuite bedrooms on two floors, but building compartments were large and bedroom doors did not have automatic closure devices. Significant fire safety issues were identified and the provider was requested to put urgent safety measures in place to ensure the safe evacuation of residents in an emergency. Overall risk management procedures were not in line with the centre’s policies and required review.
Inspectors were satisfied that residents’ health care needs were met to a good standard. There were effective systems in place for the assessment and planning of care, but systems to ensure that care plans were implemented and appropriately reviewed required strengthening.
Residents were screened for nutritional risk on admission and reviewed regularly thereafter. Where nutritional risks were identified, referrals had been made to dietetic and/or speech and language services. While acknowledging that many residents had a pleasant mealtime experience, further improvements are required to improve the social aspect of mealtimes for residents on the first floor who required assistance with eating and drinking.
There was opportunity for improvement in relation to the assessment and supports for residents with responsive behaviours (how people with dementia or other conditions may communicate or express their physical discomfort, or discomfort with their social or physical environment). While the use of restraint was low, the use of restrictive practices as a last resort was not consistently demonstrated in line with national policy.
Residents were safeguarded against abuse or harm by the systems in place in the centre. However, it was noted that approximately 12 staff required training in this regard in order to sustain effective procedures.
The premises provided residents with a comfortable and accessible environment. The centre was visibly clean on the day of inspection but daily cleaning routines and arrangements for deep cleaning required review. The premises was maintained and decorated to a high standard but the overall ambiance was clinical, especially in the sitting rooms. There was opportunity for improvement to create a more homely, interesting environment for residents, especially those with dementia.

Page 11 of 32
Regulation 12: Personal possessions
Residents had adequate space to store their clothes and display their personal possessions in their bedrooms. Inspectors noted that items of clothing were marked, laundered and returned to their bedrooms.
Judgment: Compliant
Regulation 17: Premises
The majority of actions from the previous inspection had been completed, with the exception of the restriction of access to sluice rooms. Inspectors identified additional improvements that were required. The premises is well laid out over two floors. It has a variety of communal spaces and bedrooms were single with ensuite facilities which included a shower, toilet and wash hand basin. Residents were supported to personalise their bedrooms with personal items and photographs. Building compartments were found to be large; this and other fire safety issues are discussed under regulation 28.
Action had been taken to ensure that the sluice door was secure and the sluice room could not be accessed by residents on the first floor. However, inspectors found that the door to the sluice room on the ground floor could easily be pushed open. Inspectors saw that suitable racking had been installed in sluice rooms for the storage of sanitary equipment. Storage space for equipment was limited. Inspectors observed that laundry skips were stored in an alcove along the corridor and equipment such as hoists, a wheelchair, a commode and portable radiators were stored in the ground floor bathroom. Household staff had a room to store cleaning equipment but it was not plumbed and staff used the sluice room to fill and empty their mop buckets. This posed a potential risk of cross infection for residents.
The centre was nicely decorated and well maintained. A room on the first floor had been freshly painted and plans were in place to create an activity room there. Bedrooms were spacious and many were decorated in a homely manner. Not all bedrooms had a lockable space for their belongings. Some of the chairs in the lounge downstairs were stained. Residents had a choice of communal rooms on both floors but residents did not use these rooms very often during the day. Instead they congregated in the ground floor sitting room and around the nurses' stations on both floors. It was noted that the ground floor sitting room was not large enough to accommodate all of the residents who were attending activities there, with some residents instead sitting in the reception area. Therefore there was opportunity to improve the other communal rooms and create a more homely, interesting environment for residents to enjoy spending time in.
The provider had completed the action plan to move towards compliance following the previous inspection. Floor plans with fire compartments were displayed
Page 12 of 32
throughout the centre and the CCTV cameras had been deactivated in the day room. Inspectors saw that the garden was well maintained with suitable pathways and a patio for residents to enjoy. Garden furniture had been repaired and painted in cheerful colours. Containers had been planted to provide colourful blooms for summer. A bird feeding station and a hen run had been erected so that residents would benefit from being in contact with nature. Residents and relatives were complimentary about the works completed and they told inspectors how much they enjoyed spending time in the garden.
Handrails were in place in corridors to support residents' safe movement throughout the centre.
Artwork created by residents was displayed in the reception area, and photos of some activities or special occasions were hanging throughout the centre.
Judgment: Not compliant
Regulation 18: Food and nutrition
There were systems in place to communicate each resident's food preferences and specialist dietary needs to catering staff, to ensure that each resident's dietary needs were met. The menus had been evaluated by a dietitian to ensure that meals were wholesome and nutritious. Residents had access to fresh drinking water throughout the day. Residents were offered a choice of meals at mealtimes and there was evidence of care being taken to cater to residents' individual preferences. A breakfast buffet was now operating each morning, which was welcomed by residents.
Judgment: Compliant
Regulation 26: Risk management
Inspectors were not assured that the risk management policy was implemented in practice, or that the centre's risk register was a live document. The most recently documented risk in the register was made in January 2019 despite a number of risks or hazards being identified in the intervening period, such as those relating to staff turnover, training and fire safety. Other hazards and risks identified on inspection were not included in the risk register. For example, the doors on the first floor leading to the stairwell were accessible to residents and cleaning solutions were on top of the cleaning trolley and could be accessible to residents.
Monthly risk audits were planned to form part of the annual audit schedule for 2019, but there was no evidence that any risk audits had been carried out. There
Page 13 of 32
was little evidence that accidents, incidents and near misses were analysed for root causes and no learning was identified to inform staff of improvements required to improve the quality and safety of the service.
Falls prevention is the responsibility of all staff. The risk of residents falling was mitigated by the use of a symbol on a resident's bedroom door. However not all staff were aware of what the symbol stood for.
Judgment: Not compliant
Regulation 27: Infection control
Three of the five actions from the previous inspection had been completed, but two, relating to infection control training and practices had not been adequately addressed. Three housekeeping staff did not have training in infection control. On the day of the inspection, some staff spoken with were not sufficiently knowledgeable of infection control practices.
While the roster had recently been amended to ensure that housekeeping staff were present in the centre each day, staff went off duty in the early afternoon and were not on duty again until the following morning. Cleaning rosters examined confirmed that there not all bedrooms were cleaned consistently on a daily basis. Rooms which were not cleaned on a given day were prioritised for cleaning the following day. Apart from thoroughly cleaning a room when it was vacated, there was no schedule for deep cleaning in the centre. Inspectors noted some malodours during the inspection and feedback received from relatives and residents indicated that the hours and allocation of housekeeping staff required review.
Judgment: Not compliant
Regulation 28: Fire precautions
The registered provider did not have adequate arrangements in place to contain the spread of fire. Bedroom doors did not have automatic closing devices to prevent, contain and delay the spread of smoke in the event of a fire, or to aid evacuation. Most bedroom doors were found to be open throughout the centre and some doors to communal rooms were held open. This presented a high risk to residents accommodated within this compartment. This was discussed with the management team who confirmed that an inspection by a fire safety consultant had identified this issue in late June 2019 and they were awaiting the fire safety report.
The centre had records of simulated fire drills completed in 2019. No drills were carried out to simulate night time staffing levels. The drills simulated the evacuation

Page 14 of 32
of one bedroom and did not provide assurance that all the residents in a compartment could be evacuated safely. In addition the compartments were large and the majority of residents required the assistance of two to mobilise. Inspectors were not assured that residents could be safely evacuated to another compartment in an emergency with night duty staffing levels.
Personal evacuation plans were available for all residents in the centre and had information on any mobility equipment and number of staff required as well as any sensory deficits such as poor eyesight or hearing loss. However the resident’s level of cognition and supervision needs following evacuation was not stated. According to the evacuation plans, some residents required a hoist transfer to a wheelchair in an emergency.
Annual fire training was a requirement for all staff. Training records reviewed on the day of the inspection showed that 34 staff had not completed formal fire safety training in the centre or were overdue refresher training. Seventeen staff who were employed since April 2019 had not attended fire training, including nurses on night duty who would be responsible for co-ordinating the evacuation of residents in the event of an emergency.
Records were maintained of weekly and daily fire safety checks. The registered provider had arrangements in place for the maintenance of the centre's ''L1'' fire alarm and detection system, which had been serviced quarterly and was subject to weekly testing. Arrangements were also in place for quarterly servicing of emergency lights throughout the centre.
An urgent compliance plan was issued following the inspection in relation to the issues identified in relation to fire safety. The provider submitted a compliance plan response to assure the Chief Inspector that all staff had attended fire safety training and that fire drills were carried out to ensure that residents could be safely evacuated from one compartment to another in an emergency. The registered provider also immediately increased staffing levels at night.
Judgment: Not compliant
Regulation 29: Medicines and pharmaceutical services
There was a policy in place to guide nurses on the safe management of medications. Medicines were generally administered in accordance with the prescriber's instructions and action had been taken since the previous inspection to ensure that a nurse’s signature was recorded whenever a resident refused their medicines. Some residents were administered crushed tablets without any evidence of this instruction from the prescribing general practitioner (GP). A sample of medication records was examined and two residents received crushed tablets that were not intended to be digested in a crushed format. This practice could pose a potential risk to residents.

Page 15 of 32
Medicines were stored securely in the centre. Controlled drugs balances were checked at each shift change as required by the Misuse of Drugs Regulations 1988 and in line with the centre's policy on medication management. Records of controlled drugs were found to be accurate and complete.
Judgment: Not compliant
Regulation 5: Individual assessment and care plan
Care plans were adequate and described the care required to meet the needs of residents but the process for reviewing care plans required improvement. Potential residents were assessed prior to admission to ensure the centre could meet their needs. A nursing assessment was completed on each resident within 48 hours of admission and a care plan developed to meet the individual resident's assessed needs. Care plans were updated to reflect specialist medical or allied health care advice and were routinely reviewed every four months. Inspectors found that care plans were not consistently revised or amended in line with a resident’s changing needs. For example, a care plan relating to medication management had not been updated to reflect a resident's ongoing refusal of medications. Measures to ensure that care plans were implemented required strengthening. For example, there was no evidence of monitoring the food or fluid intake for a resident who was underweight and at risk of further weight loss and dehydration.
Plans were in place to implement an electronic care planning system in the months following the inspection.
Judgment: Substantially compliant
Regulation 6: Health care
A good standard of health care was provided in this centre. Residents had good access to local GP services and some residents retained the services of their own GP. Some improvement was required to ensure that medical advice was consistently sought in a timely manner. Residents were supported to access national screening programmes and community allied health care services as required, for example, dietitian, occupational therapy, physiotherapy and optical services.
Judgment: Compliant
Regulation 7: Managing behaviour that is challenging

Page 16 of 32
The action from the previous inspection had been completed, but further issues were identified. Some residents had responsive behaviours (how people with dementia or other conditions may communicate or express their physical discomfort, or discomfort with their social or physical environment). Residents with behaviours such as resisting personal care, had a person centred care plan which was known to staff. Distraction techniques were clearly set out to support staff, such as ‘talk to her about her dog’. Behavioural assessments were completed initially but there was no evidence that ongoing behaviours, such as shouting, was assessed or monitored to determine what underlying emotion or unmet need may trigger the behaviour. Consequently, the behavioural support plans did not guide staff to respond appropriately to these behaviours. The role of health care staff to meet the social needs of residents requires review. Boredom can sometimes trigger responsive behaviours and inspectors' observations of two residents with responsive behaviours showed that they had limited interpersonal social engagement with staff during the day. Staff were busy and therefore were only available to greet the residents as they passed by, and there was over reliance on music or TV for social stimulation. Noise levels were unacceptably high on some occasions and it was not evident that staff had considered this as the underlying cause for a resident who had exit seeking behaviours.
The centre had a low level of restraint use and maintained a restrictive practices register which outlined practices in use that could impact on the freedom of a resident. Restraints in use included bedrails and lap belts, and two residents wore alarm tags which set off an alarm if they attempted to leave the building. Restrictive practices were risk assessed and there were records of two hourly safety checks in place. However some sections of the risk assessment forms were not completed and there was no evidence that alternatives were trialled and less restrictive options were used.
Judgment: Not compliant
Regulation 9: Residents' rights
Residents' rights were respected in the centre and the ethos of care was person-centred. Residents were consulted with regarding the planning and organisation of the centre.
An activity programme for residents included a range of activities facilitated by internal staff and external service providers. Examples of activities provided include pet therapy, arts and crafts, games, baking, live music and exercise programmes. Sensory-based activities, which are suitable for residents with dementia, were also included in the programme. A number of recent events in the centre included a garden party and an exhibition of residents' art. Activities were facilitated by one full time activities co-ordinator and one part-time staff member that had recently been appointed. Staff informed inspectors that the addition of this activity staff member
Page 17 of 32
would increase the provision of activities from five days to six days a week. Upon admission to the centre, residents or their families provided information about residents' lives, interests and capabilities. This was used to develop activity care plans for all residents and inform the overall activity programme. Records demonstrated that these were regularly reviewed by the activities co-ordinator. Inspectors observed a number of activities, including gardening and live music. The activities co-ordinator supported residents to engage in these activities in a meaningful manner, in line with their capabilities. However, it was noted that in the absence of support from care staff, the co-ordinator was also required to tend to residents' needs. This interrupted some activities, which negatively impacted residents' experiences.
Outings had not occurred this year due to issues accessing appropriate transport. Inspectors were informed that the activities co-ordinator occasionally supported some residents to run errands in the local village. However, a resident told inspectors that they wished to go outside of the centre but were frustrated that they couldn't.
Residents could independently access the centre's secure garden, which contained a chicken coop, garden furniture and plenty of colourful flowers and shrubbery.
While many residents had a pleasant mealtime experience, review was required to enhance the social aspect of mealtimes for residents on the first floor, who required assistance and supervision at mealtimes. Residents seated in the ground floor dining room were observed to enjoy a very social mealtime experience. Tables in this room were dressed with table cloths and flowers, and condiments were available on each table. Residents and staff were observed to be chatting throughout the meal. On the first floor, the same mealtime was a solitary dining experience for these residents. Tables did not have place settings and one or two residents ate their meal while others watched and waited. Staff explained that in order to ensure the food were hot the meals were served to a resident only when a staff member was available to provide assistance. Staff interacted well with residents but the social aspect of dining could be enhanced.
Residents were consulted with regarding anything which affected their lives in the centre, and their feedback was sought through a number of different means. Surveys were conducted with residents, as well as regular residents' and relative meetings.
All accommodation consisted of single rooms and privacy was respected with staff observed knocking on doors before entering. There was access to daily papers, television and radio. Wireless internet was accessible throughout the building and residents had access to a telephone if required.
Residents' privacy and dignity was respected by staff, who were observed knocking on residents' bedroom doors prior to entering, and administering care in a discreet manner.
Residents were facilitated to exercise their civil, political and religious rights. Roman Catholic mass was held weekly in the centre and residents were supported to

Page 18 of 32
practice their respective faiths. The process for facilitating future opportunities for voting was described to inspectors.
An independent advocate was available to meet with residents if required.
Judgment: Substantially compliant
Page 19 of 32
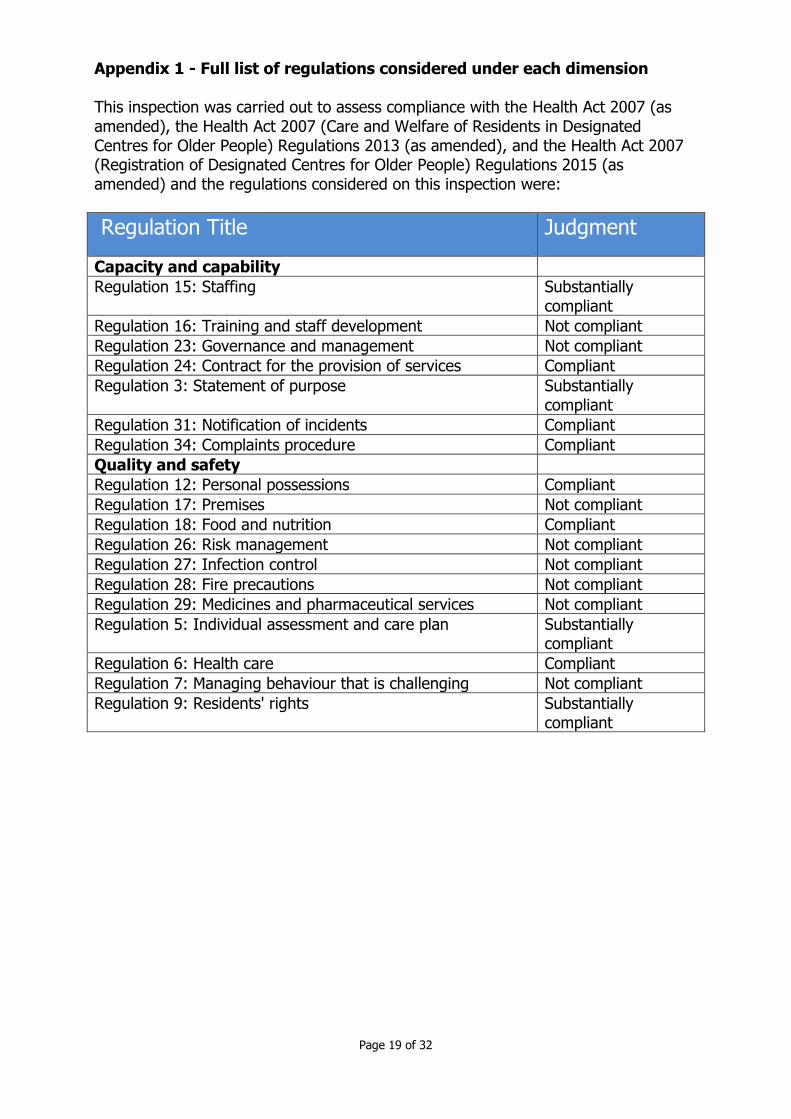
Appendix 1 - Full list of regulations considered under each dimension This inspection was carried out to assess compliance with the Health Act 2007 (as amended), the Health Act 2007 (Care and Welfare of Residents in Designated Centres for Older People) Regulations 2013 (as amended), and the Health Act 2007 (Registration of Designated Centres for Older People) Regulations 2015 (as amended) and the regulations considered on this inspection were:
Regulation Title Judgment
Capacity and capability
Regulation 15: Staffing Substantially compliant
Regulation 16: Training and staff development Not compliant
Regulation 23: Governance and management Not compliant
Regulation 24: Contract for the provision of services Compliant
Regulation 3: Statement of purpose Substantially compliant
Regulation 31: Notification of incidents Compliant
Regulation 34: Complaints procedure Compliant
Quality and safety
Regulation 12: Personal possessions Compliant
Regulation 17: Premises Not compliant
Regulation 18: Food and nutrition Compliant
Regulation 26: Risk management Not compliant
Regulation 27: Infection control Not compliant
Regulation 28: Fire precautions Not compliant
Regulation 29: Medicines and pharmaceutical services Not compliant
Regulation 5: Individual assessment and care plan Substantially compliant
Regulation 6: Health care Compliant
Regulation 7: Managing behaviour that is challenging Not compliant
Regulation 9: Residents' rights Substantially compliant

Page 20 of 32
Compliance Plan for Strathmore Lodge Nursing Home OSV-0004449 Inspection ID: MON-0027664
Date of inspection: 12/09/2019 Introduction and instruction This document sets out the regulations where it has been assessed that the provider or person in charge are not compliant with the Health Act 2007 (Care and Welfare of Residents in Designated Centres for Older People) Regulations 2013, Health Act 2007 (Registration of Designated Centres for Older People) Regulations 2015 and the National Standards for Residential Care Settings for Older People in Ireland. This document is divided into two sections: Section 1 is the compliance plan. It outlines which regulations the provider or person in charge must take action on to comply. In this section the provider or person in charge must consider the overall regulation when responding and not just the individual non compliances as listed section 2. Section 2 is the list of all regulations where it has been assessed the provider or person in charge is not compliant. Each regulation is risk assessed as to the impact of the non-compliance on the safety, health and welfare of residents using the service. A finding of:
Substantially compliant - A judgment of substantially compliant means that the provider or person in charge has generally met the requirements of the regulation but some action is required to be fully compliant. This finding will have a risk rating of yellow which is low risk.
Not compliant - A judgment of not compliant means the provider or person in charge has not complied with a regulation and considerable action is required to come into compliance. Continued non-compliance or where the non-compliance poses a significant risk to the safety, health and welfare of residents using the service will be risk rated red (high risk) and the inspector have identified the date by which the provider must comply. Where the non-compliance does not pose a risk to the safety, health and welfare of residents using the service it is risk rated orange (moderate risk) and the provider must take action within a reasonable timeframe to come into compliance.

Page 21 of 32
Section 1 The provider and or the person in charge is required to set out what action they have taken or intend to take to comply with the regulation in order to bring the centre back into compliance. The plan should be SMART in nature. Specific to that regulation, Measurable so that they can monitor progress, Achievable and Realistic, and Time bound. The response must consider the details and risk rating of each regulation set out in section 2 when making the response. It is the provider’s responsibility to ensure they implement the actions within the timeframe. Compliance plan provider’s response:
Regulation Heading Judgment
Regulation 15: Staffing
Substantially Compliant
Outline how you are going to come into compliance with Regulation 15: Staffing: • Household hours were under review at the time of inspection, increased hours have now been implemented. • Staff vacancies are being advertised and positions are being filled as required. • Call bells are being monitored daily by CNMs, audits are being carried out and reviewed. • All staff references will be verified going forward. • Staff allocation will be monitored and kept under review.
Regulation 16: Training and staff development
Not Compliant
Outline how you are going to come into compliance with Regulation 16: Training and staff development: • Staff training is being carried out regularly, a plan for training all staff and new starters in all mandatory fields is currently being reviewed. In the interim all staff have completed fire training, infection control, safeguarding, dementia and responsive behaviors, manual handling and restrictive practice. Dysphagia training will be completed in the coming weeks. • A training matrix will be kept up to date within the Centre to ensure compliance.

Page 22 of 32
Regulation 23: Governance and management
Not Compliant
Outline how you are going to come into compliance with Regulation 23: Governance and management: • The auditing system was in the process of being reviewed and improved, New and improved auditing systems are now in place and a yearly schedule is in progress. • Management meetings are held fortnightly and on site monthly. Minutes are taken, actioned and reviewed at the following meetings. • Management meetings are held monthly in the centre attended by the RPR and the Clinical director these meetings have an agenda and Minutes. • 2 weekly Skype meetings are held with reviews of KPIs and and rags these meetings will have Minutes documented. • In- house meetings will consist of- heads of department meetings held monthly. • Management meetings PIC/CNM held weekly. • All other team meetings will be held 2 monthly and as needed. • Minutes will be documented for all meetings and communicated to all staff
Regulation 3: Statement of purpose
Substantially Compliant
Outline how you are going to come into compliance with Regulation 3: Statement of purpose: • Our statement of purpose has been amended to reflect the areas that needed updating. • Deputizing arrangement for the PIC has now been documented. • List of allied health services available has been added. • More detailed information on en suite facilities added.
Regulation 17: Premises
Not Compliant
Outline how you are going to come into compliance with Regulation 17: Premises: • Sluice room doors now have coded locks to them. • Storage space has been reviewed and we have 2 new areas for storage. • All lockers will be lockable in the coming weeks. • A new cleaning system is being implemented and household staff will be using a dry mop system which will eliminate the risk of cross infection for residents, alongside a new

Page 23 of 32
cleaning regime with extended cleaning hours. • A refurbishment plan is Underway as part of building upgrade works which includes painting & decorating and furniture. • We are bringing back into use rooms which had been unused/under used in previous regime, for example, reminiscence rooms, activity rooms and relaxation rooms.
Regulation 26: Risk management
Not Compliant
Outline how you are going to come into compliance with Regulation 26: Risk management: • The risk management policy is being reviewed and updated, with a more robust system in place. Going forward all risks will be documented in the live risk register. • New and improved Audits and yearly schedule is being implemented. • Incidents and accidents will be reviewed by the DON, ADON and CNMs, with emphasis on ensuring root cause analysis is being carried out to improve practices. • Learnings from the above will be disseminated to all staff through scheduled meetings and on the floor handovers. • Using the lessons learnt to improve the service and develop practice. • Staff training on fire has been completed with all staff trained in fire safety and evacuation practices along with Falls.
Regulation 27: Infection control
Not Compliant
Outline how you are going to come into compliance with Regulation 27: Infection control: • All staff have been trained in infection control. • A new cleaning system and schedule is in place to ensure all relevant areas are being cleaned thoroughly. This will include deep cleaning regime- Monthly/3 Monthly. • A new dry mop system is in place which is allowing housekeeping staff to utilize there time more efficiently. • Housekeeping hours had been under review prior to inspection and preliminary plans were in place for the change of hours, extended hours are now in place to allow for a more robust cleaning schedule. • Regular audits will be implemented to ensure we are complaint with safe practices. • A member of the housekeeping team will be trained as a Hygiene champion. • A new Infection Control Policy will be in place.
Page 24 of 32
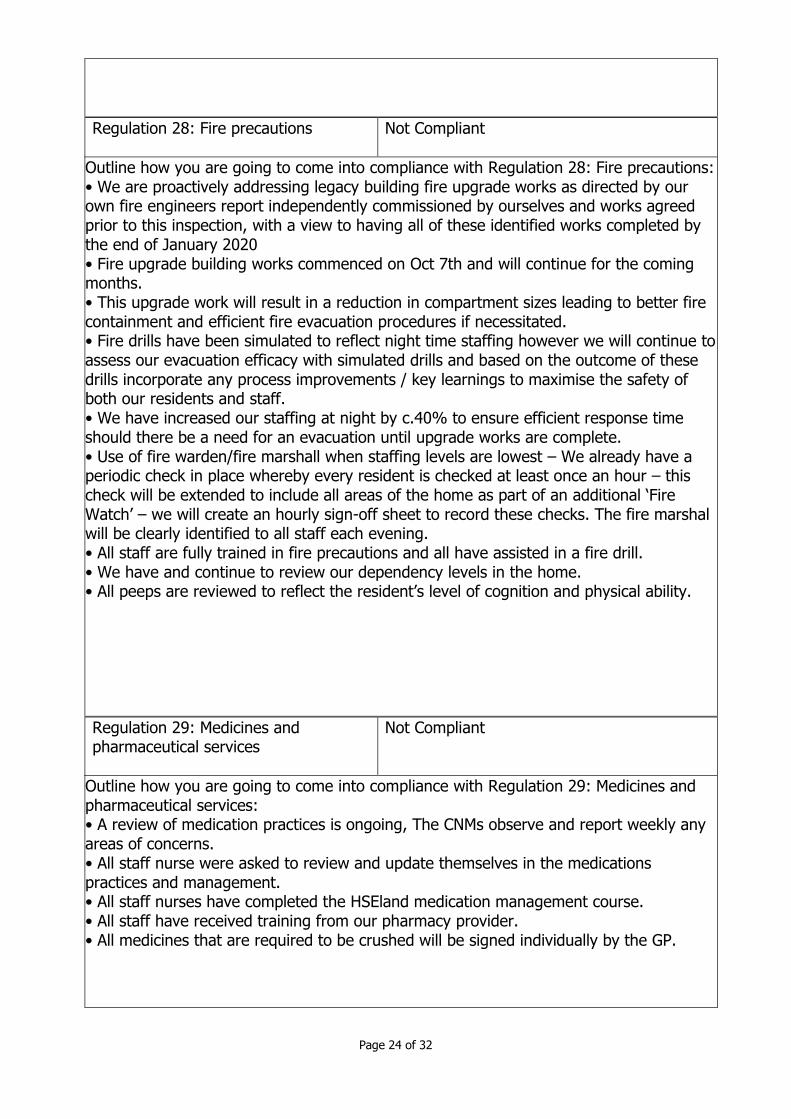
Regulation 28: Fire precautions
Not Compliant
Outline how you are going to come into compliance with Regulation 28: Fire precautions: • We are proactively addressing legacy building fire upgrade works as directed by our own fire engineers report independently commissioned by ourselves and works agreed prior to this inspection, with a view to having all of these identified works completed by the end of January 2020 • Fire upgrade building works commenced on Oct 7th and will continue for the coming months. • This upgrade work will result in a reduction in compartment sizes leading to better fire containment and efficient fire evacuation procedures if necessitated. • Fire drills have been simulated to reflect night time staffing however we will continue to assess our evacuation efficacy with simulated drills and based on the outcome of these drills incorporate any process improvements / key learnings to maximise the safety of both our residents and staff. • We have increased our staffing at night by c.40% to ensure efficient response time should there be a need for an evacuation until upgrade works are complete. • Use of fire warden/fire marshall when staffing levels are lowest – We already have a periodic check in place whereby every resident is checked at least once an hour – this check will be extended to include all areas of the home as part of an additional ‘Fire Watch’ – we will create an hourly sign-off sheet to record these checks. The fire marshal will be clearly identified to all staff each evening. • All staff are fully trained in fire precautions and all have assisted in a fire drill. • We have and continue to review our dependency levels in the home. • All peeps are reviewed to reflect the resident’s level of cognition and physical ability.
Regulation 29: Medicines and pharmaceutical services
Not Compliant
Outline how you are going to come into compliance with Regulation 29: Medicines and pharmaceutical services: • A review of medication practices is ongoing, The CNMs observe and report weekly any areas of concerns. • All staff nurse were asked to review and update themselves in the medications practices and management. • All staff nurses have completed the HSEland medication management course. • All staff have received training from our pharmacy provider. • All medicines that are required to be crushed will be signed individually by the GP.

Page 25 of 32
Regulation 5: Individual assessment and care plan
Substantially Compliant
Outline how you are going to come into compliance with Regulation 5: Individual assessment and care plan: • The care plans and assessment are under review, we have commenced the use of epicare, and hope to have our residents care plans and assessment digital in the coming months. • Further training on care plans will be implemented in the coming weeks. • All care plans will be person centered, they will be formally reviewed at least 4 monthly or more frequently if there is a change to reflect the changing needs of each resident. • Care plans will be descriptive and support/guide staff to deliver person centered care.
Regulation 7: Managing behaviour that is challenging
Not Compliant
Outline how you are going to come into compliance with Regulation 7: Managing behaviour that is challenging: • All staff have been trained in behaviours that challenge in the recent weeks, observation of practices by CNMs daily to ensure good practices are in place. • Staff nurses are aware to ensure they complete all sections of the risk assessment forms for restrictive practice. • Behaviours that challenge Care Plans will be descriptive and identify any triggers, the care plans will guide the staff in supporting the resident who have behaviours that challenge. • We will ensure that all of the care team will be involved in the social engagement of all our residents.
Regulation 9: Residents' rights
Substantially Compliant
Outline how you are going to come into compliance with Regulation 9: Residents' rights: • Activities are under review, and resident satisfaction surveys and feedback will be received in the coming weeks.

Page 26 of 32
• The above information will be collated to ensure we provide an activity service for our residents with outings/wishes that are important to them and are achieved throughout the year. • The dining experience and updating of the dining/sitting room is part of the PICs improvement plan for the home this is underway presently and should be complete in the coming weeks.

Page 27 of 32
Section 2: Regulations to be complied with The provider or person in charge must consider the details and risk rating of the following regulations when completing the compliance plan in section 1. Where a regulation has been risk rated red (high risk) the inspector has set out the date by which the provider or person in charge must comply. Where a regulation has been risk rated yellow (low risk) or orange (moderate risk) the provider must include a date (DD Month YY) of when they will be compliant. The registered provider or person in charge has failed to comply with the following regulation(s).
Regulation Regulatory requirement
Judgment Risk rating
Date to be complied with
Regulation 15(1) The registered provider shall ensure that the number and skill mix of staff is appropriate having regard to the needs of the residents, assessed in accordance with Regulation 5, and the size and layout of the designated centre concerned.
Not Compliant Orange
30/10/2019
Regulation 16(1)(a)
The person in charge shall ensure that staff have access to appropriate training.
Not Compliant Orange
30/11/2019
Regulation 16(1)(b)
The person in charge shall ensure that staff are appropriately supervised.
Not Compliant Orange
30/10/2019
Regulation 17(2) The registered provider shall, having regard to the needs of the residents of a particular designated centre,
Not Compliant Orange
31/01/2020

Page 28 of 32
provide premises which conform to the matters set out in Schedule 6.
Regulation 23(a) The registered provider shall ensure that the designated centre has sufficient resources to ensure the effective delivery of care in accordance with the statement of purpose.
Substantially Compliant
Yellow
11/10/2019
Regulation 23(c) The registered provider shall ensure that management systems are in place to ensure that the service provided is safe, appropriate, consistent and effectively monitored.
Not Compliant Orange
30/11/2019
Regulation 26(1)(a)
The registered provider shall ensure that the risk management policy set out in Schedule 5 includes hazard identification and assessment of risks throughout the designated centre.
Substantially Compliant
Yellow
30/10/2019
Regulation 26(1)(b)
The registered provider shall ensure that the risk management policy set out in Schedule 5 includes the measures and actions in place to
Substantially Compliant
Yellow
30/10/2019

Page 29 of 32
control the risks identified.
Regulation 26(1)(d)
The registered provider shall ensure that the risk management policy set out in Schedule 5 includes arrangements for the identification, recording, investigation and learning from serious incidents or adverse events involving residents.
Not Compliant Orange
30/10/2019
Regulation 27 The registered provider shall ensure that procedures, consistent with the standards for the prevention and control of healthcare associated infections published by the Authority are implemented by staff.
Not Compliant Orange
18/10/2019
Regulation 28(1)(a)
The registered provider shall take adequate precautions against the risk of fire, and shall provide suitable fire fighting equipment, suitable building services, and suitable bedding and furnishings.
Not Compliant Orange
31/01/2020
Regulation 28(1)(c)(ii)
The registered provider shall make adequate arrangements for
Substantially Compliant
Yellow
30/10/2019

Page 30 of 32
reviewing fire precautions.
Regulation 28(1)(d)
The registered provider shall make arrangements for staff of the designated centre to receive suitable training in fire prevention and emergency procedures, including evacuation procedures, building layout and escape routes, location of fire alarm call points, first aid, fire fighting equipment, fire control techniques and the procedures to be followed should the clothes of a resident catch fire.
Not Compliant Orange
11/10/2019
Regulation 28(1)(e)
The registered provider shall ensure, by means of fire safety management and fire drills at suitable intervals, that the persons working at the designated centre and, in so far as is reasonably practicable, residents, are aware of the procedure to be followed in the case of fire.
Substantially Compliant
Yellow
11/10/2019
Regulation 28(2)(i) The registered provider shall
Not Compliant Orange
11/10/2019

Page 31 of 32
make adequate arrangements for detecting, containing and extinguishing fires.
Regulation 29(5) The person in charge shall ensure that all medicinal products are administered in accordance with the directions of the prescriber of the resident concerned and in accordance with any advice provided by that resident’s pharmacist regarding the appropriate use of the product.
Not Compliant Orange
30/10/2019
Regulation 03(1) The registered provider shall prepare in writing a statement of purpose relating to the designated centre concerned and containing the information set out in Schedule 1.
Substantially Compliant
Yellow
08/10/2019
Regulation 5(4) The person in charge shall formally review, at intervals not exceeding 4 months, the care plan prepared under paragraph (3) and, where necessary, revise it, after consultation with the resident concerned and where appropriate that resident’s
Substantially Compliant
Yellow
30/11/2019

Page 32 of 32
family.
Regulation 7(1) The person in charge shall ensure that staff have up to date knowledge and skills, appropriate to their role, to respond to and manage behaviour that is challenging.
Not Compliant Orange
30/11/2019
Regulation 7(3) The registered provider shall ensure that, where restraint is used in a designated centre, it is only used in accordance with national policy as published on the website of the Department of Health from time to time.
Substantially Compliant
Yellow
30/11/2019
Regulation 9(2)(b) The registered provider shall provide for residents opportunities to participate in activities in accordance with their interests and capacities.
Substantially Compliant
Yellow
30/11/2019