Report No. 8100-ZIM Zimbabwe Issues in the Financing of...
94
Report No.8100-ZIM Zimbabwe Issues in the Financing of Health Services February 5, 1990 Population and Human Resources Development Southerr, AfricaDepartment FOROFFICIAL USE ONLY Document of the World Bank This document has a restricted distribution andmay be used by recipients only in the performance of theirofficialduties. Its contents may nototherwise be disclosed without WorldBank authorization. Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of Report No. 8100-ZIM Zimbabwe Issues in the Financing of...

Report No. 8100-ZIM
ZimbabweIssues in the Financing of Health Services
February 5, 1990
Population and Human Resources DevelopmentSoutherr, Africa Department
FOR OFFICIAL USE ONLY
Document of the World Bank
This document has a restricted distribution and may be used by recipientsonly in the performance of their official duties. Its contents may not otherwisebe disclosed without World Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

U .-
CURRENCY susIVALES(1988 Average)
US$ 1.00 - Z$ 1.8018Zs 1.00 - USS 0.555
FISCAL YEAR
Government Fiscal Year: July 1 - June 30
ABBREVIATIONS AND ACRONYMS
Danish International Development Agency - DANIDAEssential Drugs List of Zimbabwe - EDLIZEuropean Economic Community - BECGross Domestic Product - GDPGovernment Medical Stores - GMSGovernment of Zimbabwe - GOZJoint Allocation Committee - JACLength of Stay - LOSMedical Aid Society of Central Africa - HASCAMinistry of Finance, Economic Planning
and Development - MFEPDMinistry of Health - MOH
Ministry of Public Constructionand National Housing - NPCNH
National Association of Medical aidSocieties - NAMAS
Non-Governmental Organization - NGONational Health Development Fund - NHDFNational Health Insurance Scheme - NHIS
Norwegian Agency for InternationalDevelopment - NORAD
Primary Health Care - PHCPersonnel Management Information
Systems - PHIS E-
Public Sector Investment Program - PSIP
State-Certified Nurses/State-CertifiedMidwives - SCN/SCMN
Swedish International Development Authority - SIDAState Registered Nurses - SRNSexually Transmitted Diseases - STDUnited Nations Development Program - UNDPUnited Nations Children's Fund - UNICEFUnited States Agency for International
Development - USAIDVillage Health Workers - VHWVote of Credit - VOCWorld Health Organization - WHOZimbabwe Essential Drug Action Progr4m - ZEDAPZimbabwe Expanded Program of
Immunization - ZEPIZimbabwe National Family Planning
Council - ZNFPC

FOR omCIL USE ONLY
TABLE OF CONTENTS
EXECUTIVE SUARY . . . . . . . . . . * . . . . . . . . i-viii
CHAPTER I. INTRODUCTION . . . . . . . . . . . . . . . . . . . . . 1-6Rationale for Study . .. . . . . . . . . . . . . . . . . . . . . . . 2Background on Zimbabwe's Health Sector . . . . . . . . . . . . . . . . 4Government Health Policies and Strategies . . . . . . . . . . . . . . 5Outstanding Issues in Health Financing . . . . . . . . . . . . . . . . 5
CHAPTER II. FINANCIAL PROFILE OF THE HEALTH SECTOK ... . . . . . 7-17Overview of Health Expenditures .... . . . . . . . . . . . . . . . . 7Recent Trends in MOH Expenditures . . . . . . . . . . . . . . . . . . . 10
CHAPTER III. RESOURCE MOBILIZATION .... . . . . . . . . . . . . 18-36Introduction ...... . . . . .. . . . . .. . . . . .. . . . . . 18User Fees for Government Health Services . . . . . . . . . . . . . . . 19Private Health Insurance ..... . . . . . . . . . . . . . . . . . . 25Government-Operated Health Insurance .... . . . . . . . . . . . . . 29Local Government, NGO, and Community Financing . . . . . . . . . . . . 32Tax Treatment of Health Expenditures and Health Professionals Incomes . 35
CHAPTER IVf EFFPICIENT USE OF RESOURCES IN THE DEALT! SECTOR . . . 37-48Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37Allocative Efficiency . . . . . . . . . . . . . . . . . . . . . . . . . 37Issues in Technical Efficiency .4.0.................. . 40
CHAPTER Vs MANAGEAMNT OF DEALTH SXPENDITURES . . . . . . . . . . . .49-55Background .............................. . 49Budgeting and Planning . . . . . . . . . . . . . . . . . . . . . . . . . 50Manpower Planning . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Revenue Collection ..... . . . . . . . . . . . . . . . . . . . . . 54Procurement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
This report is based on the findings of a mission that visited Zimbabwe inApril-May 1988, composed of Mr. R. Becht (mission leader), Mr. C. Bonga(health administrator), Mr. M. Chaora (public health specialist), Mr. S.Fjelland (management specialist), Mr. P. Manga (economist), Mr. E. Haphenduka(accountancy specialist), Ms. M. Thomas (economist), Mr. R. Vogel (economist),and Ms. L. Zinyemba (health sector planner). Follow-up missions took place inJuly and October 1988 and in May 1989. Ms. E. Fernz, Me. G. Johnson, andMs. R. Mendoza provided secretarial assistance, Ms. M. Barton providedgraphics support and Hs. H.E. Iskenderian made final revisions and preparedannex material.
This document has a restricted distribution and may be used by recipients only in the performanceof their official duties. Its contents may not otherwise be disclosed without World Bank authorization.

CHAPTE VI. CONCLUSIONS AND RECOMEND&TIONS . . . . . . . . . . . . 56-62Resource Mobilization . . . . . . . . . . . . . . . . . . . . . . . . . 57Efficiency . . . . . . 0 . . . . . . . . . . . . . 59Management of Health Expenditures . . . . . . . . . . . . . . . . . . . 61Role of Donors .. . ........ 62
ANNEXES
Annex I: Potential Impact of Health Resource Mobilization MeasuresAnnex IIs Registered Health Personnel - 1986Annex III: Fees and Charges for Various Health Care ServicesAnnex IV: Medical Aid Societies Annual Subscriptions, 1987-88Annex Vs Government Hospitals Activity Analysis Summary and By
Province, 1987Annex VIs Kiusion Hospital Activity Analysis By Province, 1987
LIST OF TABLES IN TEXT
Table 11-1. Total Expenditures on Health Care, 1986-87Table II-2. MOH Expenditures for Health, 1980-88Table II-3. Ministry of Health Recurrent Expenditures, 1979-88Table 11-4. Composition of MOH Expenditures, 1986-87Table 11-5. Summary Data on nealth Services by Province, 1987Table II-6. Capital Expenditures f)r Health, 1.982-88Table III-1. Ministry of Health Cost Recovery, 1981-88Table III-2. Cost Recovery for Municipal Government Health Institutions,
1986-87Table III-3. Medical Aid Societies Membership, 1981-87Table 111-4. CIMAS, MASCA, and Railmed Medical Aid Societies Expenditures
for Medical Care, 1982-83 and 1986-87Table IV-1. Hospital Occupancy Rates and Average Length of Stay, 1987Table IV-2. Cost Per Admission and Per Patient-Day in MOH Hospitals, 1987Table V-1. Skilled Staff Vacancy Rates by Level of the Health Care
System, 1986-87
LIST OF FIGURES IN TEXT
Figure 2.1. Health Expeaditures By Source and Provider, 1986-87Figure 2.2. Summary Data on Health Services by Province, 1987Figure 4.1. Hospital Occupancy Rates and Average Hospital Length of Stay, 1987Figure 4.2. Cost Data by Province, 1987

EXECUTIVE StMMARY
Introduction jnd Synopsis
i. Dueing the nine years that have passed since independence in 1980,Zimbabwe has made impressive progress in providing health care to itspopulation. Millions of people have for the first time gained access tobasic care, and a range of cnst-effective preventive health programs havebeen launched. The service delivery and health status figures given belowattest to this rapid progress, much of it financed through an expansion ofGovernment spending for health.
ii. But, as Zimbabwean officials widely recognize, the country is nowfacing a mounting crisis in the financing of health services. In theprevailing environment of severe overall fiscal constraints, there is adanger that the Government may not be able to meet fully its existingfinancial commitments tc the health sector (salaries, medical equipment anddrugs, transport, manpower development, etc.). Yet not only will all ofthese commitments need to be met, but Zimbabwe will have to make a numberof additional investments in preventive and curative care, if the country'shealth objectives for the 1990s and the beginning of the next century areto be achieved. The issue of how to pay for existing and expanded futurehealth services is therefore a real and pressing one.
iii. To deal successfully with these growing difficulties in thefinancing of health care, Zimbabweans generally agree that ways must befound to mobilize additional resources for use in the sector, and to obtair.more "good health" from existing expenditures. At the same time, theGovernment's ongoing efforts to achieve greater equity in health - both inaccess to care and in paying for this care - must be maintained, and evenreinforced.
iv. This will require that Zimbabwpans develop bold and imaginativepolicies and programs, and enhance their analytical and management skillsin the financing of health care. It will also require a concerted andcoordinated effort between the public and private sectors, includingcentral, local, and municipal government, church missions and other NGOs,private modern and traditional practitioners, and industry.
v. This report offers a number of policy and program options thatcould help to resolve the crisis in financing health services in Zimbabwe.The recommended measures which are summarized below are organized intothree main groupings: measures to inject additional money into the healthsector (Resource Mobilization - including selective increases in usercharges, greater cost-sharing between central and local government andNGOs, expansion of private insurance, and creation of a National HealthDevelopment Fund); measures to help Zimbabwe get more "value for money" inhealth (Allocative and Technical Efficiency - increased budget shares forprimary and preventive health care, stronger management of hospitalexpenditures and patient stay, etc.); and measures to develop the systemsand skills needed to support stronger health financing (Management ofHealth Expenditures - revised budget and expenditure procedures, improvedfacility-based accounting skills/systems, decentralized procurement ofgoods and privatizat.on of hospital services, etc.).

-ii-
Successes of the 19809, Challenges of the 1990s
vi. Zimbabwe's achievements in health d'tring the 1980s have been trulyimpressive. More than 500 health centers have been built or upgraded, andmore than a dozen district hospitals have been completed or are underconstruction. More than 2000 auxiliary nurses (State Certified Nurses, SCN)and 4000 Village Health Workers (now Community Development Workers) havebeen trained. The percentage of children fully imiunized has nearly tripledfrom 252 in 1980 to 67Z in 1988, and the proportion of married women ofchildbearing age using modern contraceptive methods has risen from 142 to36Z during the same period. Life expectancy has increased from 55 to 59years, while infant mortality has declined to from 82 to 72 per 1,000births and maternal mortality has fallen to 90 per 100,000 deliveries. Allof these current indicators are significantly better than the averages forSub-Saharan Africa.
vii. While the private sector, including both modurn and traditionalpractitioners, for-profit and non-profit institutions, have had animportant part in providing and paying for these expanding health services,the public sector - especially the central governmernt - has played theleading role in this process. In 1986-87, the latest year for whichcomprehensive data were available, the public sector was responsible for63z of all health-related expenditures (in financial terms), includingMinistry of Health (402) and other central ministries (132), and municipaland local government (9Z). The private sector, which provided the balanceof health services. was composed of private doctors (25?), industries,mines, and commercial farms (8;, arLd NG0 (42).
viii. By source of funds, the central government was even more dominant,accounting for 612 of all expenditures, including 122 in the form offoreign aid channeled through the Government and 492 in locally-generatedrevenues. This suggests that while foreign aid makes up about a fifth ofpublic spending for health, Zimbabwe is not as heavily dependent onexternal assistance as many other developing countries. By contrast,municipal and local governments provided only 32 of all funds for healthcare, a reflection of their heavy reliance at present on central governmentsubsidies. In addition, private sources of financing met about 362 of totalexpenditures, including private insurance (172), out-of-pocket spending(10X), industry, mines, and commercial farms (8Z), and NGOs (1X).
ix. In the years immediately following independence, public spendingfor health increased rapidly, by 38% in 1981 and 13? in 1982 (in realterms), as the Government sought to expand basic health services tocommunities that had been previously neglected. A series of preventivehealth initiatives were also launched in such areas as rural water andsanitation, child immunization, pre-natal care and family planning, malariaand other communicable disease control. Large numbers of additionalparamedical staff were trained and deployed.
x. In recent years, however, the pace of Government spending forhealth has been slowing markedly, ind the per capita level of expenditurehas even started to fall slightly, because of the severely constrainedfiscal situation facing the Government coupled with a continued high rateof population growth of over 3? a year. During 1982-88, the MOH budget

- iii-.
increased by an average of just 3.92 a year, with rises of only 3.12 and2.12 in 1986-87 and 1987-88, respectively. In real terms, the MOH spentabout 2$ 12 per capita in 1987-88, the same amount as six years earlier.
xi. This situation is further complicated by the fact that the healthsector's share of the Government budget - currently running at just above52 - is not likely to rise significantly over the next few years. TheMinistry of Finance, Economic Planning and Development (MFEPD) hasindicated that any increase in MOH's budget share would probably depend onsteps taken by MOH to generate more of its required resources internallywithin the health sector or to develop new sources of revenues.
xii. U'nder these circumstances of stagnant or even declining centralgovernment financing of health services, there is a real danger that theGovernment will find it difficult to meet its existing commitments forrecurrent financing of the health system. Beyond this, there is still alarge unfinished agenda of additional investments in health care that mustbe made, if Zimbabwe is to achieve its health objectives. The country'sprimary health care infrastructure and services and a range of preventivecare activities in particular need to be further expanded over the comingyears. Despite the important progress made in these areas during thecurrent decade, the Government's health system remains somewhat top-heavyand urban-oriented, with a strong emphasis on curative, rather thanpreventive, services. In 1987, half of MOH's facility-based "patientbudget' of Z$ 188.2 million was spent at tertiary-level facilities,including Z$ 67.4 million (362) at the four central hospitals located inHarare and Bulawayo. Only about 282 of MOB e enditures were for preventivehealth activities. In addition to strengthening maternal and child health(control of diarrheal and respiratory illnesses, ante-natal care and familyplanning), the Government has Indicated that it wishes to develop programsto deal with a range of chronic adult di -ases related to environmentalfactors (diet, smoking, substance abuse, stress) and with AIDS. More needsto be done, too, to improve equity in access to basic health services, andin sharing the burden of paying for health care in Zimbabwe.
Axiii. In dealing with the growing difficulties in financing health caredescribed above, Zimbabwe is fortunate to be endowed with a large, diverse,and dynamic health systemu, embracing central and loca: government, churchmission facilities, industrial clinics, private practitioners, andtraditional healers. Funds flow into this system from a wide range ofsources, many of them non-governmental. Zimbabwe also has many talented,well-trained, and highly-committed medical personnel and managers workingin the health sector.
xiv. To address these imminent challenges in health financingsuccessfully, Zimbabwean policy-makers must pursue three basic strategies:
(a) Mobilize more resources for the sector, through a combination ofincreases in user charges, establishment of insurance programs orexpansion of existing insurance schemes, development of earmarkedtaxation, etc. The Government could also seek to induce non-governmental institutions to assume greater responsibility forproviding and paying for health services, by encouraging churchmissions, other non-profit NGOs, private practitioners, commercial

-iv-
enterprises, health insurance companies, *raditional healers, andlocal communities themselves, to increase their level ofparticipation in the nation's health system;
(b) Improve the efficiency of existing expenditures, i.e., obtain more'value for money' in health. This means improving both allocativeand technical efficiency, espzcially in the public sector but alsoamong private health providers; and
(c) Strengthen the management of health expenditures, so that publicand private health practitioners and administrators are able todesign and implement measures for enhanced resource mobilizationand efficiency. This requires the development of individual skillsand broader systems of management in financial planning, projectappraisal, expenditure control, procurement, etc.
xv. This report recommends that Zimbabw-ean policy-makers pursuesimultaneously a combination of all three strategies outlined above, andsuggests specific policy and program options for implementing thesestrategies. 'While the full list of options Is spelled out and analyzed inthe chapters which follow, some of the key recommendations are summarizedbelow.
Mobilizing More Resources for Health (Chapter III)
xvi. In the area of resource mobilization, the priority actionsshould be to:
(a) Increase user fees in public facilities, especially to cover thefull cost of patients in private wards and to meet part of thecost of basic out-patient services and drugs. The overall level offees should be raised, and adjusted periodically in line withinflation. Fee collection efforts need to be strengthenedsignificantly through a combination of procedural changes, skillstraining and automation, and incentives for individual facilities.At the same time, the poor should continue to be protected fromhigher fees through socially-accepted and administrativelyfeasible arrangements for means-testing and granting exemptions.
(b) Consider seriously the establishment of a National HealthDevelopment Fund (NHDF), financed through taxes on alcohol ortobacco, which would be used specifically to pay for essentialprimary care and preventive health services, especially in poor,underserved rural and urban communities. The NHDF, which would beincremental to the normal MOH budget, could be utilized for acombination of investment (e.g., clinic upgrading, communityhealth worker training) and recurrent expenditures (e.g., purchaseof essential drugs).
(c) Develop effective '.ormulae for sharing costs of health carebetween MOH and (i) local government (rural and district councilsand municipalities) and (ii) church mission health providers.Application of such formulae would generate additional local-levelresources for health, reduce the central government's financial

-V-
burden. and probably improve the quality of services by givinglocal government bodies and communities a stronger sense ofownership of health facilities.
(d) Expand the existing private health insurance system, byencouraging greatet competition among medical aid societies andenacting legislation requiring that formal sector employers assisttheir workers in obtaining and payinig for a basic minimum packageof health services.
xvii. If all four of these recommendations were adopted, their impact onthe financing oi health care in Zimbabwe would be protound: an estimated ZS240 million in additional annual resources (1988 prices) would be injectedinro the country's health system, equivalent to nearly 382 of the Z$ 636million actually spent for health in 1987-88 (T%ble below). Of thisincremental amount, about Z$ 130 million would potentially be available tothe MOH - equivalent to about 562 of MOH's 1987-88 budget - including Z$ 50million from user fees and ZS 80 million from the NHDF. In addition,expanded private health insurance could generate as much as Z$ 80-100mrillion a year in expenditures, part of which would flow to the Governme,tas user charges for private patients. Cost-sharing between central audlocal government and NGOs would also result in at least Z$ 10 million inextra annual resources for health.
Z IMBADWE
Potential Impact of Health Resource MobilizaLion Measures
Measure Annual Incremental Revenues(Z$ millions)
1. User Charges
- Full cost pricing for private in-patients 15-20- Standard out-patient fees 10- Drug charges on per item basis 10-15- Adjusting fees to match inflation 7
Subtotal 42-52
2. National Health Developnent Fund 80
3. Cost-Sharing Between MOE and Local Govt andChurch Mission Hosvitals 10-15
4. Expanded Private Health Insurance 80-100
TOTAL 212-247

-vi-
xviii. How should such potential incremental revenues be spent by MOH, topromote "better health for all"? As indicated below in this report,expansion of primary and preventive health activ'ities should be consideredas the first priorities for this additional Government spending. WhileZimbabwean health planners and policy-makers would have to make thedetailed expenditure decisions, incremental funds for health would open upto them a range of possibilities: with an extra Z $40 million, for example,MOH could build five new district hospitals, or upgrade about 200 rnralclinics; train and pay the salaries of thousands of additional SRN, SCN,and community health workers; quadruple the current budget of the ZimbabweNational Family Planning Counc'l; or some combination of these and a numberof other exciting options.
Utilizing Resources More Efficiently (Chapter IV)
xix. In the area of increasir.g efficiency of health expenditures,policy-makers should consider a number of priority actions, including thosetc:
(a) Improve the allocative efficiency of Government spending, byincreasing the MOH budget shares devoted to primary-level servicesand preventive care. Regarding PHC, the Ministry should seek tomodify its facility-based "patient' budget, currently distributed501/30Z/20? among tertiary/secondary/primary care, by developingrealistic plans and targets - for example, to achieve a40Z/3OX/30Z distribution by 1995. SimilarlY. MOH should settargets for raising the share of the budget devoted to preventive F
health programs from its current level of about 281 to, forexample, 351 by 1995 and 402 by the year 2000. Preventive healthactivities that merit additioral spending include community watersupply and sanitation, communicable disease control, nutritioninterventions, smoking prevention, and family planning. Setting ofthese targets and monitoring progress would be facilitated by thechanges in budgeting and cost accounting recommended elsewhere inthis report.
(b) Reduce the cost per patient-day for care in Government hospitals,especially by ensuring referrals to the appropriate (lowest-cost)level of facilities, keeping patient length-of-stay to anacceptable minimum, and eliminating unnecessary expenditures forpersonnel, drugs, transport, feeding, and other support services.MOH needs to develop systems and skills for monitoring andanalyzing these hospital expenditures, -tarting with the fournational referral hospitals and eight provincial hospitals whichaccount for half of the fpati.nt" budget and a third of all MOHexpenditures. Preliminary analysis contained in this report pointsto wide variations among hospitals in bed occupancy rates, averagelength-of-stay for maternity and general in-patients, and inaverage cost per patient admitted. One central Aiospital andseveral provinces's facilities appear to stand out as havingaverage costs well above the norm: MOH may wish to examine theircost structures, as well as possible measures to reduce unit costs(e.g., contracting out services to the private sector) while

-vii-
maintaining or improving the quality of services, as part of afirst round in improving hospital efficiency.
(c) Enhance the efficiency of resource utilization, including foreignexchange and budget funds in general, for drugs, While theZimbabwe Essential Drugs Action Program has make great strides inthis ares, more needs to be done. Scarce foreign exchange shouldbe spent initially each year to meet the basic epidemiologicalnseeds of the country's population, especially for low-cost genericdrugs. lOH should have a priority claim on adequate foreignexchang4 to cover its basic annual drug requirements, withouthaving to buy from local suppliers It. small quantities at highmark-ups, as currently takes place. To do this, the procedures forallocating foreign exchanges to the pharmaceutica' system may needto be changed. MOH will also have to improve its ability toforecast accurately ita annual drug requirements. In addition.inappropriate and excessive drug prescribing practices should becurbed, through a combination of fees for each drug item, limitson the number of drugs per out-patient attendance, monitoring ofdoctors' prescr'bing practices in hospitals, and doctor andratient education.
(d) Scrutinize the public sector investment program for health, toensure that the most cost-effective capital items are beingselected, and that their implied incremental recurrent costs aresustainable. This is partly a matter of strengthening the planningand capital .n-idgeting capabilities of the MOH. and developingenhanced procedures for preparing and assessing the sectorinvestment program. It will also require that MOH review andrevise periodically the technical specifications for standardfacilities (e.g., district hospitals, health centers) andequipment, in order to eliminate or modify any unnecessary andcostly items.
Strengthening the Management of Resources for Health (Chapter V)
xX. Finally, the health financing reforms outlined above, designed tomobilize additional resources and increase efficiency in the sector, willonly be effectively implemented if the institutions and individuals workingin the sector develop tbe complementary analytical, planning, andmanagement skills and systems required. In fact, the pace of reform may belimited in some cases by the extent and timing of these managementimprovements: for example, improved fee collection in central andprovincial hospitals may depend on automating cost accounting and billingsystems and training hospital staff to use these systems. In this regard,policy-makers should consider a series of priority actions to strengthenmanagement of health expenditures, including those to:
(a) Revise the MOH budget and expenditure formats, to make them moreresponsive to the needs of managers at various levels of thehealth care system, including individual facilities. While suchmodified formats would need to be compatible with the overallGovernment budget categories, they should also make it easier for

-viii-
MOH policy-makers and managers to express their financialrequirements, allocate resources. and track actual spendinigme-ningfully, by functions (program, service, etc.) and type ofexpenditure, for various levels of aggregation (national,provincial, district, individual facility or hospital department).
(b) Continue progressively to decentralize responsibility forpreparing budgets, incurring expenditures, and effecting payments- starting with the four central hospitals and the eightprovincial medical directors' offices. Implementation of thisrecomniendation would need to be closely linked to (a) above, andto a major training program for MOH planners, provincial anddistrict medical officers and health administrators, and hospitaland clinic managers.
(c) Build up MOH's health manpower planning capacity, so that theworkload distribution, quality of care, and salary implications ofalternative manpower scenarios can be promptly and accuratelyassessed.
(d) ImProve accounting skills and systems in all MOH, local andmunicipal aovernment, and church mission health facilities, toinclude a basic minimum set of properly-maintained account books.
(e) Decentra±ize to provincial or district level the procurement ofcertain goods and services that can be purchased locally in a moretimely and cost-effective manner than through centralizedprocurement, and also experiment with "contracting out" to theprivate sector for selected hospital services such as patientfeeding and laundry.
An Action Plan for Health Financing Reform
xxi. Once Zimbabwean policy-makers have selected the options for healthfinancing reform that they wish to see pursued, and hava gathered thenecessary broad-based support for their proposals, an action plan should beformulated. Such a plan would include a detailed description of the reformmeasures, a timetable for their phased implementation, targets or othermonitorable indicators of progress in achieving the reforms, estimates oftheir financial impacts, atd a budget covering the related training,equipment, and studies required.
xxii. While the health finance reform program itself would be a home-grown Zimbabwean initiative, the Government should be able to count onstrong interest and support from the donor community, which has been activein the country's health sector over the past decade. Donors, including theWorld Bank, could play a useful role in the reform process by providingtechnical assistance and funding for the required training and studies.Donors could also assist by focusing their project resources upon high-priority investments in primary health care and preventive services, asidentified as a result of improvements in overall health sector financialplanning and budgeting.

CHAPTER I
INTRODUCTION
Rationale for Study
1.01 Zimbabwe has made impressive gains i- providing health care to its9.3 million people during the past eight years following the country'sindependence in 1980. Progress has been especially great in redressing themarked inequities in health care that existed prior to independence. TheGovernment has extended basic health care to hitherto underserved ruralareas, by constructing and staffing about 290 clinics, reconstructing about160 war-damaged clinics, and upgrading an additional 160 facilities. Toprovide preventive and promotive - and some simple curative - services atthe grass-roots level, more than 4,400 Village Health Workers (nowCommunity Development Workers) were trained between 1980 and 1985. To staffthe clinics, large numbers of unqualified personnel were also retrained asState-Certified Nurses.
1.02 The Government's emphasis on primary health care (PHC), combinedwith other measures to improve the quality of life in the rural areas, hasalready started to bear fruit. The percentage of fully immunized childrenhas increased from 25? in 1980 to 42Z in 1984 and 67Z in 1987, and couldwell approach the target level of 80? by 1990. Infant malnutrition has alsodeclined from 292 in 1980 to 162 in 1984, and there is evidence that it ha4continued to drop to 10-12Z in selected provinces at present. The propor-tion of womea of childbearing age regularly using modern contraceptivemethods has risen from 14? in 1980 to 27Z in 1984 and to 36Z in 1986.
1.03 Despite these major achievements, Government officials recognizethat many problems remain in Zimbabwe's health sector. Some remote ruralpopulations are still underserved, with more than 100 additional clinicsrequired to reach them. PHC programs to provide clean drinking water andadequate sanitation still have a long way to go. Preventable communicablediseases including malaria, schistosomiasis, typhoid, respiratoryinfections, tuberculosis, and sexually-transmitted diseases (STD) cLntinueto take a high toll in morbidity and mortality. AIDS is also beginning toimpose a significant social and economic cost. Notwithstanding theimportant accomplishments to date of Zimbabwe's family planning program,the Government has indicated that the country's current population growthrate of 3.22 a year is unacceptably high, threatening to undermine socialand economic gains.
1.04 As Zimbabwe's health care delivery system expands, the country isalso experiencing serious shortages of staff, especially in the publicsector. These include not only doctors and nurses, but also para-medicalpersonnel such as nurse assistants and health assistants to staff healthcenters, as well as health administrators to plan anci manage provincial anddistrict health programs. These shortages are due to inadequate trainingfacilities for the various health cadres and to significant differentialsin salary and conditions of service between the public and private sectors.
1.05 The recent major expansion of health services in Zimbabwe has alsobeen accompanied by an increase in spending for health care. Total expendi-

-2-
tures for health (in real 1981 terms) have risen from Z$ 155.8 million in1981 to Z$ 291.4 million in 1987, an annual growth rate of nearly llz.Health's share of GDP has thus risen from 3.11 in 1981 to 4.22 in 1987.Increases in public expenditures for health have also outpaced overall GDPgrowth, averaging 8.72 a year in real terms. In recent years, however,Government spending for health has become constrained by the worseningoverall fiscal situation, and levels of real per capita public spendinghave started to fall.
1.06 Under these circumstances, a number of important questions arebeing asked by Zimbabwe's policy-makers:
(a) Resource Allocations How much should Zimbabwe be spending onhealth care, given the country's limited resources? What should bethe relative expenditure shares and financial contributions ofGovernment and of non-governmental entities, including bothcommercial and non-profit institutions?
(b) Resource Mobilization: How can additional revenues be generatedfor health? What is the appropriate role for user charges?Expanding coverage of medical aid (insurance) schemes? Nationalhealth insurance ? Is there scope for greater communityparticipation and for cost-sharing between central and localgovernment? Are there other innovative ways of mobilizingadditional resources for health?
(c) Equity: How can all Zimbabweans be guaranteed access to a basicminimum level of health care? Who should be paying for Zimbabwe'shealth costs? How can the basic health needs of lower-incomegroups be met while still ensuring the financial viability of theentire health care system?
(d) Allocative and Technical Efficiency Within the Sector: Areresources in the health sector being spent in priority areas,where the returns are relatively high, such as basic rural healthinfrastructure and PHC activities (immunizations, family planning,water and sanitation, etc.)? How can technical efficiency also beenhanced, for example, by reducing the average patient's length-of-stay in certain facilities or modifying procedures forprocurement and distribution of drugs? Developing alternativelower-cost staffing patterns for various levels of facilities?Devising new budgeting, expenditure, end accounting practices forGovernment health institutions? How much could be saved throughsuch changes?
(e) Improved Management of Resources: What improvements in healthresource management skills and systems are most urgently required?Does the XOH budget system need to be revised to make it moreuseful to policy-makers and health administrators? Are thefinancial implications of alternative manpower scenarios and drugpolicies being adequately analyzed? How can MOH procurementpolicies and procedures be modified to achieve greaterefficiencies?

-3-
1.07 In 1988, the Government of Zimbabwe asked the World Bank tocollaborate in the search for answers to these questions through a study ofhealth care financing. The following report is the result of thatcollaboration. The Government has long been aware of these various healthfinancing issues, and in recent years has become increasingly conc-nedabout setting priorities in the use of scarce resources in the se( ar,generating additional revenues within the health sector, enhancing equity,and containing costs while increasing efficiency. The World Bank welcomedthe Government's invitation to participate in the study, given the Bank'sinterest and involvement in the health sector, most notably through itsearlier Population, Health, and Nutrition Sector Review (1983) and theongoing Z$ 80 million Family Health project (Loan 2744-ZIM, 1987-91). Thestudy was also intended to provide a set of policy and programrecommendations to the Government that could be incorporated in existingand planned projects, including a second World Bank-assisted health projectto be formulated in 1989-90.
Background on Zimbabwe's Health Sector
1.08 Health Status. The health status of Zimbabwe's 9.3 million people(1988) is fairly typical for countries with a similar per capita income(per capita GDP of US$ 630 in 1987) and at a similar stage of development.Life expectancy is 59 years, infant mortality is 72 per 1000 live births,and maternal mortality is about 90 per 100,000 deliveries. The major causesof mortality and morbidity amc..g children are respiratory infections,malnutrition, diarrhea, meningitis, and malaria. The leading causes cfdeath and illness among adults include respiratory diseases, tuberculosis,sexually-transmitted diseases, pregnancy-related complications, accidents,and cardio-vascular diseases.
1.09 Sector Organization and Institutions. The institutional make-up ofZimbabwe's health sector is highly heterogeneous, with the centralgovernment, municipalities and local authorities, church missions and otherNGOs, industries and mines, private practitioners, and traditional healersall playing significant roles. Since independence, the Government hasgradually organized the public and NGO institutions plus some pri-atefacilities into a four-tiered system of service delivery:
(a) at the first level, 56 rural hospitals and 927 health centers(about 132 MOH, 510 local government, 70 mission, 55 urban, and160 industry-owned facilities), providing a range of preventiveservices as well as some basic curative care;
(b) at second level, 55 designated dJstrict hospitals (MOH and churchmission-run), of which 26 meet the standard requirements,providing a first line of referral;
(c) at third level, 8 provincial and 4 general hospitals; and
(d) at the fourth level, 5 central hospitals (including the specialistpsychiatric hospital) located in Harare and Bulawayo -nd intendedto serve as national referral facilities.

-4-
1.10 Health Manpower. Key personnel in Zimbabwe's health sector includeabout 1250 doctors, 9000 state-registered nurses (SRN) and state-certifiednurses and nurse-midwives (SCN/SCMN). There are also about 350 healthassistants involved in environmental health and other PHC activities, plusabout 4500 village-health workers (VHW) who are currently being absorbedinto the Ministry of Community Development, Cooperatives, and Women'sAffairs as multi-nurpose community development workers. About 12,000traditional healers are registered in a Government-sponsored association,and their total number is believed to be about 20,000.
1.11 About two-thirds of Zimbabwe's physicians and SRNs and a third ofthe country's SCNs work in the private sector, where pay and conditions ofservice generally compare favorably to the public/NGO sector. As a result,the public health institutions continue to experience shortages of staff,especially doctors, nurses, and other specialists (e.g., pharmacists) atprovincial, district, and health center levels. One of the challengesfacing the Government is to devise a system of incentives and regulationsthat ensures adequate staffing of public health institutions, given thatGovernment training facilities are graduating about 80 doctors and severalhundred nurses annually.
Government Health Policies and Strategies
1.12 The Government's main policies and strategies for the healthsector are spelled out in its 1984 white paper entitled "Planning forEquity in Health" and in its 1987 "Health for All Action Plan". The keysectoral objectives are to improve access and equity in the provision ofbasic health services and to ensure the financial sustainability of such ahealth system. In order to achieve these objectives, the Government's mainprogrammatic strategies include:
(a) Promoting PHC, especially in the rural areas. TLis meansbuilding and upgrading additiunal health centers and districthospitals and funding priority activities including immunizations,ante-natal care, control of diarrheal diseases, growth monitoringand therapeutic feeding for malnourished children, healtheducation, control of communicable diseases, and supply of safedrinking water and sanitation;
(b) Expanding family planning, especially by integrating FP servicesinto the PHC activities of all health institutions, p'iblic andprivate;
(c) Improving the supply and minimizing the cost of essential drugs;
(d) Building or upgrading district-level hospitals and clinics;
(e) Improving the patient referral system through a combination ofexpanded lower-level facilities, education, and incentives,including the structure of fees; and

-5-
(f) Encouraging increased efficiency and financial viability of thehealth system through self-help, local financing mechanisms,appropriate user charges, and health insurance.
Out-standing Issues in Health Finamcing
1.12 While Zimbabwe has made significant progress since independence inreallocating resources for health care to previously neglected low-incomegroups, a number of important problems in the financing of health systemremain. These include: (a) declining levels of per capita expenditure forhealth; (b) inadequate revenue generation within the sector from usercharges and insurance payments, at a time of increasingly strained overallfiscal performance; (c) insufficient allocation of resources to cost-effective preventive care measures, and inefficiencies in expenditures,especially for drugs and hospital patient care; (d) persisting inequitiesin the distribution of benef'ts and costs of health care; and (e)weaknesses in budgeting, the incurring of expenditures, and the monitoringof costs in the public sector. Some of the key issues investigated in thisreport include the following:
1.13 Resource Mobilization (Chapter III):
(a) Is there scope for increasing fees in Government healthfacilities? Who would be willing and able to pay more than they doat present (private patients, those covered by medical aid, othermiddle-income groups)? For which types of services? At what levelshould these fees be set? Should nominal fees be imposed for someservices (e.g. out-patient consultations) in order to deterunnecessary use? How can the poor be protected?
(b) How can the collection of fees be made more efficient, through newstaffing and accounting procedures? Can institutions be givengreater incentives to collect fees?
(c) Should private medical aid schemes be expanded? How? If so, whatwould be the likely impact on the Government budget? The demandfor, and cost of, private medical care? The availability ofpersonnel, especially doctors and nurses, for delivery of healthcare in the public sector?
(d) Does national health insurance make sense? In what form? How wouldit work in practice? What degree of coverage can be achieved? Whatwould be its net financial impact on the Government budget? On theuse of public and private care?
1.14 Allocative and Technical Efficiency (Chapter IV):
(a) Which programs with the health sector are most cost-effective, andhow can funds be reallocated to these programs?
(b) How can hospital-based services be made more efficient? Byeliminating duplication of services among institutions? Reducing

-6-
unnecessary surgery and hospitalization? Lowering average lengrhof stay? Making physicians and hospital administrators more budgetand cost-conscious, through changes in financial managementpractices?
(c) How far has the & tbabwe Essential Drugs Action Program (ZEDAP)gone in increasing the efficiency of pharmaceuticals manufactureand the supply and distribution system? What more can be done?
(d) Are there other areas of inefficiency/waste/abuse that could becurbed? Unnecessary referrals? Inefficient use of transport?
1.15 Health Resources Management (Chapter V)
(a) How can the Government's financial information system for healthbe improved to provide meaningful and timely information tomanagers at all levels of the health infrastructure and at variousdegrees of aggregation? By program as well as cost category? Canthis information be combined with service statistics to produceunit cost data?
(b) How can modified procedures for budgeting and monitoring of publicexpenditures for health help to contain costs and raise efficiencywithin the sector?
.c) What financial planning skills need to be developed for the healthsector, within the MOH head office, at provincial, district, andfacility levels? In the areas of both c-nttal and recurrentexpenditures?
(d) How adequate are basic accounting systems in Government and NGOhealth facilities, in relation to the needs for budgeting,expenditure reporting, and revenue collection? What can be done tostrengthen these systems?

-7-
CHAPTER II
FINANCIAL PROFILE OF THE HEALTH SECTOR
Overview of Health Expenditures
2.01 Expenditures for health care in Zimbabwe in fiscal 1987 are shovnin Table II-1, by source of funds and health service providers (users offunds). The size and complexity of the matrix is a reflection of the widediversity of institutirns providing health-related services in the country,and of the numerous mechanisms for financing the cost of those services.Providers include the Ministry of Health and other ministries (WaterResources, Local Government, Education, Labor); local government (districtand rural councils) and municipalities; church missions and other NGOs;private enterprises operating their own hospitals and clinics (industries,mines, and commercial farms); and private practitioners comprising about800 doctors. Sources of funds are both public and private, domestic andexternal; some providers are largely self-financing (e.g., industries,mines, and farms), while others rely heavily on outside sources of funding(e.g., church missions). Direct payment by patients is not a major sourceof financing for most of the provider categories.
2.02 As can be seen in the table, total expenditures on health andhealth-related activities covering capital, recurrent, and technicalassistance costs amounted to Z$ 636.2 million in 1987. This translates toper capita expenditures of about Z$ 70 or US$ 45 at the then prevailingexchange rate. Compared to many other developing countries, Zimbabwe's percapita expenditures for health are relatively high. According to a surveyof 29 developing countries carried out for the 1987 World Bank policystudy, Financing dealth Services in Developing Countries, Zimbabwe's percapita expenditure level of about US$ 30 in 1980 was one of the highest inSub-Saharan Africa, exceeded only by Botswana, Swaziland, and Zambia, andwas higher than a number of developing countries from other regionsincluding China, Indonesia, Morocco, and Thailand. About 90% of Zimbabwe'stotal health expenditures in 1987 were for operating and maintenancepurposes, and 1OZ for capital items. Using 1981 prices, 1987 expendituresamounted to Z$ 291.4 million, nearly twice the Z$ 155.8 million spent onhealth care in 1981. This implies an real increase of almost 11 a yearover the 1981-87 period.
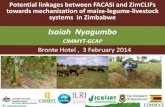
2.03 Providers of Health Care. Table II-1 and Figure 2 1 show thatwhile Government provides nearly two-thirds of health care in Zimbabwe (infinancial terms), private institutions and individuals also play a majorrole in the health system. In 1987, a little more than 631 of expenditureswere incurred by public providers of health care, with the private sectoraccounting for the remaining 37%. Among the public providers, the MOH alonewas responsible for two-fifths of all health expenditures in the country(Z$ 255.5 million), and other ministries involved mainly in water andsanitation improvements spent another 132 of the total (Z$ 84.4 million).Municipal health departments (dominated by Harare and Bulawayo, see ChapterV) were also major care providers (6Z); rural local government, whileimportant in terms of coverage (about 500 clinics serving two-thirds of thepopulation), accounted for only 22 of nationwide expenditures for health.

-8-
The bulk of health expendit'tres by private providers were incurred byprivate doctors (Z$ 156.8 million or nearly a quarter of the total) andprivate industries, mines, and commercial farms (Z$ 50.8 million or 8%).The roughly 70 church mission hospitals which account for more than a thirdof the 18,000 hospital beds in Zimbabwe reported Z$ 18.6 million inexpenditures or 3% of the national total. Voluntary organizations,including the Red Cross and a number of local NGOs, spent an additional Z$7.6 million or just over 1X of the total.
Table II -1
ZUABIETotal biqenltures on Health Care, 1986-87
Saurces of Fuids
Central JicLIp ch try Voluntary Forel insurn Private Total TotalGovt alities missons Mines Organl- Assis Scms bndiv
Comner- zatlons tance dualsclal
Service Providers Farms
1. Ministry of Health 232.20 17.30 3.00 3.00 255.50 40.22. Other Ministries 36.27 46.11 ZO00 84.38 13.33. Parastatals 5.04 3.48 8.50 1.S4. Olstrlr': and Rural
Cctcmls 11.47 2.85 0.20 14.52 2.35. Ailclpalitles 10.70 25.00 3.95 39.65 6.26. MissIons 14.50 2.56 1.50 18.58 2.97. himstry, Mines
Cuercial Farms 50.75 50.75 8.08. Voluntary Organizatlons 4.50 3.10 7.60 1.29. Private Sector 102.00 54.75 156.75 24.6
TOTAL 310.18 25.00 2.56 50.75 4.50 74.32 105.00 63.90 636.21
X 48.8 3.9 0.4 8.0 0.7 11.7 16.5 10.0 100.0
Note: (I) All flgues expressed hI 1987 pris.
2.04 Sources of Funds. If foreign (mainly public) assistance to thehealth sector is included, the public purse in 1987 covered about 642 oftotal outlays for health, roughly the same share of expenditures incurredby public providers of health care in that year. Central governmentrevenues for health amounted to Z$ 310.2 million or nearly 49% of thetotal. These revenues financed about 90% of the MOH budget and, throughdirect subventions, 80Z of the budgets of the local councils and churchmission health providers. Central government funds also made an importantcontribution to health-related expenditures by other ministries (43%) andmunicipal health departments (27Z).
2.05 Among the other important sources of financing for health care,private industry, mines, and commercial farms spent over Z$ 50 million attheir own facilities. Foreign assistance (mainly official multi-lateral andbilateral loans and grants) accounted for nearly 12% of expenditures,

-9-
FIGURE 2.1: HEALTH EXPENDITURES BY SOURCE AND PROVIDER
Total Expenditures on Health Care by sourceof Funds, 1986-87
10%
1 Central Govt.
17% UMunicipalities* Church Missions
48% Industry
1% 0. Foreign Asst.
.NGOs
12% IN X 0 F @ . mHealth Insur.
* Private
8%1%4%
Total Expenditures on Health Care byProvider, 1986-87
25%-- U ~~~~Ministry of Health
O Other Ministries- ~~~40% *Parastatals
* Loca Govt Agencies
1~ -% 0 lC3 Missions
8% UCt Eti- -_ 7_ __ | Industry
3% ss-- -- ; - - 1|1 Private Sector
8% -t
1% 13%

-10-
allocated to a wide range of Government, parastatal (ZNFPC), mission, andNGO providers. The largest share of foreign aid (Z$ 46 million) went toministries other than MOH, and was spent mainly for rural water andsanitation. Health insurance was also a significant source of financing forthe health sector, with the 27 medical aid societies in the country payingout Z$ 102 million or nearly one-sixth of ll expenditures, for health careprovided to 4Z of Zimbabwe's population. Roughly 102 of outlays for healthcame in the form of out-of-pocket expenditures by private individuals, andmost of these went to private doctors and pharmacies; d'rect payments byindividuals covered just over 1Z of MOH expenditures (2.3Z when medical aidpayments are included), and about a tenth of municipalities' expendituresfor health. This indicates the relatively low level of cost recovery in thepublic sector (see Chapter III).
Recent Trends in MOR Expenditures
2.06 Table II-2 shows the growth of the Ministry of Health (MOH;recurrent budget relative to the Government of Zimbabwe (GOZ) budget sinceindependence. Throughout the period 1981-88, the MOH budget has averagedabout 52 of total GOZ outlays, although this declined to 4.5Z in thedrought year 1983 and recovered gradually to 5.4Z in 1988. For middle-income developing countries with a per capita GDP level similar toZimbabwe, the share of health expenditures in total government spendingvaries widely, from a low of 2-32 (Egypt, Indonesia, Morocco) to a high of9-li (Dominican Republic, Paraguay). In this regard, Zimbabwe occupies themiddle ground, with its budget share allocated to health similar toBotswana (5.62) and slightly lower than a number of other African countries(Lesotho, Liberia, Zambia) v,hich spend 7-8Z of the budget for health.
TABLE 11-2
MOH EBpendltures for Health, 1980-88(a miiiions)
&ut asTotal' percent
G07 GOZ MOH VOC2 Total of GOZFiscal Bdget Vote Health IMI Budget (X)Year (1) (2) (3) (4)8(2)+(3) (5)=(4)/(1)
1980-81 1627.5 83.7 n.a. 83.7 5.11981-82 2121.7 108.9 n.a. 108.9 5.11982-8 2936.6 13 5 1.3 132.9 4.51983-84 3052.7 139.0 3.0 142.0 4.71984-85 3568.4 159.4 7.1 166.5 4.71985-86 3875.3 196.2 8.6 204.8 5.31986-87 4837.3 240.6 8.2 248.8 5.11987-883 5173.6 261.7 15.6 277.3 5.4
souc: WL iUwets
Notes:
1. Includes contractal and statutory appropriations.2. Vote of Credit: foreign-ssisted projects for which rosuress flow through the
Ministy of Finance.3. Estimate.n.a. Not available.

-11-
2.07 Table II-3 presents MOH recurrent budgetary data that has bpenadjusted to take into account increases in the general price level and inthe population. It shows that between 1979-80 and 1987-88, MOH expendituresgrew more than fivefold in nominal terms (from Z$ 54.2 million to Z$ 277.3million), by about 94Z in real terms (from Z$ 56.8 million to Z$ 110.4million), and by 48Z in real per capita terms (from Z$ 8.0 to Z$11.8).These significant increases in public spending for health reflect the post-independence government's serious commitment to improving access to healthcare for a large segment of the population that was underserved before1980.
TABLE II-3
ZIMBABWEMinistry of Health Recurrent Expenditures. 1979-88
(Z millilons)
MOH MOHReal Nominal Real
Total Total Annual Per PerMjOH MOF Growth Population Capita Capita
Year (Nominal) (Real 1981 terms) (U) (0(0) (Zt) (Zs)
1979-80 64.2 66.8 7,098 7.63 8.001980-81 83.7 78.4 87.9 7,268 11.47 10.741981-82 108.9 88.2 12.6 7,538 14.52 11.781982-83 132.9 92.9 6.4 7,817 17.04 11.911983-8' 142.0 87.6 -5.9 8,lvv 17.63 10.801984-8& 168.5 91.8 4.9 8,406 19.82 10.931985-86 204.F 100.0 9.0 8,708 23.64 11.491986-87 248.8 108.1 3.1 9,014 27.64 12.011987-88 277.a 110.4 2.1 9,323 29.82 11.87
Average real growth rate 1979-87 = 8.7X per annum.
Average real growth rate 1982-87 = 3.9X per annum.
Soeroe:
(1) MOH expenditures from Covernment budgets.
(2) Government fiscal year index c^nstructed from consumer price index for higherIncome urban familIIes, WRTERLY DIGEST OF STATISTICS.
(8) Population estimates from World Bank data.
2.08 As column 4 of Table II-3 indicates, the big surge in real MOHexpenditures occurred in the first two years following independence, whenthe budget increased by 37.9Z and 12.52, respectively. Since then, giventhe overall fiscal constraints facing the GOZ, the rate of real growth ofthe MOH budget has been much lower, averaging 3.9Z a year during the sixyear period 1982-88. During the drought year of 1983-84, the MOH budge:-actually contracted by almost 6Z. For 1987-88, the most recent year forwhich data are available, the health budget grew by only 2.1% in realterms, below the annual rate of population increase of 3.2Z. This sluggish

-12-
growth in public funding of health care has forced the Government toexamine carefully ways in which available resources for health can be moreefficiently utilized, and to search for additional sources of revenues forhealth services provided by MOH. The constrained state of public financeshas also prompted GOZ to begin considering an expanded role for localgovernment and the private sector (including NGOs) in providing health carein the future.
2.09 MOB Expenditures by Functional Category. Table II-4 contains abreakdown by functional category of the MOH budget for 1986-67. The tablewas constructed by analyzing the MOH budget contained in the GOZ budget'blue book" for that year, which utilizes standard expenditure categoriesnot very amenable to functional anal'sis. This explains the large amountclassified as "other". The blue book also includes some items (furniture,medical equipment, minor construction) which are capital rather thanrecurrent in nature. Nevertheless, the table shows that about two-thirds ofthe total MOH budget of Z$ 240.6 million was spent on salaries, reflectingthe labor-inteDsive nature of the health sector. In fact, this salaryfigure is relatively low when compared to a number of other Africancountries, and suggests that the balance between salaries and non-salaryrecurrent expenditures (drugs, transport, maintenance, etc.) is fairlygood. The budget shares alloca,ed to drugs (102) and transport (2.22) arealso relatively high in comparison with other African countries. Thisfunctional analysis is corroborated by a 1986 WHO-sponsored study ofGoromonzi District, which revealed that 602 of health expenditures went tosalaries and 92 to medical and surgical supplies.
TABLE 11-4
ZRIABWECuosmtlon of MOH Evenditures, 1986 - 87
Categor) 86-87 86-87Amount Percent Budget Reference
(ZSm !llon) (X)1. 3ataries
- MOH Adninlstratlon 8.36 3.47 vote IA- 10H Medical Services 83.02 34.50 vote IIA- WH Preventive 15.30 6.36 vote IIIA- MH Research 0.96 0.40 vote PJA- MOH Grants 33.78 14.04 2/3 Y U,IE,iH,Il11-r. lrenyatwla 19.89 8.27 V3 of IIF
Mbtotal 161.32 67.05
2. DLs/DressIngs 23.70 9.85 votes lID, IIE, IIF3. FrnIturelEqulent 7.48 3.11 varlous votes4. &,sistence/Transport 5.31 2.21 votes l-IVB5. Constructlon 1.50 0.52 votea IIE, IIIE6. Otr 41.30 17.17 varIols votes
Total 240.60 100.00
Sources:(1) Govemnment Budget, 1987-88.(2) Monthy Fnanclar Reports, Parirenyatwa Hospital.

-13-
2.10 Allocations by Level and Tspe of Service. Further analysis of theblue bonk suggests that about 712 of the 1987 MOH budget (Z$ 171.3 million)was allocated to facility-based health services, with the balance of fundsfor community-based programs (water and sanitation, disease controlcampaigns, etc. - llZ), traininR (102), central administration (5Z), grantsto ZNFPC (2Z), and research (1Z).
2.11 If the expenditures incurred by municipal and local governmenthealth authorities using their own re3ources are added to the MOH budget,then total public outlays for facility-based services come to Z$ 188.2million; this is the so-called "patient budget for GOZ health care. Ofthis amount, nearly 50? (ZS 93.5 million) was spent at tertiary level,including 36? (Z$ 67.4 million) at the four central hospitals and 12? (Z$21 million) at provincial hospitals. About 30? of the patient budget (Z$56.4 million) 1?as allocated to secondary-care facilities, including the 55district and mission hospitals, with the remaining 20X (Z$ 38.3 million)spread across the roughly 1000 urban and rural clinics at the primary-carelevel.
2.12 As Table II-5 and Figure 2.2 show, the distribution of Governmenthealth facilities by province, as measured by hospital beds per 1000population and clinics per 10,000 population, is fairly equal. However, therer capita distribution of public financial resources for health is 2-5times higher in the two provinces where the four central hospitals arelocated (Mashonaland East - Z$ 48, and Matabeleland North - Z$ 33) than inthe other six provinces (Z$ 10-15 per capita). Even when these figures areadjusted to take into account patients referred from the other provinces tothe central hospitals in Harare and Bulawayo, per capita expenditures inthe two 'urban provinces are still 1.4-2.7 times higher than in theothers.
2.13 This top-heavy allocation of financial resources, while common indeveloping countries, indicates that while much has been done sinceindependence to correct the urban, high-technology bias of Zimbabwe'shealth system, that bias still persists to some degree. Data on the averagecost per patient-day at various levels of health facilities confirms thisbias. The Government has already taken a number of positive steps toimprove the 'ituation: (a) new construction at the central hospitals hasgenerally been halted since the early 1980s; (b) district hospitals andclinics are being built or upgraded to relieve pressure on the tertiary-level facilities; and (c) MOH is implementing regulations requiring thatyoung doctors serve in the rural areas, while providing incentives (e.g.,good quality housing) to health personnel to work outs.ade of the majortowns. In addition, the GOZ may wish to consider several other measuresdesigned to reallocate resources to lower levels of the health system,including improvements in referral procedures and a fee structure thatencourages patients to seek care at the appropriate level. Costs at themajor hospitals could also be better contained if these facilitiesdeveloped effective financial information systems for use by senior medicaland administrative staff (see Chapters IV and V).

-14-
FIGURE 2.2:
Summary Data on Health Services byProvince, 1987
40 38
30 -- 226~~~~~~~~22
Health 19Expenditure per 20 18 _ _
Capita (ZS) 114 1 4
1 0
0-Manic Mash Mash Mash Masv Mat Mat Midis Nat'l.
Centr East West Nrth Sth Avg.Province
* Number of Clinics per3.0 10,000 Population
* Hospital Beds per2.5 - 1,000 populatlon
2.0,
1.5
1.0
0.5
0.0Mani Mash Mash Mash Masv Mat Mat Midis Ndt'l.
Centr East West Nrth Sth Avg.Province

-16-
TABLE II-6
ZIMBABWESummary Date on Health Services by Province, 1997
Numberof
Health Hospital Clinics Hospital OutpatlentExpenditure Beds per per Admissions HospitalPer Capita 1.000 10,000 per 1,000 Attendance(Zs) Population Population Population per Capita
(A) (9)1/ (A) (B)2/ (A) (B)2/
Manicaland 14 18 2.0 2.1 1.6 60 64 0.9Mash Central 12 16 1.6 1.6 1.2 59 67 0.7Mash East 48 88 2.0 1.8 1.0 82 71 0.6Mash West 10 14 1.4 1.4 1.0 61 67 0.9Miwvingo 10 16 2.1 2.2 0.9 66 70 1.3Mat North 33 26 8.1 2.9 1.3 92 80 0.7Mat South 10 14 2.3 2.4 1.3 66 74 0.9Midlands 15 19 2.2 2.3 1.6 63 67 0.9Nati. Average 22 22 2.1 2.1 1.2 70 70 0.8
Soyrce : MOH service and expenditure data.
Notes
1/ In version (8), the data have been adjusted for the 20% referral rate and this share ofexpenditures of the central hiepitals Is apportioned on a population-weighted basis.
2/ Version (B) distributes national referrals of central hospitals equally to all provinces,i.e. 20X of beds and admissions are national referral and are distributed equally amongthe provinces.
2.14 Government Capital Expenditure. Table II-6 contains a time serieson capital outlays for health between the years 1982-88. Capitalexpenditures for health appear in four different sections of the GOZ budgetblue book: (a) funds for equipment and minor construction financed out ofthe MOH budget using domestically-generated revenues (MOH Vote); (b) donorfunds for a range of health programs of a non-building nature, e.g.,immunizations, water and sanitation, health training, which are channeledthrough the Ministry of Finance's Vote of Credit (VOC-Health); (c) fundsfor major building projects for health undertaken by the Ministry of PublicConstruction and National Housing on behalf of MOH (MPCNH/MOH), usingdomestic resources; and (d) donor funds for health buildings put up byMPCNH on behalf of MOH, and thus channeled through the Vote of Credit (VOCMPC/MOH).
2.15 The figures in Table II-6 show a dramatic increase in capitalspending for health during 1982-88, reflecting the expansion of a range ofprimary health care-related programs (especially the Essential Drugs ActionProgram (ZEDAP), the Expanded Program of Immunizations (ZEPI), rural watersupplies and latrines, and training of PHC workers) and the implementationof projects to build multi-disciplinary health training centers, district

-16-
hospitals, and clinics in rural areas. While the local contribution to thecapital budget has generally remained constant in absolute terms, it hasdeclined relative to foreign financing, which accounted for three-quartersof the budget in 1987-88. Capital expenditures for health can be expectedto cintinue rising over the next 5-10 years, particularly in connectionwith the Z$ 80 million upgrading and equipping of eight district hospitalsand 70 clinics tmder the World Bank-assisted Family Health Project.
TABLE II-6
ZIMBABWECapital Expenditures for Health, 1982-88
(Nominal Z$ millions)
Ya 1/ VOC/ 4/ Foreign ShareYear Vote Health 2/ K PC/m 4 Total M
1982-83 14.9 1.3 n.a n.a. 16.2 8.01983-84 5.1 3.0 n.a. n.a. 8.1 37.21984-85 7.8 7.1 1.2 7.2 23.2 61.61985-86 14.3 8.6 4.6 9.3 36.8 48.51986-87 9.0 8.2 7.3 7.5 31.9 49.81987-88 5.7 15.6 8.0 25.0 54.3 74.8
Sotsce: MOH Documents
Notes
(1) MOH Vote: Capital items irclude fumiture and equipment and capital items covered by theMOH grant to councils and missions.
(2) VOC Health: Vote of credit for MOH, i.e., donor-assisted health projects, largely capital incontent. ncluding EPI, CDD, water and sanitation.
(3) MPCNH/MOH: Ministry of Public Construction vote on behalf of MOH. This covers buildingconstruction projects fully-funded by GOZ.
(4) VOC MPCIMOH: Vote of credit to Public Consruction on behalf of MOH. This covershealth construction activities managed by MPCNH and foreign-funded, e.g., district hospitalsunder the Family Healh Project.
n.a. Not available.
2.16 Capital spending for health since independence, with its strongorientation toward preventive health activities and improvements offacilities in the rural areas of the country, has helped to redress some ofthe earlier imbalances in the distribution of health-related benefits inZimbabwe. However, given the persisting urban bias and the fact that mostprivate doctors are located in the towns, the emphasis on MOH capitalexpenditures for PHC and rural facilities should probably continue for some

-17-
years to come, provided that the central and provincial Governmenthospitals are adequately mdintained.
2.17 However, in focusing on these areas of investment in health, theGOZ will need to consider three important issues:
(a) Planned capital expenditures should be related in a realisticmanner to che implementation capacity of the responsibleinstitutions. Technical and managerial staff in MOH, for example,are currently in short supply. This may soon begin to frustrateimplementation of some PHC programs, unless additional capacity iscreated; similarly, there is increasing evidence that shortages ofarchitects, engineers, and transport in MPCNH may be constraininghealth civil works projects. This situation highlights theimportance of creating additional capacity in MOH and otherGovernment agencies, through measures to improve both the supply(training and technical assistance) and demand (competitive civilservice salaries and attractive terms and conditions ofemployment) for these critical skills;
(b) Current technical specifications for major capital investments,especially new and upgraded buildings, should be carefullyscrutinized, to ensure that the most cost-effective technicalsolutions are being followed. This is especially important in thecase of standard civil works which are repeated over and overagain in many locations, e.g., district hospitals and clinics, andwhere cost reductions for relatively minor items (e.g., size ofwards, examination rooms, choice of building materials, etc.) canultimately result in major savings overall. It would be useful forMOH to review these technical specificaticns periodically, withassistance from outside architects if necessary, and revisetechnical standards as required; and
(c) The financial sustainability of the recurrent costs associatedwith capital expenditures should be closely monitored, and theseadditional costs should be fully budgeted. This issue is examinedin more detail in Chapter V.
i

-18-
CHAPTER III
ISSUES IN RESOURCE MOBILIZATION
Introduction
3.01 As mentioned in the previous chapters, since independence, theGovernment of Zimbabwe has backed up its pledge to provide adequate healthcare for the population by committing a significant level of resources tothe health sector. The share of national wealth allocated to healthcompares well with other countries at a similar stage of economicdevelopment. However, given the constrained macroeconomic situation andrelated budget austerity, Government officials recognize that it isbecoming increasingly difficult to allocate sufficient public funds,obtained from general revenues, to the health sector to keep up with thedemand for an expanded array of high-quality services for a populationgrowing at over 3Z a year. Unless other sources of financing can be tapped,both for public and privately-provided health care, the Government willfind it hard to maintain current service levels or continue its efforts tocorrect inherited imbalances. Creative solutions are required not only tostretch Government's expenditures further, but also to mobilize additionalresources.
3.02 In searching for solutions, one of Zimbabwe's strengths to beexploited is the current diversity of providers and sources of funding forhealth. As discussed in Chapter II, Government health institutions atpresent utilize general tax revenues, local taxes, insurance payments, anduser fees; NGO institutions rely on a combination of public subsidies,fees, and donations; employer health institutions (industries, mines, etc.)fund services out of internally generated revenues; and private providersreceive out-of-pocket payments from clients and insurance payments. In thesections below, some options for further developing existing sources offinancing, as well as for creating new mechanisms, are examined. Theseinclude: increasing user fees for public health services; private andgovernment insurance; local government cost-sharing and communitycontributions; and taxation of privately-provided health care.
3.03 Ae Zimbabweaa officials review the historical pattern ofexpenditures for health and consider options for the future, they may wishto assess these options in terms of a series of key criteria:
(a) financial impact: what level or amount of additional resourceswould result if the option were adopted?
(b) reliability and robustness: can the financing mechanism becounted on from year to year, or will it suffer year-to-yearshocks in response to changing circumstances? Will funds increaseover time to satisfy the needs of a growing population?

-19-
(c) efficiency: will the financing measures enhance the technicalefficiency of expenditures?
(d) equity: will the proposed option improve the distribution ofhealth benefits among the population, and ensure that even thepoorest groups have access to a basic minimum of health care?
User Fees for Government Health Services
3.04 Policy and Achievements. Following independence, the GOZarticulated its policy of making the distribution of health services inZimbabwe more equitable. Consistent with this policy, the GOZ decided thatpublic sector health institutions would provide care free of charge to thepoor. Consequently, families with monthly incomes of less than Z$150 havebeen exempt from paying fees since shortly after independence (September1980); this cut-off line has not been adjusted since 1980. For thosehouseholds above the cut-off line, the GOZ has established a schedule offees for MOH facilities, differentiated by household income and level offacility. Current charges, which have been in effect since 1985, include:
(a) for each of the four central hospitals' general wards, aninpatient fee, ranging from Z$5 to Z$35 per day depending uponincome, with aubscribers to medical aid (health insurance) chargedat the highest monthly income rate (i.e., Z$ 800 or more);
(b) f.or the central hospitals' private wards, a fixed inpatient feeof Z$60/day;
(c) at the provincial and district hospitais, a daily flat rate forinpatient care of Z$10 in general wards and Z$35 in private wards(halved after 14 days of hospitalization);
(d) an outpatient fee, which at the central hospitals is eitherZ$5 or Z$13, depending on income and insurance coverage, and isfixed at Z$3, Z$1.5 and Z$1 at the provincial, district and ruralhospitals, respectively. regardless of household income; and
(e) additional charges (not income-linked) for specific procedures,e.g., operations, injections, wound dressing, etc.
3.05 At all facilities, fees for children are lower than those quotedabove, while non-residents pay more. Both inpatient and outpatient feesinclude the cost of any drugs and supplies used in treatment. While therural and district council clinics and church mission hospitals also adhereto the MOH fee schedule, municipal health care institutions are notgoverned by the MOH fee structure, other than the exemption for poorhouseholds. The municipal health authorities set their own fees, subjectonly to the fee schedule being published in advance without receiving 20 ormore formal complaints from citizens.

-20-
3.06 For a number of reasons discussed below (low level of fees,difficulties in establishing correct charges in relation to income, weakcollection efforts, etc.), cost recovery from user fees in Governmenthealth facilities is very low, amounting to only 2-4Z of the MOH recurrentbudget during 1981-88 (Table III-1). Excluding one of the centralhospitals -
TABLE Illl-
Z3ABEMinistry of Health Cost Recovery, 1981 88
tSI uW)
Fee Collections Cost Recovery Ratios
TotalMOH Off fhih Of Uhlh
Baxbet Parlrenyatva Total Parkvruyatnw tinal ParrnyatnaYear (1) (2) (3) (4) (5)A(3)/(1) (6)-(4)/(2)
1981-82 108,936 16,344 3,975 2,326 3.61 14.211982-83 130,3C0 18,262 3,559 2,158 2.7S 11.811983-84 137,615 20,218 4,361 2,881 3.21 14.211984-85 131,374 22,784 5,594 3,464 4.31 15.2X1985-86 196,200 28,845 4,990 2,230 2.51 8.311986-87 240,600 32,822 5,730 3,000 2.41 9.111987-88 281.700 34.000 7,755 3,450 3.0X 10.11
Sauce:
Mink"y of Health and Padrirenyatwa Group of Hospitals.
Parirenyatwa - where collected fees during this period covered 8-15Z ofexpenditures, cost recovery has met less than 2Z of MOH outlays. On theother hand, municipal health departments recover a significantly largershare of their expenditures - varying from 10-30Z - in part because theirurban clientele is able to pay more (Table III-2), but also because cityhealth authorities have the incentive of knowing that MOM subventions willonly meet a portion of their total costs.

-21-
TABLE 11-2
ZIIABWEcost Recovery for &tnrdoaI Goverrumnt
(i!W i S UI1)
HUtrent fe8 WSt KscCVeryI t ExpendIre Collected Ratio
Bulawayo 3,490.5 556.6 16.2130.9 7.9 25.7X
Ch nh =yi64.0 19.0 29.7XChItiawIza 2,568.6 367.8 14.31Gveru 1,025.0 171.4 16.7XHarare 16,201.2 2,447.9 15.1XKadoma 178.7 43.4 24.31Kwekwe 364.6 88.6 23.8SMarondera 272.7 30.3 11.1lMasvIrao 266.1 32.0 12.01Mutare 1,088.9 174.9 16.0C
Sounre: Municipal Govemmefts Annual Reports.
3.07 Issues Concerning User Fees. Zimbabwe Government officialsgenerally recognize the weaknesses of the existing system of cost recoverythrough user fees: the level of cost recovery is '.oo low, and the systemdoes not effectively target users according to ability to pay, i.e., somepersons who are exempted could afford to pay at least a small fee, andothers who could meet most or all the costs of their care are beingundercharged.
3.08 There are a number of reasons for low cost recovery. First, thelevel of fees is set too low, in relation to actual costs and toindividuals' willingness to pay. While the actual cost of providing varioushealth services has not been systematically studied, it appears that eventhe maximum fees charged are well below full cost: for example, private in-patient care at Parirenyatwa is estimated to cost Z$ 100-150 a day, whilethe rate for private patients is only Z$ 60. The overall MOH fee schedulehas not been adjusted since 1985, even though inflation has averaged 10-20Za year during 1985-89: this has seriously eroded the real cost of usercharges. There is also strong anecdotal evidence (high out-of-pocketpayments to private doctors, pharmacies, and traditional practitioners) tosuggest that many Zimbabweans would be willing to pay more for reasonablequality health care.
3.09 Second, the revenue collection efforts of MOH, local government,and church mission health facilities are generally poor, in part becausethey lack incentives to collect fees, and also because trained accountingpersonnel are scarce. It 1s not known how much revenue is lost in thismanner, but probably amounts to Z$ 5-10 million a year or 2-4Z of MOH -
expenditures. The provincial hospitals collect some fees, but lack ofregistration and billing information and inability to enforce payment oftenresults in lost revenues: it has been estimated, for example, that 502 ofambulance fees are never collected. The tertiary care hospitals are

-22-
generally stricter in imposing fees, but the central government computerbureau is very slow in sending bills to patients, often taking 9-12 monthsafter the patient is discharged. As a result, MOH may be losing as much asZ$ 10-20 million annually in potential medical aid payments for privatecare in these referral hospitals.
3.10 Poor fee collection can be partly related to the lack of skilledfinancial managers and clerical staff at all levels cf health facilities.The relatively sophisticated skills required at secondary and tertiaryfacilities to apply successfully the variable fee schedule scaled tohousehold income are frequently unavailable. The fee collection proceduresthemselves tend to weaken cost recovery: hospitals do not alwavs presentin-patients with their bills before they are discharged, and patients whoare billed prior to discharge are not required to settle thei. accountsbefcre they leave. The tertiary hospitals' reliance on the highly-centralized and overworked computer bureau is also a factor. In addition,since the annual MOH budget allocati-ns and subventions to individualfacilities are not affected by their cost recovery performance during theprevious year, MOH, local government, and mission health facilities havefew incentives to strengthen their fee collection efforts.
3.11 Third, cost recovery is low because the curre-nt system forgranting the exemption from paying fees is very difficult to apply. Exceptin some of the MOH central hospitals and municipal facilities, patients canqualify for the exemption on the basis of an uncontestable verbalstatement, without having to document their income level. Monthly pay slipsare generally used as the only valid proof of income; and as only a handfulof persons in the rural areas (school teachers and other civil servants)receive a monthly wage, virtually everyone else is exempted from payinguser fees, even if their cash and in-kind income is actually above the Z$150 cut-off. It is therefore likely that large numbers of households withincomes above this level are receiving free health care. By contrast, inthe MOH central hospitals and municipal health facilities, where the burdenof proof of income - and possible indigence - is placed upon the patient,in the form of pay slips or a letter from the local social services agency,cost recovery is significantly higher.
3.12 Another weakness of the current cost recovery system, widelyacknowledged by Government officials, is its ineffectiveness in targetingfees to various socio-economic g:oups. In this sense, the system is notfully consistent with the Government's equity objectives. As mentionedabove, while the truly needy may receive health services free of charge,others who can afford to pay something are also benefitting from free care.In addition, because the highest income groups (including medical aidpatients) are not being charged the full cost of the care they receive, anda large portion of thc'e charges is not being collected, the Government iseffectively providing a large subsidy to these groups who could afford topay considerably more. Furthermore, the Government's failure to collectfees from higher income groups may ultimately be constraining its abilityto invest iu new facilities, manpower, drugs, etc., especially to servepoor rural communities.

-23-
3.13 Poor fee collection at the secondary and tertiary hospitals mayalso be compromising the efficiency of the health referral system. Bycharging more at higher level facilities, the current fee structure notonly approximates relative costs at those facilities; theoretically, such astructure should also encourage patients to seek care at the appropriatelevel of the referral system, without by-passing lower-level facilities.However, failure in practice to collect fees at provincial and centralhospitals may be one factor in the relative underutilization of peripheralfacilities - as measured by lower occupancy rates and longer length of stayfor in-patients at peripheral facilities - as compared to the higher levelhospitals.
3.14 Options for Increasing Cost Recovery. In many developingcountries, there are strong arguments for governments to provide certaintypes of health services to some groups at less than full cost: theseinclude equity considerations and the externalities associated with manypreventive health programs, e.g., infectious disease control, familyplanning, etc. The appropriate level of cost recovery will also vary fromcountry to country, depending on average household income, distribution ofincome among groups, and the income profile of those served by governmenthealth facilities (as opposed to the NGO and private sectors).
3-15 Nevertheless, most Zimbabweans recognize that cost recovery forhealth care is too low at present, and that measures to increase costrecovery are feasible in terms of ability and willingness to pay more. Itis generally acknowledged that most people (with the exception of low-income households which would have to be protected) would be willing to paymore for good quality health services: the fact that Zimbabweans incursubstantial out-of-pocket expenditures for payments to traditional healers,private practitioners, and private sellers of drugs, attests to thiswillingness to pay. While Government officials would ultimately need to setnew cost recovery targets themselves, an overall level of 15-20? of MOHrecurrent expenditures would seem attainable, especially as several othercountries with lower per capita incomes (e.g., Ghana, Lesotho) have managedto achieve cost recovery of this magnitude in recent years.
3.16 Zimbabwe faces a number of possible options with regard to userfees, that could help to increase cost recovery, promote greaterefficiency, and improve equity in access to health care. These optionscould be adopted individually or severally, depending on various politicaland administrative factors; however, the impact of many of them will begreater if adopted in tandem with other complementary options, e.g., therevenue effects of new or increased fees will be significantly enhanced byimprovements in billing and collection procedures. The options for new orincreased fees include:
(a) raising the overall level of fees in Gover.ament institutions. At aminimum, this might involve bringing fees, which were lastadjusted in 1985, back into line with price inflation over thepast four years;
(b) increasing fees for private patients (mainly covered by uiedicalaid) to cover full, or most, actual costs. While such fees could

-24-
be boosted immediately to bring them into line with charges incomparable private hospitals, a detailed study of the actual costsof various health services at different facility levels would needto be undertaken before fees could be calibrated precisely inrelation to costs;
(c) charging a small nominal fee for out-patient visits at allGovernment health facilities. Such a measure would help tosimplify the administration of out-patient fees, which currentlyinvolves scaling charges to household income and assessingeligibility for exemptions. Experience from other countries alsoshows that nominal out-patient charges can improve efficiency byeliminating much (medically) unnecessary treatment, while stillensuring that the poor are not denied access to out-patientservices they need;
(d) starting to charge separately for all drugs provided to out-patients and to those hospitalized. To preserve equity, a simple,three-tiered system of pricing for drugs might be envisioned: fullcost for those covered by medical aid, free or nominal charges for athose able to demonstrate their low-income status, and low (lessthar, full cost) fees for all others.
3.17 In addition to the above changes in the level and structure offeet, a number of management improvements are also possible. These optionsinclude:
'e) requiring that, in the case of in-patient care, the burden ofproof of income (and the related scaling of hospital fees toincome level, as well as exemptions from fees for the poor) beplaced upon the patient (see para. 3.11), rather than thehospital. In addition to pay slips or income tax returns, a letterfrom social services agencies or from the local authority(council) could also be used as proof of income status. In urbanareas, this should not create excessive difficulties. In the ruralareas, where it may be more problematic to establish householdincomes precisely, marketing board receipts or other relevantdocumented criteria, e.g., size of landholdings, could possibly beused to determine a patient's ability to pay. Another option toexplore for the rural areas would involve establishing a set ofcriteria known to be closely related to households, ability to payfor health services, based on the results of recent householdexpenditure and income surveys. These criteria might include,e.g., number of persons in household, number employed, size oflandholdings, type of dwelling, etc. Admissions clerks could theninterview patients upon their arrival at the hospital, askingquestions derived from the survey data. Patients meeting acertain number of the income criteria, and therefore judged to befrom low-income households, would then have hospital fees waived;
(f) improving billing and collection procedures. Government-operatedor subsidized facilities should strive to present bills topatients and collect fees upon discharge, as a routine matter. Adeposit could also be required of patients upon admission. This

-25-
may require hiring and training additional managerial and clericalstaff, and automating billing and other accounting systems. Animportant first step in this direction would be to decentralizebilling and fee collection at the four national referralhospitals, including the installation of micro-computer systems,in order to stem the enormous loss of potential fee revenues. Theongoing MOH initiative to train and deploy health administratorsto the provincial and district levels could also help in thisdomain, as one of the administrators' chief responsibilities wouldbe to strengthen revenue collection; and
(g) developing incentives to individual health facilities tostrengthen their revenue collection efforts. A range of approachesto providing such incentives can be envisioned, and MOH may wishto consider their appropr.ateness under Zimbabwe conditions. Areasonable target level of recoveriec could be set for eachinstitution, with MOH then allocating the remaining funds to meetan approved overall budget and each institution retaining for usethe fees collected; this is the system currently in use in Ghana.Alternatively, institutions reaching or exceeding their costrecovery targets could be given extra funds or other benefits(e.g., new uniforms, equipment, transport, etc.), in addition totheir normal budgets; this approach is being adopted in Lesotho.What is required is for MOH and other Government officials toreview these various incentive schemes, in the light of GOZaccounting procedures, institutional capacity, and health workers'and communities' preferences, and identify the most appropriateapproach.
3.18 While it is difficult to quantify precisely the financial impactof these user fee reforms, the adoption of all the above measures couldresult in increased revenues of about Z$ 40-55 million a year, including Z$7 million from adjusting fees in line with inflation, 2$ 15-20 million fromfull cost pricing for private patients, Z$ 10 million from out-patientfees, and Z$ 10-15 million from drug charges. The sum of these incrementalrevenues would be equivalent to 15-20? of the 1188 MOH budget. Of course,the costs of collection (for ext.a staff, equipmenL, etc.) would have to beset off against the additional revenues gained. For this reason, it wouldbe critically important to make the changes in the user fees system ascoat-effective as possible, by adopting the management reforms indicated inpara. 3.17.
Private Health Insurance
3.19 Background. Medical aid societies (non-profit health insurancecompanies) have been present in Zimbabwe for many years. There arecurrently about 30 such companies, serving both public and private sectoremployees, under the umbrella of the National Association of Medical AidSocieties (NAMAS). About 380,000 employees and their dependents arecurrently covered, representing about 4.6? of the population, up from about220,000 at the time of independence (Table III-3). Although severelyunderrepresented at independence, black employees now account for about 702of those covered. The three big medical aid societies (CIMAS, Public

-26-
Employees, MASCA) account for 85-90Z of subscribers covered, with CIMAS andMASCA accepting members from any type of private firm; the smallersocieties generally serve a single firm or induscry. Only CIMAS offers ahealth insurance package for individuals.
TABLE 111-3
ZNVIEMedical Aid Socleties mbershl, 1981 - 87
vmDersnp Amal wurowtnYear (000) (X)
1980-81 224.14 -1981-82 240.05 7.11982-83 268.61 11.91983-84 292.97 9.11984-85 315.56 7.71985_86 346.67 9.91988-87 384.05 1(.8
SOeX. NAMAS
3.20 Government policy has been to allow medical aid societies toconduct their own affairs, without regulation. Monthly premiums aredetermined by the societies themselves, 'jith the relative contributions ofemployees and employers decided by the firms involved. The levels of suchpremiums are scaled according to employees' income and number ofdependents. NAMAS negotiates directly with private physicians in ssttingfees to be paid by the medical aid societies for various recogniz(-6 medicalprocedures, which are then published in a Relative Value Schedule. NAMASalso negotiates the fees to be paid to GOZ hospitals for medical aidmembers admitted as in-patients. While these hospitals charge higher ratesfor those covered by medical aid (who use private wards, if available),such rates remain well below cost, with the result that the GOZ effectivelysubsidizes private care in public facilities.
3.21 Most medical aid subscribers are treated by private physicians,located mainly in the large towns of Harare and Bulawayo. As there are fewprivate hospitals in the country, the Gove-nment allows most privatephysicians to admit their patients to public hospitals, principally thefour big central hospitals, where the patients go into private wards.Despite the heavy use of Government facilities by medical aid members,Government received only about 3.5Z of all medical aid payout in 1987,because of both low overall fees and inadequate billing and collection (seepara. 3.09). Most medical aid payments go to private doctors and dentists(491), private hospitals, nursing homes, laboratories and x-ray services(26Z), drugs (18Z) and out-of-country referrals (42, Table III-4). Medicalaid generally pays directly to health care providers rather than throughreimbursement of the patient. The one exception is for drugs, where themember is reimbursed a portion of the cost, various levels of co-paymentbeing applied. There are no other co-payments or deductibles included inthe medical aid societies' policies.

-27-
TABLE 11H4
CIMAS, MASCA, and Ralkied bdka! Aid Societiesuqbenitwues tor meait! care, IW.-! ana 198587
1982 - 83 1986- 87
Amwt Sharo of Amont Share of(Z$ million) Total (Z$ milliom) Total
Payments To/For (X) (S)
T. mistry ot mealth IX b.l7 1. 3.b2. Gemal Practitiners 4.21 18.8 9.89 2t.S3. Spclalists 4.88 21.7 8.56 17.84. Dental Practitiones 2.63 11.7 4.89 10.25. Private Hospitals/
zrskl H mem 2.02 9.0 7.32 15.36. PrIate LaboratorIes 2.01 9.0 3.10 6.57. X-Ray ServIces 0.91 4.1 2.21 4.68. Out-of-Cotmtry Referrals 0.73 3.3 1.70 3.59. MrLs 3.77 16.8 8.65 18.0
Total 22.45 100.0 48.00 100.0
Soum CIMAS, MASCA, and Railmed.
3.22 Issues and Options for Medical Insurance. Policy-makers inZimbabwe recognize that the main issues concerning private insurance(medical aid) include: (a) estimating the potential for increasing thenumber of persons covered by such insurance, and the related rise inresources devoted to health care; (b-) predicting the impact of expandingmedical a4d upon the cost and quality of health services provided by thepublic sector; and (c) determining whether some of the existing features ofmedical aid schemes are inequitable and should therefore be corrected.
3.23 While the population covered by medical aid has nearly doubledsince independence, it still amounts to less than 5Z of all Zimbabweans.How much larger can the medical aid clientele grow? The largest medical aidsocieties estimate that there is a "market" consisting of an additional 0.6million persons who could be covered by private health insurance. Thiswould bring the total number of subscribers to about 1.0 million or llZ ofthe country's population. Presumably, in order to saturate that market,medical aid societies would have to seek new customers aggressively,something that the industry-specific insurance schemes have nothistorically done. The Government could be instrumental in supporting thisprocess, in part simply by encouraging firms and their employees to entermedical aid schemes, but also by requiring through legislation that allemployers over a czrtain size provide a minimum level of health benefits totheir workers. This would force these employers to establish their ownhealth services (workplace clinics, etc.) and/or enroll their workers inmedical aid programs.

-28-
3.24 While the full potential market for medical aid is difficult toestimate precisely, it does appear that private he'ith insurance couldexpand considerably beyond its current clientele base. Zimbabwe's medicalaid industry is well organized and staffed; NAMAS provides the varioussocieties with a common front in negotiating fees with private doctors. Inaddition to the political and legislative actions mentioned above, twoother factors are likely to affect the cost of medical aid coverage and itsrelated affordability for middle-income households. The first factor is thelevel of Government subsidies to health care covered by medical aid: ifthese subsidies were reduced by charging full costs in public hospitals andcutting the income tax credit for individual contributions to medical aid -the cost of private insurance would almost certainly increase, with acorresponding fall in demand. However, as the average annuai premium paidat present (around Z$275 per beneficiary) is low relative to wage incomesin Zimbabwe, the market could probably absorb a rise in premiums without asignificant drop in demand. The second factor is the share of medical aidpremiums borne by the individual and his employer: if employers assumed alarger percentage of these costs, more middle-income workers could affordmedical aid coverage. On the other hand, some of these costs wouldultimately be passed on to consumers in the form of higher prices forvarious goods and services. Some amount of switching from relatively iabor-intensive production methods to more capital-intensive ones might alsooccur.
3.25 The impact of expanded m-dical aid upon MOH revenues is hard toquantify exactly, but is likely to be positive, assuming that billing andcollection procedures at the major hospitals are strengthened. This i-because a large number of middle-income households who previously paialittle or nothing for in-patient care would be charged at a higher(possibly full-cost) fee level, with virtually no reduction in demand forhospitalization from this group. Revenues for out-patient services wouldalso rise, even if some of the new insurees went to private doctors forsuch care, since it is doubtful that they pay for out-patient visits atpresent.
3.26 The likely impact of expanded medical aid upon the overall qualityof Government health services is more controversial. One concern voiced bysome Zimbabweans is that growth of medical aid membership would expand themarket for private health care and thus cause many doctors and nursescurrently working for the Government to leave public service for privatepractice. This, in turn, would lead to a deterioration in the quality ofpublicly-provided health services. Notwithstanding the fact that atpresent, about two-thirds of Zimbabwe's 1200 doctors are already in privatepractice, it is possible that the expansion of medical aid might inducesome additional doctors to leave the public sector. The Government doeshave at its disposal, however, a number of policy options that couldcounteract such a drift to the private sector:
(a) pay and conditions of service (housing, allowances, careerdevelopment opportunities) can be enhanced in order to attract andretain more doctors and nurses;

-29-
(b) young doctors graduating from Zimbabwe's medical school can berequired to searve in the public sector for a minimum period beforebecoming eligible for licensing as a private doctor. This periodof public service has recently been increased to eight years(three years of housemanship and five years of additionalservice); and
(c) private doctors' rights to admit and attend to their privatepatients in MOH hospitals can be made conditional upon theirwillingness to treat general patients (e.g., at clinic sessions)at public sector pay levels. This system, which currently operatesat all the major hospitals, could possibly be further expanded.
3.28 Another issue related to medical -Ad is the equitability orfairness of some of its current feature., aside from the possibility,discussed above in para. 3.27, that it creates an unfair "double standard"of care between the private and public sectors. It has already been arguedin this chapter (para. 3.20) that medical aid patients do not pay the fullcost of the treatment they currently receive in MOH facilities, and this isinherently inequitdble. In addition, medical aid patients obtain animportant tax benefit, in the form of a deduction from income liable forpersonal income tax, amounting to 20? of their medical aid contributionsand other out-of-pocket medical expenses. (Employers can also deduct fromtaxable company profits the contribution they make to their employeesmedical aid scheme). Prior to the 1988 reform of tax legislation, 1002 ofindividuals' medical aid contributions were deductible. In this sense, ameasure of greater equity has been introduced as a result of the recent taxreform, and it is unlikely that further changes will take place in the nearfuture. However, inasmuch as even a partial deduction against taxes isallowed, this should be recognized as a public subsidy to private medicalcare for the better-off income groups in Zimbabwe.
3.29 One final issue is that the lack of any co-payment or deductiblerequirement by Zimbabwean medical aid societies, except for somepharmaceuticals, has probably contributed to an unnecessary increase indemand for health care by their clients. This is because they are not facedwith additional costs per unit of care consumed. The NAMAS member societiesmight look more carefully at options for introducing co-payments anddeductibles if they faced the full costs of Government-provided care, andif other existing subsidies were reduced further. Higher costs to medicalaid societies and individual members would help restrain demand for privatecare, and thus ease somewhat the pressures on Government doctors to shiftto private practice.
Government-Operated Health Insurance
3.30 Background. In 1985, Government began exploring the possibilityof introducing a public-sector "National Health Insurance Scheme" (NHIS)tied to a new social security system. Participation in the scheme would be

-30-
compulsory for all salaried workers. Several variants have been drafted anddiscussed by MOH, Ministry of Labor and Ministry of Finance. The proposalsgenerally include the following features:
(a) the scheme would be financed through payroll deductions amountingto 2.5Z of salaries, contributed partly by employees (1X) and byemployers (1.5x);
(b) these payroll deductions would be additional to those required forthe proposed social security system run by the Ministry of Labor,for which legislation is pending;
(c) the insurance "premiums" would be earmarked for public healthservices, and would be additional to the "normal" MOH budget;
(d) contributors and their dependents would present cards atGovernment health facilities, which would entitle them to receivefree care; and
(e) certain groups (e.g., MOH employees, armed forces) would obtainthe free care "benefits" without payment.
(f) those not covered by the NHIS would pay for health services atGoverrment facilities, according to the existing sliding scalewith its exemption for low-income families; and
(g) NHIS would not cover private treatment (i.e., private doctors,hospitals, etc., would not be reimbursed). These costs would haveto be met through medical aid or out-of-pocket payments.
3.31 The variants on this basic proposal have revolved around items (d)and (e) above, and other cost-recovery and demand-restraining measuresintended to enhance the revenue mobilization and efficiency benefits ofNHIS. It has been suggested that the need for insurance cards beeliminated, either by abolishing all fees for health services at GOZfacilities, or, alternatively, by requiring that even NHIS contributors paythe same fees as non-contributors (under these circumstances, contributingto NHIS would not confer a specific benefit). The idea of exempting certaingroups of civil servants from payroll deductions has been criticized asunfair and inequitable. To prevent NHIS insurees from demanding excessivecare, the imposition of some level of fees (or "co-payment") has also beenput forward.
3.32 Issues aLd Options for National Health Insurance. The principalissues surrounding NHIS concern: (a) its political acceptability; (b) netrevenue effects of such a scheme; and (c) the impact of national healthinsurance upon the efficiency of GOZ-provided health care. On the firstissue, there appears to be an increasingly prevailing view amongZimbabweans that taxation of personal incomes is becoming excessive, andthat the planned social security scheme plus NHIS could be financiallyonerous. Private employers have also expressed some opposition to thesocial security system, arguing that it will only add to their costs and,

-31-
ultimately, to the prices they must charge, thus increasing the cost ofliving and making Zimbabwean products less competitive internationally.Such a "tax on labor" might also cause firms to substitute (relativelycheaper) capital for (relatively more expensive) labor in a number ofindustries, thus increasing the level of unemployment in the economy.Whatever the intrinsic merits of NHIS might be, therefore, it may notgather the necessary political support and could have negative socialrepercussions under prevailing economic conditions in Zimbabwe, especiallyif the benefits of NHIS are perceived to be few or none - as the case wouldbe if contributors had to continue medical aid coverage for all privatehealth care.
3.33 When MOH was refining its NHIS proposals in 1986-87, the Ministryestimated that the scheme would bring in about Z$ 80 million in extrarevenues annually, when fully operational. In converting these ideal grossrevenues to actual net revenues, however, a number of factors would have tobe taken into account. These include initial resistance from employers andadministrative weaknesses in collection, which would reduce gross revenuesduring the early years of the scheme, plus administrative costs associatedwith NHIS. Experience from other developing countries has shown that theseadministrative costs can be extremely high, wiping out much of the grossrevenue gain. Related to this, administrative difficulties iu defining theboundaries of a benefitting "household" and its members (simple conjugal orextended family) can result in a higher level of health costs. In addition,if health care at MOH facilities was provided freely to insurees, therewould be both a corresponding loss of revenues from fees that wouldotherwise be collected, as well as incremental costs related to excessivedemand for free public services.
3.34 A fundamental related issue is whether any amount of net revenuesgained through NHIS would actually result in 'additionality' to the MOHbudget, or whether the Ministry's allocation from Treasury would simply bereduced by a corresponding amount. Clearly, this would depend on anyagreements reached between MOH and Ministry of Finance.
3.35 The adoption of NHIS, as proposed, could also seriously compromisethe allocative efficiency of the Government health system, if all insureesreceive free care at GOZ hospitals and clinics. Only a scheme that includedsome form of individual co-payment (through fees, deductibles, or cost-sharing) would transmit price signals to NHIS contributors that would curbexcessive demand for Government health services.
3.36 Virtually all of the NHIS variants mentioned above would improveequity to some degree, even if the net revenue yield was low and there wasno rationing of demand from the higher-income salaried workers throv 'hpositive pricing. This is because the higher-income groups would be payingmore for health: there would thus be greater equity in shouldering thefinancial burden of health care. This same result could also be achieved,however, by increasing fees for medical aid patients, strengtheningcollections, and reducing subsidies that benefit the more affluentdisproportionately. Furthermore, equity in access to health care can onlybe enhanced by investing more in health services for poor urban and rural

-32-
groups. This, in turn, depends on a number of factors not directly relatedto NHIS, including the size of the MOH budget and the budget share spent inunderserved areas. The capacity of local government, NGOs, and communitiesthemselves to finance health care is also critically important.
3.37 Another option in this area - and an alternative to NHIS - thatthe GOZ might wish to consider would be the establishment of a special fundfor improving health services in low-income communities. Such a fund - a"National Health Development Fund' (NHDF) - could be raised throughconsumption taxes on tobacco, alcoholic beverages, etc. Since payrolldeductions would either be passed on to consumers in the form of higherprices or to workers as lower wages, and could also provoke increasedunemployment (see para. 3.32), a tax on alcohol or tobacco (which woulditself have a beneficial effect on health) would probably be moreappropriate. The urgent need for supplemental financial resources forprimary and preventive health activities, as well as the direct linkbetween reduced tobacco and alcohol consumption and improved health status,would argue in favor of an earmarked tax.
3.38 The NHDF, administered by MOH, would only be financiallymeaningful if it were understood as being incremental to the Ministry's"normal" budget. It could then be used for a number of specific healthdevelopment activities targeted at low-income groups, such as clinicconstruction and renovation, drug supplies, and training of communityhealth auxiliaries. While most NHDF projects would be in rural areas, someHNDF activities would also be located in low-income urban neighborhoodswhere health services are currently inadequate. The NHDF could also help tostimulate local participation in health services, by providing grants tomatch local financing according to a cost-sharing formula linked to localincome levels (see para. 3.42 below).
3.39 Establishing an NHDF would not be an easy matter. MOH would haveto negotiate with the Ministry of Finance on incremental budgeting, as wellas on the fiscal merits of such a tax scheme. The GOZ would have to enactlegislation establishing the taxes, and this could meet some politicalopposition. Such opposition might be effectively overcome, however, if theNHDF was to receive high-level political support and was also well-publicized as a fund with basic humanitarian and egalitarian goals, e.g.,"to allow a poor mother to give birth to her child in a basic hygienicplace' or 'to enable a sick child to obtain simple care without having totravel 50 kilometers from his village, as in the past".
Local Government, NGO, and Coimmmity Financing
3.40 Local Government and NGOs. The roughly 700 clinics and hospitalsoperated by municipalities, rural and district councils, and church missionreceive sizeable subventions from the Central Government through the MOHbudget, amounting to about Z$ 36.8 million in 1987. Central Governmentgrants to rural and district council clinics accounted for virtually all oftheir operating costs in that year, while grants to the church mission

-33-
facilities made up about 902 of their recurrent expenses. Themunicipalities were somewhat less dependant on MOH financial support:subventions in 1987 covered 252 to lCd) of their recurrent budgets, with anaverage of about 42Z.
3.41 GOZ officials have recognized several problems inherent in theexisting system of financial relations between MOH and local government andNGO health institutions:
(a) MOH allocations are centralized in the Ministry's head office,which makes it difficult to tailor financial assistance to theparticular needs of individual health institutions;
(b) As there is no defined cost-sharing formula between the CentralGovernment and local health institutions, MOH allocations oftenseem arbitrary and unpredictable to the recipient institutions,making it hard for local government and NGO facilities to prepareand adhere strictly to financial plans;
(c) As mentioned above (para. 3.10), local government and NGOfacilities have little incentive to improve the range and qualityof services provided or to raise their share of internally-generated revenues. For example, under the existing procedures fordetermining Central Government subventions, district and ruralcouncil facilities have no incentive to increase cost recovery,since subventions are intended to cover gross operatingexpenditures, rather than net outlays, and fees are not retainedat the point of collection; and
(d) Most importantly for the local councils, there is a noticeableapathy and lack of commitment and "ownership" of their clinics,which is related to the 10O Central Government subvention and theabsence of any matching with local funds.
3.42 In order to foster local interest in these important primaryhealth facilities, and also to reduce their financial burden on the CentralGovernment, Zimbabwean officials should consider options for returning tolocal governments a greater share of financial responsibility and authorityfor providing health care. One possibility would be to develop cost-sharingformulae for MOH subventions to municipal and local councils. Theseformulae would take into account the relative financial strength of thesedifferent forms of local government, which vary considerably. In general,the municipalities and district councils are able to raise substantialrevenues through taxes and fees, while the rural councils (located in thecommunal farming areas) have a relatively weak fiscal base. For simplepurposes of illustration, under these circumstances, MOH might provide asmaller share of budgeted funds to urban clinics (e.g., 25Z) than todistrict council clinics (e.g., 50) and rural council clinics (e.g., 752).The same approach could be taken with church mission health facilities, inorder to give these institutions greater incentives to collect patient feesand seek private donations within Zimbabwe and from abroad. While themission hospitals provide important health services at relatively low cost,

-34-
the current level of Government subvention of nearly 80Z appears to beunnecessarily high.
3.43 The savings accruing to MOH through these revised cost-sharingarrangements could be significant. For example, by applying to the actualexpenditure figures for 1987 a set of revised MOH subvention levels of 25?for municipalities, 5O for rural councils, and 75Z for district councilsand missions, MOH would realize savings of about Z$ 11 million or 42 of theMinistry's budget.
3.44 To implement such a cost-sharing policy, MOH, in collaborationwith the Ministries of FNar4ce and Local Government, would need to analyzein detail the financial strengths and weaknesses of the municipalities,local councils, and church mission health providers. This would requirethat all these institutions openly disclose their financial position. TheCentral Government ministries would then have to negotiate with the urban,rural, and mission facilities the appropriate cost-sharing formulae.Reforms of the local government system in Zimbabwe, some of which arecurrently under active consideration by GOZ, would have an importantbearing on cost-sharing for the health sector. Any moves in the directionof expanding the financial responsibility of local government and churchmission health institutions would also need to be accompanied by stafftraining in the areas of cost accounting and financial management.
3.45 Another MOH policy which, if strictly adhered to, could reducesignificantly the cost to the Central Government of providing health carewould be to enter into scontracts" or agreements with major church missionhospitals, stipulating that the NGO institutions serve as the districtreferral hospitals in areas where no Government facility currently exists.The church missions account for a significant share of health servicesnationally, especially in the rural areas, and do so at relatively lowcost. They are therefore an integral part of Zimbabwe's health system,which the Government should strive to maintain. At the same time, however,the a-stem of public subventions should encourage the missions to generateas much local revenue as possible, and should reward facilities which meetclearly-defined standards for quality and range of care and take on addedresponsibilities. The agreements between MOH and the mission hospitalscould specify minimum care standards, cost recovery targets, and a "base'subvention level. Additional subventions would then be provided tocompensate mission hospitals for "special" services such as supervisingadjacent clinics, training paramedical staff, sponsoring PHC programs, etc.If necessary, MOB could also provide capital grants to church missionhospitals, in situations where it would be less costly to expand anexisting NGO institutions than to build a new Government facility.
3.46 One additional way in which local governments and church missionscould increase their financial contribution to the cost of health carewould be by establishing drug revolving funds. The health facilities wouldprocure their own drug supplies from Central Medical Stores or throughother channels, and would then charge prices enabling them to recover allor part of the costs. In cases where full-cost pricing would make somedrugs unaffordable to low-income households - especially in rural areas -

-35-
cost-sharing between MOH and the local institution would again be required.Drug revolving funds might be especially appealing to patients attendinglocal government and mission hospitals and clinics, since they have alreadyshown their willingness to pay others (traditional healers, privatepharmacies) for a timely supply of drugs. Since drug shortages occasionallyoccur at the rural clinics which represent the last point in the nationalpharmaceuticals distribution network, clinic customers might also beinclined to support a revolving fund which ensures them the availability ofessential drugs.
3.47 Community Participation. Zimbabwe has a long tradition ofcommunity participation in development activities, especially in thecountry's rural areas. Local communities have historically donated time andlabor to help build primary schools and to maintain access roads; sinceindependence in 1980, some communities have also constructed "waitingmothers' lodges" for women waiting to give birth at rural clinics. Thesekinds of local initiatives not only reduce the cost to the CentralGovernment of such public assets and services, bu: also instill a sense ofpride and ownership in the community which uses them. While the financialcapacity of many local communities is extremely limited, the GOZ may wishto consider additional ways in which community participation in the healthsector could be elicited, for example, in building houses for clinic staff.
Tax Treatment of Health Expenditures and Health Professionals Incomes
3.48 Taxation of Health Expenditures. Until recently, tax credits weregranted for most out-of-pocket health expenses above a Z$72 deductible, andfor individual and corporate contributions to medical aid schemes. In April1988, the GovernluLent reduced this tax credit considerably when it amendedthe Income Tax Act. The tr..- credit is now limited to 20Z of all medicalexpenses above Z$250, including medical aid subscriptions.
3.49 Given that medical aid contributions in 1987 amounted to about Z$100 million, and that private out-of-pocket expenditures were estimated atover Z$ 50 million (Table II-1), the net revenue gain to the GOZ as aresult of the new income tax legislation should be enormous. The Ministryof Finance might take this into account in reviewing with relativelygreater sympathy the annual MOH budget requests.
3.50 In considering future reforms in this aree, Government officialsmight wish to examine the household financial security and equity aspectsof the tax law. On the first point, it can be argued that the tax creditabove the Z$ 250 deductible provides a partial form of 'catastrophic"health insurance, to protect families from being wiped out financially inthe case of extremely costly care for a severe illness. If this were thecase, however, the deductible should apply to out-of-pocket expenses only,not medical aid subscriptions which already have 'risk-sharing'built intothem. Furthermore, the percentage of expenditures allowable as a tax creditshould then be graduated to the amount of out-of-pocket expenditure, sothat the percentage increases with the amount of private cost (i.e., theseverity of the 'catastrophe'). To make the tax provision equitable, too,the amount of the deductible should be graduated to the level of household

-36-
income, so that poorer families start benefitting from the tax abatement ata lower level of out-of-rocket expense.
3.51 Taxation of Private Health Professionals. The Department ofInternal Revenue is currently strengthening its capacity to review taxreturns and enforce compliance with tax laws, including tax payments fromprofessional groups (e.g., doctors, lawyers, architects, etc.) which havenot been fully collected. While the amount of additional revenue whichcould be raised through mtore rigorous application of inecl-Me tax law to stichindividuals as well as companies is difficult to estimate, Internal Revenuestaff indicated that it would be substantial, given the strength of theprivate sector in Zimbabwe. Of course, any measures to enhance collectionof income taxes from private doctors, pharmacy and laboratory workers, andnurses would have to be a part of a larger effort applied to a wide rangeof private professionals in the country.

-37-
CHAPTER IV
EFFICIERT USE OF RESOURCES IN TEE HEALTH SECTOR
Introduction
4.01 Given the fact that resources for health care, public and private,are scarce in Zimbabwe, policy-makers have recognized the importance ofutilizing those resources in a manner which maximizes their health benefitsfor the country's population. This means ensuring that resources aredevoted to those activities which will bring about the greatest improvementin health status, especially when their costs are relatively modest:conversely, large amounts of resources should not be poured int.o healthcare activities which confer only minor benefits at a high cost. perindivi ;ual treated. In other words, attention should be focused uponallocative efficiency. In addition, for any given health service provided(e.g., delivery of a child in a hospital or clinic, treatment for malaria,disinfection and dressing for a wound, etc.), the cost should kept as lowas possible, consistent with acceptable standards of care. This suggeststhat health care providers in Zimbabwe must also strive towari high levelsof technical efficiency.
4.02 In the sections that follow below, aspects of both allocative andtechnical efficiency in Zimbabwe's health sector are examined, and optionsfor enhancing such efficiency are explored. The ultimate objective of suchan exercise is to search for ways in which Zimbabr;e can obtain more "valuefor money" in its expenditures for health care.
Allocative Efficiency
4.03 The debate over allocative efficiency in Zimbabwe, as in mostcountries, boils down to the issue: how much is being spent on promotiveand preventive health activities, as opposed to the treatment of illnessesthemselves? In both developed and developing countries, health policy-makers agree that, given prevailing expenditure patterns, at the marginfinancial outlays for preventive care are more cost-effe .tive than forcurative care. In developing countries on average, the approximatetreatment cost per additional life saved by curative care ranges fromUS$500 to US$5,000, while the approximate cost per additional life saved bypreventive programs such as childhood immunizations, vector control, andsanitation improvements is less than US$250. While all countries includingZimbabwe must allocate resources for the treatment of those already ili, itmakes sense under these circumstances to devote an increasing proportl_.. ofresources to preventive measures.
4.04 In an effort to improve allocative efficiency, the Government inits post-independence policy statement, "Planning for Equity in Health,"gave first priority to establishment of a primary health care (PHC) networkresponsive to the needs of the vast majority of the population.

-38-
PHC-essentially a cwmbinatiort of preventive health activities plustreatment of basic illnesses at community or clinic level (the clir.ic beinga "primary" facility) - was to be implemented through:
(a) upgrading the few existing rural clinics and building new clinicsto ensure access by the entire population to basic services;
(b) training paramedical personnel to staff rural health centers andvillage health volunteers to educate and motivate the population;
(c) retraining doctors and nurses to supervise PHC activities; and
(d) integrating rehabilitated district and provincial facilities intoa referral system to support the PHC system.
Recognizing that it would be politically difficult to transfer existingresources away from urban and curative health services, the Governmentundertook to increase overall financial allocations for healthsubstantially. and to ensure that these incremental resources were devotedto PHC, inci.uding preventive care activities.
4.05 How has Zimbabwe performed since independence in this area ofallocat:ive efficiency, especially regarding Government expenditures? Thesystems for budgeting and monitoring spending make it exceedingly difficultto answer this question with any precision. Budgets are broken down bybroad expenditure categories (e.g., salaries, transports, drugs, etc.)rather than by program; even the distribution of funds on a geographicalbasis or by level of care (primary, secondary, tertiary) is far fromtransparent. While it is clear that the Government has been successful inincreasing substantially the overall level of public resources devoted tothe health sector, especially in the years immediately followingindependence, efforts to strengthen PHC and preventive care are harder toevaluate.
4.06 However, by re-analyzing the available expenditure data from 1987(Chapter II) and making several reasonable simplifying assumptions, itappears that as much as one-quarter of all public expenditures for healthin that year was devoted to preventive activities. More specifically, about28Z (Z$ 71.1 million) of the ZS 258.2 in public (HOH, municipal and localgovernment) spending in 1987 may have gone to prevention, including Z$ 39.8million for facility-based activities, Z$ 26.5 in community-based programs,and Z$ 4.8 for family planni-ig services provided by ZNFPC. The chiefassumption here is that 10X of spending at tertiary facilities, 202 atsecondary level, and 502 at primary level is devoted to health prevention.Since hospitals and clinics in Zimbabwe account for the overwhelmingmajority of health expenditures, the above analysis is quite sensitive toany assumptions concerning the share of hospital funds assigned topreventive care, and the results should therefore be treated with caution.
4.07 It also appears that, since independence, Zimbabwe has beenincreasing the proportion of Government health outlays targeted atpreventive health services, thus improving allocative efficienc). As statedin Chapte:7 II, since 1980 the MOH has established or expanded significantlya number of important preventive health programs, with donor support

-39-
playing a major role in several of them. These iniclude childhoodimmunizations (UNICEF, WHO, and others); rural water and sanitation (UNDP,NORAD, Netherlands, DANIDA); growth monicoring and supplemental feeding forchildren (SIDA); ante-natal care and family planning (USAID, UNDP, WorldBank); and malaria control.
4.08 In addition, the construction or rehabilitation of rural clinics(African Development Bank, EEC, SIDA, NORAD) and district hospitals (WorldBank) and their staffing has facilitated the delivery of primary andpreventive health care to underserved communities. Since 1980, access tothese health care facilities at the local level has increasedsubstantially, with the upgrading of more than 100 clinics and constructionof more than 200. Government-sponsored training programs have also producedimpressive number of paramedical personnel, including more than 3,000SCNISCNM, 300 environmental health assistants, and about 7,000 villagehealth workers (now community development workers). In this regard, theGovernment's policy and program measures designed to improve "equity inhealth" by focusing investment on rural areas have also paid off inenhancing allocative efficiency.
4.09 While these past efforts are commendable, Zimbabwean officialsrecognize that more needs to be done in the future to emphasize preventivehealth care:
(a) safe water supplies and sewerage must be expanded, to avoid thetransmission of water-borne diseases;
(b) growth monitoring, nutrition education, and measures to raise theincomes of poor households should be strengthened in order toreduce child malnutrition;
(c) a range of prevention activities for disease control need to bebuilt up, to lower the incidence of malaria, respiratoryinfections, and tuberculosis. Slowing the spread of the HIV virusand thus the incidence of AIDS cases will also depend heavily oneffective prevention measures (i.e., protecting the blood supplyand changing sexual behaviors through education); and
(d) expanding family planning services to meet growing demand willalso constitute a vital preventive activity. This is becauseeffective family planning improves maternal and child health byreducing the number high-risk pregnancies (young, over-age, andhigh-parity mothers, and too closely-spaced births).
4.10 As Zimbabwe is likely to achieve near or full coverage of thepopulation with these prevention programs for maternal and child health andinfectious e'seases control over the coming decade, health planners shouldalso begin --o consider additional prevention activities to deal with adultchronic diseases (hypertension, heart disease. stroke, diabetes, etc.). Asthe risk of acquiring these diseases has been bhown to be affectedsignificantly by a series of environmental and behavioral factors (diet,exercise, smoking, alcohol consumption), prevention efforts will need tofocus on changing such behavior.

-40-
4.11 As stated in Chapter II, a continuation of current Governmentpolicies which emphasize that most new investments (facilities, housing,transport, communications) in health and incremental personnel should betargeted in the rural areas will also help to improve allocativeefficiency. Existing urban health facilities should not be neglected: theywill need to be well maintained, and there will be cases for selectiveexpansion and upgrading in the towns and for development of a clinicstructure that prevents patients from automatically turning up at the largehospitals. This is important, if the urban health infrastructure is tocontinue serving its urban clientele, as well as providing referral care tothe entire country's population. However, given the heavy concentration ofhigh-level health workers and facilities in the urban areas - 202 of allhospital beds, 65Z of MOH doctors, and half of SRNs belong to the fourreferral hospitals in Harare and Bulawayo, for example -it would be hard tojustify any major new health investments in tne towns over the next fewyears.
Issues in Technical Efficiencr
4.12 Hospital Efficiency. Since hospital-based services account forthe bulk of health-related expenditures in Zimbabwe and other countries,enhencing the technical efficiency of hospitals should be a key priorityfor policy-makers attempting to maximize the benefits of health spending.Hospital efficiency depends heavily on keeping down the unit costs per in-patient admitted and treated, which absorbs most financial outlays at thehospitals. This in turn means maintaining low daily in-patient coststhrough high bed occupancy rates and cost-effective use of technicalinputs, especially drugs and health manpower. At the same time, in-patientlength of stay (LOS) should be kept to a minimum, consistent with go imedical practice.
4;13 The data required to analyze the technical efficiency ofZimbabwean hospitals is not easily obtained. Inrormation on numbers ofhospital beds and admissions by facility is .!outinely collected, but totalnumbers of patient-days and average LOS data are not currently availablefor the 77 church mission hospitals which account for 35Z of the 18,100Government and NGO hospitals beds in the country. No information onadmissions, patient-days, and LOS is assembled for the private andindustrial hospitals which probably cover at least ar. additional 1000 beds.Furthermore, hospital expenditure data are generally not broken down by in-patient and out-patient care or by functional category, which severelyl_mits assessments of technical efficiency. In addition, some Governmentexpenditure figures are simply recorded on an aggregate basis for allprovincial, district, and rural hospitals in a given province, making itdifficult to assign these costs to individual facilities. If in the futurehealth officials are to monitor the technical efficiency of the nation'shospitals, an appropriate facility-based budget and expenditure system willneed to be designed and put in place (see below).

-41-
4.1.4 Despite the above limitations, the available data do suggest anumber of important issues in hospital efficiency:
(a) Bed occupancy rates (Table IV-1 and Figure 4.1) are generallyhigher in central (average of 89Z) and provincial (912) hospitalsthan in district hospitals (752). In five of the eight provinces(Manicaland, Mashonaland East, Matabeleland North and South, andMidlands), district hospitals reported less than 802 occupancy.This suggests the relative under-utilization of hospitalfacilities at the district levei, especially as LOS in the higher-level hospitals does not appear to be unreasonably long. Under-utilization at district level may be a result of weaknesses in theexisting referral system, with patients either by-passing thedistrict and going directly to provincial or central hospitals, orwith district facilities referring patients to a higher-levelwithout admitting them, because of shortages of staff, drugs. etc.Overall weaknesses in these peripheral hospitals, including thoseoperated by the church missions, seem to be confirmed by theavailable data on the mission hospitals: assuming an average LOSsimilar to the district hospitals (i.e., 8.7 days, which would bevery conservative), the average occupancy rate for the missionfacilities in 1987 would be only o2?. The reasons for low-bedoccupancy in district - and probably mission - hospitals need tobe investigated, and measures taken to correct this situation.These might include improvements in the quality of health servicesin the district hospitals, as well as adjustments in the user feestluc*ure to encourage patients to refer themselves at the outsetto the nearest district or mission facility.

-42-
TABLE IV-1
Hospital Occwiancy Rates and Average Lenth of Stay, 1987
AverageLength of Stay
&rber of Avg Dally Occay (as)Central Hospitals Beds bpatients I _w_a_ _em_y_
Partrenyatwa 901 782 87 9.9 3.9Harare Central 1,258 1,198 95 8.2 3.2Linited Bulawayo 651 429 66 9.1 5.1wilb 937 935 10D 8.9 3.9
STotal 3,745 3,344 89
Proviclal Hospitals
MnIcaa 192 211 110 6.3 3.9Mashoaland Central 120 148 123 8.4 6.9MashonaIand East 453 367 81 7.5 3.7Mashomahnd West 175 154 88 7.2 6.1MvYko 239 256 107 5.9 7.3MEatabeblead Nor U- Matabelanud South 184 125 68 12.0 4.9Midlands 2 4 208 82 5.2 5.3
SLb-Total 151T t Hi
Dlstrict Hospitals
Manlcaand 862 501 76 8.8 5.3Mashorolad Central 116 106 91 7.6 2.5MashalaXnd East 169 118 70 12.7 1.3Masholad Wst 609 533 88 7.5 4.0Masvhu 325 335 103 9.1 3.1Matablelad taNrth 188 98 52 7.8 3.1Matabelaand Suth 413 318 77 9.8 4.1Midlands 728 434 60 6.3 4.7
S3b-Total 4,Z1u i,3- 71
Source: WH service and edlture data.
(b) Bed occupancy rates in the central and provincial hospitals aregenerally good, with only one of the four central facilities(United Bulawayo Hospital) and one of the eight provincialfacilities (Matabeleland South) reporting less than 80? occupancyin 1987. While one central hospital and three provincesexperienced bed occupancy rates in excess of 100?, it would seemhard to ijutify creation of additional bed capacity at higher-level facilities, except in the case of Masvingo, where bothdistrict (103Z) and provincial (107Z) hospitals are alsoovercrowded. In the case of Mpilo Hospital (100Z), future patientoverflow might be sent to United Bulawayo, which is located in thesame town. In Manicaland and Mashonaland Central (110? and 123? atprovincial level), improved referrals to the district hospitals,which still have some spare bed capacity, might mitigate oreliminate the existing overflow at the provincial hospitals.Reduced LOS, where medically justified, would also help todecongest these hospitals. While the present analysis can help tosuggest such possible low-cost solutions to these hospitalutilization problems, a more detailed study of individualfacilities is required before final decisions can be taken.

-43-
FIGURE 4.1:
Hospital OccupancyRates
100.19100 89 919080 7670
1% of soCapacIty 50Occupied 40
30
20
100. . -
Central Provincial DistrictHospitals Hospitals Hospitals
Level of Hospital
Average HospitalLength of Stay
*9 8.7
a ' 7.5
7 -65
Days4
32
0.Central Hospitals Provincial District Hospitals
HospitalsLevel of Hospital
2 . c _ _~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I

-44-
tc) Bed occupancy rates exhibit high variation among facilities at thesame level of the referral system. At central hospital level, therange is from 662 to 1002, at provincial level from 68Z to 1232,and at district level from 522 to 1032. MOH should study thereasons for this great variation, especially by examining thedistrict-provincial hospital occupancy rates within the sameprovince, ideally with rural hospital and church mission hospitaldata integrated as well. Table IV-1 suggests three types ofdistrict-provincial occupancy patterns: high-high (e.g., Masvingo,Mashonaland Central), low-high (e.g., Manicaland), and low-low(e.g., Mashonaland East, Matabeleland South). For each of thesepatterns, a somewhat different solution is probably warranted.
(d) LOS is generally lower in provincial (7.5 days) than central (9days) hospitals, but, contrary to what might be expected in asituation of good hospital management, is nearly as high atdistrict level (8.7 days). This suggests that many districthospitals may be keeping patients too long, perhaps because ofspare bed capacity. If LOS were reduced in these facilities, bedoccupancy rates would probably fall further, revealing even moreclearly the fact of current underutilization of the peripheralhospitals. LOS might be brought down at some district hospitalsthrough improvements in transport arrangements (special buses,taxi services) to eliminate unnecessary delays in ir-patientdischarge.
Ce) As in the case of bed occupancy, average LOS also shows widevariation among facilities at the same level of the referralsystem, where LOS ought to cluster closely around a norm for agiven patient caseload mix. MOH officials should identify thehospitals which represent "outliers" in LOS, and determine thereasons for upward or downward deviations in length-of-stay. TableIV-1 suggests several facilities that might be examined mo;.eclosely: for example, United Bulawayo's maternity ward (LOS of 5.1days); general wards at the provincial hospitals for MatabelelandSouth (12 days) and Mashonaland Central (8.4 days); and generalwards in selected district hospitals in Mashonaland East (12.7days) and Hatabeleland South (9.8 days). MOH might also establishI.OS norms for general, maternity, and other specialized patients(e.g. tuberculosis) at the various hospital levels, and develop anaccurate and responsive system for monitoring actual LOSperformance.
(f) Technical efficiency, as measured in terms of cost per admission(Table IV-2 and Figure 4.2), is virtually identical at three ofthe four central hospitals (Z$ 236-238), but is about three timeshigher at Parirenyatwa Hospital in Harare (Z$ 742). WhileParirenyatwa's status as a specialized referral hospital handlingcomplicated cases requiring sophisticated equipment and manpowermay explain much of this variation, hospital officials might re-examine the institution's cost structure and try to identify waysto reduce expenditures in appropriate areas.

-45-
Figure 4.2: Zimbabwe - Cost Data by Province
Cost Per Pntbnt oDy in mOm Ho"iItme. 17r
50
42
40 36 r , 36
30*_30
mi MC. EwE Mt_W. mmv MALN. mtS MidiProvinaUIDWItict/Rural Hospitals
Cotl Pu Admission In MOMoNsppttels. I9r
260 - 36--23 23.
2001 E - 17-200 ~ ~ ~ ~ ~ ~~~~~~6
10
MarV MALC. hILE MNW. Mwv MdF MEL MidiProvinclai/District/Rural Hospitlsl
'Excludes four central hospitals

-48-
TABLE W-2
ZWABWECost Per Adnisslon and Per Patient-ay
in mum fOpItulS, il0
Cost Per Cost PerAdmission Patient-Day
Central Hospitals (ZS) 1/ (ZS)
Parirenyatwa 669 75Harare Central 274 40Utlted Bulawayo 238 28liio 256 33
Provinelal/DistrIct/Rural Hospitals
Manicaland 201 30Ihshonaland Central 236 36Mashonahnd East 239 42Mascnaland West 119 19Masvir9o 169 20Matabelelad North 235 38Matabeleland SaM 143 19Mldlands 187 36
Source MOH service and expenditure data.
Note 1/ Assumes that 80% of hospital expenditure is for in-patient services and2C6 for out-patient care.
(g) Unfortunately, the figures in Table IV-2 on cost per admission athospitals below the central level aggregate the results for allfacilities within a province, thus masking inter-institutionalvariation. These figures do, however, point to wide variationsamong provinces, with several (Mashonaland Central and East andMatabeleland North) reporting costs per admission similar to thecentral hospitals, while the other five provinces show costsroughly 20-502 lower. The reasons for these variations also meritcareful investigation on a facility-by-facility basis: onestarting point might be to look at those hospitals with high per-admission costs i_ Mashonaland Central and East and MatabelelandNorth. It is also significant to note that the average cost peradmission at three typical church mission hospitals (ranging fromZ$ 87 to Z$ 144) is generally lower than in comparable Governmenthospitals. By including several church miss'on facilities in theanalysis of hospital costs, certain efficiency-enhancing measuresapplicable to MOH facilities might also be uncovered.
4.15 Expenditures for Drugs. One specific area in which Zimbabweanofficials have recognized for a number of years that technical efficiencycould be improved has been the utilization of pharmaceuticals, on both anin- and out-patient basis. At the time of independence, it was felt thatexpensive brand-name drugs, cat-zring to an urban elite, were absorbing mostof the funds (and foreign exchange) available for p1harmaceuticals: drugcost per patient treated was therefore unnecessarily high, and otherpersons who needed drugs were not receiving them, because of national

-47-
shortages, weaknesses in the distribution system, and inability to pay. Tocorrect this situation, the GOZ proposed in its policy statement "Planningfor Equity in Health' the adoption of an "essential drugs' list for use byGovernment facilities, offering the potential of greater internalefficiency and equity. The policy has been implemented through the ZimbabweEssential Drugs Action Program (ZEDAP), which since its inception in 1986has developed and published a national essential drugs list (EDLIZ) for useby Government health workers and has begun to train nurses and doctors incost-effective prescribing practices. ZEDAP also makes possible importantcost savings through bulk procurement and the use of internationalcompetitive bidding. The expansion of primary care facilities andintroduction of free services for low-income households are, in part,intended to make essential drugs more accessible to the mass of Zimbabwe'spopulation.
4.16 While ZEDAP has brought about many positive changes in theefficiency and equity of drug use in Zimbabwe, GOZ officials acknowledgethat several problems remain. First, the current system for allocating thecountry's increasingly scarce foreign exchange does not satisfy the drugneeds of Government health facilities. The foreign exchange content ofZimbabwe's pharmaceuticals is high - whether the drugs are imported infinished form or are manufactured locally using imported materials - andthe compelition for limited foreign exchange is intense. The chronicfailure of MOH to obtain centrally, through Government Medical Stores(GMS), all the drugs needed for public facilities is due to two factors:(a) inability to estimate accurately annual drug requirements, and (b)unwillingness on the part of the GOZ Joint Allocations Committee (JAC) togive MOH adequate foreign exchange. A combination of these two factorsresults in chronic shortages.
4.17 The fact that Government hospitals and clinics experience periodicshortages of drugs is neither equitable nor efficient: equity goals areinhibited because peripheral facilities serving lower-income familiessuffer the most severe shortages, while efficiency is impaired because drugshortages at primary care facilities tend to encourage referrals to higher-cost secondary and tertiary hospitals. Meanwhile, there is also theeconomic cost of patients remaining untreated. In addition, to deal withdrug shortages, MOH is forced during the course of the year to purchasedrugs in relatively small quantities on the local market from privatesuppliers, at significantly higher cost than if the same items wereprocured in bulk by GMS. This also reduces the efficiency of drug use byGovernment health facilities.
4.18 In order to enhance the efficiency of the drug procurement system,GOZ officials should consider several options:
(a) MOH's drug estimation procedures could be improved, by trainingfacility-based personnel, as well as district and provincialadministrators, and developing an effective drug informationsystem.
(b) Procedures for allocating foreign exchange for pharmaceuticalsmight also be modified, to ensure that importing agents and localmanufacturers under contract to GMS receive adequate foreign

-48-
exchange to meet the basic etpidemiological needs of the populationserved by Government health facilities.
(c) Given the tightly constrained foreign exchange situationprevailing in Zimbabwe, the Government should find ways topersuade importing agents and domestic manufacturers to restricttheir purchases to lower-cost generic versions of specific drugs,rather than the more expensive brand name items. In this regard,as of January 1, 1990, private sector drug purchases are supposedto be limited to generic products, although the number of suchproducts is larger than those contained in the EDLIZ.
4.19 Some amount of wastage also occurs through ovei prescribing orincorrectly prescribing drugs, or through the continued use of moreexpensive brand name alternatives. The ZEDAP program has made considerablestrides in curbing this wastage, by limiting the nimber of drugs dispensedby MOH personnel and educating health care workers about their proper use,and the effects and side-effects of various drugs and combinations of them.ZEDAP staff have compiled and distributed an easy-to-use desk guide ondrugs for health care workers which, while maintaining a professional level
of sophistication, provides the basic simplified elements of acceptedprescribing and usage. Both private and public doctors and pharmacists arebeing trained in better prescribing methods.
4.20 In addition to the above measures, the cost-effectiveness of drugprescribing could be further improved through several other steps whichhave been successfully applied in other countries. These include:
(a) limiting the number of drugs that can be prescribed during an out-patient visit to two or three items, and for a specific timeperiod (e.g., not more than two months supply);
(b) at least for those who are able to pay something for their healthcare, charging per drug item prescribed. This approach tends toencourage patients, as well as their prescribers, to limit thenumber of drugs and dosages to as reasonable amount; and
(c) monitoring doctors' prescribing practices for in-patients, atleast in the major hospitals. Administrators at Parirenyatwa haveapparently tried to establish such a monitoring system, by whichdoctors treating a similar mix of patients are studied for theirprescribing habits. Actual prescriptions can be compared againstone another and against an accepted norm for specific illnesses,in order to identify those doctors who deviate significantly fromthe others. The analytical results can then be presented to thedoctors and discussed with them. This system should be extended tomost of Zimbabwe's larger hospitals.

-49-
CHAPTER V
MANAGEMENT OF HEALTH EXPENDITURES
Background
5.01 The vitality and diversity of Zimbabwe's health system -comprising as it does not only significant public institutions but also alarge and heterogeneous private sector, both for-profit and non-profit,modern and traditional - complicate enormously the Government's task ofensuring that financial resources are spent where they can achieve thegreatest individual and social benefit. The GOZ must tap fully theresources available in the private sector, while providing incentives topromote their wise utilization and the growth of private activities whichare consistent with other national objectives. It must target public fundsto those households whose health needs are not, or cannot, be metadequately through private channels, and to health interventions such asimmunizations, water and sanitation, and family planning, which haveimportant social ramifications.
5.02 In the previous chapters of this report, a number of major optionsfor reforming health care financing in Zimbabwe have been reviewed. Theseoptions would support more effective recovery of the costs of healthservices provided by public institutions, and would help to mobilizeadditional resources for better "health for all" Zimbabweans, especiallythe poor. Expansion of insurance mechanisms and cost-sharing schemesi:.volving central and local government and NGOs have been discussed. Policyoptions have also been put forward which would shift the allocation ofresources toward health activities conferring relatively higher benefits,and which would improve the technical efficiency with which resources arespent for specific health services.
5.03 To meet these challenges, a wide range of financial planning andmanagement skills and systems will be required. While Zimbabwe is alreadybetter endowed with these skills and systems than many other developingcountries, GOZ officials recognize that much more must be done to improvethe management of fi-nancial resources for health in the country. This isespecially true in the light of the Government's current moves todecentralize many financial responsibilities, in health as in the othersectors of the economy. The existing publicly-funded health services arehighly centralized, in part for historical reasons (the pre-independencehealth system was based upon centralized planning, budgeting, andprocurement), in part because the post-independence government usedcentralized methods to pursue its sweeping changes in the health systemafter 1980. The equity, efficiency, and long-run financial sustainebilityof health services in Zimbabwe can be greatly enhanced through such apolicy of decentralization - but only if financial planning and managementskills and systems are present at the various levels of the MOH healthnetwork (center, province, district, facility), as well as within localgovernment institutions, NGOs, and the private sector. To achieve this, amajor initiative in human resources development - training and systemsdesign - will be needed.

-50-
5.04 In the sections below, issues and options for improving financialmanagement in the following areas are considered: financial planning andbudgeting; manpower planning; expenditure monitoring and analysis; revenuecollection; procurement of equipment and pharmaceuticals; and management ofdonor resources.
5.05 Budgeting and Planning. The MOH annual budget, which includesnearly all recurrent expenditure but omits most foreign-assisted activitiesas well as major civil works projects executed by MPCNH, consists of fourmain 'heads": Administration, Medical Care Services, P?reventative Services,and Research. MOH assembles the yearly budgets for Medical Care andPreventative Services, which account for over 902 of Ministry expenditure,from estimates made by the 44 MOH "cost centers" across the country. A costcenter may be equivalent to a single large hospital, but more often itcovers a hospital plus a number of nearby clinics. In some cases, a costcenter may have its hub at a district or provincial hospital, and extend tothe clinics in several neighboring districts which do not have an MOHhospital. The person responsible for drawing up the estimates at each costcenter is the senior medical officer of the facilities covered. assisted byan administrative officer where one is in post. The cost center estimatesare sent forward to the MOH headquarters in October-November of each yearthrough the respective Provincial Medical Directors' offices. MOHheadquarters reviews and revises these spending proposals and submits themto the Ministry of Finance, Economic Planning, and Development (MFEPD) forfurther scrutiny. Eventually, they are incorporated in the Governmentbudget which is approved by Parliament in June-July of the following year,and reflected in the actual amounts warranted for spending. The costcenters ultimately learn of the budget outcome ir September-October, nearly12 months after submitting their requests.
5.06 MOH officials acknowledge that this budgeting system exhibits anumber of serious weaknesses, many of which have been alluded to in earlierchapters of this report. Budgets are not broken down in ways which permitmeaningful analysis of allocative or technical efficiency - by facility(hospital, clinic, etc.), program (family planning, ante-natal, maternityservices, out-patient general, etc.), or type of input. Cost center budgetsdo not include health workers' salaries, which accounts for about two-thirds of all expenditures: these figures are kept aggregated at the MOHhead office. The person responsible for financial matters in each costcenter has limited control over actual spending, since he can onlyauthorize expenditures to be incurred for a restricted number of items or'sub-heads', e.g., travel and subsistence, transport, printing andstationery, bedding and linen, drugs, etc. Should shortages of funds occur,reallocations among sub-heads can only take place with the approval of MOHheadquarters. Even for these items, procurement and payment are stillhandled by MOH headquarters. In addition, even though the MOH budgetprocess begins with "bottom-up" proposals from the cost centers, thedecisions on the overall shape of the budget and its relative proportionsare made exclusively at the "top", idith little dialogue between the headoffice and the periphery.
5.07 MOH policy-makers have signaled their interest in redesigning theministry budget formats, to make them more responsive to the needs of

-51-
managers at various levels of the health care system. MFEPD have alsoindicated that they would have no objection to these changes, provided thatthe main budget sub-heads, which are used throughout Government, are leftunchanged. The real issue is how to redesign the budget and phase suchchanges, and this is no simple matter, given the large number of potentialusers of budget information (headquarters accounting officers, planners,and policy-makers; provincial and district medical officers and healthservices administrators; and hospital and clinic managers) and the limitedfinancial management skills currently existing within MOH. Probably themost single important step in redesigning the budget would be to discusswith these various users their financial information and related managementskills needs. The revised budget and financial reporting formats, systemsand technology requirements (including micro-computers), and trainingprograms, would then flow directly from such an information needs/skillsgap assessment.
5.08 Whichever way the budget is recast - and this is a job for MOHusers to undertake, along with specialized consultants - it should almostcertainly make it possible to analyze planned and actuai Governmentexpenditures according to:
(a) curative versus preventive care;
(b) major programs (family planning, malaria control, water andsanitation, etc.) and departmental functions at hospitals(maternity, surgery, etc.); and
(c) principal inputs (salaries, drugs, transport, fuel and lighting,etc.).
Furthermore, these types of expenditure data should be available forvarious degrees of aggregation, including information for:
(a) the entire MOH system;
(b) specific gecgraphica.l areas (province, district, etc.);
(c) different levels of care (primary, secondary, tertiary); and
(d) individual facilities.
In addition, specific facilities, particularly the larger hospitals, willno doubt wish to develop more detailed and customized financial managementinformation systems to meet their own special needs. This should beencouraged, as long as every effort is made to ensure that these facility-based management systems are as consistent as possible with the overall MOHsystem, and allow comparisons to be made.
5.C9 Redesign of the MOH budget should be accompanied by moves todecentralize further responsibility for preparing budgets, incurringexpenditures, making payments, and procuring goods and services (seebelow). Such moves would be consistent with'the GOZ's overaridecentralization policy, and would ensure that budgeting and relatedfinancial transactions respond to local needs in a timely manner. Of

-52-
course, decentralization of financial responsibilities can only beeffective when the necessary management skills and systems are in place. Inthis regard, financial decentralization has to be part of a larger programfor strengthening the management of health services at provincial,district, and facility levels. While the ultimate objective of such aprogram would be to devolve some degree of responsibility down to the levelof every MOH facility in the country, a first step in this direction mightbe to improve financial management and increase responsibility in the fourcentral hospitals and the eight provincial medical directors' offices.
5.10 Another important element in budget reform would be to integrateinto a single MOH accounting matrix those items - mainly but notexclusively capital ones - not currently included in the MOH budget, butwhich appear in the budgets of MPCNH and MFEPD (the Vote of Credit, forforeign-assisted projects). Until this integration takes place, MOH policy-makers will not be able to assess systematically the full range of publicexpenditures for the health sector. At the same time, capital outlaysshould be clearly separated from recurrent expenditures, with capitalspending shown on both a one-year and multi-year basis. This would permitthe crucial analysis of the allocation of new Government investments in thesector (to curative versus preventive care, PHC versus referral services,and by geographical area) and an estimate of the incremental recurrentcosts associated with these investments. The existing three-year rollingPublic Sector Investment Program (PSIP) system permits only very limitedanalysis of this kind. In the case of capital projects for which theincremental recurrent costs have not been specifically calculated, roughrules-of-thumb for various standard types of investments (e.g., districthealth training centers, new district hospitals and clinics, etc.) shouldbe developed and applied.
5.11 Manpower Planning. Since salaries and wages absorb more than two-thirds of spending in the health sector, effective personnel informationand manpower planning systems, covering MOH health facilities and the localgovernment and NGO institutions where MOH pays staff salaries, are ofcritical importance to overall financial management of the sector. Mistakesin the manpower area need to be avoided, as they can have very seriousfinancial consequences. Inappropriate staffing patterns can be very costly:for example, an additional nurse at every clinic, if not performing usefultasks, would represent an enormous waste of resources, given that there aremore than 1000 such clinics in the country. Since training of medical andparamedical personnel is very expensive, training programs must alsoconcentrate on the priority categories of health workers, while matching asclosely as possible the output of graduates to the needs of health sector.
5.12 Cognizant of the importance of goad manpower planning anddevelopment, MOH's Manpower Department is currently undertaking a number ofmajor initiatives in this management domain. The Department is establishinga personnel management information system (PHIS). Manpower planningcapacity is being developed, and the first plans relating ideal staffingpatterns to available personnel (those currently employed minus retireesplus graduates of training institutions) should be produced by late 1989 qrearly 1990. The MOH Manpower Department has also signaled its intention tocarry out a careful review of existing health training institutions in

-53-
Zimbabwe, including recommendations for pedagogical and management changesand other minor investments that could make these institutions more cost-effective.
5.13 All of these initiatives in manpower planning and development areto be welcomed. They will have to be implemented gradually, according to aphased plan, given the limited staff and experience of the ManpowerDepartment itself. At the same time, however, several additional steps tostrengthen health manpower management should be seriously considered byMOH. Current and future manpower scenarios should include a salary "module"which allows policy-makers to assess the salary and wage implications ofthese scenarios. The results can be striking. For example, using 1988salary scales and the output of health training facilities as given in theNational Investment Register, 1986-90, employing an additional 85 doctors,167 SRN, and 73 SCN annually would cost an extra Z$ 4.9 million or 2? ofthe 1988 MOH budget.
5.14 MOH also needs to continue reviewing the range of possible optionsfor attracting and retaining adequate medical, paramedical, andadministrative staff within the public sector. This is especially true ofthe district hospitals and rural clinics, where vacancy rates for allcategories of staff are significantly higher than in the central facilitiesand the towns (Table V-1). The Ministry has recently taken several boldmoves in this area, including revising the University of Zimbabwe MedicalSchool curriculum to give greater emphasis to public health and communitymedicine, and increasing the period of compulsory Government service forgraduating doctors to five years (seven including housemanship). MOH mayfurther limit the number of young doctors who are allowed to pursuespecialized training immediately upon graduation from medical school, inpart as a way of ensuring that most of these graduates perform generalpractice. In addition, the Government should periodically review publicsector salaries for health workers, to ensure that they do not move too farout of line with private sector incomes. Non-salary benefits, includinghousing, can help to make public sector employment more competitive withprivate opportunities: the construction of staff housing at districthospitals and health centers under the Family Health Project, for example,is proving to be a key factor in attracting qualified staff to the projectarea. In view of the large numbers of nurses shifting from Governmentservice into the private sector, salaries and benefits and careerdevelopment options for this critical category of health workers shouldalso be reviewed.

-54-
Table V-1
ZIMBABWESkilled Staff Vacancy Rates
by Level of the Health-Car System.1986-87
Level of the Hsalth-Care Syste Doctors SRN SCN
Central Hospitals 4.0 4.0X 1.9XProvincial Hospitals 18.8X 18.2X 6.0XDistrict Hospitals 29.8X 12.6X 11.6XMission Facilities 23.9% 28.6X 24.0XDistrict Council Clinics 64.0XRural Council Clinics 12.5% 26.1%
Source: Ministry of Health
5.15 Revenue Collection. As mentioned in Chapter III, revenuecollection by MOH and council health facilities is poor. While this ispartly due to lack of i -entives, financial management practices in theseinstitutions are also weak. The obvious place to begin making improvementswould be the central and provincial hospitals. A combination of timelyautomated billing and receipt systems, more rigorous assessment ofpatients' ability to pay, and training for financial and accountingofficers of these institutions could result in a significant increase inrevenue collected.
5.16 As a second step, accounting systems in all MOH and localgovernment facilities need to be strengthened. At many hospitals andclinics, the only accounting records currently being used are a receiptbook and a one-side cash book for aggregating revenues collected. Adebtors' control account for those failing to pay fees is missing from manyhospitals. The stock of drugs received and utilized by the facility isusually not put through a stock ledger account. And other expenditures (forallowances, transport, vehicle running costs, maintenance, etc.) aregenerally not recorded. Where accounts are kept by MOH facilities, the cashmethod of accounting is used, rather than the accrual method. This means,for example, that debts not paid promptly may be regarded as belonging to alater period, rather than the period when they were incurred. It would bepreferable if Government health institutions were to move to the accrualbasis of accounting, which is actually practiced in a number of missionhospitals. Many mission hospitals have also agreed in recent years toseparate their financial statements for the provision of health servic.-sfrom their finances connected with other (e.g. educational, religious,etc.) activities. At a minimum, MIOH health facilities should expand thenumber of accounts maintained to the following: an income and expenditureaccount, a debtors' ledger, and a drug stock account.
5.17 Procurement. Goods anti. services required by MOH and valued atmore than Z$ 5,000 are procured by the Ministry of National Supplies (whichoperates GMS) on behalf of the Health Ministry. While such centralizedprocurement of some goods and services for the health sector may be

-55-
sensible - bulk purchase of drugs, for example (Chapter IV) - for otheritems a more decentralized system may be more appropriate. Some MOHofficials at provincial level feel that for a range of goods includinghospital linens, dressings, heating fuel, and laboratory reagents, andservices including cooking, laundry, and fumigation, a decentralizedapproach would be less expensive and would result in timelier deliveriesand better quality of services. Given that provincial tender boards alreadyexist and function effectively, it might be worthwhile to experiment withdecentralized procurement for a limited number of items and assess theresults, before deciding whether to expand or curtail such a system. Itemsfor which there are many local suppliers, or for which the need arisessuddenly and urgently, might be appropriate candidates for decentralizedprocurement.
5.18 Health officials in a number of countries have also found thatwhen certain hospital services such as patient feeding and laundry arecontracted out to private sector suppliers, the result is lower-cost,higher-quality services then under circumstances where the hospital triesto provide all these services internally. MOH officials should carefullyassess the advantages and drawbacks of "contracting out" and experimentwith such arrangements in selected hospitals. The results should then beclosely monitored and reviewed before deciding whether to extend'contracting outo to additional facilities.

-56-
CHAPTER VI
CONCLUSION AND RECOMMENDATIONS
6.01 During the nine years since independence (1980), Zimbabwe has madeimpressive progress in providing health care to its population . Millionsof people have for the first time gained access to basic care, and a rangeof cost-effective preventive health programs have been launched. Theservice delivery and health status figures given earlier in this reportattest to this rapid progress, much of it financed through an expansion ofGovernment spending for the health sector.
6.02 But, as Zimbabwean officials widely recognize, the country is nowfacing a mounting crisis in the financing of health services. The centralgovernment is becoming financially overextended, especially in view of theslow growth in public spending that has prevailed for the last five years,and which is likely to continue for some time to come. The health sectoralready receives about 5Z of the central government budget, a share typicalof a middle-income developing country, and one which is not likely tochange significantly over the next few years. Under these constrainedfiscal circumstances, there is a real danger that the Government may not beable to meet fully its existing financial commitments for health workers'salaries, medical equipment and drugs, and a host of other recurrent costsassociated with the operation and maintenance of the country's healthinfrastructure. Not only must all of these commitments be met, but Zimbabwewill need to make a number of additional investments in preventive andcurative care, if the country's health objectives for the 1990s and thebeginning of the next century are to be achieved. The issue of how to payfor existing and expanded future health services is therefore a real andpressing one.
6.03 To confront successfully this growing crisis in the financing ofhealth care, Zimbabweans generally agree that ways must be found tomobilize additional resources for use in the sector, and to obtain more"good health" from existing expenditures. At the same time, theGovernment's ongoing efforts to achieve greater equity in health - both inaccess to care and in paying for this care - must be maintained, and evenreinforced.
6.04 This will require that Zimbabweans develop bold and imaginativepolicies and programs, and enhance their analytical and management skillsin the financing of health care. It will also require a concerted andcoordinated effort between the public and private sectors, includingcentral, local, and municipal government, church missions and other NGOs,private modern and traditional practitioners, and industry.
6.05 This report offers a number of policy and program options thatcould help to resolve the crisis in financing health services in Zimbabwe.The recommendPd measures vWch are summeri7ed below are organized intothree main groupings: measures to inject additional money into the healthsector (Resource Mobilization); measures to help Zimbabwe get more "value

-57-
for money" in health (Allocative and Technical Efficiency); and measures todevelop the systems and skills needed to support stronger health financing(Management of Health Expenditures).
Resource Mobilization
6.06 To mobilize additional resources for the public sector, the GOZshould consider pursuing a range of measures including increased usercharges, and expansion of health insurance, cost-sharing between centraland local government, and enhanced community participation in healthactivities. In particular, the GOZ should generate more income from userfees by:
(a) raising the overall level of fees in Government healthinstitutions and adjusting this level periodically, in line withprice inflation;
(b) increasing in-patient and other charges for private patients, whoare mainly covered by medical aid, to meet the full cost of thecare they receive;
(c) imposing a nominal fee for out-patient visits at all Governmenthealth facilities; and
(d) charging separately for each drug prescribed, both for out-patients and those hospitalized.
6.07 To make these changes in the level and structure of user feeseffective, a number of procedures and management practices would also haveto be improved. These include: requiring that the burden of proof ofhousehold income be placed upon the patient; strengthening billing andcollection procedures substantially; and developing incentives forindividual health facilities to improve their revenue collection efforts.If all of these reforms were undertaken together, the revenue impact couldbe substantial, with at least an additional Z$ 40-55 million (in 1987prices) collected annually. Reforms (a) and (b) should be relatively easyto implement, the former because fees have not even kept pace withinflation in recent years, and the latter because there can be littlejustification, on equity or efficiency grounds, for the Government tosubsidize medical care for the highest-income groups in the country, whoare also covered by health insurance. Reforms (c) and (d) may be somewhatmore difficult politically to carry out, but they would also have a seriesof very positive effects: not only would additional resources be raised,but unnecessary use of out-patient care az.d of drugs would be curbed, whilestill ensuring tnat the truly poor receive the health services theydeserve.
6.08 If the GOZ ultimately decides to impose a consumption tax onalcohol or tobacco to help finance Government-provided health care,channeling those funds through a National Health Development Fund (NHDF)for primary and preventive care would probably be preferable to theestablishment of a National Health Insurance Scheme. Provided that such anNHDF proved to be politically acceptable, it would target additionai

-58-
resources for badly-needed health services to poor rural groups - thuspromoting tne Government's equity objectives - and for preventive healthprograms which are highly cost-effective. At the same time, the NHDFapproach would avoid some of the potential weaknesses of national healthinsurance, i.e.: the administrative costs associated with issuingmembership cards and determining eligibility for free care; the loss ofrevenues as a result of such free care; and the increased demand fortreatment with little or no benefit, in the absence of price-driven supplyrationing.
6.09 The GOZ should also encourage greater decentralized financing ofhealth services through measures that could complement increased user fees:cost-sharing between central and local government, and community supportfor local health facilities are both viable options that should beexplored. Cost-sharing formulae which take into account local diseasepatterns, per capita incomes, and availability of private and NGO healthservices, would be equitable and would probably also improve the qualityand productivity of health care delivered, by giving local governmentbodies a greater sense of ownership' of hospitals, clinics, and preventivehealth programs. Formal agreements or "contracts" between MOH and churchmission health institutions could also include provisions for cost-sharing.The cost-sharing formula explored in this report for illustrative purposeswould result in more than Z$ 10 million in additional local revenues forthe health sector, thus reducing the financial burden upon centralgovernment. Other formulae could generate even more local resources.Community participation, in the form of donated labor, materials, and cashfor clinic upgrading and cons.ruction of housing for rural health workers,would have similar positive effects. Drug-revolving funds, when organizedon a community, council, or district basis, would be another option forexpanding local financial participation in health care, especially whencombined with the recommendation above to begin charging part- or full-costfor drugs (para. 6.06).
6.10 Changes introduced in 1987 to the legislation governing taxationof individual incomes reduced substantially the tax allowance permitted formedical aid contributions and private out-of-pocket payments, thus loweringthe level of effective Government subsidization of private care andincreasing general revenues correspondingly. However, the Z$ 250 deductibleshould apply to out-of-pocket payments only, not medical aid contributions;the percentage of private expenditure allowable as a tax credit should begraduated to the level of spending; and the amount of the deductible shouldbe further graduated to household income. More rigorous application of thetax code to the incomes of health workers (doctors, nurses, pharmacists,lab technicians, etc.), as part of a larger effort to collect taxes fromprivate professionals, might also yield important government revenues.
6.11 Finally, expansion of existing medical aid schemes could inject alarge amount of additional resources into the health sector, and improvethe Government's financial position by increasing the number of medical aid

-59-
patients who could be charged full cost for care in public hospitals, whileeliminating some current Government outlays for free out-patient care thatwould then be provided by private practitioners. While it is difficult toquantify these effects precisely, a doubling of medical aid subscribersfrom 0.4 million at present to 0.8 million over the coming decade, couldresult in an additional Z$ 100 million (1987 prices) in healthexpenditures. The medical aid industry would have to play a major role insuch an expansion of medical aid, by developing imaginative low-costinsurance policies and promoting greater competition among societies. TheGovernment could also support this process in important ways, such asrequiring through legislation that all firms over a certain size provide aminimum level of health benefits to their employees.
6.12 Some of the above recommendations would shift an increasing shareof the burden of providing and financing health care away from the centralgovernment to local government, NGOs, and the privaLe sector. Many of therecommendations - especially higher user charges, changes in the taxationof private health expenditures and of health workers' incomes, and creationof the NHDF - would also increase the volume of financial resourcesgenerated within the public sector, and would thus enhance the MOH's claimsupon additional Government revenues. How should such incremental revenuesbe spent, to promote 'better health for all"? As indicated elsewhere inthis report, primary (PHC) and preventive health activities should beconsidered as the first priorities for this additional Government spending.While Zimbabwean health planners and policy-makers would have to make thedetailed expenditure decisions, incremental funds for health would open upa range of possibilities: with an extra Z $40 million, for example, MOHcould build five new district hospitals, or upgrade about 200 ruralclinics; train and pay the salaries of thousands of additional SRN, SCN,and community health workers; quadruple the current budget of the ZimbabweNational Family Planning Council; or some combination of these and a numberof other exciting options.
6.13 Efficiency. To improve the allocative efficiency of Governmentexpenditures for health, GO'ir should continue to increase the proportion ofpublic spending for PHC and preventive care. At present, the allocation ofMOH's facility-based 'patient' bvdget to tertiary/secondary/primary care is50Z/30X/20Z (para. 2.11). Over time, MOH should striv-e to increase theshare for primary care facilities, for example, by setting a target of40Z/30Z/30Z by 1995. Similarly, MOH should set targets for raising theshare of the budget devoted to preventive health programs from its currentlevel of about 282 (para. 4.06) vo, for example, 35Z by 1995 and 402 by theyear 2000. Preventive health activities that merit additional sperdinginclude community water supply and sanitation, disease controls nutritioninterventions, and family planning. Setting of these targets and monitoringprogress would of course be facilitated by the change& in budgeting andcost accounting recommended elsewhere in this report (Chapter V and para.6.17 below).
6.14 MOH and other local government health providers could also obtaingreater health benefits from their current spending by increasing technicalefficiency in the sector. Two prime areas for reform would be the

-60-
efficiency of hospital in-patient care and of drug utilization. Regardingthe efficiency of hospital services, MOH should consider the followingactions:
(a) investigating the reasons for generally low bed-occupancy rates indistrict and mission hospitals at present, and adopting measuresto correct this situation (e.g., improving quality of services inthese facilities through additional staff and drugs, adjusting thestructure of fees to encourage greater use of lower-levelhospitals and clinics);
(b) developing policies to decongest those central and provincialhospitals which are overcrowded, by transferring patients tonearby "equivalent" facilities, reducing LOS, etc., so that costlyinvestments in additional bed capacity can be postponed as long aspossible. In general, Zimbabwe appears to have adequate bedcapacity overall, even though some parts of the country may stillbe underserved;
(c) reducing LOS in district hospitals and in selected central andprovincial hospitals to acceptable norms, through improvements infacility management, patient transportation, etc., once thereasons for excessive LOS are thoroughly established and agreed toby hospital administrators; and
(d) analyzing in detail the cost-structure of specific hospitals whichappear to be spending significantly more per admission than othersimilar facilities, so that strategies and programs forcontaining, and even reducing, unit costs can be developed. Basedon the very preliminary assessment contained in this report(paras. 4.12-4.14), one starting point for this analysis might beto examine per admission spending at Parirenyatwa and atprovincial and district hospitals in Hashonaland Central and Eastand Matabeleland! North.
6.15 Regarding the efficiency of drug expenditures, MOH has alreadymade important progress under the Zimbabwe Essential Drugs Action Program.To reinforce these positive results, the GOZ should consider the followingcomplementary measures to enhance the efficiency of drug procurement:
(a) improving MOH's drug forecasting procedures;
(b) modifying the rules and procedures for allocating foreign exchangefor pharmaceuticals, to ensure that importers and localmanufacturers under contract to GMS receive adequate foreignexchange; and
(c) developing regulations and incentives to encourage the privatesector to utilize lower-cost generic drugs.
Ongoing efforts to curb unnecessary spending for drugs which currentlytakes place because of inappropriate or excessive prescribing could also bestrengthened if GOZ were to take further steps, including: limiting the

-61-
number of drugs that can be prescribed at each out-patient visit; chargingpatients part or full-cost for drugs; and monitoring doctors' prescribingpractices for hospital in-patients.
6.16 While the modern private medical sub-sector serving mainly higher-income groups has managed to restrain increases in costs in recent years,this may have been largely the result of Government-imposed price freezesand substantial public subsidies to private care (through under-pricing ofprivate care in Government hospitals and tax benefits), rather thanefficiency gains per se. One obvious way for the GOZ to promote greaterefficiency by the private sub-sector would be to reduce progressively thesesubsidies, so that patients - and their medical aid societies - bear thetrue cost of the services they receive. Another measure would be to includemore deductibles and co-payments in medical aid benefit policies, as thiswould give patients added incentives to forgo unnecessary treatment: whilethe medical aid societies, under the NAMAS umbrella, have developed aneffective mechanism for negotiating with private health providers,deductibles and co-payments would give them an additional tool forcontrolling expenditures. A move away from fee-for-service payment to acapitation (a fixed annual amount per patient) system would prevent a majorescalation of prices and unnecessary private expenditures, but this isunlikely to be accepted under conditions prevailing in Zimbabwe at thistime.
6.17 Management of Health Expenditures. The health financing reformsoutlined above, designed to mobilize additional resources and increaseefficiency, can only be effectively realized if the health sector developsthe complementary analytical, planning, and management skills and systemsrequired. In fact, the pace of reform may be limited in some cases (e.g.,improved fee collection in central and provincial hospitals) by the extentand timing of these management improvements. In this regard, the GOZ shouldconsider the following actions:
(a) revising the MOH budget and expenditure formats, to make them moreresponsive to the needs of managers at various levels of thehealth care system, including individual facilities;
(b) continuing to decentralize responsibility for preparing budgets,incurring expenditures, and effecting payments - starting with thefour central hospitals and the eight provincial medical directors'offices;
(c) developing an integrated MOH budget which covers all capital andrecurrent items (some of which currently appear in the budgets ofother ministries) and which includes estimates of recurrentspending associated with planned investments;
(d) strengthening health manpower planning capacity in MOH, so thatthe salary implications of alternative manpower sctaarios can beassessed;
(e) improving accounting skills and systems in all MOH and localgovernment health facilities, to include a basic minimum set ofproperly-maintained account books (para. 5.16); and

-62-
(f) moving progressively toward decentralization of procurement ofthose goods and services for the health sector which can beefficiently purchased at provincial or district level.
6.18 Role of Donors. Once the Government has committed itself to aprogram of health financing reforms, the numerous donor agencies which haveassisted Zimbabwe since independence - including the World Bank - couldplay a constructive role in supporting the reform effort. Donor assistancecould be instrumental in three areas. First, donors should continue tofocus their investment resources on PHC and preventive health services:construction and upgrading of district hospitals and clinics; rural healthtransport and communications; training of rural health workers; support tofamily planning, disease control campaigns, water and sanitation, etc.Second, donors should increasingly target funds for technical assistance,training, and equipment (e.g., micro-computers) to improve financialplanning and management skills and systems. Third, as identified in thisreport, a number of additional studies in health financing may need to becarried out, for example, to investigate bed occupancy rates, LOS, and unitcosts in selected hospitals. Donors should be prepared to provide technicalassistance and funding of local costs (including use of Zimbabweanconsultants) for such studies. As part of a comprehensive health financingreform effort, an action plan could be drawn up covering technicalassistance, training, equipment, and other needs, and a suitable budgetprepared for submission to the donor community.

-63-
ANNEX I
ZIMBABWE
POTENTIAL IMPACT OF HEALTH RESOURCE MOBILIZATION MEASURES
Measure Annual Incremental Revenues(Z$ millions)
Adjusting current fees to match inflation 7
Assumes user fees, which have not beenadjusted since 1985. reflect the 88Zincrease in inflation over that time period.Fees collected in 1988-89 are estimated to be$8.77 million.
Full cost pricing for private in-patients 15-20
Assumes Government hospitals bill (and collect)20Z of total medical aid payout for hospitalizationrather than the current 3.5X.
Standard out-Patient fees 10-15
Based on 5 million actual out-patient attendancesat clinics (1988), charging a standard $1.00 fee;and 4.33 million out-patient attendances atdistrict hospitals, charging $1.50-$2.00 per visit.
Druz charges on a per item basis 10-15
Assumes drug charges cover, on average, 502of MOB drug expenditures ($27.3 million in 1987).
TOTAL 42-52
Sources World Bank estimates

-64-
AhNEX II
ZIMBABWE
REGISTERED HEALTH PERSONNEL -- 1986
Medical Practitioners lt57Dental Practitioners 124Pharmaceutical Chemists 318Opticians 15Dispensing Opticians 13Physiotherapists 88Speech Therapists 7Radiographers 109Occupational Therapists 27Prosthetists and Orthotists 16Medical Laboratory Technologists 141Health Inspectors 97Cyto Technologists 5Meat Inspectors 38Dental Technicians 24Dental Hygienists 13Electroencepholograph Technicians 5Nurses 9206Chiropodists 14Dieticians 13Trauma Medical Assistants 41Pharmaceutical Technicians 107X-Ray Oper3tors 26Rehabilitation Assistants 94Med. SCE 11HLTA 144Village Health Workers 1384
Source: Ministry of Health data

-65-
ANNEX IIIPage 1 of 2
ZIMBABWE
FEES AND CHARGES FOR VARIOUS HEALTH CARE SERVICES
Ward Fees (per day)
I. Parirenyatwa Group of Hospitals, U.B.H., Harare. and Mpilo
Private wards $60Private wards (non-resident) $80General Wards (Adults)
Monthly Income$151 - $300 $ 5$301 - $400 $10$401 - $500 $15$501 - $600 $20$601 - $700 $25$701 - $800 $30
Over $800 or with Medical Aid $35
General Wards (Children)Monthly Income
$151 - $300 $ 3$301 - $400 $ 6$401 - $500 $ 9$501 - $600 $12$601 - $700 $15$701 - $800 $20
Over $800 or with Medical Aid $25
General Wards (Non-resident) $60
II. General and District Hospitals
Private Wards $35Private Wards (Non-resident) $50General Wards $10/day for first 14 days,
$5/day thereafterGeneral Wards (Children) $3/day for first 14 days,
$1.50/day thereafterGeneral Wards (Non-resident) $30
III. Rural Hospitals
General WardsAdult $ 2Child $ 1

-66-ANNEX IIIPage 2 of 2
Outpatient and Casualty Fees
I. Central Hospitals (including Harare and tpilo)Public Health Consultant Attendance
Monthly Income Under $800 $ 5Monthly Income Over S800 orMedical Aid $13
Dressings $ 5Injections
By doctor/nurse during consultation $ 2.50Outside of consultation $ 5
Occupational therapy $ 5.55 - $10Yellow Fever Inoculation $ 5
II. General HospitalsAdult $ 3Child $ ;;50
III.District HospitalsAdult $ 1.50Child $ 1
IV. Rural HospitalsAdult $ 1Child $ 0.50
Operating Theatre FeesCentral HospitalsMajor operations $50Minor operations
general anaesthesia $20local anaesthesia $10without anaesthesia $ 8
ICU/CCU with Medical Aid $80/dayHemodialysis $44.15/treatmentPlaster of Paris Treatments $10
Maternity Ward Fees (per day)I. Central Hospitals
Booked Cases $20Unbooked Cases $30Non-Residents $175
II. General Hospitals (including Hara-' and Mpilo)Direct Admissions $15Transferred Cases $7 - $12
III.District HospitalsDirect Admissions $ 7Transferred Cases $0.50 - $6
IV. Rural HospitalsBooked Cases $ 3Unbooked cases $ 4
Sourcet Ministry of Health data

-67-
ANNEX IV
ZIMBABWE
MEDICAL AID SOCIETIES' ANNUAL SUBSCRIPTIONS, 1987-88
SOCIETY BENEFICIARIES
Anglo American Medical Aid Fund 1,097Bankmed 7,965Beverley Building Society Medical Aid Scheme 360Building Industry Medical Fund 1,238Cement Medical Benefit Society 393Chibuku Breweries Ltd. 910C.I.M.A.S. 127,389Engineering Medical Fund 12,878Harare Municipal Medical Aid Society 6,825Industrial Steel & Pipe Medical Fund 747Legal & General Medical Aid Society 899Lonrho Medical Aid Fund 3,250Manica Medical Aid Society 910M.A.S.C.A. 9,813Motor Industry Medical Fund 2,065Municipality of Bulawayo Medical Aid Society 5,740Northern Medical Aid Society 4,767Oxyco Group Medical Aid Society 604Prudential Medical Aid Scheme 503P.S.M.A.S. 101,720Railmed 43,568Rio Tinto Group Medical Benefit Society 1,300Shell/BP Medical Aid Society 1,473Triangle Ltd. Medical Aid Scheme 1,503Turnall Medical Aid Scheme -Union Carbide Medical Benefit Society 2,085Workers Compensation Insurance Fund -Zimbabwe Newspapers Medical Benefit Society 1,373Zimglass Medical Aid Society 329Zisco Medical Benefit Society 8,8'.5
Total 369,385
Source: N.A.M.A.S. data

ANNEX V-68- Page 1 of 10
GOVERNENT NOSPITALS ACTIVITY ANALTSIS euM?Y 196
* SWd Bed Irpetints Avera" Out OutpatlentEstablishment Occ,pacy OCct.upwy Ad4llans Dislchar9es Sally Stay Patient and Clinic
Rate Avere SCays) Cames Attendance.................... ........................................... , ..... *.....................
NanicalwwProv/DIst/1uWat hasp 1129 38243 To 42614 36452 790 6.7 2"69? 522202
Nashonalond CentralProvJDlst/Ruta hasp 381 10667 S7 1962 1267 301 5.6 216284 ?4r19
Nashonaleld EastCentral Nosp (Narern) 156 437210 9r s0M2 00106 119S 7 129059 265006Centrat Hsp (Part) 901 25332 87 31910 30541 782 6.9 112496 1T1203
Sub-totat 21s? 722592 92 94312 91027 190 7.7 24155s 436209
Prov/Dist/Surat hosp 610 2ROM? 6 35267 33618 SS4 5.7 19905 409369
Total Nash. East 2967 924799 8 1299 1246 253 7.1 440630 84SS78w"Ims ~ ~ ~ ~ ~ ~ ~ ~ ~ m
Nashonalad vstProv/Dlstlturat hasp 1135 294606 71 m4235 42962 so7 6. 356m 7388120
NasvinfoSp. Hasp Nhmkura 332 92480 76 334 229 253 277 7618 12140Prov/Dst/Rural hasp 810 240999 61 3946 3s591 60 6.2 233267 694923
totat masvngo 1142 333479 so 39230 3420" 913 8.5 240885 707063
matebelelard NorthCentral Hasp USN 651 156800 46 141S 17486 429 6.5 434S2 53564Central Nosp p1ito 937 341090 100 43303 41346 934 7.9 141014 31904
...............................................................................................
Suibtotal 155 49790 66 61718 56752 1343 6.1 164466 372612
Spec Hasp Ingutahini 670 235409 96 157 692 645 149.2 2946 3369Prov/istJRuratl bhap 474 691M S1 4403 124S9 244 6.2 119496 308349
....................................................... ....................................................................
totatl Nt. North 2732 322453 82 77499 7T9M3 22S2 10.6, 306910 664330Rss= a _ _ _ _ S_ _ _ _ _ *-U*U--
NatahaleLnd SouthProv/Dist/Rural hosp D45 l61527 61 24767 20631 SI5 7.6 1563S5 371151
NidtandsProv/Dst/Ranl %_P *iM 261343 56 50456 46123 716 S.2 246813 5889O3
GRAID TOTAL 11619 3223349 76 432619 399246 860 7.s 2260511 4832816.

-69- ANNEX V
Page 2 of 10
OSPITAL ACTVItI ANALYSIS 69 HOYIMCE - 6 -(Test Ending 0ocn- 1W9)
Central lod Sod AdiesIens Dischars In patients Avorae bot patient Out patioNoepitate Establishnt Occwcy Dily Avere Stay (Da") Caam d Clint
Attncde...........................................................................................................
United UulteoHospittate tIN SO9 14201 1SS2$ 1422 369.2 9.1 43S2 S356
Apitlo:aart l 25 2S74S1 26766 271 M.3 6.9 14011 316592TSB 120 30219 249 46 62.8 121.4 503 2456
H raro:Geral 96 336 41067 382 928.S 8.2 119M 2S5 9Psychic 110 34446 1685 1716 94.4 20.0 9Y#S 10167
Perirenyatma 632 264919 2666 25615 725. 9.9 112496 l1203
............................... ...........................................................................................
TOtAL 3342 10M799 114156 10W 9.4 426021 $08l21...........................................................................................................
Waternity:
tiN 42 14)52 2690 28OW 40.4 5.1pi lo 92 53420 14266 13786 146.4 3.9Narare Ise 63906 19650 1 161 175.1 3.2Pertreny tus 49 20413 5046 5226 55.9 3.9
TOTAL 403 152493 41674 41546 3.7...........................................................................................................
spitl opitats:............
PsychietricsUgina u 332 "M480 3$ 229 23.4 M 38 7618 12140Inguthni 670 D 54U9 1576 492 645.0 319 2948 3369......... ................. ...................................................... ...........................................................................
Please note that irsof ton contained In this tableIs not co*lot* f.e. an to fawt mnths my be misaliu or nil retuwn has be reeved.

ANNEX V-70- Page 3 of 10
led l,d AdisuIons DifchCrges In peticnts Averw Out pet:int Out patientEstabltia-_nt OccWinsy Daily Average Stay (DOYS)C4M5 aN Ctinic
Attendmnces
Provine Hospitals.............
e Geeralloutere 171 66169 10541 10002 181.3 6.3 65106 1235"- MaternityNutar* 1 11002 309 ZU 30.1 3.9District Hospitals:.............
GeneralRUN" 257 63590 680r 6011 174.2 10.1 46116 6742Clippiru 135 49109 6067 4707 134.5 9.6 429 41051ya1g 90 2360 2522 2123 ".6 10. 22219 36070
Saku 102 27626 24? 2267 75.7 12.1 5002 5950
51- 5s7 16395 17543 S1O1 110.1 6.5 116033 174867
- Materni tyRua 27 T75 2614 2033 19.3 3.5Chipirnw 30 934 1424 1267 25.6 7.2my"" 18 2475 506 462 6.6 5.1.................... .............................................................. ... ... I..................................................................
SO-TOTAL 75 160 4344 3602 .2 5.3
wrat Nospitats:..........
* GeneratSlrcheo* Srid 26 4193 937 9V. 11.50 4.40 16223 37611iri uIrn 34 6200 255 24 17.00 25.20 4659 11779WIher 34 2225 52 55 6.10 3.60 13146 28S70
Nakni 14 91? 5 479 2.50 1.90 14040 27817urn 34 6575 1159 96 16.00 6.70 $166 33316
lledmeko 30 12a 690 45 3.50 2.00 O97 20301ywwai 25 12 95 353 3.50 3.60 80 28649
Wm 15 12U 844 610 5.00 2.20 14965 33704
SW-TOTAL 212 24506 S36 5041 6.4 6.2 90556 223755........................................ ...................................................................................................................
* Maternityirchnough grid 9 53 293 279 1.5 1.9
Sirl Wiri 6 246 46 0.6 4.9tber 7 100 103 104 0.3 1.0
Nakoni 11 411 367 356 1.1 1.2lNwwinp 9 150I 269 246 4.1 6.1lldtumdbo 3 216 216 216 0.6 1.0Myanyadal 8 a36 69 46 1.1 5.?Wmys 10 341 3s 342 0.9 1.0...................................... .. ............................................................................. , ,.., ............
SB 0*TAL as 319 171 1659 1.3 2.9........................................ .......................................................................
Totat Cnl 973 254662 3370 30151 6.1 29167 522202

-71- MANNEX VPage 4 of 10
PASIOULA CENTRAL............. .............. Out patio
led led Arission DIschargs In patints Average Out patient ud Clintastablishment Occupancy Oeity Avera" stay COeys Caes Attendanc
.............................................................................................................................
Province ospitalte..................
- G4enerllindjra 102 *4712 554 $129 1225.0 .4 7332 59114* ternity
18 9069 1345 1321 24.J 6.9District Hospitase:........... ............. ...
- GenwerlConcession 49 11209 2727 27 30.7 4.0 34762 69935Mt Darwin 42 23629 2600 20"9 64.7 11.2 554SS 04920.... .........................................................................................................................
SUB-IOTAo 91 34183 5327 4122 336.3 7.63 90248 154811...................................................................... t.............................
aternityConcession 16 3006 8J0 744 8.2 4.0Nt Darwin 9 886 8B5 ur 2.4 1.0.... .........................................................................................................................
SUOBTOTA1L 25 3892 1765 1631 5.3 2.5
.........................................................................................................................ara w Hospitals:...............
Curuve 39 2096 539 516 5.7 4.1 7873 14088Nudziwa 32 1770 71o 651 4.8 2.7 21379 39165Ro" 24 50 428 426 4.1 3.5 2245 3836
vh 32 9592 2240 2143 26.3 4.5 37046 69130...................... .......................................... ..............................
SUg0- JtAL 12r 14956 3917 37M 10.2 3.7 85754 160747.............................. .............................................................................................................................
M aternityGuruve 6 178 16? 167 0.5 1.1Ntaiu 3 1134 621 531 3.1 2.1tso 4 358 253 20 1 1.4Shows S m 68 65 2 1.1.............................................................................................................................
So-TOTAL Is a9 12 1436 1.7 1.4
Total e Cwral 320 94508 14788 4379 258.9 6.5 2162t 3747`19Total - aternity 61 15359 49 4585 42.1 3.3

-72- ANNEX VPage S of 10
PASIOIALAi EAST............. ... --- 0d A...aaIn 0isrge In patilntc Averao Out patient Out patio
Istobl Oetup eitly Average Stay (Dayo) Cuss VW Clln1Attsn
...............................................................................................................
Province Nospitals* Gemrsl ..............Chitungwiae 1V1 50106 693a am 137.3 5.6 36122 55413Nerarnderc 164 60305 4077 6099 165.2 9.4 30679 San3...............................................................................................................
SUW-TOTAL 335 110411 15009 1424 151.3 7.5 64801 114150...............................................................................................................
* paternityChiturqwlaa 102 16614 5678 5557 3.0Marcmdere 16 7160 1610 1639 19., 4.4...............................................................................................................
SUW-TOTAL 118 2374 7361 7196 32.6 3.7...............................................................................................................
Olstrict Hospitals:- General -----
NukLbi 44 19020 1275 1037 52.1 18.1 13666 17m
NuseNutako s0 21440 3 200 9 S8.? 7.2 2546b 63097.. v ........ *sv .............. . .......................................................
SBWTOTAL 144 40460 4555 3926 55.4 12.? 39132 82670....................... ............................................... , .o.................
* MatetnityNukXubi 13 241 233 233 0.7 1.0Nurewa
outoko 12 2331 1460 1457 6.4 1.6,...............................................................................................................
SW-TOTAL 25 2572 1693 1690 3.6 1.3....................... ............................................. **.*.......................................
Rural HospitalstCGneral .............
*.trioe 23 67 171o 1452 10.4 4.6 2499 46451Chi kmok 24 53J6 1102 1152 14.8 4.7 14616 61432Chioto 31 690 244 226 1.9 3.0 6J62 12963Nakaa 30 6457 915 m 17.7 8.2 13748 35991MyszAle 13 105 269 2S2 2.5 3.9 15089 32042Wdas 2J 2a0m S5c 494 7.4 5.5 16036 23450...............................................................................................................
SUB-TOTAL 144 226t 4*90 4361 10.5 4.S 93942 212549...............................................................................................................
- Maternity
Beatrice ? 341 I91 391 0.9 0.9Ch1ibakma 4 629 361 354 1.7 1.Jchiota 11 2 131 126 0.8 2.3Nakos 10 243 250 250 0.7 1.0yoaltue 2 196 201 201 0.5 1.0wuda 10 307 335 299 0.8 1.0...............................................................................................................
SW-TbTAL 4 2006 1669 1621 0.9 1.0........................................... ...............................................................................
Trtal - Geeowal 6ZS 1T75M5 24544Total - ateornity 16s 28352 lO101

-73- ANNEX VPage 6 of 10
MAIMMNALAD M11 Rd led Atisaim OldwrueI gtnsteiU rAwsp *A p551gMt Out patfnt......... . G btliehmelt Oe way Daily Awrastay (Dta) cases wd Clinic
£ttadeI....................................................................... .....................................................................................................
Pr.vi0eJ kepits* Geral ..................Chiroyi 156 4326 r50 5943 121.A 7.1 566 148
- MaternityChirayl 19 11601 1039 1914 31.8 6.1
District Hospitats:- GeneralKadam 248 5651 67 0 16.0 9.5 51040 116141shkat 47 17T81 3164 1a32 49.0 5.7 am900 4210?
Chgtu 43 21400 3447 271 56.6 7.6 13415 61653Karlbs 90 2076 2 279 56.6 .S 1742 25673
aro 106 4745 5s 470 122. 9.1 26766 54174................................. .............................................................................................................................
US-TOTAL 5S34 1554 21324 19111 8.3 T.5 158943 319748.............................................................................................
- MaternityKadms 24 9214 3020 5T4 25.2 3.6sn&.t S 609 610 597 1.7 1.0Chlautu 12 445 1740 1569 12.7 3.0Kariba IC 2073 426 540 s.? 3.8Karol 24 13512 145 154U 37.0 8.7
~~~~.............................................. I...............
SU-l^otAL 75 30043 7424 66o 16.5 4.0..........................................................................................................................
tural Hospitals:enral ................
Oarwele 40 468 1091 n50 12.8 4.8 17561 38m25Wirunpes 50 5210 1502 155 14.3 3.4 2486 250Ilherdoro 33 2427 S17 Xl 6.6 4.7 204" 37536mu_ i 3? 8706 U9 907 23.9 9.6 16749 22714Ugezi 49 393 7 713 10.9 5.6 17426 26047laffinor 38 5926 1035 694 16.2 6.5 19060 35579Zvim 55 6164 9o 706 16.9 8.6 2U616 53m.............. .................................... ................................................................................................
US-TOTAL 302 37054 6706 65 14.5 6.2 143124 270624..........................................................................................................................
* MaternityDarewAle 10 211 167 164 0.6 1.3Hurmne 2 343 37 340 0.9 1.0
ordoro 10 454 37 351 1.2 1.3_{omi 3 197 199 199 0. 1.01t92i 3 176 173 178 0.5 1.0R1ffingora 6 254 269 2m 0.7 0.9Zvib 5 75 709 "S 2.0 1.1Morton 10 W 95 ns 12.8 5.9...... ....................................................................................................................
SUI-TOTAL 49 7030 3235 n9u 2.2 1.6
*otal Genertl 992 245934 35537 3159 675.8 7.6Total . Mternity 143 474 1269l 11723 133.3 4.1

,? 6o0 050 UKc nu3 f9 W=i-S
Z'l tl't i" 5 15 t 01aNsVI 01t 633 EU 611 Ot nan9' 0.1 OR1 @2 OK 9 91S1U11131-1 Olt 6a 6o 11 GU1 9 Au¢
Cs9 O*t "1 at 9 £9 3 SOMPOO9l 5-0 0t a9 "t 0 rq0143
01165 33513 15 I'll 1901 3911 0595 61 ~ ~ ~ 6010 su
63 I0D W IL 1 9 Sallie
Asiume am -
.......... ..................................................................................................................
315139 11631t tot 6t1 695 £19 1403 11 63)116I
................................................ ........................................... ,,......
0°166 t1s S'll £U1 193 Om 6101 1ttSJ61159 09# 2' lt VI Wt Mt gmOft9ZR at- I' es 9" in ate2 et
AaL zt SW& 1 tst Ato 69 mg 9 s 041AM1
0Om9 9105£ 1. 9W19 3913 9611 11901 563 iqnWLOL
osoz Zia& Olt 915 "O L3 M9t 9 JIAUlN
9131uJ3sfl
099 t11039 **S S9U OS 39 66 6UIAflWleilk"
.. . .. ~~~~~~~~~~~~~~~~~~~~~~~~~.......
A1tu _te .
............................................................................................................................
campe "ause .sM Vma)5UE wa saqt ai n1.'II VLLW
............................................................................................................................
We# "tO 6'st tAS osi dolt 96MK 01mm
e * 01 10D £ e ned
Amt us t1 *N9t NVt
60m& sum 6 s *40 "a "at 1" uns t
............................................................................................................................
3|1U11 P op _ao Ati eta AXl ISO AmbM tomp8$2wsed v al u w e Sr om* MnMt SOU"1 bo lnm pe P .........
OT °O L 029dX-4NNV~ ~ ~~~PL

99190 MM61 III 1113i 396 atilt 39141 1to lejaum
..........................................................................................................................
*-9 got 9'1 6M6t 91t 09 W -o
* tto m u Not I 1"401e49LI's 6'9 "I a vio l t dedsMs ?I a a ot I WWS
Al 61t I1s 19 Ot9 t 9o9 16 t19 "3 16 9 ISW19lt Olt 9 GM In * s*i1o
9t VS 393 at 1ilt 9 AqlA
......................................................................................................................... I
YOM1 49m9 Ile 9.03 1065 9311 969 993 19101-US..........................................................................................................................
O1669 610t 5*9 Ile *Kt 6tt1 tOZ6 £5 WI$39191 MO9 Ile 9Olt 91 on 31t 1 WmSs30t09 6£ Z1 9o91 13 3M1 5 uABlE
5t91s 315 V6o 9f 99 m 9 199 s1s 5l53913 £991 69 VO 31 o69EL 3061 rt S*inai
.~~~~~~~~~~}
198 59 559 099 6011 o6
S9015 13Sf 691 zlIZ GU6 "1 9m13 AlI oil- a
...........................................................................................................................
~~~~~~~tOtWA D- 1 gm " tEt IVA01-o.................................. ........................... II........................................... ,,,..........,....
95991 05121 6- Cl! 199 191 3101 U A'oeu^£6131 51101 0'1 01 43 011 0339 59toS"Ott 1 SN
:lsaldsoM auis aio
s-N
..................................................................................................
uluI,dsoN *a1IAJd
..................................................................................................
91u11 IR ub s aAuo Asi as.aA A" A" A3fhia@ 1uI'AI11A
01 JO 8 a 8 'dA X3NMV

-76- ANNEX VPage 9 of 10
NATAELEAD $UUTN.......................... SW ed Adesi is In patlugtg Averp Oe t patlent Out putlmnts
Esteti e"m t 0spou Saflty Averag Stay (Cane) Came wd CtinicAttdoe ae
............................................................................................................................
Proui1 NospitalsG ra ..................
cGua 116 32 300 am 6.7 12.0 300 34369
* Noternityandsl 23 9143 174 1 25.6 4.9
Diterict Hospitats:* nrat ..................AntelWo Nine 8 32072 241? 14Z7 67.9 1.5 16027 36Soit Bridge 36 7305 1676 1570 20.0 4.6 21136 101594Esiodini 9 IM 1629 15n3 22.8 5.2 940 244Filaui 86 20493 1318 m 56. 21.6 11431 29Ke:i IT 4367 44 412 12.0 10.6 195 14246Plustree 64 267! W4 29MT 76.6 9.5 2668 si57............................................................................................................................
SUBTOTAL S0 10126 11460 m 46.2 9. 9359 259178............................................................................................................................
* NaternityAntelpe Nine 22 5492 107 517 15.0 10.6Solt Brids. a 2239 109 1069 6.1 2.1Esigodini 11 Z36 332 322 6.4 7.2Fitsbus 12 3490 69 719 9.6 4.9K*zI 4 427 95 69 I.? 7.0Ptuatree 6 32 728 715 2.0 1.0
SS-TOTAL 43 140906 3740 3431 4.0 4.1
turat Hospitatls:CMrst ................
Avoca 48 4531 768 7 12.4 6.3 1656 26452Lady Barirg 53 2121 547 427 5.6 4.9 6934 19517Lady Stantey 52 1315 414 9 3.8 3.5 6886 1i212Natabo 30 659 81 648 19.1 10.1 4079 7241Shanqani 42 4457 57i 514 12.2 8.6 791 1202................................................. ................................................
SW-TOTAL 25 194 3107 2736 10.7 6.7 42456 77404
* ternityAves 6 4610 359 369 13.2 13.0Ledy saring 3 131 a2 56 0.4 2.3La Stantley 4 s 49 47 0.1 1.1Natbo 6 2a 172 160 6.6 t.2lpnu. 4 Is5 159 158 0.4 1.0
SO-TOTAL 2a 7574 61 92 4.1 6.3. .....................................................................................................
Totat Ga- erlt 731 156704 14a 1467 429.3 11,.6 1S5357 711S5Totat Nternity 114 31823 605 6143 .2 5.2
Totat 845 16s2 24767 2030 15s57 371151

ANNEX VPage 10 of 10
......... . . . .led Ad issiuw D aIg In pat1nts Aver" ut patient Out patients
ftbUs'n Ocuac oaty °vra h1S 'tW (00") CG Z Clinic.
Attendies.. .. ,........ --...... b.................................... ............... ....................
Province Nietas* enral .Gtmru 210 5ao7 15669 1010 ¶55.6 5.2 6631 ¶18S
* MaternityGweri 44 944 366 373 53.3 5.3
District Nospitals:Grst ..........
Chi.u 55 7501 1361 116 20.6 6.1 517m 10627two 1W. 232 56769 9l1 7m 155.5 7.0 3614 101063Cook.. 93 3646 944 49 6.2 6.6 40235 12S5Marena 37 291 374 334 6.2 3.4 360 11%38NVR 110 6005 1913 1700 21.9 4.7 1790 66143Shurugwi 62 ¶473 1337 10lO 39.7 11.6 17659 26642Zvi$Mvse
SUB-TOTAL 609 1264S5 19209 1416 70.1 6.3 121448 341897............................................................................................................................
* MaternityChivtu 1U 1137 306 296 3.1 3.6Km tK 63 13064 3312 2MG 35.6 43
CGok a 6138 3736 3511 16.6 1.6eXrenpa 3 671 215 1" 1.6 3.6
7 977 *23 396 2.7 2.Shurugqi 24 791 774 60 21.6 11.9Zvi shaven
SIX-TOTAL 119 29011 a16 6243 13.6 4.7
Rural H"pitals:* Genral Chiligmui 46 269 471 45 7.4 6.2 T996 15662Lurdi 56 26 1048 631 26.1 ¶1.4 7391 16506Uharira
Seda 40 1191 653 *2 4.9 2.6 6446 13864Si tobetl 43 3597 2601 1861 9.9 1.9 26141 49600
Zvmbande 49 6256 1191 1142 17.1 5.3 10060 32459..........................................................................................................................
VA32SOTAL 56 564 594 am2 13.1 5.5 56534 128473..........................................................................................................................
- MaternityChi nimnu 13 l11 57 53 0.3 2.1Ludi 2 a2 60 is 0.2 1.1NheriesSea& 2 160 159 159 0.4 l.0Sitotel 43 1162 925 3.2 1.3Ztvba nde 1O la 1326 ar5 3.6 1.5.............................................. ............................................................ _
SA-TAJAL 70 2M40 2152 2072 1.5 1.2...........................................................................................................................
total Genral 1055 209S6 34063 32105 57.0 6.3Total * Maternity D3 521s 4 616 14015 143.0 3.7
Grnd Yetotl 128S 261343 50on 4615a 244613 58953

- - - - - - - - - - -'. -1 , - - -,. .. . . .~~ ~ . . . .3
-i-- -l - . a-- - - - - - -o -- -* * .," " .-. , , , .S .S . I. .. . . . . .~ . O . .~
- - - - - - - - - - .ii..~ 5 .......... _ ..... .if. .. ... ..... _ .. ............... sO .. ........ ... ...... ....... ... ~ I... a ~ ,. .. .. a a a as a.-'if a.if--ifa a
|~ I z!~ I fi | i
if .. 00 n * " " " " " .. a a a a if" .. " . s
: : : : : : : : : |~~~~~~~~~~~~~~~~~~~~~~~~~~~~ :
.... .~~~~.. ifi a , ... , ,-
*. 0. 0 0 S S I. SIx
.E ~~ . . . . . . o:30ol
s ff~~~~a,,~~~~~~~~~~~~~~~~~~~~~~~~~~~~

~~~~~~~~~~~~~1~ ~ ~ ~~~~~~~~1
=~~~~~ - - ^ - Fg -K r - ^ ,' - - - - t - g - | {S - f S - _ - g - - -
- I - - -- ,. - - - -
7 4 * 4
.. ~~~~~~~~~~~~~* a. X. a .
* .. . . .. .. 4
.~ ~ ~ ~~~~~ - -& - - -1 - - -- i- - - -- --
- - ----- --- : -± :
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~0 .9
- - -- --- - -- - -- - a - a - -a - a- - 4---
- 0 9- - - i 2 - - - - s - X X - - - - - - - - --
a a a . a . a a a a a a a a a a a a .. - - a a - -a - a - ..- a .- - a . a - - -
'!'

-4. . 3-4*oWlf , t ,-|. _
" "" " "" " . "- *- g *-. * §
a '. 3
w ;to"OtI" 0t8't-'-
__*@@@4 *@ ***- @0-rn@ U I - * 4
% 3. S.Z. .... - 2 S
" _ " " " " " " " " X " " " " " " " | t * 4 | i .
* .4 3 -3|o S.X. 2t,
_~~~~ - ............... ... ..____...._ - - - - - - .' -
i~~~~~~~' W' wiliE§e -A G3§g ..
, a .4 - .... --- - ---..- n .. a -- -... - - - - -
- - - - - - - - - -
.......*........... 4. . ............ ....................................... ................. ...... ............ -................... a......... ..................... ea
- 4 0~--- ---
a a ace a -s - - -a -a- - - - - n - ----
4111
f 4~~~~
'A 0. 0 .I-

* - 4 I * S3
* ' a 9 fii XY9 'ii''* | '
* * "sywt¢_w ow8 . :s8$ 2£.
_ _ __ _ __ " "_ _ __ _ _ _ _ ." __ _ "* 4 a a
o 4 S am S 4C
= 0
a a a a a a .. 4 a a .... a... a .... a - a - - - - - - - - a - -*-4
* 4 @* * £- - - - - - - - - - - - -- -- - - : {
- a. .4.4a *.4.4a..4.. - "UG ...... - - - - - - - --
" ~~~~~~~~~~~.. a...a .4.4 .4.4 . . *4. 4.4 i .4 -
E |E§N"g.13aZ* e a lwX. ol
4 ............ .. .. .. Z .. .. - : >
a.. .4.4.4.4.4.4.4.4 a aa a 3~~~~~~ UK~.W.
- - -- - - - - - - - - - - - - -~~~~~~~~~.4.444 - -4 4 -.. - . a-.- a - --4. --

16RD17026v- ' W *^NtANIA $ ~~~~~~28- 30. 32.
Z IMBA BWE
OCA4 $M ZA A 8I
lU)
O BOdlWvAA \- IS N
b R- UlH <'is'S /Fa/'ffl's .E S TZ I A~L N
T~ ~~~~~~~~~~~r Lurka
-I l l¢rrh dnSAH A T,A A ABN D r
,o-"~~~~ ~ ~~~~ A9H N M A N I -- A L D -
NI., JR TS
Llt , bh , .. Bal A T R A L--- .7
m 8'\ A T A B <d< N D t\ a RDcbff b'l I DOLA Be A )& ' AA
B-d.,.., S O~~~~~~~~~~~~~~~~ OA TDAS'H1
T2fr2'dAIAI \ IS\ 225
Hard 5 0E00RS B O T S WAR o M O Z A M B I Q
kIOETR ALf..d. I. M.Irl~ Ao r* AWI 8'EAAN3 L B DJ4'-
ILE 0 .0 100
--1- - roSOUTH AFRICA260 28- 30- 32-
MAV t9/