Repair of pulmonary vein rupture after deceleration injury
3
to which he succumbed. At that time the chest roentgen- ogram was clear and without clinical evidence of rejec- tion or infection. Comment Ectodermal dysplasia is a rare condition involving abnor- malities of the ectodermally derived tissues such as the skin, hair, teeth, and nails, with an incidence estimated at 1/100,000 live births [4]. As many as 117 varieties are thought to exist; however, the most common type is hypohidrotic ectodermal dysplasia, named for the com- plete lack or significant diminution of eccrine sweat glands [3]. This condition is thought to be an X-linked trait, as males are overwhelmingly affected with the complete syndrome. The patient presented here exhib- ited a number of the classic signs and symptoms of the disorder, which variably include thinning or sparse hair, frontal bossing of the skull, periorbital hyperpigmenta- tion, prominent lips, abnormal dentition, and chronic fevers secondary to an inability to autoregulate skin temperature. Pulmonary complications are frequent— approximately 30% of all affected males die during the first 2 years of life secondary to either hyperpyrexia or pulmonic infection [2]. In the classic study by Clarke and colleagues [3], 52 anhidrotic ectodermal hypoplasia fam- ilies were evaluated. Forty-four percent of children were noted to suffer from severe recurrent respiratory tract infections, and death due to the sequelae of these re- peated insults was common in both children and affected adult survivors. Although no consistent abnormality has been noted in either B- or T-cell function, an associated immune deficiency has been noted with this condition [5]. In the report by Clarke and colleagues [3], the most common abnormality noted at assessment of humoral immunity was elevated IgM concentration, and this was also noted in the patient presented here. Although im- mune abnormalities are variably noted, the increased susceptibility to pulmonic infections is thought primarily to be a result of abnormal mucous gland (absent or hypoplastic) development in the lung [2]. The discrete molecular genetic defect for ectodermal dysplasia is not known; however, by linkage analysis the affected gene for this disorder has been localized to a region on the long arm of the X chromosome (Xq12–13.1). A recent study has noted that fibroblasts from affected patients exhibit a significant decrease in binding capacity for epidermal growth factor, and a decreased expression of both the epidermal growth factor receptor protein and mRNA [6]. In summary, a case of lung transplantion for a patient suffering from end-stage pulmonary disease secondary to anhidrotic ectodermal dysplasia is presented. Lung transplantation was successful; however, the patient eventually succumbed to a nonpulmonic infectious pro- cess. A disease with a similar clinical and pathologic (Fig 1) presentation, cystic fibrosis, is actually the most com- mon indication for lung transplantation in children, and results to date have been quite good [1]. Pulmonary disease in infant males with ectodermal dysplasia less than 2 years of age carries a particularly bad prognosis; therefore, the option of lung transplantation in this group should be considered as early as possible. The potential long-term impact of various forms of the associated immune deficiency is unknown. References 1. Noyes BE, Kurland G, Orenstein DM. Lung and heart–lung transplantation in children. Pediatr Pulmonol 1997;23:39– 48. 2. Masse J-F, Perusse R. Ectodermal dysplasia. Arch Dis Child 1994;71:1–2. 3. Clarke A, Phillips DJM, Brown R, Harper PS. Clinical aspects of X-linked ectodermal dysplasia. Arch Dis Child 1987;62: 989–96. 4. Stevenson AC, Kerr CB. On the distribution and frequencies of mutation to genes determining harmful traits in man. Mutation Res 1967;4:339–52. 5. Brooks EG, Klimpel GR, Vaidya SE, et al. Thymic hypoplasia and T cell deficiency in ectodermal dysplasia: case report and review of the literature. Clin Immunol Immunopathol 1994; 71:44–52. 6. Vargas GA, Fantino E, George-Nascimento C, Gargus JJ, Haigler HT. Reduced epidermal growth factor receptor ex- pression in hypolidrotic ectodermal dysplasia and tabby mice. J Clin Invest 1996;97:2426–32. Repair of Pulmonary Vein Rupture After Deceleration Injury David Varghese, MBChB, Hitesh Patel, FRCS, Ewan W. J. Cameron, FRCS, and Mike Robson, FRCA Cardiothoracic Surgery, Royal Infirmary of Edinburgh, Edinburgh, Scotland Injuries to the major pulmonary vessels are uncommon and are extremely difficult to manage. We report a case of an isolated pulmonary vein injury following a road traffic accident that was repaired successfully. (Ann Thorac Surg 2000;70:656 – 8) © 2000 by The Society of Thoracic Surgeons I njuries to the major pulmonary vessels resulting from blunt chest trauma are uncommon and when encoun- tered pose difficulties in management. An isolated injury to the pulmonary vein as a cause of a massive hemotho- rax is extremely rare. We present the case of a 43-year- old man who was admitted to a peripheral hospital after suffering blunt chest trauma. Subsequent thoracotomy revealed a torn left inferior pulmonary vein which was successfully repaired. Accepted for publication Oct 20, 1999. Address reprint requests to Dr Patel, Department of Surgery, Chelsea and Westminster Hospital, Imperial College School of Medicine, 369 Fulham Rd, London SW10 9NH, England; e-mail: [email protected]. 656 CASE REPORT VARGHESE ET AL Ann Thorac Surg PULMONARY VEIN INJURY 2000;70:656 – 8 © 2000 by The Society of Thoracic Surgeons 0003-4975/00/$20.00 Published by Elsevier Science Inc PII S0003-4975(00)01199-1
-
Upload
david-varghese -
Category
Documents
-
view
214 -
download
0
Transcript of Repair of pulmonary vein rupture after deceleration injury

to which he succumbed. At that time the chest roentgen-ogram was clear and without clinical evidence of rejec-tion or infection.
Comment
Ectodermal dysplasia is a rare condition involving abnor-malities of the ectodermally derived tissues such as theskin, hair, teeth, and nails, with an incidence estimated at1/100,000 live births [4]. As many as 117 varieties arethought to exist; however, the most common type ishypohidrotic ectodermal dysplasia, named for the com-plete lack or significant diminution of eccrine sweatglands [3]. This condition is thought to be an X-linkedtrait, as males are overwhelmingly affected with thecomplete syndrome. The patient presented here exhib-ited a number of the classic signs and symptoms of thedisorder, which variably include thinning or sparse hair,frontal bossing of the skull, periorbital hyperpigmenta-tion, prominent lips, abnormal dentition, and chronicfevers secondary to an inability to autoregulate skintemperature. Pulmonary complications are frequent—approximately 30% of all affected males die during thefirst 2 years of life secondary to either hyperpyrexia orpulmonic infection [2]. In the classic study by Clarke andcolleagues [3], 52 anhidrotic ectodermal hypoplasia fam-ilies were evaluated. Forty-four percent of children werenoted to suffer from severe recurrent respiratory tractinfections, and death due to the sequelae of these re-peated insults was common in both children and affectedadult survivors. Although no consistent abnormality hasbeen noted in either B- or T-cell function, an associatedimmune deficiency has been noted with this condition[5]. In the report by Clarke and colleagues [3], the mostcommon abnormality noted at assessment of humoralimmunity was elevated IgM concentration, and this wasalso noted in the patient presented here. Although im-mune abnormalities are variably noted, the increasedsusceptibility to pulmonic infections is thought primarilyto be a result of abnormal mucous gland (absent orhypoplastic) development in the lung [2].
The discrete molecular genetic defect for ectodermaldysplasia is not known; however, by linkage analysis theaffected gene for this disorder has been localized to aregion on the long arm of the X chromosome (Xq12–13.1).A recent study has noted that fibroblasts from affectedpatients exhibit a significant decrease in binding capacityfor epidermal growth factor, and a decreased expressionof both the epidermal growth factor receptor protein andmRNA [6].
In summary, a case of lung transplantion for a patientsuffering from end-stage pulmonary disease secondary toanhidrotic ectodermal dysplasia is presented. Lungtransplantation was successful; however, the patienteventually succumbed to a nonpulmonic infectious pro-cess. A disease with a similar clinical and pathologic (Fig1) presentation, cystic fibrosis, is actually the most com-mon indication for lung transplantation in children, andresults to date have been quite good [1]. Pulmonary
disease in infant males with ectodermal dysplasia lessthan 2 years of age carries a particularly bad prognosis;therefore, the option of lung transplantation in this groupshould be considered as early as possible. The potentiallong-term impact of various forms of the associatedimmune deficiency is unknown.
References
1. Noyes BE, Kurland G, Orenstein DM. Lung and heart–lungtransplantation in children. Pediatr Pulmonol 1997;23:39–48.
2. Masse J-F, Perusse R. Ectodermal dysplasia. Arch Dis Child1994;71:1–2.
3. Clarke A, Phillips DJM, Brown R, Harper PS. Clinical aspectsof X-linked ectodermal dysplasia. Arch Dis Child 1987;62:989–96.
4. Stevenson AC, Kerr CB. On the distribution and frequenciesof mutation to genes determining harmful traits in man.Mutation Res 1967;4:339–52.
5. Brooks EG, Klimpel GR, Vaidya SE, et al. Thymic hypoplasiaand T cell deficiency in ectodermal dysplasia: case report andreview of the literature. Clin Immunol Immunopathol 1994;71:44–52.
6. Vargas GA, Fantino E, George-Nascimento C, Gargus JJ,Haigler HT. Reduced epidermal growth factor receptor ex-pression in hypolidrotic ectodermal dysplasia and tabby mice.J Clin Invest 1996;97:2426–32.
Repair of Pulmonary Vein RuptureAfter Deceleration InjuryDavid Varghese, MBChB, Hitesh Patel, FRCS,Ewan W. J. Cameron, FRCS, and Mike Robson, FRCA
Cardiothoracic Surgery, Royal Infirmary of Edinburgh,Edinburgh, Scotland
Injuries to the major pulmonary vessels are uncommonand are extremely difficult to manage. We report a case ofan isolated pulmonary vein injury following a road trafficaccident that was repaired successfully.
(Ann Thorac Surg 2000;70:656–8)© 2000 by The Society of Thoracic Surgeons
Injuries to the major pulmonary vessels resulting fromblunt chest trauma are uncommon and when encoun-
tered pose difficulties in management. An isolated injuryto the pulmonary vein as a cause of a massive hemotho-rax is extremely rare. We present the case of a 43-year-old man who was admitted to a peripheral hospital aftersuffering blunt chest trauma. Subsequent thoracotomyrevealed a torn left inferior pulmonary vein which wassuccessfully repaired.
Accepted for publication Oct 20, 1999.
Address reprint requests to Dr Patel, Department of Surgery, Chelsea andWestminster Hospital, Imperial College School of Medicine, 369 FulhamRd, London SW10 9NH, England; e-mail: [email protected].
656 CASE REPORT VARGHESE ET AL Ann Thorac SurgPULMONARY VEIN INJURY 2000;70:656–8
© 2000 by The Society of Thoracic Surgeons 0003-4975/00/$20.00Published by Elsevier Science Inc PII S0003-4975(00)01199-1

A 43-year-old male motorcyclist traveling at 40 miles perhour hit a stationary motor car. On admission to theEmergency Department, Queen Margaret Hospital, hewas fully conscious and alert with a Glasgow Coma Scaleof 15. He was complaining of chest pain and shortness ofbreath. He had a respiratory rate of 20 breaths per minutewith an oxygen saturation of 85%, a regular pulse of100 beats per minute, and blood pressure of 90/70 mm Hg.
On examination there was tenderness in the rightupper quadrant of his abdomen with guarding, anddecreased breath sounds along with surgical emphysemaon the right side. There were no obvious external woundsor bony deformity and examination revealed no chestwall or pelvic tenderness.
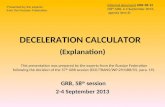
He was resuscitated with intravenous colloids and wasgiven oxygen through a nonrebreather facemask. Hisblood pressure rose to 111/76 mm Hg and his pulse ratedecreased to 80 beats per minute. A chest roentgenogramshowed a large right hemopneumothorax with mediasti-nal shift to the left and surgical emphysema. A right chesttube was inserted and drained 400 mL of blood. Thepatient subsequently had a computed tomography scanof the chest and abdomen. During the scan his bloodpressure dropped to 70/40 mm Hg. He responded well tovolume replacement with blood and colloid. The com-puted tomography scan (Fig 1) showed a persisting largeright hemopneumothorax despite the presence of thechest tube. There was no significant mediastinal hema-toma. The left lung contained a 3-cm pneumatocele in thelower lobe indicating a left pulmonary contusion. Nofractured ribs were seen. Also, an irregular low attenua-tion area was seen within the superior liver in segmentfour, suggestive of hepatic laceration. The spleen and kid-neys appeared normal. A second chest tube was placedmore inferiorly in the right pleural cavity and the patientwas transferred to the Royal Infirmary, Edinburgh.
After transfer and admission it was evident that therelease of blood through the chest drains was intermit-tent because of blockage by the thrombus. When therewas an episode of rapid blood release the patient’s
hemodynamics deteriorated with hypotension andtachycardia. Recovery occurred with ongoing volumereplacement and clamping of the chest drains. Thisobservation, along with the desaturation of the drainedblood, led to the clinical diagnosis of pulmonary hilarvessel rupture, probably vein. The patient was taken tosurgery with the chest drains clamped.
A right thoracotomy was performed. The chest wasrapidly opened and the lung hilum compressed manuallywhile the hemothorax was emptied of blood and bloodclots. On release of the hilar compression it was evidentthat the inferior pulmonary vein was torn inferiorly at thelevel of the pericardium. Cross clamps were applied tocontrol a 1-cm tear that was then repaired with continu-ous sutures. There was also some pulmonary parenchy-mal bleeding in the medial segment of the lower lobe thatwas closed with Teflon felt-supported sutures. The vas-cular clamps were released and a period of observationensured that there was no infarction of the lower lobe. Aperipheral laparotomy allowed confirmation that theliver injury was stable.
The patient made a steady postoperative recovery andwas fit enough to be sent for rehabilitation 10 days afteroperation.
Comment
Blunt chest trauma occurs in up to 50% of all fatal motoraccidents and is the primary cause of death in 12% to 25%[1] of such accidents. Pulmonary vein laceration as acause of massive hemothorax is extremely rare. Theclinical presentation is that of hypotension, hypovolemia,and massive hemothorax [2]. In such an injury, as in thiscase, the hemodynamic behavior of the patient reflectsthe fact that the left atrium and pulmonary venouscirculation is a low-pressure, low-impedance system. It istheorized that following rupture of the pulmonary veinand subsequent development of a low-pressure hemo-thorax, the pleural cavity becomes part of this low-pressure system and effectively functions as a giant leftatrium. Hence, retention of blood in the pleural cavityallows maintenance of hemodynamics (as during chestdrain clamping), whereas release of blood from thehemothorax merely causes rapid volume depletion.Clearly blood loss into a pleural cavity from a high-pressure system such as a systemic artery has malevolentcompression effects not present in an injury such aspulmonary vein rupture. The formation of thrombuswithin the right hemothorax occluded the first chest tube,which is why only 400 mL of blood were drained initiallyand subsequent drainage was for the same reason inter-mittent and not persistent and torrential, as might havebeen expected if the drains were at all times patent. Thisoccurrence was fortunate for the patient because un-blocked drains would simply have acted as a conduitallowing him to exsanguinate.
Many factors are involved in the decision to proceed tothoracotomy. We suggest earlier intervention in cases ofcardiovascular instability after intercostal drainage and
Fig 1. Computed tomography scan of thorax showing a large righthemopneumothorax with mediastinal shift, with extensive mediasti-nal and subcutaneous air.
657Ann Thorac Surg CASE REPORT VARGHESE ET AL2000;70:656–8 PULMONARY VEIN INJURY

that the rate of blood loss via the chest tube [3] as thebasis for urgent thoracotomy can be inaccurate becauseof the formation of clots.
References
1. Hawkins ML, Carraway RP, Ross SE, Johnson RC, Tyndal EC,Laws HL. Pulmonary artery disruption from blunt thoracictrauma. Am Surg 1988;54:148–52.
2. McKeown PP, Rosemurgy A, Conant P. Blunt traumaticrupture of pulmonary vein, left atrium and bronchus. AnnThorac Surg 1991;52:1171–2.
3. Miura H, Taira O, Hiraguri S, et al. Blunt thoracic injury. JpnJ Thorac Cardiovasc Surg 1998;46:556–60.
INVITED COMMENTARY
This case, with its discussion, again emphasizes theimportance of a working familiarity with basic patho-physiology when treating thoracic trauma. Althoughtrauma systems—centers and organized training pro-grams—have increased the salvage rate of severely in-jured patients, the high volume, necessary “check list”approach, and usual absence of thoracic surgeons ininitial management may be deleterious.
This patient survived because the improperly function-ing chest tubes did not allow exsanguination. The bleed-ing raised the intrapleural pressure to above atrial andpulmonary vein pressures, arresting further hemorrhage.When the tubes were blocked by clot or clamps thepatient could be resuscitated and transferred, and surgi-cal repair successfully accomplished.
Two generations ago, observations of many similarcases led to a policy of delaying chest tube insertion fortreatment of hemothorax until the patient was fullyevaluated and definitive treatment could be undertaken.The beneficial factors of low pulmonary vascular andatrial pressures and intrinsic lung clotting factors arenegated with an immediate chest tube, especially withsuction applied. Chest tube insertion for hemothoraxmay occasionally precipitate massive exsanguination in apreviously relatively stable patient. Delay in tube drain-age for an hour or two while the patient is evaluated andan operating room made available is usually wiser. (Se-rious respiratory distress from airway or systemic vascu-lar leaks obviously requires immediate tube decompres-sion of the pleural space.)
Interestingly, this patient did not require endotrachealintubation and artificial ventilation even though his oxy-gen saturation was only 85%, equivalent to a PaO2 ofabout 60 mm Hg, or lower. I wonder what would havehappened in most American trauma centers.
James W. Pate, MD
Department of SurgeryUniversity of Tennessee956 Court AveMemphis, TN 38163
Ventricular Thrombosis andSystemic Embolism in Bodybuilders:Etiology and ManagementKathryn McCarthy, MB, BS, Augustine T. M. Tang,FRCS, Malcolm J. R. Dalrymple-Hay, FRCS, andMarcus P. Haw, FRCS
Department of Cardiac Surgery, Wessex Cardiac & ThoracicUnit, Southampton General Hospital, Southampton, UnitedKingdom
Increased thrombogenicity and acute embolism are well-recognized complications of chronic anabolic steroidabuse. The following cases highlight such dangers insteroid-enhanced bodybuilders who developed intracar-diac thrombosis that subsequently embolized. Systemicanticoagulation and surgical thrombectomy constitutedthe mainstay treatment. This represents the first report ofsuch devastating cardiovascular complications after ana-bolic steroid abuse and their management.
(Ann Thorac Surg 2000;70:658–60)© 2000 by The Society of Thoracic Surgeons
Adverse systemic effects of anabolic steroid abuseincluding arterial thrombosis are well documented.
However, thrombosis in the left ventricle and the pro-pensity for systemic embolism have hitherto not beenrecognized. We describe our experience of this compli-cation in two young bodybuilders who followed differentmanagement strategies.
Case Reports
Patient 1
A 35-year-old competitive bodybuilder presented with a3 day history of central chest pain, back pain, andbreathlessness following a 4 to 6 week flulike illness. Hewas an exsmoker with a family history of coronary arterydisease and had been “cycling” various testosteroneanalogs including nandrolone and nandralone for manyyears. Cycling involves 2 to 3 months of continuousadministration of the drug punctuated by abstinence of 2to 3 weeks. Electrocardiography confirmed sinus rhythm.Myocarditis was initially diagnosed for which angioten-sin-converting enzyme inhibitors and diuretics were in-stituted. The patient was allowed to continue with ana-bolic steroid treatment to avoid withdrawal problems.However, despite treatment he developed pulmonaryedema and transthoracic echocardiography demon-strated dilated cardiomyopathy with severe global left
Accepted for publication Dec 14, 1999.
Address reprint requests to Dr Tang, Department of Cardiac Surgery,Wessex Cardiac & Thoracic Unit, Southampton General Hospital, Tre-mona Rd, Southampton SO16 6YD, United Kingdom; e-mail: [email protected].
658 CASE REPORT McCARTHY ET AL Ann Thorac SurgANABOLIC STEROID AND VENTRICULAR THROMBECTOMY 2000;70:658–60
© 2000 by The Society of Thoracic Surgeons 0003-4975/00/$20.00Published by Elsevier Science Inc PII S0003-4975(00)01572-1