Repair of burst abdominal incisions
2
Br. J. Surg. Vol. 61 (1974) 456-457 Repair of burst abdominal incisions DONALD YOUNG* SUMMARY A technique is described for the repair of burst abdominal incisions which ensures that pressure from below the incision tends to bring together the walls of the wound. This technique is most useful for fat flabby abdomens. Pressure from below the wound pulls down the rubber tubes and approximates the wound more firmly at the site of the pressure. The following technique has been used by the author at the Warrington Infirmary with complete A MAJOR cause of dehiscence of abdominal incisions is failure of the posterior rectus sheath and peritoneum to heal by first intention. This allows the creation of a hydraulic pressure cone which separates the muscle and fat layers so that the abdominal wall is held together only by the sutures in the skin layer. On the removal of the skin sutures the whole wound gapes. As the peritoneum is often friable from inflammatory change and difficult to resuture, sutures through all layers have been used traditionally to close the abdominal wall. In fat and friable abdominal walls these sutures, with or without a decoration of fine rubber tubing, will cut through the skin and allow further gaping. The use of deep mattress sutures of braided nylon, 2cm apart, tied over a firm rubber tube running parallel to and 6-7 cm from the incision on either side, will avoid cutting through the skin. Fig. 3. Photograph of the repair. Fig. 1. Cross-section showing details of suture insertion. Fig. 4. After removal o f sutures on the tenth day. Fig. 2. Cross-section showing final position of sutures. 456 * Newsham General Hospital, Liverpool.
-
Upload
donald-young -
Category
Documents
-
view
216 -
download
0
Transcript of Repair of burst abdominal incisions

Br. J. Surg. Vol. 61 (1974) 456-457
Repair of burst abdominal incisions D O N A L D Y O U N G *
SUMMARY A technique is described for the repair of burst abdominal incisions which ensures that pressure from below the incision tends to bring together the walls of the wound. This technique is most useful for fat flabby abdomens.
Pressure from below the wound pulls down the rubber tubes and approximates the wound more firmly at the site of the pressure.
The following technique has been used by the author at the Warrington Infirmary with complete
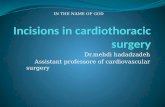
A MAJOR cause of dehiscence of abdominal incisions is failure of the posterior rectus sheath and peritoneum to heal by first intention. This allows the creation of a hydraulic pressure cone which separates the muscle and fat layers so that the abdominal wall is held together only by the sutures in the skin layer. On the removal of the skin sutures the whole wound gapes. As the peritoneum is often friable from inflammatory change and difficult to resuture, sutures through all layers have been used traditionally to close the abdominal wall. In fat and friable abdominal walls these sutures, with or without a decoration of fine rubber tubing, will cut through the skin and allow further gaping. The use of deep mattress sutures of braided nylon, 2cm apart, tied over a firm rubber tube running parallel to and 6-7 cm from the incision on either side, will avoid cutting through the skin.
Fig. 3. Photograph of the repair.
Fig. 1. Cross-section showing details of suture insertion.
Fig. 4. After removal of sutures on the tenth day.
Fig. 2. Cross-section showing final position of sutures.
456
* Newsham General Hospital, Liverpool.

Repair of burst abdominal incisions
I
success for 20 years. The success of the operation is believed to be due to the fact that pressure from below pulls the skin down and the sides of the wound together, which allows the whole depth of the wound to heal.
Technique The suture is passed through all the layers from skin to peritoneum and peritoneum to skin, then brought back over the rubber tubing in a shallower path at the level of the anterior sheath of the rectus, to emerge from the skin again medial to the point of entry, so that the suture can be tied over the rubber tubing on
that side (Fig. 1). Braided nylon on an atraumatic 90-mm curved needle is most useful for this technique. When all the sutures have been placed the wound is approximated by pulling all the sutures tight, then they are tied firmly in succession over the rubber tube while the assistant holds the remainder taut. If the peritoneum and muscle layer is not too friable a continuous atraumatic chromic catgut suture may be used to approximate this layer. The skin and sub- cutaneous fat are closed by alternate vertical mattress sutures to evert the skin edges, which tend to turn in, and by ordinary loosely tied sutures of thread or nylon to approximate the skin edges (Figs. 2 , 3 , 4).
A differential sign in torsion of a testicular appendage WHEN torsion occurs in one of a pair of fully descended testes, the involved organ lies higher than its fellow. If the involved testis is lower than its fellow, the diagnosis is almost certainly ‘torsion of an appendage of the testis’. The lower position occurs because the testis is not pulled up by the twisting of the mesentery as in testicular torsion and the dartos muscle remains relatively relaxed on the involved side owing to the heat generated by the inflammatory reaction to the gangrenous appendage. J. P. GOLDEN, International Missionary Training Hospital, Drogheda, Co. Louth.
457