
Renal Trauma
37
Renal Trauma Background Renal trauma may manifest in a dramatic fashion for both the patient and the clinician. The incidence of renal trauma somewhat depends on the patient population being considered. Renal trauma accounts for approximately 3% of all trauma admissions and as many as 10% of patients who sustain abdominal trauma. Also, renal trauma may occur in settings other than those thought of as a classic trauma setting. The approach to renal injuries has changed over time, requiring diligent attention to recent literature. Namely, the tolerance for nonoperative or expectant management has increased, even in the most seriously injured kidneys, replacing the past tendency toward aggressive renorrhaphy. Problem Most renal trauma occurs as a result of blunt trauma. Renal injuries may be generally divided into 3 groups: renal laceration, renal contusion, and renal vascular injury. All subsets of renal trauma require a high index of clinical awareness and prompt evaluation and management. Epidemiology Frequency The frequency of renal injury somewhat depends on the patient population being considered. Renal trauma accounts for approximately 3% of all trauma admissions and as many as 10% of patients who sustain abdominal trauma. Etiology The mechanism of injury should alert the clinician to the possibility of renal trauma. The following list is not all-
-
Upload
maisyah-nelzima -
Category
Documents
-
view
18 -
download
1
description
trauma renal
Transcript of Renal Trauma
Renal Trauma
Background
Renal trauma may manifest in a dramatic fashion for both the patient and the clinician. The incidence of renal trauma somewhat depends on the patient population being considered. Renal trauma accounts for approximately 3% of all trauma admissions and as many as 10% of patients who sustain abdominal trauma. Also, renal trauma may occur in settings other than those thought of as a classic trauma setting. The approach to renal injuries has changed over time, requiring diligent attention to recent literature. Namely, the tolerance for nonoperative or expectant management has increased, even in the most seriously injured kidneys, replacing the past tendency toward aggressive renorrhaphy.
Problem
Most renal trauma occurs as a result of blunt trauma. Renal injuries may be generally divided into 3 groups: renal laceration, renal contusion, and renal vascular injury. All subsets of renal trauma require a high index of clinical awareness and prompt evaluation and management.
Epidemiology
Frequency
The frequency of renal injury somewhat depends on the patient population being considered. Renal trauma accounts for approximately 3% of all trauma admissions and as many as 10% of patients who sustain abdominal trauma.
Etiology
The mechanism of injury should alert the clinician to the possibility of renal trauma. The following list is not all-inclusive, but it highlights the major mechanisms that generate renal injuries.
Penetrating (eg, gunshot wounds, stab wounds) Blunt (eg, pedestrian struck, motor vehicle crash, sports, fall) Iatrogenic (eg, endourologic procedures, extracorporeal shock-wave lithotripsy,[1]
renal biopsy, percutaneous renal procedures) Intraoperative (eg, diagnostic peritoneal lavage[2] ) Other (eg, renal transplant rejection, childbirth[3] [may cause spontaneous renal
lacerations])
Presentation

The diagnosis of renal injury begins with a high index of clinical awareness. The mechanism of injury provides the framework for the clinical assessment. Particular attention should be paid to complaints of flank or abdominal pain. Urinalysis, both gross and, if necessary, microscopic, should be performed in patients who are thought to have renal trauma. Based on these initial measures, radiographic or operative investigation may follow.
Indications
Most blunt renal injuries are low-grade; therefore, they are usually amenable to treatment with observation and bed rest alone. Penetrating trauma is more likely to be associated with more severe renal injury, thus requiring a higher index of clinical awareness. Further, penetrating trauma is more often associated with other abdominal injuries requiring laparotomy, thus providing the opportunity for intraoperative renal staging and/or repair.
Patients with indications for emergent exploration include those with hemodynamic instability. Expanding hematomas or active hemorrhage suggests the possibility of high-grade renal injury. Patients with penetrating trauma who are stable and do not require urgent laparotomy for other possible intra-abdominal injuries may be observed without immediate renal exploration.
Unrelenting gross hematuria may require urgent exploration. However, the presence of a renal contusion does not typically require specific intervention. Findings from imaging studies may appear quite alarming, but most renal contusions resolve, particularly if the lesion appears to be of grade I-III.
Laboratory Studies
Urinalysis o Urinalysis provides rapidly available information in patients who may have a renal
laceration; however, the data obtained must be viewed within a rational framework. o If gross hematuria is not present, a microscopic examination is advisable. Although a
generalization exists that the degree of hematuria correlates with the likelihood of urinary tract trauma, renal injury with no hematuria has been reported. Reliance on urinalysis as the only modality to help diagnose renal trauma is fraught with difficulty. In fact, injuries such as renal artery laceration or avulsion may not generate any hematuria.
o One study documents that 63% of patients with multisystem trauma had hematuria, of which 12.5% had a proven injury. Other investigators have shown that as many as 13% of patients with renal gunshot wounds did not have hematuria.
o Thus, the presence or absence of hematuria should be viewed in the clinical context and not used as the sole decision point in the assessment of a patient with a possible renal laceration.
Imaging Studies
Intravenous pyelogram o Traditionally, intravenous pyelography (IVP) has been performed in the
radiology department and consists of multiple images, including tomograms. In the era before CT scans, this modality provided the most detailed information on renal anatomy. In the trauma setting, the system was modified to a "one-shot" technique, in which a single image is obtained. Although opinions regarding the utility of the one-shot system differ, the traditional IVP should not, in general, be used in the urgent evaluation of renal trauma.
o Advantages of IVP are that it (1) allows functional and anatomic assessment of both kidneys and ureters, (2) establishes the presence or absence of 2 functional kidneys, and (3) may be performed in the emergency department or operating room.
o Disadvantages of IVP are that (1) it requires multiple images for maximal information, although a one-shot technique can be used; (2) the radiation dose is relatively high (0.007-0.0548 Gy); (3) a full IVP usually requires a trip to the radiology suite; and (4) findings do not reveal the full extent of injury. (One investigation of penetrating trauma showed normal findings from 6 IVP examinations out of 27 studies. These 6 patients all had renal injuries.)
Computed tomography o Advantages are that it (1) allows unsurpassed functional and anatomic
assessment of the kidneys and urinary tract, (2) helps establish the presence or absence of 2 functional kidneys, and (3) allows for the diagnosis of concurrent injuries.
o Disadvantages are that (1) it requires intravenous contrast in order to maximize information about functionality, hematoma, and, possibly, bleeding; (2) the patient must be stable enough to go to the scanner; and (3) full urinary assessment is dependent on the timing of contrast and scanning in order to view the bladder and ureters.
Angiography o Advantages are that it (1) has the capacity to aid in both the diagnosis and
treatment of renal injuries and (2) may further define injury in patients with moderate IVP abnormalities or with vascular injuries.
o Disadvantages are that (1) it is invasive; (2) it requires contrast; (3) it requires mobilization of resources to perform the study, which may be time-consuming; and (4) the patient must travel to the radiology suite.
Ultrasonography o Advantages are that it (1) is noninvasive, (2) may be performed in real
time in concert with resuscitation, and (3) may help define the anatomy of the injury.
o Disadvantages are that (1) optimal study results related to anatomy require an experienced sonographer; (2) the focused abdominal sonography for
trauma, ie, FAST examination, does not define anatomy and, in fact, looks only for free fluid; and (3) bladder injuries may be missed.
Diagnostic Procedures
Operative diagnosis o Depending on the mechanism of injury, many patients who sustain renal
laceration have associated intra-abdominal injuries that require urgent exploration.
o The clinical situation may have precluded the opportunity to perform the aforementioned diagnostic modalities.
o The surgeon should be prepared to make the diagnosis of renal injury intraoperatively.
o Lateral retroperitoneal hematomas may alert the surgeon to the presence of renal laceration.
o Direct evidence of penetrating trauma should also provide evidence of renal laceration. Other renal trauma, including renal pelvis or ureteral injuries, should be sought and identified.
o Although the medical consensus is not complete, evidence exists that not all perirenal hematomas discovered at laparotomy require exploration. Theories range from simple observation to exploration with vascular control. The optimal course depends on the physician's experience and the institution's resources. Increasingly, even severe renal injuries are being safely managed nonoperatively.
Medical Therapy
Nonoperative treatment
In the setting of blunt renal trauma and selected instances of penetrating renal trauma, a nonoperative approach may be selected. Patient selection is the preliminary step in adopting a nonoperative management strategy to renal trauma. One series, with predominantly blunt mechanisms of injury, documented that 85% of patients were treated successfully without surgery. Ultimately, the exclusion of concurrent injury may be the key point in treating patients nonoperatively.
The anatomic structure of the kidney lends itself to nonoperative management in the setting of blunt trauma. The kidney has an end artery blood supply with a segmental pattern of division that supplies the renal parenchyma. When subjected to blunt force that causes a laceration, the laceration tends to occur through the parenchyma. The resulting hematoma may displace renal tissue, but the segmental vessels themselves often are not lacerated. The closed retroperitoneal space around the kidney also promotes tamponade of bleeding renal injuries. Finally, the kidney is rich in tissue factor, the molecule that activates the extrinsic coagulation cascade, further promoting hemostasis after injury.
Interventional radiology has extended the ability to use a nonoperative approach. Percutaneous drainage of perinephric fluid collections or urinomas has been used to address one clinical complication of a nonoperative approach. In addition, angiography with selective embolization has been used in the setting of isolated renal trauma.[4]
Another method to enhance a nonoperative approach includes endourologic stenting. With these approaches, successful nonoperative management of renal lacerations may be achieved in a greater number of patients.
Surgical Therapy
Operative treatment
The goals of operative therapy for renal laceration incorporate the 2 basic principles of hemorrhage control and renal tissue preservation, which must be balanced for each individual patient. Attempts to find a universal plan for this approach have generated controversy in the medical literature. The mindset of the medical community has also been changing as established practice patterns have been examined, challenged, and reassessed.
An additional benefit of operative therapy is the ability to address concurrent injuries. One study documented that 80% of patients with renal laceration had other associated injuries. In that same study, 47% of the patients with renal laceration had an associated injury that required immediate laparotomy.
At the time of the emergent laparotomy, the associated injury may be addressed. Evaluation and treatment of the renal injury is also possible. Patients with expanding hematomas or active hemorrhage should have their kidneys explored. Also, if the mechanism is penetrating trauma, most authors believe that the kidneys should be explored.
Patients with sound indications for emergent exploration include those with hemodynamic instability or missile injury to the abdomen. Unrelenting gross hematuria may require urgent exploration.
Operative technique can play a significant role in renal salvage. One study documented a decrease in the nephrectomy rate from 56% to 18% when a systematic approach was used for central control of the renal vessels at their junction with the aorta and cava. In this manner, vascular control is obtained outside of the Gerota fascia prior to entry into the zone of injury. Without both the arterial and venous systems isolated, the decompression of the renal hematoma that occurs during exploration tends to lead to a higher incidence of nephrectomy.
Some controversy remains with the use of postoperative drains in the setting of renal trauma. The general trend has been away from the routine use of drains in this setting, although some centers still advocate their use. Suction drains should be avoided after renal repair.
Complications
Perioperative complications may be specific to the kidney or more generalized. Those specific to the kidney may include urinoma, hematoma, or infection. General complications may include deep vein thrombosis, systemic inflammatory response syndrome, or acute renal insufficiency.
Outcome and Prognosis
In many cases of renal trauma, the outcome and prognosis depend on the associated injuries. In situations in which nonoperative management is used, concern exists about leaving perfused but nonviable renal tissue in situ, which may lead to hypertension. However, the occurrence of hypertension in this setting seems to be rare. One study documents no evidence of hypertension after 5 years of follow-up in children who had sustained renal trauma. Other series report only isolated instances of hypertension. Therefore, the risk of hypertension alone does not seem to warrant surgical exploration in cases with nonperfused renal segments.
Bladder Trauma
Background
Bladder injuries are caused by blunt or penetrating trauma.[1, 2] The probability of bladder injury varies according to the degree of bladder distention; therefore, a full bladder is more likely to become injured than an empty one.
Although uniformly fatal in the past, a timely diagnosis with appropriate medical and surgical management now offers an excellent outcome. Early clinical suspicion, appropriate and reliable radiologic studies, and prompt surgical intervention, when indicated, are the keys to successful diagnosis and management of bladder trauma.[3]
For excellent patient education resources, visit eMedicine's Kidneys and Urinary System Center and Procedures Center. Also, see eMedicine's patient education articles Blood in the Urine, Intravenous Pyelogram, Cystoscopy, and Foley Catheter.
History of the Procedure
Patients with signs and symptoms suggestive of a bladder injury have a history typical for pelvic trauma, which is fairly straightforward for motor vehicle collisions, deceleration injuries, or assaults to the lower abdomen. If the patient is unconscious, family members or, more often, emergency services personnel may be able to provide the history.

Bladder injury from a motor vehicle collision may occur from direct impact with the car or indirectly from the steering wheel or seatbelt.
Deceleration injuries of the urinary bladder usually result from falling from a great height and landing on unyielding ground.
Assault to the lower abdomen by a sharp kick or blow may result in a bladder perforation.
Penetrating injuries to the bladder usually result from high-velocity gunshots or sharp stab wounds to the suprapubic area.
Problem
Blunt trauma
Deceleration injuries usually produce both bladder trauma (perforation) and pelvic fractures. Approximately 10% of patients with pelvic fractures also have significant bladder injuries. The propensity of the bladder to sustain injury is related to its degree of distention at the time of trauma.[4, 5, 6]
Penetrating trauma
Assault from a gunshot or stabbing typifies penetrating trauma. Often, concomitant abdominal and/or pelvic organ injuries are present.
Obstetric trauma
During prolonged labor or a difficult forceps delivery, persistent pressure from the fetal head against the mother's pubis can lead to bladder necrosis. Direct laceration of the urinary bladder is reported in 0.3% of women undergoing a cesarean delivery. Previous cesarean deliveries with resultant adhesions are a risk factor. Undue scarring may cause obliteration of normal tissue planes and facilitate an inadvertent extension of the incision into the bladder. Unrecognized bladder injuries may lead to vesicouterine fistulas and other problems.
Gynecologic trauma
Bladder injury may occur during a vaginal or abdominal hysterectomy. Blind dissection in the incorrect tissue plane between the base of the bladder and the cervical fascia results in bladder injury.
Urologic trauma
Perforation of the bladder during a bladder biopsy, cystolitholapaxy, transurethral resection of the prostate (TURP), or transurethral resection of a bladder tumor (TURBT) is not uncommon. Incidence of bladder perforation is reportedly as high as 36% following bladder biopsy.

Orthopedic trauma
Orthopedic pins and screws can commonly perforate the urinary bladder, particularly during internal fixation of pelvic fractures. Thermal injuries to the bladder wall may occur during the setting of cement substances used to seat arthroplasty prosthetics.
Idiopathic bladder trauma
Patients diagnosed with alcoholism and individuals who chronically imbibe a large quantity of fluids are susceptible to this type of injury. Previous bladder surgery is a risk factor. In reported cases, all bladder ruptures were intraperitoneal. This type of injury may result from a combination of bladder overdistention and minor external trauma (eg, a simple fall).
Epidemiology
Frequency
Frequency of bladder rupture varies according to the following mechanisms of injury:
External trauma (82%) Iatrogenic (14%) Intoxication (2.9%) Spontaneous (< 1%)
Of all bladder injuries, 60%-85% are from blunt trauma and 15%-40% are from a penetrating injury.[7] The most common mechanisms of blunt trauma are motor vehicle collisions (87%), falls (7%), and assaults (6%). In penetrating traumas, the most frequent culprit is gunshot wounds (85%), followed by stabbings (15%).
Approximately 10%-25% of patients with a pelvic fracture also have urethral trauma. Conversely, 10%-29% of patients with posterior urethral disruption have an associated bladder rupture.
Traumatic bladder ruptures
Of traumatic ruptures, extraperitoneal bladder perforations account for 50%-71%,[8]
intraperitoneal accounts for 25%-43%, and combined perforations account for 7%-14%.[9]
The incidence of intraperitoneal bladder rupture is significantly higher in children because of the predominantly intra-abdominal location of the bladder prior to puberty.
Combined intraperitoneal and extraperitoneal ruptures account for approximately 10% of all traumatic bladder-perforating injuries. Mortality rates in these patients approach 60%, as compared to 17%-22% overall, reflecting the severity of concomitant injuries associated with combined bladder ruptures.

Associated bowel injuries
Among patients with bladder trauma due to a gunshot, the incidence of associated bowel injuries is reportedly as high as 83%. Colon injuries are reported in 33% of patients with stab wounds, and vascular injuries are reportedly as high as 82% in patients with a penetrating trauma (with a 63% mortality rate).
Etiology
Main causes of bladder injury are penetrating and blunt trauma. Iatrogenic causes include surgical misadventures from gynecologic, urologic, and orthopedic operations near the urinary bladder. Less common causes involve obstetric trauma. Spontaneous or idiopathic bladder injuries without an obvious underlying pathology constitute the remainder.
Pathophysiology
Bladder contusion is an incomplete or partial-thickness tear of the bladder mucosa. A segment of the bladder wall is bruised or contused, resulting in localized injury and hematoma. Contusion typically occurs in the following clinical situations:
Patients presenting with gross hematuria after blunt trauma and normal imaging findings
Patients presenting with gross hematuria after extreme physical activity (ie, long-distance running)
The bladder may appear normal or teardrop-shaped on cystography. Bladder contusions are relatively benign, are the most common form of blunt bladder trauma, and are usually a diagnosis of exclusion. Bladder contusions are self-limiting and require no specific therapy, except for short-term bedrest until hematuria resolves. Persistent hematuria or unexplained lower abdominal pain requires further investigation.
Extraperitoneal bladder ruptures
Traumatic extraperitoneal ruptures are usually associated with pelvic fractures (89%-100%). Previously, the mechanism of injury was believed to be from a direct perforation by a bony fragment or a disruption of the pelvic girdle. It is now generally agreed that the pelvic fracture is likely coincidental and that the bladder rupture is most often due to a direct burst injury or the shearing force of the deforming pelvic ring.
These ruptures are usually associated with fractures of the anterior pubic arch, and they may occur from a direct laceration of the bladder by the bony fragments of the osseous pelvis. The anterolateral aspect of the bladder is typically perforated by bony spicules. Forceful disruption of the bony pelvis and/or the puboprostatic ligaments also tears the wall of the bladder. The degree of bladder injury is directly related to the severity of the fracture.
Some cases may occur by a mechanism similar to intraperitoneal bladder rupture, which is a combination of trauma and bladder overdistention. The classic cystographic finding is contrast extravasation around the base of the bladder confined to the perivesical space; flame-shaped areas of contrast extravasation are noted adjacent to the bladder. The bladder may assume a teardrop shape from compression by a pelvic hematoma. Starburst, flame-shape, and featherlike patterns are also described.
With a more complex injury, the contrast material extends to the thigh, penis, perineum, or into the anterior abdominal wall. Extravasation will reach the scrotum when the superior fascia of the urogenital diaphragm or the urogenital diaphragm itself becomes disrupted.
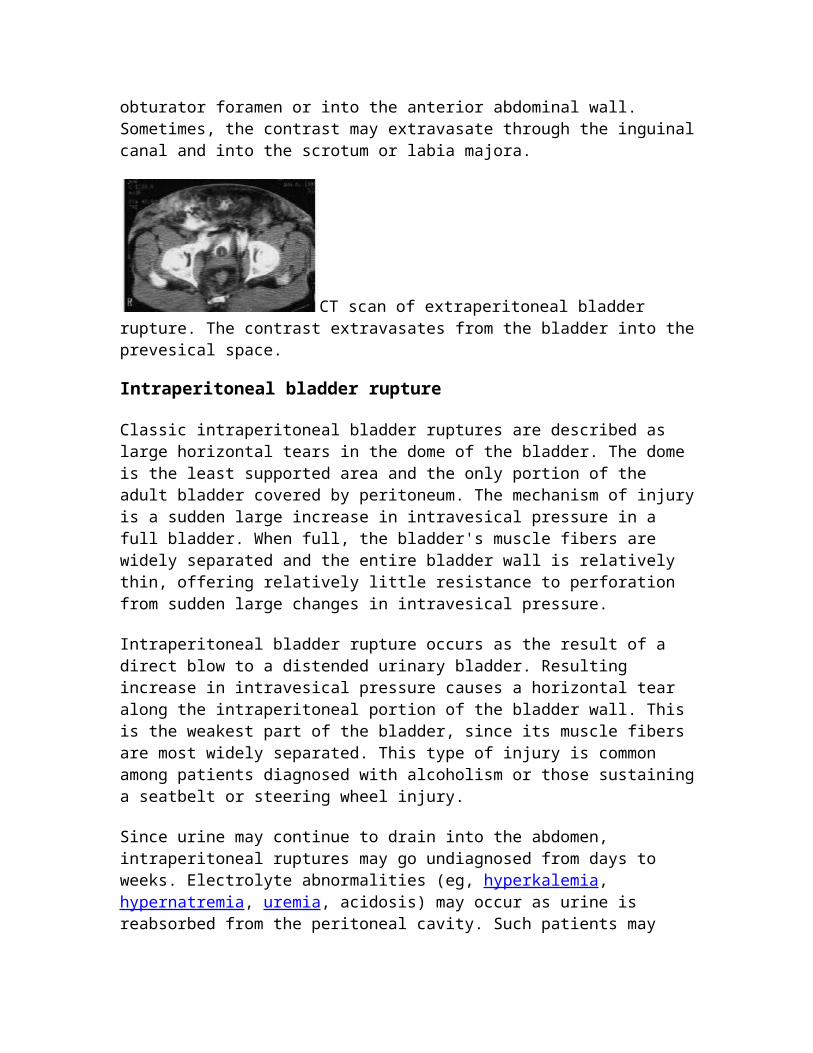
If the inferior fascia of the urogenital diaphragm is violated, the contrast material will reach the thigh and penis (within the confines of the Colles fascia). Rarely, contrast may extravasate into the thigh through the obturator foramen or into the anterior abdominal wall. Sometimes, the contrast may extravasate through the inguinal canal and into the scrotum or labia majora.
CT scan of extraperitoneal bladder rupture. The contrast extravasates from the bladder into the prevesical space.
Intraperitoneal bladder rupture
Classic intraperitoneal bladder ruptures are described as large horizontal tears in the dome of the bladder. The dome is the least supported area and the only portion of the adult bladder covered by peritoneum. The mechanism of injury is a sudden large increase in intravesical pressure in a full bladder. When full, the bladder's muscle fibers are widely separated and the entire bladder wall is relatively thin, offering relatively little resistance to perforation from sudden large changes in intravesical pressure.
Intraperitoneal bladder rupture occurs as the result of a direct blow to a distended urinary bladder. Resulting increase in intravesical pressure causes a horizontal tear along the intraperitoneal portion of the bladder wall. This is the weakest part of the bladder, since its muscle fibers are most widely separated. This type of injury is common among patients diagnosed with alcoholism or those sustaining a seatbelt or steering wheel injury.
Since urine may continue to drain into the abdomen, intraperitoneal ruptures may go undiagnosed from days to weeks. Electrolyte abnormalities (eg, hyperkalemia, hypernatremia, uremia, acidosis) may occur as urine is reabsorbed from the peritoneal

cavity. Such patients may appear anuric, and the diagnosis is established when urinary ascites are recovered during paracentesis.
Intraperitoneal ruptures demonstrate contrast extravasation into the peritoneal cavity, often outlining loops of bowel, filling paracolic gutters, and pooling under the diaphragm. An intraperitoneal rupture is more common in children because of the relative intra-abdominal position of the bladder. The bladder usually descends into the pelvis by age 20 years.
Cystogram of intraperitoneal bladder rupture. The contrast enters the intraperitoneal cavity and outlines loops of bowel.
Combination of intraperitoneal and extraperitoneal ruptures
Cystogram reveals contrast outlining the abdominal viscera and perivesical space. External penetrating injuries deserve special mention. A penetrating injury of the urinary bladder results from a high-velocity bullet traversing the bladder, knife wounds, or impalement by various sharp objects. These may result in intraperitoneal, extraperitoneal, or a combined bladder injury.
Cystogram of extraperitoneal bladder rupture. Note the fractured pelvis and contrast extravasation into the space of Retzius.
The high incidence of associated injury to abdominal viscera and vascular structures mandates surgical exploration in virtually every case. Often, cystography is bypassed, and the diagnosis is made during an exploratory laparotomy. Cystography results may be falsely negative in patients with penetrating bladder injuries secondary to small-caliber bullet wounds. In such patients, these injuries may not be appreciated until exploratory surgery is performed.
Presentation

Clinical signs of bladder injury are relatively nonspecific; however, a triad of symptoms is often present (eg, gross hematuria, suprapubic pain or tenderness, difficulty or inability to void).
Most patients with bladder rupture complain of suprapubic or abdominal pain, and many can still void; however, the ability to urinate does not exclude bladder injury or perforation. Hematuria invariably accompanies all bladder injuries. Gross hematuria is the hallmark of a bladder rupture. More than 98% of bladder ruptures are associated with gross hematuria, and 10% are associated with microscopic hematuria; conversely, 10% of patients with bladder ruptures have normal urinalysis results.
An abdominal examination may reveal distention, guarding, or rebound tenderness. Absent bowel sounds and signs of peritoneal irritation indicate a possible intraperitoneal bladder rupture. A rectal examination should be performed to exclude rectal injury and, in males, to evaluate prostate position. If the prostate is "high riding" or elevated, it may further suggest proximal urethra and bladder disruption.
In the setting of a motor vehicle collision or a crush injury, bilateral palpation of the bony pelvis may reveal abnormal motion, indicating an open-book fracture or a disruption of the pelvic girdle.
If blood is present at the urethral meatus, suspect a urethral injury. Perform retrograde urethrography to assess the integrity of the urethra before attempting to blindly pass a Foley catheter.
Indications
Foley catheter
Blood at the urethral meatus is an absolute indication for retrograde urethrography. Approximately 10%-20% of men with a posterior urethral injury have an associated bladder injury; therefore, do not place a urethral catheter in these patients. Passage of a urethral catheter may convert a partially disrupted urethra into a complete tear.
Place a Foley catheter only after urethral injuries are excluded. In the setting of a posterior urethral injury, insert a percutaneous suprapubic catheter.
CT scanning
This is often the first test performed in patients with blunt abdominal trauma. The CT scan of the pelvis provides information on the status of the pelvic organs and osseous pelvis and has replaced conventional cystography as the most sensitive test for bladder perforation. Once the urethra has been cleared by a retrograde urethrogram, a urethral catheter can be placed. Dilute Cysto-Conray is then passed through the urethral catheter, and an abdominal/pelvic CT scan is performed. Subtle perforations are often revealed, and the intraperitoneal and extraperitoneal nature of these ruptures can be determined.
Cystography
The criterion standard for imaging a suspected bladder injury is a well-performed cystography. Although it is preferable to perform the examination under fluoroscopy, clinical circumstances often do not permit this. A static cystography is satisfactory, even when performed at the bedside with portable equipment.
Most patients with bladder trauma have multiple injuries and require abdominal or pelvic CT scans as part of their trauma evaluation. This does not preclude obtaining a separate contrast cystogram if the bladder findings of the CT scan are equivocal.[10]
A properly performed cystography consists of an initial kidney-ureter-bladder (KUB) followed by anteroposterior (AP) and oblique views of the bladder filled with contrast, plus another AP film obtained after drainage. The following procedure is recommended:
Obtain a scout radiograph. Place a urethral catheter in the bladder. Using a diluted contrast medium, slowly fill the bladder by gravity
(approximately 75 cm above the pelvis) to a volume of 300-400 mL. (Diluted contrast media are usually 50% contrast and 50% sterile saline or water). Use a contrast media suitable for absorption.
Obtain a single AP film of the pelvis and lower abdomen after the first 100 mL of contrast is instilled.
If gross extravasation is noted, discontinue the procedure. If extravasation is absent, give the patient the remainder of the contrast.
Obtain a KUB, followed by a postdrainage film of the pelvis. Obtain the postdrainage film after a complete drainage of the contrast. This is the
most critical part of the study because it checks for extravasation that may be hidden by the distended bladder.
If possible, obtain lateral and oblique films of the bladder. In children, obtain the estimated filling for the cystogram based on the following formula:
Bladder capacity = 60 mL + (30 mL X age in years)
The importance of proper filling and drainage films cannot be overemphasized. A significant number of injuries may be missed if the cystogram is not performed correctly.
As oblique films may be difficult to obtain in a trauma patient with pelvic fractures, they may be omitted in selected cases. The volume infused is less important than achieving an adequate bladder pressure to demonstrate small bladder injuries that may go undetected. Small puncture wounds or lacerations may be self-sealing because of mucosal edema. Overlying hematomas, omentum, a sigmoid colon, or a small bowel may seal the wound. Full distention helps to prevent this false-negative result, and the accuracy of a well-performed static cystogram ranges from 85%-100%.
If the patient is immediately taken to the operating room for an exploratory laparotomy and/or placement of a formal suprapubic cystostomy, the bladder is inspected at the time
of surgery and the bladder injury is repaired. If surgery is delayed or an exploratory laparotomy is not contemplated, perform the cystogram via a percutaneous suprapubic tube (SPT) so that no bladder injury is overlooked.[11]
Although static cystography is used to accurately diagnose a bladder injury, the same cannot be said of intravenous pyelography (IVP). The inaccuracy of IVP stems from incomplete bladder distension, poor opacification, or a combination of both.
Relevant Anatomy
The adult bladder is located in the anterior pelvis and is enveloped by extraperitoneal fat and connective tissue. It is separated from the pubic symphysis by an anterior prevesical space known as the space of Retzius. The dome of the bladder is covered by peritoneum, and the bladder neck is fixed to neighboring structures by reflections of the pelvic fascia and by true ligaments of the pelvis.
In males, the bladder neck is contiguous with the prostate, which is attached to the pubis by puboprostatic ligaments. In females, pubourethral ligaments support the bladder neck and urethra.
The body of the bladder receives support from the urogenital diaphragm inferiorly and the obturator internus muscles laterally.
The superior fascia of the urogenital diaphragm is continuous and includes the pelvic, obturator, and endopelvic fasciae. The inferior fascia of the urogenital diaphragm fuses with the Colles fascia. It continues as the Scarpa fascia anteriorly, the dartos muscle and fascia in the scrotum, and the fascia lata of the thigh.
The type of extravasation (intraperitoneal or extraperitoneal) depends upon the location of the laceration and its relationship with the peritoneal reflection.
If the perforation is above the peritoneal reflection, the extravasation is intraperitoneal.
If the injury is below the peritoneal reflection, the extravasation is extraperitoneal.
With an anterosuperior perforation, urinary extravasation may be intraperitoneal, extraperitoneal (space of Retzius), or both. If the tear is posterosuperior, fluid can spread intraperitoneally and/or retroperitoneally.
In a bladder rupture, the superior fascia of the urogenital diaphragm, when intact, prohibits extravasation from escaping the pelvis. Inferior fascia of the urogenital diaphragm, when intact, also prevents urinary extravasation from flowing into the perineum.
Contraindications
Posterior urethral injury is a specific contraindication to insertion of a urethral Foley catheter. Suspect a posterior urethral injury if blood is present at the meatus, in all pelvic fractures, or if a high-riding prostate is found on digital rectal examination.
When posterior urethral injury is suspected, perform a retrograde urethrogram before attempting to insert a Foley catheter. Perform a retrograde urethrogram as follows:
Gently stretch the penis and hold it at an obtuse angle from the pelvis. Insert a 16F Foley catheter into the distal urethra, and inflate the balloon (3 mL)
within the fossa navicularis. Alternatively, if available, a Brodney clamp may be used, which allows a better seal at the urethral meatus.
Inject a diluted x-ray contrast medium suitable for intravenous infusion into the catheter using a 60-mL piston syringe.
Obtain radiographic images of the urethra and the bladder. Oblique views are usually the most helpful. An extravasation indicating urethral injury will be readily apparent.
Alternatively, the tip of a 60-mL piston syringe may be engaged into the urethral meatus and contrast injected directly into the urethra. Lead-lined gloves must be worn when contrast is injected directly into the urethra to prevent radiation exposure to the examiner's hands.
After excluding posterior urethral injury, radiographic evaluation of suspected bladder injury may commence. In the presence of a documented urethral injury, a percutaneous SPT must be placed and primary urethral realignment attempted once the patient is stable; this is often efficacious in the prevention of severe urethral stricture formation. Primary realignment may often be attempted with flexible cystoscopy at the bedside and may help to obviate the need for a formal urethroplasty at a later date.
Medical Therapy
Most extraperitoneal ruptures can be managed safely with simple catheter drainage (ie, urethral or suprapubic).[12] Leave the catheter in for 7-10 days and then obtain a cystogram. Approximately 85% of the time, the laceration is sealed and the catheter is removed for a voiding trial.[13, 14]
Virtually all extraperitoneal bladder injuries heal within 3 weeks. If the patient is taken to the operating room for associated injuries, extraperitoneal ruptures may be repaired concomitantly if the patient is stable.
Surgical Therapy

Intraperitoneal bladder rupture
Most, if not all, intraperitoneal bladder ruptures require surgical exploration.[15] These injuries do not heal with prolonged catheterization alone. Urine takes the path of least resistance and continues to leak into the abdominal cavity. This results in urinary ascites, abdominal distention, and electrolyte disturbances.
Surgically explore all gunshot wounds to the lower abdomen. Because of the nature of associated visceral injuries, immediately take patients with high-velocity missile trauma to the operating room, where the bladder injuries can be repaired concomitantly with other visceral injuries.
Stab wounds to the suprapubic area involving the urinary bladder are managed selectively. Surgically repair obvious intraperitoneal injuries, and manage small extraperitoneal injuries expectantly with catheter drainage.
Extraperitoneal extravasation
Bladders with extensive extraperitoneal extravasation are often repaired surgically. Early surgical intervention decreases the length of hospitalization and potential complications, while promoting early recovery.
Complications
Potential complications of bladder surgery o Urinary extravasationo Wound dehiscenceo Hemorrhageo Pelvic infectiono Small-capacity bladdero De novo urge incontinence
Other complications o Despite technically proper reconstruction, urinary extravasation through
the bladder closure may occur. This usually responds to extended catheter drainage.
o Abdominal fascial dehiscence presents as persistent drainage from the incision site.
o Violation of pelvic hematomas during surgery results in severe hemorrhage.
o If infected, pelvic hematomas become pelvic abscesses.o Aggressive surgical débridement of the bladder may result in a small
bladder, giving rise to bladder spasms and urge incontinence. Over time, the bladder may gradually enlarge to more physiologic volumes.
Outcome and Prognosis

Traumatic bladder ruptures, once uniformly fatal, are currently managed quite successfully. Timely evaluation and proper management are critical for optimal outcomes.
Gross hematuria is the hallmark of bladder injury. Physicians evaluating patients with blunt or penetrating lower abdominal trauma must have a high index of suspicion for urologic injury, especially bladder and urethral injuries.
Almost all extraperitoneal bladder ruptures are associated with pelvic fractures. Most extraperitoneal ruptures can be treated conservatively with catheter drainage alone; however, ensure that all intraperitoneal, combined intraperitoneal and extraperitoneal ruptures, and penetrating injuries are treated with immediate exploration and repair in the operating room.
Urethra Trauma
Background
Trauma to the male urethra must be efficiently diagnosed and effectively treated to prevent serious long-term sequelae. Patients with urethral stricture disease secondary to poorly managed traumatic events are likely to have significant voiding problems and recurring need for further interventions. Many of these men have significant orthopedic and neurologic injuries, as well. Rehabilitation requires reconstruction of the urinary tract in a manner that does not interfere with the healing process.
History of the Procedure
Most urethral injuries are associated with well-defined events, including major blunt trauma such as caused by motor vehicle collisions or falls. Penetrating injuries in the area of the urethra may also cause urethral trauma. Straddle injuries may cause both short- and long-term problems. Iatrogenic injury to the urethra from traumatic catheter placement, transurethral procedures, or dilation is not uncommon.
Problem
Urethral injuries can be classified into 2 broad categories based on the anatomical site of the trauma. Posterior urethral injuries are located in the membranous and prostatic urethra. These injuries are most commonly related to major blunt trauma such as motor vehicle collisions and major falls, and most of such cases are accompanied by pelvic fractures. Injuries to the anterior urethra are located distal to the membranous urethra. Most anterior urethral injuries are caused by blunt trauma to the perineum (straddle injuries), and many have delayed manifestation, appearing years later as a urethral stricture.
External penetrating trauma to the urethra is rare, but iatrogenic injuries are quite common in both segments of the urethra. Most are related to difficult urethral catheterizations.
Epidemiology
Frequency
Posterior urethral injuries are most commonly associated with pelvic fracture, with an incidence of 5%-10%. With an annual rate of 20 pelvic fractures per 100,000 population, these injuries are not uncommon.[1] Anterior urethral injuries are less commonly diagnosed emergently; thus, the actual incidence is difficult to determine. However, many men with bulbar urethral strictures recall an antecedent perineal blunt injury or straddle injury, making the true frequency of anterior urethral injury much higher. Penetrating injury to the urethra is rare, with major trauma centers reporting only a few per year.
Etiology
As with many traumatic events, the etiology of a urethral injury can be classified as blunt or penetrating. In the posterior urethra, blunt injuries are almost always related to massive deceleration events such as falls from some distance or vehicular collisions. These patients most often have a pelvic fracture involving the anterior pelvis.[2] Blunt injury to the anterior urethra most often results from a blow to the bulbar segment such as occurs when straddling an object or from direct strikes or kicks to the perineum. Blunt anterior urethral trauma is sometimes observed in the penile urethra in the setting of penile fracture.
Penetrating trauma most often occurs to the penile urethra. Etiologies include gunshot and stab wounds. Iatrogenic injuries to the urethra occur when difficult urethral catheterization leads to mucosal injury with subsequent scarring and stricture formation. Transurethral procedures such as prostate and tumor resections and ureteroscopy can also lead to urethral injury.
Pathophysiology
Injury to the posterior urethra occurs when a shearing force is applied at the prostatomembranous junction in blunt pelvic trauma. The prostatic urethra is fixed in position because of the attachments of the puboprostatic ligaments. Displacement of the bony pelvis from a fracture type injury thus leads to either tearing or stretching of the membranous urethra.[3]
Anterior urethral injury most often results from a blunt force blow to the perineum, producing a crushing effect on the tissues of the urethra. The initial injuries are often ignored by the patient, and urethral injury manifests years later as a stricture. The
stricture results from scarring induced by ischemia at the site of the injury. Penetrating injuries also occur in the anterior urethra as a result of external violence.
Presentation
Diagnosis of urethral injuries requires a reasonably high index of suspicion. Urethral injury should be suspected in the setting of pelvic fracture, traumatic catheterization, straddle injuries, or any penetrating injury near the urethra. Symptoms include hematuria or inability to void. Physical examination may reveal blood at the meatus or a high-riding prostate gland upon rectal examination. Extravasation of blood along the fascial planes of the perineum is another indication of injury to the urethra. "Pie in the sky" findings revealed by cystography usually indicate urethral disruption.
The diagnosis of urethral trauma is made by with retrograde urethrography, which must be performed prior to insertion of a urethral catheter to avoid further injury to the urethra. Extravasation of contrast demonstrates the location of the tear. Further management is predicated on the findings of urethrography in combination with the patient's overall condition. Urethrogram demonstrating partial urethral disruption. Urethrogram demonstrating complete urethral disruption.
Relevant Anatomy
The male urethra may be divided into 2 portions. The posterior urethra includes the prostatic urethra, which extends from the bladder neck through the prostate gland. It then joins the membranous urethra, which lies between the prostatic apex and the perineal membrane. The anterior urethra begins at that point and includes 3 segments. The bulbar urethra courses through the proximal corpus spongiosum and ischial cavernosus-bulbospongiosus muscles to reach the penile urethra. The penile urethra then extends through the pendulous portion of the penis to the final segment, the fossa navicularis. The fossa navicularis is invested by the spongy tissue of the glans penis.
Potential areas for injury can be deduced from further study of the urethral anatomy. The membranous urethra is prone to injury from pelvic fracture because the puboprostatic ligaments fix the apex of the prostate gland to the bony pelvis and thus cause shearing of the urethra when the pelvis is displaced. The bulbar urethra is susceptible to blunt force injuries because of its path along the perineum. Straddle-type injuries from falls or kicks to the perineal area can result in bulbar trauma. Conversely, the penile urethra is less likely to be injured from external violence because of its mobility, but iatrogenic injury from catheterization or manipulation can occur, which is also possible in the fossa navicularis.
Contraindications
In cases of urethral trauma, patients often have multiple injuries. Immediate urethral repair is relatively contraindicated because life-threatening injuries must be corrected first

in any trauma algorithm. Urethral repair should be undertaken after the patient has stabilized, when hemorrhage is less of a concern. If open repair is planned, it is better to allow the pelvic hematoma to subside prior to the procedure.
Penetrating anterior urethral injuries should be explored; however, defects longer than 2 cm in the bulbar urethra and longer than 1.5 cm in the penile urethra should never be emergently repaired. They should be reconstructed at an interval following the injury to allow for resolution of other injuries and proper planning of the tissue transfers required for the repair.[4]
Ureteral Trauma
Background
Ureteral injuries due to external trauma are rare. The ureter is well-protected in the retroperitoneum by the bony pelvis, psoas muscle, and vertebrae. Damage to the ureter usually results from a significant traumatic event that is almost always associated with collateral injury to other abdominal structures. Much of the presentation and management of ureteral injuries are dictated by the severity and management of the associated injuries. This article discusses the etiology, presentation, evaluation, and management of ureteral injuries due to external causes.
For excellent patient education resources, visit eMedicine's Kidneys and Urinary System Center. Also, see eMedicine's patient education articles Blood in the Urine and Intravenous Pyelogram.
Etiology
While injuries to the ureter can result from external trauma, iatrogenic causes are more common. These are usually associated with abdominopelvic surgery or ureteroscopy. Reported intraoperative injuries include ligation, transection, electrocautery, and avulsion. The ureter can be secondarily affected during fibrotic or inflammation reactions. Iatrogenic injuries are typically isolated and thus tend to present differently from those associated with external violence.
External trauma
The ureter is involved in less than 1% of all genitourinary injuries caused by external trauma. External trauma can be penetrating (ie, gunshot wounds, stab wounds) or blunt. Interestingly, when all penetrating and blunt traumas were evaluated, the ureter was damaged in less than 4% and 1% of cases, respectively. The type of external trauma also matters; gunshot wounds accounted for 91% of injuries, with stab wounds and blunt trauma accounting for 5% and 4%, respectively.[1]

The relative frequency of ureteral involvement in gunshot trauma is related to the mechanism of the injury. Ballistic injuries affect the ureter in two ways. First, they may directly injure the ureter with varying degrees of severity, ranging from a contusion to complete transection. Secondly, the intramural blood supply of the ureter may be disrupted, resulting in ureteral necrosis. Microvascular studies have shown that this damage may extend as far as 2 cm above and below the point of transection, suggesting that the zone of bullet-associated ureteral injuries extend beyond what is observed grossly. Fortunately, fewer than 3% of gunshot injuries involve the ureters.
Stab wound–related injuries to the ureter are less common than those caused by gunshot injuries. Nevertheless, long-bladed weapons or stab-wounds posterior to the midaxillary line should always raise suspicion for possible ureteral involvement.
Blunt trauma can cause ureteral injury from several mechanisms. These mostly involve deceleration or acceleration mechanisms with sufficient force to disrupt the ureter from either the ureteropelvic or ureterovesical junctions. Such injuries can result from a high-speed motor-vehicle collision, a fall from a significant height, or a direct blow to the region of the L2-3 vertebrae.
Iatrogenic causes Gynecologic surgery
o The abdominal hysterectomy was once the most common cause of iatrogenic ureteral injury. However, ureteral injuries can occur during any abdominopelvic surgery. Risk factors for ureteral injury during open surgery include previous operations, bulky tumors, retroperitoneal fibrosis, previous radiation, inflammatory processes, ureteral duplication, and ectopic kidneys. These all have the potential to alter the expected course of the ureter. Iatrogenic injury may result from crushing, suture ligation, devascularization, electrocautery, cryoablation, avulsion, or transection of the ureter.
o Approximately 52%-82% of surgical ureteral injuries occur during gynecologic procedures. Hysterectomy accounts for most of these cases. However, the modality used plays a role; ureteral injury occurs 1.3%-2.2% of abdominal hysterectomies and in only 1.3% and 0.03% of laparoscopic and vaginal hysterectomies, respectively.[2, 3, 4, 5, 6] The risk factors for ureteral injury include a large uterus, pelvic organ prolapse, and prior pelvic surgery. The injury typically occurs in the distal ureter in the region of the infundibulopelvic ligament or as a ureter crosses inferior to the uterine artery, often from blind clamping and ligature placement to control hemorrhage. The ureter may also be injured during laparoscopic gynecologic procedures, most commonly by cauterization or clipping. Interestingly, 33%-87% of ureteral injuries caused during laparoscopic surgery are not recognized at the time.[7, 8, 9, 6]
Colorectal surgery: After gynecologic procedures, colorectal surgery is the next most common cause of iatrogenic ureteral injuries. Together, low anterior resection (LAR) and abdominal perineal resection (APR) account for 9% of all

such incidences in a combined series and 67% of all general surgical injuries. The incidence of ureteral injury during LAR or APR is 0.3%-5.7%.[10] The left ureter is involved more commonly than the right, as it may be elevated with the sigmoid mesentery and mistaken for a mesenteric vessel.
Vascular surgery o The overall incidence of ureteral involvement during vascular surgery has
been reported as 2%-4%. Ureteral injury may result from direct injury during the procedure or may present as a fistula or hydronephrosis postoperatively. Patients undergoing repeat aortoiliac surgery appear to be at the greatest risk for ureteral injury.
o The incidence of asymptomatic hydronephrosis after abdominal vascular surgery has been estimated to be as high as 20%, while only 2% of cases are symptomatic. Of those who are symptomatic, 35% present within 2 months, 50% within 12 months, and 18% after 5 years.[11] Risk factors include ureteral devascularization, retroperitoneal fibrosis, radiation exposure, graft infections, graft dilations, false aneurysms, and anterior graft placement. In patients with early obstruction (< 6 mo), it tends to resolve spontaneously.
o Another condition related to vascular surgery is the development of an aortoureteric or graft-ureteric fistula, which can lead to massive hematuria and vascular collapse. The risk factors for the development of the fistulae include anterior graft placement, prolonged use of a ureteral stent, compression, and obstruction.
Urologic procedures o Ureteral injuries that occur during urologic procedures are becoming
increasingly common. In a recent series, they comprised 42% of all iatrogenic injuries.[12] The increased incidence of ureteral injuries during urologic procedures is directly related to the increased use of ureteroscopic equipment. Endoscopic procedures accounted for 79% of injuries, while open surgery accounted for 21%. Most of these injuries occurred in the distal ureter (87%).[12] The injuries include perforation, stricture, avulsion, false passage, intussusception, and prolapse into the bladder. Risk factors for these injuries include radiation, tumor, inflammation, and impacted stones. Injury also may be related to the equipment used, such as wires, baskets, and lithotriptors (eg, electrohydraulic lithotriptor [EHL]).
o The increasing use of thermoablation and cryoablation for renal tumors have placed the ureter is at risk for injury. This risk is theoretically higher for lower pole and medially located tumors.
Other iatrogenic causes o Other surgical procedures that may injure the ureters include spinal
surgery for disc disease, vaginal surgery for pelvic prolapse, and appendectomy.
o Radiation injury to the ureter is rare. The ureter is more resistant to the effects of radiation than the bladder. The incidence of ureteral obstruction due to radiation is 0.04%, while the incidence of obstruction due to recurrent tumor is 95%.
Presentation
The key to managing any ureteral injury, regardless of its etiology, is maintaining a high index of suspicion.
Most iatrogenic injuries (70%-80%) are diagnosed postoperatively. The presenting signs and symptoms may include flank pain (36%-90%), fever and sepsis (10%), fistula (ureterovaginal and/or ureterocutaneous), urinoma, prolonged ileus, or renal failure secondary to bilateral obstruction (10%).[5] Other rare but reported injuries include an aortoureteric or graft-ureteric fistula, which may present as mild-to-massive gross hematuria, or a silent obstruction, which can present later as hypertension and nephrotic syndrome. Again, with the patient's history in mind, findings on a physical examination performed carefully may be revealing, especially in light of the following signs: an abdominal or flank mass, costovertebral angle tenderness, peritoneal signs, or fluid drainage from the wound or vagina.
In patients with external trauma, ureteral involvement may not be obvious, especially when associated with multiorgan involvement. Therefore, the diagnosis of a ureteral injury may be delayed as other critical injuries are addressed. Nevertheless, as discussed above, a high index of suspicion for ureteral involvement must be maintained.
Indications
The choice of treatment is based on the location, type, extent, and timing of presentation, as well as the patient's medical history, overall condition, and survival prognosis (see Surgical therapy).
Relevant Anatomy
The ureters are peristaltic tubular structures that course from the kidney to the bladder in the retroperitoneum. Histologically, they are composed of an outer serous layer, a smooth muscle layer, and an inner mucosal layer. The smooth muscle layer consists of 2 circular layers separated by a longitudinal layer. The ureters can be divided into 3 segments. The proximal ureter is the segment that extends from the ureteropelvic junction to the area where the ureter crosses the sacroiliac joint, the middle ureter courses over the bony pelvis and iliac vessels, and the pelvic or distal ureter extends from the iliac vessels to the bladder. The terminal portion of the ureter may be subdivided further into the juxtavesical, intramural, and submucosal portions.
The ureters are at risk during open surgery because of their proximity to many abdominal and pelvic structures. They lie anterior to the psoas muscles and adhere to the posterior peritoneum. The left ureteropelvic junction is posterior to the pancreas and duodenal-jejunal junction. On the right, it lies posterior to the duodenum and just lateral to the inferior vena cava (IVC). The left ureter is crossed anteriorly by the inferior mesenteric artery and sigmoidal vessels. The right ureter is crossed by the right colic and ileocolic

vessels. As they descend into the pelvis, the ureters course anterior to the iliac vessels but posterior to the gonadal vessels.
In males, the ureter is crossed anteriorly by the medial umbilical ligament, and, before entering the bladder, it passes under the vas deferens. In females, the ureter courses posterior to the ovary, lateral to the infundibulopelvic ligament, and medial to the ovarian vessels. It then passes posterior to the broad ligament and lateral to the uterus. As the ureter approaches the bladder, it is about 2 cm lateral to the cervix. The uterine vessels run just anterior to the ureter near the ureterovesical junction. Most commonly, the ureter is injured in the ovarian fossa near the infundibulopelvic ligament and where the ureter courses posterior to the uterine vessels.
The ureteric arteries course in the adventitia longitudinally. They are supplied by branches from the renal, aortic, gonadal, iliac, and vesical arteries. The ureteric arteries are continuous in 80% of cases. In the abdominal portion, the blood supply is derived medially, and, in the pelvis, the blood supply comes from the lateral aspect. The richest blood supply is to the pelvic ureter.
Lymphatic drainage from the ureter drains to regional lymph nodes. No continuous lymph channels extend from the kidney to the bladder. The regional nodes that serve as drainage include the common iliac, external iliac, and hypogastric lymph nodes.
Contraindications
Relative contraindications to a vesicopsoas hitch include small-capacity bladders (eg, neurogenic bladder, irradiated bladders) and evidence of significant bladder outlet obstruction.
Relative contraindications to a Boari bladder flap include small, contracted, irradiated, and neuropathic bladders; transitional cell carcinoma; and previous bladder mobilization that threatens the blood supply to the pedicle.
The absolute contraindications to transureteroureterostomy (TUU) include a short donor ureter or a diseased recipient ureter. Relative contraindications include a urothelial tumor, nephrolithiasis, pelvic or abdominal irradiation, retroperitoneal fibrosis, and ureteral injury caused during aortoiliac bypass surgery.
Autotransplantation is contraindicated in patients who are older than 60 years and in those with underlying aortoiliac atherosclerosis or renal disease. The presence of retroperitoneal fibrosis is a relative contraindication because of the potential of venous obstruction.
Contraindications to ileal ureteral substitution include a serum creatinine level of greater than 2 mg/dL, neurogenic bladder, bladder outlet obstruction, inflammatory disease, radiation enteritis, and hepatic dysfunction.
Surgical treatments of injured ureters are discussed in Surgical therapy.


















