renal MR techniques V2 - Heidelberg University · 2010-03-16 · 2 Bernstein, King and Zhou:...
9
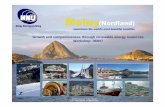
1 Prof. Dr. Stefan O. Schoenberg Professor and Chairman of Radiology Department of Clinical Radiology and Nuclear Medicine University Medicine Mannheim Annual RSNA meeting, Chicago, 2009 Annual RSNA meeting, Chicago, 2009 Renal artery disease: MR Techniques and Interpretation 1. To understand the basic technical principles of MR-Angiography with and without IV contrast agents, renal flow, perfusion and filtration measurements using magnetic resonance imaging (MRI) 2. To compare the various functional MRI techniques in terms of diagnostic value, complexity and clinical practicability 3. To demonstrate the added value of a comprehensive use of these techniques for assessment of different types of renovascular and renoparenchymal disease Learning objectives http://www.ikrn-mannheim.de/RSNA2009/renalMRtechniques.html Background N Engl J Med 2001; 344: 431-442 From macro- to microcirculation: technical possibilities of MRI MRA 0 5 10 15 20 25 30 35 0 100 200 300 400 500 600 time [ms] velocity [cm/s] Flow Michaely HJ, et al. Abdominal Imaging 2006 Possibilities of MRI Perfusion Oxygenation Inflammation Tissue structure Possibilities of MRI Dynamic MRA Time-resolved Perfusion / Filtration / Excretion 0 100 200 300 400 500 600 0 10 20 30 40 50 60 Plasma volume Tubular volume
Transcript of renal MR techniques V2 - Heidelberg University · 2010-03-16 · 2 Bernstein, King and Zhou:...

1
Prof. Dr. Stefan O. SchoenbergProfessor and Chairman of Radiology
Department of Clinical Radiology and Nuclear MedicineUniversity Medicine Mannheim
Annual RSNA meeting, Chicago, 2009Annual RSNA meeting, Chicago, 2009
Renal artery disease:MR Techniques and Interpretation
1. To understand the basic technical principles of MR-Angiography with and without IV contrast agents, renal flow, perfusion and filtration measurements using magnetic resonance imaging (MRI)
2. To compare the various functional MRI techniques in terms of diagnostic value, complexity and clinical practicability
3. To demonstrate the added value of a comprehensive use of these techniques for assessment of different types of renovascular and renoparenchymal disease
Learning objectives
http://www.ikrn-mannheim.de/RSNA2009/renalMRtechniques.html
Background
N Engl J Med 2001; 344: 431-442
From macro- to microcirculation:technical possibilities of MRI
MRA
0
5
10
15
20
25
30
35
0 100 200 300 400 500 600time [ms]
velo
city
[cm
/s]
Flow
Michaely HJ, et al. Abdominal Imaging 2006
Possibilities of MRIPerfusion
Oxygenation
Inflammation
Tissue structure
Dynamic MR-Urography
Possibilitiesof MRI
Dynamic MRA
Time-resolved Perfusion / Filtration / Excretion
0
5
10
15
20
25
30
35
0 100 200 300 400 500 600Zeit [ms]
Ges
chw
indi
gke
it[c
m/s
]
0
100
200
300
400
500
600
0
10
20
30
40
50
60
Plasma volume
Tubular volume

2
Parallel imaging, PAT ×2
26 s acquisition time, 0.9x0.9x0.9 mm
DSAMRA
Schoenberg SO et al. Radiology 2005; 235:687–698
Problem: eccentric stenoses
Voxel size: 3.4 0.7 mm3
y = 0.8208x + 6.0133R
2= 0.9087
y = 0.883x – 0.6697R
2= 0.7614
0
10
20
30
40
50
60
70
80
90
100
30 40 50 60 70 80 90 100
Degree of area stenosis on IVUS [%]
Deg
ree
of a
rea
sten
osis
on
MR
A [%
]
20
Accuracy of high res. MRA vs. IVUS
Schoenberg SO et al. Radiology 2005; 235:687–698
FMD: PAT and 3T- a perfect marriage
25s>1.5mm³
19s1mm³
16s0.65mm³
1.5T, no PAT 1.5T, PAT 3 3.0T, PAT 3
Run-off MRA: renal artery findings
3T CTM MRA1.2 mm isotropic resolution0.1mmol/kg BW Gd-DOTA
SLE: Microaneurysms & systemic imaging
Inflammatory LNs Thick pericardium Pleural effusion
Flow: Cine phase-contrast flow measurements
1 2 3 4 5
6 7 8 9 10
11 12 13 14 15
16 17 18 19 20
21 22 23 24 25
dt)( ttGVV
time [ms]
0 200 400 600 800 1000 1200
velo
city
[cm
/s]
0
5
10
15
20
25
30
35
40
45
50

3
04/1997
1998
2000
2001
08/1997
Right renal artery
0
5
10
15
20
25
30
35
0 200 400 600 800 1000 1200
time [ms]
velo
cit
y[c
m/s
]
Apr 97Aug 9720002001
Re-stenosis
Schoenberg SO, et al. Abdom Imaging 2006; 31: 200-212
Grading scheme of renal artery stenosis
time [ms]0 200 400 600 800 1000
velo
city
[cm
/s]
0
5
10
15
20
25
30
35
time [ms]0 200 400 600 800 1000
velo
city
[cm
/s]
0
5
10
15
20
25
30
35
velo
city
[cm
/s]
time [ms]0 200 400 600 800 1000
0
5
10
15
20
25
30
35
time [ms]0 200 400 600 800 1000
velo
city
[cm
/s]
0
5
10
15
20
25
30
35
grade 1 grade 2
grade 3 grade 4
Schoenberg SO, et al. JASN 2002, 13: 158-169
0
10
20
30
40
50
60
15 125 235 345 455 565 675time [ms]
Vel
ocity
[cm
/s] Left renal artery
Right renal artery
DSA
Improved grading: MRA + PC Flow Post-interventional control of hemodynamics
0 200 400 600 800 1000
velo
city
[cm
/s]
0
5
10
15
20
25
30
35
40
45 preoperativepostoperative
time [ms]0 200 400 600 800 1000
velo
city
[cm
/s]
0
5
10
15
20
25
30
35
40
45
left
right
Schoenberg SO, et al. Radiologe 1997; 37: 651-662
-20
0
20
40
60
80
100
120
140
160
1 21 41 61 81 101 121 141
AU
ds/dt (maximum)
MTT
„MR-Renography“
Time [sec]
Time to Max
Dynamic renal perfusion with Gd chelates
Michaely HJ, Schoenberg SO. Radiology 2006; 238: 586-596
Postprocessing
0
100
200
300
400
500
600
700
0 50 100
time in sec
sign
al
0
100
200
300
400
500
600
700
0 50 100 150
time in sec
sig
nal
First Pass Perfusion
0
100
200
300
400
500
600
700
0 50 100 150
time in sec
sign
al
Filtration
+
t - 0s
t - 7s
t - 11s
t - 14s
t - 70s
t - 120s

4
1,5 Tesla 3 Tesla
Advantages of 3 Tesla for renal perfusion
1.5 Tesla 3.0 Tesla P-value
Baseline SNR kidney 9.6 ± 2.4 15.6 ± 5.3 p = 0.00005
Peak SNR kidney 60.1 ± 39.0 92.1 ± 38.7 p = 0.009
Michaely HJ,…, Schoenberg SO. Invest Radiology 2007; 42: 406-411
High-Grade RAS: MRA + Perfusion
60 y/o male with hypertension
0
20
40
60
80
100
120
140
160
180
0 25 50 75t[sec]
Signal [A.U.]
100
Right kidney
Renal artery aneurysm: decreased segmental perfusion
DSA
Segmental RAS: hemodynamic significance
30 y/o male with FMD perfusiondeficit at the lower pole of the kidney
Michaely HJ, Schoenberg SO. Radiology 2006; 238: 586-596
Maximum upslope (dS/dT)
5,250
2,182
Therapy Monitoring of RAS
0
100
200
300
400
500
600
0 20 40 60 80 100 120 140 160
time [s]
sig
na
l in
ten
sity
[A
.U.]
after Stent
before Stent
before after PTA
Severe HTN with low-grade RAS
• 32 y/o female with severe HTN• RAS not significant• Biopsy: 2° nephrosclerosis0
20406080
100120140160180
0 25 50 75 100
PatientNormal

5
Patient with glomerulonephritis
Normal MRA, abnormal perfusion study
Plasma flow (80ml/100ml/min)
Tubular flow (8ml/100ml/min)
Perfusion abnormal
Perfusion normal
MRAabnormal
MRAnormal
No renal disease
Renovascular diseasewith renoparenchymaldisease
Renovascular diseaseno renoparenchymaldisease
Renoparenchymaldisease
Selection of patients for intervention
Diagnostic Approach
FP < 100< 100ml/100ml/min
FP > 100> 100ml/100ml/min
94.7%100%58.1%Negative
predictive value
92.9%90%87.5%Positive predictive
value
90%85%90%Specificity
96.3%100%51.9%Sensitivity
either/orMRP-
positiveMRA-
positive
Detection of clinically significant renal disease
Attenberger UI et al. JMRI 2009,in press
350
0
188 ml/100ml/min
194 ml/100ml/min
Fibromuscular Dysplasia Chronic renal failure
Comprehensive assessment of renal disease
100
47 ml/100ml/min47 ml/100ml/min55 ml/100ml/min55 ml/100ml/min
0
• 60 y/o male S/P RTx 5 years agowith rise of serum creatinine
• No RAS
• Biopsy revealed chronic ischemia at the upper pole
Michaely HJ, Schoenberg SO. Radiology 2006; 238: 586-596
From macroFrom macro-- to microcirculationto microcirculation
28 ± 144 ± 114 ± 74 ± 468 ± 3446 ± 37Treated Tumors
5 ± 93 ± 382 ± 6015 ± 820 ± 6150 ± 89Untreated Tumors
12 ± 221 ± 7171 ± 5815 ± 415 ± 2188 ± 45Normal Kidneys
E [%]FE [ml/100ml/min]
FP [ml/100ml/min]
VP [ml/100ml]
TTP [s]MER [%]
Therapy Monitoring with MRI
Before Therapy
After Therapy
FP FE
Notohamiprodjo M,… Michaely HJ, JMRI 20009 in press

6
Dynamic MRA at 3 T with PATDynamic MRA at 3 T with PAT
Michaely HJ, … Schoenberg SO, et al. J Magn Reson Imag 2006; 24: 1413–1419
13.5 ± 2.113.8 ± 1.7MTT [s]
10.2 ± 1.710.4 ± 1.3TTP [s]
TREAT@3,0T
TFL@1,5T
• Dynamic MRA (1.4 s temporal resolution) agrees with TurboFLASH for semi-quantitative perfusion measurements
• No significant differences for MTT and TTP between technique and field strength
Intravascular contrast agents (gadofosveset) @ 3 T:Time-resolved first pass (1.4 s temporal resolution)
Intravascular contrast agents (gadofosveset) @ 3 T:Time-resolved first pass (1.4 s temporal resolution)
Identification of target lesion
Measurement of area stenosis
Intravascular contrast agents (gadofosveset) @ 3T:Steady-State (0.9 x 0.9 x 0.9 mm)
Intravascular contrast agents (gadofosveset) @ 3T:Steady-State (0.9 x 0.9 x 0.9 mm)
CE-MRA, 1.1x1x1.2mm3 CE-MRA, 1.1x1x1.2mm3
Comprehensive protocols in the decade of NSF
Native-MRA (TrueFISP), 1x1x1mm³, 2-4min Native-MRA (TrueFISP), 1x1x1mm³, 2-4min
Non-contrast MRA: excellent in normal flow states
inconsistent results with low-flow
normal patient
Global Inversion and Readout
Selective Inversion and Readout after TI=1.2s
Subtraction of Images
Perfusion measurements with ASL (FAIR) ASL Perfusion – Improvement after therapy
• 56y/o female patient with right sided RAS (>70%)
• Affected left kidney shows reduced signal intensity
• After intervention the blood flow to the kidney is restored with signal intensity equal to the opposite side
9.2 5.50246
8101214
ASL-SNR
HealthySignificant RAS
Michaely HJ, Schoenberg SO, et al. Invest Radiol 2004; 39: 698-705

7
Courtesy of Prasad PV, et al. Circulation 1996; 94:3271-3275
Intrarenal oxygenation by BOLD MRI
• Oxyhemoglobin is diamagnetic
• Deoxyhemoglobin is paramagnetic
• R2* (1=1/T2*) is directly proportional to the tissue content of deoxyhemoglobin
• A decrease in the slope implies an increase in the Po2
of blood
• Surrogate for medullaryperfusion
Effect of Water Diuresis On Relative Medullary Oxygenation
Pre
Pre
-- wa
ter
loa
dw
ate
r lo
ad
Po
st
Po
st --
wa
ter
loa
dw
ate
r lo
ad
AnatomicalAnatomical RR22* Map* Map
Courtesy of Prasad PV J J MagnMagn ResonReson Imaging 1997; 7: 1163Imaging 1997; 7: 1163--11651165
Changes in medullary pO2 post-waterload:Effect of endogenous prostaglandins
Courtesy of Prasad PV, et al. Kidney Int 1999; 55: 294-298
Perfusion: mean transit time R
340ml/min
Mean flow 340ml/minloss of early systolic peak
Mean flow 420ml/minnormal flow profile
T2* (BOLD): oxygenation R
Perfusion: plasma flow R
45 y old male with HTN and 50% stenosis R RA
pre PTA after 1st PTA after 2nd PTA
DSA pre and post PTA Plasma flow l > 200ml/min, r 70-90ml/min
Oxygenation (BOLD)
Tubular flow
Patient with FMD and spontaneous dissection

8
a b c
Sadowski E et al, Radiology 2005
normal ATN Rejection
R2* loss – reflecting renal transplant rejection Threshold value for medullary R2* - 18/sec
Sadowski E et al, Radiology 2005
Relaxation times
Na H
Longitudinal relaxation T1 [ms] 301 9002
Transversal relaxation T2 [ms] 0.51 / 161 902
2311 1
1
1. Very short time of echo (TE)23Na:
T2s (60%)
T2F (40%)
0.0
0.2
0.4
0.6
20 40 Zeit [ms]
Amplitude
1 S. Nielles-Vallespin; PhD-thesis (2004)
2 Bernstein, King and Zhou: „Handbook of MRI Pulse Sequences“; Academic Press (2004)
Courtesy of Lothar Schad, PhD, CKM, Mannheim
Sodium Imaging
Maril N et al. (2006) Sodium MRI of the Human Kidney at 3 Tesla
3D gradient-echo sequence using an in-housebuilt quadrature surface coil with TR/TE 30/1.8 ms, FOV 38 x 38 x 24 cm3, and matrix128 x 128 x 16.
Water deprivation (12 hr) induced a significantincrease of 25% (P<0.05) in this gradient.
Magnetic Resonance in Medicine 56:1229-1234
Sodium Imaging
Healthy volunteer (5 x 5 x 5 mm3 )
Before water load After water load
Duration = 16 min; TE = 5,5ms; TR = 120ms; projections = 8000; flip angle = 85°
Sodium Imaging
Courtesy of Lothar Schad, PhD, CKM and Stefan Haneder MD, IKRN, Mannheim
Free diffusion
Restricted diffusion
Isotropy
Anisotropy
Structu
re
Analysis of tissue structure: Diffusion tensor ImagingAnalysis of tissue structure: Diffusion tensor Imaging

9
Notohamiprodjo M et al. Invest Radiol 2008; 43: 677-685
RAS: measurement of fractional anisotropy
ADC left cortex << rightFA left cortex > rightFA left medulla >> right
ADC map
FA map
Signal change :-C: -65 %-OM: -62 %-IM: -60 %
T2*w MRI pre-USPIO T2*w MRI day 3 post-USPIO
• 53 yo male with purpura, acute renal insufficiency and proteinuria
Imaging of glomerulonephritis with USPIO
• Proliferative glomerulopathy with positive CD68 inflammatory cells (55/mm2)
USPIO Imaging of the kidneys
• Phase II study in 12 patients with renal biopsy as standard of reference
• USPIO – ultra small particles of iron oxide
• 1.7–2.6 mg Fe/kg KG (Sinerem®)
• T2* imaging before and 72h after USPIO administration
• For >5 macrophages/mm² mean signal decrease in renal cortex by 33±18%
• Detection of acute transplant rejection and ATN
T2* 72h after USPIO
T2* before USPIO
Acute tubular necrosis
(ATN) day 8 after renal TPx
Hauger O, et al. Eur Radiol 2007; 17: 2898-2907
1. MRA: spatial resolution <1mm3 for accurate stenosis quantification
2. Flow measurements for detection of hemodynamic significance
3. MRP for detection of renal parenchymal disease
4. Combined approach of MRA and MRP detection of clinically significant renal disease
5. NCE-MRA + ASL + BOLD allow (future) protocols without CM
6. USPIO for detection of inflammatory disease on a cellular level
Summary
http://www.ikrn-mannheim.de/RSNA2009/renalMRtechniques.html
Acknowledgment
• Department of Clinical Radiology and Nuclear Medicine, University Medicine Mannheim:Henrik J. Michaely MD, Ulrike I. Attenberger MD, Stefan Haneder MD, Steffen J. Diehl MD
• Department of computer-assisted clinical medicine (CKM):Lothar R. Schad PhD, Frank Zoellner PhD
• Department of Radiology, Evanston, University of Chicago:Pottumarthi V. Prasad PhD
• Department of Radiology, University of Bordeaux, France:Nicolas Grenier MD
http://www.ikrn-mannheim.de/RSNA2009/renalMRtechniques.html