Renal Hemodynamics
15
REGULATION OF RENAL HEMODYNAMICS L. Gabriel Navar Department of Physiology, Tulane University School of Medicine, New Orleans, Louisiana 70112 B eginning the renal physiology section with a detailed consideration of renal microvascular dynamics allows a smooth transition from cardiovascular-related topics to kidney-related topics. In addition, reductions in renal blood flow (RBF) and glomerular filtration rate (GFR) are often associated with many pathophysiological conditions including hypertension, renal failure, heart failure, and diabetes, and it is essential for the student to obtain a solid foundation regarding the principal mechanisms regulating renal hemodynamics. The following learning objectives provide a clear guide for the student. 1) Be able to define and calculate the renal fraction of the cardiac output and the factors that influence it. 2) Know the average values for RBF and GFR in adult humans. 3) Be able to define and calculate the filtration fraction. 4) Know the major sites of renal vascular resistance and describe the hydrostatic pressure profile along the renal vasculature. 5) Describe the roles of hydrostatic and colloid osmotic pressures in regulating glomerular and peritubular capillary dynamics. 6) Explain in a quantitative manner the determinants of GFR and how these are regulated. 7) Identify the extrinsic, neural, and hormonal systems that regulate renal hemodynamics. 8) Describe the roles of the major paracrine systems that participate in the intrinsic control of renal vascular resistance. 9) Define the phenomenon of renal autoregulation and describe the myogenic mechanism and the tubuloglomerular feedback mechanism in mediating autoregulatory behavior. It is not possible to discuss all these learning objectives in the present article. Consequently, attention has been focused on those aspects that are conceptually more difficult or that cause confusion among the students. In particular, the recent recognition of multiple humoral and paracrine factors regulating renal microvascu- lar dynamics requires a very discriminating selection of specific topics. AM. J. PHYSIOL. 275 (ADV. PHYSIOL. EDUC. 20): S221–S235, 1998. The renal circulation is sometimes briefly described during the cardiovascular section of a physiology course, but this is often not done from the perspective of a renal physiologist. Because of the unique charac- teristics of the renal microvasculature, it has always seemed more appropriate to me to begin the section of the course dealing with renal, fluid, and electrolyte physiology with a detailed consideration of intrarenal microcirculatory dynamics and the factors regulating the renal circulation. Renal hemodynamics is an inte- gral aspect of renal physiology because the intrarenal hemodynamic environment determines the formation of the glomerular filtrate, the reabsorption of fluid by the peritubular capillaries, and the maintenance of a hyperosmotic medullary environment (1). These forces are controlled by the vascular smooth muscle cells of the renal vasculature, which respond to a myriad of neural, hormonal, and paracrine stimuli. Because of the close association between renal hemodynamics and renal excretory capability, it is important that the student achieve a clear understanding about the control of renal hemodynamics. Indeed, there are A P S R E F R E S H E R C O U R S E R E P O R T 1043 - 4046 / 98 – $5.00 – COPYRIGHT r 1998 THE AMERICAN PHYSIOLOGICAL SOCIETY VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998 S221
Transcript of Renal Hemodynamics

REGULATION OF RENAL HEMODYNAMICS
L. Gabriel Navar
Department of Physiology, Tulane University School of Medicine,New Orleans, Louisiana 70112
Beginning the renal physiology section with a detailed consideration of renal
microvascular dynamics allows a smooth transition from cardiovascular-related
topics to kidney-related topics. In addition, reductions in renal blood flow (RBF)
and glomerular filtration rate (GFR) are often associated with many pathophysiological
conditions including hypertension, renal failure, heart failure, and diabetes, and it is
essential for the student to obtain a solid foundation regarding the principal mechanisms
regulating renal hemodynamics. The following learning objectives provide a clear guide
for the student. 1) Be able to define and calculate the renal fraction of the cardiac output
and the factors that influence it. 2) Know the average values for RBF and GFR in adult
humans. 3) Be able to define and calculate the filtration fraction. 4) Know the major sites
of renal vascular resistance and describe the hydrostatic pressure profile along the renal
vasculature. 5) Describe the roles of hydrostatic and colloid osmotic pressures in
regulating glomerular and peritubular capillary dynamics. 6) Explain in a quantitative
manner the determinants of GFR and how these are regulated. 7) Identify the extrinsic,
neural, and hormonal systems that regulate renal hemodynamics. 8) Describe the roles of
the major paracrine systems that participate in the intrinsic control of renal vascular
resistance. 9) Define the phenomenon of renal autoregulation and describe the
myogenic mechanism and the tubuloglomerular feedback mechanism in mediating
autoregulatory behavior. It is not possible to discuss all these learning objectives in the
present article. Consequently, attention has been focused on those aspects that are
conceptually more difficult or that cause confusion among the students. In particular, the
recent recognition of multiple humoral and paracrine factors regulating renal microvascu-
lar dynamics requires a very discriminating selection of specific topics.
AM. J. PHYSIOL. 275 (ADV. PHYSIOL. EDUC. 20): S221–S235, 1998.
The renal circulation is sometimes briefly describedduring the cardiovascular section of a physiologycourse, but this is often not done from the perspectiveof a renal physiologist. Because of the unique charac-teristics of the renal microvasculature, it has alwaysseemed more appropriate to me to begin the sectionof the course dealing with renal, fluid, and electrolytephysiology with a detailed consideration of intrarenalmicrocirculatory dynamics and the factors regulatingthe renal circulation. Renal hemodynamics is an inte-gral aspect of renal physiology because the intrarenal
hemodynamic environment determines the formationof the glomerular filtrate, the reabsorption of fluid bythe peritubular capillaries, and the maintenance of ahyperosmotic medullary environment (1). These forcesare controlled by the vascular smooth muscle cells ofthe renal vasculature, which respond to a myriad ofneural, hormonal, and paracrine stimuli. Because ofthe close association between renal hemodynamicsand renal excretory capability, it is important that thestudent achieve a clear understanding about thecontrol of renal hemodynamics. Indeed, there are
A P S R E F R E S H E R C O U R S E R E P O R T
1043 - 4046 / 98 – $5.00 – COPYRIGHT r 1998 THE AMERICAN PHYSIOLOGICAL SOCIETY
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S221

many clinical problems that are linked to derange-ments in renal hemodynamics, and assessment ofglomerular filtration rate (GFR), either directly orindirectly, based on plasma creatinine concentrations,is an important part of most nephrological exams.
Recent developments related to endothelial factorsregulating vascular smooth muscle cells and the forma-tion of numerous vasoactive agents by the epithelialcells have revealed the complexity of the varioushumoral and paracrine systems interacting to controlrenal hemodynamics (28). It is clearly not possible tocover all of these aspects in the limited time availablein the medical physiology course, and thus difficultdecisions must be made regarding the appropriatedepth necessary to provide students with an adequateunderstanding of renal hemodynamics.
Starting the section on renal physiology with a discus-sion of overall cardiovascular dynamics and renalhemodynamics allows a smooth transition from cardio-vascular-related topics to kidney-related issues. As anentry point, I start with an overall discussion of saltand water homeostasis, which links the long-termcontrol of blood volume, cardiac output, and arterialpressure with sodium balance and the control of
extracellular fluid volume, using an illustration shownin Fig. 1. This drives home the concept championedby Homer Smith, ‘‘In the last analysis, it is the ability ofthe kidneys to respond rapidly and appropriately todeviations in body fluid volume and composition thatenables us to maintain a constant internal environ-ment.’’
THE MAGNITUDE OF RENAL BLOOD FLOW
Once the more holistic issues are covered, it becomeseasier to explain the huge magnitude of renal bloodflow (RBF). About 20% of the cardiac output (renalfraction) goes to the kidneys, which means that,expressed per unit of weight, RBF is 10–50 timesgreater than for most other organs. It is also worth-while to emphasize that the RBF is far in excess ofwhat is needed to provide the O2 and metabolic needsof the kidneys. Even though O2 consumption by thekidneys per unit of organ weight is still very highbecause of the extensive activity of the sodium-potassium ATPase in the transporting epithelial tis-sues, the supply is many times greater than needed(1). The exception is the renal medulla. Because of theunique countercurrent arrangement of the vasa recta,there is substantial O2 shunting from the descending
FIG. 1.Salt and water homeostasis. Interrelationships among salt and water intake, extracellularfluid volume, cardiovascular function, and renal function are shown.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S222

vasa recta to the ascending vasa recta, and thus the O2
supply to the deep medullary structures is ratherlimited, requiring a greater degree of anaerobic metabo-lism in this region. Nevertheless, the very high bloodflow perfusing renal cortical tissue has led to theconclusion that the mechanisms that regulate RBF aredistinct from the metabolically linked mechanismsthat regulate blood flow to other tissues.
THE NEPHROVASCULAR UNIT
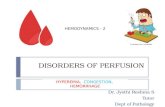
It is extremely important to go over the characteristicsof the nephrovascular unit in detail and emphasize theunique nature of the dual microvascular beds that arein series, namely, the glomerular and postglomerularvascular beds, and also the important differencesbetween the cortical peritubular vasculature and themedullary vasculature (25, 26). A review of the criticalmorphology is appropriate. The differences in theforces operating within the glomerular and peritubu-
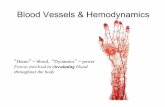
lar capillary systems should also be discussed in detail.A diagram such as that of Fig. 2 describing thehydrostatic pressure profile along the nephrovascularis very useful. The diagram helps the student under-stand the specific roles of the preglomerular resis-tance, which is localized primarily to the afferentarterioles, and the postglomerular resistance, which isimposed primarily by the efferent arterioles. The‘‘nesting’’ of the glomerular capillaries between theafferent and the efferent arterioles allows the mainte-nance of a high glomerular pressure that can beregulated very precisely. The diagram helps explainthat the high glomerular pressure is primarily respon-sible for formation of filtrate and that the low hydro-static pressure within the peritubular capillaries al-lows the elevated plasma colloid osmotic pressure topredominate and thus be responsible for the return ofthe tubular reabsorbate to the circulation. Once thequalitative considerations are clearly established, it is
FIG. 2.Representative hydrostatic pressure profile along nephrovascular unit. Equations forcalculating preglomerular (afferent) and efferent resistances and normal values forhumans are provided. RA and RE, afferent and efferent arteriolar resistances; RBF, renalblood flow; RPF, renal plasma flow: PRA, renal arterial pressure, PG, glomerular pressure;PC, peritubular capillary pressure; GFR, glomerular filtration rate; FF, filtration fraction.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S223

then useful to analyze glomerular dynamics quantita-tively so that the students obtain a clear understandingof the determinants of effective filtration pressure.
GLOMERULAR DYNAMICS AND GFR
Consideration of glomerular dynamics has beenclouded somewhat by the concept of ‘‘filtration equi-librium’’ and its significance (17). The available textstreat this issue very differently, and this topic oftencauses a great deal of confusion among the students.However, the concepts can be explained reasonablywell without going into excessive detail.
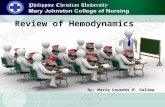
The filtration process can operate under one of twoconditions. The first condition is the case in whichfiltration continues throughout the entire length ofthe glomerular capillaries and in which there remainsa finite positive effective filtration pressure at theefferent end of the glomerular capillaries. This patternof continued filtration throughout the glomerularcapillaries is thought to be the norm in humans and isdepicted in Fig. 3. Under these conditions, the average
values for the intraglomerular determinants provide aclose approximation of the actual integrated values,and the following equation is sufficient
GFR 5 Kf(PG 2 PB 2 PG)
where Kf is the filtration coefficient, PG is the glomeru-lar hydrostatic pressure, PB is the counteracting pres-sure in Bowman’s space, and PG is the average colloidosmotic pressure in the glomerular capillaries. Theterms within parentheses define the effective filtrationpressure (EFP).
A detailed discussion of the regulation of the filtrationcoefficient is beyond the scope of the first-year coursebecause there is still no clear consensus on how muchphysiological regulation there is; nevertheless, theimportant role of decreases in the filtration coefficientin certain pathophysiological conditions such as hyper-tension, diabetes, and glomerulosclerosis should be ex-plained. This can occur as a consequence of changes ineither the surface area or the hydraulic conductivity.
FIG. 3.Summary of glomerular and peritubular capillary dynamics with represen-tative values for humans. EFP, effective filtration pressure; PG, PC, and PI,plasma colloid osmotic pressure in glomerulus, peritubular capillaries,and renal interstitium, respectively; RV, vascular resistance of renalvenous system; Kf, glomerular filtration coefficient; PCU, peritubularcapillary uptake; ERP, effective reabsorptive pressure; Kr, reabsorptioncoefficient of peritubular capillaries.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S224

The alternative filtration process occurs when theincrease in colloid osmotic pressure within the glo-merular capillaries is so rapid that the forces opposingfiltration become equal to the forces favoring filtrationat some point within the capillary system. This condi-tion is termed filtration equilibrium (17). Underequilibrium conditions, the latter part of the availablefiltering surface area is not utilized and becomes afunctional reserve. Under conditions of filtrationequilibrium, an increase in plasma flow minimizes theincrease in colloid osmotic pressure along the lengthof the glomerular capillaries. Thus effective filtrationpressure is not dissipated as quickly, and the point ofequilibration of hydrostatic and colloid osmotic forcesis moved toward more terminal sites, which, in effect,results in recruitment of additional filtering surfacearea and an increase in the functional Kf. Conse-quently, increases in plasma flow will increase theGFR proportionately even when glomerular capillarypressure is unchanged. In the case of filtration disequi-librium, increases in plasma flow increase GFR onlymodestly as a consequence of a reduced colloidosmotic pressure profile, and there is no net recruit-ment of previously unused surface area. Thus themagnitude of the effects of selective increases inplasma flow is greater during filtration pressure equilib-rium than during nonequilibrium conditions. In eithercase, however, the hydrostatic pressure gradient isstill the most significant determinant of GFR (1). It issometimes suggested erroneously that glomerular pres-sure is not the main determinant of GFR when thesystem is in filtration equilibrium. In humans, the lowfiltration fraction and the relative lack of plasma flowdependence of GFR indicate that the filtration processcontinues throughout the entire length of the glomeru-lar capillaries. If time is very limited, it is not reallynecessary to discuss the concept of filtration equilib-rium, and filtration dynamics can be explained ad-equately by considering the average forces operatingacross the glomerular capillary. Every student shouldclearly understand and be able to work problemsbased on average values for the intraglomerular forces.
Another aspect of glomerular dynamics that oftencauses a great deal of confusion is related to therelative effects of selective changes in afferent andefferent arteriolar resistances on GFR and RBF. Theratio of GFR to renal plasma flow is the filtration
fraction, and many students, teachers, and cliniciansmake the serious mistake of using the changes infiltration fraction to estimate the relative changes inthe pre- and postglomerular resistances in response toa specific stimulus or drug. It is often stated that renalvasoconstriction associated with an increase in filtra-tion fraction and renal vasodilation associated withdecreases in filtration fraction indicate that the resis-tance changes occurred predominately at efferentarterioles. However, this conclusion fails to recognizethat disproportionate changes in GFR and RBF alsooccur when both resistances are altered (1). Theconfusion can be clarified by consideration of theeffects of increases or decreases in afferent or efferentarteriolar resistances on glomerular dynamics andGFR. A selective increase in afferent resistance re-duces both plasma flow and glomerular hydrostaticpressure; however, GFR decreases more than plasmaflow, and thus the filtration fraction falls. In contrast,an increase in efferent arteriolar resistance reducesplasma flow but increases glomerular pressure. GFRinitially increases slightly but eventually decreasesbecause of the counteracting effects of the increasesin glomerular colloid osmotic pressure. Thus RBF fallsmore than GFR, and the filtration fraction increases.However, combined increases in afferent and efferentresistances also reduce the plasma flow more than theGFR, and the filtration fraction increases. Likewise,when a drug such as an angiotensin converting-enzyme (ACE) inhibitor increases RBF without increas-ing GFR, this can be explained best by combineddecreases in both afferent and efferent arteriolarresistances and not by a selective decrease in efferentarteriolar resistance as is often concluded. It can bereadily appreciated that a selective decrease in effer-ent arteriolar resistance would increase blood flowand markedly lower GFR, because the associateddecreases in glomerular pressure would cause dispro-portionately much greater relative decreases in effec-tive filtration pressure and, thus, GFR (10). Actually,this problem can be expanded in laboratory sessions,and there are several good mathematical models thatcan be used to explain the effects of various combina-tions of changes in afferent and efferent arteriolarresistances on glomerular pressure and GFR (10). Ifthe students can obtain a clear understanding of thefundamental aspects of these difficult issues, they areless likely to be confused in future discussion.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S225

REGULATION OF RENAL VASCULARRESISTANCE AND THEAUTOREGULATORY MECHANISM
Once the basic forces operating across the glomerularand peritubular capillary membranes are appreciated,the students then can readily recognize the impor-tance of the mechanisms that regulate vascular smoothmuscle tone in the renal microcirculation. The majorchallenge in teaching this section is how to limitdiscussion to the most critical control factors. If theteacher attempts to discuss every humoral, paracrine,endothelial, and neural factor that has been identifiedto date (23, 28), the litany will be quite confusing tothe students and they likely will not remember the keyfundamentals.
The regulatory systems can be categorized as thoseoriginating outside the kidney (such as circulatingvasoactive agents or renal sympathetic nerve activity)and those intrinsic to the kidney. The autoregulatoryintrinsic mechanism is responsible for maintainingRBF and GFR within narrow limits in the face of avariety of external perturbations including alterationsin arterial pressure. This autoregulatory mechanism isimportant in stabilization of the glomerular pressure
and filtered volume to the tubules under conditions ofmoderate variations in cardiovascular function. Forexample, mean arterial pressure may decrease asmuch as 15–20 mmHg during deep sleep. Without anautoregulatory response, this would lead to decreasesin glomerular pressure and GFR. In addition, thekidney is protected from the effects of variations inarterial pressure due to normal daily activities. Evensmall increases in arterial pressure can cause markedincreases in filtered load and sodium excretion in theabsence of normal autoregulatory capability. Thusautoregulation is a continuously operating negativefeedback servocontrol system that maintains an opti-mum filtered load in the face of varying externalinfluences. Autoregulation also contributes to thekidney’s reserve capability that can be utilized inresponse to a variety of injurious processes that couldotherwise lead to diminished renal function.
As illustrated in Fig. 4, autoregulatory responses aremediated by active adjustments of smooth muscletone, primarily in the afferent arterioles. This explainsthe highly efficient autoregulation of both RBF andGFR in response to changes in perfusion pressure. Inaddition, the intrarenal pressure in the glomerular and
FIG. 4.Renal autoregulation. In response to alterations in renal arterial pressure, PG, proximaltubular pressure (PPT), and PC all exhibit autoregulatory behavior in association with RBFand GFR. These parallel responses indicate that the predominant site of the vascularresistance changes is preglomerular (RA). RE does not change very much during theautoregulatory response.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S226

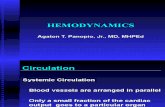
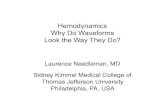
peritubular capillaries and in the proximal tubulesexhibit autoregulatory behavior, again indicating thatthe major site for autoregulatory resistance adjust-ments is preglomerular. As shown in Fig. 5, there aretwo mechanisms mediating renal autoregulation: themacula densa tubuloglomerular feedback (TGF) mech-anism and the myogenic mechanism. The myogenicmechanism allows preglomerular arterioles to sensechanges in vessel wall tension and respond withappropriate adjustments in vascular tone. An increasein wall tension, occurring as a passive response to anelevation in arterial pressure, stimulates a sensorelement and initiates vascular smooth muscle contrac-tion. Interlobular arteries and afferent arterioles ex-hibit myogenic responses to changes in wall tension.The macula densa-TGF mechanism responds to distur-bances in distal tubular fluid flow past the maculadensa. Increases in flow elicit vasoconstriction,whereas decreases in flow cause vasodilation. Micro-puncture experiments have shown that increases indistal volume delivery in a single nephron elicitreductions in single-nephron GFR (SNGFR), glomeru-lar capillary hydrostatic pressure, and glomerularplasma flow. Furthermore, interruption of fluid deliv-ery to the distal nephron increases SNGFR abovevalues obtained under conditions of maintained distalflow. This manipulation, depicted in Fig. 6, opens thefeedback loop and impairs autoregulation of SNGFRand glomerular pressure, indicating that an intact TGFmechanism is required for complete and efficient
autoregulation. Autoregulatory responses seen at thelevel of the whole kidney thereby represent onemanifestation of this homeostatic mechanism, whichmaintains a balance between filtered load and thereabsorptive capabilities of each nephron.
Several recent experiments have demonstrated that aresidual autoregulatory capacity, although with sub-stantially diminished efficiency, occurs during block-ade of the TGF mechanism. Thus both the myogenicmechanism and the TGF mechanism participate in theautoregulatory response of the renal vasculature, butthe TGF mechanism is responsible for the extremelyhigh autoregulatory efficiency characteristic of therenal microvasculature. Autoregulatory behavior hasbeen demonstrated in all regions of the kidney, anddeep nephrons autoregulate as efficiently as superfi-cial nephrons. Thus the autoregulatory mechanismprovides a critical mechanism for stabilizing the micro-circulatory environment throughout the kidney.
The TGF mechanism contributes significantly to theoverall regulation of GFR and, ultimately, to thelong-term control of sodium balance and extracellularfluid volume. By operating in concert with glomerulo-tubular balance, the TGF mechanism stabilizes deliv-ery of volume and solute to the distal nephron. Undernormal conditions, flow-related changes in the tubularfluid composition at the macula densa are sensed and
FIG. 5.Myogenic (left) and tubuloglomerular feedback (TGF) mechanisms (right) mediating renal autoregulatory responses.Myogenic mechanism is intrinsic to arterial tree and regulates blood flow by regulating transmural wall tension (T).Tension is determined by the pressures inside (Pi ) and outside (Po) and by the radius (R). TGF mechanism primarilyregulates tubular fluid composition (osmolality, NaCl concentration) at level of macula densa and adjusts filtered load byregulating afferent arteriolar tone. Direct lines indicate direct effects, and dashed lines indicate inverse effects. [TGFdiagram adapted from Braam et al. (6).]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S227

signals are transmitted to the afferent arterioles toregulate the filtered load. Early distal tubular fluid ishypotonic (,100 mosmol/kg H2O), and its composi-tion is closely coupled to fluid flow along the ascend-ing loop of Henle such that increases in flow causeincreases in tubular fluid osmolality and NaCl concen-tration at the macula densa. The specific intraluminalconstituent and the intracellular transduction mecha-nisms responsible for mediation of feedback signalsremain unresolved, and it is best not to get into toomuch detail in explaining these issues to the students.However, the inquisitive students will be curiousabout the mechanisms and mediators involved. At thecellular level, it has been postulated that increases intubular fluid osmolality elicit increases in cytosolicCa21 concentration in macula densa cells, whichresult in the release of a vasoconstrictive factor fromthese cells. Suggested mediators of TGF include purin-ergic compounds, such as adenosine or ATP, and oneor more of the eicosanoids, such as 20-hydroxyeico-satetraenoic acid. The factor mediating TGF responsesvasoconstricts afferent arteriolar vessels through theopening of voltage-gated Ca21 channels in vascularsmooth muscle cells.
The sensitivity of the TGF mechanism can be modu-lated by many agents and circumstances, some ofwhich are associated with changes in extracellularfluid volume. TGF sensitivity is diminished duringvolume expansion, thus allowing a greater delivery offluid and electrolytes to the distal nephron for anygiven level of GFR. By allowing GFR to be maintainedor even augmented at elevated distal nephron volumedelivery rates, reductions in TGF sensitivity allowcorrection of the volume expansion. In contrast,contraction of extracellular fluid and blood volume isassociated with an enhanced sensitivity of the TGFmechanism, which, together with an augmented proxi-mal reabsorption, helps to conserve fluid and electro-lytes. One major regulator of TGF sensitivity is angio-tensin II (ANG II). In states of low ANG II activity (i.e.,extracellular volume expansion, salt loading) the TGFmechanism is less responsive, whereas feedback sensi-tivity is enhanced during conditions of high ANG IIactivity such as that occurring during dehydration,hypotension, or hypovolemia. As shown in Fig. 6,several other hormones that are responsive to thestatus of extracellular fluid volume also participate inmodulating TGF sensitivity (23).
FIG. 6.Schematic of micropuncture procedures used to assess TGF responses (left) and representative relation-ships between distal nephron volume delivery and single-nephron GFR TGF responses. Effects of someagents that decrease (7) sensitivity of TGF responses and agents that increase (9) sensitivity of TGFresponses are indicated. NOS, nitric oxide synthase; HETE, 20-hydroxyeicosatetraenoic acid; PGI2,prostacyclin. [Nephron illustration courtesy of Dr. Pamela Carmines.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S228

CONTRASTING THE TGF MECHANISMAND MACULA DENSA MECHANISMFOR RENIN RELEASE
In discussing the TGF mechanism, a particularlydifficult dilemma that is often raised by the inquisitivestudents relates to the role of the macula densa in thecontrol of renin release and its role in mediatingchanges in afferent arteriolar vascular tone. Uponinitial analysis, these two mechanisms seem diametri-cally opposed to each other. As explained, the TGFmechanism responds to increases in flow, which leadsto flow-dependent increases in NaCl concentrationand osmolality at the level of the macula densa. Inturn, this elicits afferent arteriolar vasoconstriction.There is also a macula densa mechanism for thecontrol of renin release. Overall, the control of reninrelease involves multiple mechanisms and is bestdiscussed in a separate session specifically focused onthe renin-angiotensin system (see Ref. 30). Neverthe-less, it is difficult to ignore the apparent dilemmaraised by the macula densa-mediated control of reninrelease. In essence, reduced flow to the macula densasuch as that occurring with reduced perfusion pres-sure, reduced filtered load, or augmented proximaltubular fluid reabsorption rate leads to decreaseddistal sodium delivery and NaCl concentration at thelevel of the macula densa. Although the initial conse-quence would be afferent arteriolar vasodilation medi-ated through the TGF mechanism, a parallel maculadensa mechanism responds to sustained reductions inNaCl concentration and elicits signals to the juxtaglo-merular cells of the afferent arterioles to increaserenin release. Renin catalyzes formation of ANG I,which is then converted to ANG II by ACE. BecauseANG II constricts the afferent and efferent arterioles,this system thus seems to be operating directly oppo-site to the tubuloglomerular feedback mechanism.Whereas the actual interrelationships between thesetwo mechanisms are quite complex (7, 8, 20), theycan be explained satisfactorily along the followinglines. The TGF mechanism is a rapidly acting mecha-nism that responds within a few seconds and adjustsafferent arteriolar resistance to maintain filtered load.It is particularly powerful in response to increases indistal volume delivery, eliciting afferent arteriolarvasoconstriction to protect against overloading of thelimited transport capability of distal nephron seg-ments. In contrast, the macula densa mechanism for
renin release responds to sustained decreases in distalNaCl concentration, which occur with decreases inarterial pressure and with decreases in extracelluarvolume (8, 20). It is important to emphasize that this isonly one of several mechanisms regulating reninrelease and that increased renal sympathetic nerveactivity is probably a more powerful regulator of reninrelease. Indeed, increases in renal nerve sympatheticactivity stimulate renin release at lower levels ofactivity than are required to elicit renal vasoconstric-tion. Regardless of the initiating signals, the stimula-tion of renin release leads to increases in intrarenalrenin content, which lead to augmented intrarenallevels of ANG II. These elevated ANG II levels theninfluence the TGF mechanism indirectly by modulat-ing the sensitivity of the vascular smooth muscle tosignals from the macula densa cells. In essence,although these two distinct macula densa mechanismsshare a common transmission station (7), they aretemporally dissociated and have their major influenceover different operating ranges. Furthermore, it isimportant to emphasize strongly that angiotensin II isnot the mediator of the TGF response but does serve avery important function, which is to modulate thesensitivity of this mechanism (20, 28).
CONTROL OF RENAL HEMODYNAMICS BY THERENIN-ANGIOTENSIN SYSTEM
The renin-angiotensin system is best treated as aseparate topic because of the multiple actions ofangiotensin II on vascular and epithelial tissues (20,22, 30). Nevertheless, its importance in regulating renalvascular function cannot be neglected, so it also mustbe discussed when mechanisms regulating renal micro-vascular function are being considered. Also, becauseof the widespread clinical use of drugs that antagonizeor block the renin-angiotensin system, this topic has avery high degree of clinical relevance. Renin is anaspartyl proteinase that cleaves the decapeptide ANGI from angiotensinogen, an a2-globulin formed primar-ily by the liver but also in the kidneys and othertissues. The major site of renin formation in thekidneys is the juxtaglomerular epithelioid cells of theafferent arteriole. Renin release is stimulated by de-creases in sodium intake, reduced extracellular fluidand blood volume, decreases in arterial pressure, andincreased sympathetic activity. ANG I generation isdetermined by renin activity because substrate availabil-ity is usually ample. The decapeptide is subsequently
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S229

cleaved to the octapeptide, ANG II, by ACE. ACE isabundant in the lungs, bound to endothelial cells, butis also found in many other organs including thekidney. The major renal sites of ACE localization areon the luminal surfaces of endothelial cells liningafferent and efferent arterioles and glomerular capillar-ies and on the proximal tubular cells bound to thebrush border. Functional data also indicate the pres-ence of ACE in the renal interstitium. ANG II can beformed from angiotensinogen extrarenally and deliv-ered in the circulation, or it may be formed locally.
Thus ANG II can function as a hormone and as aparacrine factor. Recent studies have shown thatintrarenal ANG II levels in certain compartmentswithin the kidney, including the proximal tubules andthe interstitium, are much higher than plasma levels,thus supporting the premise that much of the intrare-nal ANG II is formed endogenously (27).
The multiple actions of ANG II, some of which areshown in Fig. 7, act in concert to minimize renal fluidand sodium losses and to maintain arterial blood
FIG. 7.Multiple actions of ANG II on renal function. PT, proximal tubule; BS, Bowman’s space; GC,glomerular capillaries; EA, efferent arteriole; PC, peritubular capillaries; TAL, thickascending limb; AA, afferent arteriole. [Original drawn by Dr. Daniel Casellas.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S230

pressure (20, 22). In addition to its renal vasculareffects, ANG II stimulates aldosterone release, en-hances proximal tubular reabsorption rate, stimulatesthirst, and enhances sympathetic nerve activity. ANGII exerts powerful vascular effects that elicit decreasesin RBF and, to a lesser extent, in GFR; thus there isusually an increase in filtration fraction. Although it issometimes stated that ANG II primarily constricts theefferent arterioles, many studies have demonstratedclearly that ANG II vasoconstricts both preglomerularas well as postglomerular arterioles (9, 20, 28). Thepreglomerular effects of ANG II include direct vasocon-strictive actions as well as indirect effects caused byincreased sensitivity of the TGF mechanism, as previ-ously described. ANG II can also decrease the glomeru-lar filtration coefficient by reducing hydraulic conduc-tivity of glomerular capillaries. ANG II may alsoinfluence medullary hemodynamics at concentrationslower than those required to elicit cortical vasoconstric-tion, which may be related to the greater ANGII-receptor density in the outer medulla (1, 4, 17, 24,25, 28).
ANG II-receptor antagonists and ACE inhibitors arefrequently utilized clinically to block the effects ofendogenous ANG II in various conditions such ashypertension, congestive heart failure, and diabetes.Thus there are many patient-oriented problems thatcan be used to discuss the actions of ANG II. Duringconditions associated with an enhanced ANG II activ-ity, inhibition of the renin-angiotensin system in-creases RBF, whereas GFR either increases or does notchange. However, GFR may sometimes decrease inassociation with decreases in arterial pressure orwhen there is severe arteriolar sclerosis or stenoses.Under most conditions, however, blockade of therenin-angiotensin system causes decreases in bothpreglomerular and postglomerular resistances.
At the cellular level, ANG II increases cytosolic Ca21
concentration by enhancing Ca21 entry through volt-age-dependent Ca21 channels as well as by mobiliza-tion of the ion from intracellular storage sites. ANGII-induced depolarization of preglomerular vascularsmooth muscle cells elicits opening of voltage-gatedCa21 channels and subsequent vasoconstriction. Ac-cordingly, the preglomerular vasoconstrictor re-sponse to ANG II is blocked by Ca21-channel blockers.Interestingly, efferent arterioles respond to ANG II
even in the presence of Ca21-channel blockers, indicat-ing that there are separate vasoconstrictive mecha-nisms for ANG II-induced afferent and efferent constric-tion (9, 21, 23, 28).
ENDOTHELIAL AND OTHERPARACRINE FACTORS
As mentioned earlier, there are many paracrine agentsthat influence the renal microvasculature, and it isimpossible to cover all of them. However, it isimportant to discuss several that are clinically veryimportant. One particularly intriguing and growingarea of interest is related to the formation and releaseof paracrine agents by adjoining endothelial cells.
From studies in many organ systems, it has beendetermined that the endothelial cells respond tovarious physical stimuli (e.g., shear stress) and hor-monal agents (e.g., thrombin, bradykinin) to releasevasoactive factors. Some of these are shown in Fig. 8.The substance that has received the most intenseinvestigation recently is nitric oxide (NO), which isnow known to be endothelium-derived relaxing factor(12, 16, 28). NO is formed intracellularly by NOsynthases (NOS), which cleave NO from L-arginine. Inendothelial cells, NO is formed constitutively anddiffuses out of the cell into adjoining cells. Throughstimulation of soluble guanylate cyclase and increasedcGMP levels in smooth muscle cells, NO exertspowerful vasodilator actions. Substantial interest hasbeen focused recently on the role of NO in regulatingrenal vascular function in normal and pathophysiologi-cal conditions. Because NO is derived from arginine,several nonmetabolizable analogs of arginine havebeen used to block the formation of NO. Administra-tion of these arginine analogs causes a 25–40% in-crease in renal vascular resistance. In general, thedecreases in RBF are greater than the decreases in GFR(3, 19, 28, 31). Some of this increase in renal vascularresistance is thought to be mediated by an enhancedactivity of the renin-angiotensin system during NOblockade. There are also important interactions be-tween intrarenal ANG II and intrarenal NO such thatincreased intrarenal NO partially buffers the vascularactions of increased ANG II. Both preglomerular andpostglomerular arterioles are responsive to NO, thusexplaining why NO blockade decreases GFR less thanRBF (13, 28, 29).
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S231

Whereas it is generally recognized that NO is formedby NOS in endothelial cells, there is also growinginterest in the specific role of the neuronal isoform ofNOS that has been localized in macula densa cells (2,33). Several recent studies indicate that the NOproduced by the macula densa cells exerts an impor-tant modulating influence on the TGF mechanism thatcounteracts the vasoconstrictor response (5, 32, 34).In particular, during sustained increases in distalnephron volume and NaCl delivery, there is an in-creased activation of vasodilatory influences exertedby neuronal NOS-mediated NO (14). These recentstudies have established important roles for NO in theoverall regulation of renal hemodynamics. It shouldalso be mentioned that intrarenal NO also has impor-tant effects on sodium excretion and is thought toserve as the mediator of pressure natriuresis (18).However, the topic of pressure natriuresis is bestcovered within the context of an overall integrativediscussion on the control of arterial pressure and thepathophysiology of hypertension (22).
Renal prostaglandins or eicosanoids constitute an-other very significant paracrine family that also influ-ences renal vascular resistance, arterial pressure, so-
dium and water excretion, and renin release.Prostaglandins are synthesized from arachidonic acidat several sites within the kidney and can influence avariety of cellular processes. Although this is a verycomplex topic, it is another highly clinically relevantarea because there are so many pharmacologicalagents that target some aspect of this system. Thussome mention of the roles of these substances in thecontrol of renal hemodynamics should be included. Asshown in Fig. 9, endoperoxides (PGE2, PGF2, PGI2,and thromboxane A2) are synthesized by the cyclooxy-genase enzymatic pathway while the leukotrienes andlipoxins are formed by lipoxygenases. Administrationof PGE2 or PGI2 (prostacyclin) into the renal arterycauses vasodilation; thromboxane A2 and leukotrienesconstrict the renal vasculature. A rapidly growing fieldis related to the eicosanoids formed through thecytochrome P-450 monooxygenase enzyme system.Several of the resultant epoxides and their derivativesexert actions on both the renal vasculature and thetubules (15, 23, 28). In teaching this subject, it isworthwhile to provide the student with an overallschematic of the arachidonic acid family similar to thatshown in Fig. 9 (28). In terms of understandingmechanisms, however, it is important to focus on only
FIG. 8.Multiplicity of endothelium-vascular smooth muscle interactions with release of vasoac-tive agents. Examples of constricting and relaxing factors are indicated. EDHF, endothe-lium-derived hyperpolarizing factor; NO, nitric oxide; TXA2, thromboxane A2; EDCF,endothelium-derived constricting factor, ACE, angiotensin-converting enzyme.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S232

a few select issues that are particularly relevant. Inessence, it is currently thought that prostaglandins arenot major determinants of resting renal vascular toneunder normal states of hydration and sodium balance.In conscious animals, prostaglandin metabolites areformed at low rates and cyclooxygenase inhibitors donot appreciably alter RBF or GFR. Rather, there is ageneral consensus that prostaglandins exert protec-tive effects in response to vasoconstrictor stimuli,hypovolemic states, or hypotensive episodes. Whenthe kidney is under the sustained influence of vasocon-strictor stimuli such as elevated catecholamine levels,increased renal nerve activation and increased activityof the renin-angiotensin system, activation of prosta-glandin production helps counteract the vasoconstric-tor effects of these stimuli. When prostaglandin produc-tion is blocked with cyclooxygenase inhibitors, theunopposed actions of the coexisting vasoconstrictoragents are manifested by greater reductions in RBFand renal function (1). Thus prostaglandins may take
on a greater regulatory role in pathophysiologicalconditions that compromise renal hemodynamics. Insuch conditions, the blockade of prostaglandins withnonsteroidal antiinflammatory drugs (which blockcyclooxygenase activity) may leave unopposed thevasoconstrictor influence of elevated levels of ANG IIand catecholamines and decrease RBF, GFR, andsodium excretion. This is probably the most impor-tant clinically relevant information related to prosta-glandins that should be remembered by the students.Additional exposure to the arachidonic acid familyand the drugs that are used to block selective path-ways of formation is best left for the pharmacologycourse.
Many other vasoactive agents are produced by thekidney. Some of these agents may be released undernormal physiological conditions, whereas others mayreach effective concentrations only under adversecircumstances such as prolonged ischemia, decreases
FIG. 9.Arachidonic acid cascade showing metabolism by 3 major enzymatic pathways: cyclooxygenases, lipoxygenases, andcytochrome P-450 monooxygenases. Cascade has been simplified to show only a few of the metabolites that have beenshown to exert vasoactive actions. PLA2, phospholipase A2; HPETE, hydroperoxyeicosatetraenoic acid; EETS,epoxyeicosatrienoic acids.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S233

in extracellular volume, or during inflammatory re-sponses. The list of such vasoactive systems is poten-tially endless and includes the kallikrein-kinin system,purinergic agents such as adenosine and ATP, andother peptide hormones including endothelin andatrial natriuretic peptide (1, 28). Time constraintsprevent detailed consideration of this large assortmentof vasoactive agents, and it is sufficient to list them andto point out the general effects of vasodilators andvasoconstrictors and their consequences without go-ing into too much detail.
NEURAL CONTROL OF RENAL CIRCULATION
It is important not to neglect the influence of renalnerves on the renal circulation (11). RBF is markedlyinfluenced by extrinsic stimuli such as stress, trauma,hemorrhage, pain, and exercise. These conditionselicit increases in sympathetic nervous activity to thekidney that directly increase renal vascular resistance.Strong activation of the renal sympathetic nervesresults in marked renal vasoconstriction mediated bya-adrenoreceptors, leading to decreases in both RBFand GFR, increases in renin release, and increases inproximal tubular sodium and water reabsorption.Increases in renal sympathetic nerve activity can be apart of an overall sympathetic response or may bemore selective. Decreases in renal nerve activity canbe elicited reflexively through cardiopulmonary recep-tors and renorenal reflexes.
As previously mentioned, low-level renal nerve stimu-lation may elicit increases in renin release mediated bya direct action on juxtaglomerular apparatus cells viab-adrenergic receptor activation along with increasesin tubular sodium reabsorption even in the absence ofperceptible renal vasoconstriction. Moderate levels ofrenal nerve stimulation elicit parallel increases inafferent and efferent arteriolar resistance, leading toslightly greater decreases in RBF than in GFR. Withhigher stimulation frequency, a powerful preglomeru-lar vasoconstrictor response predominates and Kf isdecreased, causing major decreases in GFR. Theincrease in renal vascular resistance induced by a-adre-noceptors also represents a pathway for a-adrenocep-tor influence over renin secretion through the barocep-tor mechanism. The influence of neural activity on themedullary circulation may also be of importance,because outer medullary descending vasa recta re-ceive sympathetic innervation. It should be empha-
sized, however, that the tonic influence of the sympa-thetic nervous system on renal hemodynamics underunstressed conditions is thought to be relatively low.
In addition to control by sympathetic nerves, the renalcirculation is subject to influences by the adrenalmedulla, which releases epinephrine systemically inresponse to many stress conditions. Smooth muscle-containing vessels of all sizes, from the main renalarteries to afferent and efferent arterioles, respond toexogenous norepinephrine and epinephrine. Afferentarterioles appear to be more sensitive than efferentarterioles to the vasoconstrictive effect of norepineph-rine. GFR is maintained at near-normal levels duringinfusion of relatively small doses of catecholamines;however, larger doses of norepinephrine are capableof inducing marked renal vasoconstriction, leading tomajor decreases in GFR.
In summary, a serious consideration of the control ofrenal hemodynamics is a critical aspect of teachingrenal physiology and should not be neglected orshifted over to the cardiovascular segment. The main-tenance of optimum renal excretory function dependscritically on the contribution of many different sys-tems that interact to establish and maintain an appro-priate intrarenal hemodynamic environment. Becauseof the growing complexity of the area, it is importantto focus on the most critical issues needed to providea solid foundation requisite for further understandingof renal physiology, pharmacology, and pathophysiol-ogy.
The author thanks Agnes C. Buffone for assistance in preparing thismanuscript and its figures.
Address for reprint requests: L. G. Navar, Dept. of Physiology,Tulane Univ. School of Medicine, 1430 Tulane Ave., New Orleans,LA 70112.
References
1. Arendshorst, W. J., and L. G. Navar. Renal circulation andglomerular hemodynamics. In: Diseases of the Kidney, editedby R. W. Schrier and C. W. Gottschalk. Boston, MA: Little,Brown, 1997, p. 59–106.
2. Bachmann, S., H. M. Bosse, and P. Mundel. Topography ofnitric oxide synthesis by localizing constitutive NO synthases inmammalian kidney. Am. J. Physiol. 268 (Renal Fluid ElectrolytePhysiol. 37): F885–F898, 1995.
3. Baylis, C., J. Harvey, and K. Engels. Acute nitric oxideblockade amplifies the renal vasoconstrictor actions of angioten-sin II. J. Am. Soc. Nephrol. 5: 211–214, 1994.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S234

4. Blantz, R. C., K. S. Konnen, and B. J. Tucker. Angiotensin IIeffects upon the glomerular microcirculation and ultrafiltrationcoefficient of the rat. J. Clin. Invest. 57: 419–426, 1976.
5. Braam, B., and H. A. Koomans. Nitric oxide antagonizes theactions of angiotensin II to enhance tubuloglomerular feedbackresponsiveness. Kidney Int. 48: 1406–1411, 1995.
6. Braam, B., K. D. Mitchell, H. A. Koomans, and L. G. Navar.Relevance of the tubuloglomerular feedback mechanism inpathophysiology. J. Am. Soc. Nephrol. 4: 1257–1274, 1993.
7. Briggs, J. P., and J. Schnermann. Macula densa control ofrenin secretion and glomerular vascular tone: evidence forcommon cellular mechanisms. Renal Physiol. 9: 193–203,1986.
8. Briggs, J. P., and J. Schnermann. Control of renin release andglomerular vascular tone by the juxtaglomerular apparatus. In:Hypertension: Pathophysiology, Diagnosis, and Manage-ment, edited by J. H. Laragh and B. M. Brenner. New York:Raven, 1995, p. 1359–1385.
9. Carmines, P. K., and L. G. Navar. Disparate effects of Cachannel blockade on afferent and efferent arteriolar responsesto ANG II. Am. J. Physiol. 256 (Renal Fluid Electrolyte Physiol.25): F1015–F1020, 1989.
10. Carmines, P. K., M. D. Perry, J. B. Hazelrig, and L. G.Navar. Effects of preglomerular and postglomerular vascularresistance alterations on filtration fraction. Kidney Int. 31,Suppl. 20: S-229–S-232, 1987.
11. DiBona, G. F., and U. C. Kopp. Neural control of renalfunction. Physiol. Rev. 77: 75–197, 1997.
12. Forstermann, U., J.-P. Boissel, and H. Kleinert. Expres-sional control of the ‘‘constitutive’’ isoforms of nitric oxidesynthase (NOS I and NOS III). FASEB J. 12: 773–790, 1998.
13. Ichihara, A., J. D. Imig, E. W. Inscho, and L. G. Navar.Interactive nitric oxide-angiotensin II influences on renal micro-circulation in angiotensin II-induced hypertension. Hyperten-sion 31: 1255–1260, 1998.
14. Ichihara, A., E. W. Inscho, J. D. Imig, and L. G. Navar.Neuronal nitric oxide synthase modulates rat renal microvascu-lar function. Am. J. Physiol. 274 (Renal Physiol. 43): F516–F524, 1998.
15. Imig, J. D., and L. G. Navar. Afferent arteriolar response toarachidonic acid: involvement of metabolic pathways. Am. J.Physiol. 271 (Renal Fluid Electrolyte Physiol. 40): F87–F93,1996.
16. Kone, B. C. Nitric oxide in renal health and disease. Am. J.Kidney Dis. 30: 311–333, 1997.
17. Maddox, D. A., W. M. Deen, and B. M. Brenner. Glomerularfiltration. In: Handbook of Physiology. Renal Physiology.Bethesda, MD: Am. Physiol. Soc., 1992, sect. 8, vol. I, chapt. 13,p. 545–638.
18. Majid, D. S. A., and L. G. Navar. Nitric oxide in the mediationof pressure natriuresis. Clin. Exp. Pharmacol. Physiol. 24:595–599, 1997.
19. Majid, D. S. A., A. Williams, P. J. Kadowitz, and L. G. Navar.Renal responses to intra-arterial administration of nitric oxidedonor in dogs. Hypertension 22: 535–541, 1993.
20. Mitchell, K. D., and L. G. Navar. The renin-angiotensin-aldosterone system in volume control. In: Bailliere’s ClinicalEndocrinology and Metabolism, edited by P. H. Baylis. Lon-don: Bailliere Tindall, 1989, p. 393–430.
21. Mitchell, K. D., and L. G. Navar. Tubuloglomerular feedbackresponses during peritubular infusions of calcium channelblockers. Am. J. Physiol. 258 (Renal Fluid Electrolyte Physiol.27): F537–F544, 1990.
22. Navar, L. G. The kidney in blood pressure regulation anddevelopment of hypertension. Med. Clin. North Am. 81:1165–1198, 1997.
23. Navar, L. G. Integrating multiple paracrine regulators of renalmicrovascular dynamics. Am. J. Physiol. 274 (Renal Physiol.43): F433–F444, 1998.
24. Navar, L. G., P. D. Bell, and A. P. Evan. The regulation ofglomerular filtration rate in mammalian kidneys. In: Physiologyof Membrane Disorders, edited by T. E. Andreoli, J. Hoffman,D. Fanestil, and S. G. Shultz. New York: Plenum Medical Book,1986, p. 637–667.
25. Navar, L. G., P. K. Carmines, and K. D. Mitchell. Renalcirculation. In: Textbook of Nephrology, edited by S. G. Massryand R. J. Glassock. Baltimore, MD: Williams and Wilkins, 1994,p. 41–53.
26. Navar, L. G., A. P. Evan, and L. Rosivall. Microcirculation ofthe kidneys. In: The Physiology and Pharmacology of theMicrocirculation, edited by N. Mortillaro. New York: Aca-demic, 1983, p. 397–488.
27. Navar, L. G., J. D. Imig, L. Zou, and C.-T. Wang. Intrarenalproduction of angiotensin II. Semin. Nephrol. 17: 412–422,1997.
28. Navar, L. G., E. W. Inscho, D. S. A. Majid, J. D. Imig, L. M.Harrison-Bernard, and K. D. Mitchell. Paracrine regulationof the renal microcirculation. Physiol. Rev. 76: 425–536, 1996.
29. Ohishi, K., P. K. Carmines, E. W. Inscho, and L. G. Navar.EDRF-angiotensin II interactions in rat juxtamedullary afferentand efferent arterioles. Am. J. Physiol. 263 (Renal FluidElectrolyte Physiol. 32): F900–F906, 1992.
30. Reid, I. A. The renin-angiotensin system: physiology, patho-physiology, and pharmacology. Am. J. Physiol. 275 (Adv.Physiol. Educ. 20): S236–S245, 1998.
31. Romero, J. C., V. Lahera, M. G. Salom, and M. L. Biondi.Role of the endothelium-dependent relaxing factor nitric oxideon renal function. J. Am. Soc. Nephrol. 2: 1371–1387, 1992.
32. Thorup, C., and A. E. G. Persson. Inhibition of locallyproduced nitric oxide resets tubuloglomerular feedback mech-anism. Am. J. Physiol. 267 (Renal Fluid Electrolyte Physiol.36): F606–F611, 1994.
33. Tojo, A., S. S. Gross, L. Zhang, C. C. Tisher, H. H. H. W.Schmidt, C. S. Wilcox, and K. M. Madsen. Immunocytochemi-cal localization of distinct isoforms of nitric oxide synthase inthe juxtaglomerular apparatus of normal rat kidney. J. Am. Soc.Nephrol. 4: 1438–1447, 1994.
34. Wilcox, C. S., W. J. Welch, F. Murad, S. S. Gross, G. Taylor,R. Levi, and H. H. H. W. Schmidt. Nitric oxide synthase inmacula densa regulates glomerular capillary pressure. Proc.Natl. Acad. Sci. USA 89: 11993–11997, 1992.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 20 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1998
S235