Renal Failure Wendy DeMartino, MD PGY-2 Objectives Anatomy Function Acute Renal Failure (ARF) Causes...
38
Renal Failure Wendy DeMartino, MD PGY-2
-
Upload
emerald-bruce -
Category
Documents
-
view
232 -
download
8
Transcript of Renal Failure Wendy DeMartino, MD PGY-2 Objectives Anatomy Function Acute Renal Failure (ARF) Causes...

Renal Failure
Wendy DeMartino, MDPGY-2

Objectives Anatomy Function Acute Renal Failure (ARF)
Causes Symptoms Management
Chronic Renal Failure (CRF) Causes Symptoms
Dialysis

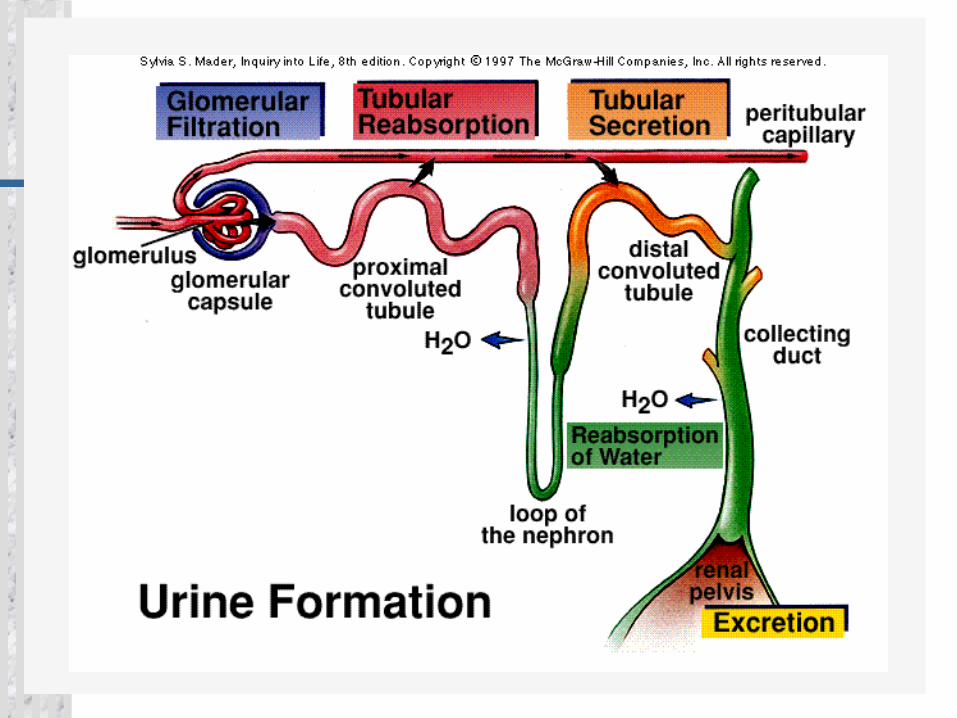
Anatomy 2 Kidneys 2 Ureters Bladder Urethra


Kidney Function Detoxify blood Increase calcium absorption
calcitriol Stimulate RBC production
erythropoietin Regulate blood pressure and
electrolyte balance renin

Classifications Acute versus chronic Pre-renal, renal, post-renal Anuric, oliguric, polyuric
Acute Versus Chronic Acute
sudden onset rapid reduction in urine output Usually reversible Tubular cell death and regeneration
Chronic Progressive Not reversible Nephron loss
75% of function can be lost before its noticeable
Acute Renal Failure
Pre-renal = 55%
Renal parenchymal (intrinsic)= 40%
Post-renal = 5-15%
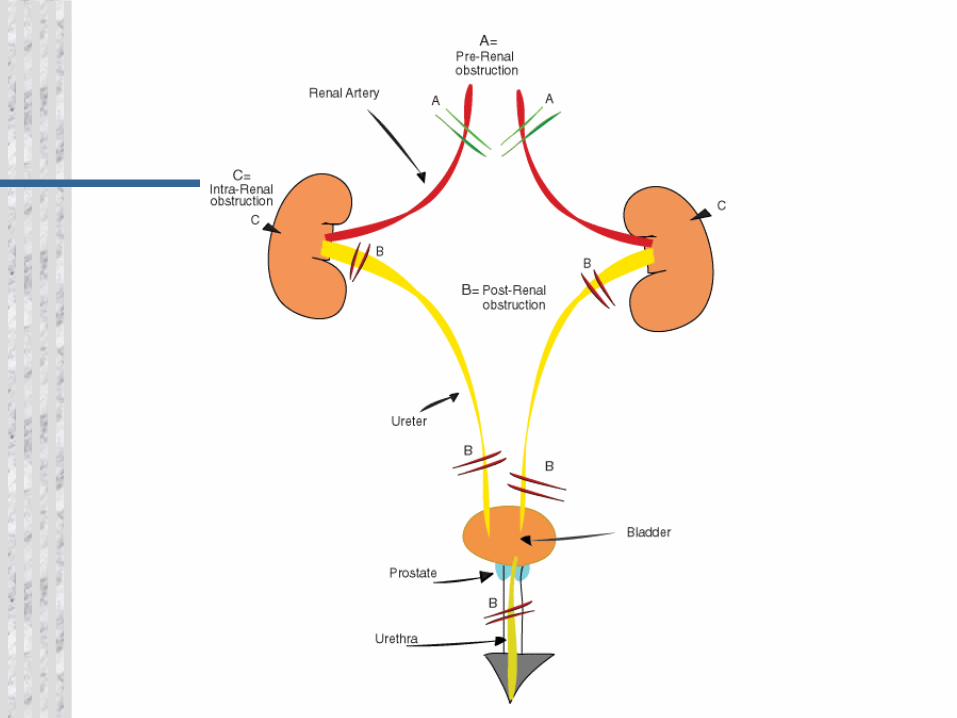

Causes of ARF Pre-renal =
vomiting, diarrhea, poor fluid intake, fever, use of diuretics, and heart failure
cardiac failure, liver dysfunction, or septic shock Intrinsic
Interstitial nephritis, acute glomerulonephritis, tubular necrosis, ischemia, toxins
Post-renal = prostatic hypertrophy, cancer of the prostate or cervix, or
retroperitoneal disorders neurogenic bladder bilateral renal calculi, papillary necrosis, coagulated blood,
bladder carcinoma, and fungus

Symptoms of ARF Decrease urine output (70%) Edema, esp. lower extremity Mental changes Heart failure Nausea, vomiting Pruritus Anemia Tachypenic Cool, pale, moist skin

Diagnosis of Renal Failure
Acute Renal Failure Management Make/think about the diagnosis Treat life threatening conditions Identify the cause if possible
Hypovolemia Toxic agents (drugs, myoglobin) Obstruction
Treat reversible elements Hydrate Remove drug Relieve obstruction
ARF: Life Threatening Conditions Hyperkalemia Volume overload Vascular access

Hyperkalemia Symptoms Weakness Lethargy Muscle cramps Paresthesias Hypoactive DTRs Dysrhythmias

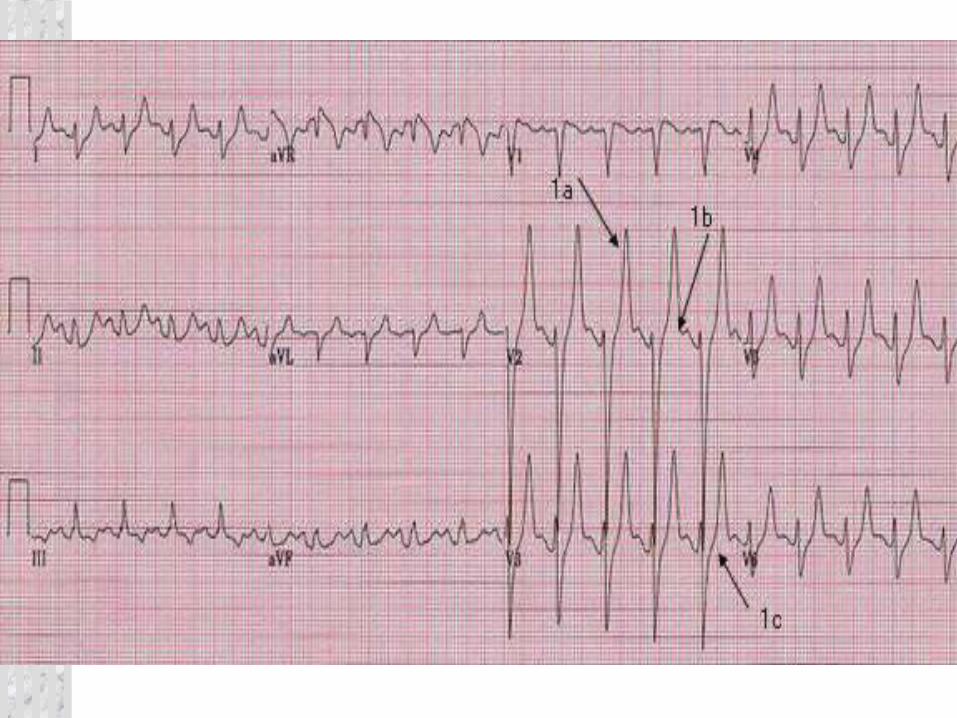
Hyperkalemia & EKG K > 5.5 -6 Tall, peaked T’s Wide QRS Prolong PR Diminished P Prolonged QT QRS-T merge –
sine wave



Hyperkalemia Treatment Calcium gluconate (carbonate) Sodium Bicarbonate Insulin/glucose Kayexalate Lasix Albuterol Hemodialysis
Chronic Renal Failure 150–200 cases per million people =
new cases each year Chronic renal failure and ESRD affect
more than 2 out of 1,000 people in the U.S
Mortality = 20%
Chronic Renal Failure Causes Diabetic Nephropathy Hypertension Glomerulonephritis HIV nephropathy Reflux nephropathy in children Polycystic kidney disease Kidney infections & obstructions

CRF Symptoms Malaise Weakness Fatigue Neuropathy CHF Anorexia Nausea Vomiting
Seizure Constipation Peptic ulceration Diverticulosis Anemia Pruritus Jaundice Abnormal
hemostasis

Acute Problems in CRF Relating to underlying disease Relating to ESRD Dialysis related problems

Problems Related to ESRD Metabolic – K/Ca Volume overload Anemia, platelet disorder, GI bleed HTN, pericarditis Peripheral neuropathy, dialysis
dementia Abnormal immune function
Dialysis ½ of patients with CRF eventually
require dialysis Diffuse harmful waste out of body Control BP Keep safe level of chemicals in body 2 types
Hemodialysis Peritoneal dialysis
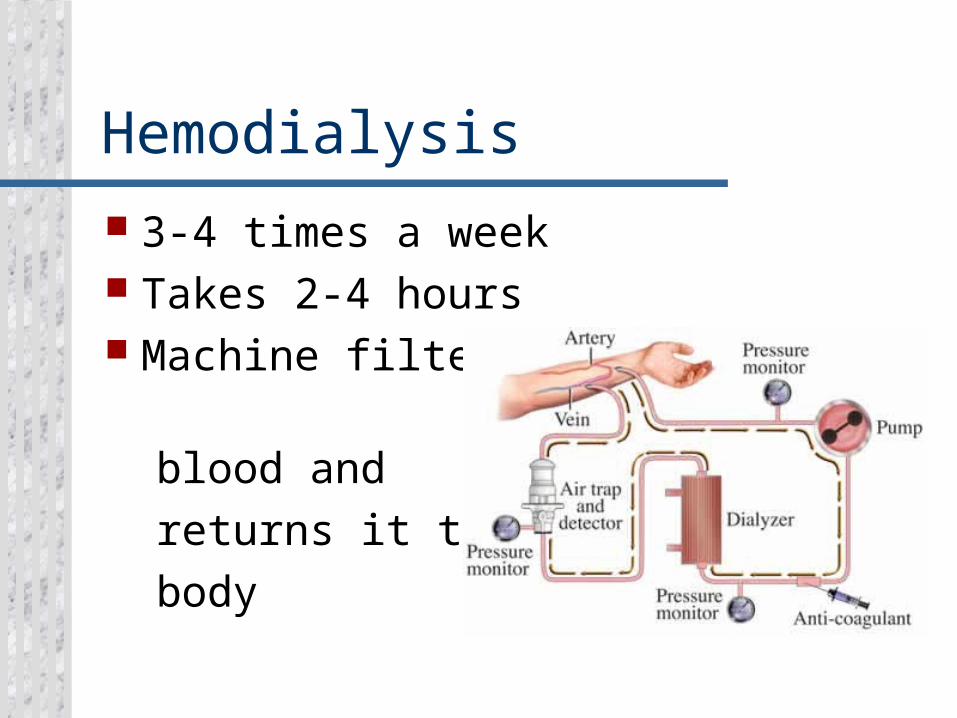
Hemodialysis 3-4 times a week Takes 2-4 hours Machine filters blood and returns it to body
Types of Access Temporary site AV fistula
Surgeon constructs by combining an artery and a vein
3 to 6 months to mature AV graft
Man-made tube inserted by a surgeon to connect artery and vein
2 to 6 weeks to mature
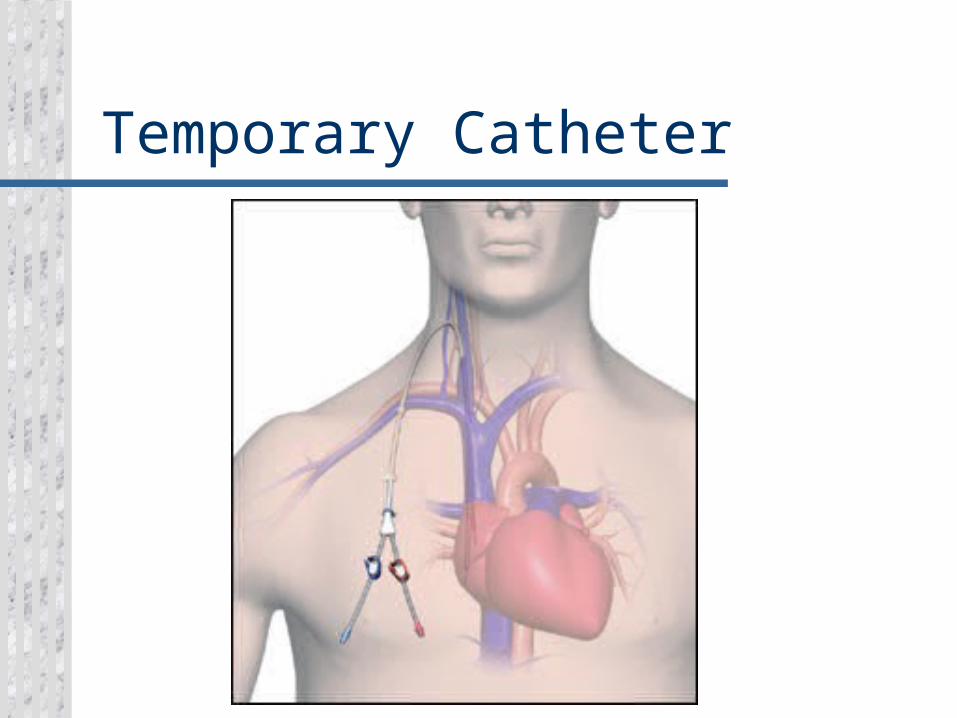
Temporary Catheter

AV Fistula & Graft

What This Means For You No BP on same arm as fistula Protect arm from injury Control obvious hemorrhage
Bleeding will be arterial Maintain direct pressure
No IV on same arm as fistula A thrill will be felt – this is normal

Access Problems AV graft thrombosis AV fistula or graft bleeding AV graft infection Steal Phenomenon
Early post-op Ischemic distally Apply small amount of pressure to
reverse symptoms

Peritoneal Dialysis Abdominal lining filters blood 3 types
Continuous ambulatory Continuous cyclical Intermittent

EMS Considerations Make sure the dressing remains
intact Do not push or pull on the catheter Do not disconnect any of the
catheters Always transport the patient and
bags/catheters as one piece Never inject anything into catheter

Dialysis Related Problems Lightheaded –give fluids Hypotension Dysrhythmias Disequilibration Syndrome
At end of early sessions Confusion, tremor, seizure Due to decrease concentration of blood
versus brain leading to cerebral edema