
RENAL FAILURE M. Tatár Dept of Pathophysiology. Definition Kidneys lose their ability to mantaine...
32
RENAL FAILURE M. Tatár Dept of Pathophysiology
-
Upload
martin-cunningham -
Category
Documents
-
view
221 -
download
5
Transcript of RENAL FAILURE M. Tatár Dept of Pathophysiology. Definition Kidneys lose their ability to mantaine...

RENAL FAILURE
M. Tatár
Dept of Pathophysiology

Definition
• Kidneys lose their ability to mantaine normal volume and composition of the body fluids (homeostasis) under conditions of normal dietary intake (~ 0.5 g/kg/day of protein)
• Renal insuficiency – decline in renal functions to about 25% of normal; GFR of 25-30 ml/min; serum creatinin and urea will be mildly elevated
• Renal failure – significant loss of renal functions; less than 10% of renal function remains = end-stage renal failure
• Uremia – elevated blood urea and creatinin levels accompanied by fatigue, anorexia, mausea, vomiting, pruritus, and neurologic changes (clinical syndrome)
• Azotemia – increased serum urea levels and frequently increased creatinine levels

Classification
• Acute renal failure– rapidly progressive– may be reversible– cellular dysfunction
• Chronic renal failure– progressing over a period of months and years– irreversible– reduction of functioning nephrons

Acute Renal Failure (ARF)
• Prerenal– renal vasoconstriction, renal blood flow GFR– tubular cell function is not disturbed ( reabsorptive
capacity is mantained– overall kidney function will improve with normalisation of
intravascular fluid volume• Intrarenal (acute tubular insufficiency)
– primary damage of tubular epithelial cells– tubular function is disturbed: urinary sodium
concentration is increased above 40 mmol/l– renal function remains depressed after correction of
circulatory disorders or termination of the insult– recovery only after tubule cells regeneration (2-3 weeks)
• Postrenal– obstruction of urine outflow affecting 75% of renal
parenchyma

Characteristics of ARF
• Reduction in glomerular and tubular function– low GFR– high fractional Na excretion– reduced tubular secretory activity (metabolic acidosis)– diminished concentrating ability
• Cellular and molecular basis– intracellular accumulation of Na and Cl, water influx, cell
swelling– membrane depolarisation, reduction of transport systems– loss of extracellular fluid, Er aggregation, vascular
congestion and stasis impairing perfusion oxygen depletion
– excessive accumulation of Ca2+ cell damage– cell acidosis inhibits activation of enzymes– lipid peroxidation – oxidative stress

Heterogeneity of cellular insufficiency along the nephron (1)
Main activities of the tubule cells is the reabsorption of filtered Na (driving force for the reabsorption of water and for the coupled transport of organic solutes); Na+,K+,ATP-ase
• Intrarenal heterogenenity of cellular metabolismeffect of ischemia and nephrotoxins on specific cells in the
kidneyis related to specific biochemical properties– enzymes of the glycolytic pathway are abundant
throughout the distal tubule more resistant to hypoxia– capacity to transport substances: inward transport of
nephrotoxic substances by normally existing transport systems increase their intracellular concentrations to levels at which they become cytotoxic

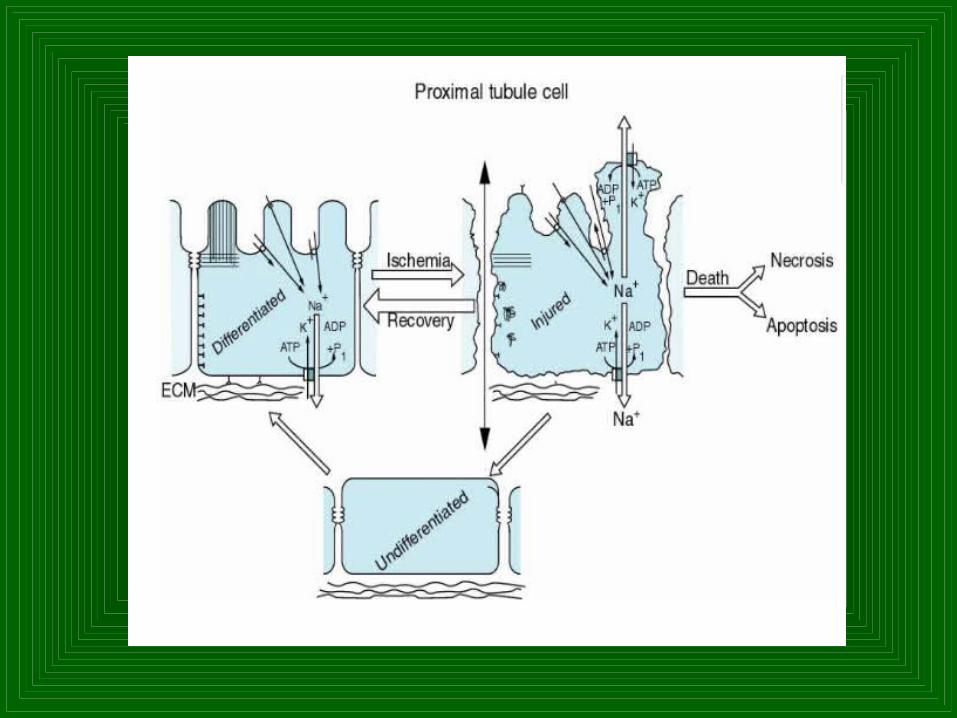
Heterogeneity of cellular insufficiency along the nephron (2)
• Proximal tubule– is most pronounced to ischemic cell injury reduced
reabsorption of Na+, Cl-, HCO3- and glucose
• Thick ascending limb of the loop of Henle– reduced concentrating capacity
• Distal convolution, collecting duct– structural derangements resulting from ischemic
episodes are more discrete

Heterogeneity of cellular insufficiency along the nephron (3)

Vascular components of acute renal failure (1)
• Circulatory dysfunction (prerenal failure) GFR reduction in renal excretory functions (no
cell damage)– reduction of renal functions is fully reversed when
circulation is normalised
• Persistent decrease in renal excretory function following normalisation of circulation– Evidence of kidney damage during the period of
circulatory dysfunction – „prerenal“ renal failure is replaced by an „intrarenal“ one
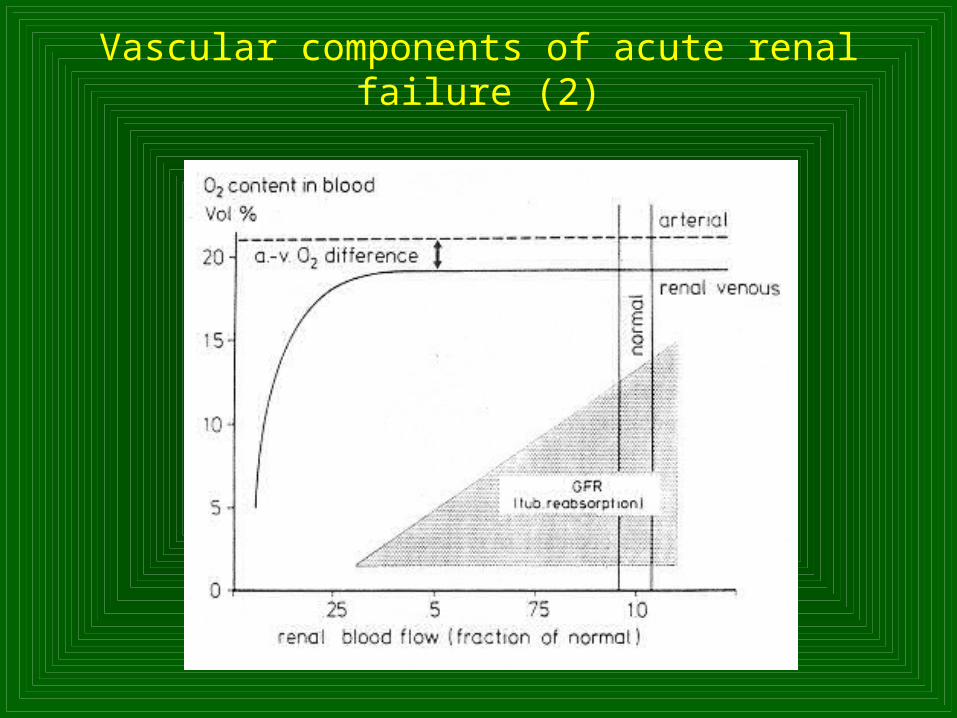
Vascular components of acute renal failure (2)

Acute clinical renal failure
• Syndrome– caused by an abrupt reduction in GFR (frequently to
20% or less) progressive rise in blood urea nitrogen and creatinine over hours, days, or weeks
• Serious condition with substantial morbidity and a high mortality– even severe ARF is potentially reversible in most
cases if correctly managed
• Oliguria– May be the first manifestation of ARF (daily urine
output of < 400ml/24 hours– but often urine volume is normal (nonoliguric ARF)

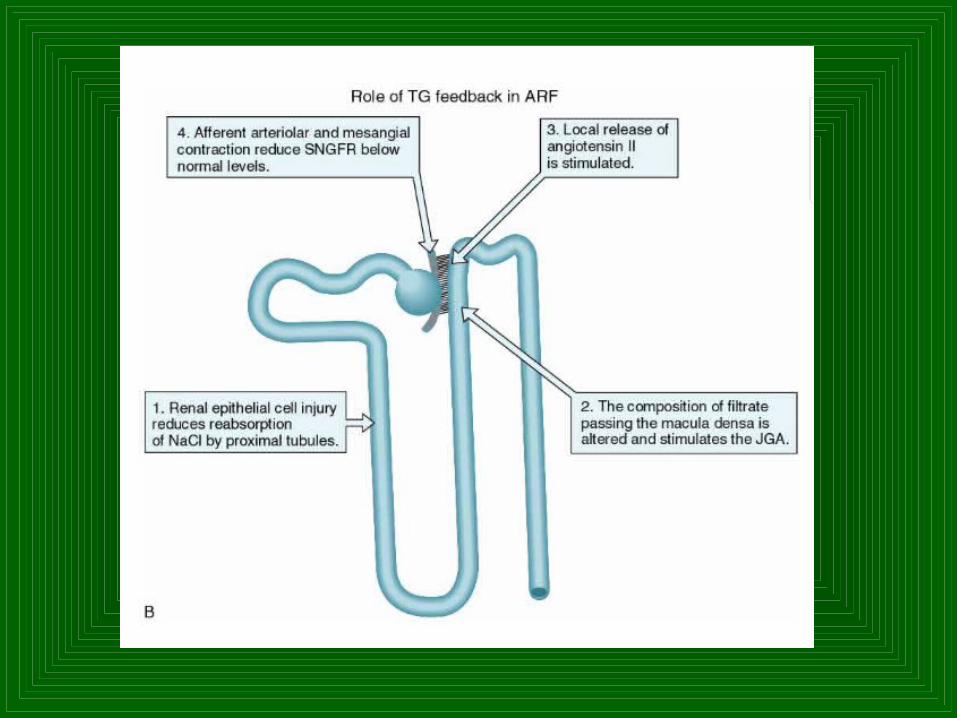
ARF due to prerenal failure
• Impaired glomerular perfusion– in the absence of any structural kidney damage– GFR is promptly restored to normal if the cause of the
renal hypoperfusion can be corrected– can be precipitated by: volume depletion, cardiac failure,
systemic vasodilatation
• Activation of the sympathetic and R-A systems and release of vasopresin cause intrarenal vasoconstriction
• Renal adaptive responses preserve GFR in the early stages of prerenal failure– local generation of vasodilator prostaglandins– angiotensine preferentially constricts the efferent arteriol
• Urine– is concentrated, sodium concentration is below 40 mmol/l

ARF due to acute tubular necrosis
• Causes of ATN based on the mechanism of injury– ischemic and toxic ATN
• Ischemic ATN– more severe and prolonged reduction in renal blood flow– restoration of renal perfusion will not promptly reverse renal
dysfunction– Common clinical situations:
postoperative patients, especially with cardiac, aortic, and gastrointestinal surgery
complication following burns: volume depletion, myoglobinuria, antibiotic toxicity
fluid loses, severe cardiac failure, sepsis
• ATN due to toxins– Aminoglycoside antibiotics and radiocontrast media:
damage of mitochondrial function, membrane structire, lysosomal integrity



Clinical course of ATN
• Initiating phase– patients are subject to factors causing ATN but have not
yet developed frank parenchymal injury– may last hours or days– with development of tubular necrosis, GFR falls abruptly to
very low levels (typically below 5-10 ml/min)
• Maitenance phase– GFR remains markedly depressed– may last a few days or as long as several weeks– characterized by progressive accumulation of nitrogenous
wastes and by development of the manifestation of uremia
• „Recovery phase“– cellular repair and regeneration ultimately leads to a
progressive rise in GFR

Chronic renal failure (CRF)
• The degree of the reduction in functional mass– rather than the underlying disease, was generally to
blame for the clinical manifestation of patients with CRF
• The degree of reduction in glomerular filtration rate – is good determinant or predictor of the clinical
manifestations
• Rate of progression of CRF and possible mechanisms– role of proteinuria: increased protein flux through
glomerular basement membrane cause mesangial cell injury and proliferation, increased production of mesangial matrix, and glomerular sclerosis
– glomerular capillary hyperperfusion and hypertension of the remaining nephrons: kidney may be protected from glomerular injury by the ACE inhibitors (reduce glomerular capillary hypertension)
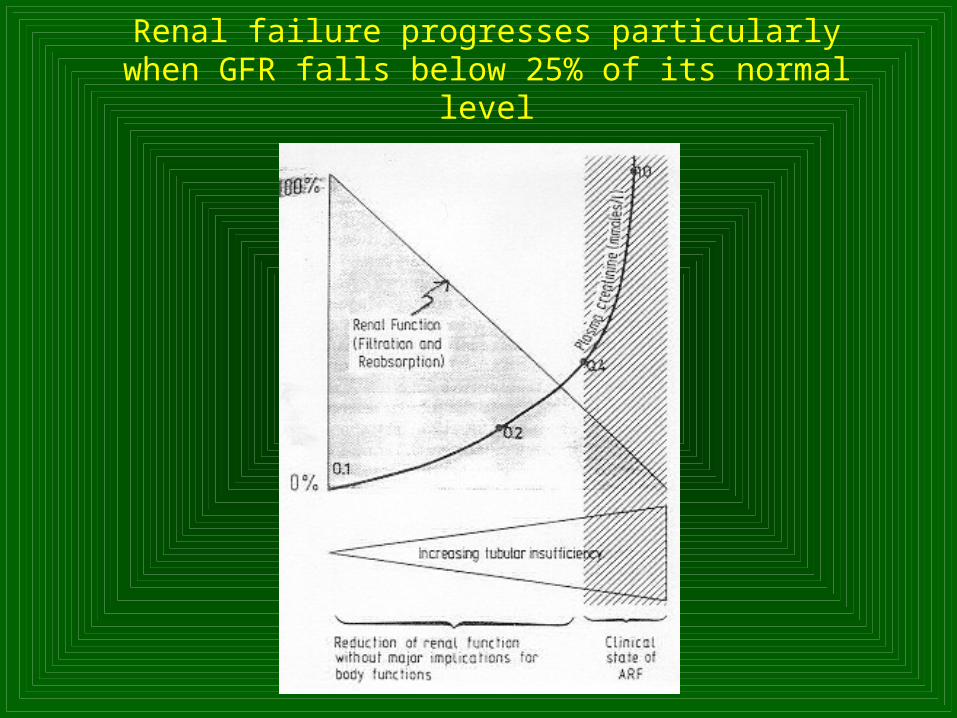
Renal failure progresses particularly when GFR falls below 25% of its normal level
Water handling in CRF
• Ability to excrete a concentrated urine becomes impaired as nephron number declines
• mechanisms: – remaining nephrons must increase their capacity to
excrete water– single-nephron GFR rises, but it cannot compensate
overall GFR falls– solute load to the distal nephron is increased volume
of water removed from the filtrate is less than normal– transfer of osmotically active solute to the medullary
interstitium is reduced decreased water reabsobtion– under normal circumstances (urine osmolality of 1200
mosm/kg) man can excrete 600 mmol of solute in 500 ml of water; in CRF (urine osmolality of 500 mosm/kg) excretion of 500 mmol require 1000 ml of water

Ability to excrete a concentrated urine

Sodium excretion in CRF
• Remain surprisingly controlled, despite the progressive nephron damage
• Sodium balance is maintained until GFR falls below 10% of the control value

Abnormalities of acid-base balance
• Formation of hydrogen ions– metabolism of sulfur-containing amino acids, nucleic acids,
and the incomplete oxidation of carbohydrates and fats
• Kidney final task – Excretion of the acid and regeneration of bicarbonates to
replenish the organism buffering capacity
• Metabolic acidosis appears when GFR falls to 20-30% of normala) initially is hyperchloremic MA with a normal anion gap
Defect in H+ excretion resulting in decresed bicarbonate reabsorption
Sodium is reabsorbed with chloride as an accompanying anion
b) As CRF progresses and GFR falls below 10-20 ml/min it becomes a high anion gap MA
retention of anions increases the anion gap
diminished ammonium (NH4+) excretion

Proximal tubuleProximal tubule

Distal nephronDistal nephron

Anion gapAnion gap
[ Na+ ] - ( [Cl-] + [ HCO3-] ) = 10 - 12
mmol.l-1
140 - ( 104 + 24 ) = 12 mmol.l140 - ( 104 + 24 ) = 12 mmol.l-1-1

Nervous system
• Uremic encephalopathy– electrolytes derangements, vitamin deficiency, drug
intoxication, subdural hematoma – depressed cerebral oxygen consumption: brain uptake
of glutamine, brain uses less ATP, calcium overload of mitochondria
– symptomatology: fatigability, daytime drowsiness and insomnia, variable disorders of speech, confusion, hallucinations, delirium, and coma
• Severe polyneuropathy– predominantly afflicts the autonomic system: postural
hypotension and impotence
Gastrointestinal disturbances• Nausea, vomiting, hiccups, and diarrhea
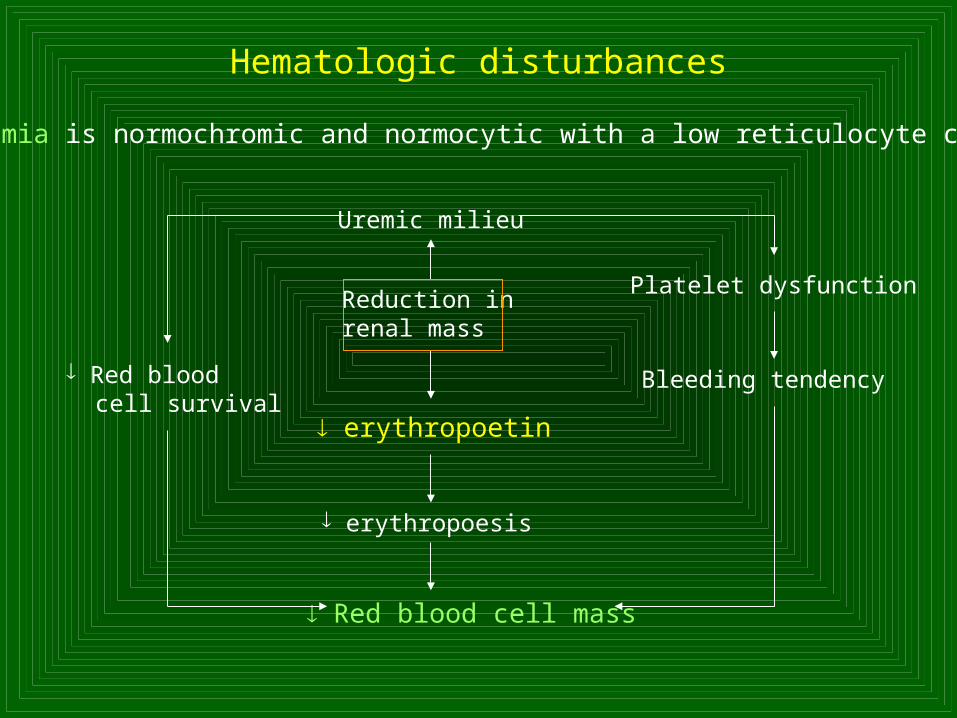
Hematologic disturbances
Anemia is normochromic and normocytic with a low reticulocyte count
Uremic milieu
Reduction inrenal mass
erythropoetin
erythropoesis
Red blood cell mass
Red blood cell survival
Platelet dysfunction
Bleeding tendency

Renal osteodystrophy
Alterations in plasma calcium and phosphate concentration altered parathyroid gland function
– classic theory: secondary hyperparathyroidism in renal failure, phosphate retention causes a small decrease in plasma calcium stimulates PTH secretion osteitis fibrosa cystica
– other factors:
1. cell from parathyroid tissue of CRF patient with secondary hyperparathyroidism have shown that higher Ca concentrations are required to suppress PTH secretion
2. calcitriol deficiency: metabolic inhibitors of 1--hydroxylase in kidney
- decreased intestinal calcium absorption- calcitriol may directly inhibit PTH secretion

Cardiovascular manifestations

Pulmonary manifestations
• „Uremic lung“– mechanisms: metabolic acidosis, volum overload, left
ventricular dysfunction– degenerative changes of the capillary endothelium,
focal accumulation of interstitial edema fluid, altered alveolocapillary basement membrane
Lipid metabolism disturbances
• Incresed risk of atherosclerosis– hypertriglyceridemia, elevated VLVD (reduced activity
of the major lipolytic enzymes)– decrease in HDL cholesterol














![Department for Education · different types of scientific enquiries that help them to answer scientific questions ... of the combined double ... kidneys in homeostasis and excretion]](https://static.fdocuments.in/doc/165x107/5b83d2847f8b9a7d3a8d9b1c/department-for-education-different-types-of-scientific-enquiries-that-help-them.jpg)