Renal failure and hyponatremia in patients with cirrhosis and skin and soft tissue infection. A...
7
Renal failure and hyponatremia in patients with cirrhosis and skin and soft tissue infection. A retrospective study Gustavo Pereira 1,2,3,4 , Mónica Guevara 1,2,3,4 , Claudia Fagundes 1,2,3,4 , Elsa Solá 1,2,3,4 , Ezequiel Rodríguez 1,2,3,4 , Javier Fernández 1,2,3 , Marco Pavesi 2,3 , Vicente Arroyo 1,2,3 , Pere Ginès 1,2,3,4,⇑ 1 Liver Unit, Hospital Clínic, University of Barcelona, Barcelona, Catalunya, Spain; 2 Institut d’Investigacions Biomèdiques August-Pi-Sunyer (IDIBAPS), Spain; 3 Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBEREHED), Spain; 4 Instituto Reina Sofia de Investigación Nefrologia (IRSIN), Spain Background & Aims: Skin and soft tissue infection in cirrhosis is considered a non-severe infection, but specific information is lacking. This study aimed at assessing the characteristics, occur- rence of renal failure, and outcome of cirrhotic patients with skin and soft tissue infection. Methods: Ninety-two patients with cirrhosis and skin and soft tissue infection admitted to hospital within a 6-year period were retrospectively analyzed. A control group matched by severity of liver disease, admitted for reasons other than infection, was also studied. Results: Resolution of the infection was achieved in 96% of patients. Twenty (21.7%) patients with skin and soft tissue infec- tion developed renal failure, compared to only five patients (5.4%) of the control group (p= 0.001). Renal failure was persistent despite infection resolution in 10 of the 20 patients vs. none of the control group. Renal failure was associated with poor progno- sis. Hyponatremia developed in 40% and 25% of the infection and control group, respectively (p= 0.028). Within a 3-month follow- up period, 25 patients (23%) with skin and soft tissue infection died or were transplanted compared to only four patients (4%) of the control group (p<0.001). Factors independently associated with mortality in the infection group were: site of acquisition of the infection and MELD–sodium score at diagnosis. Conclusions: Skin and soft tissue infection is a severe complication of cirrhosis with high frequency of renal failure and hyponatremia that may persist despite resolution of the infection. MELD–sodium score is useful to assess 3-month mortality in these patients. Ó 2012 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Introduction Bacterial infections are a very common cause of morbidity and mortality in patients with cirrhosis [1,2]. Infections represent a triggering factor for development of complications of cirrhosis, mainly renal failure, hyponatremia, gastrointestinal bleeding, hepatic encephalopathy, and eventually multiorgan failure [3]. Several lines of evidence indicate that bacterial infections stimu- late a cascade of inflammatory events leading to increased syn- thesis of proinflammatory cytokines and vasoactive substances that may cause organ failure and eventually death in some patients [4,5]. Particularly severe is the development of renal fail- ure associated with bacterial infections [6]. The increased levels of vasodilator factors (i.e. nitric oxide, carbon monoxide, and vasodilator cytokines) related to the infection may lead to an impairment of the circulatory dysfunction characteristic of cir- rhosis and cause a further arterial vasodilation and increased activation of vasoconstrictor systems that may lead to hyponatre- mia and hepatorenal syndrome [7–10]. These pathogenic events have been studied extensively in spontaneous bacterial peritoni- tis, which is a paradigmatic infection of patients with cirrhosis [11,12], but may occur in spontaneous sepsis, urinary tract infec- tions, and pneumonia as well [13,14]. Patients with cirrhosis may develop skin and soft tissue infec- tion (SSTI), particularly in the legs due to the frequent presence of edema. Although not infrequent in clinical practice, this type of infection has received little attention. Besides sporadic reports [15,16], there are no specific studies analyzing this infection in cirrhosis and its possible relationship with renal dysfunction. The recent clinical observation in our Unit, of several patients with SSTI who developed severe renal failure in close chronolog- ical relationship with the infection, prompted us to evaluate this type of infection in a large series of patients. Patients and methods Study population Study group: patients with cirrhosis and skin and soft tissue infection We retrospectively identified all consecutive patients with cirrhosis and SSTI (n = 92) hospitalized at the Liver Unit of the Hospital Clínic of Barcelona (Catalo- nia, Spain) between 2004 and 2009. Patients with advanced hepatocellular carci- noma (outside the Milan Criteria [17]) and those with HIV infection were not included. SSTI was diagnosed on clinical grounds by the presence of pain and inflammatory signs (red color of the skin together with increased temperature with or without presence of fluid or formation of bullae). Skin cultures were obtained in some patients but positive cultures were not required for the diagno- sis. Blood cultures were taken in patients showing signs of systemic infection, Journal of Hepatology 2012 vol. 56 j 1040–1046 Keywords: Hepatorenal syndrome; Hepatic encephalopathy; Acute-on-chronic liver failure. Received 21 July 2011; received in revised form 7 November 2011; accepted 26 November 2011; available online 13 January 2012 ⇑ Corresponding author. Address: Liver Unit, Hospital Clínic, Villarroel, 170, 08036 Barcelona, Spain. Tel.: +34 932271713; fax: +34 93 4515522. E-mail address: [email protected] (P. Ginès). Research Article
-
Upload
gustavo-pereira -
Category
Documents
-
view
213 -
download
0
Transcript of Renal failure and hyponatremia in patients with cirrhosis and skin and soft tissue infection. A...

Research Article
Renal failure and hyponatremia in patients with cirrhosis andskin and soft tissue infection. A retrospective study
Gustavo Pereira1,2,3,4, Mónica Guevara1,2,3,4, Claudia Fagundes1,2,3,4, Elsa Solá1,2,3,4,Ezequiel Rodríguez1,2,3,4, Javier Fernández1,2,3, Marco Pavesi2,3, Vicente Arroyo1,2,3, Pere Ginès1,2,3,4,⇑
1Liver Unit, Hospital Clínic, University of Barcelona, Barcelona, Catalunya, Spain; 2Institut d’Investigacions Biomèdiques August-Pi-Sunyer(IDIBAPS), Spain; 3Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBEREHED), Spain; 4Instituto Reina
Sofia de Investigación Nefrologia (IRSIN), Spain
Background & Aims: Skin and soft tissue infection in cirrhosis is triggering factor for development of complications of cirrhosis,
considered a non-severe infection, but specific information islacking. This study aimed at assessing the characteristics, occur-rence of renal failure, and outcome of cirrhotic patients with skinand soft tissue infection.Methods: Ninety-two patients with cirrhosis and skin and softtissue infection admitted to hospital within a 6-year period wereretrospectively analyzed. A control group matched by severity ofliver disease, admitted for reasons other than infection, was alsostudied.Results: Resolution of the infection was achieved in 96% ofpatients. Twenty (21.7%) patients with skin and soft tissue infec-tion developed renal failure, compared to only five patients (5.4%)of the control group (p = 0.001). Renal failure was persistentdespite infection resolution in 10 of the 20 patients vs. none ofthe control group. Renal failure was associated with poor progno-sis. Hyponatremia developed in 40% and 25% of the infection andcontrol group, respectively (p = 0.028). Within a 3-month follow-up period, 25 patients (23%) with skin and soft tissue infectiondied or were transplanted compared to only four patients (4%)of the control group (p <0.001). Factors independently associatedwith mortality in the infection group were: site of acquisition ofthe infection and MELD–sodium score at diagnosis.Conclusions: Skin and soft tissue infection is a severe complicationof cirrhosis with high frequency of renal failure and hyponatremiathat may persist despite resolution of the infection. MELD–sodiumscore is useful to assess 3-month mortality in these patients.� 2012 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.Introduction
Bacterial infections are a very common cause of morbidity andmortality in patients with cirrhosis [1,2]. Infections represent a
Journal of Hepatology 20
Keywords: Hepatorenal syndrome; Hepatic encephalopathy; Acute-on-chronicliver failure.Received 21 July 2011; received in revised form 7 November 2011; accepted 26November 2011; available online 13 January 2012⇑ Corresponding author. Address: Liver Unit, Hospital Clínic, Villarroel, 170,08036 Barcelona, Spain. Tel.: +34 932271713; fax: +34 93 4515522.E-mail address: [email protected] (P. Ginès).
mainly renal failure, hyponatremia, gastrointestinal bleeding,hepatic encephalopathy, and eventually multiorgan failure [3].Several lines of evidence indicate that bacterial infections stimu-late a cascade of inflammatory events leading to increased syn-thesis of proinflammatory cytokines and vasoactive substancesthat may cause organ failure and eventually death in somepatients [4,5]. Particularly severe is the development of renal fail-ure associated with bacterial infections [6]. The increased levelsof vasodilator factors (i.e. nitric oxide, carbon monoxide, andvasodilator cytokines) related to the infection may lead to animpairment of the circulatory dysfunction characteristic of cir-rhosis and cause a further arterial vasodilation and increasedactivation of vasoconstrictor systems that may lead to hyponatre-mia and hepatorenal syndrome [7–10]. These pathogenic eventshave been studied extensively in spontaneous bacterial peritoni-tis, which is a paradigmatic infection of patients with cirrhosis[11,12], but may occur in spontaneous sepsis, urinary tract infec-tions, and pneumonia as well [13,14].
Patients with cirrhosis may develop skin and soft tissue infec-tion (SSTI), particularly in the legs due to the frequent presence ofedema. Although not infrequent in clinical practice, this type ofinfection has received little attention. Besides sporadic reports[15,16], there are no specific studies analyzing this infection incirrhosis and its possible relationship with renal dysfunction.The recent clinical observation in our Unit, of several patientswith SSTI who developed severe renal failure in close chronolog-ical relationship with the infection, prompted us to evaluate thistype of infection in a large series of patients.
Patients and methods
Study population
Study group: patients with cirrhosis and skin and soft tissue infectionWe retrospectively identified all consecutive patients with cirrhosis and SSTI(n = 92) hospitalized at the Liver Unit of the Hospital Clínic of Barcelona (Catalo-nia, Spain) between 2004 and 2009. Patients with advanced hepatocellular carci-noma (outside the Milan Criteria [17]) and those with HIV infection were notincluded. SSTI was diagnosed on clinical grounds by the presence of pain andinflammatory signs (red color of the skin together with increased temperaturewith or without presence of fluid or formation of bullae). Skin cultures wereobtained in some patients but positive cultures were not required for the diagno-sis. Blood cultures were taken in patients showing signs of systemic infection,
12 vol. 56 j 1040–1046

JOURNAL OF HEPATOLOGY
such as fever or high leukocyte count. Patients were treated with systemic anti-biotic therapy during the first days followed by oral antibiotics. Initial antibiotictherapy included amoxicillin–clavulanic acid (51 patients), third-generationcephalosporins (17 patients), cloxacillin alone or in combination with third-gen-eration cephalosporins (14 patients), clindamycin alone or in combination withciprofloxacin (six patients), ciprofloxacin alone (three patients) or aztreonam plusvancomycin (one patient). Albumin (1 g/kg for one day) was administered only topatients with serum creatinine greater than 1.5 mg/dl (133 lmol/L). Complica-tions of cirrhosis developing during hospitalization were treated according tostandard protocols [18]. Survival was analyzed at 3 months.Control group: patients with cirrhosis without infectionThe control group was composed of 92 contemporary hospitalized patients,matched by the severity of the disease, as assessed by the Child–Pugh score thatneither had signs of infection at admission nor developed an infection during hos-pitalization. These patients were admitted to hospital for a variety of reasons,including treatment of ascites (40 patients), gastrointestinal bleeding (35patients), hepatic encephalopathy (14 patients), and miscellaneous reasons (threepatients).
Statistical analysis
The definitions of renal failure and hyponatremia were done according to previ-ous studies [13,19] and are provided as Supplementary material. Comparisons ofcontinuous variables among groups were performed using Student’s t test andMann–Whitney test. Categorical variables were compared with v2 test andWilcoxon test. Univariate analyses of predictive factors of development of renal
Table 1. Characteristics of patients with skin and soft tissue infection and patients
Skin and soft tissue infectio(n = 92)
Age (yr) 61 ± 12Sex (M/F) 54/38Alcoholic cirrhosis 48%Diabetes mellitus 30%Previous complications of cirrhosis:
Ascites 69%Hepatic encephalopathy 38%Gastrointestinal bleeding 25%Spontaneous bacterial peritonitis 8%
Ascites at inclusion 61%Hepatic encephalopathy at inclusion 26%Serum bilirubin (mg/dl) 3.7 ± 3.3Serum albumin (g/L) 27 ± 5INR 1.4 ± 0.3Serum creatinine (mg/dl) 1.2 ± 0.6Serum sodium (mEq/L) 132 ± 6Temperature (°C) 36.9 ± 0.9Heart rate (bpm) 86 ± 15Mean arterial pressure (mmHg) 85 ± 13Presence of shock 3%Leukocyte count (x 109/L) 8.3 ± 4.9Presence of SIRS* 37%Child-Pugh score (A/B/C) 9/47/36 MELD score 16 ± 5MELD-sodium score 21 ± 6
Values are expressed as mean ± SD.⁄Available in 82 patients in the study group and 59 patients in the control group.
Journal of Hepatology 2012
failure, hyponatremia, and survival were performed using standard statisticaltests. Multivariate analysis including variables with predictive value in the uni-variate analysis (p <0.10) was performed using stepwise logistic regression. Prob-ability curves were constructed using the Kaplan–Meier method. Statisticalanalysis was performed using the SPSS 14 for Windows (SPSS Inc., Chicago, IL).Results are expressed as mean ± SD. p <0.05 was considered statisticallysignificant.
Results
Characteristics of the patients
The baseline characteristics of patients from the two groups areshown in Table 1. Both groups were similar with respect to themajority of variables except for an expectedly higher bodytemperature and leukocyte count, and slightly higher serum bil-irubin levels and lower serum sodium levels in the SSTI group.Of note, there was no difference in the prevalence of SIRS andthe frequency of shock at admission was slightly higher in thecontrol group. Out of the 92 patients with SSTI, the infectionwas community-acquired in 46 (50%), health care-associatedin 37 (40%), and hospital-acquired in the remaining 9 (10%)[20,21].
from the control group.
n Control group(n = 92)
p value
60 ± 13 0.8867/25 0.0452% 0.5528% 0.75
62% 0.3125% 0.0732% 0.3110% 0.5470% 0.2129% 0.622.8 ± 2.4 0.0327 ± 4 0.881.5 ± 0.8 0.061.1 ± 0.5 0.33135 ± 6 0.00136.2 ± 0.6 <0.00186 ± 19 0.8689 ± 18 0.117% 0.316.4 ± 3.6 0.00437% 0.939/48/35 0.9916 ± 5 0.5319 ± 6 0.02
vol. 56 j 1040–1046 1041

Baseline Diagnosis End
Seru
m c
reat
inin
e (m
g/dl
)
3.5
2.5
2.0
1.5
0.5
3.0
1.0
0.0Peak
No renal failure (n = 72)Transient renal failure (n = 10)Persistent renal failure (n = 10)
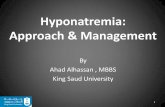
Fig. 1. Serum creatinine concentration before the infection (baseline), atdiagnosis of the infection, peak values, and values at the end of the 14-dayperiod in all patients with cirrhosis and skin and soft tissue infection dividedin three groups: no renal failure (n = 72), transient renal failure (n = 10), andpersistent renal failure (n = 10). The baseline value of serum creatinine was themost recent value available within the previous 3 months. Values are mean ± SD.
Baseline Diagnosis EndTrough
No hyponatremia (n = 55)Transient hyponatremia (n = 14)Persistent hyponatremia (n = 23)
120
125
130
135
140
145
Seru
mso
dium
(mEq
/L)
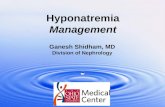
Fig. 2. Serum sodium concentration at baseline, at diagnosis of the infection,trough values, and values at the end of the 14-day period in all patients withcirrhosis and skin and soft tissue infection divided in three groups: nohyponatremia (n = 55) transient hyponatremia (n = 14) and persistent hypo-natremia (n = 23). The value of serum sodium before the infection was the mostrecent value available within the previous 3 months. Values are mean ± SD.
Research Article
In the study group, SSTI was the cause of admission in themajority of patients (83 out of 92, 90%). In most cases (72 outof 92, 78%) infection occurred in the legs and was associated withedema, which was severe in most cases. In the remaining 20patients, infection occurred in the abdomen, dorsum, arms, but-tocks, and scrotum in 11, 3, 3, 2, and 1 patient, respectively.The microbiological characteristics are shown in SupplementaryTables 1 and 2. Gram-positive bacteria were isolated more fre-quently than Gram-negative bacteria. Up to one third of culturesyielded Gram-negative bacteria.
Resolution of the infection was achieved in 88 patients (96%).Among those patients, only four had the initial antibiotic to bechanged either due to the results of cultures or empirically (car-bapenems in all of them). In the remaining four cases, infectiondid not resolve despite the change of antibiotics (carbapenemsin two, vancomycin in one, and ciprofloxacin plus teicoplanin inone) and patients died with unrelenting infection and multiorganfailure. Resolution was less common in patients with hospital-acquired infection (78%) compared to those with health care-associated or community-acquired infection (97% and 98%,respectively; p = 0.045).
Renal failure
Renal failure occurred in 20 patients with SSTI compared to onlyfive patients in the control group without infection (21.7% vs.5.4%, respectively, p = 0.001). In 16 out of the 20 patients withSSTI, renal failure was already present at the time of admission.Out of the 20 patients, 10 (50%) had transient renal failure, withserum creatinine values returning towards baseline during hospi-talization. In the remaining 10 patients, renal failure persistedafter the resolution of the infection. In the control group, renalfailure was present at admission in four out of the five patientsand was transient in all of them (100%) (serum creatinine from2.2 ± 0.6 to 1.1 ± 0.2 mg/dl, p = 0.028). Fig. 1 shows mean serumcreatinine concentration in patients with SSTI categorized inthree groups according to absence of renal failure and presenceof transient or non-transient renal failure.
Patients with SSTI and renal failure had significantly lowermean arterial pressure (79 ± 13 mmHg) and serum sodium con-centration (129 ± 5 mEq/L) at the time of diagnosis of infection
1042 Journal of Hepatology 2012
compared to patients without renal failure (87 ± 13 and 132 ± 6,respectively; p <0.05 for both). Moreover, the frequency of hepa-tic encephalopathy was higher in the former than in the lattergroup of patients (50% vs. 19%, respectively; p = 0.006). Renal fail-ure was more frequent in patients with hospital-acquired andhealth care-associated infection (44% and 27%, respectively) thanin those with community-acquired infection (13%; p = 0.021).Interestingly, there was no relationship between renal failureand presence of SIRS, shock or positive cultures.
Out of the 10 patients with non-transient renal failure, 4patients met the criteria of HRS, two type-1 and two type-2[22]. Four other patients developed renal failure likely due toacute tubular necrosis, in coincidence with septic shock, andtwo of them subsequently underwent hemodialysis. The remain-ing two patients had an acute deterioration of a previouslyknown renal failure due to parenchymal renal disease. None ofthe three patients treated with potentially nephrotoxic antibiot-ics (vancomycin in two and teicoplanin in one) developed renalfailure during treatment.
Hyponatremia
The development of hyponatremia was more common in patientswith SSTI compared to patients in the control group (37 patients–40%– vs. 23 patients –25%–, p = 0.028). In the whole group ofpatients with SSTI, serum sodium concentration decreased from135 ± 5 at baseline to a minimum value of 129 ± 5 mEq/L(p <0.001). In 19 out of the 37 patients with SSTI who developedhyponatremia, serum sodium decreased between 5 and 10 mEq/L, while in the remaining 18 patients it decreased more than10 mEq/L. Mean trough serum sodium values in these two sub-sets of patients were 126 ± 3 and 122 ± 5 mEq/L, respectively(p = 0.04). In 14 (38%) out of the 37 patients with hyponatremia,hyponatremia was transient and serum sodium values returnedto baseline, while in the remaining 23 patients (62%) hyponatre-mia persisted after the resolution of the infection (Fig. 2). Nospecific treatment for hyponatremia was given except for fluidrestriction to 1–1.5 liters per day. Patients with hyponatremiahad higher serum bilirubin (4.5 ± 4.3 mg/dl), serum creatinineconcentration (1.5 ± 0.7 mg/dl), and leukocyte count (9800 ±5700 per mm3) at the time of diagnosis of infection compared
vol. 56 j 1040–1046

p = 0.007
Patients at risk
7220
6915
6010
568
1.0
0.0
0.2
0.4
0.6
0.8
0 30Days
60 90
Surv
ival
No renal failure
Renal failure
Fig. 3. Probability of survival of patients with cirrhosis and skin and softtissue infection categorized in two groups according to the presence orabsence of renal failure. Numbers below the graph represent patients at risk atany given period.
JOURNAL OF HEPATOLOGY
to patients without hyponatremia (3.2 ± 2.3, 1.1 ± 0.5, and7300 ± 3900, respectively; p <0.05 for all). There was no relation-ship between development of hyponatremia and presence ofSIRS, shock, positive cultures or site of acquisition of the infection(either community-acquired or not). Hyponatremia was morecommon in patients with renal failure than in those without(65% vs. 33%, respectively, p <0.05).
Among the 23 patients from the control group who developedhyponatremia, serum sodium levels decreased between 5 and10 mEq/L in 13 patients, while in the remaining 10 it decreasedmore than 10 mEq/L. Hyponatremia was transient in eightpatients (35%) and persistent in the remaining 15 (65%).
Other complications of cirrhosis in patients with skin and soft tissueinfection
Twenty-nine patients (32%) had hepatic encephalopathy, in 24 itwas already present at the time of diagnosis of the infection(three patients grade 1, eight grade 2, nine grade 3, and fourgrade 4) and in five occurred during hospitalization (two patientsgrade 1, two grade 2, and one grade 4). There was no relationshipbetween the presence of SIRS at diagnosis of the infection andencephalopathy. Six patients developed gastrointestinal bleedingdue to a variety of reasons.
Mortality
At 3 months of follow-up, 64 out of the 92 patients with SSTIwere alive, 21 had died, four had been transplanted, and threewere lost to follow-up. Seven patients died during hospitalization(four of them with unrelenting skin infection and multiorgan fail-ure and the remaining three because of superimposed infections:sepsis in two patients and pneumonia in one). Fourteen patientsdied during follow-up. Causes of death were sepsis in seven, liverfailure in three, hepatorenal syndrome and unknown cause intwo patients each. In the whole series of patients with SSTI, theprobability of survival at 3 months was 76%. The developmentof renal failure during the infection was associated with poor out-come. Patients with renal failure had a 3-month probability ofsurvival lower than that of patients without renal failure (55%vs. 81%, respectively, p = 0.007) (Fig. 3). Factors associated with
Journal of Hepatology 2012
survival were baseline serum sodium concentration, mean arte-rial pressure, serum creatinine concentration, MELD, andMELD–sodium scores, presence of hepatic encephalopathy, shock,site of acquisition of the infection, and development of renal fail-ure during the infection (Table 2). The presence of SIRS at diagno-sis of the infection was related to in-hospital mortality (17% vs.4% in patients with and without SIRS, respectively; p = 0.04) butnot to 3-month mortality (27% vs. 21%, respectively, p = NS). Onmultivariate analysis, site of acquisition of the infection andMELD–sodium score were the only factors independently associ-ated with survival (OR 4.66 (95% CI 1.55–14.01) and 1.15 (95% CI1.06–1.25), respectively). Three-month mortality in patients withhealth care-associated or hospital-acquired SSTI was 30% and67%, respectively, compared to only 9% in patients with commu-nity-acquired SSTI (p <0.001). The best cut-off level of MELD–sodium that predicted survival as assessed by receiver operatingcharacteristics curves was 22. Three-month survival in patientswith MELD–sodium equal to or inferior than 22 was 92% com-pared to only 57% in patients with MELD–sodium greater than22 (p <0.005) (Fig. 4).
In the control group, among the 92 studied patients, threepatients died, one was transplanted and four were lost to fol-low-up during a 3-month period. Causes of death were liver fail-ure, sepsis and upper gastrointestinal bleeding in one patienteach. The probability of survival at 3 months was 96%, (p <0.001vs. study group).
Discussion
Patients with cirrhosis may develop infections of the skin andsoft tissue. For comparison with other infections occurring in cir-rhosis, such as spontaneous bacterial peritonitis or sepsis fromunknown origin, SSTI is generally considered a non-severe infec-tion. The results of the current study challenge this general belief.In fact, the evaluation of a large cohort of consecutive patientswith cirrhosis and SSTI indicate that it should be considered asevere infection because it is frequently associated withimportant complications of cirrhosis, particularly renal failure,hyponatremia, and hepatic encephalopathy, and a relatively high3-month mortality.
The most outstanding result of our study is that SSTI was asso-ciated with development of renal failure in up to 22% of patients,an incidence similar or only slightly lower than those reported forother infections, such as spontaneous bacterial peritonitis, uri-nary tract infections or pneumonia [11,14,23–25]. This incidenceof renal failure is ten times higher than that reported for SSTI inthe general population, which is only of 2.3% [26] and four timeshigher than that observed in the current study in a control groupof patients with cirrhosis admitted to the hospital for conditionsother than infections. The pathogenic mechanism(s) leading torenal failure in patients with SSTI was not specifically assessedin the current study. In other infections in cirrhosis, renal failureis considered to be related to impairment in circulatory dysfunc-tion that causes renal vasoconstriction and reduced glomerularfiltration rate, although other mechanisms such as injury of renaltubular cells may also play a role [27]. In the current study, thefact that patients with renal failure had lower mean arterial pres-sure than those without renal failure suggests a role for circula-tory dysfunction in the occurrence of renal failure. Of note, in agreat proportion of patients, renal failure was already present
vol. 56 j 1040–1046 1043

Table 2. Baseline factors associated with 3-month survival.
Alive (n = 71) Dead (n = 21) p valueAge (yr) 59 ± 12 65 ± 11 0.056Alcoholic cirrhosis 49% 43% 0.60Previous treatments*:
Diuretics 64% 75% 0.35Lactulose 26% 40% 0.23Beta-blockers 16% 25% 0.35Norfloxacin 11% 20% 0.31
Serum bilirubin (mg/dl) 3.6 ± 3.4 4.2 ± 3.1 0.45Serum albumin (g/L) 27 ± 5 27 ± 6 0.73INR 1.3 ± 0.2 1.5 ± 0.5 0.18Serum creatinine (mg/dl) 1.2 ± 0.6 1.5 ± 0.7 0.049Renal failure 17% 38% 0.039Serum sodium (mEq/L) 133 ± 5 129 ± 6 0.009Heart rate (bpm) 86 ± 15 85 ± 16 0.70Mean arterial pressure (mmHg) 87 ± 12 79 ± 14 0.012Presence of shock 0% 14% 0.01Leukocyte count (x 109/L ) 8.1 ± 5.0 9.1 ± 4.7 0.39Presence of SIRS** 34% 42% 0.51Health care-associated or Hospital-acquired infection
29/71 (41%) 17/21 (81%) 0.001
Hepatic encephalopathy 20% 48% 0.01Child-Pugh score C 34% 57% 0.14MELD score 16 ± 5 18 ± 5 0.032MELD-sodium score 20 ± 6 24 ± 5 0.004
Values are expressed as mean ± SD.⁄Treatments that patients were receiving at time of diagnosis of the infection.⁄⁄Available in 82 patients.
1.0
0.0
0.2
0.4
0.6
0.8
0 30Days
60 90
Surv
ival
MELD-sodium <22
MELD-sodium ≥22
p <0.001
Patients at risk
4052
3449
2446
1943
Fig. 4. Probability of survival of patients with cirrhosis and skin and softtissue infection categorized in two groups according to MELD–sodium scoreat the time of diagnosis of infection: lower than 22 and equal to or greaterthan 22. Numbers below the graph represent patients at risk at any given period.
Research Article
at the time of hospital admission, indicating that renal failure isan early event of SSTI in cirrhosis. As reported with other infec-tions in cirrhosis, in more than half of the patients renal failurepersisted despite the resolution of infection [13,28].
1044 Journal of Hepatology 2012
In recent years, it has become increasingly evident that bacte-rial infections in cirrhosis may impair the renal capacity toexcrete solute-free water and lead to the development of hypona-tremia [13,29]. The pathogenesis of hyponatremia in the settingof infection is not well understood but it is probably related, atleast in part, to the circulatory dysfunction that occurs as a con-sequence of the infection with increased secretion of antidiuretichormone [13]. The reduction in serum sodium concentration maybe of clinical significance bearing in mind that hyponatremia isassociated with an increased risk of hepatic encephalopathyand impaired prognosis [30,31]. In the current study, up to 40%of patients developed hyponatremia in association with SSTI, anincidence significantly higher than the 25% observed in the con-trol group of patients without infection. Besides, in almost twothirds of patients, hyponatremia persisted despite the resolutionof the infection.
Another frequent complication observed in the current cohortof patients was hepatic encephalopathy, which occurred inalmost one third of patients during hospitalization. Bacterialinfections, mainly spontaneous bacterial peritonitis and sepsis,are well known triggering factors of hepatic encephalopathy incirrhosis and their pathogenesis is probably related to the localsynthesis of inflammatory mediators at the site of the infection,together with a possible participation of renal dysfunction andhyponatremia [14,32,33]. Our findings are in agreement with this
vol. 56 j 1040–1046

JOURNAL OF HEPATOLOGY
hypothesis and indicate that hepatic encephalopathy is commonin patients with an apparently limited infection, such as SSTI. Theresults of our study also indicate a relationship between presenceof SIRS at diagnosis of the skin infection and in-hospital mortal-ity, in agreement with other reports [34,35]. However, therewas no relationship between SIRS and renal failure or hepaticencephalopathy.Three-month mortality in the current series of patients washigh (23%), a mortality slightly lower than that observed forpatients with cirrhosis and sepsis, excluding patients with spon-taneous bacterial peritonitis, which was of 27% [13]. Although inour series of patients SSTI was the direct cause of death in onlyfour patients, it is likely that it contributed to death in otherpatients through the development of complications, particularlyrenal failure, hepatic encephalopathy or by causing acute-on-chronic liver failure. The occurrence of renal failure was associ-ated with poor outcome, the 3-month mortality in patientswho developed renal failure being 45% compared with only 19%in patients without renal failure. Independent predictive factorsof survival were the site of acquisition of the infection andMELD–sodium score. The good predictive ability of MELD–sodium score in the setting of cirrhosis with SSTI is probablyaccounted for by the fact that it combines the presence of renalfailure and hyponatremia, both important prognostic factors incirrhosis that occur frequently in patients with SSTI [27,36]. Pre-vious studies have demonstrated that the site of acquisition ofinfection has a prognostic value in different infections in cirrho-sis, particularly sepsis, and spontaneous bacterial peritonitis[1,37]. Our study extends these observations to patients with SSTIand indicates that not only patients with hospital-acquired SSTI,but also those with health care-associated SSTI have an impairedprognosis. These findings are consistent with those of a recentstudy in a series of patients with cirrhosis and different typesof infections [21].
A last issue that deserves discussion is that, in a significantproportion of cases in our cohort, SSTI was due to Gram-negativebacilli. This had already been reported in small case series ofpatients with cirrhosis [15,16,38], and contrasts with the largepredominance of Gram-positive bacteria, mainly Staphylococcusaureus and Streptococci that cause SSTI in the non-cirrhotic pop-ulation [39].
The current study has several limitations. First, it has theintrinsic limitations of retrospective studies. Nonetheless, it isworth mentioning that taking into account the relatively low fre-quency of SSTI, it would be very difficult to collect a sufficientnumber of patients in a prospective study within a reasonableperiod of time. Second, the local characteristics of the infectioncould not be evaluated because they were not appropriatelyrecorded. It is possible that some of these characteristics mayhave a relationship with some of the complications reported aswell as outcome but this could not be investigated. Finally,although this study includes all consecutive patients with thediagnosis of SSTI admitted to our Unit, we cannot rule out com-pletely that some patients with mild infections were treated asoutpatients and therefore not included in the current analysis,thus causing a bias towards more severe cases.
In conclusion, the results of the current study indicate thatSSTI is not a benign complication of patients with cirrhosis.Instead, it should be included in the list of severe bacterial infec-tions complicating the natural course of cirrhosis. SSTI is fre-quently associated with renal failure, hyponatremia, and
Journal of Hepatology 2012
hepatic encephalopathy, and may be a triggering factor foracute-on-chronic liver failure. All these findings suggest that SSTIshould be diagnosed as early as possible and treated promptlywith iv antibiotics. MELD–sodium score is the best availablemethod to evaluate prognosis in patients with cirrhosis and SSTI.
Conflict of interest
The authors who have taken part in this study declared that theydo not have anything to disclose regarding funding or conflict ofinterest with respect to this manuscript.
Financial support
This work was supported by a Grant from Fondo de InvestigaciónSanitaria (FIS PI080126; to P.G.). G.P. and E.S. were supported by aGrant from the Fundación Banco de Bilbao–Vizcaya–Argentaria(FBBVA). C.F. was supported by a Grant from Instituto Reina Sofíade Investigación Nefrológica. CIBEREHD is funded by the Institutode Salud Carlos III.
Author’s contributions
G.P., M.G., and P.G. participated in the design of the study, anal-ysis and interpretation of data, and drafting of the manuscript.G.P., C.G., M.P., E.S., and E.R. participated in the collection of dataand data analysis. J.F. and V.A. participated in the interpretationof data and critical review of the manuscript for important intel-lectual content.
Acknowledgments
The authors would like to thank Raquel Cela R.N. and the nursingstaff of the Liver Unit and Intensive Care Unit for their participa-tion in the study.
Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.jhep.2011.11.023.
References
[1] Fernandez J, Navasa M, Gomez J, Colmenero J, Vila J, Arroyo V, et al. Bacterialinfections in cirrhosis: epidemiological changes with invasive proceduresand norfloxacin prophylaxis. Hepatology 2002;35:140–148.
[2] Arvaniti V, D’Amico G, Fede G, Manousou P, Tsochatzis E, Pleguezuelo M,et al. Infections in patients with cirrhosis increase mortality four-fold andshould be used in determining prognosis. Gastroenterology 2010;139:1246–1256.
[3] Tandon P, Garcia-Tsao G. Bacterial infections, sepsis, and multiorgan failurein cirrhosis. Semin Liver Dis 2008;28:26–42.
[4] Wong F, Bernardi M, Balk R, Christman B, Moreau R, Garcia-Tsao G, et al.Sepsis in cirrhosis: report on the 7th meeting of the International AscitesClub. Gut 2005;54:718–725.
[5] Gustot T, Durand F, Lebrec D, Vincent JL, Moreau R. Severe sepsis in cirrhosis.Hepatology 2009;50:2022–2033.
[6] Martin-Llahi M, Guevara M, Torre A, Fagundes C, Restuccia T, Gilabert R, et al.Prognostic importance of the cause of renal failure in patients with cirrhosis.Gastroenterology 2011;140:488–496.
vol. 56 j 1040–1046 1045

Research Article
[7] Martin PY, Ohara M, Gines P, Xu DL, St John J, Niederberger M, et al. Nitricoxide synthase (NOS) inhibition for one week improves renal sodium andwater excretion in cirrhotic rats with ascites. J Clin Invest1998;101:235–242.
[8] Fernández J, Monteagudo J, Bargallo X, Jimenez W, Bosch J, Arroyo V, et al.Randomized unblinded pilot study comparing albumin versus hydroxyethylstarch in spontaneous bacterial peritonitis. Hepatology 2005;42:627–634.
[9] Arroyo V, Terra C, Gines P. Advances in the pathogenesis and treatment oftype-1 and type-2 hepatorenal syndrome. J Hepatol 2007;46:935–946.
[10] Ruiz-del-Arbol L, Urman J, Fernandez J, Gonzalez M, Navasa M, Monescillo A,et al. Systemic, renal, and hepatic hemodynamic derangement in cirrhoticpatients with spontaneous bacterial peritonitis. Hepatology 2003;38:1210–1218.
[11] Sort P, Navasa M, Arroyo V, Aldeguer X, Planas R, Ruiz-del-Arbol L, et al.Effect of intravenous albumin on renal impairment and mortality in patientswith cirrhosis and spontaneous bacterial peritonitis. N Engl J Med1999;341:403–409.
[12] Navasa M, Follo A, Filella X, Jimenez W, Francitorra A, Planas R, et al. Tumornecrosis factor and interleukin-6 in spontaneous bacterial peritonitis incirrhosis: relationship with the development of renal impairment andmortality. Hepatology 1998;27:1227–1232.
[13] Terra C, Guevara M, Torre A, Gilabert R, Fernandez J, Martin-Llahi M, et al.Renal failure in patients with cirrhosis and sepsis unrelated to spontaneousbacterial peritonitis: value of MELD score. Gastroenterology 2005;129:1944–1953.
[14] Fasolato S, Angeli P, Dallagnese L, Maresio G, Zola E, Mazza E, et al. Renalfailure and bacterial infections in patients with cirrhosis: epidemiology andclinical features. Hepatology 2007;45:223–229.
[15] Corredoira JM, Ariza J, Pallares R, Carratala J, Viladrich PF, Rufi G, et al. Gram-negative bacillary cellulitis in patients with hepatic cirrhosis. Eur J ClinMicrobiol Infect Dis 1994;13:19–24.
[16] Horowitz Y, Sperber AD, Almog Y. Gram-negative cellulitis complicatingcirrhosis. Mayo Clin Proc 2004;79:247–250.
[17] Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al.Liver transplantation for the treatment of small hepatocellular carcinomas inpatients with cirrhosis. N Engl J Med 1996;334:693–699.
[18] Cárdenas A, Ginès P. Management of complications of cirrhosis in patientsawaiting liver transplantation11. J Hepatol 2005;42:S124–S133.
[19] Solà E, Lens S, Guevara M, Martin-Llahi M, Fagundes C, Pereira G, et al.Hyponatremia in patients treated with terlipressin for severe gastrointes-tinal bleeding due to portal hypertension. Hepatology 2010;52:1783–1790.
[20] Venditti M, Falcone M, Corrao S, Licata G, Serra P. Study Group of the ItalianSociety of Internal Medicine. Outcomes of patients hospitalized withcommunity-acquired, health care-associated, and hospital-acquired pneu-monia. Ann Intern Med 2009;6 (150):19–26.
[21] Merli M, Lucidi C, Giannelli V, Giusto M, Riggio O, Falcone M, et al. Cirrhoticpatients are at risk for health care-associated bacterial infections. ClinGastroenterol Hepatol 2010;8:979–985.
[22] Salerno F, Gerbes A, Ginès P, Wong F, Arroyo V. Diagnosis prevention andtreatment of the hepatorenal syndrome in cirrhosis. A consensus workshopof the international ascites club. Gut 2007;56:1310–1318.
[23] Kim JH, Lee JS, Lee SH, Bae WK, Kim NH, Kim KA, et al. Renal dysfunctioninduced by bacterial infection other than spontaneous bacterial peritonitis
1046 Journal of Hepatology 2012
in patients with cirrhosis: incidence and risk factor. Gut Liver2009;3:292–297.
[24] Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis.Hepatology 2008;48:2064–2077.
[25] Terg R, Gadano A, Cartier M, Casciato P, Lucero R, Munoz A, et al. Serumcreatinine and bilirubin predict renal failure and mortality in patients withspontaneous bacterial peritonitis: a retrospective study. Liver Int2009;29:415–419.
[26] Figtree M, Konecny P, Jennings Z, Goh C, Krilis SA, Miyakis S. Risk stratificationand outcome of cellulitis admitted to hospital. J Infect 2010;60:431–439.
[27] Ginès P, Schrier RW. Renal failure in cirrhosis. N Engl J Med2009;361:1279–1290.
[28] Follo A, Llovet JM, Navasa M, Planas R, Forns X, Francitorra A, et al. Renalimpairment after spontaneous bacterial peritonitis in cirrhosis: incidence,clinical course, predictive factors and prognosis. Hepatology1994;20:1495–1501.
[29] Porcel A, Diaz F, Rendon P. Dilutional hyponatremia in patients withcirrhosis and ascites. Arch Intern Med 2002;162:323–328.
[30] Guevara M, Baccaro ME, Torre A, Gomez-Anson B, Rios J, Torres F, et al.Hyponatremia is a risk factor of hepatic encephalopathy in patients withcirrhosis: a prospective study with time-dependent analysis. Am J Gastro-enterol 2009;104:1382–1389.
[31] Heuman DM, Bou-Assi SG, Habib A, Williams LM, Stravitz RT, Sanyal AJ, et al.Persistent ascites and low serum sodium identify patients with cirrhosis andlow MELD scores who are at high risk for early death. Hepatology2004;40:802–810.
[32] Wright G, Jalan R. Ammonia and inflammation in the pathogenesis ofhepatic encephalopathy: pandora’s box? Hepatology 2007;46:291–294.
[33] Córdoba J, Minguez B. Hepatic encephalopathy. Semin Liver Dis2008;28:70–80.
[34] Cazzaniga M, Dionigi E, Gobbo G, Fioretti A, Monti V, Salerno F. The systemicinflammatory response syndrome in cirrhotic patients: relationship withtheir in-hospital outcome. J Hepatol 2009;51:475–482.
[35] Thabut D, Massard J, Gangloff A, Carbonell N, Francoz C, Nguyen-Khac E,et al. Model for end-stage liver disease score and systemic inflammatoryresponse are major prognostic factors in patients with cirrhosis and acutefunctional renal failure. Hepatology 2007;46:1872–1882.
[36] Kim WR, Biggins SW, Kremers WK, Wiesner RH, Kamath PS, Benson JT, et al.Hyponatremia and mortality among patients on the liver-transplant waitinglist. N Engl J Med 2008;359:1018–1026.
[37] Cheong HS, Kang CI, Lee JA, Moon SY, Joung MK, Chung DR. Clinicalsignificance and outcome of nosocomial acquisition of spontaneous bacterialperitonitis in patients with liver cirrhosis. Clin Infect Dis 2009 May 1;48(9):1230–1236.
[38] Carratala J, Roson B, Fernandez-Sabe N, Shaw E, Del RO, Rivera A, et al.Factors associated with complications and mortality in adult patientshospitalized for infectious cellulitis. Eur J Clin Microbiol Infect Dis2003;22:151–157.
[39] Jenkins TC, Sabel AL, Sarcone EE, Price CS, Mehler PS, Burman WJ. Skin andsoft-tissue infections requiring hospitalization at an academic medicalcenter: opportunities for antimicrobial stewardship. Clin Infect Dis2010;51:895–903.
vol. 56 j 1040–1046