Relationship Concentration Enamel, Community Area High...
6
Relationship Between Fluoride Concentration in Enamel, DMFT Index, and Degree of Fluorosis in a Community Residing in an Area with a High Level of Fluoride J. I. BISCHOFF, E. H. Al. AN DER MERWE, D. H. RETIEF, F. H. BARBAKOW, and P. E. CLEA TON-JONES Dental Research Unit of the University of the Witwatersrand, and the South African Medical Research Council, Johannesburg, Republic of South Africa The DMFT index, degree of fluorosis (DEGF), fluoride concentration in enamel (F), and depth of etch (D) were determined in participants living in an area with a high fluoride level. A statistically significant dif- ference was found between men and women for F and D. A significant correlation was established between F and DEGF and be- tween F and age for men, but not for women. Dental fluorosis is a condition that has been recognized and reported on since the be- ginning of the century. McKay observed it in Colorado Springs in 19011 and by 1916 it had been connected with decreased caries incidence.2 Two years later it was coIn- cluded that some element present in the wa- ter consumed by people who had mottled teeth was responsible for the staining.3 In 1931, Churchill4 suspected a correlation be- tween mottled enamel and fluoride concen- tration in water. This correlation was con- firmed later that year by Smith and Smith,5 who experimentally produced mottled enamel in rats by feeding them varying amounts of sodium fluoride. More recently, the phenomenon of de- creased caries experience in areas having a fluoride concentration in water of 1 ppm or more has been well documented.6-13 In ad- dition, Richards et al6 and Binder'0 have shown a positive relationship between den- tal fluorosis and reduced caries incidence. Furthermore, it has been reported that an increase in the concentration of fluoride in the water supply resulted in an increase in Received for publication December 30, 1974. Accepted for publication August 5, 1975. the fluoride concentration in enamel.14-18 The object of the present study was an attempt to relate these factors, namely flu- oride concentration in enamel, caries ex- pericnce, and the degree of fluorosis in a community residing in an area with a high fluioride level. Materials and Methods Since the fluoride concentration of South African waters has been documented,19,20 a well-defined geographical area northwest of Johnannesburg having an average fluoride concentration in the water greater than 1 ppm could be selected. The African village of Saulspoort, where endemic fluorosis is rampant, was chosen for this study. Samples of water from subterranean sources such as wells and boreholes, which constituted the main source of drinking wa- ter of the population, were collected in plastic containers. The various fluoride con- centrations in the water were determined2122 using a fluoride ion combination electrodea coupled to a digital pH meter.b The participants were chosen from pupils who attend one of the high schools in Saulspoort and who had been residing in the area from birth. Their ages ranged from 14 to 23 years and the sample was com- posed of 41 females and 47 males (Fig 1). The DMFT index of each participant was determined in good natural light with the use of a mouth mirror and sharp dental probe. The teeth were systematically ex- a Orion model 96-09, Orion Research Inc., Cambridge, Mass. b Orion model 701, Orion Research Inc., Cambridge, Mass. 37
Transcript of Relationship Concentration Enamel, Community Area High...

Relationship Between Fluoride Concentration in Enamel,DMFT Index, and Degree of Fluorosis in a CommunityResiding in an Area with a High Level of Fluoride
J. I. BISCHOFF, E. H. Al. AN DER MERWE, D. H. RETIEF,F. H. BARBAKOW, and P. E. CLEA TON-JONES
Dental Research Unit of the University of the Witwatersrand, andthe South African Medical Research Council, Johannesburg, Republic of South Africa
The DMFT index, degree of fluorosis(DEGF), fluoride concentration in enamel(F), and depth of etch (D) were determinedin participants living in an area with a highfluoride level. A statistically significant dif-ference was found between men and womenfor F and D. A significant correlation wasestablished between F and DEGF and be-tween F and age for men, but not for women.
Dental fluorosis is a condition that has beenrecognized and reported on since the be-ginning of the century. McKay observed itin Colorado Springs in 19011 and by 1916it had been connected with decreased cariesincidence.2 Two years later it was coIn-cluded that some element present in the wa-ter consumed by people who had mottledteeth was responsible for the staining.3 In1931, Churchill4 suspected a correlation be-tween mottled enamel and fluoride concen-tration in water. This correlation was con-firmed later that year by Smith and Smith,5who experimentally produced mottledenamel in rats by feeding them varyingamounts of sodium fluoride.More recently, the phenomenon of de-
creased caries experience in areas having afluoride concentration in water of 1 ppm ormore has been well documented.6-13 In ad-dition, Richards et al6 and Binder'0 haveshown a positive relationship between den-tal fluorosis and reduced caries incidence.Furthermore, it has been reported that anincrease in the concentration of fluoride inthe water supply resulted in an increase in
Received for publication December 30, 1974.Accepted for publication August 5, 1975.
the fluoride concentration in enamel.14-18The object of the present study was an
attempt to relate these factors, namely flu-oride concentration in enamel, caries ex-pericnce, and the degree of fluorosis in acommunity residing in an area with a highfluioride level.
Materials and MethodsSince the fluoride concentration of South
African waters has been documented,19,20 awell-defined geographical area northwest ofJohnannesburg having an average fluorideconcentration in the water greater than 1ppm could be selected. The African villageof Saulspoort, where endemic fluorosis isrampant, was chosen for this study.Samples of water from subterranean
sources such as wells and boreholes, whichconstituted the main source of drinking wa-ter of the population, were collected inplastic containers. The various fluoride con-centrations in the water were determined2122using a fluoride ion combination electrodeacoupled to a digital pH meter.bThe participants were chosen from pupils
who attend one of the high schools inSaulspoort and who had been residing inthe area from birth. Their ages ranged from14 to 23 years and the sample was com-posed of 41 females and 47 males (Fig 1).The DMFT index of each participant was
determined in good natural light with theuse of a mouth mirror and sharp dentalprobe. The teeth were systematically ex-
a Orion model 96-09, Orion Research Inc., Cambridge,Mass.
b Orion model 701, Orion Research Inc., Cambridge,Mass.
37
J Dent Res January-February 1976
FIG 1.-Age distribution of sample.
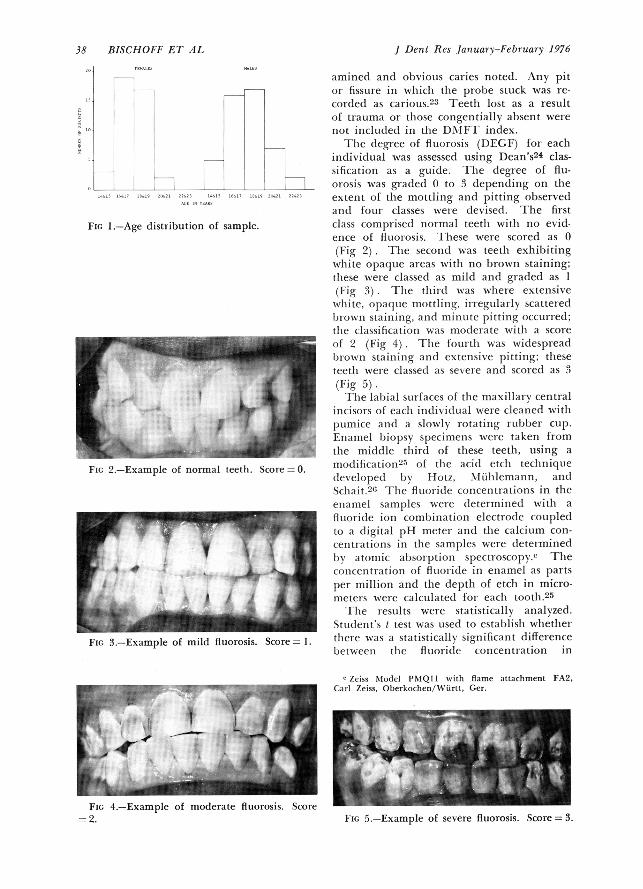
FIG 2.-Example of normal teeth. Score 0.
Fic, 3.-Example of mild fluorosis. Score -1.
aminedi and obvious caries noted. Any pitor fissure in wlhiclh thie prole stuck was re-corded as carious 3 Teethi lost as a resultof trauma or tlhose congentially al)sent werenot inclu(le(l in the DMIFT index.The degree of fluorosis (DEGF) for eaclh
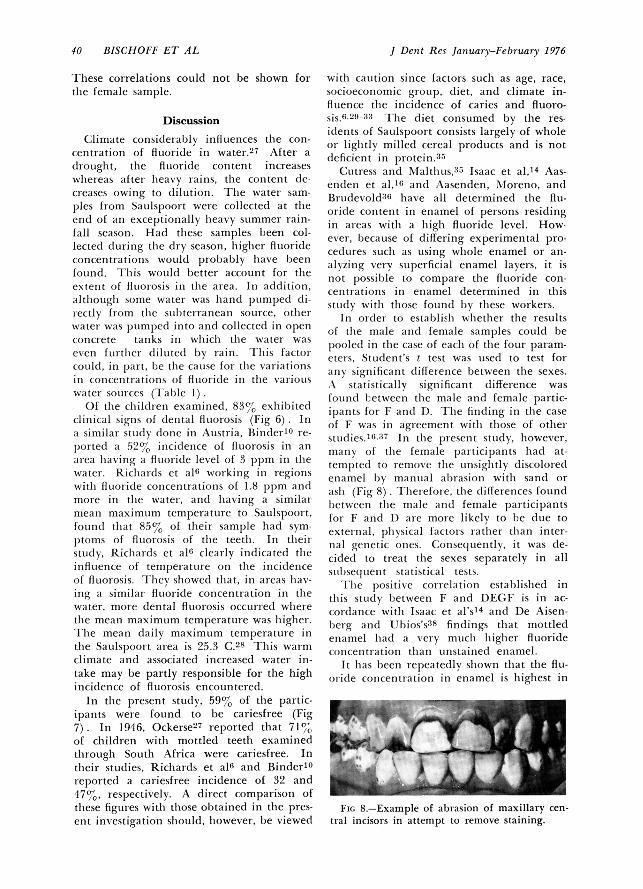
individual was assessed using Dean's24 clas-sification as a guide. Ihlie degree of flu-orosis was graded 0 to 3 depending on theextent of the mottling and pitting observedand foui classes wet-e dlevised. The firstclass comprised normal teetlh witlh no evid-en-ce of fltuotosis. Ihliese were scored as 0(Fig 2). The second was teeth exhibitingwhite opaqutie areas witlh no brown staining;these were classed as mild and graded as I(Fig 3) The tllirdI was wlhere extensivewilite, opaquLec mottlillg, irregularly scatteredbrown staiilng, and minullte pitting occturred;the classification was modertate withi a scoreof 2 (Fig 4). The fotll tlh was widespreadl)rowsn staining andl extensive pitting; theseteetlh wet-e classedl as severe and scored as 3(Fig 5).
Ilihe labial suirfaces of the maxillary centralincisors of each individual were cleaned witlpumice and ai slowly rotating rubber cup.Enamel biopsy specimenis were taken fromthe middle tlhird of these teeth, using amodificiltion125 of the acid etch teclhnique(levelopedl by Hotz, A7liihlemann, andSchait.2" I ihe fluoride concentrations in theenatmel samples were (letermined witlh afBiorodie ion combination electrode coupledto a digital pH metex antI tlhe calciuim con-centrationis in the samples were dleterminedby atomic al)sorption spectroscopy.c Theconcentration of fluori(le in eniamel as partsper million and the depth of etch in micro-meters wei-e calculated for eaclh tooth.25
lie -estults were statistically analyzed.Stud(lenit's t test was uised to establish wlhetlherthere wats a statistically significant differencebetweeni the fluioricle concentration in
e Zeiss Model PMIQII with flame attachment FA2,Carl Zeiss, Oberkochen/WXurtt, Ger.
FIG 4.-Example of moderate fluorosis. Score2. FIG 5.-Example of severe fluorosis. Score= 3.
38 BISCHOFF ET AL
ENAMEL FLUORIDE, DMFT, & FLUOROSIS 39
TABLE 1FLUORIDE CONCENTRATIONS OF SAULSPOORT
DRINKING WATER
Water Sample ppm F
1 6.162 4.423 3.604 0.405 3.566 4.427 1.868 1.009 0.9610 0.6411 1.1212 0.93
enamel for the left and right incisors (FL,FR) and was similarly applied in the caseof depth of etchi (DL, DR). As no signif-icant differences were found, two new para-meters were created for each individual.These were fluoride concentration in enamel(F) and depth of etch (D), each being re-spectively equal to FL + FR and DL + DR.
2 2The differences between the male and
female participants for the four parameters-F, D. DMFT index, and DEGF-were testedusing Student's t test.
Treating the male and female sampleseparately, the relationship between all pairsof variables was tested by computing thePearson (product moment) correlation coef-ficient. Spearman's correlation coefficient wasalso computed in the case of the nonpara-metric data, for example, DMFT index andDEGF.
TABLE 2MEANS OF FOUR PARAMETERS MEASURED FOR
EACH SEX
Mean Value
Parameter Males Females
Enamel fluorideconcentration(ppm) ± SD
Depth of etch(gm) + SD
DMFT index + SD
Degree offluorosis ± SD
1,762 ± 1,598 1,159 + 890
40
30En
,W
CD[, 200
z10
0 1 2
DEGREE OF FLUOROSIS
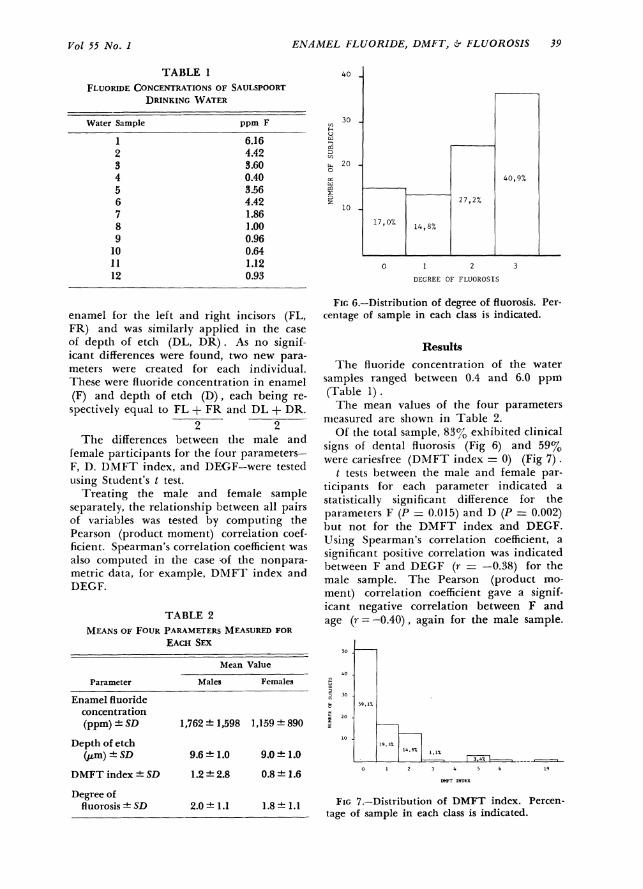
FIG 6.-Distribution of degree of fluorosis. Per-centage of sample in each class is indicated.
ResultsThe fluoride concentration of the water
samples ranged between 0.4 and 6.0 ppm(Table 1)The mean values of the four parameters
nieasured are shown in Table 2.Of the total sample, 83% exhibited clinical
signs of dental fluorosis (Fig 6) and 59%were cariesfree (DMFT index = 0) (Fig 7).
t tests between the male and female par-ticipants for each parameter indicated astatistically significant difference for theparameters F (P = 0.015) and D (P = 0.002)but not for the DMFT index and DEGF.Using Spearman's correlation coefficient, asignificant positive correlation was indicatedbetween F and DEGF (r = -0.38) for themale sample. The Pearson (product mo-ment) correlation coefficient gave a signif-icant negative correlation between F andage (r=-0.40), again for the male sample.
40-
. 30
10
9.6 ± 1.0 9.0 ± 1.0
1.2 + 2.8 0.8 ± 1.6
59,1%
9,3%
14,8%
2.0 + 1.1 1.8 + 1.1 FIG 7.-Distribution of DMFT index. Percen-tage of sample in each class is indicated.
, A
19
Vol, 55 No. I
0 1 2 3 4 5 6
DMFT INDEX
J Dent Res January-February 1976
These correlations could not be shown forthe female sample.
Discussion
Climate considerably inifluences the con-cenitration of fluoride in water.27 After a(boughlt, the fluoride content increaseswlhereas after lheavy rainis, the conitent de-creases owing to (lilutioni. Thle water sam-ples from Saulspoort weie collected at theend of an exceptionally heavy summer rain-fall season. Hacl these samples b)een col-lectedl (Iltring the dry seasoni, hiighier fluorideconcentrations would probably hiave beenfound. 1 hlis would better account for thee\tent of fluloiosis in the area. In addition,although some water wats lhand pumped di-rectly from the sUbterranean source, oth-erwatul was pumpedhlito and collected in openconcrete tanks in whiiclh the water wasoxen fLll-tller (lilLted by rain. This factor(0111(1, in part, be thle caulse foi- the vairiationsin concentrations of fluoi ide in thte vxai iouswater sources (TIalle 1).Of the childclren examinied, 83% exhlibitedl
clinical signs of dlenital fluLorosis (Fig 6) . Ina similar studly (lonie in Austria, Ii ndieil10 re-I)orte(l a 52%CX incidence of fIltorosis in an
area having a filuoride level of 3 ppm in thewater. Richaids et al" woi king in regionsWitll fluai ide conicentrationis of 18 ppm anclmoi-c in the water, andl having a similairmean maximtum temperattire to Saulspooi t,foulndi that 85% of their sample lhad sym-ptoms of fluiorosis of tlhe teethi. In tlheiistudly, Richards et al" cleaily indicated theinifluence of temperatuire on the incidenceOf fltorosis. iYhey showedl tihat, in areas h1a-sing a similar fltoride conicentration in thewater, more dlental fluoi-osis occturredl wlherethe mean maximuim temperature was hiigler.'Ilhe mean (laily maximum temperature inthe Satulspoort area is 25.3 C.28 T1his warmclimate and associated increased water in-take may be partly responsible for the highinicidlence of fluorosis encouinteredl.
In thle present study, 59% of the partic-ipanits were found to be cariesfree (Fig7). In 1946, Ockerse27 reported that 71%/Oof clhildren witlh mottled teetlh examinedtlhroughi Southi Africa were cariesfree. Intheir studies, Richards et al" and Binder10ieported a cariesfree incidence of 39 and47%, respectively. A direct comparison ofthlese figuires witlh those obtained in the pres-eut investigation should, lhowever, be viewed
with caution sinice factors suchI as age, race,socioeconiomic group, (liet, and climate in-filuence the incidence of caries and fluoro-Sis.629-3' I'lhe diet consumed by the res-icdents of Saulspoort consists largely of wholeo0 liglitly milled cereal products and is not(deficient in protein.3'5
Cutress and Mlalthlus,;15 Isaac et al,14 Aas-endlen et al,1(; and Aasenden, Mforeno, andiBriutdex old8"6 lhave all (leterminedl tile flLu-oridle conitenit in enamel of persons residingin ai-eas withi a hiighi fluoride level. How-ever, b)ecause of differing experimental pro-cedltires suchi as iusing whole enamel or an-alyiing very superficial enamel Layers, it isnot possible to compare the fluori(le con-centriations in enamel determinied in thisstuidy with those fouincd by these workers.
In orider to estalblisll w Ilethler the result.sof the male and female samples could beioole(l in tile case of eaclh of the four param-eters, Stud(lent's t test was tisedI to test forany significa nit dlifferenice between tlhe sexes.iX statistically signiificant difference wasfuCnd 1.etween the male and female partic-if)ants for F and r). Tlhe finding in tile caseof F was in agreement witil those of otlheistudies.'63 In tile )resent stuLdiy, liowever,many of the female participanlts ilad at-temltedl to remoxve tl1e tinsiglltly rliscoloreclenamel by manuial abrasion witlh sandc orashl (Fig 8) Therefoie, tlhe rliflerences fotundIi)etween the male and female pairticipantsfor F andl I) are more likely to be cdiue toexte nal, plhysical factors rather tilan inter-ilal gelletic ones. Consequently, it was de-cidedl to treat tile sexes separately in allstuibsequienit statistical tests.
Tlie positixe correlation established inthils stuLdy between F and DEGF is in ac-cordance witlh Isaac et al's14 andl De Aisen-berg and Ubios's38 findings tiht mottledenalmel hladl a \ ery much Iliglier fltioridecolcentration tilali uiinstainied enamel.
It hlas b)een repeatedly sliown that tlhe flu-0ride concentrationl in enamel is Iligllest in
Fic 8.-Example of abrasion of maxillary cen-tial incisors in attempt to remove staining.
40 BISCHOFF ET AL
ENAMEL FLUORIDE, DMFT, - FLUOROSIS 41
the outer region and falls steeply from thesurface to a plateau in the interior.36,39 Be-cause of this very characteristic distribution,only a small amount of wear is required toproduce a considerable change in the flu-oride concentration of the enamel surface.This would account for the significant neg-ative correlation between F and age estab-lislhed lhere. The tendency for the level offlu-oride concentration in enamel to decreasewith age has also been previously demon-strated.40,41 The correlation established inthis study supports the conclusion made byWeatherall, Hallsworth, and Robinson4' thatthe fluoride lost from the outer enamel sur-face as a result of wear is not restored to anappreciable extent even in areas where thefluoride content of the water supply is Ihigh.The correlations between F and DEFG
and F and age could not be shown for thefenmale sample. A possible reason for thismay again be the removal of stained enamelby many of the female participants. Theywould thereby remove the layer of super-ficial enamel that contains the highest flu-oride concentration. This would mask anycorrelation involving fluoride concentrationthat could otherwise emerge.No correlation was found wlhen testing
DMFT index against any of the other pa-rameters. This may be accounted for bytwo factors. First, the whole sample was ex-posed to hiigh levels of fluoride that wouldconfer a highi degree of protection againstcaries. Second, Retief, Cleaton-Jones, andWalker42,43 have reported low caries inci-dence in a sample of a similar racial andsocioeconomic group residing in a nearbyfluoride-deficient area. These two factorsmay explain the low and narrow range ofDMFT indexes recorded in the presentstudy (Fig 7). In other etlinic groups wheretlhe DMFT index range is greater,42 correla-tion involving the DMFT index may befound.
ConclusionsThe object of the present study was an
attempt to relate fluoride concentration inenamel, caries experience, and the degree offluorosis in a community residing in an areawith a high level of fluoride. A significantdifference was found between the male andfemale samples for the F and D parameters.A positive correlation was established forthe male participants between DEGF and
F, and a negative correlation between ageand F. These correlations were not foundfor the female participants. Because of thelow and narrow range of DMIFT indexes,no correlation involving this parametercould be established.
The authors thank Mr. Phiri, the principal of theNIoruleng High School, Saulspoort, for his cooperationin availing his staff, his students, and facilities; Mrs. C.Sjolde of the Computer Center of the University ofthe Witwatersrand for her assistance in the statisticalanalysis; and the staff of the Dental Research Unit forphotography and typing of the manuscript.
References1. MURRAY, J.J.: A History of Water Fluorida-
tion, Br Dent J 134: 247-250, 299-302, 347-350, 1973.
2. McKAY, F.S., and BLACK, G.V.: An Investiga-tion of Mottled Teeth: An Endemic Devel-opmental Imperfection of the Enamel of theTeeth, Heretofore Unknown in the Litera-ture of Dentistry: Part I, Dent Cosmos 58:477-484, 1916.
3. McKAY, F.S., and BLACK, G.V.: An Investiga-tion of Mottled Teeth: An Endemic Devel-opmental Imperfection of the Enamel of theTeeth, Heretofore Unknown in the Litera-ture of Dentistry: III, Dent Cosmos 58: 781-792, 1916.
4. CHURCHILL, H.V.: Occurrence of Fluorides inSome Waters of the United States, IndustrialEngineering Chem 23: 996-998, 1931.
5. SMITH, H.V., and SMITH, M.C.: cited byMURRAY, J.J.: A History of Water Fluorida-tion, Br Dent J 134: 247-350, 1973.
6. RICHARDS, L.F.; WESTMORELAND, WV.W.; TA-SHIRO, M.; MCKAY, C.H.; and MORRISON, J.T.:Determining Optimum Fluoride Levels forCommunity Water Supplies in Relation toTemperature, JADA 74: 389-397, 1967.
7. MURRAY, J.: Caries Experience of 15-Year-Old Children from Fluoride and Non-Flu-oride Communities, Br Dent J 127: 128-131,1969.
8. MURRAY, J.J.: Adult Dental Health in Flu-oride and Non-Fluoride Areas: Part 1. MeanDMF Values by Age, Br Dent J 131: 391-395,1971.
9. MURRAY, J., and ATKINSON, K.: Caries Ex-perience of West Hartlepool Children Aged2-18 Years, Dent Pract 21: 385-388, 1971.
10. BINDER, K.: Comparison of the Effects ofFluoride Drinking Water on Caries Fre-quency and Mottled Enamel in Three Sim-ilar Regions of Austria over a 10-Year Pe-riod, Caries Res 7: 179-183, 1973.
11. JACKSON, D.; MURRAY, J.J.; and FAIRPO, C.G.:The Effect of Fluoride in Drinking Water onthe Number of Cavities in Teeth of 15-Year-Old Children, Br Dent J 134: 480-481, 1973.
12. JACKSON, D.; MURRAY, J.J.; and FAIRPO, C.G.:
Vol 55 No. I

J Dent Res January-February 1976
Life-Long Benefits of Fluoride in DrinkingWater, Br Dent J 134: 419-422, 1973.
13. AASENDEN, R., and PEEBLES, T.C.: Effects ofFluoride Supplementation from Birth onHuman Deciduous and Permanent Teeth,Arch Oral Biol 19: 321-326, 1974.
14. ISAAC, S.; BRUDEVOLD, F.; SMITH, F.A.; andGARDNER, D.E.: The Relation of Fluoride inthe Drinking Water to the Distribution ofFluoride in Enamel, J Dent Res 37: 318-325,1958.
15. WEATHERELL, J.A., and HARGREAVES, J.A.:The Fluoride Content of Surface Enamelfrom Permanent and Deciduous Teeth, AdvFluorine Res 4: 181-191, 1966.
16. AASENDEN, R.; ALLUKIAN, M.; BRUDEVOLD, F.;and WELLOCK, W.D.: An In Vivo Study onEnamel Fluoride in Children Living in aFluoridated and in a Non-Fluoridated Area,Arch Oral Biol 16: 1399-1411, 1971.
17. RYTOMAA, I.; KLEEMOLA-KUJALA, E.; KEINO-NEN, J.; and ANTTILA, A.: Fluoride Contentsof Surface Enamel in High- and Low-Flu-oride Areas Studied with a Sensitive PhysicalMethod, Scand J Dent Res 82: 197-201, 1974.
18. CHARLTON, G.; BLAINEY, B.; and SCHAM-SCHULA, R.G.: Associations Between DentalPlaque and Fluoride in Human SurfaceEnamel, Arch Oral Biol 19: 139-143, 1974.
19. OCKERSE, T.: Report on the Incidence oJDental Caries Among School Children inSouth Africa, Pretoria: Government Printer,1944, pp 15-17.
20. Report of the Commission of Inquiry intoFluoridation, Pretoria: Government Printer,1966, pp 140-141.
21. FRANT, M.S., and Ross, J.W.: Use of a TotalIonic Strength Adjustment Buffer for Elec-trode Determination of Fluoride in WaterSupplies, Anal Chem 40: 1169-1171, 1968.
22. HARWOOD, J.E.: The Use of an Ion-SelectiveElectrode for Routine Fluoride Analyses onWater Samples, Water Res 3: 273-280, 1969.
23. STAZ, J.: Dental Caries in South Africa, SAfr J Med Sci 3 (suppl): 1-63, 1938.
24. DEAN, H.T.: Classification of Mottled EnamelDiagnosis, in MCCLURE, F.J. (ed): FluorideDrinking Waters, Public Health Service Pub-lication No. 825, US Department of Health,Education, and Welfare, 1962, pp 23-26.
25. VAN DER MERWE, E.H.M.; RETIEF, D.H.;BARBAKOW, F.H.; and FRIEDMAN, M.: AnEvaluation of an In Vivo Enamel Acid EtchBiopsy Technique for Fluoride Determina-tion, J Dent Assoc S Afr 29: 81-87, 1974.
26. HOTZ, P.; MUHLEMANN, H.R.; and SCHAIT,A.: A New Method of Enamel Biopsy forFluoride Determination, Helv Odontol Acta14: 26-29, 1970.
27. OCKERSE, T.: Fluorine and Dental Caries inSouth Africa, in MOULTON, F.R. (ed): Den-
tal Caries and Fluorine, Lancaster, Pa.: TheScience Press Printing Co., 1946, pp 36-42.
28. TYSON, P.D.: Personal communication.29. TABRAH, F.: Absence of Dental Caries in a
Nigerian Bush Village, Science 138: 38-39,1962.
30. SHEIHAM, A.: The Prevalence of DentalCaries in Nigerian Populations, Br Dent J123: 144-148, 1967.
31. HOFFMANN-AXTHELM, W.: Acht Jahre Karies-statistik in einem Endemischen Fluorgebiet,Arch Oral Biol 6: 12-16, 1961.
32. JANSEN VAN RENSBURG, B.G.: Protein-Defi-cient Diet, Fluoride and Amelogenesis, JDent Assoc S Afr 27: 204-209, 1972.
33. ENWONWU, C.O.: Socio-Economic Factors inDental Caries Prevalence and Frequency inNigerians: An Epidemiological Study, CariesRes 8: 155-171, 1974.
34. WALKER, A.R.P.: Nutritional, Biochemical,and Other Studies on South African Popu-lations, S Afr Med J 44: 814-852, 1966.
35. CUTRESS, T.W., and MALTHUS, R.S.: TheFluoride Concentrations and Acid Solubilityof Teeth from Fluoridated (I ppm) andLow-Fluoride Areas, NZ Dent J 66: 229-234,1970.
36. AASENDEN, R.; MORENO, E.C.; and BRUDEVOLD,F.: Fluoride Levels in the Surface Enamelof Different Types of Human Teeth, ArchOral Biol 18: 1403-1410, 1973.
37. AASENDEN, R.: Fluoride Concentrations inthe Surface Tooth Enamel of Young Menand Women, Arch Oral Biol 19: 697-701,1974.
38. DE AISENBERG, E.Y., and UBIos, A.M.: Deter-mination of Fluoride Content in HumanTeeth by Neutron Activation Analysis, JDent Res 53: 755, 1974.
39. BARBAKOW, F.H.; DE KOCK, A.C.; and RETIEF,D.H.: The Fluoride Concentration in theEnamel of Permanent Central Incisors, JDent Assoc S Afr 26: 134-138, 1971.
40. WEATHERELL, J.A.; ROBINSON, C.; and HALLS-WORTH, A.S.: Changes in the Fluoride Con-centration of the Labial Enamel Surface withAge, Caries Res 6: 312-324, 1972.
41. WEATHERELL., J.A.; HALLSWORTH, A.S.; andROBINSON, C.: The Effect of Tooth Wear onthe Distribution of Fluoride in the EnamelSurface of Human Teeth, Arch Oral Biol18: 1175-1189, 1973.
42. RETIEF, D.H.; CLEATON-JONES, P.E.; andWALKER, A.R.P.: Dental Caries in SouthAfrican Negro and Caucasian Schoolchildren,Lancet 2: 1456, 1973.
43. RETIEF, D.H.; CLEATON-JONES, P.E.; andWALKER, A.R.P.: Dental Caries and SugarIntake in South African Pupils of 16-17Years in Four Ethnic Groups, Br Dent J 138:463-469, 1975.
42 BISCHOFF ET AL