Additive Manufactured Models of Fetuses Built from 3D Ultrasound
Upload
giuseppe-rizzoCategory
view
215download
0
PRENATAL DIAGNOSISPrenat Diagn 2008; 28: 1042–1047.Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pd.2121
Relationship between aortic isthmus and ductus venosusvelocity waveforms in severe growth restricted fetuses
Giuseppe Rizzo1* , Alessandra Capponi2, Marianne Vendola1, Maria Elena Pietrolucci1and Domenico Arduini1
1Department Obstetrics and Gynecology, Universita di Roma “Tor Vergata”, Italy2Department Obstetrics and Gynecology, Ospedale GB Grassi Roma, Italy
Objective To evaluate the incidence of abnormalities in velocity waveforms from ductus venosus (DV)and aortic isthmus (AoI) in fetuses with intrauterine growth restriction (IUGR) and their reciprocal temporalrelationship.
Methods DV and AoI velocity waveforms were recorded in 31 IUGR fetuses characterized either by absentend diastolic (20) or reverse flow (11) in umbilical artery. Abnormal velocity waveforms in DV and AoI weredefined in presence of reverse diastolic flows.
Results Abnormal DV velocity waveforms were present in 10 fetuses and were always associated withabnormalities. Abnormal AoI flows were also present in 10 fetuses of the remaining 21 fetuses with normal DVvelocity waveforms (47.6%). Longitudinal monitoring of fetuses with normal DV flows showed a significantlyshorter time interval in the onset of reverse flow in DV when abnormalities in AoI were present (4 vs 14 daysp = 0.001) irrespectively of gestational age or other potential confounding variables.
Conclusions Our data suggest that AoI velocity waveforms become abnormal at an earlier stage of fetalcompromise than DV. Copyright 2008 John Wiley & Sons, Ltd.
KEY WORDS: fetal aortic isthmus; ductus venosus; IUGR; doppler ultrasound
INTRODUCTION
Fetuses with intrauterine growth restriction (IUGR)secondary to placental insufficiency are characterized byevident hemodynamic changes that usually start with aredistribution of the arterial circulation with preferentialdistribution of cardiac output toward the left ventricle,finalized to maintain an adequate oxygen supply to boththe brain and the heart (Rizzo and Arduini, 1991; Hecheret al., 1995; Baschat, 2004). Evident modifications occuralso at the level of the venosus circulation with aprogressive increase of ductus venosus (DV) shuntingand a concomitant reduction in umbilical flow to theliver, changes that seem to progress with the severity offetal compromise (Bellotti et al., 2004; Kiserud et al.,2006). With further fetal deterioration, these adaptivemechanisms are overwhelmed and cardiac dysfunctionoccurs. This condition results in an increased preloadwith the appearance of reverse velocity waveforms infetal DV, a condition usually associated with acidemia(Hecher et al., 1995; Rizzo et al., 1996). On this basisthe Doppler study of the DV is increasingly usedin the evaluation of IUGR fetuses. Despite this wideapplication of DV examination, there is no agreementon the clinical role DV as an indicator of the timing ofdelivery (Baschat et al., 2007; Ghidini, 2007).
*Correspondence to: Giuseppe Rizzo, Department Obstetricsand Gynecology, Universita di Roma Tor Vergata, Ospedale“Fatebenefratelli S. Giovanni Calabita”, Isola Tiberina 89, 00186Roma, Italy. E-mail: [email protected]
The aortic isthmus (AoI) is a physiological shunt inthe human fetus linking right and left ventricles (Fouron,2003). As a consequence, AoI blood flow velocity pat-terns reflect the balance between left and right ventric-ular outputs and are influenced by differences in theimpedance to flow in the placental and cerebral vascularsystems (Makikallio, 2008). Its role as an indicator ofthe progression of the hemodynamic deterioration occur-ring in IUGR and as a marker of short-term (Makikallioet al., 2003; Del Rio et al., 2008) and long-term out-comes (Fouron et al., 2005) has been recently suggested.However there is a lack of data on the temporal sequenceof the hemodynamic changes occurring in DV and AoIin IUGR fetuses. In this study, we analyzed the inci-dence of abnormalities in DV and AoI in IUGR fetusesand their temporal relationship.
MATERIAL AND METHODS
The 31 patients included in this study were part ofour high-risk pregnancies database and were collectedin the time interval between March 2006 and May2008. Patients gave informed written consent and thestudy protocol was approved by our local review board[granted as an RSA project 2006 (ateneum researchactivity)]. Pregnancies were selected according to thefollowing criteria: (1) gestational age confirmed byultrasound examination at 11–14 weeks of gestation,(2) fetal weight <10th percentile for our population
Copyright 2008 John Wiley & Sons, Ltd. Received: 19 July 2008Revised: 29 August 2008
Accepted: 1 September 2008

AORTIC ISTHMUS AND DUCTUS VENOSUS IN IUGR FETUSES 1043
standard confirmed at birth, (3) absence of fetal struc-tural and chromosomal abnormalities detected prena-tally and confirmed after birth, (4) absence of mater-nal diseases such as chronic or gestational hyperten-sion, preeclampsia and maternal diabetes, (5) abnormalumbilical artery velocity waveforms as expressed byabsence (20) or reverse flow (11) during end dias-tole, and (6) successful recordings from both DV andAoI. When serial Doppler recordings were available,we selected the first recording with absent or reverseend diastolic flow in umbilical artery. In such patients,fetal heart rate tracings were obtained at least dailyand Doppler recordings were repeated every 2 days.The median number of Doppler studies per patientwas 4 days (range 1–18) and the median time inter-val between the last Doppler recording and delivery orintrauterine death was 1 day (range 0–2 days).
Indications for delivery as determined by the manag-ing physician were: intrauterine fetal death, nonreassur-ing fetal heart rate tracing (repetitive variable/late decel-erations), cessation of fetal growth in the last 2 weeks.Doppler ultrasound was not an indication for delivery.Biophysical profile was not used in the study. All fetuseswere delivered in our institution.
Recordings were performed, using previously reportedtechniques (Rizzo et al., 1994, 2008a) by transabdom-inal ultrasonography (RAB 4–8 probe, Voluson 730and Voluson E8, GE Medical Systems, Milwaukee, WI,USA) with color and pulsed Doppler functions on fiveconsecutive and uniform velocity waveforms obtainedin absence of fetal breathing and body movements. Thehigh-pass filter was set at 90 Hz. The DV was sampledclose to its origin from umbilical vein in a transversescan of the abdomen. Velocity waveforms obtained weredivided according to their end diastolic velocity as flowpresent or reverse. DV pulsatility index (PI) was alsocalculated and compared with our previously constructedreference limits for gestation (Rizzo et al., 1996).
AoI velocity waveforms were recorded from the threevessels and trachea view obtained at the level of theupper fetal mediastinum in a transverse plane in whichaorta and ductus arteriosus join in a V-shaped vascularstructure. The color Doppler function was activated andthe pulsed Doppler sample volume was placed in theaorta close to the ductus arteriosus. The presence offorward diastolic flow was considered normal, whereasthe presence of reversed flow was considered abnormal.
Birthweights were expressed as absolute values andas number of standard deviations (z score); they dif-fered from the expected mean calculated from Ital-ian population standards after correction for gestationalage and sex of the newborn for newborns ≥28 weeks(Parazzini et al., 1991) and our local reference limits fornewborns delivered earlier than 28 weeks of gestation.Further perinatal outcome endpoints considered were:Apgar score 5′ < 7, intracerebral hemorrhage grade IIIor IV according to Papile classification (Papile et al.,1978) and requirement of respiratory support. Compar-ison between continuous and categorical variables wasperformed respectively by a Mann–Witney U test andFisher’s exact test. Relationships between variables wereestimated by Pearson’s correlation coefficient.
Finally multiple regression analysis was performed inorder to model the effect of individual variables (i.e.presence of forward or reverse end diastolic flow inAoI and DV, gestational age at first Doppler recording,birthweight and birthweight z score) on the time intervalbetween the first Doppler recordings and delivery. Thecategorical variables such as presence forward andreverse flow in AoI or DV were converted to a number ofbinary variables using dummy coding (Pedhazur, 1997).A p value <0.05 was considered as significant.
RESULTS
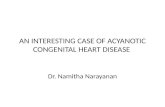
The characteristics of the study population are reportedin Table 1. Reverse end diastolic flow in DV was presentin 10 fetuses and in all these cases it was associated witha reverse flow in the AoI (Figure 1). When these 10pregnancies were compared with patients with positiveend diastolic flow in DV, they showed a higher incidenceof intrauterine death, a shorter interval between thefirst Doppler examination and delivery and a lowerabsolute birthweight (Table 2). No differences werefound in gestational age at the first Doppler examinationand in birthweight z score and neonatal complications(Table 2).
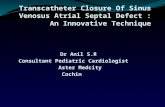
Considering the 21 fetuses with presence of enddiastolic flow in DV, a forward flow in AoI wasevidence in 11 cases (47.6%) and a reverse flow inthe remaining 10 cases (53.4%) (Figure 2). There wereno significant differences in gestational age at thefirst Doppler recordings (Table 3). However the timeinterval between the first Doppler recording and deliverywas significantly lower and a lower birthweight wasevidenced. No differences were found in birthweightz score and in the incidence of neonatal complications(Table 3). In these 21 fetuses with end diastolic forwardflow in DV, the DV PI values were greater than the 95thof our reference limits in six cases (6/21 28.6%) andwithin the reference limits in 15 (15/21 71.4%) cases.Grouping fetuses according to DV PI values did notallow evidencing of any significant differences in theperinatal variables tested.
Table 1—Characteristics of the study population
Median (range); no.%
Gestational age at Dopplerexamination (weeks)
26.1 (22.6–29.1)
Gestational age at deliveryor intrauterine fetal death(weeks)
28.3 (23.6–30.4)
Intrauterine fetal death(no.%)
7 (22.6%)
Birthweight (g) 590 (312–915)Neonatal death (no.%) 3 (9.6%)Total mortality (no.%) 10 (32.2%)Apgar score 5′ < 7 9/24 (37.5%)Respiratory support required 16/24 (66.6%)Intracerebral hemorrhagegrade III–IV
6/24 (25.0%)
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 1042–1047.DOI: 10.1002/pd

1044 G. RIZZO ET AL.
Table 2—Characteristics of the fetuses studied divided according to DV findings. Data are presented as median and range or nand %
DV end diastolicreverse flow
(no. 10)
DV end diastolicforward flow
(no. 21) Significance
Gestational age at Doppler examination (weeks) 25.4 (22.6–29.1) 26.3 (23.3–28.6) z = 0.90p = 0.363
Interval first Doppler examination delivery 4 (0–7) 14.3 (4–33) z = 3.61p = 0.0003
Intrauterine fetal death (no. %) 5/10 (50%) 2/21 (9.5%) p = 0.0218Birthweight (g) 475 (310–770) 630 (390–930) z = 2.813
p = 0.004Birthweight z score −4.5 (−2.5 to −6.3) −3.2 (−2.4 to −6.2) z = 1.85
p = 0.0063Apgar score 5′ < 7 (no. %) 2/5 (49%) 7/19 (36.8%) p = 0.9Respiratory support requirement (no. %) 4/5 (80%) 12/19 (63.1%) p = 0.14Intracerebral hemorrhage grade III–IV 2/5 (40%) 4/19 (21.0%) p = 0.568
(a)
(b)
Figure 1—Velocity waveforms obtained from the same fetusesobtained from (A) ductus venosus with reverse flow during atrialcontraction and from (B) aortic isthmus were reverse flow duringdiastole is also present
In 18 of the fetuses with DV forward end diastolicflow, a shift to reverse flow in DV was evidencedlater in pregnancy. The time interval between the firstDoppler recording and the onset of reverse flow in
(a)
(b)
Figure 2—Velocity waveforms obtained from the same fetuses in(A) ductus venosus showing normal flow pattern with anterogradeflow during end diastole and (B) from aortic isthmus in which theretrograde flow is evident
DV was significantly shorter in fetuses with retro-grade flow in AoI than in those with forward flow[AoI forward flow median 4 days (vs) AoI retrogradeflow 14 days z = 3.165 p = 0.0014]. This time interval
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 1042–1047.DOI: 10.1002/pd

AORTIC ISTHMUS AND DUCTUS VENOSUS IN IUGR FETUSES 1045
Table 3—Characteristics of the fetuses studied divided according to AoI findings. Data are presented as median and range or nand %
AoI reverse flow(no. 10)
AoI forward flow(no. 11) Significance
Gestational age at Doppler examination (weeks) 25.3 (23.3–28.1) 26.1 (23.7–27.9) z = 0.56p = 0.573
Interval first Doppler examination delivery 11.0 (4–18) 18.0 (4–33) z = 2.465p = 0.013
Intrauterine fetal death (no. %) 1/10 (10%) 1/11 (9.09%) p = 0.999Birthweight (g) 710 (570–930) 535 (390–675) z = 2.143
p = 0.031Birthweight z score −4.5 (−2.4 to −6.3) −4.6 (−2.5 to −6.2) z = 0.282
p = 0.778Apgar score 5′ < 7 4/9 (44.4%) 3/10 (30%) p = 0.649Respiratory support requirement (no. %) 6/9 (66.6%) 6/10 (60%) p = 0.99Intracerebral hemorrhage grade III–IV 2/9 (22.2%) 2/10 (20%) p = 0.99
resulted unrelated to gestational age at Doppler record-ings (constant 56.351, slope −1.842, residual standarddeviation (SD) 6.051, r = 0.262, p = 0.312), gestationalage at delivery (constant −19.856, slope 0.954, resid-ual SD 6.562, r = 0.178, p = 0.439), absolute birth-weight (constant −3.841 slope 0.019, residual 6.205r = 0.366, p = 0.102) and birthweight z score (constant15.611, slope 1.613, residual SD 6.454, r = 0.251, p =0.273). At the time of the onset of reverse flow in DVvelocity waveforms from AoI resulted always with ret-rograde flow.
Multivariate analysis demonstrated that the time inter-val between the first Doppler recordings and deliverywas related to the presence of reverse or forward flow inAoI (coefficient 6.419, standard error 1.907, p = 0.002)and to presence of reverse or forward flow in DV (coeffi-cient 7.284, standard error 2.045, p = 0.0015) but not togestational age at first Doppler examination (coefficient3.054, standard error 1.578, p = 0.0823), birthweight(coefficient 7.284, standard error 2.045, p = 0.0015) orbirthweight z score (coefficient 0.013, standard error0.009, p = 0.143). The multiple correlation coefficient(r2) was 0.372 (p < 0.0001).
DISCUSSION
These data describe the Doppler changes occurring inDV and AoI in severely IUGR fetuses from patientswithout any medical complication in pregnancy. Theresults obtained confirm previous reports that the pres-ence of reverse flow in DV is associated with a pooreroutcome IUGR when compared with matched pairs withanterograde end diastolic flow (Bilardo et al., 2004;Baschat et al., 2007). We further provide evidence thatabnormalities in AoI precede the occurrence of reverseflow in DV. This is supported first by the findings that inall the cases with pathological DV waveforms, studiedAoI was also abnormal and secondly by the longitudi-nal observation hereby obtained showing the progressionof hemodynamic modifications affecting first AoI andsubsequently DV. This observation confirms a previousreport from Del Rio et al. (2008) who found in four offive IUGR fetuses that reversed flow in the AoI was
present before the onset of reverse flow in DV. Animportant aspect of our observation is the intentionalexclusion from this study of pregnancies with medicalcomplications such as preeclampsia. These conditionsmay in fact abruptly change fetal hemodynamics (Mariet al., 2008) not allowing to properly follow, as we didin this study, the sequence of Doppler changes occurringin IUGR with progressive fetal deterioration.
A new interesting aspect resulting from this study isthe role of AoI in predicting the progression of Dopplerabnormalities in DV and the time of delivery. Indeedin IUGR fetuses with anterograde end diastolic flowin DV, a retrograde flow in AoI is associated witha significant reduction in the time interval before theonset of abnormal DV velocity waveforms as well aswith a shorter time interval to delivery when comparedwith fetuses with normal AoI flows, independently fromgestational age, birthweight and severity of IUGR.
Reverse flow in DV has been considered a usefulparameter for timing delivery of IUGR fetuses (Bilardoet al., 2004; Baschat et al., 2007). However DV abnor-malities occur usually close to severe fetal compromiseand earlier predictors allowing to identify fetuses atthe verge of compromise are desirable (Ghidini, 2007).To this end, the study of AoI velocity waveforms is apromising tool allowing a comprehensive study of thefetal circulation when peripheral resistances to ventricu-lar output are changed. Indeed during diastole, when theaortic and pulmonary valves are closed, the direction ofblood flow in AoI solely reflects the differences betweenthe downstream impedances of the right (mainly pla-cental vascular resistance) and left ventricles (mainlycerebral vascular resistance) (Fouron, 2003; Makikallio,2008). Under normal conditions, there is an anterogradeflow in AoI velocity waveforms as placental resistancesare lower than those of the fetal upper body. In presenceof IUGR, placental vascular resistances are increasedand this condition induces a redistribution of cardiacoutput with a prevalence of left ventricle output (Rizzoand Arduini, 1991; Hecher et al., 1995) due to changesin foramen ovalis shunting, pulmonary circulation andintrahepatic arterial and venous supply (Kiserud et al.,2004, 2006; Mari et al., 2008; Rizzo et al., 2008b) whichallow to maintain a positive pressure gradient across the
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 1042–1047.DOI: 10.1002/pd

1046 G. RIZZO ET AL.
AoI. As a consequence, the anterograde flow in velocitywaveforms is maintained during diastole. With progres-sive fetal deterioration, this compensatory mechanism isoverwhelmed and associated with retrograde flow duringdiastole in AoI. In this condition, blood with low oxy-gen content, such as that ejected from the right ventricle,is directed toward the heart and brain with subsequentsuboptimal oxygen delivery to these vital organs. Thepresence of a poorer neurodevelopmental outcome infetuses with abnormal AoI velocity waveforms whencompared with fetuses with normal AoI velocity wave-forms matched for gestational age underlines the impor-tance of this shift in AoI hemodynamics (Fouron et al.,2005; Del Rio et al., 2008).
Despite these evidences, the clinical use of AoI inthe monitoring of fetal deterioration in IUGR is so farlimited when compared to study of venous circulationwhere extensive studies have been conducted (Senatet al., 2000; Costa Carvalho et al., 2005; Baschat et al.,2007; Moreira de Sa et al., 2007). This limitation ismainly secondary to the difficulties in obtaining AoIvelocity waveforms from the conventional long axisview of the aortic arch particularly in presence ofsevere IUGR and reduced amniotic fluid volume. Thesedifficulties may be overcome by recording AoI velocitywaveforms from the three vessels trachea view of thefetal mediastinum as done in this study. Indeed, we andothers (Del Rio et al., 2005; Rizzo et al., 2008a) haverecently demonstrated how recordings from AoI can bereliably obtained from this latter plane in shorter timeand with a higher reproducibility that from the aorticarch view.
Of interest is the combined role of DV and AoI inthe prediction in the time interval from the first Dopplerrecordings resulting from the multivariate analysis per-formed in this study. This may suggest a combined roleof the study of both vessels in the monitoring of deteri-orating IUGR fetuses.
A limitation of this study is the relative low num-ber of subjects included. This is due to the strict cri-teria of inclusion that we followed and the relativelow incidence, present also in high-risk populations, ofearly severe IUGR without maternal complications thatrequired us more than 2 years to collect this study pop-ulation. Under these conditions caution is necessary ininterpreting the statistical results obtained and the lackof difference in the perinatal variables tested may besecondary to low number of cases included. This is par-ticularly important when the results of the multivariateanalysis were considered. Further prospective studies onlarger populations are therefore required to validate ourobservations.
In conclusion, our data suggest that in severely IUGRfetuses abnormalities in velocity waveforms occur ear-lier in AoI than in DV. The role of AoI as an additionalclinical parameter in the assessment of hemodynamicallycompromised IUGR fetuses deserves further evaluationin large prospective studies.
REFERENCES
Baschat AA. 2004. Fetal responses to placental insufficiency: anupdate. Br J Obstet Gynaecol 111: 1031–1041.
Baschat AA, Cosmi E, Bilardo CM, et al. 2007. Predictors of neonataloutcome in early-onset placental dysfunction. Obstet Gynecol 109:253–261.
Bellotti M, Pennatti G, De Gasperi C, Bozzo M, Battaglia FC,Ferrazzi E. 2004. Simultaneous measurements of umbilical venous,fetal hepatic, and ductus venosus blood flow in growth-restrictedhuman fetuses. Am J Obstet Gynecol 19: 1347–1358.
Bilardo CM, Wolf H, Stigter RH, et al. 2004. Relationship betweenmonitoring parameters and perinatal outcome in severe, earlyintrauterine growth restriction. Ultrasound Obstet Gynecol 23:119–125.
Costa Carvalho FH, Moron AM, Mattar R, et al. 2005. Ductusvenosus Doppler velocimetry in the prediction of acidemia at birth:which is the best parameter? Prenat Diagn 25: 1212–1216.
Del Rio M, Martinez JM, Figueras F, et al. 2005. Doppler assessmentof fetal aortic isthmus blood flow in two different sonographicplanes during the second half of gestation. Ultrasound ObstetGynecol 26: 170–174.
Del Rio M, Martinez JM, Figueras F, et al. 2008. Doppler assessmentof the aortic isthmus and perinatal outcome in preterm fetuses withsevere intrauterine growth restriction. Ultrasound Obstet Gynecol31: 41–47.
Fouron JC. 2003. The unrecognized physiological and clinicalsignificance of the fetal aortic isthmus. Ultrasound Obstet Gynecol22: 441–447.
Fouron JC, Gosselin J, Raboisson MJ, et al. 2005. The relationshipbetween an aortic isthmus blood flow velocity index and thepostnatal neurodevelopmental status of fetuses with placentalcirculatory insufficiency. Am J Obstet Gynecol 192: 497–503.
Ghidini A. 2007. Doppler of the ductus venosus in severe pretermgrowth restriction. A test in search of a purpose? Obstet Gynecol109: 250–251.
Hecher K, Snijders R, Campbell S, Nicolaides K. 1995. Fetal venous,intracardiac and arterial blood flow measurements in intrauterinegrowth retardation: relationship with fetal blood gases. Am J ObstetGynecol 173: 10–15.
Kiserud T, Chedid G, Rasmussen S. 2004. Foramen ovale changes ingrowth-restricted fetuses. Ultrasound Obstet Gynecol 24: 141–146.
Kiserud T, Kessler J, Ebbing C, Rasmussen S. 2006. Ductus venosusshunting in growth-restricted fetuses and the effect of umbilicalcirculatory compromise. Ultrasound Obstet Gynecol 28: 143–1499.
Makikallio K. 2008. Is it time to add aortic isthmus evaluation tothe repertoire of Doppler investigations for placental insufficiency?(Opinion) Ultrasound Obstet Gynecol 31: 6–9.
Makikallio K, Jouppila P, Rasanen J. 2003. Retrograde aortic isthmusnet blood flow and human fetal cardiac function in placentalinsufficiency. Ultrasound Obstet Gynecol 22: 351–357.
Mari GC, Hanif F, Kruger M. 2008. Sequence of cardiovascularchanges in IUGR in pregnancies with or without preeclampsia.Prenat Diagn 28: 377–383.
Moreira de Sa RA, Salomon LJ, Carvalho PNC, Lopes LM, Ville Y.2007. Predicting adverse neonatal outcome in severe fetalcompromise: A pivotal role for estimated fetal weight Z scores.Prenat Diagn 27: 1129–1132.
Papile LA, Burstein J, Burstein R, Koffler H. 1978. Incidence andevolution of subependymal and intraventricular hemorrhage∼: astudy of infants of birthweight less than 1500 gm. J Pediatr 92:529–534.
Parazzini F, Cortinovis I, Bortolus R, Fedele L. 1991. Standards ofbirth weight in Italy. Ann Ostet Ginecol Med Perinat 112: 203–246.
Pedhazur E. 1997. Multiple Regression in Behavioural Research:Explanation and Prediction (3rd edn). Harcourt Brace CollegePublishers: Fort Worth, TX.
Rizzo G, Arduini D. 1991. Fetal cardiac function in intrauterinegrowth retardation. Am J Obstet Gynecol 165: 876–882.
Rizzo G, Capponi A, Arduini D, Romanini C. 1994. Ductus venosusvelocity waveforms in appropriate and small for gestational agefetuses. Early Hum Dev 39: 15–26.
Rizzo G, Capponi A, Talone PE, Arduini D, Romanini C. 1996.Doppler indices from inferior vena cava and ductus venosusin predicting pH and oxygen tension in umbilical blood at
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 1042–1047.DOI: 10.1002/pd

AORTIC ISTHMUS AND DUCTUS VENOSUS IN IUGR FETUSES 1047
cordocentesis in growth retarded fetuses. Ultrasound ObstetGynecol 7: 401–410.
Rizzo G, Capponi A, Cavicchioni O, Pietrolucci ME, Arduini D.2008a. The use of the three vessel view to record Doppler velocitywaveforms from the aortic isthmus in normal and growth restrictedfetuses: comparison with the long axis long arch view. J UltrasoundMed 27: 1617–1622.
Rizzo G, Capponi A, Cavicchioni O, Vendola M, Arduini D. 2008b.Low cardiac output to the placenta: an early hemodynamic adaptive
mechanism in growth restriction. Ultrasound Obstet Gynecol 32:155–159.
Senat MV, Schwarzler P, Alcais A, Ville Y. 2000. Longitudinalchanges in the ductus venosus, cerebral transverse sinus andcardiotocogram in fetal growth restriction. Ultrasound ObstetGynecol 16: 19–24.
Copyright 2008 John Wiley & Sons, Ltd. Prenat Diagn 2008; 28: 1042–1047.DOI: 10.1002/pd