Rehabilitation and recovery from mental illness
40
Rehabilitation and Recovery from Mental Illness: “The Road Ahead” Alan S. Unis, M.D. Medical Director, Youth Services Kootenai Behavioral Health Center Coeur d’Alene, ID
-
Upload
alan-s-unis-md -
Category
Presentations & Public Speaking
-
view
78 -
download
1
Transcript of Rehabilitation and recovery from mental illness

Rehabilitation and Recovery from Mental Illness:
“The Road Ahead”
Alan S. Unis, M.D.Medical Director, Youth Services
Kootenai Behavioral Health CenterCoeur d’Alene, ID

Agenda
• Epidemiology of psychiatric disorders and their illness burden on individuals and society
• New societal commitments to address the problems of care delivery
• Promising research to advance evidence-based intervention outcomes that will mitigate clinical trajectories or prevent chronic mental illness.
• The road ahead . . .

The Facts . . .
• Point prevalence: Over 25% of adults experience a mental health disorder.– 1 in 17 suffers from a serious mental illness such
as schizophrenia, major depression or bipolar disorder.
– 1 in 10 children live with a serious emotional disorder such as autism, attention deficit disorder or anxiety disorders.

I. Economic Burden: Indirect Costs
• The annual indirect costs of mental illness is estimated to be $79 billion (2001 figures).– Lost productivity: $63 billion.– Incarceration: 20% of adult prisoners and 70% of
adolescent detainees.– Unemployment: 70% of the chronically mentally ill
are unemployed.– Under education: 50% high school drop out rate,
the highest of any disability group.

II. Economic Burden: Direct Costs
Sources of coverage for direct costs from hospitalization, outpatient and alternative treatment settings: In 1997, the United States spent more than $1 trillion on health care, but only $71 billion on treating mental illnesses.

III. Economic Burden: Lost productivity
• Mental disorders, alcohol and drug abuse disorders and dementias are the leading 3 causes of disability for all ages combined in the US, Canada and western Europe.

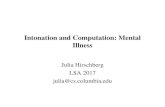
Suicide Is the Leading Cause of Violent Deaths Worldwide:

Percentage of High School Students Whose Suicide Attempt Resulted in an Injury, Poisoning, or an Overdose That Had to Be Treated by a Doctor or Nurse,*
1991 – 2009†
1991 1993 1995 1997 1999 2001 2003 2005 2007 20090
20
40
60
80
100
1.7 2.7 2.8 2.6 2.6 2.6 2.9 2.3 2.0 1.9
Perc
ent
* During the 12 months before the survey.† No change 1991–2003, decreased 2003–2009, p < 0.05.
National Youth Risk Behavior Surveys, 1991–2009

IV. Economic Burden: Suicide• In the U.S., suicide claims approximately 30,000 lives each year. • Overall, suicide was the 11th leading cause of death among Americans in
2000. • In 1999, more than 152,000 hospital admissions and more than 700,000
visits to hospital emergency rooms were for self-harming behaviors.• The vast majority of all people who die by suicide have a mental illness
— often undiagnosed or untreated.• Suicide was also the fourth leading cause of death among youth aged
10-14, third among those between 15 and 24, second among 25- to 34-year olds, and fourth among those 35-44 years in 1999.
• The rate of suicide is highest among older men, compared with all other age groups. But alarmingly, the rate of teen suicide (for those from ages 15 to 19) has tripled since the 1950’s.

V. Economic Burden: Fragmented Systems of Care
• While each program provides essential assistance, together they create a financing approach that is complex, fragmented, and inconsistent in its coverage:
– State and local general fund appropriations,– Medicare, – Social Security (Social Security Income/Social Security and Disability Income
payments), – Vocational rehabilitation, – Education, – Temporary Assistance for Needy Families (TANF), – Juvenile justice and criminal justice, – Child welfare, and – Federal block grants.

The President’s New Freedom Commission on Mental Health (July, 2003) defined recovery as:
• “… the process in which people are able to live, work, learn and participate fully in their communities. For some individuals, recovery is the ability to live a fulfilling and productive life despite a disability.
• For others, recovery implies the reduction or complete remission of symptoms.
• Science has shown that having hope plays an integral role in an individual's recovery.”

Challenges to Recovery
• Stigma that surrounds mental illnesses,• Treatment limitations and financial
requirements placed on mental health benefits in private health insurance, and
• The fragmented mental health service delivery system.

Recovery is not a partisan issue:
• President Bush said,“… Americans must understand and send this message: mental
disability is not a scandal — it is an illness. And like physical illness, it is treatable, especially when the treatment comes early.”
• President Obama said,“. . . somebody who has severe depression has a more debilitating and dangerous illness than somebody who's got a broken leg. But a broken leg, nobody argues that's covered. Severe depression, unfortunately, oftentimes isn't even under existing insurance policies.”

Recovery is not a scientific issue:
• In the Institute of Medicine report, Crossing the Quality Chasm: A New Health System for the 21st Century, the lag between discovering effective forms of treatment and incorporating them into routine patient care is unnecessarily long, lasting about 15 to 20 years.

Recovery is an implementation issue:
• “Today not only is there a shortage of providers, but those providers who are available are not trained in evidence-based and other innovative practices. This lack of education, training, or supervision leads to a workforce that is ill-equipped to use the latest breakthroughs in modern medicine.”

In a Transformed Mental Health System …
• GOAL 1: Americans Understand that Mental Health Is Essential to Overall Health.
• GOAL 2: Mental Health Care Is Consumer and Family Driven.
• GOAL 3: Disparities in Mental Health Services Are Eliminated.
• GOAL 4: Early Mental Health Screening, Assessment, and Referral to Services Are Common Practice.
• GOAL 5: Excellent Mental Health Care Is Delivered and Research Is Accelerated.
• GOAL 6: Technology Is Used to Access Mental Health Care and Information.

Transformation Endpoints:• In a transformed system, consumers and family members will have
access to timely and accurate information that promotes learning, self-monitoring, and accountability.
• Effective mental health treatments will be more readily available for most common mental disorders and will be better used in primary care settings.
• Primary care providers will have the necessary time, training, and resources to appropriately treat mental health problems.
• Informed consumers of mental health service will learn to recognize and identify their symptoms and will seek care without the fear of being disrespected or stigmatized.

GOAL 1: Americans Understand that Mental Health Is Essential to Overall Health.
• Understanding that mental health is essential to overall health is fundamental for establishing a health system that treats mental illnesses with the same urgency as it treats physical illnesses.
– 1.1 Advance and implement a national campaign to reduce the stigma of seeking care and a national strategy for suicide prevention.
– 1.2 Address mental health with the same urgency as physical health.

GOAL 2: Mental Health Care Is Consumer and Family Driven:
• The plan of care will be at the core of the consumer-centered, recovery-oriented mental health system.
– 2.1 Develop an individualized plan of care for every adult with a serious mental illness and child with a serious emotional disturbance.
– 2.2 Involve consumers and families fully in orienting the mental health system toward recovery.
– 2.3 Align relevant Federal programs to improve access and accountability for mental health services.
– 2.4 Create a Comprehensive State Mental Health Plan.
– 2.5 Protect and enhance the rights of people with mental illnesses.

GOAL 3: Disparities in Mental Health Services Are Eliminated.
• In a transformed mental health system, all Americans will share equally in the best available services and outcomes, regardless of race, gender, ethnicity, or geographic location.
– 3.1 Improve access to quality care that is culturally competent.
– 3.2 Improve access to quality care in rural and geographically remote areas.

GOAL 4: Early Mental Health Screening, Assessment, and Referral to Services Are Common Practice.
• For consumers of all ages, early detection, assessment, and links with treatment and supports will help prevent mental health problems from worsening.
– 4.1 Promote the mental health of young children.
– 4.2 Improve and expand school mental health programs.
– 4.3 Screen for co-occurring mental and substance use disorders and link with integrated treatment strategies.
– 4.4 Screen for mental disorders in primary health care, across the lifespan, and connect to treatment and supports.

GOAL 5: Excellent Mental Health Care Is Delivered and Research Is Accelerated.
• Research discoveries will become routinely available at the community level.
– 5.1 Accelerate research to promote recovery and resilience, and ultimately to cure and prevent mental illnesses.
– 5.2 Advance evidence-based practices using dissemination and demonstration projects and create a public-private partnership to guide their implementation.
– 5.3 Improve and expand the workforce providing evidence-based mental health services and supports.
– 5.4 Develop the knowledge base in four understudied areas: mental health disparities, long-term effects of medications, trauma, and acute care.

GOAL 6: Technology Is Used to Access Mental Health Care and Information.
• The privacy of personal health information — especially in the case of mental illnesses — will be strongly protected and controlled by consumers and families.
– 6.1 Use health technology and telehealth to improve access and coordination of mental health care, especially for Americans in remote areas or in underserved populations.
– 6.2 Develop and implement integrated electronic health record and personal health information systems.

Summary
• When a serious mental illness or a serious emotional disturbance is first diagnosed, the health care provider — in full partnership with consumers and families — will develop an individualized plan of care for managing the illness.
• This partnership of personalized care means basically choosing who, what, and how appropriate health care will be provided:– Choosing which mental health care professionals are on the team,– Sharing in decision making, and– Having the option to agree or disagree with the treatment plan.

Summary
• Good mental health can have a positive impact on the course of other illnesses, such as cancer, heart disease, and diabetes.
• Improving services for individuals with mental illnesses will require paying close attention to how mental health care and general medical care systems work together.
• While mental health and physical health are clearly connected, the transformed system will provide collaborative care to bridge the gap that now exists.

Neurodevelopmental Models of Early-Onset Psychopathology: Opportunities for Prevention and/or Intervention
• A sensitive period is when the impact of experience is particularly strong over a limited time. – The developmental path is malleable and constantly influenced by
numerous interacting external and internal influences (genetic, hormonal, behavioral, environmental, etc.).
• A critical period is the time over which experience can change the state of a developing system, after which fundamental alterations can no longer occur. – Neurodevelopment is a multifaceted, dynamic process that involves
gene-environment interactions resulting in both short- and long-term changes in gene expression, cellular interactions, circuit formation, neural structures and behavior over time. A target that may be present at one moment in time may be absent at another.

Risks and Limitations
• Absent specific mechanism-based understanding of the disorder under study, most prevention or intervention strategies are inefficient, but are not without effect or benefit.
• Most empirical interventions take advantage of normal learning and brain development in the broadest sense.

Lessons from Fetal Alcohol Spectrum Disorders
• General education or training.
• Teaching specific skills typically expected to be learned by observation or abstraction.
• Integration into existing systems of treatment.
Bertrand, et al. (2009);Peadon et al. (2009)

Evidence-Based Interventions
• Autism and Developmental Disorders• Attention Deficit Disorder and other disruptive
behavior disorders• Mood Disorders: Major Depression and
Bipolar Disorder• Obsessive-Compulsive Disorder• Schizophrenia

Autism
*DSM-IV TR. Washington, DC: American Psychiatric Association; 2000.
Autism is characterized by deficits in 3 core areas.At least 6 items are needed for diagnosis*
• Marked impairment in multiple nonverbal behaviors
• Failure to have developmentally appropriate peer relationships
• Lack of showing, bringing, or pointing out objects of interest
• Lack of social or emotional reciprocity
• Delay in, or total lack of, development of spoken language
• Marked impairment in ability to initiate or sustain conversation
• Stereotyped and repetitive use of language, or use of idiosyncratic language
• Lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level
• Preoccupation with 1/more stereotyped and restricted patterns of interest that are abnormal in intensity or focus
• Apparently inflexible adherence to specific, nonfunctional routines or rituals
• Stereotyped and repetitive motor mannerisms
• Persistent preoccupation with parts of objects
Social Interaction: Communication: Behavior:

Examples of treatments for core symptoms of autism spectrum disorder
• Socialization– Educational curricula
• Treatment and education of autistic and related communication handicapped children (TEACCH), strategies for teaching based on autism research (STAR), parent training, and inclusion with trained shadow
• Communication and language– Didactic and intensive training, and Milieu teaching
• Social-skills training– Social skills training and social stories
• Behavioral treatment – Discrete trial instruction, pivotal response training, and relationship development intervention
• Communication• Communication intervention
– Within a comprehensive program (eg, pivotal response training, or other centre), social pragmatics approach, and parent training
– Augmentative and assistive communication– Picture exchange communication system, sign language, and assistive technology (eg, vocal output devices)– Behavioural (eg, play, reciprocal communication)– Floor time/developmental, individual differences, relationship-based approach, applied verbal behavior
• Educational– TEACCH, STAR
• Behaviour– Behavioural intervention– Discrete trial instruction, and other comprehensive programmes using applied behaviour analysis

Complementary and Alternative Medical Treatments
• Biological– Supplements—eg, vitamin B6
or magnesium ion, dimethyl glycine, and cod-liver oil)
– Anti-infectives—eg, antibiotics, antifungals, and antivirals
– Immunoglobulins– Off-label drugs—eg, secretin– Chelation medications– Gastrointestinal medications– Elimination or special diets—eg,
gluten free or casein free– Hyperbaric oxygen
administration
• Non-biological– Auditory integration
training– Chiropractic therapy– Craniosacral manipulation– Facilitated communication– Massage and qigong– Interactive metronome– Reiki– Transcranial stimulation– Yoga

Attention Deficit Disorder
• Nonspecific clinical phenotype with variable causes, clinical course and/or outcome.
• Some common neural areas consistently involved.
• Indicative of future risk of psychopathology

ADHD Developmental Risk Trajectory
LDDevelopmental Delay
ODDCD
ASP
SA Mortality/Morbidity
Enhancing Good Outcomes with Disruptive Behavior Disorders and Substance Abuse
7-10 yr 12-16 yr 18-20 yr
TS Mood Bipolar Schiz
Oth
er p
rove
n tr
eatm
ents
Developmental Decay
Continuous Display
Mortality/Morbidity

Trajectories of physical aggression from 17 to 42 months of age.

Right Prefrontal Activation Predicts Response to Special Instruction
Mood Disorders
• Bipolar disorder
• Major Depressive disorder
• Dysthymic disorder

Beyond Drugs and Cognitive Psychotherapy
• Exercise– Stress management
• Diet• Nutritional supplementation
– Fish oil– B vitamin complex– Vitamin D
• Life skills/Time management

Schizophrenia
• Indications of neurodevelopmental “lesion”.• Insidious onset: two-year average prodromal
phase.• Psychosis (hallucinations and delusions) and
disordered thinking.• Protracted convalescent phase with
pronounced residual psychological and social deficits.

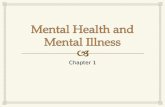
Schematic exaggerating the putative cytoarchitectural features of schizophrenia.
Harrison P J Brain 1999;122:593-624
© Oxford University Press 1999