Regionalization : A New Strategy for TB Control & Elimination The New England Experience
29
Regionalization: A New Strategy for TB Control & Elimination The New England Experience Mark Lobato, M.D. Division of Tuberculosis Elimination Centers for Disease Control and Prevention Advisory Committee for the Elimination of TB Atlanta, GA March 3-4, 2009
description
Regionalization : A New Strategy for TB Control & Elimination The New England Experience Mark Lobato, M.D. Division of Tuberculosis Elimination Centers for Disease Control and Prevention. Advisory Committee for the Elimination of TB Atlanta, GA March 3-4, 2009. Connecticut - PowerPoint PPT Presentation
Transcript of Regionalization : A New Strategy for TB Control & Elimination The New England Experience

Regionalization:A New Strategy for
TB Control & EliminationThe New England Experience
Mark Lobato, M.D.Division of Tuberculosis Elimination
Centers for Disease Control and Prevention
Advisory Committee for the Elimination of TB
Atlanta, GA March 3-4, 2009

New England TB ConsortiumConnecticutLynn Sosa, Heidi Jenkins,Tom Condren, MaureenWilliams, Gary Budnick,James Hadler, CACET
MaineDiane Brooks, Kathy Gensheimer, Joyce Roy,Julie Crosby
MassachusettsSue Etkind, Kathy Hursen,Sharon Sharnprapai, Marilyn DelValle, John Bernardo, Janice Boutotte, Alex Sloutsky, MACET
New HampshireJill Fournier, Lisa Roy,Jody Smith, Peggy Sweeny
Rhode IslandUtpala Bandy, Mike Gosciminski, Paula Pullano, Toby Bennett
VermontSusan Shoenfeld, Susan Cook,Becky Temple
RTMCCNicolette Patrick
DTBEDan Ruggiero, Kashef Ijaz, PatrickMoonan, Maria Fraire, Ken Castro

RegionalizationThe Time Has Come
• Orients to field-based interventions– Rapid response to problems– Increases program capacity– Promotes federal-state cooperation
• Attempts to improve program effectiveness
• Reflects a changing relationship between DTBE and the states

The Perfect Storm The Next TB Upsurge
• Flat funding• Weakened public
health infrastructure• Loss of TB expertise• Ongoing immigration• Continued outbreaks• Few new diagnostics
and drugs

“In the middle of difficulty, lies opportunity.” – Albert Einstein

New England TB, 2007
• TB cases- 408 cases- 3.0 / 100,000
(range 0.5–4.3)- 67% among FB
• Equivalent to state with 8th highest TB burden
Kent
Sharon
StaffordSalisbury
Lebanon
Newtown Lyme
Goshen
Norfolk
Litchfield
Killingly
Woodstock
Guilford
Granby
Haddam
Suffield
TollandPomfret
Danbury
Cornwall
Hebron
New Milford
Ashford
Ledyard
Union
Salem
Enfield
Colchester
Oxford
Groton
Thompson
Mansfield
Montville
Greenwich
Plainfield
Canaan
Avon
Berlin
Preston
East Haddam
Glastonbury
EastonMadison
Shelton
Stamford
Coventry
Wilton
Griswold
Bristol
Hamden
Hartland
Southbury
Somers
Torrington
Redding
Warren
Cheshire
Ellington
Windsor
Voluntown
Stonington
Simsbury
Canterbury
Fairfield
MiddletownWoodbury
Canton
Eastford
Waterford
Sterling
Wallingford
Norwich
Monroe
Ridgefield
Washington
North Stonington
Willington
Colebrook
Brooklyn
Roxbury
Winchester
Southington
Milford
Barkhamsted
Harwinton
Durham
Portland
Windham
Meriden
Burlington
Bozrah
Weston
Waterbury
Morris
Hampton
New Hartford
WatertownWolcott
Putnam
Sherman
Norwalk
Bethel
Bethany
Trumbull
Vernon
Chaplin
Old Lyme
Farmington
Branford
Lisbon
Manchester
Orange
Franklin
Bloomfield
Westport
Columbia
Chester
Clinton
BoltonHartford
Essex
East Windsor
South Windsor
Darien
Bethlehem Sprague
Prospect
Seymour
Naugatuck
Cromwell
East LymeKillingworth
East Hampton
Plymouth
Scotland
Stratford
BrookfieldNew Fairfield
Andover
Marlborough
New Canaan
North BranfordNorth Haven
New Haven
West Hartford
Woodbridge
Middlebury
Bridgeport
Westbrook
East Granby
Bridgewater
North Canaan
East Hartford
Rocky Hill
Deep River
Newington
Old Saybrook
Middlefield
East Haven
New BritainThomaston
Wethersfield
Plainville
West Haven
Derby
Beacon Falls
Ansonia
Windsor Locks
New London
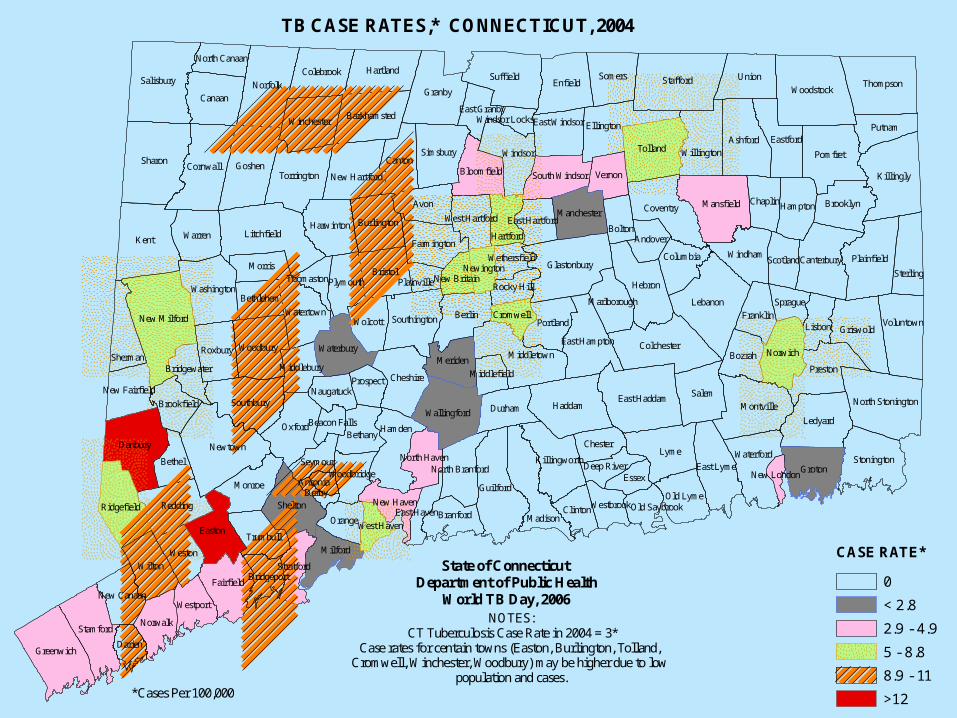
TB CASE RATES,* CONNECTICUT, 2004
*Cases Per 100,000
NOTES:CT Tuberculosis Case Rate in 2004 = 3*
Case rates for centain towns (Easton, Burlington, Tolland, Cromwell, Winchester, Woodbury) may be higher due to low
population and cases.
CASE RATE*
0
< 2.8
2.9 - 4.9
5 - 8.8
8.9 - 11
>12
State of ConnecticutDepartment of Public Health
World TB Day, 2006

“So, why did you do it?”

Value Added
New England TB.org

New England TB Consortium Collaboration for Change
• Leadership• Education
– TB Talk– Eliminating TB Case by Case
• Communication• Genotyping• Public Health Law• Awards

Interactive Web PresentationJune 24, 2008
Noon
Accreditation: CME, CNE, CHES
“TB testing using QuantiFeron Gold:What the provider needs to know”
Eliminating TB Case by CaseA Case Series for Providers and Clinicians
Nira Pollock, MD, PhDDivision of Infectious Diseases,
Beth Israel Deaconess Medical Center, Boston
Access the TB Case Series atwww.mymeetings.com/nc/join.php?i=PG1678747&p=2006&t=c
Toll free audio access: 888 -552 -9191 Password = 2006 #
Eliminating TB Case by Case
• Presented by master clinicians• Designed to reach private providers• Created basis for distance learning
– web-based– continuing education credit
• Need for ongoing marketing“People love the case presentations.Since we are very rural, and we can’t goout of state for training, this is a greatopportunity.” - Consortium stakeholder

TB Talk – New England A case discussion by and for nurses, outreach
educators, and case management staff
January 13, 2009 12:00 – 1:00 pm John Bernardo, M.D., Boston University
“Ask the Expert”Lloyd Friedman, M.D. (Pulmonary), Milford Hospital, Yale
Joseph Gadbaw, Jr., M.D. (ID), Lawrence & Memorial HospitalRobert Husson, M.D. (Pediatrics), Childrens Hospital Boston
Phone: 866-774-8920 Passcode: 8612841#
New Engl andTB ConsortiumConnecticut M aine M assachusetts New Hampshire Rhode I sl and Vermont
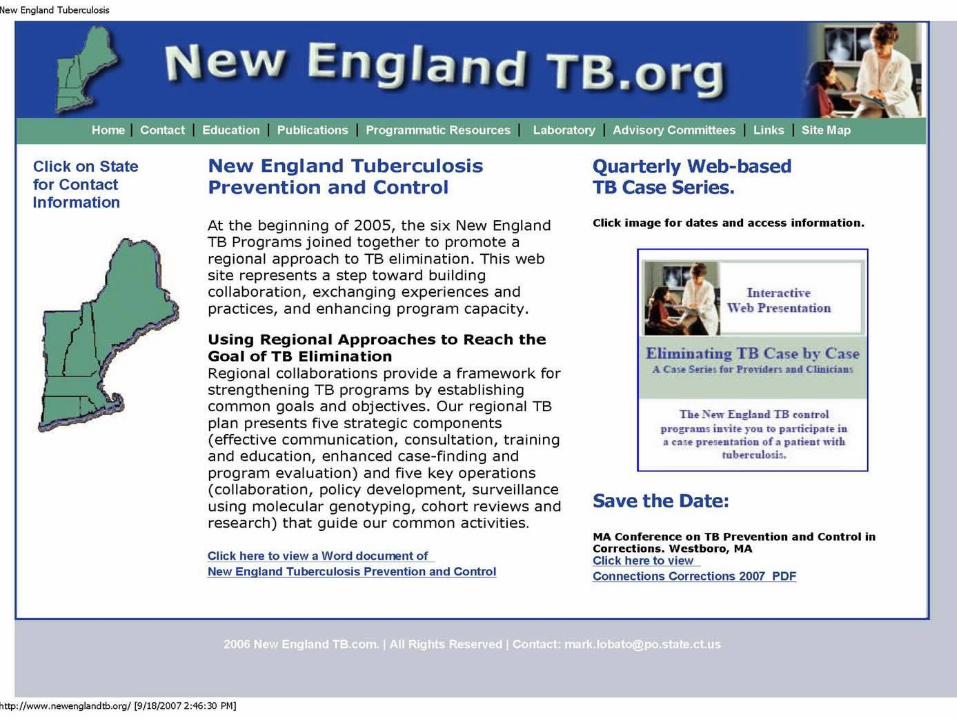

NewEnglandTB.org
• Built a website– To increase cohesiveness and visibility– To promote regional and state education– To exchange tools and materials
• Partnered with HHS Region I (wiki)

Genotyping Work Group
• Defined data management capacity• Identified instances of interstate
transmission in 2 clusters• Highlighted missed opportunities• Measured strain dispersion across
states “The genotyping calls are an opportunity to exchange information and to feel we are not in a vacuum… It is hard when you are in a void.”- Consortium stakeholder
Consultation
• Early detection of an outbreak and need for a CDC investigative team
• Facilitated technical support for 3 large contact investigations
• Performed on average 7 consultations for CIs and 20 for complex cases per year

New England Public Health Law Project
• Call to Action sent to NTCA• Addresses gap in Model TB Act• Formed a broad partnership• Defining options for involuntary
isolation of patients from another state• Applied for CDC award “Innovations in
Public Health Policy”

TB Heroes Award
• To recognize exceptional contributions to TB control and the well-being of patients and the community
• First annual award presented at the 2008 northeast TB meeting
• Article in current TB Notes

Call for nominations
New
TBEngland
Heroes
New England TB Heroes Award
In recognition of an exceptional contribution to TB control and the well-being of patients and the community
Please send nominations to your TB program by April 1st
Presented by the New England TB Consortium

PCSI• The best programs are the best
collaborators• Beginning collaboration between TB
and STD• TB Notes (2008)

Lab Collaboration
• 5 states using uniform lab survey• Questions regarding lab capacity and
practices• Marketing tool
Dissemination• Presentations
– NTCA (plenary): 2008– NTCA (posters): 2008 (“TB Talk” - D. Orcutt)
2007 (Regionalization), 2006 (Education)– ATS: 2007 (Genotyping)– IUTLD: 2008 (Isolation - Gensheimer; Regionalization)– TB ETN: 2009 (Education)– Northeast TB Conference: 2005, 2006, 2007– DTBE Brown Bag: 2006, 2009
• Publications– TB in the foreign born (Lobato, et al.)– Prison outbreak in CT (Sosa, et al.)– Community outbreak (Buff, et al.)– TB Notes:
• 2009 (TB Heroes – New England)• 2008 (PCSI)• 2007 (Regionalization)• 2006 (Education)

Evaluation of the NETC• Carried out by Maureen Wilce, DTBE• To determine the factors promoting or
hindering this regionalization effort• Results
– Created a formal framework with a consensus plan of action
– Provided a structure for all voices to be heard equally
– Facilitated the sharing of knowledge and resources– Found resource limitations that limit program staff
from optimizing involvement
Evaluation Conclusion
The New England TB Consortium “provides a model for building consensus through strategic planning [and] establishing formal agreements”
“Regional assignees can be effective to promote regionalization, providing skills and resources as incentives to promote collaborative efforts.”

Lessons Learned
• Modern TB control requires– Building a team leadership– Coordination and collaboration across
jurisdictions• Regional efforts enhance programs• Regionalization offers advantages CDC
“The conference calls are comfortable and supportive… I found we are all struggling with the same issues.”- Consortium stakeholder

Next Steps
• Hold a leadership retreat– Improve collaborative efforts– Update the strategic plan– Examine how to replicate model
• Extend the model to labs and refugee coordinators
• Enhance resources for treating complex or non-adherent patients

Future Outlook
• Extend the model nationally
• Strategic placement of TB staff

Prepare, you’ll sleep better…


















