
Libri TresDe Facultatum Naturalium Substantia Quod Animi ...

ARTICLE OPEN ACCESS
Regional microglial activation in the substantianigra is linked with fatigue in MSTarun Singhal MD Steven Cicero BS Hong Pan PhD Kelsey Carter BS Shipra Dubey PhD Renxin Chu PhD
Bonnie Glanz PhD Shelley Hurwitz PhD Shahamat Tauhid MD Mi-Ae Park PhD Marie Kijewski DSc
Emily Stern MD Rohit Bakshi MD MA David Silbersweig MD and Howard L Weiner MD
Neurol Neuroimmunol Neuroinflamm 20207e854 doi101212NXI0000000000000854
Correspondence
Dr Singhal
tsinghalbwhharvardedu
AbstractObjectiveThe goal of our study is to assess the role of microglial activation in MS-associated fatigue(MSAF) using [F-18]PBR06-PET
MethodsFatigue severity was measured using the Modified Fatigue Impact Scale (MFIS) in 12 subjectswith MS (7 relapsing-remitting and 5 secondary progressive) and 10 healthy control partici-pants who underwent [F-18]PBR06-PET The MFIS provides a total fatigue score as well asphysical cognitive and psychosocial fatigue subscale scores Standardized Uptake Value (SUV)60ndash90 minute frame PET maps were coregistered to 3T MRI Voxel-by-voxel analysis usingStatistical Parametric Mapping and atlas-based regional analyses were performed SUV ratios(SUVRs) were global brain normalized
ResultsPeak voxel-based level of significance for correlation between total fatigue score and PETuptake was localized to the right substantia nigra (T-score 467 p = 0001) Similarly SUVRsderived from atlas-based segmentation of the substantia nigra showed significant correlationwith MFIS (r = 076 p = 0004) On multiple regression the right substantia nigra was anindependent predictor of total MFIS (p = 002) and cognitiveMFIS subscale values (p = 0007)after adjustment for age disability and depression Several additional areas of significantcorrelations with fatigue scores were identified including the right parahippocampal gyrusright precuneus and juxtacortical white matter (all p lt 005) There was no correlation betweenfatigue scores and brain atrophy and lesion load in patients with MS
ConclusionSubstantia nigra microglial activation is linked to fatigue in MS Microglial activation across keybrain regions may represent a unifying mechanism for MSAF and further evaluation of neu-roimmunologic basis of MSAF is warranted
From the Partners MS Center (TS SC KC BG RB HLW) Ann Romney Center for Neurological Diseases Department of Neurology Brigham and Womenrsquos Hospital HarvardMedical School Boston MA PET Imaging Program in Neurologic Diseases (TS SC KC) Ann Romney Center for Neurological Diseases Department of Neurology Brigham andWomenrsquos Hospital Harvard Medical School Boston MA Functional Neuroimaging Laboratory (HP RB DS) Department of Psychiatry Brigham and Womenrsquos Hospital HarvardMedical School Boston MA Division of Nuclear Medicine and Molecular Imaging (SD M-AP MK) Department of Radiology Brigham and Womenrsquos Hospital Harvard MedicalSchool Boston MA Laboratory for Neuroimaging Research (RC ST) Ann Romney Center for Neurological Diseases Department of Neurology Brigham and Womenrsquos HospitalHarvardMedical School Boston MA Department of Medicine (SH) Brigham andWomenrsquos Hospital HarvardMedical School BostonMA Ceretype Neuromedicine (ES)Departmentof Radiology (RB) Brigham and Womenrsquos Hospital Harvard Medical School Boston MA
Go to NeurologyorgNN for full disclosures Funding information is provided at the end of the article
The Article Processing Charge was funded by the authors
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 40 (CC BY-NC-ND) which permits downloadingand sharing the work provided it is properly cited The work cannot be changed in any way or used commercially without permission from the journal
Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 1
Defined as an overwhelming sense of tiredness lack of energyor feeling of exhaustion12 fatigue is reported as the mostdisabling symptom in up to 60 of patients with MS3 and isestimated to have a lifetime prevalence of 804 Moreoverthe prevalence of fatigue increases with disease progression(46 in patients with clinically isolated syndrome [CIS] and80 in patients with secondary progressive MS [SPMS])5
Importantly fatigue has been described as the leading cause ofabsence from work in MS6 Fatigue may also have prognosticimplications in patients with MS For example in patientswith CIS up to 46 of patients may present with fatiguewhich has recently been shown to predict conversion toclinically definite MS7 Among patients with relapsing-remitting MS (RRMS) fatigue scores were higher in pa-tients who converted to a confirmed Expanded DisabilityStatus Scale (EDSS) score ge3 after at least 3 years of follow-upcompared with nonconverters This association remainedsignificant after adjusting for depression scales and baselineEDSS8 Despite the high prevalence and significance of fatiguein MS its anatomic and physiologic substrate and its mech-anism are not clear
Inflammation is proposed as a potential mechanism for fa-tigue in MS but has the lack of sufficient evidence3 Abnor-malities in functional connectivity of the resting default modenetwork have been linked with fatigue in MS9 However thebiological processes underlying these abnormalities are notknown
Microglial activation may play a role in the pathogenesis ofMS1011 but it has not been systematically studied in relationto MS-associated fatigue (MSAF) [F-18]PBR06 is a second-generation longer half-life PET radioligand targeting the18-kDa translocator protein for noninvasive assessment of ce-rebral microglial activation that we have recently reported to beincreased in subcortical gray matter and normal-appearingwhite matter in MS12ndash17 Our aim is to assess the role ofmicroglial activation in MSAF using [F-18]PBR06 PET
MethodsParticipantsParticipants were recruited from the Partners Multiple Scle-rosis Center at the Brigham and Womenrsquos Hospital andthrough an online recruitment portal for healthy controlparticipants (HCs) Initially 18 participants with MS and 12HC participants were consecutively enrolled Two
participants with MS and 2 HC participants were low-affinitybinders and were excluded from the study (see the Geno-typing section below) Four additional patients with MSsubsequently changed their minds about participating in thestudy or were lost to follow-up following consent Twelvepatients with MS (5 SP and 7 RR 8 women and 4 men) and10 HC participants (4 women and 6 men) completed thestudy Table 1 contains a summary of characteristics for allstudy participants and table 2 contains detailed individualizedparticipant characteristics Our findings regarding the re-lationship of the [F-18]PBR06 PET scans from these patientswith MS with disability and brain atrophy were previouslyreported16
In terms of the inclusion criteria we included patients withSPMS if they experienced a worsening of their EDSS score byat least 05 (if their baseline EDSS score was ge55) or at least10 (if their baseline EDSS score was lt5) over a period of 1year before PET scanning In addition we included patientswith RRMS who had a relapse or if there was evidence of anew or enlarging T2 bright lesion on MRI or a gadolinium-enhancing lesion on T1-weighted MRI in the last year Pa-tients who were treated with corticosteroids during a period of1 month before the PET scan were excluded PET scanningwas performed within a median time interval of 51 (range11ndash256) weeks in relation to the subjectsrsquo clinical assess-ment Patients did not experience a relapse between theclinical and PET imaging visits
Standard protocol approvals registrationsand patient consentsThe clinicaltrialsgov ID for our study is NCT02649985 Thestudy was approved and overseen by the Institutional ReviewBoard Radiation Safety Committee and Radioactive DrugResearch Committee at our hospital Written informed consentwas obtained from all study participants before participation
GenotypingBlood samples were collected during the initial visits andgenotyping was performed for screening purposes Geno-typing used a TaqMan assay to identify the DNA poly-morphism of the translocator protein (TSPO) gene onchromosome 22q132 Study participants with high-affinity(HAB) and medium-affinity binding (MAB) were included inthe study whereas ones with low-affinity binding were ex-cluded Among the 12 patients with MS who completed thestudy 7 were HABs and 5 were MABs Among the HC par-ticipants 6 were HABs and 4 were MABs (table 1) The
GlossaryAAL = automated anatomic labeling BPV = brain parenchymal volume CFS = chronic fatigue syndrome CIS = clinicallyisolated syndrome DMN = default mode network EDSS = Expanded Disability Status Scale ES = effect size HAB = high-affinity bindingHC = healthy controlHDRS = Hamilton Depression Rating ScaleMAB = medium-affinity binding RRMS =relapsing-remitting MS SN = substantia nigra SPM = Statistical Parametric Mapping SPMS = secondary progressive MSTSPO = translocator protein
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
proportion of HABs andMABs in theMS and HC groups wasnot significantly different (table 1)
Radiopharmaceutical productionWe have previously described the radiopharmaceutical pro-duction methodology at our center16
MRI acquisition and corresponding analysisEach study participant completed an MRI scan on the samescanner (Siemens 3T Skyra Erlangen Germany) according to apreviously described acquisition protocol18ndash20 The protocolincluded a 2D T1-weighted spin-echo axial series (repetitiontime = 611ndash943ms echo time = 79 ms and voxel size = 043 times043 times 3mm3) and a 3D fluid-attenuated inversion recovery andmagnetization-prepared rapid gradient-echo series (voxel sizesfor both 1 times 1 times 1mm3) Using a previously reported techniquenormalized whole-brain parenchymal volume (BPV) was de-rived by applying the latter images to a fully automated algo-rithm (SIENAX v 50 Analysis Group fslfmriboxacuk)21
Hyperintense lesions on 3D T2 FLAIR and hypointense le-sions on T1-weighted spin-echo images were marked by atrained observer (KC) and verified by a senior observer(ST or TS) We determined that to qualify as a T1 hypo-intense lesion the lesion had to be both hypointense onT1-weighted images and hyperintense on Fluid AttenuationInversion Recovery (FLAIR) images2223 A semiautomatededge-finding tool was then used for volumetric lesion con-touring using Jim (version 7 Xinapse Systems West BergholtUnited Kingdom xinapsecom) Our previous work has shownhigh reliability for this semiautomated method of measuringMS cerebral lesion burden2223
PET acquisition and corresponding analysis[F-18]PBR06 was injected as a bolus injection for PET scan-ning using an IV catheter into an arm or hand vein images were
acquired in a list mode acquisition mode using a high-resolution PETCT scanner (GEDiscovery ECATWaukeshaWI) Statistical Parametric Mapping (SPM) was used as theprimary analysis technique for this study SPM12 software (theWellcome Institute of Cognitive Neurology London UnitedKingdom filionuclacukspmsoftware) was used to processthe [F-18]PBR06 PET SUV images24 PET images were ster-eotactically normalized to the Montreal Neurologic Instituteversion of Talairach space Whole-brain multiple linear re-gression modeling of the within-group effects of SUV imageswas used on a voxel-by-voxel basis to examine their associationwith Modified Fatigue Impact Scale (MFIS) as the main re-gressor and age sex and global SUV as covariates of no in-terest in an analysis of covariance (ANCOVA) setting Thesegroup-level correlation effect estimates generated statisticalparametric maps of the t-statistic that demonstrated the age-adjusted and sex-adjusted correlations of MFIS total and sub-scale scores with PET uptake in the MS group
Furthermore we coregistered the summed [F-18]PBR06-PET images acquired 60ndash90 minutes following tracer in-jection to the individual MRIs and segmented the images intogray and white matter regions of interest and subregions asdefined by the automated anatomical labeling (AAL) atlastemplate25 using PNEURO 38 software (PMOD Technol-ogies Zurich Switzerland pmodcomweb) This is an au-tomated pipeline and reduces risk of operator-dependent biasin region-of-interest delineation To account for inter-participant differences partial volumendashcorrected SUV ratios(SUVRs) were calculated for participants based on normali-zation of the individual regionrsquos SUV60-90 to the global brainSUV60-90 similar to our previous reports1626ndash28 SUVRs forindividual supratentorial AAL template regions of interest(ROIs) were also obtained and assessed for correlations withfatigue scores Because the substantia nigra (SN) showed thestrongest significant correlations with fatigue scores on SPM
Table 1 Summary of participant characteristics
MS (N = 12) HC (N = 10) p Value
Age (y) 42 plusmn 117 46 plusmn 155 054
Sex distribution 7 F 5 M 4 F 6 M 039
TSPO binding affinity 7 high 5 medium 6 high 4 medium 093
Median EDSS score 35
MFIS score 36 plusmn 21
MFIS physical score 17 plusmn 10
MFIS cognitive score 17 plusmn 10
MFIS psychosocial score 3 plusmn 2
HDRS score 5 plusmn 65
Abbreviations EDSS = ExpandedDisability Status Scale HC =healthy control HDRS =HamiltonDepression Rating ScaleMFIS =Modified Fatigue Impact ScaleTSPO = translocator proteinData are mean plusmn SD unless otherwise indicated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 3
analysis the SN region was specifically segmented using theHammers atlas applied to PET images in the standard spaceusing PVIEW tool of PMOD 38 platform SN SUVRs werecalculated based on Hammers atlas brain parenchymal ROIsdelineated in PVIEW without partial volume correction owingto the small size of the SN ROI PET uptake in right left andaverage of right and left SN ROIs were further investigated forgroup differences between participants with MS with fatigueand participants withMSwithout fatigue (defined asMFIS gt37andMFIS le37 respectively) andHCs and for correlations withMFIS and its subscales in participants with MS In addition forillustration purposes individualized maps of increased sub-stantia nigra PET uptake in a patient withMSwith fatigue and apatient with MS without fatigue represented as voxel-basedz-score values gt2 compared with a healthy data set of 9 healthyvolunteers were generated using the PNEURO platform
Patient-reported outcome measuresParticipants withMS completed the following patient-reportedoutcome measures MFIS29 and Hamilton Depression RatingScale (HDRS)30 The MFIS is a 21-item fatigue scale with 5scaled responses ranging from ldquoneverrdquo to ldquoalmost alwaysrdquo Totalfatigue scores as well as physical cognitive and psychosocialsubscale scores are derived The HDRS is a 17-item rating scalethat evaluates the severity of depression symptoms using asemistructured interview
Statistical analysisThe exact Wilcoxon-Mann-Whitney test with accompanyingexact Hodges-Lehmann 95 CIs was used to evaluate groupdifferences in SUVRs Associations were evaluated usingPearson correlations and partial correlations with 95 CIscalculated using the Fisher transformation The studyrsquos nature
Table 2 Detailed participant characteristics
Participantnumber Sex
Age(y)
TSPObindingaffinity Group
Diseaseduration(y)
CurrentDMT
EDSSscore MFIS
MFISPhysical
MFISCognitive
MFISPsychosocial HDRS
1 F 37 HAB RRMS 52 Fingolimod 4 64 25 35 4 13
2 M 37 HAB RRMS 196 Rituximab 3 33 12 19 2 1
3 F 34 MAB RRMS 48 Fingolimod 1 16 7 9 0 0
4 M 32 MAB RRMS 119 Fingolimod 1 15 13 2 0 1
5 F 23 HAB RRMS 82 Natalizumab 15 6 2 3 1 0
6 F 41 HAB RRMS 96 Fingolimod 15 21 9 9 3 17
7 F 27 MAB RRMS 35 Fingolimod 2 37 15 20 2 0
8 M 52 MAB SPMS 149 Rituximab 65 15 8 6 1 0
9 M 53 HAB SPMS 19 Rituximab 6 37 21 15 1 2
10 F 59 MAB SPMS 19 Glatirameracetate
6 54 23 25 6 7
11 F 59 HAB SPMS 19 None 65 71 34 29 8 17
12 F 50 HAB SPMS 17 Rituximab 45 62 31 26 5 2
13 M 25 MAB HC
14 F 45 HAB HC
15 M 60 MAB HC
16 F 25 HAB HC
17 F 34 MAB HC
18 M 33 HAB HC
19 M 70 MAB HC
20 M 65 HAB HC
21 M 48 HAB HC
22 F 54 HAB HC
Abbreviations DMT = disease-modifying treatment EDSS = ExpandedDisability Status Scale HAB = high-affinity binding HDRS =Hamilton Depression RatingScaleMAB =medium-affinity bindingMFIS =Modified Fatigue Impact Scale HC = healthy control RRMS = relapsing-remittingMS SP = secondary progressiveMS TSPO = translocator proteinDisease duration refers to time from first MS symptom onset
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
was exploratory as a relatively large number of regions wereevaluated therefore results should be considered hypothesisgenerating
Data availabilityAfter due anonymization we will make any unpublished studydata available for sharing with other qualified investigators ifrequested
ResultsRelationship of MFIS with MRI andclinical parametersBPV was lower in patients with MS (n = 12) compared withHCs (n = 9) (14028 plusmn 571 mL vs 14751 plusmn 669 mL) butthere was no correlation between BPV and total MFIS or itsphysical cognitive or psychosocial subscale scores (r = minus005minus009 minus002 and 0004 n = 12) There was no correlationbetweenMFIS and T1 lesion volume (r = 0002 n = 12) or T2lesion volume (r = minus011 n = 12) In terms of clinical cor-relations MFIS increased with increasing age and EDSS (bothr = 058) and a positive correlation with increasing HDRS(r = 052)
SPM analysis
Voxel-level correlations of PET uptake with MFISStrongest voxel-wise peaks for age- and sex-adjusted cor-relation with MFIS (figure 1A) were seen in the right SN(T-score 467) left SN (T-score 425) cerebellar vermisright inferior cerebellar cortex (T-scores 423 and 415respectively) bilateral angular gyri (T-scores 422 and
418 for the right and left side respectively) right pre-cuneus (T-score 421) left premotor and supplementalmotor area (BA6) (T-score 408) and juxtacortical whitematter (T-score 406 figure 1B) A complete list of regionswith voxels demonstrating peak positive correlations be-tween PET uptake and MFIS with p lt 001 is provided intable 3
Strongest voxel-wise peaks for negative correlations withMFIS were seen in the right orbital inferior frontal gyrus (BA47) (T-score 403) and the right temporal pole (BA 38)(T-score 314)
Regional analysis
Relationship of substantia nigra PET uptake with MFISin MSThe finding of strongest correlation between fatigue scoresand PET in the SNwas endorsed by a regional analysis as wellOn regional analysis there was a significant correlation be-tween the SUVR in the SN and total MFIS score (r = 07695 CI 033 to 093 figure 2A) The correlation coefficientsof right and left SN SUVRs with total MFIS (figure 2B) were0795 (95 CI 041 to 094) and 0427 (95 CI minus020 to080) respectively
An overall model consisting of right SN SUVR age EDSSand HDRS explained the majority of variability of MFIS inparticipants with MS (r2 = 07751 adjusted r2 = 06466 n =12) with right SN SUVR remaining an independent predictorof MFIS (r = 073 95 CI 014 to 094 p = 002) afteradjustment for the other covariates
Figure 1 SPM analysis
(A) Statistical Parametric Mapping (SPM)-basedvoxel-by-voxel maps of correlation betweenModified Fatigue Impact Scale (MFIS) and PETuptake The strongest positive correlation wasseen in the right substantia nigra (cross-bars)Additional regions of significant correlationswere seen in the left substantia nigra peri-aqueductal gray pons medulla precuneusmidcingulate cerebellar vermis and insularcortex regions (B) SPM-based voxel-by-voxelmaps demonstrate widespread positive correla-tion in juxtacortical white matter between MFISscores and PET uptake
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 5
Table 3 SPM voxel level correlations with MFIS scores
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
Positive correlations
Brainstem
Right substantia nigra 10 minus16 minus14 467 305
Left substantia nigra minus10 minus10 minus10 425 289
Pons minus8 minus24 minus28 398 279
Medulla minus2 minus34 minus48 390 275
Midbrain periaqueductal gray (PAG) 4 minus30 minus18 344 255
Frontal lobe
Left premotor cortex and supplementary motor area (BA6) minus12 minus24 48 408 283
Left pars opercularis of the inferior frontal gyrus Broca area (BA44) minus50 20 26 384 273
Right Broca area (BA45) 40 30 2 313 240
Right insula (BA13) 32 28 0 320 243
Right dorsolateral and medial prefrontal cortex (BA9) 8 46 36 304 235
Parietal lobe
Right parietal lobe including the angular gyrus near the TPO junction (BA39) 40 minus62 40 422 288
Right precuneus (BA7) 42 minus42 50 421 288
Left parietal lobe including the angular gyrus near the TPO junction (BA39) minus50 minus54 42 418 287
Left dorsal posterior cingulate area (BA31) minus6 minus56 34 393 277
Left precuneus (BA7) minus20 minus68 38 323 245
Right inferior parietal lobesupramarginal gyrus parietal operculum (BA40) 58 minus32 26 303 235
Temporal lobe
Right fusiform (BA37) 46 minus54 minus2 363 264
Right PrimAuditory (BA41) 54 minus12 0 341 254
Left superior temporal gyrus included in the Wernicke area (BA22) minus60 minus6 minus10 321 244
Right parahip (BA36) 28 minus16 minus26 318 242
Left middle temporal gyrusauditory cortex (BA21) minus64 minus18 minus12 312 239
Occipital lobe
Right PrimVisual (BA17) 12 minus66 10 342 254
Right extra striate cortex receives input from pulvinar (BA19) 30 minus82 minus14 338 252
Right VisualAssoc (BA18) 16 minus92 10 317 241
Cerebellum
Cerebellar vermis minus2 minus70 minus20 423 289
Right inferior cerebellar cortex 14 minus74 minus46 415 285
Left superior cerebellar cortex minus38 minus52 minus24 386 274
Right superior cerebellar cortex 18 minus62 minus18 325 246
Left cerebellar cortex minus46 minus60 minus32 318 242
Left inferior cerebellar cortex minus24 minus42 minus54 309 238
Continued
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Defined as an overwhelming sense of tiredness lack of energyor feeling of exhaustion12 fatigue is reported as the mostdisabling symptom in up to 60 of patients with MS3 and isestimated to have a lifetime prevalence of 804 Moreoverthe prevalence of fatigue increases with disease progression(46 in patients with clinically isolated syndrome [CIS] and80 in patients with secondary progressive MS [SPMS])5
Importantly fatigue has been described as the leading cause ofabsence from work in MS6 Fatigue may also have prognosticimplications in patients with MS For example in patientswith CIS up to 46 of patients may present with fatiguewhich has recently been shown to predict conversion toclinically definite MS7 Among patients with relapsing-remitting MS (RRMS) fatigue scores were higher in pa-tients who converted to a confirmed Expanded DisabilityStatus Scale (EDSS) score ge3 after at least 3 years of follow-upcompared with nonconverters This association remainedsignificant after adjusting for depression scales and baselineEDSS8 Despite the high prevalence and significance of fatiguein MS its anatomic and physiologic substrate and its mech-anism are not clear
Inflammation is proposed as a potential mechanism for fa-tigue in MS but has the lack of sufficient evidence3 Abnor-malities in functional connectivity of the resting default modenetwork have been linked with fatigue in MS9 However thebiological processes underlying these abnormalities are notknown
Microglial activation may play a role in the pathogenesis ofMS1011 but it has not been systematically studied in relationto MS-associated fatigue (MSAF) [F-18]PBR06 is a second-generation longer half-life PET radioligand targeting the18-kDa translocator protein for noninvasive assessment of ce-rebral microglial activation that we have recently reported to beincreased in subcortical gray matter and normal-appearingwhite matter in MS12ndash17 Our aim is to assess the role ofmicroglial activation in MSAF using [F-18]PBR06 PET
MethodsParticipantsParticipants were recruited from the Partners Multiple Scle-rosis Center at the Brigham and Womenrsquos Hospital andthrough an online recruitment portal for healthy controlparticipants (HCs) Initially 18 participants with MS and 12HC participants were consecutively enrolled Two
participants with MS and 2 HC participants were low-affinitybinders and were excluded from the study (see the Geno-typing section below) Four additional patients with MSsubsequently changed their minds about participating in thestudy or were lost to follow-up following consent Twelvepatients with MS (5 SP and 7 RR 8 women and 4 men) and10 HC participants (4 women and 6 men) completed thestudy Table 1 contains a summary of characteristics for allstudy participants and table 2 contains detailed individualizedparticipant characteristics Our findings regarding the re-lationship of the [F-18]PBR06 PET scans from these patientswith MS with disability and brain atrophy were previouslyreported16
In terms of the inclusion criteria we included patients withSPMS if they experienced a worsening of their EDSS score byat least 05 (if their baseline EDSS score was ge55) or at least10 (if their baseline EDSS score was lt5) over a period of 1year before PET scanning In addition we included patientswith RRMS who had a relapse or if there was evidence of anew or enlarging T2 bright lesion on MRI or a gadolinium-enhancing lesion on T1-weighted MRI in the last year Pa-tients who were treated with corticosteroids during a period of1 month before the PET scan were excluded PET scanningwas performed within a median time interval of 51 (range11ndash256) weeks in relation to the subjectsrsquo clinical assess-ment Patients did not experience a relapse between theclinical and PET imaging visits
Standard protocol approvals registrationsand patient consentsThe clinicaltrialsgov ID for our study is NCT02649985 Thestudy was approved and overseen by the Institutional ReviewBoard Radiation Safety Committee and Radioactive DrugResearch Committee at our hospital Written informed consentwas obtained from all study participants before participation
GenotypingBlood samples were collected during the initial visits andgenotyping was performed for screening purposes Geno-typing used a TaqMan assay to identify the DNA poly-morphism of the translocator protein (TSPO) gene onchromosome 22q132 Study participants with high-affinity(HAB) and medium-affinity binding (MAB) were included inthe study whereas ones with low-affinity binding were ex-cluded Among the 12 patients with MS who completed thestudy 7 were HABs and 5 were MABs Among the HC par-ticipants 6 were HABs and 4 were MABs (table 1) The
GlossaryAAL = automated anatomic labeling BPV = brain parenchymal volume CFS = chronic fatigue syndrome CIS = clinicallyisolated syndrome DMN = default mode network EDSS = Expanded Disability Status Scale ES = effect size HAB = high-affinity bindingHC = healthy controlHDRS = Hamilton Depression Rating ScaleMAB = medium-affinity binding RRMS =relapsing-remitting MS SN = substantia nigra SPM = Statistical Parametric Mapping SPMS = secondary progressive MSTSPO = translocator protein
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
proportion of HABs andMABs in theMS and HC groups wasnot significantly different (table 1)
Radiopharmaceutical productionWe have previously described the radiopharmaceutical pro-duction methodology at our center16
MRI acquisition and corresponding analysisEach study participant completed an MRI scan on the samescanner (Siemens 3T Skyra Erlangen Germany) according to apreviously described acquisition protocol18ndash20 The protocolincluded a 2D T1-weighted spin-echo axial series (repetitiontime = 611ndash943ms echo time = 79 ms and voxel size = 043 times043 times 3mm3) and a 3D fluid-attenuated inversion recovery andmagnetization-prepared rapid gradient-echo series (voxel sizesfor both 1 times 1 times 1mm3) Using a previously reported techniquenormalized whole-brain parenchymal volume (BPV) was de-rived by applying the latter images to a fully automated algo-rithm (SIENAX v 50 Analysis Group fslfmriboxacuk)21
Hyperintense lesions on 3D T2 FLAIR and hypointense le-sions on T1-weighted spin-echo images were marked by atrained observer (KC) and verified by a senior observer(ST or TS) We determined that to qualify as a T1 hypo-intense lesion the lesion had to be both hypointense onT1-weighted images and hyperintense on Fluid AttenuationInversion Recovery (FLAIR) images2223 A semiautomatededge-finding tool was then used for volumetric lesion con-touring using Jim (version 7 Xinapse Systems West BergholtUnited Kingdom xinapsecom) Our previous work has shownhigh reliability for this semiautomated method of measuringMS cerebral lesion burden2223
PET acquisition and corresponding analysis[F-18]PBR06 was injected as a bolus injection for PET scan-ning using an IV catheter into an arm or hand vein images were
acquired in a list mode acquisition mode using a high-resolution PETCT scanner (GEDiscovery ECATWaukeshaWI) Statistical Parametric Mapping (SPM) was used as theprimary analysis technique for this study SPM12 software (theWellcome Institute of Cognitive Neurology London UnitedKingdom filionuclacukspmsoftware) was used to processthe [F-18]PBR06 PET SUV images24 PET images were ster-eotactically normalized to the Montreal Neurologic Instituteversion of Talairach space Whole-brain multiple linear re-gression modeling of the within-group effects of SUV imageswas used on a voxel-by-voxel basis to examine their associationwith Modified Fatigue Impact Scale (MFIS) as the main re-gressor and age sex and global SUV as covariates of no in-terest in an analysis of covariance (ANCOVA) setting Thesegroup-level correlation effect estimates generated statisticalparametric maps of the t-statistic that demonstrated the age-adjusted and sex-adjusted correlations of MFIS total and sub-scale scores with PET uptake in the MS group
Furthermore we coregistered the summed [F-18]PBR06-PET images acquired 60ndash90 minutes following tracer in-jection to the individual MRIs and segmented the images intogray and white matter regions of interest and subregions asdefined by the automated anatomical labeling (AAL) atlastemplate25 using PNEURO 38 software (PMOD Technol-ogies Zurich Switzerland pmodcomweb) This is an au-tomated pipeline and reduces risk of operator-dependent biasin region-of-interest delineation To account for inter-participant differences partial volumendashcorrected SUV ratios(SUVRs) were calculated for participants based on normali-zation of the individual regionrsquos SUV60-90 to the global brainSUV60-90 similar to our previous reports1626ndash28 SUVRs forindividual supratentorial AAL template regions of interest(ROIs) were also obtained and assessed for correlations withfatigue scores Because the substantia nigra (SN) showed thestrongest significant correlations with fatigue scores on SPM
Table 1 Summary of participant characteristics
MS (N = 12) HC (N = 10) p Value
Age (y) 42 plusmn 117 46 plusmn 155 054
Sex distribution 7 F 5 M 4 F 6 M 039
TSPO binding affinity 7 high 5 medium 6 high 4 medium 093
Median EDSS score 35
MFIS score 36 plusmn 21
MFIS physical score 17 plusmn 10
MFIS cognitive score 17 plusmn 10
MFIS psychosocial score 3 plusmn 2
HDRS score 5 plusmn 65
Abbreviations EDSS = ExpandedDisability Status Scale HC =healthy control HDRS =HamiltonDepression Rating ScaleMFIS =Modified Fatigue Impact ScaleTSPO = translocator proteinData are mean plusmn SD unless otherwise indicated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 3
analysis the SN region was specifically segmented using theHammers atlas applied to PET images in the standard spaceusing PVIEW tool of PMOD 38 platform SN SUVRs werecalculated based on Hammers atlas brain parenchymal ROIsdelineated in PVIEW without partial volume correction owingto the small size of the SN ROI PET uptake in right left andaverage of right and left SN ROIs were further investigated forgroup differences between participants with MS with fatigueand participants withMSwithout fatigue (defined asMFIS gt37andMFIS le37 respectively) andHCs and for correlations withMFIS and its subscales in participants with MS In addition forillustration purposes individualized maps of increased sub-stantia nigra PET uptake in a patient withMSwith fatigue and apatient with MS without fatigue represented as voxel-basedz-score values gt2 compared with a healthy data set of 9 healthyvolunteers were generated using the PNEURO platform
Patient-reported outcome measuresParticipants withMS completed the following patient-reportedoutcome measures MFIS29 and Hamilton Depression RatingScale (HDRS)30 The MFIS is a 21-item fatigue scale with 5scaled responses ranging from ldquoneverrdquo to ldquoalmost alwaysrdquo Totalfatigue scores as well as physical cognitive and psychosocialsubscale scores are derived The HDRS is a 17-item rating scalethat evaluates the severity of depression symptoms using asemistructured interview
Statistical analysisThe exact Wilcoxon-Mann-Whitney test with accompanyingexact Hodges-Lehmann 95 CIs was used to evaluate groupdifferences in SUVRs Associations were evaluated usingPearson correlations and partial correlations with 95 CIscalculated using the Fisher transformation The studyrsquos nature
Table 2 Detailed participant characteristics
Participantnumber Sex
Age(y)
TSPObindingaffinity Group
Diseaseduration(y)
CurrentDMT
EDSSscore MFIS
MFISPhysical
MFISCognitive
MFISPsychosocial HDRS
1 F 37 HAB RRMS 52 Fingolimod 4 64 25 35 4 13
2 M 37 HAB RRMS 196 Rituximab 3 33 12 19 2 1
3 F 34 MAB RRMS 48 Fingolimod 1 16 7 9 0 0
4 M 32 MAB RRMS 119 Fingolimod 1 15 13 2 0 1
5 F 23 HAB RRMS 82 Natalizumab 15 6 2 3 1 0
6 F 41 HAB RRMS 96 Fingolimod 15 21 9 9 3 17
7 F 27 MAB RRMS 35 Fingolimod 2 37 15 20 2 0
8 M 52 MAB SPMS 149 Rituximab 65 15 8 6 1 0
9 M 53 HAB SPMS 19 Rituximab 6 37 21 15 1 2
10 F 59 MAB SPMS 19 Glatirameracetate
6 54 23 25 6 7
11 F 59 HAB SPMS 19 None 65 71 34 29 8 17
12 F 50 HAB SPMS 17 Rituximab 45 62 31 26 5 2
13 M 25 MAB HC
14 F 45 HAB HC
15 M 60 MAB HC
16 F 25 HAB HC
17 F 34 MAB HC
18 M 33 HAB HC
19 M 70 MAB HC
20 M 65 HAB HC
21 M 48 HAB HC
22 F 54 HAB HC
Abbreviations DMT = disease-modifying treatment EDSS = ExpandedDisability Status Scale HAB = high-affinity binding HDRS =Hamilton Depression RatingScaleMAB =medium-affinity bindingMFIS =Modified Fatigue Impact Scale HC = healthy control RRMS = relapsing-remittingMS SP = secondary progressiveMS TSPO = translocator proteinDisease duration refers to time from first MS symptom onset
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
was exploratory as a relatively large number of regions wereevaluated therefore results should be considered hypothesisgenerating
Data availabilityAfter due anonymization we will make any unpublished studydata available for sharing with other qualified investigators ifrequested
ResultsRelationship of MFIS with MRI andclinical parametersBPV was lower in patients with MS (n = 12) compared withHCs (n = 9) (14028 plusmn 571 mL vs 14751 plusmn 669 mL) butthere was no correlation between BPV and total MFIS or itsphysical cognitive or psychosocial subscale scores (r = minus005minus009 minus002 and 0004 n = 12) There was no correlationbetweenMFIS and T1 lesion volume (r = 0002 n = 12) or T2lesion volume (r = minus011 n = 12) In terms of clinical cor-relations MFIS increased with increasing age and EDSS (bothr = 058) and a positive correlation with increasing HDRS(r = 052)
SPM analysis
Voxel-level correlations of PET uptake with MFISStrongest voxel-wise peaks for age- and sex-adjusted cor-relation with MFIS (figure 1A) were seen in the right SN(T-score 467) left SN (T-score 425) cerebellar vermisright inferior cerebellar cortex (T-scores 423 and 415respectively) bilateral angular gyri (T-scores 422 and
418 for the right and left side respectively) right pre-cuneus (T-score 421) left premotor and supplementalmotor area (BA6) (T-score 408) and juxtacortical whitematter (T-score 406 figure 1B) A complete list of regionswith voxels demonstrating peak positive correlations be-tween PET uptake and MFIS with p lt 001 is provided intable 3
Strongest voxel-wise peaks for negative correlations withMFIS were seen in the right orbital inferior frontal gyrus (BA47) (T-score 403) and the right temporal pole (BA 38)(T-score 314)
Regional analysis
Relationship of substantia nigra PET uptake with MFISin MSThe finding of strongest correlation between fatigue scoresand PET in the SNwas endorsed by a regional analysis as wellOn regional analysis there was a significant correlation be-tween the SUVR in the SN and total MFIS score (r = 07695 CI 033 to 093 figure 2A) The correlation coefficientsof right and left SN SUVRs with total MFIS (figure 2B) were0795 (95 CI 041 to 094) and 0427 (95 CI minus020 to080) respectively
An overall model consisting of right SN SUVR age EDSSand HDRS explained the majority of variability of MFIS inparticipants with MS (r2 = 07751 adjusted r2 = 06466 n =12) with right SN SUVR remaining an independent predictorof MFIS (r = 073 95 CI 014 to 094 p = 002) afteradjustment for the other covariates
Figure 1 SPM analysis
(A) Statistical Parametric Mapping (SPM)-basedvoxel-by-voxel maps of correlation betweenModified Fatigue Impact Scale (MFIS) and PETuptake The strongest positive correlation wasseen in the right substantia nigra (cross-bars)Additional regions of significant correlationswere seen in the left substantia nigra peri-aqueductal gray pons medulla precuneusmidcingulate cerebellar vermis and insularcortex regions (B) SPM-based voxel-by-voxelmaps demonstrate widespread positive correla-tion in juxtacortical white matter between MFISscores and PET uptake
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 5
Table 3 SPM voxel level correlations with MFIS scores
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
Positive correlations
Brainstem
Right substantia nigra 10 minus16 minus14 467 305
Left substantia nigra minus10 minus10 minus10 425 289
Pons minus8 minus24 minus28 398 279
Medulla minus2 minus34 minus48 390 275
Midbrain periaqueductal gray (PAG) 4 minus30 minus18 344 255
Frontal lobe
Left premotor cortex and supplementary motor area (BA6) minus12 minus24 48 408 283
Left pars opercularis of the inferior frontal gyrus Broca area (BA44) minus50 20 26 384 273
Right Broca area (BA45) 40 30 2 313 240
Right insula (BA13) 32 28 0 320 243
Right dorsolateral and medial prefrontal cortex (BA9) 8 46 36 304 235
Parietal lobe
Right parietal lobe including the angular gyrus near the TPO junction (BA39) 40 minus62 40 422 288
Right precuneus (BA7) 42 minus42 50 421 288
Left parietal lobe including the angular gyrus near the TPO junction (BA39) minus50 minus54 42 418 287
Left dorsal posterior cingulate area (BA31) minus6 minus56 34 393 277
Left precuneus (BA7) minus20 minus68 38 323 245
Right inferior parietal lobesupramarginal gyrus parietal operculum (BA40) 58 minus32 26 303 235
Temporal lobe
Right fusiform (BA37) 46 minus54 minus2 363 264
Right PrimAuditory (BA41) 54 minus12 0 341 254
Left superior temporal gyrus included in the Wernicke area (BA22) minus60 minus6 minus10 321 244
Right parahip (BA36) 28 minus16 minus26 318 242
Left middle temporal gyrusauditory cortex (BA21) minus64 minus18 minus12 312 239
Occipital lobe
Right PrimVisual (BA17) 12 minus66 10 342 254
Right extra striate cortex receives input from pulvinar (BA19) 30 minus82 minus14 338 252
Right VisualAssoc (BA18) 16 minus92 10 317 241
Cerebellum
Cerebellar vermis minus2 minus70 minus20 423 289
Right inferior cerebellar cortex 14 minus74 minus46 415 285
Left superior cerebellar cortex minus38 minus52 minus24 386 274
Right superior cerebellar cortex 18 minus62 minus18 325 246
Left cerebellar cortex minus46 minus60 minus32 318 242
Left inferior cerebellar cortex minus24 minus42 minus54 309 238
Continued
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

proportion of HABs andMABs in theMS and HC groups wasnot significantly different (table 1)
Radiopharmaceutical productionWe have previously described the radiopharmaceutical pro-duction methodology at our center16
MRI acquisition and corresponding analysisEach study participant completed an MRI scan on the samescanner (Siemens 3T Skyra Erlangen Germany) according to apreviously described acquisition protocol18ndash20 The protocolincluded a 2D T1-weighted spin-echo axial series (repetitiontime = 611ndash943ms echo time = 79 ms and voxel size = 043 times043 times 3mm3) and a 3D fluid-attenuated inversion recovery andmagnetization-prepared rapid gradient-echo series (voxel sizesfor both 1 times 1 times 1mm3) Using a previously reported techniquenormalized whole-brain parenchymal volume (BPV) was de-rived by applying the latter images to a fully automated algo-rithm (SIENAX v 50 Analysis Group fslfmriboxacuk)21
Hyperintense lesions on 3D T2 FLAIR and hypointense le-sions on T1-weighted spin-echo images were marked by atrained observer (KC) and verified by a senior observer(ST or TS) We determined that to qualify as a T1 hypo-intense lesion the lesion had to be both hypointense onT1-weighted images and hyperintense on Fluid AttenuationInversion Recovery (FLAIR) images2223 A semiautomatededge-finding tool was then used for volumetric lesion con-touring using Jim (version 7 Xinapse Systems West BergholtUnited Kingdom xinapsecom) Our previous work has shownhigh reliability for this semiautomated method of measuringMS cerebral lesion burden2223
PET acquisition and corresponding analysis[F-18]PBR06 was injected as a bolus injection for PET scan-ning using an IV catheter into an arm or hand vein images were
acquired in a list mode acquisition mode using a high-resolution PETCT scanner (GEDiscovery ECATWaukeshaWI) Statistical Parametric Mapping (SPM) was used as theprimary analysis technique for this study SPM12 software (theWellcome Institute of Cognitive Neurology London UnitedKingdom filionuclacukspmsoftware) was used to processthe [F-18]PBR06 PET SUV images24 PET images were ster-eotactically normalized to the Montreal Neurologic Instituteversion of Talairach space Whole-brain multiple linear re-gression modeling of the within-group effects of SUV imageswas used on a voxel-by-voxel basis to examine their associationwith Modified Fatigue Impact Scale (MFIS) as the main re-gressor and age sex and global SUV as covariates of no in-terest in an analysis of covariance (ANCOVA) setting Thesegroup-level correlation effect estimates generated statisticalparametric maps of the t-statistic that demonstrated the age-adjusted and sex-adjusted correlations of MFIS total and sub-scale scores with PET uptake in the MS group
Furthermore we coregistered the summed [F-18]PBR06-PET images acquired 60ndash90 minutes following tracer in-jection to the individual MRIs and segmented the images intogray and white matter regions of interest and subregions asdefined by the automated anatomical labeling (AAL) atlastemplate25 using PNEURO 38 software (PMOD Technol-ogies Zurich Switzerland pmodcomweb) This is an au-tomated pipeline and reduces risk of operator-dependent biasin region-of-interest delineation To account for inter-participant differences partial volumendashcorrected SUV ratios(SUVRs) were calculated for participants based on normali-zation of the individual regionrsquos SUV60-90 to the global brainSUV60-90 similar to our previous reports1626ndash28 SUVRs forindividual supratentorial AAL template regions of interest(ROIs) were also obtained and assessed for correlations withfatigue scores Because the substantia nigra (SN) showed thestrongest significant correlations with fatigue scores on SPM
Table 1 Summary of participant characteristics
MS (N = 12) HC (N = 10) p Value
Age (y) 42 plusmn 117 46 plusmn 155 054
Sex distribution 7 F 5 M 4 F 6 M 039
TSPO binding affinity 7 high 5 medium 6 high 4 medium 093
Median EDSS score 35
MFIS score 36 plusmn 21
MFIS physical score 17 plusmn 10
MFIS cognitive score 17 plusmn 10
MFIS psychosocial score 3 plusmn 2
HDRS score 5 plusmn 65
Abbreviations EDSS = ExpandedDisability Status Scale HC =healthy control HDRS =HamiltonDepression Rating ScaleMFIS =Modified Fatigue Impact ScaleTSPO = translocator proteinData are mean plusmn SD unless otherwise indicated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 3
analysis the SN region was specifically segmented using theHammers atlas applied to PET images in the standard spaceusing PVIEW tool of PMOD 38 platform SN SUVRs werecalculated based on Hammers atlas brain parenchymal ROIsdelineated in PVIEW without partial volume correction owingto the small size of the SN ROI PET uptake in right left andaverage of right and left SN ROIs were further investigated forgroup differences between participants with MS with fatigueand participants withMSwithout fatigue (defined asMFIS gt37andMFIS le37 respectively) andHCs and for correlations withMFIS and its subscales in participants with MS In addition forillustration purposes individualized maps of increased sub-stantia nigra PET uptake in a patient withMSwith fatigue and apatient with MS without fatigue represented as voxel-basedz-score values gt2 compared with a healthy data set of 9 healthyvolunteers were generated using the PNEURO platform
Patient-reported outcome measuresParticipants withMS completed the following patient-reportedoutcome measures MFIS29 and Hamilton Depression RatingScale (HDRS)30 The MFIS is a 21-item fatigue scale with 5scaled responses ranging from ldquoneverrdquo to ldquoalmost alwaysrdquo Totalfatigue scores as well as physical cognitive and psychosocialsubscale scores are derived The HDRS is a 17-item rating scalethat evaluates the severity of depression symptoms using asemistructured interview
Statistical analysisThe exact Wilcoxon-Mann-Whitney test with accompanyingexact Hodges-Lehmann 95 CIs was used to evaluate groupdifferences in SUVRs Associations were evaluated usingPearson correlations and partial correlations with 95 CIscalculated using the Fisher transformation The studyrsquos nature
Table 2 Detailed participant characteristics
Participantnumber Sex
Age(y)
TSPObindingaffinity Group
Diseaseduration(y)
CurrentDMT
EDSSscore MFIS
MFISPhysical
MFISCognitive
MFISPsychosocial HDRS
1 F 37 HAB RRMS 52 Fingolimod 4 64 25 35 4 13
2 M 37 HAB RRMS 196 Rituximab 3 33 12 19 2 1
3 F 34 MAB RRMS 48 Fingolimod 1 16 7 9 0 0
4 M 32 MAB RRMS 119 Fingolimod 1 15 13 2 0 1
5 F 23 HAB RRMS 82 Natalizumab 15 6 2 3 1 0
6 F 41 HAB RRMS 96 Fingolimod 15 21 9 9 3 17
7 F 27 MAB RRMS 35 Fingolimod 2 37 15 20 2 0
8 M 52 MAB SPMS 149 Rituximab 65 15 8 6 1 0
9 M 53 HAB SPMS 19 Rituximab 6 37 21 15 1 2
10 F 59 MAB SPMS 19 Glatirameracetate
6 54 23 25 6 7
11 F 59 HAB SPMS 19 None 65 71 34 29 8 17
12 F 50 HAB SPMS 17 Rituximab 45 62 31 26 5 2
13 M 25 MAB HC
14 F 45 HAB HC
15 M 60 MAB HC
16 F 25 HAB HC
17 F 34 MAB HC
18 M 33 HAB HC
19 M 70 MAB HC
20 M 65 HAB HC
21 M 48 HAB HC
22 F 54 HAB HC
Abbreviations DMT = disease-modifying treatment EDSS = ExpandedDisability Status Scale HAB = high-affinity binding HDRS =Hamilton Depression RatingScaleMAB =medium-affinity bindingMFIS =Modified Fatigue Impact Scale HC = healthy control RRMS = relapsing-remittingMS SP = secondary progressiveMS TSPO = translocator proteinDisease duration refers to time from first MS symptom onset
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
was exploratory as a relatively large number of regions wereevaluated therefore results should be considered hypothesisgenerating
Data availabilityAfter due anonymization we will make any unpublished studydata available for sharing with other qualified investigators ifrequested
ResultsRelationship of MFIS with MRI andclinical parametersBPV was lower in patients with MS (n = 12) compared withHCs (n = 9) (14028 plusmn 571 mL vs 14751 plusmn 669 mL) butthere was no correlation between BPV and total MFIS or itsphysical cognitive or psychosocial subscale scores (r = minus005minus009 minus002 and 0004 n = 12) There was no correlationbetweenMFIS and T1 lesion volume (r = 0002 n = 12) or T2lesion volume (r = minus011 n = 12) In terms of clinical cor-relations MFIS increased with increasing age and EDSS (bothr = 058) and a positive correlation with increasing HDRS(r = 052)
SPM analysis
Voxel-level correlations of PET uptake with MFISStrongest voxel-wise peaks for age- and sex-adjusted cor-relation with MFIS (figure 1A) were seen in the right SN(T-score 467) left SN (T-score 425) cerebellar vermisright inferior cerebellar cortex (T-scores 423 and 415respectively) bilateral angular gyri (T-scores 422 and
418 for the right and left side respectively) right pre-cuneus (T-score 421) left premotor and supplementalmotor area (BA6) (T-score 408) and juxtacortical whitematter (T-score 406 figure 1B) A complete list of regionswith voxels demonstrating peak positive correlations be-tween PET uptake and MFIS with p lt 001 is provided intable 3
Strongest voxel-wise peaks for negative correlations withMFIS were seen in the right orbital inferior frontal gyrus (BA47) (T-score 403) and the right temporal pole (BA 38)(T-score 314)
Regional analysis
Relationship of substantia nigra PET uptake with MFISin MSThe finding of strongest correlation between fatigue scoresand PET in the SNwas endorsed by a regional analysis as wellOn regional analysis there was a significant correlation be-tween the SUVR in the SN and total MFIS score (r = 07695 CI 033 to 093 figure 2A) The correlation coefficientsof right and left SN SUVRs with total MFIS (figure 2B) were0795 (95 CI 041 to 094) and 0427 (95 CI minus020 to080) respectively
An overall model consisting of right SN SUVR age EDSSand HDRS explained the majority of variability of MFIS inparticipants with MS (r2 = 07751 adjusted r2 = 06466 n =12) with right SN SUVR remaining an independent predictorof MFIS (r = 073 95 CI 014 to 094 p = 002) afteradjustment for the other covariates
Figure 1 SPM analysis
(A) Statistical Parametric Mapping (SPM)-basedvoxel-by-voxel maps of correlation betweenModified Fatigue Impact Scale (MFIS) and PETuptake The strongest positive correlation wasseen in the right substantia nigra (cross-bars)Additional regions of significant correlationswere seen in the left substantia nigra peri-aqueductal gray pons medulla precuneusmidcingulate cerebellar vermis and insularcortex regions (B) SPM-based voxel-by-voxelmaps demonstrate widespread positive correla-tion in juxtacortical white matter between MFISscores and PET uptake
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 5
Table 3 SPM voxel level correlations with MFIS scores
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
Positive correlations
Brainstem
Right substantia nigra 10 minus16 minus14 467 305
Left substantia nigra minus10 minus10 minus10 425 289
Pons minus8 minus24 minus28 398 279
Medulla minus2 minus34 minus48 390 275
Midbrain periaqueductal gray (PAG) 4 minus30 minus18 344 255
Frontal lobe
Left premotor cortex and supplementary motor area (BA6) minus12 minus24 48 408 283
Left pars opercularis of the inferior frontal gyrus Broca area (BA44) minus50 20 26 384 273
Right Broca area (BA45) 40 30 2 313 240
Right insula (BA13) 32 28 0 320 243
Right dorsolateral and medial prefrontal cortex (BA9) 8 46 36 304 235
Parietal lobe
Right parietal lobe including the angular gyrus near the TPO junction (BA39) 40 minus62 40 422 288
Right precuneus (BA7) 42 minus42 50 421 288
Left parietal lobe including the angular gyrus near the TPO junction (BA39) minus50 minus54 42 418 287
Left dorsal posterior cingulate area (BA31) minus6 minus56 34 393 277
Left precuneus (BA7) minus20 minus68 38 323 245
Right inferior parietal lobesupramarginal gyrus parietal operculum (BA40) 58 minus32 26 303 235
Temporal lobe
Right fusiform (BA37) 46 minus54 minus2 363 264
Right PrimAuditory (BA41) 54 minus12 0 341 254
Left superior temporal gyrus included in the Wernicke area (BA22) minus60 minus6 minus10 321 244
Right parahip (BA36) 28 minus16 minus26 318 242
Left middle temporal gyrusauditory cortex (BA21) minus64 minus18 minus12 312 239
Occipital lobe
Right PrimVisual (BA17) 12 minus66 10 342 254
Right extra striate cortex receives input from pulvinar (BA19) 30 minus82 minus14 338 252
Right VisualAssoc (BA18) 16 minus92 10 317 241
Cerebellum
Cerebellar vermis minus2 minus70 minus20 423 289
Right inferior cerebellar cortex 14 minus74 minus46 415 285
Left superior cerebellar cortex minus38 minus52 minus24 386 274
Right superior cerebellar cortex 18 minus62 minus18 325 246
Left cerebellar cortex minus46 minus60 minus32 318 242
Left inferior cerebellar cortex minus24 minus42 minus54 309 238
Continued
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

analysis the SN region was specifically segmented using theHammers atlas applied to PET images in the standard spaceusing PVIEW tool of PMOD 38 platform SN SUVRs werecalculated based on Hammers atlas brain parenchymal ROIsdelineated in PVIEW without partial volume correction owingto the small size of the SN ROI PET uptake in right left andaverage of right and left SN ROIs were further investigated forgroup differences between participants with MS with fatigueand participants withMSwithout fatigue (defined asMFIS gt37andMFIS le37 respectively) andHCs and for correlations withMFIS and its subscales in participants with MS In addition forillustration purposes individualized maps of increased sub-stantia nigra PET uptake in a patient withMSwith fatigue and apatient with MS without fatigue represented as voxel-basedz-score values gt2 compared with a healthy data set of 9 healthyvolunteers were generated using the PNEURO platform
Patient-reported outcome measuresParticipants withMS completed the following patient-reportedoutcome measures MFIS29 and Hamilton Depression RatingScale (HDRS)30 The MFIS is a 21-item fatigue scale with 5scaled responses ranging from ldquoneverrdquo to ldquoalmost alwaysrdquo Totalfatigue scores as well as physical cognitive and psychosocialsubscale scores are derived The HDRS is a 17-item rating scalethat evaluates the severity of depression symptoms using asemistructured interview
Statistical analysisThe exact Wilcoxon-Mann-Whitney test with accompanyingexact Hodges-Lehmann 95 CIs was used to evaluate groupdifferences in SUVRs Associations were evaluated usingPearson correlations and partial correlations with 95 CIscalculated using the Fisher transformation The studyrsquos nature
Table 2 Detailed participant characteristics
Participantnumber Sex
Age(y)
TSPObindingaffinity Group
Diseaseduration(y)
CurrentDMT
EDSSscore MFIS
MFISPhysical
MFISCognitive
MFISPsychosocial HDRS
1 F 37 HAB RRMS 52 Fingolimod 4 64 25 35 4 13
2 M 37 HAB RRMS 196 Rituximab 3 33 12 19 2 1
3 F 34 MAB RRMS 48 Fingolimod 1 16 7 9 0 0
4 M 32 MAB RRMS 119 Fingolimod 1 15 13 2 0 1
5 F 23 HAB RRMS 82 Natalizumab 15 6 2 3 1 0
6 F 41 HAB RRMS 96 Fingolimod 15 21 9 9 3 17
7 F 27 MAB RRMS 35 Fingolimod 2 37 15 20 2 0
8 M 52 MAB SPMS 149 Rituximab 65 15 8 6 1 0
9 M 53 HAB SPMS 19 Rituximab 6 37 21 15 1 2
10 F 59 MAB SPMS 19 Glatirameracetate
6 54 23 25 6 7
11 F 59 HAB SPMS 19 None 65 71 34 29 8 17
12 F 50 HAB SPMS 17 Rituximab 45 62 31 26 5 2
13 M 25 MAB HC
14 F 45 HAB HC
15 M 60 MAB HC
16 F 25 HAB HC
17 F 34 MAB HC
18 M 33 HAB HC
19 M 70 MAB HC
20 M 65 HAB HC
21 M 48 HAB HC
22 F 54 HAB HC
Abbreviations DMT = disease-modifying treatment EDSS = ExpandedDisability Status Scale HAB = high-affinity binding HDRS =Hamilton Depression RatingScaleMAB =medium-affinity bindingMFIS =Modified Fatigue Impact Scale HC = healthy control RRMS = relapsing-remittingMS SP = secondary progressiveMS TSPO = translocator proteinDisease duration refers to time from first MS symptom onset
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
was exploratory as a relatively large number of regions wereevaluated therefore results should be considered hypothesisgenerating
Data availabilityAfter due anonymization we will make any unpublished studydata available for sharing with other qualified investigators ifrequested
ResultsRelationship of MFIS with MRI andclinical parametersBPV was lower in patients with MS (n = 12) compared withHCs (n = 9) (14028 plusmn 571 mL vs 14751 plusmn 669 mL) butthere was no correlation between BPV and total MFIS or itsphysical cognitive or psychosocial subscale scores (r = minus005minus009 minus002 and 0004 n = 12) There was no correlationbetweenMFIS and T1 lesion volume (r = 0002 n = 12) or T2lesion volume (r = minus011 n = 12) In terms of clinical cor-relations MFIS increased with increasing age and EDSS (bothr = 058) and a positive correlation with increasing HDRS(r = 052)
SPM analysis
Voxel-level correlations of PET uptake with MFISStrongest voxel-wise peaks for age- and sex-adjusted cor-relation with MFIS (figure 1A) were seen in the right SN(T-score 467) left SN (T-score 425) cerebellar vermisright inferior cerebellar cortex (T-scores 423 and 415respectively) bilateral angular gyri (T-scores 422 and
418 for the right and left side respectively) right pre-cuneus (T-score 421) left premotor and supplementalmotor area (BA6) (T-score 408) and juxtacortical whitematter (T-score 406 figure 1B) A complete list of regionswith voxels demonstrating peak positive correlations be-tween PET uptake and MFIS with p lt 001 is provided intable 3
Strongest voxel-wise peaks for negative correlations withMFIS were seen in the right orbital inferior frontal gyrus (BA47) (T-score 403) and the right temporal pole (BA 38)(T-score 314)
Regional analysis
Relationship of substantia nigra PET uptake with MFISin MSThe finding of strongest correlation between fatigue scoresand PET in the SNwas endorsed by a regional analysis as wellOn regional analysis there was a significant correlation be-tween the SUVR in the SN and total MFIS score (r = 07695 CI 033 to 093 figure 2A) The correlation coefficientsof right and left SN SUVRs with total MFIS (figure 2B) were0795 (95 CI 041 to 094) and 0427 (95 CI minus020 to080) respectively
An overall model consisting of right SN SUVR age EDSSand HDRS explained the majority of variability of MFIS inparticipants with MS (r2 = 07751 adjusted r2 = 06466 n =12) with right SN SUVR remaining an independent predictorof MFIS (r = 073 95 CI 014 to 094 p = 002) afteradjustment for the other covariates
Figure 1 SPM analysis
(A) Statistical Parametric Mapping (SPM)-basedvoxel-by-voxel maps of correlation betweenModified Fatigue Impact Scale (MFIS) and PETuptake The strongest positive correlation wasseen in the right substantia nigra (cross-bars)Additional regions of significant correlationswere seen in the left substantia nigra peri-aqueductal gray pons medulla precuneusmidcingulate cerebellar vermis and insularcortex regions (B) SPM-based voxel-by-voxelmaps demonstrate widespread positive correla-tion in juxtacortical white matter between MFISscores and PET uptake
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 5
Table 3 SPM voxel level correlations with MFIS scores
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
Positive correlations
Brainstem
Right substantia nigra 10 minus16 minus14 467 305
Left substantia nigra minus10 minus10 minus10 425 289
Pons minus8 minus24 minus28 398 279
Medulla minus2 minus34 minus48 390 275
Midbrain periaqueductal gray (PAG) 4 minus30 minus18 344 255
Frontal lobe
Left premotor cortex and supplementary motor area (BA6) minus12 minus24 48 408 283
Left pars opercularis of the inferior frontal gyrus Broca area (BA44) minus50 20 26 384 273
Right Broca area (BA45) 40 30 2 313 240
Right insula (BA13) 32 28 0 320 243
Right dorsolateral and medial prefrontal cortex (BA9) 8 46 36 304 235
Parietal lobe
Right parietal lobe including the angular gyrus near the TPO junction (BA39) 40 minus62 40 422 288
Right precuneus (BA7) 42 minus42 50 421 288
Left parietal lobe including the angular gyrus near the TPO junction (BA39) minus50 minus54 42 418 287
Left dorsal posterior cingulate area (BA31) minus6 minus56 34 393 277
Left precuneus (BA7) minus20 minus68 38 323 245
Right inferior parietal lobesupramarginal gyrus parietal operculum (BA40) 58 minus32 26 303 235
Temporal lobe
Right fusiform (BA37) 46 minus54 minus2 363 264
Right PrimAuditory (BA41) 54 minus12 0 341 254
Left superior temporal gyrus included in the Wernicke area (BA22) minus60 minus6 minus10 321 244
Right parahip (BA36) 28 minus16 minus26 318 242
Left middle temporal gyrusauditory cortex (BA21) minus64 minus18 minus12 312 239
Occipital lobe
Right PrimVisual (BA17) 12 minus66 10 342 254
Right extra striate cortex receives input from pulvinar (BA19) 30 minus82 minus14 338 252
Right VisualAssoc (BA18) 16 minus92 10 317 241
Cerebellum
Cerebellar vermis minus2 minus70 minus20 423 289
Right inferior cerebellar cortex 14 minus74 minus46 415 285
Left superior cerebellar cortex minus38 minus52 minus24 386 274
Right superior cerebellar cortex 18 minus62 minus18 325 246
Left cerebellar cortex minus46 minus60 minus32 318 242
Left inferior cerebellar cortex minus24 minus42 minus54 309 238
Continued
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

was exploratory as a relatively large number of regions wereevaluated therefore results should be considered hypothesisgenerating
Data availabilityAfter due anonymization we will make any unpublished studydata available for sharing with other qualified investigators ifrequested
ResultsRelationship of MFIS with MRI andclinical parametersBPV was lower in patients with MS (n = 12) compared withHCs (n = 9) (14028 plusmn 571 mL vs 14751 plusmn 669 mL) butthere was no correlation between BPV and total MFIS or itsphysical cognitive or psychosocial subscale scores (r = minus005minus009 minus002 and 0004 n = 12) There was no correlationbetweenMFIS and T1 lesion volume (r = 0002 n = 12) or T2lesion volume (r = minus011 n = 12) In terms of clinical cor-relations MFIS increased with increasing age and EDSS (bothr = 058) and a positive correlation with increasing HDRS(r = 052)
SPM analysis
Voxel-level correlations of PET uptake with MFISStrongest voxel-wise peaks for age- and sex-adjusted cor-relation with MFIS (figure 1A) were seen in the right SN(T-score 467) left SN (T-score 425) cerebellar vermisright inferior cerebellar cortex (T-scores 423 and 415respectively) bilateral angular gyri (T-scores 422 and
418 for the right and left side respectively) right pre-cuneus (T-score 421) left premotor and supplementalmotor area (BA6) (T-score 408) and juxtacortical whitematter (T-score 406 figure 1B) A complete list of regionswith voxels demonstrating peak positive correlations be-tween PET uptake and MFIS with p lt 001 is provided intable 3
Strongest voxel-wise peaks for negative correlations withMFIS were seen in the right orbital inferior frontal gyrus (BA47) (T-score 403) and the right temporal pole (BA 38)(T-score 314)
Regional analysis
Relationship of substantia nigra PET uptake with MFISin MSThe finding of strongest correlation between fatigue scoresand PET in the SNwas endorsed by a regional analysis as wellOn regional analysis there was a significant correlation be-tween the SUVR in the SN and total MFIS score (r = 07695 CI 033 to 093 figure 2A) The correlation coefficientsof right and left SN SUVRs with total MFIS (figure 2B) were0795 (95 CI 041 to 094) and 0427 (95 CI minus020 to080) respectively
An overall model consisting of right SN SUVR age EDSSand HDRS explained the majority of variability of MFIS inparticipants with MS (r2 = 07751 adjusted r2 = 06466 n =12) with right SN SUVR remaining an independent predictorof MFIS (r = 073 95 CI 014 to 094 p = 002) afteradjustment for the other covariates
Figure 1 SPM analysis
(A) Statistical Parametric Mapping (SPM)-basedvoxel-by-voxel maps of correlation betweenModified Fatigue Impact Scale (MFIS) and PETuptake The strongest positive correlation wasseen in the right substantia nigra (cross-bars)Additional regions of significant correlationswere seen in the left substantia nigra peri-aqueductal gray pons medulla precuneusmidcingulate cerebellar vermis and insularcortex regions (B) SPM-based voxel-by-voxelmaps demonstrate widespread positive correla-tion in juxtacortical white matter between MFISscores and PET uptake
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 5
Table 3 SPM voxel level correlations with MFIS scores
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
Positive correlations
Brainstem
Right substantia nigra 10 minus16 minus14 467 305
Left substantia nigra minus10 minus10 minus10 425 289
Pons minus8 minus24 minus28 398 279
Medulla minus2 minus34 minus48 390 275
Midbrain periaqueductal gray (PAG) 4 minus30 minus18 344 255
Frontal lobe
Left premotor cortex and supplementary motor area (BA6) minus12 minus24 48 408 283
Left pars opercularis of the inferior frontal gyrus Broca area (BA44) minus50 20 26 384 273
Right Broca area (BA45) 40 30 2 313 240
Right insula (BA13) 32 28 0 320 243
Right dorsolateral and medial prefrontal cortex (BA9) 8 46 36 304 235
Parietal lobe
Right parietal lobe including the angular gyrus near the TPO junction (BA39) 40 minus62 40 422 288
Right precuneus (BA7) 42 minus42 50 421 288
Left parietal lobe including the angular gyrus near the TPO junction (BA39) minus50 minus54 42 418 287
Left dorsal posterior cingulate area (BA31) minus6 minus56 34 393 277
Left precuneus (BA7) minus20 minus68 38 323 245
Right inferior parietal lobesupramarginal gyrus parietal operculum (BA40) 58 minus32 26 303 235
Temporal lobe
Right fusiform (BA37) 46 minus54 minus2 363 264
Right PrimAuditory (BA41) 54 minus12 0 341 254
Left superior temporal gyrus included in the Wernicke area (BA22) minus60 minus6 minus10 321 244
Right parahip (BA36) 28 minus16 minus26 318 242
Left middle temporal gyrusauditory cortex (BA21) minus64 minus18 minus12 312 239
Occipital lobe
Right PrimVisual (BA17) 12 minus66 10 342 254
Right extra striate cortex receives input from pulvinar (BA19) 30 minus82 minus14 338 252
Right VisualAssoc (BA18) 16 minus92 10 317 241
Cerebellum
Cerebellar vermis minus2 minus70 minus20 423 289
Right inferior cerebellar cortex 14 minus74 minus46 415 285
Left superior cerebellar cortex minus38 minus52 minus24 386 274
Right superior cerebellar cortex 18 minus62 minus18 325 246
Left cerebellar cortex minus46 minus60 minus32 318 242
Left inferior cerebellar cortex minus24 minus42 minus54 309 238
Continued
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Table 3 SPM voxel level correlations with MFIS scores
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
Positive correlations
Brainstem
Right substantia nigra 10 minus16 minus14 467 305
Left substantia nigra minus10 minus10 minus10 425 289
Pons minus8 minus24 minus28 398 279
Medulla minus2 minus34 minus48 390 275
Midbrain periaqueductal gray (PAG) 4 minus30 minus18 344 255
Frontal lobe
Left premotor cortex and supplementary motor area (BA6) minus12 minus24 48 408 283
Left pars opercularis of the inferior frontal gyrus Broca area (BA44) minus50 20 26 384 273
Right Broca area (BA45) 40 30 2 313 240
Right insula (BA13) 32 28 0 320 243
Right dorsolateral and medial prefrontal cortex (BA9) 8 46 36 304 235
Parietal lobe
Right parietal lobe including the angular gyrus near the TPO junction (BA39) 40 minus62 40 422 288
Right precuneus (BA7) 42 minus42 50 421 288
Left parietal lobe including the angular gyrus near the TPO junction (BA39) minus50 minus54 42 418 287
Left dorsal posterior cingulate area (BA31) minus6 minus56 34 393 277
Left precuneus (BA7) minus20 minus68 38 323 245
Right inferior parietal lobesupramarginal gyrus parietal operculum (BA40) 58 minus32 26 303 235
Temporal lobe
Right fusiform (BA37) 46 minus54 minus2 363 264
Right PrimAuditory (BA41) 54 minus12 0 341 254
Left superior temporal gyrus included in the Wernicke area (BA22) minus60 minus6 minus10 321 244
Right parahip (BA36) 28 minus16 minus26 318 242
Left middle temporal gyrusauditory cortex (BA21) minus64 minus18 minus12 312 239
Occipital lobe
Right PrimVisual (BA17) 12 minus66 10 342 254
Right extra striate cortex receives input from pulvinar (BA19) 30 minus82 minus14 338 252
Right VisualAssoc (BA18) 16 minus92 10 317 241
Cerebellum
Cerebellar vermis minus2 minus70 minus20 423 289
Right inferior cerebellar cortex 14 minus74 minus46 415 285
Left superior cerebellar cortex minus38 minus52 minus24 386 274
Right superior cerebellar cortex 18 minus62 minus18 325 246
Left cerebellar cortex minus46 minus60 minus32 318 242
Left inferior cerebellar cortex minus24 minus42 minus54 309 238
Continued
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

There was no significant correlation betweenMFIS and globalbrain microglial activation (r = minus001 95 CI minus058 to 057)or between MFIS and total brainstem microglial activation (r= 024 95 CI minus039 to 071) When analyzed separatelyboth patients with RRMS and SPMS showed at least a trendfor an increase in the MFIS increasing right SN SUVR (r =070 95 CI minus011 to 095 for RRMS [n = 7] and r = 09495 CI 033 to 099 for SPMS [n = 5] respectively)
Additional regional correlations of PET withtotal MFISIn addition on segmentation of the brain using the AAL tem-plate significant increases in MFIS were seen with increasingSUVRs in the right parahippocampus (r = 075 95 CI 031 to093) right precuneus (r = 065 95 CI 013 to 089) and leftputamen (r = 062 95 CI 007 to 088) in patients with MSAmong these regions after adjustment for age and EDSS rightprecuneus remained significantly correlated with MFIS (r =065 95 CI 003 to 091) in patients with MS
Correlations between MFIS subscales and PETin MS on regional analysis
Cognitive subscale of the MFISThe SN SUVR correlated significantly with the cognitivesubscale of the MFIS (r = 071 95 CI 023 to 091 figure 2C)that remained significant after adjustment for age and EDSS (r= 065 95 CI 004 to 091) Again the right SN SUVRshowed a significant correlation with the cognitive subscale(084 95 CI 051 to 095) that also remained significant afteradjustment for age and EDSS (r = 084 95 CI 045 to 096)The left SN SUVR did not show a significant correlation withcognitive MFIS (r = 030 95 CI minus033 to 075)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake increases in the
cognitive subscale of theMFIS in the right precuneus (r = 07195 CI 022 to 091) and the right parahippocampus (r = 06795 CI 016 to 090) Among these regions after adjustmentfor age and EDSS the right precuneus remained significantlycorrelated with cognitive MFIS (r = 078 95 CI 029 to 095)in patients with MS
Physical subscale of the MFISThe SN SUVR also correlated significantly with the physicalsubscale of theMFIS (r = 0774 95CI 036 to 093 figure 2D)that remained significant after adjustment for age and EDSS (r =064 95 CI 003 to 091) There was a significant correlationbetween the right SN SUVR and the physical subscale of theMFIS (068 95 CI 017 to 090) that also remained significantafter adjustment for age (r = 068 95 CI 036 to 093) but notafter adjustment for both age and EDSS (r = 059 95CI minus006to 089) The correlation between the left SN SUVR and theMFIS physical subscale showed a trend but did not attain sta-tistical significance (r = 056 95 CI minus002 to 086)
On segmentation of the brain using the AAL template sig-nificant increases were seen in PET uptake with increasingvalues of the physical subscale of MFIS in the left calcarinegyrus (r = 059 95 CI 002 to 087) right parahippocampus(r = 077 95CI 034 to 093) left putamen (r = 066 95CI013 to 089) right thalamus (r = 064 95 CI 010 to 089)and vermis 10 (r = 066 95 CI 014 to 090) A decrease inPET uptake with increasing values of the physical subscale ofMFIS was seen in the left superomedial frontal gyrus (r =minus062 95 CI minus088 to minus007)
Psychosocial subscale of the MFISThe correlation between the average SN SUVR and thepsychosocial MFIS subscale did not attain statistical signifi-cance (r = 0556 95 CI minus003 to 086) but the right SN
Table 3 SPM voxel level correlations with MFIS scores (continued)
Brodmann area descriptionMNI coordinates(x y and z) Peak-level t value Peak-level z value
White matter
Subcorticaljuxtacortical WM 26 minus62 34 406 282
Juxtacorticaldeep WM in the left occipital lobe minus20 minus76 16 344 255
JWM right frontal (inferior occipitofrontal fascicle) 24 24 minus10 339 252
Right inferior occipitofrontal fasciculus 32 minus6 minus10 327 247
Right frontal JWM 32 minus20 42 322 244
Negative correlations
Orbital part of the right inferior frontal gyrus (BA47) 30 22 minus26 403 281
Right temporal pole (BA38) 20 6 minus46 314 240
Abbreviations JWM= juxtacortical whitematter MFIS =Modified Fatigue Impact Scale SPM = Statistical ParametricMapping TPO = temporoparietooccipitalp lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 7
SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

SUVR showed a significant correlation with the psychosocialsubscale of the MFIS (r = 067 95 CI 016 to 090 figure2E) The left SN SUVR did not show a significant correlationwith the psychosocial subscale of the MFIS (r = 022 95 CIminus040 to 071)
On segmentation of the brain using the AAL templatesignificant increases were seen in PET uptake with in-creasing values of the psychosocial subscale of MFIS in theleft cuneus (r = 058 95 CI 001 to 087) right para-hippocampus (r = 066 95 CI 014 to 090) and vermis10 (r = 058 95 CI 002 to 087) A decrease in PETuptake with increasing values of the psychosocial subscaleof MFIS was seen in vermis 12 (r = minus059 95 CI minus087to minus004)
Group comparisons of SN PET uptake betweenpatients with MS with fatigue and patientswith MS without fatigue and HCsMFIS scores were 6ndash37 in patients with MS without fatigueand 54 to 71 in patients with MS with fatigue The SN SUVRwas higher in participants with MS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1053 plusmn 0031 vs 0976 plusmn 0045 vs 0932 plusmn 0069 95CI for effect size [ES] 003 to 014 and 003 to 021 re-spectively figures 3 A and B) Similarly the right SN SUVRwas also higher in participants withMS with fatigue comparedwith participants with MS without fatigue and HC partici-pants (1066 plusmn 0034 vs 0971 plusmn 0059 vs 0933 plusmn 0102 95CI for ES 002 to 016 and 003 to 026 respectively figure3C) The left SN SUVR was higher in participants with MS
Figure 2 Correlational analysis between regional PET SUVR and fatigue scores
Correlations between (A) average substantia nigra (SN) SUVR and total MFIS (B) right SN SUVR and total MFIS (C) average SN SUVR and cognitive MFIS (D)average SN SUVR and physical MFIS and (E) right SN SUVR and psychosocial MFIS MFIS = Modified Fatigue Impact Scale
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

with fatigue compared with HC participants (1041 plusmn 0041vs 0930 plusmn 0085 95 CI for ES 003 to 024) but not ascompared to participants with MS without fatigue (1041 plusmn0041 vs 0980 plusmn 0073 95 CI for ES minus003 to 013)(figure 3D)
Group comparisons of PET uptake in AALtemplate regions between patients with MSwith fatigue and patients with MS withoutfatigue and HCsAmong the AAL template regions that showed correlationswith MFIS or its subscales in patients with MS only the rightparahippocampus and right thalamus showed increasedSUVRs in patients with MS with fatigue compared with HCs(10 plusmn 0056 vs 092 plusmn 013 and 124 plusmn 008 vs 112 plusmn 011respectively) but they were not statistically significant (95CI for ES minus004 to 021 and minus005 to 027)
DiscussionThe major findings of our study are that substantia nigramicroglial activation is linked to fatigue scores in patients withMS and that patients with MS with fatigue have a highersubstantia nigra microglial activation than HCs Specificallyright substantia nigra microglial activation correlated withfatigue scores in patients with MS independent of age dis-ability and depression severity highlighting the potentialspecificity of this observation On subsequent exploratoryanalysis we found correlation of fatigue scores with microglialactivation in widespread cortical and subcortical gray matterregions including the right precuneus parahippocampal gy-rus putamen thalamus and juxtacortical white matter
It has been previously proposed that fatigue in MS is linked toregional changes rather than global brain damage31 Rocca
Figure 3 Comparison of substantia nigra PET uptake between subjects with MS with fatigue and subjects with MS withoutfatigue and healthy participants
(A) Individualized z-score maps showing increased [F-18]PBR06 PET uptake in the bilateral substantia nigra in a patient with MS with fatigue with a high totalMFIS score (total MFIS score = 64) compared with a patient with MS without fatigue with a comparable EDSS score (35 vs 4) and a low total MFIS score (MFISscore = 33) For the latter patient the ROIs for the substantia nigra are delineated but do not demonstrate an increased z-score of gt2 comparedwith a healthycontrol group (B) Increased average substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (C) Increased right substantia nigra SUVR in patients with MS with fatigue compared with patients with MS without fatigue and healthyparticipants (D) Increased left substantia nigra SUVR in patients with MS with fatigue compared with healthy controls MFIS = Modified Fatigue Impact Scalep lt 005 p lt 001
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 9
et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

et al31 found that total lesional load measured on T2- and T1-weighted MRIs and global brain atrophy did not distinguishpatients with MS with fatigue from patients with MS withoutfatigue Instead injury to strategic gray and white matter re-gions manifesting as atrophy and microstructural changesmeasured on diffusion tensor imaging significantly contrib-uted to fatigue in MS The lack of correlations between BPVand total T2- and T1 lesional load with fatigue scores in ourstudy is consistent with these observations Other studies havefound in terms of anatomic substrates abnormalities in cor-ticocortical connections corticostriatal networks deep graymatter structures and a cortico-striato-thalamo-cortical loopin relation to fatigue in MS32 In terms of functional andmolecular changes abnormalities in the dopaminergic system(dopamine hypothesis)33 the neuroendocrine system in-volving the hypothalamo-pituitary axis (neuroendocrine hy-pothesis)34 and altered functional connectivity of the restingdefault mode network (functional disconnection hypothesis)3536 have been linked to fatigue in MS in various studies butthe underlying biological bases of these abnormalities are notknown3237 Microglial activation may represent a unifyingmechanism underlying these myriad abnormalities detectedin patients with MS with fatigue It is also possible howeverthat some of these changes are linked to fatigue in generalrather than being specific for MS-related fatigue Notablyinflammation in widespread cortical areas has been associatedwith severity of symptoms in patients with chronic fatiguesyndrome (CFS)myalgic encephalomyelitis38
Abnormal functional activation of the SN in association withfatigue39 has been previously reported in patients with MS Thisis consistent with our results and the microglial activation in theSN may underly the reported abnormal functional activation inthis population The SN is a major seat of dopaminergic neuronsin the brain and microglial activation in the SNmay be linked todopaminergic imbalance which has also been proposed as apotential mechanism for MS-related fatigue33 Increased ironaccumulation in the SN40 has previously been reported in MSbut its association with fatigue in MS has not been studied
Moreover a brainstem fatigue generator model has beenproposed in postviral fatigue syndromes and fatigue thatfollows poliomyelitis41 that may be relevant for un-derstanding fatigue in MS In this model a central role ofsubstantia nigra lesions in inhibiting the functional activityof thalamus cerebral cortex and reticular formation viadecreased dopaminergic stimulation of the putamen andresultant excitation of the globus pallidus externa and in-hibition of the globus pallidus interna has beenproposed4142 Recently a fatigue nucleus that is triggered bycytokines produced by neuroinflammation has been postu-lated to be responsible for the behavioral changes seen inCFS43 Further studies are albeit needed to directly assessthe associations of substantia nigra microglial activation withregional and widespread metabolic electrophysiologic andneurochemical alterations and to assess whether the SNcould be the fatigue nucleus in MS
The association of [F-18]PBR06 PET uptake in the para-hippocampal gyrus posterior cingulate and precuneus ce-rebral cortical areas with fatigue scores supports the role ofmicroglial activation in these regions in the manifestation offatigue in MS Precuneus is a hub of the default mode net-work (DMN)44 Microglial activation may play a role in thereported abnormalities in functional connectivity of theDMN which has been linked with fatigue in MS9 Para-hippocampal gyrus has been reported to connect the defaultmode network with the memory system in the medial tem-poral lobe45 Inflammation of the parahippocampus pre-cuneus and posterior cingulate may interfere withphysiologic activation and deactivation of the DMN andretrieval of memory contributing to fatigue in patients withMS45 The association of right parahippocampal microglialactivity with psychosocial fatigue is consistent with its role inaffective and cognitive empathy46 and detecting sarcasm ininterpersonal interactions47 More studies are needed toassess the relationship between gray matter inflammationand fatigue in MS and their modification by various treat-ment approaches
Our study has several limitations The sample size is small andour results need to be confirmed in larger studies The cross-sectional and observational design of our study allows us toexplore an association between microglial activation and fa-tigue but does not allow us to establish causality We did notformally assess cognition and sleep disturbances althoughnone of our participants with MS were diagnosed with a sleepdisorder Our conclusions rest on the validity of the MFISwhich is a subjective scale but has been otherwise validated inthe assessment of fatigue in MS Other brainstem nuclei suchas locus coeruleus may be involved in fatigue pathogenesis inMS but our approach may lack the resolution and statisticalpower to detect changes in this small-sized structure48 TSPOis not completely specific for micrgolia and approximately20 of the PET signal may originate from astrocytesexpressing glial fibrillary acid protein49
Future research studies are needed to compare the fatigue-related microglial changes in MS with other diseases such asCFS and Parkinson disease and identify common and disease-specific mechanisms of fatigue in neurologic disordersStudies with a longitudinal design can help evaluate a causalrelationship between microglial activation and fatigue in MSLink of microglial activation with neurochemical and regionalneurodegenerative changes in the context of MS-related fa-tigue also needs to be further investigated Furthermore theprognostic value of fatigue and related microglial activation inthe context of progressiveMS is also a potentially exciting areafor further research
Widespread microglial activation particularly in the SN islinked to fatigue in MS Such findings if replicated and ex-panded could provide a foundation for novel therapeuticstrategies and targets for fatigue in MS Further evaluation ofneuroimmunologic basis of fatigue in MS is warranted
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

AcknowledgmentThe authors gratefully acknowledge the participation of ourpatients and contributions of the staff of Biomedical ImagingResearch Core and PET technologists in the Division ofNuclear Medicine and Molecular Imaging Department ofRadiology at Brigham and Womenrsquos Hospital
Study fundingThe authors gratefully acknowledge research grants from NancyDavis Foundationrsquos ldquoRace to Erase MSrdquo program Ann RomneyCenter for Neurologic Diseases Harvard Neuro-DiscoveryCenter and Water Cove Charitable Foundation for their sup-port of this work Funding agencies did not have any role in theperformance of the research or preparation of the manuscript
DisclosureT Singhal S Cicero H Pan K Carter S Dubey R ChuB Glanz S Hurwitz S Tauhid M Park M Kijewski andE Stern report no disclosures relevant to the manuscriptDr Bakshi has received consulting fees from Bayer BiogenCelgene EMD Serono Genentech Guerbet Sanofi-Genzyme and Shire and research support from EMDSerono and Sanofi-Genzyme D Silbersweig reports no dis-closures relevant to the manuscript HL Weiner has receivedconsulting fees from Biogen Tiziana Novartis MerckSerono and Teva Neurosciences and has received grantsupport from Merck Serono and Sanofi-Genzyme and VerilyLife Sciences Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationMarch 24 2020 Accepted in final form June 18 2020
References1 Calabrese M Rinaldi F Grossi P et al Basal ganglia and frontalparietal cortical
atrophy is associated with fatigue in relapsing-remitting multiple sclerosis Mult Scler2010161220ndash1228
2 Comi G Leocani L Rossi P Colombo B Physiopathology and treatment of fatigue inmultiple sclerosis J Neurol 2001248174ndash179
3 Newland P Starkweather A Sorenson M Central fatigue in multiple sclerosis areview of the literature J Spinal Cord Med 201639386ndash399
4 Krupp LB Serafin DJ Christodoulou C Multiple sclerosis-associated fatigue ExpertRev Neurother 2010101437ndash1447
5 Feinstein A Freeman J Lo AC Treatment of progressive multiple sclerosis whatworks what does not and what is needed Lancet Neurol 201514194ndash207
6 Fischer A Heesen C Gold SM Biological outcome measurements for behavioralinterventions in multiple sclerosis Ther Adv Neurol Disord 20114217ndash229
7 van der Vuurst de Vries RM van den Dorpel JJ Mescheriakova JY et al Fatigue after afirst attack of suspected multiple sclerosis Mult Scler 201824974ndash981
8 Cavallari M Palotai M Glanz BI et al Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients Mult Scler 2016221841ndash1849
9 Bisecco A Nardo FD Docimo R et al Fatigue in multiple sclerosis the contributionof resting-state functional connectivity reorganization Mult Scler 2018241696ndash1705
Appendix Authors
Name Location Contribution
TarunSinghal MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studymajor role in the acquisitionof data analyzed andinterpreted the datadrafted and revised themanuscript for intellectualcontent and providedfunding
StevenCicero BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
Hong PanPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
KelseyCarter BS
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Major role in the acquisitionof data and analyzed andinterpreted the data
ShipraDubey PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyand major role in theacquisition of data
Appendix (continued)
Name Location Contribution
Renxin ChuPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
BonnieGlanz PhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShelleyHurwitzPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
ShahamatTauhid MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data
Mi-Ae ParkPhD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
MarieKijewskiDSc
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
Emily SternMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyanalyzed and interpretedthe data and revised themanuscript for intellectualcontent
RohitBakshi MDMA
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
DavidSilbersweigMD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Analyzed and interpretedthe data and revised themanuscript for intellectualcontent
Howard LWeiner MD
Brigham and WomenrsquosHospital Harvard MedicalSchool Boston MA
Designed andconceptualized the studyrevised the manuscript forintellectual content andprovided funding
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 11
10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

10 Gandhi R Laroni A Weiner HL Role of the innate immune system in the patho-genesis of multiple sclerosis J Neuroimmunol 20102217ndash14
11 Weiner HL The challenge of multiple sclerosis how do we cure a chronic hetero-geneous disease Ann Neurol 200965239ndash248
12 Fujimura Y Kimura Y Simeon FG et al Biodistribution and radiation dosimetry inhumans of a new PET ligand (18)F-PBR06 to image translocator protein (18 kDa)J Nucl Med 201051145ndash149
13 Fujimura Y Zoghbi SS Simeon FG et al Quantification of translocator protein (18kDa) in the human brain with PET and a novel radioligand (18)F-PBR06 J NuclMed2009501047ndash1053
14 JamesML BelichenkoNP Nguyen TV et al PET imaging of translocator protein (18kDa) in a mouse model of Alzheimerrsquos disease using N-(25-dimethoxybenzyl)-2-18F-fluoro-N-(2-phenoxyphenyl)acetamide J Nucl Med 201556311ndash316
15 Lartey FM AhnGO Shen B et al PET imaging of stroke-induced neuroinflammationin mice using [18F]PBR06 Molecular imaging and biology Mol Imaging Biol 201416109ndash117
16 Singhal T OrsquoConnor K Dubey S et al Gray matter microglial activation in relapsingvs progressive MS a [F-18]PBR06-PET study Neurol Neuroimmunol Neuro-inflamm 20196e587 doi101212NXI0000000000000587
17 Singhal T OrsquoConnor K Dubey S et al 18F-PBR06 versus 11C-PBR28 PET forassessing white matter translocator protein binding in multiple sclerosis Clin NuclMed 201843e289ndashe295
18 Dupuy SL Tauhid SHurwitz S ChuR Yousuf F Bakshi RThe effect of dimethyl fumarateon cerebral gray matter atrophy in multiple sclerosis Neurol Ther 20165215ndash229
19 KimG Chu R Yousuf F et al Sample size requirements for one-year treatment effectsusing deep gray matter volume from 3T MRI in progressive forms of multiple scle-rosis Int J Neurosci 2017127971ndash980
20 Meier DS Guttmann CRG Tummala S et al Dual-sensitivity multiple sclerosis lesionand CSF segmentation for multichannel 3T brainMRI J Neuroimaging 20182836ndash47
21 Chu R Tauhid S Glanz BI et al Whole brain volume measured from 15T versus 3TMRI in healthy subjects and patients with multiple sclerosis J Neuroimaging 20162662ndash67
22 Bermel RA Sharma J Tjoa CW Puli SR Bakshi R A semiautomated measure ofwhole-brain atrophy in multiple sclerosis J Neurol Sci 200320857ndash65
23 Ceccarelli A Jackson JS Tauhid S et al The impact of lesion in-painting and regis-tration methods on voxel-based morphometry in detecting regional cerebral graymatter atrophy in multiple sclerosis AJNR Am J Neuroradiol 2012331579ndash1585
24 Friston KJ Penny WD Nichols TE Kiebel SJ Ashburner JT Statistical ParametricMapping The Analysis of Functional Brain Images London UK Elsevier Ltd 2007
25 Tzourio-Mazoyer N Landeau B Papathanassiou D et al Automated anatomicallabeling of activations in SPM using amacroscopic anatomical parcellation of theMNIMRI single-subject brain NeuroImage 200215273ndash289
26 Singhal T OrsquoConnor K Pan H Dubey S et al The relationship of microglial acti-vation and multiple sclerosis-associated fatigue a [F-18]PBR06 PET study BerlinGermany ECTRIMS 2018
27 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 vs [C-11]PBR28 PETfor Assessing White Matter TSPO Binding in Multiple Sclerosis Paris FranceECTRIMSACTRIMS 2017
28 Singhal T OrsquoConnor K Chu R Tauhid S et al [F-18]PBR06 PET to Assess TSPOBinding and its Association with Brain Atrophy and Disability in Multiple SclerosisParis France ECTRIMSACTRIMS 2017
29 Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J Evaluation of the modifiedfatigue impact scale in four different European countries Mult Scler 20051176ndash80
30 Williams JB A structured interview guide for the Hamilton Depression Rating ScaleArch Gen Psychiatry 198845742ndash747
31 Rocca MA Parisi L Pagani E et al Regional but not global brain damage contributesto fatigue in multiple sclerosis Radiology 2014273511ndash520
32 Chalah MA Riachi N Ahdab R Creange A Lefaucheur JP Ayache SS Fatigue inmultiple sclerosis neural correlates and the role of non-invasive brain stimulationFront Cell Neurosci 20159460
33 Dobryakova E Genova HM DeLuca J Wylie GR The dopamine imbalance hy-pothesis of fatigue inmultiple sclerosis and other neurological disorders Front Neurol2015652
34 Burfeind KG Yadav V Marks DL Hypothalamic dysfunction and multiple sclerosisimplications for fatigue and weight dysregulation Curr Neurol Neurosci Rep 20161698
35 Finke C Schlichting J Papazoglou S et al Altered basal ganglia functional connec-tivity in multiple sclerosis patients with fatigue Mult Scler 201521925ndash934
36 Hidalgo de la Cruz M drsquoAmbrosio A Valsasina P et al Abnormal functional con-nectivity of thalamic sub-regions contributes to fatigue inmultiple sclerosis Mult Scler2018241183ndash1195
37 Chalah MA Ayache SS Is there a link between inflammation and fatigue in multiplesclerosis J Inflamm Res 201811253ndash264
38 Nakatomi Y Mizuno K Ishii A et al Neuroinflammation in patients with chronicfatigue syndromemyalgic encephalomyelitis an (1)(1)C-(R)-PK11195 PET studyJ Nucl Med 201455945ndash950
39 Engstrom M Flensner G Landtblom AM Ek AC Karlsson T Thalamo-striato-cortical determinants to fatigue in multiple sclerosis Brain Behav 20133715ndash728
40 Blazejewska AI Al-Radaideh AM Wharton S et al Increase in the iron content of thesubstantia nigra and red nucleus in multiple sclerosis and clinically isolated syndromea 7 Tesla MRI study J Magn Reson Imaging 2015411065ndash1070
41 Chaudhuri A Behan PO Fatigue in neurological disorders Lancet 2004363978ndash988
42 Bruno RL Creange SJ Frick NM Parallels between post-polio fatigue and chronicfatigue syndrome a common pathophysiology Am J Med 199810566Sndash73S
43 Komaroff AL Advances in understanding the pathophysiology of chronic fatiguesyndrome JAMA Epub 2019 Jul 5
44 Raichle ME The brainrsquos default mode network Annu Rev Neurosci 201538433ndash447
45 Ward AM Schultz AP Huijbers W Van Dijk KR Hedden T Sperling RA Theparahippocampal gyrus links the default-mode cortical network with the medialtemporal lobe memory system Hum Brain Mapp 2014351061ndash1073
46 Toller G Adhimoolam B Rankin KP Huppertz HJ Kurthen M Jokeit H Rightfronto-limbic atrophy is associated with reduced empathy in refractory unilateralmesial temporal lobe epilepsy Neuropsychologia 20157880ndash87
47 Rankin KP Salazar A Gorno-Tempini ML et al Detecting sarcasm from para-linguistic cues anatomic and cognitive correlates in neurodegenerative diseaseNeuroImage 2009472005ndash2015
48 Niepel G Bibani RH Vilisaar J et al Association of a deficit of arousal with fatigue inmultiple sclerosis effect of modafinil Neuropharmacology 201364380ndash388
49 Kaunzner UW Kang Y Zhang S et al Quantitative susceptibility mapping identifiesinflammation in a subset of chronic multiple sclerosis lesions Brain 2019142133ndash145
12 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 5 | September 2020 NeurologyorgNN
DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

DOI 101212NXI000000000000085420207 Neurol Neuroimmunol Neuroinflamm
Tarun Singhal Steven Cicero Hong Pan et al Regional microglial activation in the substantia nigra is linked with fatigue in MS
This information is current as of August 7 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent75e854fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent75e854fullhtmlref-list-1
This article cites 44 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionpetPET
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm








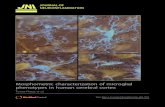









![Review Article The Role of Microglia in Diabetic Retinopathydownloads.hindawi.com/journals/joph/2014/705783.pdf · change in microglial morphology [ ]. erefore, microglial responses](https://static.fdocuments.in/doc/165x107/5f0513557e708231d411234b/review-article-the-role-of-microglia-in-diabetic-change-in-microglial-morphology.jpg)