Regional Anesthesia
47
Regional anaesthesia is potentially dangerous in anaesthetised adult patients - con Barrie Fischer, M.D. Chestons Cottage Uphampton, United Kingdom As the benefits of regional anaesthesia become more widely recognised both central and peripheral nerve blocks are used with increasing frequency during the perioperative period. Some RA techniques are traditionally used as the sole technique but in the majority of cases RA is combined with a light general anaesthetic. Opinion is divided between those anaesthetists who perform the regional anaesthetic after induction of the general anaesthetic and those who advise against this practice on the grounds of safety. A number of medical experts strongly advise against the practice and yet it remains a common practice in many countries. Bromage describes the practice as one of the potential causes of "masked mischief" [1] and together with others has consistently argued against performing central neural blocks [2,3], in particular thoracic epidurals, on anaesthetised patients, whereas others positively recommend it in thoracic surgery [4,5]. A survey by the American Society of Regional Anaesthesia amongst its members showed that the practice was common in the USA for both adult and paediatric patients [6] although the response rate was low. A more recent survey by Romer amongst thoracic anaesthetists in the UK showed that the majority of those who perform thoracic epidurals, invariably insert them after general anaesthesia has been induced [7]. The opinions of medical experts rightly carry great weight, so why do it? Who is right? The subject has been debated with increasing frequency but with no firm conclusions as there is a lack of rigorous data to support both sides of the argument. There is a perception that nerve damage due to regional anaesthesia is becoming more common and the potential for serious nerve damage focuses considerable, possibly disproportionate, attention on the risk which cannot be supported by the scientific data. In a review of litigation against anaesthetists published in 1994 [8] Aitkenhead noted a recent rise in the number of claims from patients who have had regional anaesthesia, whether awake or under anaesthesia but given the weaknesses of currently available data it is difficult to establish whether any rise in complaints is due to bad practice, or is just a reflection of increasing usage of RA and a greater
description
Regional Anesthesia
Transcript of Regional Anesthesia

Regional anaesthesia is potentially dangerous in anaesthetised adult patients - con
Barrie Fischer, M.D.Chestons CottageUphampton, United Kingdom
As the benefits of regional anaesthesia become more widely recognised both central and peripheral nerve blocks are used with increasing frequency during the perioperative period. Some RA techniques are traditionally used as the sole technique but in the majority of cases RA is combined with a light general anaesthetic. Opinion is divided between those anaesthetists who perform the regional anaesthetic after induction of the general anaesthetic and those who advise against this practice on the grounds of safety. A number of medical experts strongly advise against the practice and yet it remains a common practice in many countries. Bromage describes the practice as one of the potential causes of "masked mischief" [1] and together with others has consistently argued against performing central neural blocks [2,3], in particular thoracic epidurals, on anaesthetised patients, whereas others positively recommend it in thoracic surgery [4,5].A survey by the American Society of Regional Anaesthesia amongst its members showed that the practice was common in the USA for both adult and paediatric patients [6] although the response rate was low. A more recent survey by Romer amongst thoracic anaesthetists in the UK showed that the majority of those who perform thoracic epidurals, invariably insert them after general anaesthesia has been induced [7]. The opinions of medical experts rightly carry great weight, so why do it? Who is right?
The subject has been debated with increasing frequency but with no firm conclusions as there is a lack of rigorous data to support both sides of the argument. There is a perception that nerve damage due to regional anaesthesia is becoming more common and the potential for serious nerve damage focuses considerable, possibly disproportionate, attention on the risk which cannot be supported by the scientific data.
In a review of litigation against anaesthetists published in 1994 [8] Aitkenhead noted a recent rise in the number of claims from patients who have had regional anaesthesia, whether awake or under anaesthesia but given the weaknesses of currently available data it is difficult to establish whether any rise in complaints is due to bad practice, or is just a reflection of increasing usage of RA and a greater tendency for resorting to litigation.
While researching this topic for an editorial [9] I contacted the two major Medical Defence Organisations in the United Kingdom for a medico-legal perspective. Both organisations are currently unaware of any cases of neurological damage occurring where the sole risk factor was general anaesthesia being induced prior to the block being performed. The Medical Defence Union has a risk management analysis of cases where general anaesthesia preceded regional anaesthesia (spinal or epidural block) and serious neurological damage subsequently occurred. The prime risk factor was poor patient management where the standard of care fell below acceptable standards. Separate analysis of morbidity due to regional anaesthesia alone (spinal, epidural, thoracic sympathetic block, brachial plexus and paravertebral block) showed a similar profile of patient outcomes and risk factors i.e. poor patient management. Neither organisation views the administration of a general anaesthetic before a regional anaesthetic as inherently bad practice. Nevertheless isolated case reports, anecdotal experience and a few medico-legal reports, together with patient’s innate dislike of needles, provide a background of suspicion which is difficult to refute with a lack of data either for or against the

practice.
There are no prospective randomised controlled studies which compare the relative risks of regional anaesthesia performed on anaesthetised or conscious patients. The data that does exist comes from retrospective qualitative studies (critical incident reporting, closed claim analysis and case reports) where there has been a negative outcome. These studies have inherent weaknesses including reporting bias, incomplete voluntary reporting and an increasing frequency of medicolegal claims which means that the numerator is unknown. Similarly, the total population at risk and the frequency with which different techniques are used (which form the denominator) are also unknown so that the incidence with which these rare but serious events occur cannot be calculated. Because of the time lag of up to 10 years between the closure of a claim and the subsequent analysis, original material may not be available for scrutiny and clinical practice can change radically, reducing the value of the findings.
A number of recent studies on very large patient populations totalling nearly 900,000 patients show that serious morbidity related to regional anaesthesia is extremely rare. Auroy [10] carried out one of the few prospective surveys available. In 1994 103,000 patients received RA in France and whilst there is no data on the combination with GA, there is a three - fold increase in the risk of complications associated with spinals compared to epidural and peripheral blocks. If we assume that spinals are rarely if ever performed on anaesthetised patients the conclusion must be that neural damage can occur even in the awake patient and that factors other than pain from intraneural injection can be responsible. Aromaa [11] surveyed all the anaesthesia insurance claims made in Finland between 1987-1993, which included 25 cases of serious morbidity from a total of 550,000 spinals and 170,000 epidurals. The coincident use of general anaesthesia was not noted but the relative risk of complications was 8.6:1 for spinals compared to epidurals. Dahlgren [12] examined the records of 18,000 central neural blocks again confirming their good safety but all these studies highlight the importance of recognising the role of pre-existing disease, technical difficulties and the need for high standards of patient management perioperatively in reducing the risk of subsequent neurological complications. There are no large studies in adults which specifically look at peripheral blocks but an audit of 16,000 nerve blocks (9000 central and 7000 peripheral) performed in my department between 1991 and 1995 revealed that 85% of blocks were performed on anaesthetised patients with no serious neurological sequelae.
Bromage recently published a closed claim case report which precisely highlights the difficulties of determining the exact cause of neurological damage [13]. A 62 year old female with a history of previous lumbar laminectomy had multiple unsuccessful attempts at a lumbar epidural under general anaesthesia, performed by a trainee. After a successful catheter placement above the level of the laminectomy scar by a more experienced colleague, several episodes of inadequately treated perioperative hypotension occurred and the patient developed permanent paraplegia. MRI scans subsequently showed a small air bubble at the level of T10 and spinal cord infarction at T5. The pattern of injury suggested that anterior spinal artery ischaemia was the most likely cause rather than spinal cord damage so exactly which aspect of her management was responsible for the outcome? Technical difficulty, inexperience and serious hypotension are all major risk factors in adverse outcome from regional anaesthesia whether general anaesthesia is employed or not. A detailed and damning response to this case report was not long in coming [14]. Sixty paediatric anaesthetists published an editorial in Regional Anesthesia and Pain management which is a telling indication of the strong feelings case reports like this generate when conclusions are drawn which cannot be justified by the events described.

In a frequently quoted review [15] of the American Society of Anesthesiologists closed claims analysis of complications following anaesthesia, 15% of all claims were for nerve damage - 227 patients in all of whom 61% received a general anaesthetic and 36% a regional technique. The ulnar nerve was damaged in 34% of cases, the brachial plexus in 23% and lumbosacral nerve damage in 16%. Ulnar nerve damage was predominantly related to general anaesthesia, lumbosacral damage was related to regional anaesthesia and brachial plexus damage was distributed between both techniques but it was not possible to assess the mechanisms of damage in the majority of cases. The frequency with which nerve damage occurs under general anaesthesia tend to be forgotten; poor patient positioning, inadequate padding, tourniquet compression, ischaemia, retractors and surgical technique have all been reported to cause peripheral nerve damage. Anaesthetic factors can be directly or indirectly associated with nerve damage and many of the causes are equally likely to occur whether or not the patient is awake.
Paediatric regional anaesthesia poses a particular problem for the critics of those who perform regional anaesthesia on anaesthetised or heavily sedated patients. In common with adult practice, there has been a sustained growth in the use of perioperative regional anaesthesia in children and general anaesthesia is usually administered prior to the block. A prospective 12 month survey of paediatric anaesthesia in France and Belgium, looked at data from over 85,000 anaesthetics which included 15,000 central neural blocks and 9,300 peripheral blocks [16] . General anaesthesia preceded the regional block in 89% of patients, 6% were "sedated" with intravenous induction agents or inhaled halogenated drugs - only 5% were fully conscious. There were 25 reports of complications with no deaths and no neurological damage. All the complications occurred in the central block group, with an incidence of 1.5 per 1000 and a zero incidence in the peripheral group.
So from a database of 881,000 patients - adult and paediatric what conclusions can be drawn regarding the risks of central and peripheral nerve blocks under anaesthesia? Frankly we are little the wiser.
We know that serious morbidity from regional anaesthetic techniques is vanishingly rare - thankfully.We also know that paediatric anaesthetists have no qualms about anaesthetising their patients prior to performing both central and peripheral blocks. The consequences of permanent neurological damage might reasonably be expected to be greater and last for longer in children, especially neonates whose nervous systems are still immature. It would appear then that we are expected to apply different rules to adults even though nerve damage is an extremely rare risk and there is no scientifically rigorous evidence that general anaesthesia per se increases that risk. The major factors in preventing neurological sequelae are the experience and dexterity of the anaesthetist, proper training and supervision of trainees, detailed assessment of pre-existing vascular and neurological disease, avoidance of repeated attempts due to technical difficulties and prompt recognition and treatment of complications to prevent permanent damage. The issue of whether to administer a general anaesthetic prior to regional anaesthesia becomes less contentious if the correct systems are in place to ensure high standards of practice.
Which blocks can be safely performed under general anaesthesia and which should only be performed on fully conscious patients? Infiltration techniques, field blocks and the discrete blockade of small peripheral nerves do not appear to cause problems and in the absence firm data to the contrary, the weight of clinical practice suggests that the majority of larger peripheral nerve and plexus blocks, with the possible exception of the interscalene approach to the brachial plexus [17] can be safely performed under sedation or light general anaesthetic in spontaneously

breathing patients. Caudal and lumbar epidurals performed below the conus medullaris cannot directly cause spinal cord damage and even thoracic epidurals are safe when carried out by experienced anaesthetists where the benefits to the patient justify the practice[18]. This assumes that the anaesthetist is painstaking in the execution of the technique, pays great attention to the feedback from the needle and has a high index of suspicion in the event of any difficulties. Although pain on injection cannot be verbalised by an anaesthetised patient, other cardinal signs do warn of neural contact; reflex muscle movement, increasing resistance to needle movement and, most importantly, any resistance to injection. Most peripheral nerves are surrounded by loose connective tissue and correctly placed needles should offer no appreciable resistance to flow. Some of these practical nuances are subtle and may escape the novice unless properly supervised but they can be safely taught by skilled practitioners. Peripheral nerve stimulators are valuable teaching tools; they aid nerve location and improve success rates but there is no evidence that they reduce the potential for nerve damage in either anaesthetised or conscious patients.The key to safe regional anaesthesia is not whether the patient is asleep or awake - it rests entirely on the skills and experience of the anaesthetist who must have an awareness of the risks, take all reasonable steps to avoid them and manage the patient with a high standard of care throughout the perioperative period.
References:1. Bromage PR Masked Mischief. Regional Anesthesia 1996; 21(6S); 62-632. Bromage P R. Epidural Analgesia. Philadelphia; W B Saunders 1978: 6673. Bromage P R. The control of post thoracotomy pain. Anaesthesia 1989; 44: 4454. Gough J D, Williams A B, Vaughan R S, Khalil J F, Butchart E G. The controlof post thoracotomy pain. A comparative evaluation of thoracic epidural fentanylinfusions and cryo-analgesia. Anaesthesia 1988; 43: 780-7835. Vaughan R S, Gough J D. The control of post thoracotomy pain. Anaesthesia1989; 44: 4456. Horlocker T T. Regional Anesthesia Survey. ASRA News, August 1997; 1-37. Romer HC, Russell GN. A survey of the practice of thoracic epidural analgesiain the United Kingdom. Anaesthesia 1998; 53: 1016-228. Aitkenhead A R. The pattern of litigation against anaesthetists. British Journalof Anaesthesia 1994; 73: 10-219. Fischer HBJ Regional Anaesthesia - before or after general anaesthesia?Anaesthesia 1998; August10. Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B, Samii K. Serious complicationsrelated to regional anesthesia. Anesthesiology 1997; 87: 479-48611. Aromaa V, Lahdensuu M, Cozanitis DA. Severe complications associated withepidural and spinal anaesthesias in Finland 1987-1993. A study based on patientinsurance claims. Acta Anaesthesiol Scand. 1997; 41: 445-452 12. Dahlgren N, Tornebrandt K Neurological complications after anaesthesia. Afollow-up of 18,000 spinal and epidural anaesthetics performed over three years.Acta Anaesthesiol Scand 1995; 39:872-88013. Bromage PR Benumof JL. Paraplegia following intracord injection during attemptedepidural anesthesia under general anesthesia. Regional Anesthesia and PainMedicine 1998; 23: 104-10714. Krane EJ et al. The safety of epidurals placed during general anesthesia. RegAnes and Pain Man 1998; 23; 433-438 15. Kroll D A, Caplan R A, Posner K, Ward R J, Cheney F W. Nerve injury associatedwith anesthesia. Anesthesiology 1990; 73: 202-20716. Giaufre E, Dalens B, Gombert A. Epidemiology and morbidity of regionalanesthesia in children: a one year prospective survey of the French languageSociety of Paediatric Anesthesiologists. Anesth Analg 1996; 83: 904-91217. Passannante A N. Spinal anesthesia and permanent neurological deficit after

interscalene block. Anesth Analg 1996; 82: 873-87418. Bromage P R. Neurological complications of subarachnoid and epidural anaesthesia. Acta Anaesthesiol Scand 1997; 41: 439-444
Peripheral nerve blocks in children
Bernard DalensPavillon GosselinHôtel-Dieu BP 69F-63003 Clermont-Ferrand Cedex 1France
Peripheral nerve blocks have long been underused in pediatric patients, both for theoretical and practical reasons. During the last decade, many conditions have changed: the importance of adequate pain management has been universally accepted, the limitations and adverse effect of central block procedures have been put in light and new devices allowing both easy and safe location of mixed nerve and/or fascial planes have become available at reasonable cost. Currently, a growing number of anesthesiologists are considering peripheral blocks for providing intra- and post-operative pain relief in a localized area either as single shot procedures (short duration pain relief, especially in the context of ambulatory surgery) or continuous procedure with the placement of reinjection catheters (thus allowing long lasting pain relief on a limited area of the body) (1,2).
SELECTION OF APPROPRIATE DEVICES AND ANESTHETIC SOLUTIONS
Location of mixed nervesMixed nerves trunks and plexuses are best localized by using electrical stimulation to elicit twitches in supplied muscles. Whether unsheathed (cheap) needles have been successfully used pediatric patients (3), sheathed needles of appropriate length are the best devices for achieving the goal of safe and precise location of mixed nerves. More sophisticated devices are now available which permit inserting a reinjection catheter either through a cannulas mounted over a metallic blunt needle, or directly through the insulated needle connected to a nerve stimulator. Still more recently, the catheter itself, with a built-in spiraled metallic wire, can be connected to the nerve stimulator, thus allowing its precise placement in close contact to the relevant nerve path.
Location of fascial planes during compartment blocksPrecise identification of fascial planes is the essential step of compartment blocks such as the fascia iliaca compartment block or the ilioinguinal nerve block. To achieve this goal, it is necessary to use a short bevel needle to allow good identification of the relevant fascial plane. Using this kind of needle also improves considerably the safety of the procedure. In most cases, the fascial plane to be identified is the external fascia. Since the internal fascia has the same structure (and resistance), it is as difficult to cross it as it is to cross the external fascia; therefore, using a short-beveled needle virtually eliminates the risk of piercing simultaneously the two fascias and threatening underlying structures (organs or vessels). Several commercially available short

bevel needles allows safe placement of a reinjection catheter along the inner surface of the relevant fascial plane, thus allowing continuous or intermittent injection of anesthetic solutions for both passive and active (reeducation and joint mobilization) post-operative pain relief.
Selection of local anestheticsThe same solutions as those used in adults are commonly used in children, at doses and volumes adapted to patients' age and size.
LOCAL ANESTHETIC Usual concentration (%)
Usual doses (mg/kg) (plain)
Maximum(a) dose (mg/kg) (mg/kg)
Maximum(b) dose with epinephrine
AMINOESTERS
Procaine 1-2 7 10 10
Chloroprocaine 2-3 7 10 10
AMINOAMIDE
Lidocaine 0.5-2 5 7.5 10
Mepivacaine 0.5-1.5 5-7 8 10
Bupivacaine 0.25-0.5 2 2.5 3
Etidocaine(c) 1 3-5 5 7
Ropivacaine 0.2 - 1 2-3 3.5 Not used
(a): Maximum doses are controversial; the doses mentioned above are safe when given as single injections. (b): Danger of severe methemoglobinemia in infants (even with low therapeutic doses).(c): Etidocaine should not be administered alone because sensory blockade can be insufficient.
Use of additivesLocal anesthetics have a limited duration of action which can be significantly prolonged by a sound selection of additives mixed with the injected solution. Alpha2-adrenergic agonists have long been added to local anesthetics. Epinephrine is the most commonly used of such agents, usually in concentrations ranging from 1:200,000 to 1:400,000; when not contraindicated, this addition offers two main advantages: 1) vascular absorption (thus systemic toxicity) is decreased; 2) inadvertent intravascular injection can be detected (within 20 seconds) by checking the electrocardiographic tracings (ST segment elevation, T wave change (4) and, occasionally, heart rate changes) provided the injected dose of epinephrine is, at least, 0.5 جg/kg (5).Clonidine, another ·2-adrenergic agonist, is now commonly added to local anesthetics for central and peripheral(6,7) blocks. Administered at doses ranging from 1 to 1.5 جg/kg, clonidine consistently increases the duration of nerve blockade with no perceptible hemodynamic effects in children; a slight sedation for 1 to 3 hours, more beneficial than detrimental is produced and usually allows a quiet emergence from anesthesia.Sodium bicarbonate has been added to various solutions of local anesthetics with the aim of increasing the non-ionized form of the drug, allowing more molecules to

cross cell membranes with the expected benefit of shortening the latency and increasing the potency of the solution. However, the clinical relevance of this addition remains controversial (8).
Ketamine has recently been used as an additive to epidural and spinal local anesthetics due to its local effects on spinal NMDA receptors (9,10,11). Its addition to solutions injected nerve paths seems to have a similar considerable prolongation effect of sensory blockade and this light play a consistent role in the very next future.
Placement of a re-injection catheterDue to greater attention being paid to pain relief and availability of adequate devices, placement of re-injection catheters is increasingly used in adult and, more recently, pediatric patients (1,12,13). This technique allows provision of excellent analgesia for a limited (iterative injections) or extended (continuous infusion) period of time over a limited body area with virtually no systemic side effects and impairment of major functions.
SAFETY PRECAUTION
Peripheral nerve blocks are anesthetic techniques. They should only be performed by experienced anesthesiologists in an operating theater environment with monitoring procedures and safety procedures recommended for any general anesthetic. Prior establishment of an intravenous line is essential (14) and (automated) control of electrocardiographic tracings, blood pressure, respiratory rate and central temperature are the minimal monitoring required. Vital parameters as well as the agents, doses and techniques used should be recorded on a complete anesthesia chart.In adults, most peripheral nerve blocks are performed in conscious or lightly sedated patients. The same management is applicable to cooperative children who are willing to remain conscious throughout the procedures and are able to dominate theirs fears and anxiety. More frequently, children do not want to be conscious and fear needle punctures at most, thus requesting being given a general anesthetic. If not contraindicated for medical reasons (poor physical status, full stomach etc.), light general anesthesia can be safely used and is both very commonly practiced and widely accepted in pediatrics (15).The technique of injection is a key factor of safety and early diagnosis of complications. All block procedures require that an aspiration test and evaluation of a test dose (with 0.5 to 1 جg/kg of epinephrine if not contra-indicated) be performed before large amounts of local anesthetic are injected. The injection must be performed slowly and any unusual resistance requires immediate cessation of the technique.
UPPER EXTREMITY CONDUCTION NERVE BLOCKS
Indications, contraindications and complicationsWhether all techniques are suitable, axillary first, then supraclavicular approaches to the brachial plexus are the main techniques used in children. Axillary blocks are recommended for elective as well as emergency surgery on the forearm and the hand, both for providing intra- and postoperative analgesia, especially for outpatient surgery.

Contraindications are scarce, mainly represented by lymphadenopathy (infectious or malignant) and the morbidity of the technique is very low. Supraclavicular brachial plexus blocks are recommended for emergency surgery of the upper limb in a patient with a full stomach when the lesions involve the proximal part of the limb (shoulder, arm and elbow) or when the limb cannot be moved, either due to pain or due to the lesion. Supraclavicular approaches are preferred to axillary approaches unless a tourniquet is used during surgery or in case of anomalies in the axillary region (infectious or malignant adenopathies especially). Occasionally, a supraclavicular block is performed not only for analgesic purposes but for its vasodilatory properties when blood supply to the limb is compromised or to produce full motor blockade of the limb in case of fragile tendon repair, nerve reconstruction, skin graft, especially in boisterous children. Classical contraindications to (most) supraclavicular approaches include bilateral blockade and marked respiratory insufficiency (acute or chronic) due to the potential danger of pneumothorax and (bilateral) phrenic nerve palsy. The parascalene approach, however, does not have the same limitations as the technique does not threaten any vital organs, especially the apical pleura. Nonetheless, an axillary approach has to be envisaged first, and is preferable for suitable surgery of the forearm and hand), each time a brachial plexus block seems to be mandatory.
Auxiliary block proceduresAll the techniques initially described in adults series of patient can be directly transposed to pediatric patients except for transaxillary approaches which should not be used. The main limitation of the axillary approach is the inconstant blockade of the musculocutaneous nerve. As this nerve runs within the coracobrachialis muscle, which is easily identifiable by palpation, a trans-coracobrachialis approach considerably improves the success rate of the technique. While the arm is abducted by 90ئ as in classical approaches, the needle is inserted vertically at the crossing of the coracobrachialis muscle with the lower edge of the pectoralis major muscle, pointing to the lower border of the humerus, just above the axillary artery which is firmly held by finger compression, until a "click" is felt and twitches are elicited. A reinjection catheter can be introduced and securely taped. Long-lasting postoperative pain relief can be achieved either by repeated injections of 0.3 to 0.5 ml/kg (up to 20 ml) of 1% lidocaine or mepivacaine, not exceeding 4 injections per day or continuous infusion of 0.1 or 0.125% plain bupivacaine (or 0.2% ropivacaine) at a rate of 0.5 ml per hour and per year of age.
The parascalene approach (16)The technique is performed with the child in the supine position, arms extended along the chest wall, head turned to opposite side, and a rolled sheet slipped under the shoulders aiming at extending the neck and stretching the brachial plexus components. The puncture site lies on the line uniting the transverse process of C6 to the midpoint of the clavicle,

at the union of the lower third with the upper two thirds. The needle is inserted vertically, toward the back plane until twitches are elicited in the upper limb and 0.5 to 0.75 ml/kg (not exceeding 25 ml) of local anesthetic is then injected. The overall success rate of the technique is high (16,17,18) and the morbidity is extremely low (even Horner syndrome is infrequent). A reinjection catheter can be inserted and the same anesthetic regimen as for axillary blocks is suitable.
LOWER EXTREMITY NERVE BLOCKS
Lumbar plexus nerve blocksIndications, contraindications and complicationsThe lumbar plexus can be percutaneously approached from posteriorly but the technique is not as commonly used in children as are femoral nerve blocks and, furthermore, multi-effective techniques both for elective and emergency procedure (fractured shaft of the femur). The latter two techniques may represent a good, and safer, alternative to epidural anesthesia, the more so as placement of a catheter would allow long-lasting pain relief (19,20). Conscious and slightly sedated children tolerate quite well the performance of a muscle biopsy under femoral and lateral cutaneous nerve block (21). The saphenous nerve block is an excellent complement of a sciatic nerve block for providing complete analgesia of the lower with low or reasonable amounts of local anesthetics. These blocks are virtually free of complications.
Specific femoral nerve block Specific femoral nerve block is performed by inserting the needle at right angles to the thigh, 0.5-1 cm both distal to the inguinal ligament and lateral to the femoral artery until paresthesia or twitches are elicited in the thigh. High quality block is obtained with the injection of 0.5 to 0.75 ml/kg of a local anesthetic (as for parascalene blocks). A reinjection catheter can be left in place for iterative of continuous injections (same regimen as for axillary block), thus allowing long lasting postoperative pain relief (including pain-free mobilization of joints).
Fascia iliaca compartment block (22) A multi-effective lumbar plexus nerve block is easily obtained by injecting a local anesthetic at the inner surface of the fascia iliaca under which run all the nerves emerging from the lumbar plexus. The needle is inserted vertically 0.5-1 cm caudal to the junction of the lateral with the medial two thirds of the inguinal ligament. Two losses of resistance are sought, the first corresponding to the fascia and the second one to the fascia iliaca: the local anesthetic is then injected following the safety rules. The volume injected (1 ml/kg up to a maximum of 30 ml) is critical and massaging the swollen area favors upward and lateral spread of the solution at the inner surface of the fascia iliaca. This technique allows easy insertion of a reinjection catheter for long-lasting postoperative relief.
Saphenous/Vastus medialis nerve block (23)The saphenous nerve is the terminal branch of the femoral nerve which supplies the medial part of the leg, ankle and foot. Its block completes to the whole limb (below the knee) the distribution of anesthesia provided by a sciatic nerve block. This sensory nerve runs just lateral to the motor branch supplying the vastus medialis muscle, which can be easily located by nerve stimulation 0.5 cm lateral to the femoral artery and 3 to 6 cm (depending on patient's age and size) below the inguinal ligament. An insulated needle is inserted vertically until twitches are elicited in the vastus medialis; then 0.1 to 0.2 ml/kg of local anesthetic is injected, which results in a constant and complete saphenous nerve block (additionally, the vastus

medialis nerve is blocked, but this has no practical interest). The very small doses of local anesthetic required to achieve complete blockade makes this block the ideal complement to a sciatic nerve block to ensure complete nerve blockade of the leg below the knee.
Sciatic nerve blocks Indications, contraindications and complicationsSciatic nerve blocks are recommended for all surgery involving the lower extremity below the knee, especially at ankle and foot levels; as the medial part of the leg down to the medial malleole and, sometimes, the great toe, is supplied by the saphenous nerve, a complementary block of this nerve is required to ensure full anesthesia of the leg and foot. Sciatic nerve blocks have no specific contraindications. Whether irreversible damage to the sciatic nerve following intragluteal injections has been reported in the first quarter of this century, both experimental data and clinical experience with the use of local anesthetics have confirmed the safety of the procedure.
Proximal Lateral approachThis technique allows approaching the sciatic nerve with the patient lying supine. The insulated needle is inserted horizontally 1 to 2 cm below the lateral skin projection of the greater trochanter of the femur, pointing to the lower border of the femur until twitches are elicited in the foot. A volume of 1 ml/kg (up to 35 ml) of a local anesthetic is then injected to achieve blockade (which lasts longer than with any other nerve block with the same local anesthetic agent). Recently, new devices have been released which allow insertion of a catheter, thus permitting iterative as well as continuous injection of local anesthetics for long lasting postoperative pain relief. The lateral approach is the easiest and safest proximal approach to the sciatic nerve, with a very high success, even in the hands of a beginner.
Sciatic block in the popliteal fossaThe sciatic nerve can be approached in the popliteal fossa with smaller doses of local anesthetics than following a proximal approach. A simplified single-shot technique was recently reported for use in children placed in the lateral decubitus position with the affected extremity lying uppermost (24). An insulated needle is inserted cephalad at a 45ئ angle to the skin both lateral to the midline and proximal to the popliteal fold until twitches are elicited in the sciatic territory; complete blockade of the sciatic nerve was obtained in all 50 reported patients and no adverse effects were observed.
BLOCK OF NERVES SUPPLYING THE TRUNK
Trunk nerve blocks are being increasingly used in pediatric patients. Many of them are known and used, often only occasionally, in children for decades. These include intercostal nerve and interpleural (or intrapleural) block, both techniques allowing placement of a reinjection catheter for long-lasting pain relief ; however, the danger of systemic toxicity must not be underestimated. The thoracic paravertebral block has gained in renewed interest in recent years and can represent an effective alternative to intercostal nerve blocks, the more so as it does not require that several punctures are performed at different levels. However, the technique is not that simple and its indications are scarce. Several simple and safe compartment block techniques are available and should be used more extensively as their benefit/risk ratio is very high.
Para-umbilical or rectus sheath block (25,26)This old technique that has recently regained considerable interest as it provides excellent analgesia of the peri-umbilical area, which makes it an ideal block for repair of umbilical hernia and hernias of the linea alba. The technique consists of

inserting a short bevel needle 2 cm lateral to the linea alba, on each side, at a 60 degree angle to the skin pointing to the upper border of the umbilicus until it pierces (with difficulty), the rectus abdominis sheath with a characteristic and audible give. The local anesthetic (0.5% bupivacaine, plain of with 1/200,000 epinephrine) is then injected on a weight basis (0.2 ml/kg) in a fan shape manner. When the needle is withdrawn, injection 0.5-1 ml of the solution subcutaneously would still improve the quality of analgesia. The same technique is repeated on the other side.
Iliohypogastric and ilioinguinal nerve blocks
The iliohypogastric and ilioinguinal nerve block provides adequate ipsilateral analgesia for intra and postoperative pain relief of most operations in the inguinal region (herniorrhaphy, orchidopexy, hydrocele) including emergency procedures (strangulated hernia with intestinal obstruction). The technique compares favorably with caudal anesthesia; it has no specific contraindications, no true complications but undesired femoral nerve block, which may preclude discharge from hospital in patients scheduled for outpatient surgery, is not unusual especially when large volumes of local anesthetics (more than 0.4 ml/kg) have been injected. Unexpectedly high plasma bupivacaine concentrations (without clinical signs of toxicity) have been reported in children weighing 10-15 kg (from a series of 30 patients) (27), but no further similar data have been reported yet. Ropivacaine might improve the safety of the block procedure but no data are currently available and this agent has no approval for use in this indication.
Penile blocks via the subpubic spacePenile block via the subpubic space is the ideal block procedure for anesthetizing the penis and its envelopes. The technique has no specific contraindications but, as the penis is supplied by terminal arteries, epinephrine must not be added to the anesthetic solution. While the penis is pulled down, a short-bevel needle is inserted almost perpendicularly to the skin, with a slight caudal and medial slope, 0.5 cm below the symphysis pubis and lateral to the linea alba (on both sides) until it pierces Scarpa's fascia which covers the subpubic space. A 0.1 ml/kg volume (not exceeding 5 ml) of local anesthetic is then injected at both sites of puncture. Long-lasting pain relief is obtained with use of 0.5% plain bupivacaine.
Pudendal/perineal nerve blockThis block procedure was once very popular in obstetric patients and is regaining interest in pediatrics to complement an ilioinguinal/iliohypogastric nerve block when a surgical incision of the posterior part of the scrotum is necessary. The child is placed in the supine position, thighs abducted, knee flexed and the plantar aspects of his feet conjoined (as for girl's bladder catheterization). The ischial tuberosity is identified just above and lateral to the anus. A short-beveled needle is then inserted in the frontal plane, pointing to the medial aspect of the ischial tuberosity until a give is felt as the obturator fascia is pierced. The epinephrine-free local anesthetic is then injected on a weight basis (0.1 ml/kg up to 5 ml).
CONCLUSION
Peripheral nerve blocks are still underused in pediatric patients in spite of their

many advantages. They result in a limited distribution of anesthesia with virtually no general or systemic effects. Due the considerable improvements in the design of devices made by the manufacturers, virtually all peripheral nerve block procedures can be safely performed at any age, with a very high success rate. Additionally, several now available devices allow placement of a catheter which permits accurate management of pain relief both in terms of duration and intensity. The application of such continuous techniques should develop considerably in forthcoming years due to its high benefit/risk ratio and compete considerably with continuous epidurals the morbidity of which is considerably greater.
References1. Taras JS, Behrman MJ. Continuous peripheral nerve block in replantation andrevascularization. J Reconstr Microsurg 1998;14:17-21.2. Sutherland ID. Continuous sciatic nerve infusion: expanded case report describing anew approach. Reg Anesth Pain Med 1998;23:496-501.3. Bosenberg AT. Lower limb nerve blocks in children using unsheathed needles and anerve stimulator. Anaesthesia 1995; 50: 206-210.4. Freid EB, Bailey AG, Valley RD. Electrocardiographic and hemodynamic changesassociated with unintentional intravascular injection of bupivacaine with epinephrinein infants. Anesthesiology 1993,79:394-398.5. Felberg MA, Berkowitz RA, Chowdhury P, McDonald TB. Variable epinephrineconcentrations in local anesthetic test doses for caudal anesthesia in pediatric patients.Anesthesiology 85: A 1073, 1996.6. Singelyn FJ, Dangoisse M, Bartholomee S, Gouverneur JM. Adding clonidine tomepivacaine prolongs the duration of anesthesia and analgesia after axillary brachialplexus block. Reg Anesth 1992;17: 69-74.7. Singelyn FJ, Gouverneur JM, Robert A. A minimum dose of clonidine added tomepivacaine prolongs the duration of anesthesia and analgesia after axillary brachialplexus block. Anesth Analg 1996;83:1046-1050.8. Chow MYH, Sia ATH, Koay CK, Chan YW. Alkalinization of lidocaine does not hastenthe onset of axillary brachial plexus block. Anesth Analg 1998; 86: 566-568.9. Naguib M, Sharif AMY, Seraj M, El Gammal M, Dawlatly AA. Ketamine for caudalanalgesia in children: comparison with caudal bupivacaine. Br J Anesth67: 559-564, 1991.10. Tverskoy M, Oren M, Vaskovich M, Dashkovsky I, Kissin I. Ketamine enhances localanesthetic and analgesic effects of bupivacaine by peripheral mechanism: a study inpostoperative patients. Neurosci Lett 1996; 215:5-8.11. Semple D, Findlow D, Aldridge LM, Doyle E. The optimal dose of ketamine for caudalepidural blockade in children. Anesthesia 1996;51:1170-1172. 12. Mezzatesta JP, Scott DA, Schweitzer SA, Selander DE. Continuous axillary brachialplexus block for postoperative pain relief. Intermittent bolus versus continuous infusion.Reg Anesth 1997;22:357-362.13. Ebert B, Ganser J. [Axillary plexus catheter block in childhood and adolescence].Handchir Mikrochir Plast Chir 1997;29:303-306.14. Eyres RL. Local anaesthetic agents in infancy. Paediatr Anaesth 1995; 5: 213-218.

15. Krane E.J., Dalens B.J., Murat I., Murrell D., et al. The safety of epidurals placedduring general anesthesia [editorial]. Regional Anesthesia and Pain Medicine1998;23:433-438.16. Dalens B, Vanneuville G, Tanguy A. A new parascalene approach to the brachial plexusin children: comparison with the supraclavicular approach. Anesth Analg1987;66:1264-1271.17. McNeely JK, Hoffman GM, Eckert JE. Postoperative pain relief in children from theparascalene injection technique. Reg Anesth 1991;16: 20-22.18. Vongvises P, Beokhaimook N. Computed tomographic study of parascalene block.Anesth Analg 1997;84:379-382.19. Johnson CM. Continuous femoral nerve blockade for analgesia in children with femoralfractures. Anesth Intensive Care 1994;22: 281-283.20. Tobias JD. Continuous femoral nerve block to provide analgesia following femur fracturein a paediatric ICU population. Anesth Intensive Care 1994;22:616-618.21. Maccani RM, Wedel DJ, Melton A, Gronert GA. Femoral and lateral cutaneous nerveblock for muscle biopsy in children. Paediatr Anesth 1995;5:223-227.22. Dalens B, Vanneuville G, Tanguy A. Comparison of the fascia iliaca compartment blockwith the 3-in-1 block in children. Anesth Analg 1989;69:705-713.23. Bouaziz H, Benhamou D, Narchi P. A new approach for saphenous nerve block. RegAnesth 1996;21:490.24. Konrad C, J ِhr M. Blockade of the sciatic nerve in the popliteal fossa: a system forstandardization in children. Anesthe Analg 1998; 87: 1256-1258.25. Ferguson S, Thomas V, Lewis I. The rectus sheath block in paediatric anesthesia: newindications for an old technique ? Paediatr Anesth 1996;6:463-466.26. Courrèges P, Poddevin F, Lecoutre D. Para-umbilical block: a new concept for regionalanesthesia in children. Paediatr Anesth 1997;7:211-214.27. Smith T, Moratin P, Wulf H. Smaller children have greater bupivacaine plasmaconcentrations after ilioinguinal block. Br J Anesth 1996;76:452-455.
Sympathetic blocks in pain management.Hypogastric plexus block
Nagy A. Mekhail, M.D., Ph.D.Director, Pain Management CenterThe Cleveland Clinic FoundationCleveland, Ohio, U.S.A.
AUTONOMIC INNERVATION OF PELVIC VISCERA
Location The superior hypogastric plexus, sometimes referred to as the presacral nerve, is located in the retroperitoneum within loose connective tissue, anterior to the lower portion of the body of the fifth lumbar vertebra, sacral promontory, and upper portion of the first sacral vertebra. Its anterior relations include the bifurcation of the

aorta, both common iliac arteries, the left common iliac vein, and the median sacral vessels.
FormationThe superior hypogastric plexus is formed by the confluence of the lumbar sympathetic chains and branches of the aortic plexus that contains fibers that have traversed the celiac and inferior mesenteric plexuses. In addition it contains parasympathetic fibers that originate in the ventral roots of S2-S4 and travel as slender nervi erigentes (pelvic splanchnic nerves).
BranchesThe superior hypogastric plexus divides into the right and left hypogastric nerves, which descent lateral to the sigmoid colon and rectosigmoid junction, to reach the two inferior hypogastric plexuses. The superior plexus gives off branches to the ureteric and testicular (or ovarian) plexuses, the sigmoid colon, and to the plexus that surrounds the common and internal iliac arteries.
In addition to pathways that traverse the superior hypogastric plexus, sympathetic fibers also reach the pelvis through perivascular pathways that include the inferior mesenteric plexus (sigmoid colon and rectum), and renal plexus (ureteric and ovarian or testicular plexuses). The lumbar and sacral parts of the sympathetic trunks are directly contiguous at the level of the pelvic brim. The sacral sympathetic trunks lie in the parietel pelvic fascia behind the parietal peritoneum and rectum, and on the ventral surface of the sacrum, just medial to its anterior foramina and the exiting sacral nerves. Below, they converge and unite to form a solitary, small "ganglion impar", located anterior to the sacrococcygeal junction.
Presacral NeurectomySurgical interruption of the hypogastric plexus (presacral neurectomy) is a time-honored procedure that has been demonstrated to relieve a variety of painful pelvic conditions, predominantly of nononcologic origin (i.e., dysmenorrhea) as shown by Frier (1965). In one series, presacral neurectomy for chronic pelvic pain (Lee, et al., 1986) showed a success rate of 73% in dysmenorrhea, 77% in dyspareunia, and 63% in other pelvic pains.
Superior Hypogastric Plexus BlockSuperior hypogastric plexus block, a percutaneous procedure that is analogous to presacral neurectomy, has emerged recently as an important option in the management of intractable pelvic pain.
Plancarte (1990) published the first report on using neurolytic superior hypogastric plexus block to treat 28 patients with pelvic pain secondary to cancer [20=cancer of cervix; 4=cancer of prostate; 1=testicular cancer; 3=radiation injury]. His results showed significant pain relief without complications (70% mean reduction of pain scores). Residual pain seemed to be of somatosensory origin and was treated with epidural steroid injections or oral administration of non-narcotic analgesics. A global reduction of pain scores of 90% resulted.
Kent (1992) looked at 26 patients with pelvic cancer who were treated with superior hypogastric block for intractable pain:69% achieved satisfactory, lasting pain relief (VAS decreased from 10/10 to 3/10).31% achieved partial pain relief (VAS reduced from 10/10 to 4-7/10).No complications encountered.
Waldman (1991) and Wechsler (1995) used a computed tomography scan-

guided neurolytic superior hypogastric plexus block for a variety of chronic, painful pelvic conditions
From the previous reports it appears that the superior hypogastric plexus block is an effective way to provide good palliation for visceral pelvic cancer pain.
Indications for Superior Hypogastric Plexus Block1. Pelvic cancer pain arising from one or more of the following pelvic organs
Uterus and upper vagina Bladder, prostate, seminal vesicles and urethra
Sigmoid colon and rectum
2. Pelvic pain secondary to radiation injury3. Sympathetically-maintained pelvic pain, e.g., after rectal anastomosis, APR, etc.
Technique of Superior Hypogastric Plexus Block1. Local anesthesia achieved by:
Local infiltration of skin, subcutaneous tissue and intervening muscles with 1% lidocaine
L4-5 single shot epidural block with 10ml of 1% lidocaine "reduces reflex muscle spasm and ameliorates the discomfort associated with contact of needles with periosteum"
2. Position:
Patient assumes the prone position with padding placed beneath the pelvis to flatten the lumbar lordosis
Lumbosacral region is cleansed aseptically
3. Landmarks:
L4-5 interspace Iliac crest
Skin wheals are raised 5-7 cm bilaterally at the L4-5 interspace level
4. Procedure:A six inch, 22-gauge, short beveled needle is inserted through one of the skin wheals. From a position perpendicular in all planes to the skin, the needle is oriented about 30 degrees caudad and 45 degrees mesiad so that its tip is directed toward the anterolateral aspect of the bottom of the L5 vertebral body. The iliac crest and the transverse process of L5, which sometimes is enlarged are potential barriers to needle passage. If the transverse process of L5 is encountered during advancement of the needle, the needle is withdrawn to the subcutaneous tissue and redirected slightly caudad or cephalad. The needle is readvanced until the body of the L5 vertebrae is encountered or until its tip is observed fluoroscopically to lie at its anterolateral aspect. If the vertebral body is encountered, the needle is withdrawn, and without altering its cephalocaudal orientation, is redirected in a slightly less mesiad plane so that its tip is "walked off" the vertebral body. The needle tip is advanced using the loss of resistance technique. Loss of resistance indicates that the needle tip has traversed the anterior fascial boundary of the psoas major muscle and lies in the retroperitoneal space.

Biplanar fluoroscopy is used during needle passage. Correct needle placement in an anteroposterior view should demonstrate the needle tip locations at the level of the junction of the L5 and S1 vertebral bodies, and lateral views confirm placement of the needle tip just beyond the vertebral body’s anterolateral margin. The injection of a contrast medium is recommended to further verify accuracy of placement and visualize the spread of medications. In the anteroposterior view, the spread of the contrast media should be confined to the paramedian region at the L5-S1 junction. In the lateral view, a smooth posterior contour corresponding to the anterior psoas fascia indicates that the needle depth is appropriate. Alternatively, computerized axial tomography may be used, permitting visualization of vascular structures.
ComplicationsVascular puncture with a risk of subsequent hemorrhage and hematoma formation are possible due to the close proximity of the bifurcation of the common iliac vessels. Intramuscular or intraperitoneal injection may result from an improper estimate of needle depth. Subarachnoid and epidural injection, somatic nerve injury (e.g., obturator, genitofemoral or lumbosacral trunk), and ureteral puncture usually can be avoided by careful observation of technique.
Drugs
Diagnostic hypogastric plexus block: 6-8ml of 0.25% or 0.375% bupivacaine through each needle
Neurolytic hypogastric plexus block: 6-8ml of 6% to 10% phenol dissolved in contrast medium through each needle
Ganglion Impar Block [Ganglion of Walther]The ganglion impar is a solitary retroperitoneal structure located at the level of the sacrococcygeal junction and marks the termination of the paired paravertebral sympathetic chains.Pain arising from disorders of the viscera and somatic structures within the pelvis and perineum is a frequent cause of discomfort and disability, especially among women. The perineum refers to the anatomic area immediately below the pelvis, and is comprised of diverse anatomic structures with mixed sympathetic and somatic innervation. Although various intervention have been proposed for the management of intractable perineal pain, their efficacy and applications are limited by the same factors that complicate the management of pelvic pain. In addition, the target of nerve blocks in this region historically has focused on somatic rather than sympathetic components. Plancarte (1990) introduced the presacral blockade of ganglion impar as an alternative means of managing intractable perineal pain especially those with significant sympathetic component.
SMP of the perineal region is characterized by being:
Vague and poorly localized Accompanied by sensations of burning and urgency
In this first report Plancarte (1990) treated sixteen patients with intractable perineal pain by ganglion impar blockade:
All patients had advanced cancer: cervix=9, colon=2, bladder=2, rectum=1, endometrium=2
All had localized intractable perineal pain in spite of surgery, chemotherapy

and/or radiation
Pain was burning in 8 patients and of mixed character in the rest
After neurolytic block:
8 patients had 100% pain relief
1 patient had 90% pain relief
2 patients had 80% pain relief
1 patient had 70% pain relief
4 patients had 60% pain relief
Block was repeated in two patients for further pain relief
Residual somatic pain was treated with epidural steroid injections or sacral nerve blocks
TechniqueThe patient assumes the prone position with padding beneath the pelvis to flatten the lumbar lordosis. The sacrococcygeal region including the greater intergluteal crease is cleansed aseptically. A skin wheal is raised in the midline at the superior aspect of the intergluteal crease, over the anococcygeal ligament and just above the anus. A standard 22-gauge 3.5 inch spinal needle, which is manually bent to acquire a "C" or "J" shape depending on the length of the coccyx is made. This maneuver facilitates positioning of the needle tip anterior to the concavity of the sacrocyccygeal junction. The needle is inserted through the skin wheal with its concavity oriented posteriorly, and under fluoroscopic guidance is directed anterior to the coccyx, until its tip is observed to have reached the sacrococcygeal junction. Retroperitoneal location of the needle is verified by observation of the spread of 2 ml contrast medium which typically assumes a smooth-margined configuration resembling an apostrophe. Anteroposterior view should demonstrate the tip of the needle is exactly midline. 0.25% bupivacaine is injected for diagnostic purposes, or alternatively 5-7ml 6% phenol is injected for the therapeutic neurolytic blockade.
Under most circumstances, needle placement is relatively straightforward. Local tumor invasion, particularly from rectal cancer, may prohibit the spread of injected solutions.
Unless care is taken to confirm the needle’s postero-anterior orientation, perforation of the rectum or anal canal, or periosteal injection are possible. Also, spread into the epidural space within the caudal canal can be avoided by observing the spread of contrast medium in a lateral view projection.
References
De Leon-Casasola OA, Kent E, Lema MJ: Neurolytic superior hypogastric plexusblock for chronic pelvic pain associated with cancer. Pain 54:145-151, 1993.
Frier A: Pelvic Neurectomy in gynecology. Obstet Gynecol 25:48-55, 1965.
Jain S, Kestenbaum A, Shah N, Khan Y: Hypogastric plexus block: a new

technique for treatment of perineal pain. Anesth Analg 70:S175, 1990.
Kent E, de Leon-Casasola OA, Lema M: Neurolytic superior hypogastric plexus block for cancer related pelvic pain. Regional Anesthesia 17 (suppl):19, 1992.
Lee RB, Stone K, Magelsen D, Belts RP, Benson WL: Presacral neurectomy for chronic pelvic pain. Obstet Gynecol 68(4):517-521, 1986.
Plancarte R, Amescua G, Patt RB, Aldrete JA: Superior hypogastric plexus block for pelvic cancer pain. Anesthesiology 73:236-239, 1990.
Plancarte R, Amescua C, Patt RB: Presacral blockade of the ganglion impar (ganglion of Walther). Anesthesiology 73:A751, 1990.
Plancarte R, et al.: Neurolytic superior hypogastric plexus block for chronic pelvic pain associated with cancer. Reg Anesth 22(6):562-8, 1997.
Waldman SD, Wilson WL, Kreps RD: Superior hypogastric plexus block using a single needle and computed tomography guidance: description of modified technique. Reg Anes 16:286, 1991.
Wechsler RJ, et al.: Superior hypogastric plexus block for chronic pelvic pain in the presence of endometriosis: CT technique and results. Radiology 196(1):103-6, 1995.
Anesthesia for Ankle & Foot SurgerFOOT
SURGERYANESTHESIA FOR ANKLE AND FOO Anatomy and Innervation of the Foot and Ankle Choice of Anesthetic Technique According to the Surgical Procedure Advantages and Limitations of Various Techniques Postoperative Pain Management Special Considerations

Choice of Anesthetic Agents o Popliteal block - lateral approach o Popliteal block - lithotomy approach o Ankle block
Summary References
Regional anesthesia has a lot to offer in lower extremity surgery. The peripheral location of the surgical site in foot surgery and the possibility to block the pain pathways at multiple levels present a clear advantage over general anesthesia techniques. Judiciously and skillfully conducted regional anesthetic can largely prevent hemodynamic disturbances and pulmonary complications of general anesthesia, facilitate postoperative pain management and timely discharge. For instance, anesthesia can be limited to the spinal cord level (spinal and/or epidural anesthesia), major trunks of the sciatic and femoral nerves (sciatic, popliteal and femoral nerve blocks), or to their terminal branches (ankle and metatarsal blocks). This allows one use of regional anesthesia even in patients in whom some regional anesthesia techniques could be contraindicated. For instance, while neuraxial anesthesia may be contraindicated in patients with sepsis and anticoagulation, there are no reports of complications when ankle or popliteal blocks are used in this setting. Similarly, when infection and swelling at the foot and ankle prevents use of the ankle block, surgical anesthesia can be achieved using the sciatic or popliteal blocks with or without the femoral nerve block.
In order to deliver anesthesia in a safe, efficient and competent manner, the selection of a regional anesthetic must be based on site, degree and duration of the operation and the requirement for pain control in the postoperative period. In this review we offer some anatomical considerations for proper selection of regional anesthesia techniques for foot and ankle surgery, and discuss some important aspects, advantages and limitations of the commonly used regional anesthesia techniques in this setting.
Anatomy and Innervation of the Foot and Ankle
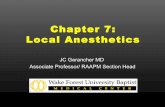
The ankle includes the ankle joint and the surrounding structures. The ankle joint consists of the articulation between the tibia and fibula superiorly, and the talus inferiorly. (Figure 1). The joint is covered with the capsule, stabilizing ligamentous structures and distal projections of the tibia and fibula, which form medial and lateral malleoli respectively. The foot is divided into the hindfoot, midfoot and forefoot (Table 1 and Figure 1). Innervation to the foot and ankle is provided by five separate nerves: saphenous nerve, the longest branch of the femoral nerve and four branches of the sciatic nerve, deep peroneal (anterior tibial), posterior tibial, superficial peroneal,
and sural
Figure 1. Anatomy of the foot and ankle. Legend:1. Tibia2. Fibula3. Tallus4. Calcanous

5. Navicular6. Cuboid7. Cuneiform bones8. Metatarsal bones9. PhalangesRed and blue shaded areas depict hindfoot and midfoot, respectively.
Table 1. Functional division of the anatomical regions of the foot and ankle.
Hindfoot Achilles tendon, calcaneus and talus bones
Midfoot Navicular, cuboid and three cuneiform bones
Forefoot Five metatarsal bones and phalanges
The sciatic nerve gives sensory and motor branches to all structures below the knee except the anteromedial part of the lower leg and foot, which are supplied by the saphenous nerve (Figure 2). In the popliteal fossa the sciatic nerve divides into two main branches: posterior tibial and common peroneal nerves. The common peroneal (lateral popliteal) nerve arises from the posterior part of the sacral plexus(L4-5 and S1-2). The nerve separates from the tibial nerve to descend along the tendon of the biceps femoris muscle and around the neck of the fibula (the nerve is at this level easily palpated and accessible for blockade). Just below the head of the fibula the common peroneal nerve divides into its terminal branches: the deep peroneal and superficial peroneal nerves, both covered by the peroneus longus muscle (Figure 3).
Figure 2. Saphenous nerve emerges just below the medial aspect of the knee and branches into subpatellar branches (1) and long branch (2) to the anterio-medial aspect of the foot. Saphenous vein (3) accompanies the saphenous nerve.

Figure 3. Common peroneal nerve and its terminal branches. Legend:1. Common peroneal nerve2. Superficial peroneal nerve3. Deep peroneal nerve.Peroneus longus muscle removed to exposure the nerves.
The deep peroneal nerve runs downwards below the layers of the peroneus longus, extensor digitorum longus and extensor hallucis longus muscles to the front of the leg (Figure 2). At the ankle level, the nerve lies anteriorly to the tibia and the interosseous membrane and close to the anterior tibial artery. It is usually "sandwiched" between the tendons of the anterior tibial and extensor digitorum longus muscles. Here the nerve divides into two terminal branches for the foot, the medial and the lateral branches. The medial branch passes over the dorsum of the foot, along the medial side of the dorsalis pedis artery, to the first interosseous space, where it divides into two dorsal digital branches for the supply of the first web space between the big toe and the second toe. The lateral branch of the deep peroneal nerve is directed anterolaterally, penetrates and innervates the extensor digitorum brevis muscle and terminates as the second, third and fourth dorsal interosseous nerves. These branches provide the nerve supply to the tarsometatarsal, metatarsophalangeal and interphalageal joints of the lesser toes. The superficial peroneal nerve (also called musculocutanous nerve of the leg) is a branch of the common peroneal nerve. The superficial peroneal nerve gives muscular branches to the peroneus longus and brevis muscles. After piercing the deep fascia covering the muscles, the nerve eventually emerges from the anterolateral compartment of the lower part of the leg and surfaces from beneath the fascia 5-10 cm above the lateral maleolus. Here the nerve divides into terminal cutanous branches: the medial and lateral dorsal cutanous nerves (Figure 4). These branches carry sensory innervation to the dorsum of the foot and communicate with saphenous nerve medially, with deep peroneal nerve (Figure 5) in the first web space and sural nerve on the lateral aspect of the foot.

Figure 4. Superficial peroneal nerve (1) emerges on the lateral aspect of the lower leg and divides into medial (2) and lateral (3) dorsal cutanous nerves.
Figure 5. Deep peroneal nerve (1) emerges on the anterior aspect of the foot between extensor digitorum (2) and extensor hallucis longus (3) tendons. It is accompanied by dorsal pedal artery (4).
The tibial nerve (medial popliteal or posterior tibial nerve) arises from the anterior aspect of L4-5 and S1-3. It separates from the common popliteal nerve at a various distance from the popliteal fossa crease and joins the tibial artery behind the knee joint. The nerve runs distally in the thick neuro-vascular fascia and emerges at the inferior third of the leg, from beneath the soleus and gastrocnemei muscles on the medial border of the Achilles tendon (Figure 6). At the level of the medial malleolus, the tibial nerve is covered by the superficial and deep fasciae of the leg and it is positioned lateral and posterior to the posterior tibial artery, and midway between the posterior aspect of the medial malleolus and posterior aspect of the Achilles tendon.

Figure 6. Tibial nerve at the level of the ankle. Legend:1. Tibial nerve2. Achilles tendon3. Medial malleolus
Figure 7. Plantar nerve (1) divides into medial (2) and lateral (3) plantar nerve.
Figure 8. Sural nerve (1) emerges on the lateral aspect of the achilles tendon 15 cm above the lateral malleolus. The nerve divides into multiple branches (2,3) and innervates the lateral aspect of the foot.
Just beneath the malleolus, the nerve divides into lateral and medial plantar nerves (Figure 7). The posterior tibial nerve provides cutanous, articular and vascular branches to the ankle joint, medial malleolus, inner aspect of the heel and achilles tendon. It also carries the branches to the skin, subcutanous tissue, muscles and bones of the sole. The sural nerve is a sensory nerve formed by the union of the medial

sural nerve - a branch of the tibial nerve - and lateral sural nerve a branch of the common peroneal nerve. The sural nerve courses between the heads of the gastrocnemius muscle and after piercing the fascia covering the muscles, emerges on the lateral aspect of the Achilles tendon, 10 to 15 cm above the lateral mallelus (Figure 8). After giving lateral calcaneal branches to the heel, the sural nerve descends 1-1.5 cm behind the lateral malleolus, anterolateral to the short saphenous vein and on the surface of the fascia covering the muscles and tendons. At this level the nerve supplies the lateral malleolus, Achilles tendon and the ankle joint. The sural nerve continues on the lateral aspect of the foot supplying the skin, subcutanous tissue, fourth interosseous space and sensory innervation of the fifth toe.
Choice of Anesthetic TechniqueAccording to the Surgical Procedure
While limiting the anesthesia to the very periphery of the extremity has obvious advantages over more proximal or general anesthesia techniques, occasionally local factors (infection, swelling) may not permit use of ankle or mid-tarsal blocks. Fortunately, the advantageous anatomy of the lower extremity allows use of neuronal blockade at different levels, as one ascends in the neuronal axis (mid-tarsal level, ankle level, knee level, groin and hip levels, and the spinal/epidural level). Some common surgical procedures and considerations regarding the choice of regional anesthesia techniques are discussed in Table 2.
Table 2. Anesthesia Techniques for Common Foot and Ankle Operations
Surgical
procedureAnesthesia Technique
Remarks
Forefoot*
Hallux valgusMetatarsal, Ankle, Popliteal Block
Block of the surral nerve not necessary for the operation
AmputationsAnkle, Popliteal Block
Popliteal block is the anesthetic of choice whenever swelling or infection prevents reliable ankle block
Midfoot*Transmetatarsal amputations
Ankle, Popliteal Block
Hindfoot*
Ankle arthroscopy
Usually performed under spinal, epidural or general anesthesia
Usually the operation requires good muscle relaxation of the leg for manipulation and traction.
Achilles Tendon Repair
Popliteal block, spinal or epidural anesthesia
Spinal or epidural anesthesia preferredwhenever thigh tourniquet is considered

Ankle fracturesSpinal, popliteal or epidural
Epidural block requires low lumbar blockade L5-S1.
Triple arthrodesis Popliteal Block
Neuroaxial blockade preferred for bone graft harvesting; popliteal blockade for postoperative pain management
Legend: The anesthetic techniques are listed in the order of these authors preference.* Femoral or saphenous nerve block required if the incision extends on the medial part of the foot or ankle.
Advantages and Limitations of Various Techniques
Limiting extent of anesthesia to the most distal neuronal tree has number of potential advantages. First, the more distally the neuronal blockade is approached, the easier is to access the nerves. Secondly, systemic absorption of local anesthetic is of a lesser magnitude when injected peripherally than when the local anesthetics is injected proximally (e.g. epidurally). , Finally, peripheral blocks avoid the cardiovascular, respiratory and other side-effects of neuraxial anesthetics. For that reason, for example, metatarsal block is an excellent choice for most distal operations, especially when muscle relaxation of the calf muscles and tourniquet are not required. This technique provides reliable anesthesia of fast onset for operations on the toes. However, when surgery involves more proximal parts of the foot, ankle or popliteal blocks are better choices. Popliteal block is especially useful when soft tissue swelling and/or infection at the ankle joint are present. Neuroaxial anesthesia also results in excellent surgical conditions for ankle and foot surgery, but attention should be paid to the level of blockade. For instance, epidural anesthesia may fail to produce blockade in the sacral segments unless the needle is inserted at the lower lumbar segments (L5-S1) and larger volumes of local anesthetics are used.
The main disadvantage of peripheral nerve blocks (e.g. popliteal, saphenous, sciatic and/or femoral) for foot and ankle surgery is that these techniques do require some expertise for consistent success rate. For those practitioners with less exposure to these techniques, intravenous regional anesthesia may be better suited. Its simplicity and relatively high success rate make the intravenous regional anesthesia (including the upper extremity) probably the single most common type of regional block practiced in the US. The duration of surgery however, is limited by the tourniquet pain. Therefore, we avoid using this technique for operations that may last longer than 1 hour.
Postoperative Pain Management
Regional anesthesia techniques are also well suited for management of postoperative pain after foot and ankle surgery. Many of the previously discussed peripheral nerve block techniques (with exemption of intravenous regional anesthesia) when used for surgical anesthesia will also provide excellent pain relief for extended period. For example, customary doses of 0.5% bupivacaine for ankle-foot block will give

extended pain control after the operation. Similarly, when 1.5% mepivacaine with bicarbonate and epinephrine is used for popliteal block, analgesia up to 10 hours is frequently observed. The popliteal block can then be repeated using bupivacaine with epinephrine, which frequently results in analgesia for 12-24 hours. Additionally, ankle or popliteal block can also be repeated using lower concentration of bupivacaine (0.25-0.375%).
Prolonged postoperative analgesia can be achieved by using longer-acting local anesthetics for peripheral nerve blocks or adding epinephrine or clonidine to solutions of local anesthetics. For instance, when epinephrine-containing solutions of bupivacaine are used for popliteal or femoral blocks, duration of sensory blockade can easily exceed 12-24 hours. It should be remembered here that epinephrine should not be used for ankle or metatarsal blocks, since there is a risk of foot ischemia. Similarly, combining clonidine with lidocaine (10 mcg/ml) for ankle or metatarsal blocks for foot surgery significantly increases duration and quality of postoperative analgesia. Another option is to repeat neuronal blockade or employ a continuous infusion of local anesthetics through a catheter placed in the epineural sheath of the sciatic (popliteal) nerve.
Special Considerations
Majority of elective foot and ankle operations are performed on an outpatient basis. Ideal anesthetic for ambulatory operations would be administered in a time-wise fashion, without unnecessary delays, and it would provide good intraoperative anesthesia, rapid emergence and uneventful recovery with effective postoperative analgesia. Regional anesthesia with its selective local action offers an excellent anesthetic choice for ambulatory patients. In our institution majority of these operations are performed under popliteal, ankle or metatarsal block, with excellent results. Others have also documented an excellent safety record for regional anesthesia in this setting. Ability to perform the blocks in the holding area prior to surgery allowing fast turnover time, and high patient satisfaction , also add to the value of these techniques in this setting.
Elderly patients, with smaller physiological reserves, higher frequency of concomitant medical problems are also among the greatest beneficiaries of regional anesthesia. The smaller body temperature decrease during operation, smaller blood loss and lesser incidence of ischemia are some examples of advantages of regional anesthesia in this group of patients. However, it should be remembered that local anesthetics may have a more profound effect in the elderly, secondary to slower metabolism, concomitant diseases or intake of medications which interfere with local anesthetic metabolism. Thus, it would be prudent to choose regional techniques which result in lower blood levels of local anesthetics (e.g., peripheral nerve blocks or spinal anesthesia vs. epidural anesthesia).
Another group of patients that is likely to benefit most from regional anesthesia are patients with diabetes mellitus. Reduction of stress response associated with surgery and anesthesia is clearly beneficial in this patient population. For instance, the glucose metabolism in patients with diabetes mellitus remains unaffected after retrobulbar block for eye surgery, whereas considerable disturbance is likely after general anesthesia. Patients with diabetes may have a number of vascular and infectious

complications of long standing disturbances of glucose metabolism, frequently requiring foot surgery (e.g., ulcers, infection, gangrene). At the time of surgery, these patients are often in sub-optimal condition due to sepsis or gangrene, yet the surgery is emergent in nature (toes or foot amputation or debridment). Metatarsal or ankle blocks are frequently difficult to perform or contraindicated in these patients, due to the swelling and tissue acidosis at the ankle area. On the other hand, dehydration and commonly present significant coexistent diseases (coronary artery disease, anticoagulation) may present disadvantage to, or contraindicate neuroaxial anesthesia. In this group of patients the popliteal block with or without saphenous nerve block is an extremely valuable anesthetic option. The newer technique (e.g., lateral approach to popliteal block) makes this approach suitable even in patients that can not assume the prone position, which had traditionally been a prerequisite. It should be noted that when performing a peripheral nerve stimulator-assisted neuronal blockade, diabetes mellitus, sepsis, hypotherma, hypothyroidism and old age all may increase requirements for stimulating current during nerve localization. While duration of neuronal blockade in these patients may also be substantially prolonged, there is no evidence that they are at increased risk of neurologic injury.
Choice of Anesthetic Agents
Choice of local anesthetics and various additives is based on the type of the planned peripheral nerve block or neuraxial anesthesia, duration of the surgical procedure, requirement for continuous postoperative analgesia, and need for ambulation.
With spinal anesthesia, in general, outpatient procedures are best performed using short or intermediate acting local anesthetics. However, because of disturbing reports of transient neurologic irritation after spinal anesthesia with lidocaine regardless of its baricity, lidocaine is nowadays less commonly used. While it remains uncertain whether mepivacaine has any advantages over lidocaine in this respect, hyperbaric bupivacaine, has been shown to have a favorable recovery profile in the outpatient setting, and provides reliable anesthesia of predictable duration. Addition of small doses of fentanyl intrathecally can further augment anesthesia without prolonging the recovery time.
Many local anesthetics can be employed for epidural anesthesia. Nevertheless, we prefer using pH-adjusted 2% lidocaine (1mEq of bicarbonate added per 10 ml of lidocaine) with 1:300,000 epinephrine as an initial bolus. Injection of local anesthetic through the needle as a bolus may shorten the time to onset of the block and enhance the quality of the block. If the surgery extends beyond the duration of the local anesthetic, additional doses of lidocaine or 0.5% bupivacaine may be injected.
For peripheral nerve blocks (except ankle or midtarsal blocks), we prefer using pH-adjusted solutions of 1.5% mepivacaine with bicarbonate and epinephrine 1:200,000. Alternatively, 2% lidocaine can also be used. While short duration and fast onset of action of chloroprocaine is theoretically advantageous for minor procedures in the outpatient setting, , our experience is that this agent does not give adequate dense anesthesia for bone surgery. In patients who are planned for admission, bupivacaine and/or ropivacaine can be added if prolonged postoperative analgesia is desired. Personal bias of these authors is however, that mepivacaine and lidocaine provide the

most consistent surgical anesthesia and that longer-acting agents are best reserved for postoperative pain management.
Ankle block for foot surgery is usually performed using a mixture of 0.5% bupivacaine with 1% lidocaine. This combination of local anesthetic gives fast onset of surgical anesthesia and prolong postoperative analgesia. At the level of the ankle there is no motor nerve supply to the foot other than the intrinsic muscles which stabilize the foot but do not participate significantly during patient ambulation. Thus, one of the advantages of the ankle block is the prolonged sensory block without significant motor blockade. One should remember that with all techniques which are likely to result in a prolong sensory block, it is important to instruct the patients regarding the foot care until the sensation returns.
While major texts of regional anesthesia, as well as many previous issues of this journal are replete with various nerve block techniques, we would like to turn our focus to several newer techniques of lower extremity blocks which are particularly well suited for foot and ankle surgery.
Popliteal block - lateral approach
While the posterior approach to popliteal block has traditionally mandated that patients assume prone position during placement of the block, the lateral technique is performed with a patient in supine position. Leg is extended at the knee joint and the long axis of the foot is positioned at a 90° angle relative to the table. A 100 mm, long insulated short bevel needle, attached to a low-output nerve stimulator is inserted in a horizontal plane 7 cm cephalad to the most prominent point of the lateral femoral epicondyle. The needle is inserted in the groove between the biceps femoris and the vastus lateralis muscles until the shaft of the femoral bone is intentionally contacted (Figure 9).
Figure 9. Popliteal block - lateral approach.The needle is inserted horizontally in the groove between the biceps femoris and the vastus lateralis muscles, 7 cm proximal to the lateral femoral epicondyle. The depth at which the tip of the needle encounters the femur is noted.
Once the femoral bone is contacted, the needle is withdrawn to the skin, and redirected posteriorly at a 30° angle to the horizontal plane (Figure 10). If the sciatic nerve is not stimulated, the needle is withdrawn to the skin and reinserted through the

same skin puncture, first 5 to 10° anterior and then 5 to 10° posterior relative to the initial insertion (30°) plane. If these redirections do not result in nerve localization, the same technique is repeated through new skin punctures in 5mm increments posterior to the initial insertion plane.
Figure 10. Popliteal block - lateral approach.After the femoral shaft is intentionally contacted, the needle is withdrawn to the skin and redirected posteriorly at a 30 degree angle to the initial insertion plane. The popliteal nerve is contacted at a depth 1-1.5 cm beyond the measured skin-femur distance.
After obtaining plantar flexion (tibial nerve), or dorsal flexion (common peroneal nerve) of the foot or toes 40 mL or more of 1.5% alkalinized mepivacaine (1 mEq of NaHCO3 per 30 mL of mepivacaine) with 1:200,000 epinephrine is used. This dose and volume of local anesthetic results in 4 to 6 hours of surgical anesthesia. Bupivacaine 0.25-0.375 % with epinephrine is superior to mepivacaine for postoperative analgesia. Ideally, stimulation of the nerve is achieved using a current of 0.4 mAmp or less. When this is not possible (e.g., diabetic, elderly or septic patients), stimulation of the division of the sciatic nerve that predominantly innervates the surgical area should be obtained. Block of the saphenous (or femoral) nerve is required for surgery involving medial aspect of the leg.
Popliteal block - lithotomy approach
This approach is also performed with a patient in the supine position, but it allows use of the identical landmarks as those used in the posterior approach. The leg is flexed at both hip and knee joints, and supported by an assistant. Anatomical landmarks include: popliteal fossa crease, the semimembranosus and semitendinosus muscles tendons medially, and the long head of the biceps femoris muscle tendon laterally are readily identified in this position (Figure 11). The insulated needle, attached to a peripheral nerve stimulator, is inserted 7 cm above the popliteal crease, at the midline and directed 45 degrees cephalad. When the nerve is not localized on the first insertion, the needle is slowly withdrawn and reinserted laterally 5 to 10 degrees, until the desired response is obtained. If these redirections do not result in nerve localization, the needle is removed and reinserted 5 mm laterally to the initial insertion site

Figure 11. Popliteal block - lithotomy approach.The surface anatomy of the popliteal fossa is accentuated in the in the lithotomy position. Legend:1. Popliteal fossa crease2. Tendons of the semitendinosus and semimembranosus muscles3. Tendon of the biceps femoris muscle4. Midpoint between the biceps femoris and semitendinosus muscle tendons5. The needle is inserted 7 cm above the popliteal fossa crease at the midpoint between the semitendinosus and biceps femoris muscles.
The principles of nerve stimulation, motor response and type and volumes of local anesthetics are otherwise identical to the ones in the lateral approach.
Saphenous or femoral nerve
Saphenous nerve block required for foot and ankle surgery can be performed at multiple levels. Femoral nerve block at the inguinal area invariably results in anesthesia of all branches of the saphenous nerve. If femoral nerve block, however, is not sought, saphenous nerve block can also be accomplished more distally. These approaches include the trans-sartorial approach, or saphenous nerve block at the knee or ankle level (reference). Finally, the terminal branch of the nerve can also be blocked using the midtarsal approach.
Ankle block
Ankle block can be performed at the midtarsal level for operations of the forefoot or at the level of malleoli when surgery involves the midfoot or the heel. It is important to remember that at the foot and ankle level, saphenous, sural and superficial peroneal nerves are superficially located just above the fascia covering the muscles and tendons. Thus, the needle should be inserted tangentially to the skin in order to maintain the course of the needle above the level of the fascia. Additionally, these superficial nerves have highly variable course and multiple branches. Therefore, for their successful block, infiltration of local anesthetic must be done in a ring-type fashion. In contrast, the anterior tibial (deep peroneal) and posterior tibial nerves are located deeper, below the fascial level and usually at the level of tendons and arteries. Therefore the needle should to be inserted perpendicularly to the skin for sub-fascial placement of the needle tip. Contact with bone is frequently necessary to properly identify position of these nerves.
Summary

Several highly efficacious regional anesthesia techniques can be used to provide excellent surgical anesthesia and good postoperative analgesia for foot and ankle surgery. Despite the absence of mounting scientific evidence that regional anesthesia is safer than general anesthesia in lower extremity surgery, it is almost universally accepted that regional anesthesia (peripheral nerve blocks in particular) offers numerous advantages in this setting. By limiting the action of anesthetics to the site of surgical interest, many highly undesirable side-effects of general anesthesia can be avoided. This can especially be important among the ambulatory, diabetic and patients with significant concomitant diseases, where nausea, vomiting, urinary obstruction, orthostatic hypotension and intractable postoperative pain remain the main postoperative challenges, frequently causing unplanned hospital admissions. For that reason, regional anesthesia is undoubtedly the anesthetic of choice for majority of patients undergoing foot and ankle surgery.
References
1. Chung F, Mezei G: What are the factors causing prolonged stay after ambulatory anesthesia? Anesthesiology 89:A3,1998 (abstr)2. Vandermeulen EP, Van Aken H, Vermylen J: Anticoagulation and spinal-epidural anesthesia. Anesth Analg 79:1165-1177, 19943. Hadzic A, Vloka JD, Kitain E: Division of the Sciatic Nerve and its Possible Implications in Popliteal Nerve Blockade. Anesthesiology 85(3A): A733, 1996 (abstr)4. Sharrock NE, Mineo R. Venous levels of lidocaine and bupivacaine after midtarsal ankle block. Reg Anes 17:47-49, 1992.5. Tucker GT, Mather LE: Physicochemical properties, absorption and disposition of local anesthetic agents. In Cousins, M.J., and Bridenbaugh PP (eds): Neuronal Blockade in Clinical Anesthesia and Management of Pain. Philadelphia, PA, J.B. Lippincott, 1988, pp 47-110.6. Sharrock NE, Waller JF, Fierro LE: Midtarsal block for surgery of the forefoot. Br J Anaesth 58:37-40,1986.7. Davies JAH, Walford AJ: Intravenous regional anesthesia for foot surgery. Acta Anaesthesiol Scand 30:145, 1986.8. Nusbaum LM, Hemelberg W. Intravenous regional anesthesia for surgery on the foot and ankle. Anesthesiology, 64:91, 1986.9. Holmes CMcK. Intravenous regional neuronal blockade, in Cousins MJ, Bridenbaugh PO (ed): Neural Blockade in Clinical Anesthesia and Management of Pain. Philadelphia,PA, Lippincott - Raven, 1998, pp 395-409.10. Hadzic A,Vloka JD, Kuroda MM: The use of peripheral nerve blocks in anesthesia practice. A national survey. Reg Anesth Pain Med 23:241-246,199811. Sarrafian SK, Ibrahim IN, Breihan JH: Ankle-foot peripheral nerve block for mid and forefoot surgery. Foot Ankle Int 4:86-90,198012. Reinhart DJ, Wang W, Stagg KS: Postoperative analgesia after peripheral nerve block for podiatric surgery: Clinical efficacy and chemical stability of lidocaine versus lidocaine plus clonidine. Anesth Analg 83:760-5,199613. Singelyn FJ, Aye F, Gouverneur JM: Continuous popliteal sciatic nerve block: an original technique to provide postoperative analgesia after foot surgery. Anesth Analg 84:383-6, 199714. Urmey WF, Stanton J, Sharrock NE: Initial one-year experience of a 97.3% regional anesthesia ambulatory surgery center. Reg Anesth 18:69,199315. Hadzic A, Vloka JD. A comparison of the posterior versus lateral approaches to the block of the sciatic nerve in the popliteal fossa. Anesthesiology 1998;88:1480-6.16. Singelyn FJ, Gouverneur J-M, Gribomont BF. Popliteal sciatic nerve block aided by a nerve stimulator: A reliable technique for foot and ankle surgery. Reg Anesth 1991;16:278-281.17. Emerick TH, Ozaki M, Sessler DI: Epidural anesthesia increases apparent leg temperature and decreases the shivering threshold. Anesthesiology 81:289-298,199418. Sharrock NE, Mineo R, Urguhart B: The effect of two levels of hypotension on intraoperative blood loss during total hip arthroplasty performed under lumbar epidural anesthesia. Anesth Analg 76:580-4,1993

19. Hershey LA: Avoiding adverse drug reactions in the elderly. Mt Sinai J Med 55:244-50,198820. Barker JP, Robinson PN, Vafidis GC: Metabolic control of noninsulin dependent diabetic patients undergoing cataract surgery: comparison of local and general anaesthesia. Br J Anaesth 74:500-5,199521. Vloka JD, Hadzic A, Reiss W: Diabetes Mellitus Increases Current Requirements for Popliteal Nerve Response During Nerve Stimulator-Aided Peripheral Nerve Blockade. Reg Anesth Pain Med 23(3):75,1998 (abstr)22. Schneider M, Ettlin T, Kaufmann M: Transient neurologic toxicity after hyperbaric subarachnoid anesthesia with 5% lidocaine. Anesth Analg 76:1154-7, 199323. Pollock J, Neal J, Stephenson C: Prospective study of the incidence of transient radicular irritation inpatients undergoing spinal anesthesia. Anesthesiology 84; 1361-7, 199624. Freedman JM, Li De-Kun, Drasner K: Transient neurologic symptoms after spinal anesthesia. Anesthesiology 89:633-41,199825. Liu SS, Ware PD, Allen HW: Dose response characteristics of spinal bupivacaine in volunteers: Clinical implications for ambulatory anesthesia. Anesthesiology 85:729-36,199626. Liu s, Chiu AA, Carpenter RL: Fentanyl prolongs lidocaine spinal anesthesia without prolonging recovery. Anesth Analg 80:730-4,199527. Vloka JD, Hadzic A, Mulcare R: Combined blocks of the sciatic nerve at the popliteal fossa and posterior cutaneous nerve of the thigh for short saphenous vein stripping in outpatients: An alternative to spinal anesthesia. J Clin Anesth 9:618-22, 199728. Vloka JD, Hadzic A, Mulcare R: Femoral nerve block versus spinal anesthesia for outpatients undergoing long saphenous vein stripping surgery. Anesth Analg 84:749-52,199729. Vloka JD, Hadzic A, Kitain E: Anatomic Considerations for Sciatic Nerve Block in the Popliteal Fossa Through the Lateral Approach. Reg Anesth 21:414-8,199630. Vloka JD, Hadzic A, Koorn R, Thys DM. Supine approach to the sciatic nerve in the popliteal fossa. Can J Anaesth 43(9):964-967, 1996